complication of extraction
TRANSCRIPT

COMPLICATIONS OF EXTRACTION
Presenter:Pushpa Lal ShahRamesh BasnetRoshan Kumar ShahBDS,2011
1

2
Contents • Complications of extraction• Management of complications• Post-operative care

3
Complication : Any adverse , unplanned events that tend to increase the morbidity above what would be expected from a particular operative procedure under normal circumstances.

4
Classification • Operative complications• Failure of Anesthesia• Problems with tooth being extracted• Injury to adjacent teeth • Extraction of wrong tooth• Fracture of alveolar bone• Fracture of maxillary tuberosity• Maxillary sinus perforation• Gingival and mucosal laceration• Injury to inferior alveolar nerve• Hemorrhage• TMJ trauma
• Post-operative complications• Hemorrhage• Ecchymosis and hematoma• Post-operative pain• Post-operative swelling• Dry socket

5
Failure Of Local Anesthesia
Failure of local anesthesia is usually the result of either:• inaccurate placement of the anesthetic solution• too small a dosage • not waiting long enough for the anesthesia to act before commencing surgery
Check for subjective signs and objective signs to confirm LA has worked.
If anesthesia cannot be secured by using conventional techniques of infiltration or regional block
intraligamental, intraraosseous or intrapulpal injections may be indicated, provided that the cause of the failure is not local infection around the tooth

6
Problems with tooth being extracted• Root Fracture and Displacement• Tooth lost in pharynx

7
Root Fracture and DisplacementPrevention of Root Fracture and Displacement1. Always consider the possibility of root fracture.2. Use surgical (i.e., open) extraction if high probability of fracture exists.3. Do not use strong apical force on a broken root.
Management: open extraction root fragment(5 mm in greatest dimension) is left , lf tooth was
healthy

8
Question???? You are posted at remote place . What would you do if tooth fracture
during extraction and you don’t have time and or facilities required to complete extraction???
Remove any exposed pulpal tissueCover the fragment with zinc oxide eugenol dressing
in which cotton wool fibers are incorporatedArrangement is made for removal of fragments by
own / referred to maxillofacial surgeon

9
Root displaced in the sinus• Mostly in case of 1st PM and buccal roots of 1st molars (maxillary)

10
Management1. Nose blow test to visualize the root2. Placement of suction tip in the socket may aspirate small root fragment3. A long piece of iodoform gauze, ½ inch wide is placed in the antrum through
socket and pulled out in 1 stroke ( sometime removes the root by friction or because it sticks to gauze).
Should be performed only if opening is large, opening should never be enlarged4. If previous methods are ineffective Radiograph is takenMucoperiosteal flap should be raised above the socket/ Caldwell-Luc approachRemoval of rootSocket is closed to avoid creation of oro-antral fistula

11

12
Root displaced in submandibular spaceCause: Root of the 2nd and 3rd molar may be pushed through a perforation in the lingual
surface of the mandible into the region of the submandibular fossa Periapical infection may facilitate root displacement during instrumentation
Management: The index finger of the left hand is inserted onto the lingual aspect of the floor of
the mouth To place pressure against lingual aspect of the mandible and force the root back
into the socket Then be grasp it with the root tip elevator or small hemostatIf this fails, reflect a soft tissue flap on the lingual aspect of the mandible and
gently dissect the overlying mucoperiosteum and remove the root tip Antibiotic prophylaxis

13
Tooth Lost into the PharynxManagement: • Patient should be turned toward the surgeon • Placed into a position with the mouth facing the floor as much as
possible.• The patient should be encouraged to cough and spit the tooth out
onto the floor. • The suction device can sometimes be used to help remove the tooth.

14
If swallowed or aspirated:• Transport to emergency room• chest and abdominal radiographs taken
If the tooth has been aspirated, oconsultation with regard to the possibility of removing the tooth with a
bronchoscope should be requested.oThe urgent management is to maintain the patient’s airway and breathing.oSupplemental oxygen may be appropriate if signs of respiratory distress
are observed.

15
If the tooth has been swallowed,
o It is highly probable that it will pass through the gastrointestinal tract within 2 to 4 days (Because teeth are not usually jagged or sharp, unimpeded passage occurs in almost all situations)
oA radiograph of the abdomen taken to confirm location of the tooth
o Follow-up radiographs are probably not necessary because swallowed teeth are ultimately passed out along with feaces.

16
Injuries to adjacent tooth• Fracture or dislodgement of adjacent restoration• Luxation of adjacent tooth

17
Fracture or dislodgement of adjacent restorationIf a large restoration exists: Patient should be warned about possibility of
fracturing or displacing during extraction.
• Straight elevator should be inserted entirely into the periodontal ligament space, or not used at all to luxate the tooth before extraction
• During elevation a finger should be placed upon the adjacent tooth to support it and enable any force transmitted to it to be detected.

18
Management• The surgeon should make sure the restoration is removed from the
mouth and does not fall into the empty tooth socket
• Once the surgical procedure has been completed, the injured tooth should be treated by replacement of the displaced crown or placement of a temporary restoration

19
Luxation Of An Adjacent Tooth• Caused due to Inappropriate use of the extraction instrumentsPrevention• Judicious use of force with elevators and forceps• Other teeth should not be used as fulcrum for an elevator.• Narrow forceps may be useful for the extraction of tooth that is crowded and
has overlapping adjacent teeth (eg. Mandibular anterior crowding)

20
Management
If an adjacent tooth is significantly luxated or partially avulsed• Reposition in the tooth socket and left alone• Occlusion should be checked to ensure that the tooth has not been displaced into a
hyperocclusion and traumatic occlusion
If the luxated tooth is mobile• The tooth should be stabilized with semirigid fixation to maintain it in its position• For this a simple silk suture that crosses the occlusal table and is sutured to the
adjacent gingiva is usually sufficient
(NOTE: Rigid fixation with circumdental wires and arch bars should be avoided because it results in increased chances for external root resorption and ankylosis of the tooth.)

21
• Occur as a result of uncontrolled forces.
• Usually occurs when buccolingual forces inadequately mobilize a tooth, excessive tractional forces are used or both
• Tooth is suddenly released from the socket and the forceps strikes the teeth of the opposite arch, chipping or fracturing a cusp
• Mostly occur with extraction of lower teeth because these teeth may require more vertical tractional forces for their delivery, especially when using cowhorn forceps.
Injury of Teeth in the opposite arch

22
Prevention• Avoid using excessive tractional forces• The surgeon or assistant should hold a finger or suction tip against
them to absorb the blow of the forceps released in that direction.
Management• The tooth should be smoothed or restored ,as necessary, to keep the
patient comfortable until a permanent restoration can be constructed.

23
Extraction of the Wrong Tooth
Causes• A dentist removes a tooth for another dentist• Use of differing tooth numbering systems• Differences in the mounting of radiographs
Prevention• Focus attention on the procedure.• Check with the patient and the assistant to ensure that the correct tooth is
being removed.• Check, then recheck, images and records to confirm the correct tooth

24
Management
Immediately• The tooth should be replaced quickly into the tooth socket • Splinting is done• Endodontic treatment after successful reattachment

25
Fracture of alveolar bone
Prevention• Conduct thorough preoperative clinical and radiographic
examinations.• Do not use excessive force.• Use surgical ( i.e. open) extraction technique to reduce the force
required.

26
Management1. If bone has been completely removed from the tooth socket along
with the tooth :- tooth is not replaced - sharp margin should be smoothed - soft tissue should be positioned and sutured
2. If bone remain attached to the periosteum:- - bone is separated from tooth and left attached to overlying soft tissue -tooth is removed -bone and soft tissue flap are re approximated and sutured
27
• What would be the sequence of extracting 1st PM , Canine and lateral incisor ?1. 1st PM , Canine and lateral incisor 2. Lateral incisor , canine and 1st PM3. Canine , 1st PM and lateral incisor
WHY?

28
Fracture of the maxillary tuberosity
• Most commonly occur due to extraction of maxillary 3rd molar/ 2nd molar , if it is the last tooth in the arch.
Management• If the bone remains attached to the periosteum:-should take measures to ensure the survival of the fractured bone.

29
• If the tuberosity is excessively mobile and cannot be dissected from the tooth:
Option 1: • Splint the tooth being extracted to adjacent teeth • Defer the extraction by 6 to 8 weeks (allowing time for bone to heal)• The tooth is then extracted with an open surgical techniqueOption 2 :• Section the crown of the tooth from the roots• Defer the extraction of the roots by 6 to 8 weeks( allowing time for the
tuberosity and root section to heal )• Remove the tooth roots

30
If the maxillary tuberosity is completely separated from soft tissue
oSmooth the sharp edges of the remaining bone oReposition and suture the remaining soft tissueoCheck for an oro-antral communication (if present provide the necessary
treatment)
Advice:• If this occur patient should be warned this could occur in next similar
extraction• If preoperative radiograph reveals such possibility extract tooth by careful
dissection

31
Maxillary sinus Perforation• Predisposing factor:Presence of large antrumReduced bone heightRoots of maxillary molars(divergent) and premolars approaching antrum
Prevention is best management
But how• Preoperative radiographs• Decision is made to extract tooth either by closed/open technique• In closed technique: never apply excessive apical force Leave apical one third of the palatal root of molars if it is retained unless there is
positive indication of extraction• If indicated undergo open extraction

32
Management :
Diagnosis Presence of bone on apex of root Nose-blowing test
what to do After the diagnosis of oroantral communication has been established or a strong suspicion exists???????
If the communication is small (2 mm in diameter or less)No additional surgical treatment is necessaryMeasures to ensure the formation of a high-quality blood clot in the socketadvise the patient to take sinus precautions to prevent dislodgment of the blood clot.

33
Sinus precaution• Avoid blowing the nose, sneezing violently, sucking on straws, and
smoking
Patients who smoke and who are unable to stop (even temporarily) should be advised to take only small puffs, not deep drags
• Surgeon must not probe through the socket into the sinus with a dental curette or a root-tip pick
34
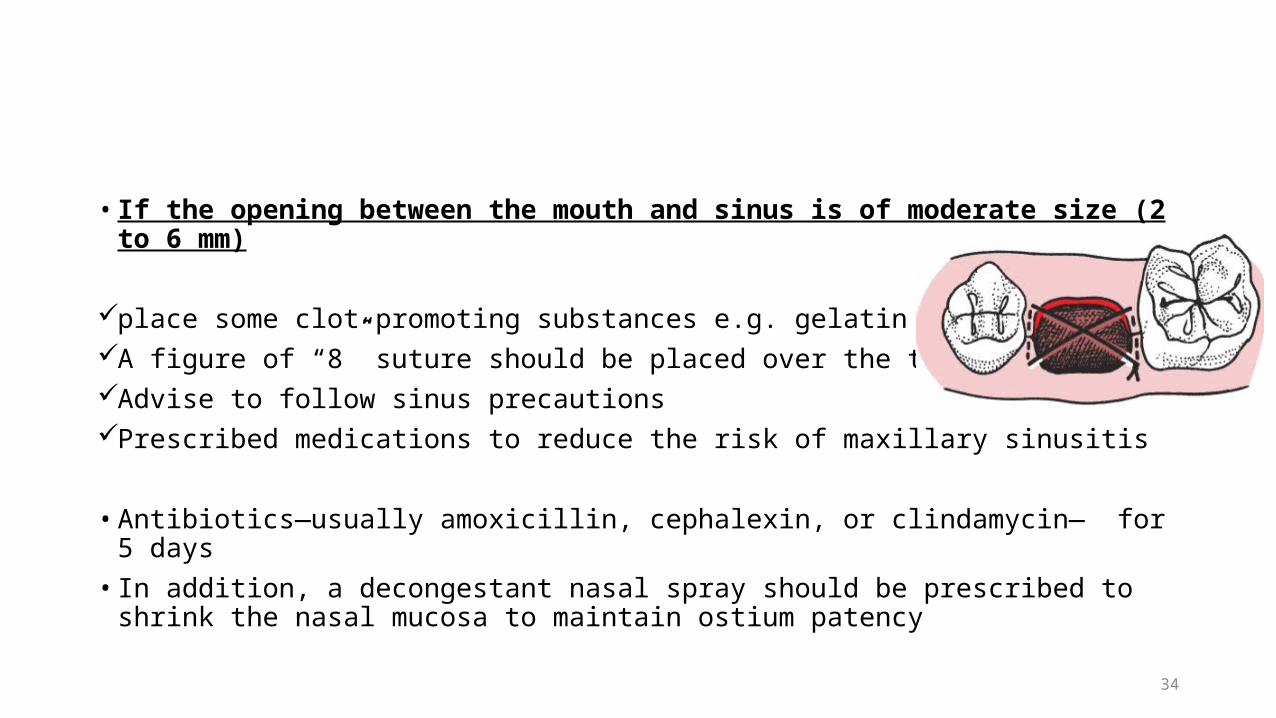
• If the opening between the mouth and sinus is of moderate size (2 to 6 mm)
place some clot-promoting substances e.g. gelatin spongeA figure of “8” suture should be placed over the tooth socketAdvise to follow sinus precautionsPrescribed medications to reduce the risk of maxillary sinusitis
• Antibiotics—usually amoxicillin, cephalexin, or clindamycin— for 5 days• In addition, a decongestant nasal spray should be prescribed to shrink the nasal
mucosa to maintain ostium patency

35
• If the sinus opening is large (7 mm or larger):
Repair with buccal and with a flap Advise to follow sinus precautionsPrescribed medications to reduce the risk of maxillary sinusitis
• Antibiotics—usually amoxicillin, cephalexin, or clindamycin— for 5 days• In addition, a decongestant nasal spray should be prescribed to shrink the nasal mucosa
to maintain ostium patency
Follow up after 2 weeks

36
Mandible fracture Rare
Causes Removal of deeply impacted mandibular 3rd molar Removal of teeth from a severely atrophic mandible Application of excess force that needed to remove a tooth
Management Treated by methods applied for treating jaw fractures

37
Gingival and mucosal lacerations
Causes• Mostly in difficult and complicated extractions.• Usually an indication of faulty technique or selection of the wrong
method of extraction.
Management• Most injuries heal without complication – because of remarkable
resistance of the tissues. • Wound cleansed for any foreign matter.

38
Injury of the inferior alveolar nerve
Causes• Uncommon occurrence in the extraction of erupted mandibular teeth. • Injudicious curettage or improper use
of elevators to remove root apices.
• Result in paresthesia and sometimes anesthesia of half the lower lip and chin.

39
Management• Most cases - the nerve regenerates within 6 weeks to 6
months.• If the nerve does not regenerate, the bony walls of the
mandibular canal may have been displaced, impinging on it.• This condition sometimes can be remedied by a
decompression operation.• Traumatic neuroma – excised and the nerve reanastomosed
or grafted.

40
Hemorrhage
Cause• Due to the accidental tearing or cutting of a large artery or vein.• More often, it is encountered in regions of inflammation where tissues are
excessively hyperemic.
Management• Arrested generally by manual pressure on gauze pack placed over the area.
• If large vessel involved – clamped with a hemostat and tied with 3-0 catgut suture.

41
Subcutaneous emphysemaCauses• Air forced into the connective tissue of intramuscular or facial spaces.• Most often after air-driven dental hand piece or a compressed air
spray bottle for irrigation.
• Swelling – rapid onset, elastic consistency.• Such air is absorbed very slowly, in 1 to 2 weeks, and no treatment is
needed.

42
TMJ trauma• If the jaw is inadequately supported during the extraction of mandibular
molars, patient may experience : - Pain in TMJ - dislocation
Prevention• Controlled force and adequate support to the jaw• Use of a bite block on contralateral side aid in mandible stabilization.
Management• Moist heat, resting the jaw, a soft diet, and 600 to 800 mg of Ibuprofen every
4 hours for several days• 500 to 1000mg of Acetaminophen

43
Management of TMJ dislocation

44
Postoperative Care• Satisfactory recovery – surgeon’s responsibility.
• Main purpose – expedite healing and prevent or relieve pain and swelling.

45
Rest• For prompt healing of wounds.
• No strenuous exercise should be performed for the first 12 to 24 hours after extraction because the increased blood pressure may result in greater bleeding.• A malpositioned gauze pack is not effective in controlling bleeding
because the pressure of biting is not precisely directed onto the socket.

46
DietWhen should one start eating???
• Only liquids and soft solids – 1st day.• Warm or cold food.• Chewing form the unoperated side.• Increased fluid intake to prevent dehydration from limited food
intake.
Why to give specific diet instructions???

47
Oral hygiene• Advice to keep their teeth and the whole mouth clean - for rapid
wound healing.• On the day of surgery – gently brush the teeth that are away from the
area of surgery -Prevent a new bleeding episode -Avoid disturbing sutures and -Avoid inducing pain• After a day – rinsing should begin.• Half tea spoon of salt in a glass of warm water.• Commercial mouthwash??

48
Pain• Begins after the effects of anesthetic have left.
• Intermittent application of cold to surgical site during 1st 24 hours helps to reduce pain in two ways:-Diminishes nerve conduction and thereby has an anesthetic effect-Helps to reduce swelling and thus decreases pain associated with tissue distention.
• Small doses of an analgesic drug at short intervals rather than large doses infrequently.

49
Swelling• Direct proportion to the degree of surgical trauma.• 1st step to reduce swelling – Careful handling of the tissues.• Application of cold to the operated site – Produce vasoconstriction
and thereby reduces the exudation of fluid and blood into the tissue spaces.• Prolonged use – Compensatory vasodilation.• Pressure dressing are also beneficial.• After 24 to 48 hours – heat in the form of moist compresses.

50
Smoking• Increase the incidence of alveolar osteitis.• Tobacco smoke and nicotine interfere with wound healing.• Discontinued for 5 days.

51
POST OPERATIVE COMPLICATIONS

HEMORRHAGE
• PRIMARY HEMORRHAGE
• SECONDARY HEMORRHAGE

LOCAL CAUSES
• Trauma• Mechanical dislodgement of the clot• Damage to blood vessel or soft tissue• Fracture of alveolar bone• Damage to nutrient blood vessel• Infection • Presence of granulation tissue• Chronic inflammation of gingiva• Acute infection of bone and soft tissue

• Local abnormality • Unusually large bone marrow space• Presence of Hemangioma
SYSTEMIC CAUSES• Disorder related to systemic disease• Leukemia, Aplastic anaemias• Platelet disorders: Thrombocytopenia• Coagulation defects : Hemophilia
• Structural malformation : Hereditary Hemorrhagic Telengectesia• Drug therapy: Aspirin, Anti coagulant therapy

Management• Pressure packs• Use of LA solution with vasoconstrictors• Socket suturing• Hemostatic forceps• Splints• Thermal measures- cautery , hot saline packs

Firm gauze roll should be placed upon the socket & patient asked to bite upon it .
Horizontal mattress suture

ECCHYMOSIS AND HEMATOMA• Mild ecchymosis especially in elderly patient with increased capillary
fragility and poor tissue elasticity
• Extensive ecchymosis and hematoma formation result from improper hemostasis during surgery

Management
• Intermittent ice pack(30 min per hour )for the 1st 24 hour after surgery
• Following which intermittent hot moist packs are used to resolve the
condition
• Patient should be advised that discoloration is from bleeding into the tissues and is not a bruise or a gangrenous process.
Postoperative painDue to traumatized hard tissues - Bruising of bone during instrumentation or overheating of bur during bone
removal.
Soft tissues :-Ragged flap – heals slowly (incision not proper)Soft tissue become entangled with bur Proper Retraction

Postoperative swelling • EDEMA : 1. If the soft tissues are not handled carefully during an
extraction traumatic edema may be formed.2. The use of blunt instrument, the excessive retraction of badly
designed flap, or a bur becoming entangled in the soft tissues predispose to this condition.
3. IF sutures are tied too tightly post operative swelling due to edema or haematoma formation may cause sloughing of the soft tissues and breakdown of the suture line.
4. Usually both conditions regress if the patient uses hot saline mouth baths frequently for 2-3 days.

b. INFECTION :-
• Pain and swellingMild - hot saline mouth baths Severe – antibiotic & analgesics

Management
• External hot moist packs for 20 min/hour• Warm isotonic saline mouth rinse every 3-4 hours and the use of antibiotics.

Dry socket / alveolar osteitis / alveolitis sicca dolorosa
• Condition in which there is loss of the blood clot from the socket
• Initially the clot has a dirty grey appearance and then it disintegrates
• Ultimately leaving a grey or greyish yellow bony socket bare of granulation tissue
• Diagnosis :
• Gently pass a small probe into the extraction wound
• Bare bone, extremely sensitive
• Suppuration generally absent

• Foul odor is present
• Severe radiating pain usually described as throbbing ache
• The symptoms generally start on the 3-5 day after extraction of tooth
• If untreated will last for about 7-14 days

Nitzan’s hypothesis of dry socket
• Suggested that fibrinolytic activity was due to organisms like Treponema
denticola , Bacteroid Melaninogenicus and Bacteroid oralis

Birn’s Hypothesis of Dry Socket• Most accepted explanation of dry socket till date
Trauma and inflammation causes release of stable tissue activator from the adjacent bony socket and soft-tissues
Tissue activator converts plasminogen (present in the blood clot) to the plasmin

Predisposing factors :-
1. Infection of socket : release of plasminogen activators2. Trauma - use of excessive force3. Vasoconstrictors (contributory factor)4. Mandibular extractions (dense & less vascular,
contaminated with food debris)5. Bacteriological origin – Treponema denticolum .6. Pt. on oral contraceptives, smokers

ETIOPATHOGENESIS

Clinical features• Pt. usually presents within 2-4 days : granulation tissue appears in 2-4 days,
it is absent in cases of dry socket.
• Dull, boring pain to severe throbbing pain, may radiate Gingival margin of socket – swollen & red
• Socket may be filled with food debris or a brown friable clot on removal of which exposes the bare bone which is severely tender to touch
• Regional lymph nodes may be tender
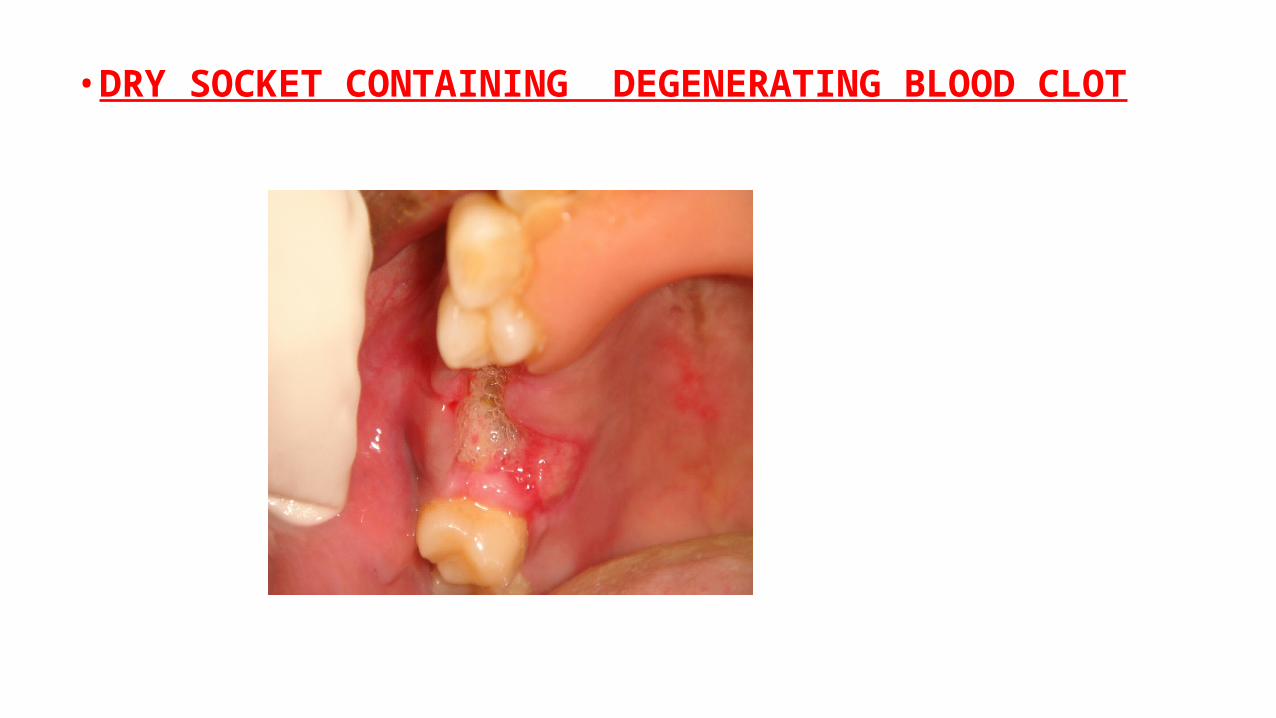
• DRY SOCKET CONTAINING DEGENERATING BLOOD CLOT

Prevention :-1. Scaling & any gingival inflammation – (1 week prior to
extraction).2. Antiseptic mouth wash before extraction3. Minimum amount of local anesthetic
4. Atraumatic tooth removal 5. Prophylactic use of antibiotics especially metronidazole 6. Nerve blocks preferred to LA infiltrations7. Irrigation of extraction socket8. Warm saline rinse

Management1. Aim – relief of pain & speeding of resolution
2. Socket irrigation with warm saline & all degenerating blood clot removed.
3. Sharp bony spurs - excised with rongeur forceps or removed with a wheel stone
4. Loose dressing – zinc oxide & oil of cloves on cotton wool is tucked into the socket.
5. Analgesic tab & hot saline mouth baths
6. Recall after 3 days

73
CONCLUSION• Prevention of complications should be a major goal of the surgeon.
• Complications should be diagnosed as soon as they occur & dealt promptly and effectively.
• The surgeon who anticipates a reasonable probability of an unusual specific complication should inform the patient.

74
REFERENCES• Howe Geoffrey L. The Extraction of Teeth. 2nd edition• Oral And Maxillofacial Surgery , vol.2, Daniel M. Laskin• CONTEMPORARY ORAL AND MAXILLOFACIAL SURGERY, 6th edition• Exodontia Practice, Abhay N. Datarkar