complications of intravenous therapy
DESCRIPTION
Complications of Intravenous Therapy. Principles of IV Therapy ADN136 Fall Qr 09. Complications of IV Therapy. Nursing assumed the role of intravenous therapy in the 1940’s Application of the nursing process is critical in the prevention of complications - PowerPoint PPT PresentationTRANSCRIPT
Complications of Intravenous Therapy
Principles of IV Therapy
ADN136
Fall Qr 09
Complications of IV Therapy Nursing assumed the role of intravenous
therapy in the 1940’s Application of the nursing process is critical
in the prevention of complications 90% of hospitalized patients receive IV fluids
and medications
Complications of IV Therapy Classified according to their location
Local complication: at or near the insertions site or as a result of mechanical failure
Systemic complications: occur within the vascular system, remote from the IV site. Can be serious and life threatening

Local complications
Occur as adverse reactions or trauma to the surrounding venipuncture site
Assessing and monitoring are the key components to early intervention
Good venipuncture technique is the main factor related to the prevention of most local complications associated with IV Therapy.
Local complications include: hematoma, thrombosis, phlebitis, postinfusion phlebitis, thrombophlebitis, infiltration, extravasation, local infection, and veno spasm.
Hematoma Hematoma and ecchymosis demote
formations resulting from the infiltration of blood into the tissues at the venipuncture site Related to venipuncture technique Use of large bore cannula: Trauma to the vein
during insertion Patients receiving anticoagulant therapy and long
term steroids
Hematoma Subcutaneous hematoma is the most common
complication Can be a starting point for other complications:
thrombophlebitis and infection Related to:
Nicking the vein Discontinuing the IV without apply adequate pressure Applying the tourniquet to tightly above a priviously
attempted venipuncture site.
Hematoma Signs and symptoms:
Discoloration of the skin Site swelling and discomfort Inability to advance the cannula all the way into
the vein during insertion Resistance to positive pressure during the lock
flushing procedure
HematomaPrevention
Use of an indirect method Apply tourniquet just before venipuncture Use a small need in the elderly and patients
on steriods, or patients with thin skin. Use blood pressure cuff to apply pressure Be gentle
HematomaTreatment
Apply direct, light pressure for 2-3 minutes after needle removed
Have patient elevate extremity Apply Ice
Document
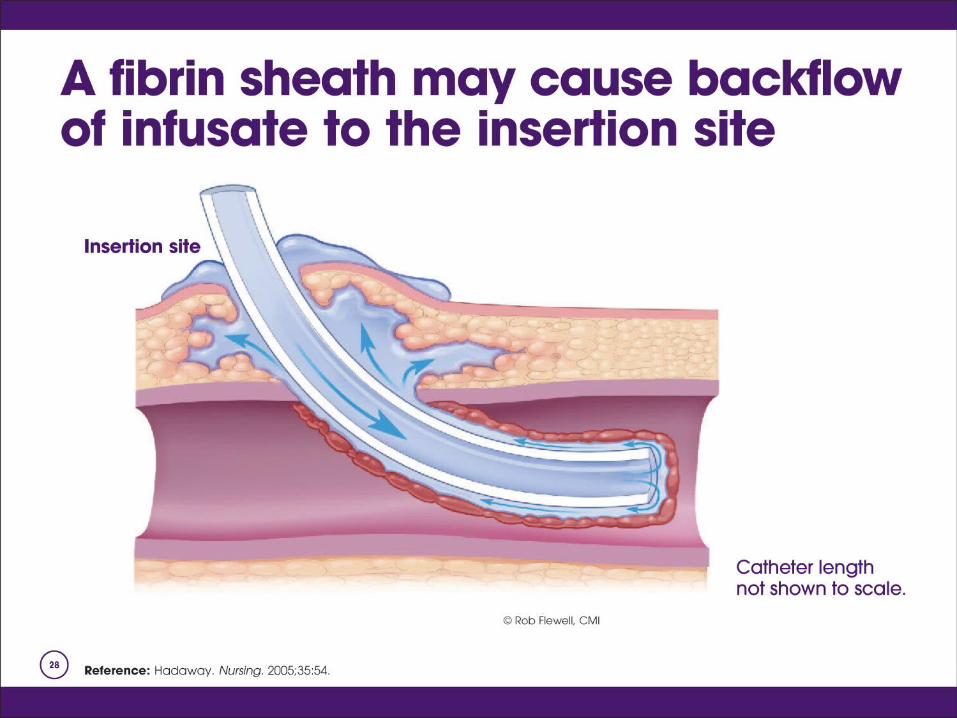
Thrombosis Catheter-related obsturctions can be
mechanical or non-thrombotic Trauma to the endothelial cells of the venous
wall causes red blood cells to adhere to the vein wall, forms a clot or Thrombosis
Drip rate slows, line does not flush easily, resistance is felt
Never forcible flush a catheter
ThrombosisTypes of Thrombus or occlusion
Persistent withdrawal occlusion Partial occlusion Complete occlusion Fibrin tail Fibrin sheath Mural thrombosis

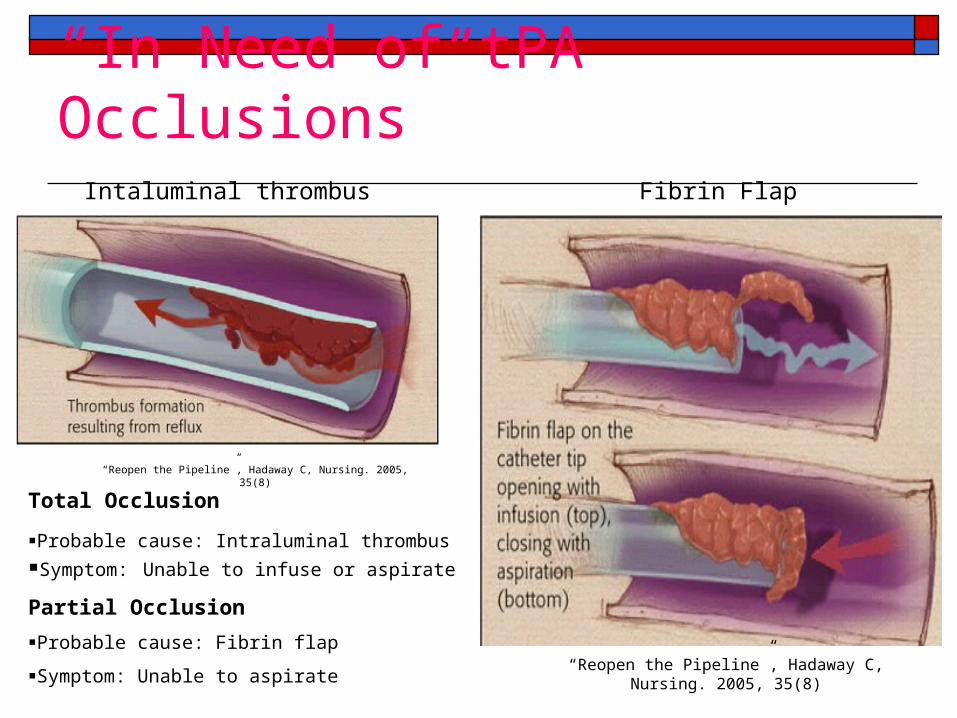
“In Need of tPA Occlusions”
“Reopen the Pipeline”, Hadaway C, Nursing. 2005, 35(8)
“Reopen the Pipeline”, Hadaway C, Nursing. 2005, 35(8)
Fibrin FlapIntaluminal thrombus
Total Occlusion
Probable cause: Intraluminal thrombus Symptom: Unable to infuse or aspirate
Partial Occlusion
Probable cause: Fibrin flap
Symptom: Unable to aspirate
ThrombosisTypes of Thrombus or occlusion
Thrombosis related to: Hypertensive pt; blood backing up Low flow rate Location of the IV cannula Compression of the IV line for an extended
period of time Trauma to the wall of the vein
Thrombosis Signs and Symptoms
Fever and Malaise Slowed or stopped infusion rate Inability to flush
Prevention Use pumps and controllers to manage flow rate Microdrip tubing for rate below50mL/hr Avoid areas of flexion Use filters Avoid lower extremeties
Thrombosis Treatment
Never flush a cannula to remove an occlusion Discontunue the cannula Notify the physician and assess the site for
circulatory impairment
Document
Phlebitis Inflammation of the vein in which the
endothelial cells of the venous wall become irritated and cells roughen, allowing platelets to adhere and predispose the vein to inflamation-induced phlebitis Tender to touch and can be very painful
Phlebitis Mechanical:
To large a catheter for the size of the vein Manipulation of the catheter: improper stabilization
Chemical: vein becomes inflamed by irritating or vessicant solutions or medication Irritation medication or solution Improperly mixed or diluted Too-rapid infusion Presence of particulate matter
Phlebitis Chemical (cont):
The more acidic the IV solution the greater the risk
Additives: Potassium Type of material Length of dwell:
30% by day 2, 39-40% by day 3 (Macki and Ringer)
The slower the rate of infusion the less irritation
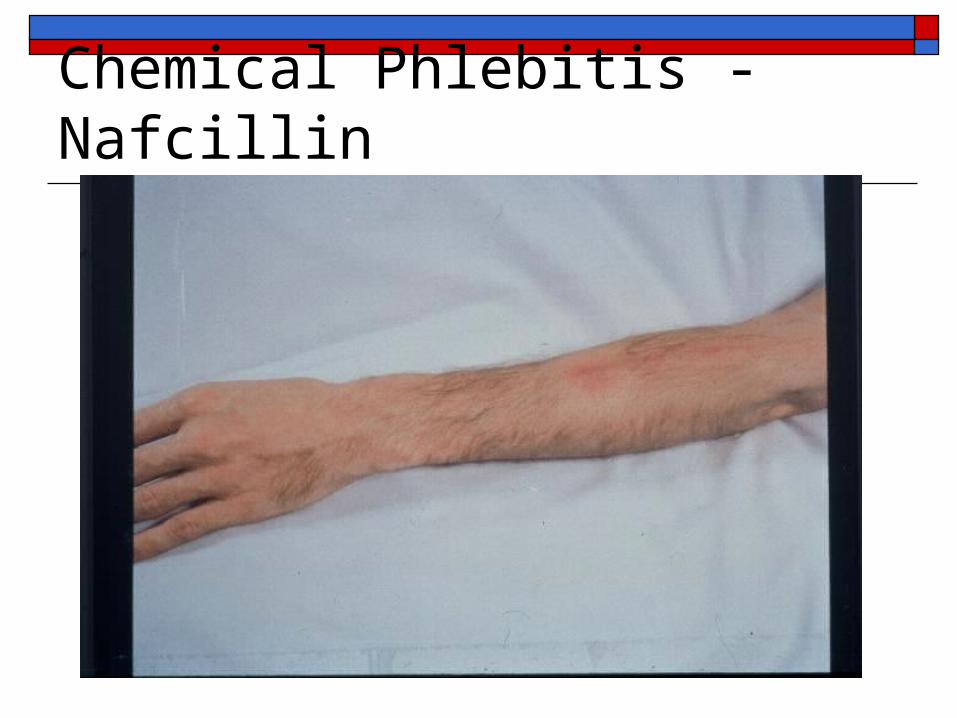
Chemical Phlebitis - Nafcillin
PhlebitisBacterial
Also called Septic phlebitis: least common Inflammation of the intima of the vein Contributing factors
Poor aseptic technique Failure to detect breaks in the integrity of the equipment Poor insertion technique Inadequate stabilization Failure to perform site assessment Aseptic preparation of solutions Hand washing and preparing the skin
PhlebitisPostinfusion
Inflamation of the vein 48-96 hr after discontinued Factors that contribute:
Insertion technique Condition of the vein used Type, compatibility, pH of solution used Gauge, size, length, and material Dwell time Infrequent dressing change Host factors: age, gender, age and presence of disease
Phlebitis Immune system causes leukocytes to gather at
the inflamed site Pyrogens stimulate the hypothalamus to raise
body temperature Pyrogens stimulate bone marrow to release
more leukocytes Redness and tenderness increase
Phlebitis Signs and Symptoms
Redness at the site Site warm to touch Local swelling Palpable cord along the vein Sluggish infusion rate Increase in basal temperature of 1degree C or more
Prevention Use larger veins for hypertonic solutions Central lines for Infusions lasting longer than 5 days
Phlebitis Scale 0 – No clinical symptoms 1- Erythema at access site with or without pain 2- Pain at access site, with erythema and / or edema 3- Pain at access site with erythema and / or edema,
streak formation, and palpable venous cord 4- Pain at access site with erythema and / or edema,
streak formation, palpable venous cord > 1 inch, purulent drainage


Thrombophlebitis Thrombophlebitis denotes a twofold injury:
thrombosis and inflammation Related to:
Use of veins in the lower extremity Use of hypertonic or highly acidic infusion
solutions Causes similar to those leading to phlebitis
Thrombophlebitis Signs and Symptoms
Sluggish flow rate Edema in the limbs Tender and cord like vein Site warm to the touch Visible red line above venipuncture site Diminished arterial pulses Mottling and cyanosis of the extremities
Thrombophlebitis Prevention
Use veins in the forearm rather than the hands Do not use veins in a joint Assess site q 4 hr in adults, q 2 hr in children Catheter securment Infuse at rate prescribed Use the smallest size catheter to do the job Proper dilution
Thrombophlebitis Septic thrombophlebits can be prevented:
Appropriate skin preparation Aseptic technique in the maintance of infusion Proper hand hygiene
60% from patients skin 35% from the line itself 5% from hands
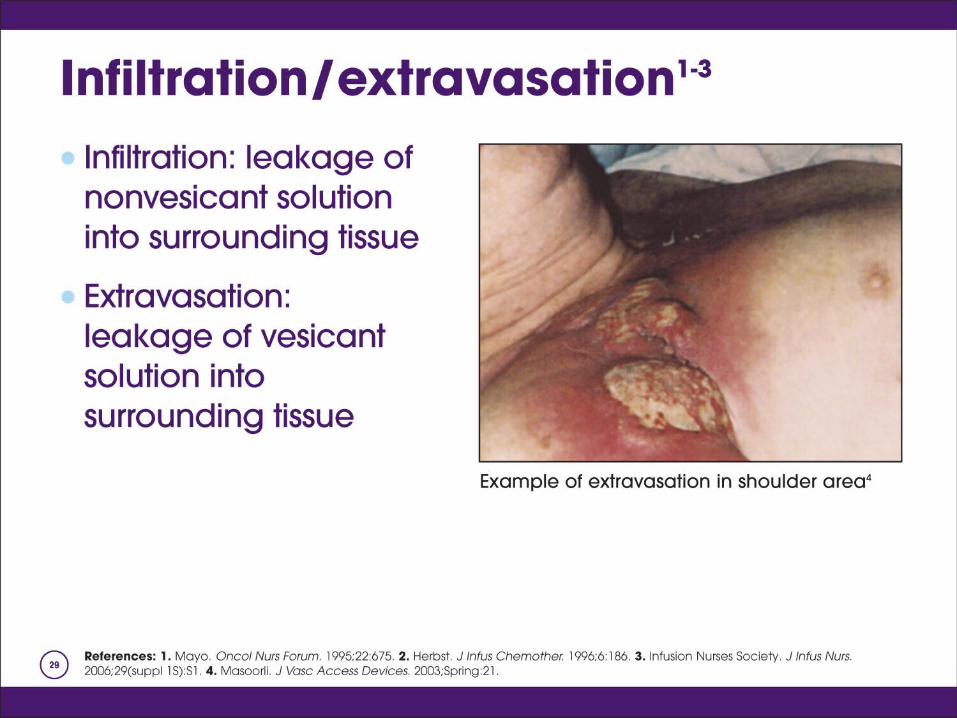
Infiltration The inadvertent administration of a non-
vesicant solution into surrounding tissue Dislodgment of the catheter from the vein Second to phlebitis as a cuase of IV therapy
morbidity
Infiltration Related to:
Puncture of the distal vein wall during access Puncture of the vein wall by mechanical friction Dislodgement of the catheter from the intima of
the vien Poor securment High delivery rate Overmanipulation
Infiltration Signs and Symptoms
Coolness of the skin around site Taut skin Dependent edema Absence of blood return “Pinkish” blood return Infusion rate slows
Infiltration Complications fall into 3 catagories
Ulceration and possible tissue necrosis Compartment syndrome Reflex sympathetic dystrophy syndrome
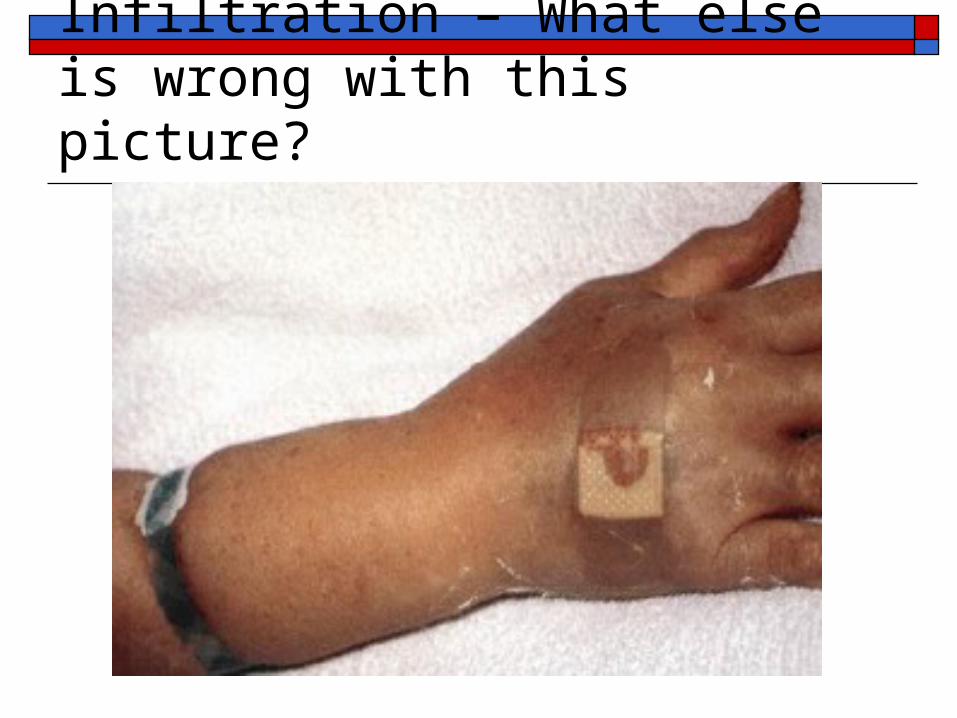
Infiltration – What else is wrong with this picture?
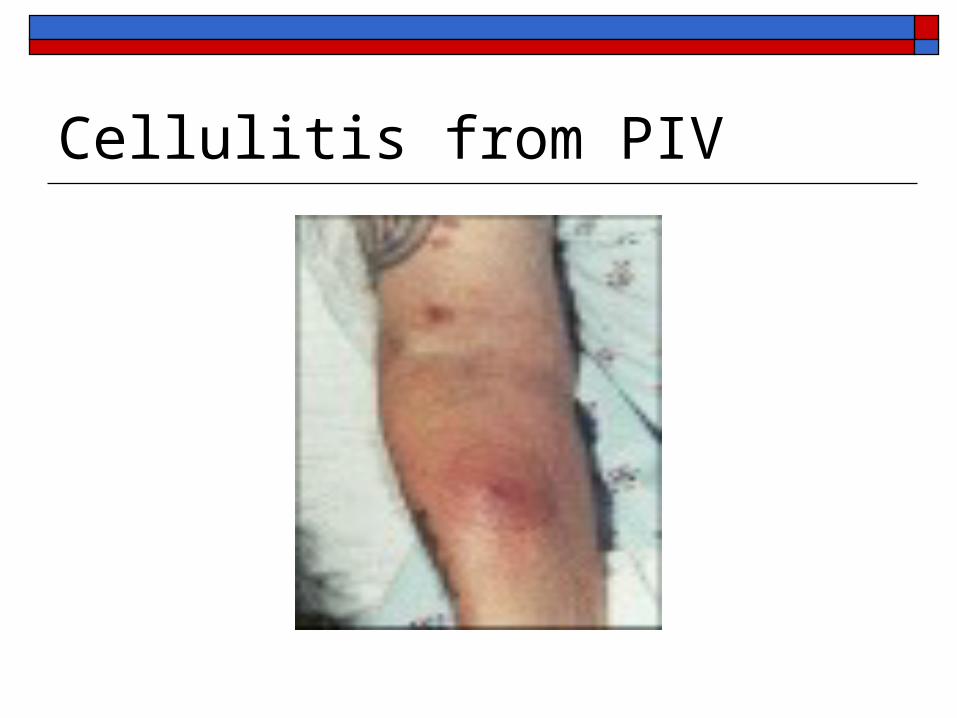
Cellulitis from PIV
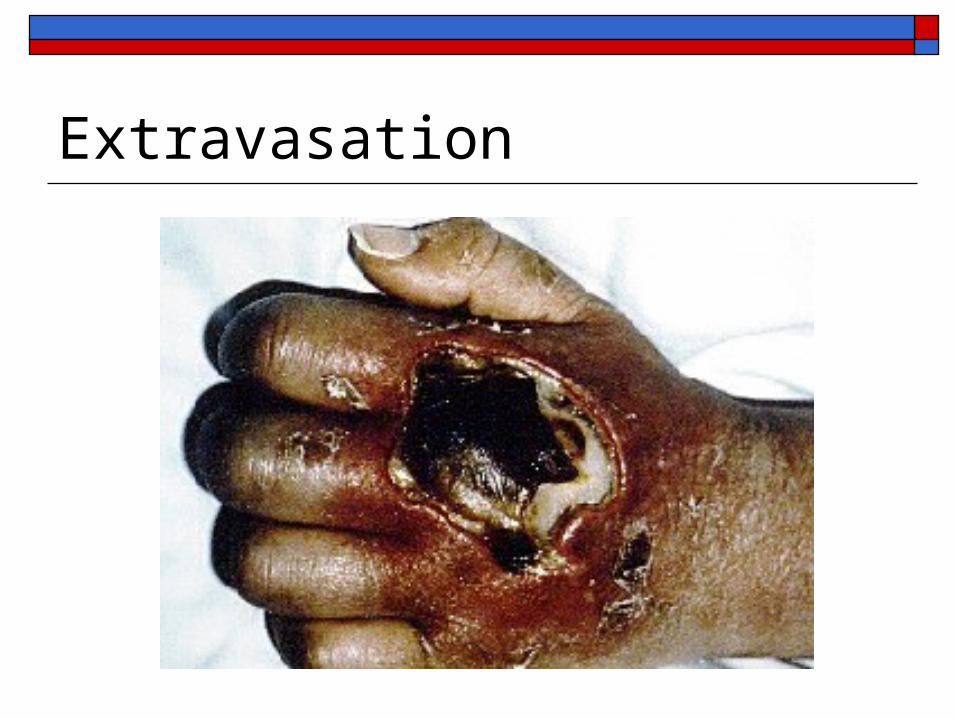
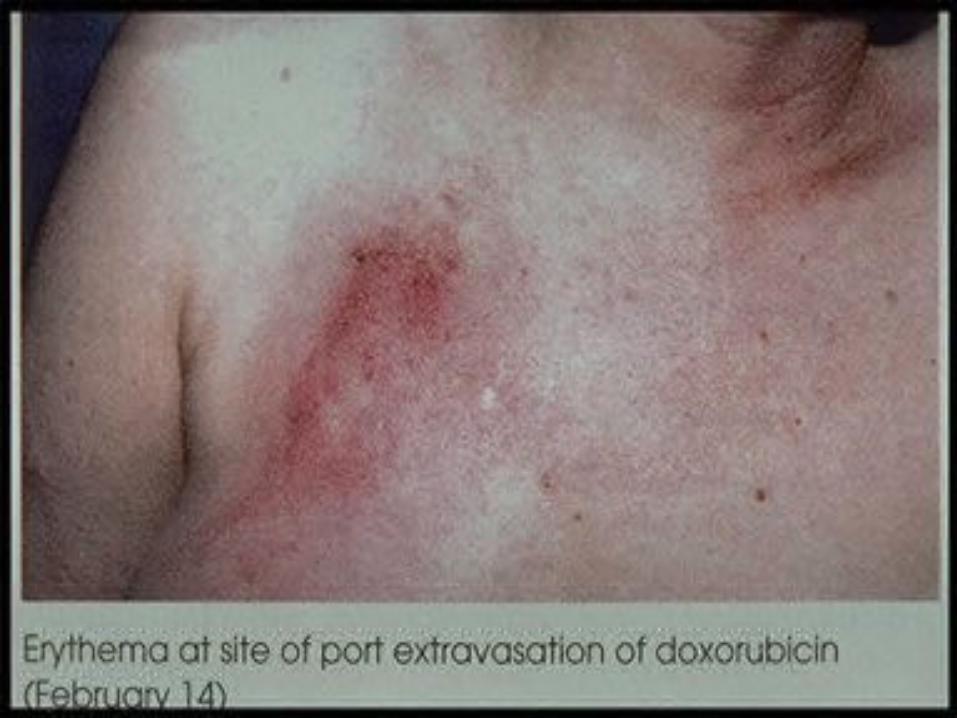
Extravasation Inadvertent administration of a vesicant
solution into surrounding tissue Vesicant is a fluid or medication that causes the
formation of blisters, with subsequent sloughing of tissues occurring from the tissue necrosis
Extravasations related to: Puncture of the distal wall Mechanical friction Dislodgement of the catheter
Examples of Vesicants Phenergan pH is 4 to 5.5 Dilantin pH is 12 (Drano has a pH of 14) High concentration KCL pH is 5 to 7.8 Calcium gluconate pH is 6.2 Amphotericin B pH is 5.7 to 8 Dopamine pH is 2.5 to 5 Nipride pH is 3.5 to 6 10%, 20% or 50% dextrose pH is 3.5 to 6.5 Sodium bicarbonate pH is 7 to 8.5
Extravasations Signs and Symptoms
Complaints of pain or burning Swelling proximal to or distal to the IV site Puffiness of the dependent part of the limb Skin tightness at the veinpuncture site Blanching and coolness of the skin Slow or stopped infusion Damp or wet dressing
Extravasations Prevention:
Use of skilled practitioners Knowledge of vesicants Condition of the patients veins Drug administration technique
If continuous give in CVAD Only with brisk blood return of 3-5 cc Use of a free flow IV Do not use a pump on vesicants given peripherally Assess for blood return frequently
Extravasations (cont) Prevention (cont)
Site of venous access Condition of the patient
Vomiting, coughing, retchin Sedated Unable to communicate
Treatment
Extravasation
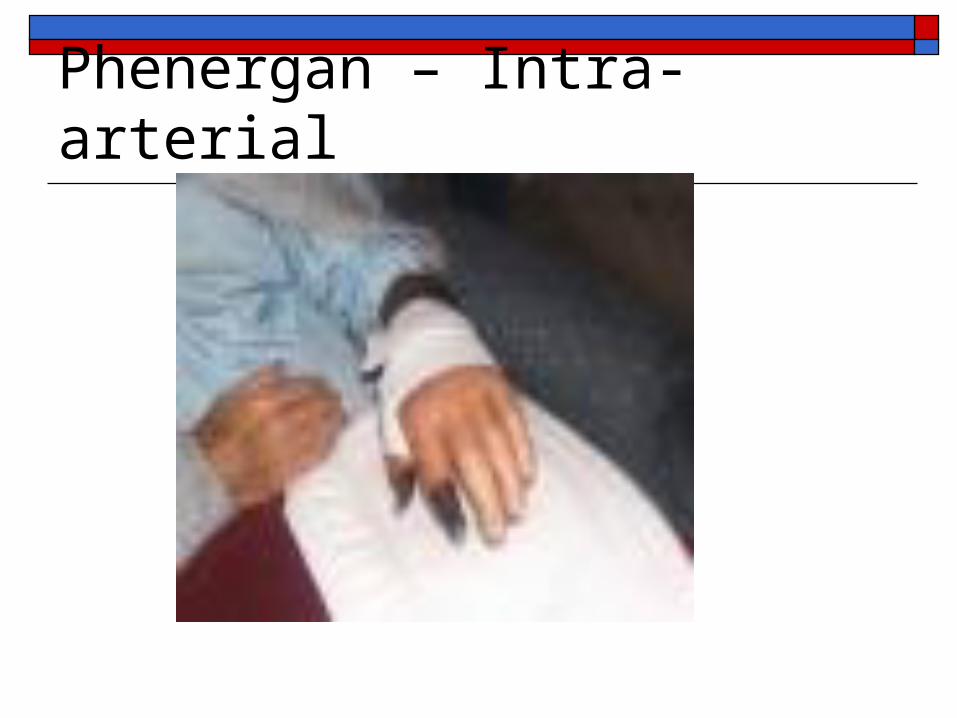
Phenergan – Intra-arterial

Phenergan Intra-arterial

Dilantin Extravasation








Other Complications Local infection:
Microbial contamination of the cannula or the infusate
Thrombus becomes infected Venous Spasm: a sudden involuntary
contraction of a vein or an artery resulting in temporary cessation of blood flow through a vessel
Systemic Complications We will cover when we talk about Central
Venous Access Devices