complications of radiation therapy to the head and neck · complications of radiation therapy to...
TRANSCRIPT

Complications of Radiation Therapy to the Head and Neck
Donita Dyalram DDS, MD Assistant Professor
Associate Program Director Maxillofacial Oncology/Microvascular Surgery
Department of Oral Maxillofacial Surgery University of Maryland

Lecture Goals • Understand the use of Radiation in H&N • Early effects • Late effects • Dental Implications • Treatment protocol for:
– Candidiasis – Xerostomia – Dental Extractions in irradiated Jaw – Implants in the irradiated Jaw

Radiotherapy • Therapeutic radiation is
delivered by 2 main methods: – Electromagnetic (photons):
x-rays, gamma rays – Particulate radiation
• Electrons • Protons • Neutrons
• Depth of penetration required is the main criterion used in choosing which energy to employ

Radiotherapy
• Roentgenmeasure of ionization in air – Used for radiation safety
• Gray (Gy)
– Dose absorbed by the tissue (clinically relevant) – 1 Gy = the absorption of 1 joule/kg – 1 Gy = 100 cGy = 100 rad
• There is no absolute resistance to radiation
– Normal tissue tolerance limits the dose

Radiotherapy – Brachytherapy
• Radium • Cesium • iridium

Radiotherapy • Mechanism of action
– Interacts with atoms and molecules of the cells
– Produces free radicals – Damages DNA – Affects all phases of the
cell cycle but cells going mitosis are most affected
Radiation • The sensitivity of cells to radiation is most pronounced
shortly before and during mitosis; thus, the effect is greatest in rapidly dividing cells.
• Highly radiosensitive tissues are mucosa, skin, bone marrow, nerve, and muscle tissue.
• Of the bone cells, osteoblasts are more radiosensitive than are osteoclasts and osteocytes.
What orofacial tissues are affected by Radiation therapy?
• Oral mucosa • Skin • Subcutaneous tissue • Cartilage • Muscles of mastication • Temporomandibular joint • Teeth • Oral flora • Salivary glands • Nasolacrimal drainage system • Bone • Thyroid and parathyroid glands • Pituitary gland • Peripheral and cranial nerves • Lymphatics • Paranasal sinuses

Tissue Effect – Early • Acute skin reactions
• Hyperemia
• Reduced salivary gland
function
• Mucositis
• Loss of taste

8 weeks post radiotherapy

Tissue Effect – Long Term
• Seem not to occur when the tissues are
exposed to less than about 45 Gy
• Chronic damage to skin, muscle, nerves, and bone
• Seem not to occur when the tissues are
exposed to less than about 45 Gy
• Chronic damage to skin, muscle, nerves, and bone

Mucositis
• A term given for widespread oral erythema, ulceration and soreness

Mucositis
• Presents with: – Pain – Erythema – Ulceration – Bleeding
Mucositis World Health Organization Toxicity Grading
Grade Clinical features 0 - 1 Soreness/erythema 2 Erythema, Ulcers but able to eat solids 3 Ulcers, but requires liquid diet 4 Oral alimentation not possible
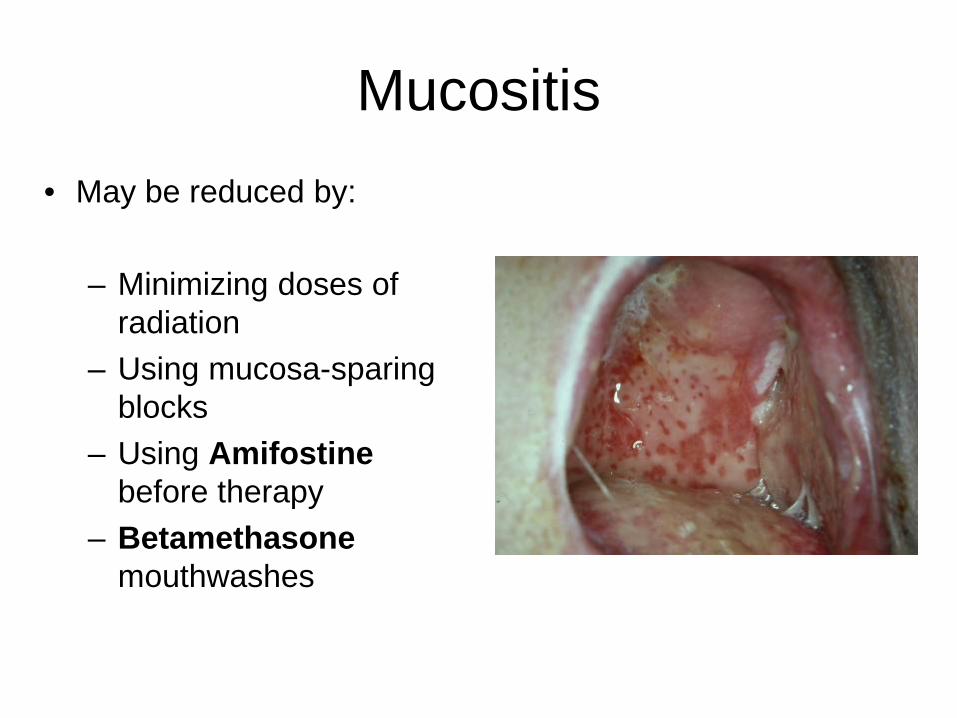
Mucositis • May be reduced by:
– Minimizing doses of
radiation – Using mucosa-sparing
blocks – Using Amifostine
before therapy – Betamethasone
mouthwashes

Mucositis • Opioids (MSO4 etc..) • Avoiding irritants (smoking, spirits, or spicy foods) • Good oral hygiene • Oral cooling using ice chips • Topical analgesics (especially before meals)
– 2% lidocaine solution mouthwash – Magic Mouth Wash
• Benadryl, Mylanta, and Carafate and viscous lidocaine in a 1:1:1:1

Mucositis
• The time to healing depends on the dose intensity and is usually complete within 3 weeks after the end of treatment.

Candidiasis
Candidiasis
• Infections by Candida albicans are commonly seen in irradiated patients
• Can be painful
Candidiasis
•Rinses
•Nystatin
•Amphotericin
• Clotrimazole (Mycelex) trouches
•Caution trouches contain sugars
•Oral/Systemic medications
•Diflucan

Xerostomia
Xerostomia
• Salivary Gland – Transient tenderness – Occasionally swelling – Occurs within a few hours after 1st dose – Decrease salivary flow noted within 24 hrs – May have ~50% decrease flow after 1st wk – Flow continues to decrease throughout treatment
course and may become barely measurable at 6 wks.
RTOG 96-04 LENT Study

Xerostomia
• Salivary changes – Increased viscosity – Decrease pH – Increased [Na], [Ca], [Mg] – Decreased [HCO3] – Decreased IgA
RTOG 96-04 LENT Study

Xerostomia • Persists for several months to year • May not recover • Depends on volume of radiated salivary glands,
total dose, individual patient • Causes difficulty with:
– Swallowing – Chewing – Talking – Denture wear

Xerostomia • Prevention
– IMRT – Amifostine (Ethyol)
• Cytoprotective agent
– RTOG 0244 • Phase II study of submandibular gland transfer to the
submental space prior to therapy
– RTOG 97-09 • Phase II study to test the efficacy of the prophylactic use of
oral pilocarpine to reduce hyposalivation and mucositis. Closed. No improvement in mucositis but improved salivation

Xerostomia - Treatment
• Sialogogues • Pilocarpine (Salagen) 5 mg tid • Salivix (Malic acid)
• Salivary replacements • Glandosane • Luborant • Oralbalance • Salivace • Saliveze

Radiation Caries • Circumferential
cervical decay • Incisal decay
• Related to:
– Xerostomia • Change in oral flora • Pulpal death • Dentine dehydration • Enamel loss
Prevention of Radiation Caries • Daily flouride
application • 0.4% stannous flouride
gel • 1.1% neutral sodium
flouride • Tray worn for 5-10
minutes • Must cover cervical
portion of teeth

Osteoradionecrosis ORN

Pathophysiology of ORN • Watson & Scarborough (1938) • Meyer (1970)
– Triad: • Radiation Therapy • Local trauma • Infection
• Marx’s Theory – 3 H’s
• Hypovascular • Hypocellular • Hypoxic
What is the Incidence of ORN?
• Recent studies
– 5% to 15% – overall incidence of 5.4% – Bimodal distribution
• 12 months and 24-60 months
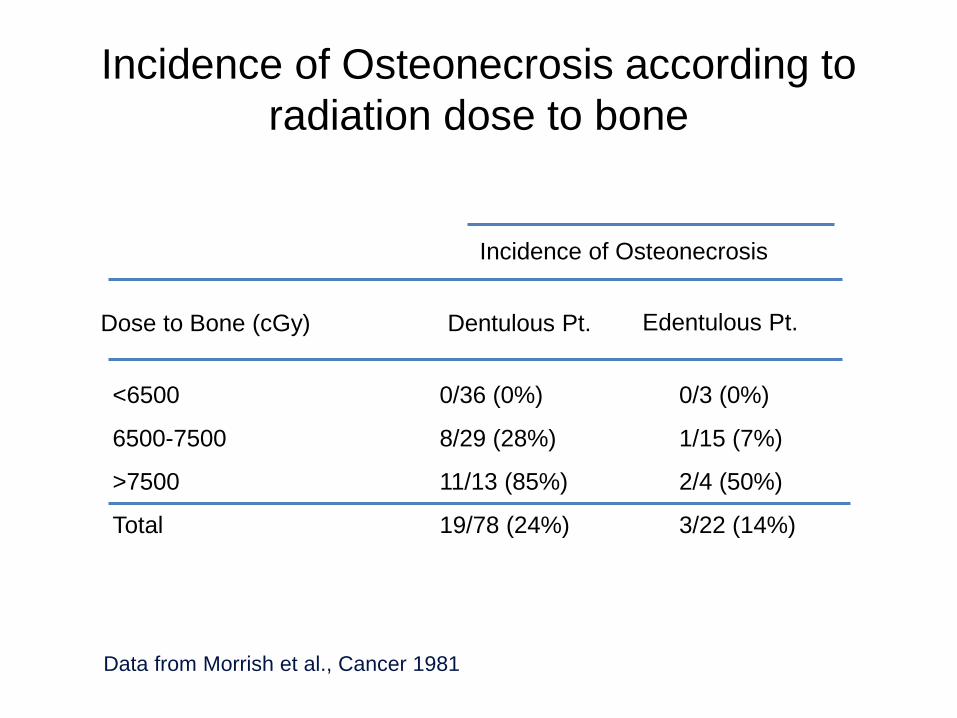
Incidence of Osteonecrosis according to radiation dose to bone
Edentulous Pt.
Incidence of Osteonecrosis
Dose to Bone (cGy) Dentulous Pt.
<6500
6500-7500
>7500
Total
0/36 (0%)
8/29 (28%)
11/13 (85%)
19/78 (24%)
0/3 (0%)
1/15 (7%)
2/4 (50%)
3/22 (14%)
Data from Morrish et al., Cancer 1981

Osteoradionecrosis
• Almost all cases occur within the field of radiation
• Most cases associated with a dental extraction

Osteoradionecrosis
Thorn JJ et al. JOMS 2000
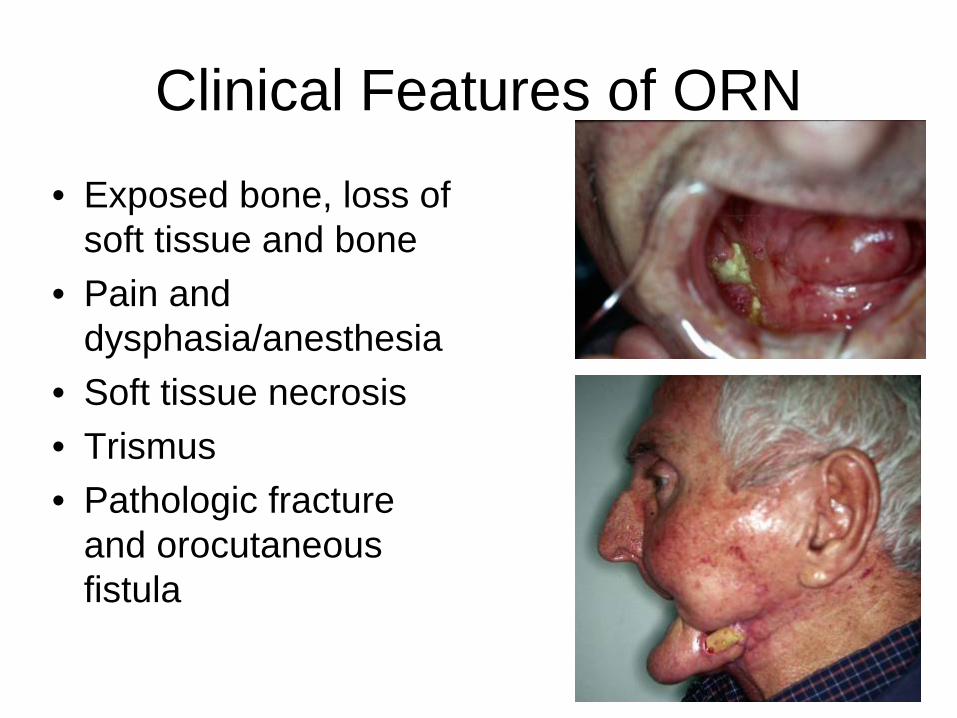
Clinical Features of ORN • Exposed bone, loss of
soft tissue and bone • Pain and
dysphasia/anesthesia • Soft tissue necrosis • Trismus • Pathologic fracture
and orocutaneous fistula

Radiographic Features of ORN • Diffuse radiolucency
without sclerotic demarcation
• CT / MRI to evaluate extent of ORN
• Must Biopsy to rule out tumor recurrence
Conservative Management of ORN
• Daily local irrigation (saline, NaHCO3, Chlorhexidine)
• Systemic antibiotics • Avoidance of irritants • Good oral hygiene instructions • Gentle removal of sequestrum

HBO • Administration of 100%
oxygen in a special chamber at 2.4 atmosphere absolute pressure for 90 minutes each session.
• Delivered once a day, 5 times per week
What is the Mechanism of HBO • Improve tissue healing
by: – Angiogenesis – Inducing fibroplasia and
neocellularity – Promoting survival of
osteoprogenitor cells – Promoting the formation
of functional periosteum

Controversies regarding use of HBO in ORN
• Hyperbaric Oxygen Therapy for Radionecrosis of the Jaw: a randomized, placebo-controlled, double-blind trial from the ORN96 study group.
• Annane D, Depondt J, Aubert P, Villart M, Gehanno P, Gajdos P, Chevret S • J Clin Oncol 2004 Dec 15; 22(24): 4893-900
Conclusion: Patients with overt mandibular osteoradionecrosis did not benefit from hyperbaric oxygenation

HBO and Osteoradionecrosis
• The influence of HBO on the outcome of patients treated for osteoradionecrosis:8 year study
• 23 patients • HBO group – 12.5% cure rate • Non-HBO group – 86% cure rate
• D’Souza et al. IJOMS 2007

ORN – Fibrosis Theory
• Damage to bone caused by radiation induced fibrosis
• Bone cells damaged by free radicals , acute inflammation and chronic activation of fibroblasts
Lyons A, Ghazali N Br J Oral Maxillofac Surg 2008

Treatment ORN– Fibroblast Activation Theory
• Pentoxifyline – Vasodilator – Anti -TNFα – Inhibits dermal fibroblasts
• Vitamin E
– Anti-oxidant – Reduce free radical damage
Delanian S et al. Int J Radiat Oncol Biol Phys 2010

ORN treatment failure

Fibula Osteocutaneous Free Flap

ORN treatment failure

Dental Management Pre-Radiation

Dental Management Prior to Radiation
• Complete oral/dental examination and treatment plan
• Any necessary extraction and surgery • Maintenance of teeth and caries control • Restoration of restorable teeth • Prothetic examination to prevent postradiation
trauma from ill-fitting dentures

Dental Management Prior to Radiation
• Consider: – Condition of the
dentition – Level of oral hygiene
and patient attitude – Age of the patient – Radiation field and
dose – Urgency of radiation
treatment

Dental Management Prior to Radiation
• Caries control – Prophylactic care before and at the end of
therapy – Oral hygiene instructions – Daily administration of fluoride – Weekly follow-up during therapy and every 3-4
weeks afterward
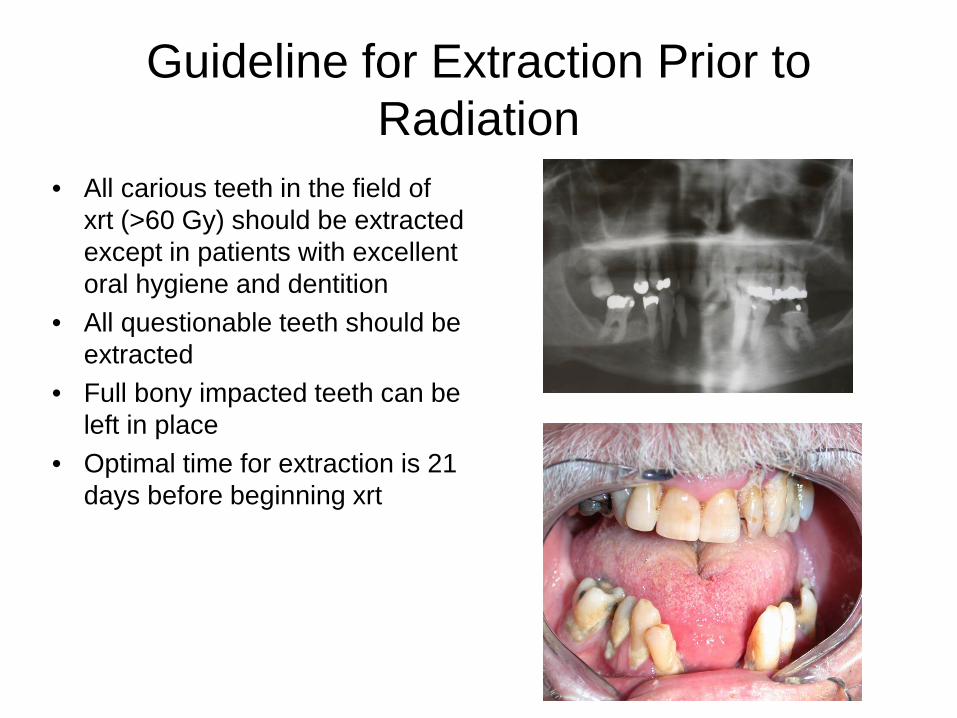
Guideline for Extraction Prior to Radiation
• All carious teeth in the field of xrt (>60 Gy) should be extracted except in patients with excellent oral hygiene and dentition
• All questionable teeth should be extracted
• Full bony impacted teeth can be left in place
• Optimal time for extraction is 21 days before beginning xrt
Extractions
• Atraumatic extractions • perform an alveolectomy • smooth the bone • Perform a primary closure • Allow a minimum of 1 week to 10 days for
healing prior to beginning XRT • Preferable to allow 14 to 21 days

Dental Management Post-Radiation

Management of patient post radiation
• Obtain records of radiation fields and dose
• Recall for prophylaxis q 3 months
• Daily fluoride treatment for life
• Wait for mucositis to resolve prior to prosthesis placement
• Avoid invasive procedure involving irradiated bone
• HBO vs. Pentoxifylline & Vitamin E

Implants in Irradiated Jaw

• 48 patients • 271 implants placed • Implant survival
– 1 year (99%) – 10 year (72%)
• Higher incidence of implant failures – Maxilla – Posterior oral cavity
• Conclusion – Dental implants placed into irradiated bone have a
higher failure rate than non-irradiated bone
Buddha A. et al. Clin Implant Dent Relat Res 2010

• HBO for irradiated patients who require dental implants: a Cochrane review of randomised clinical trials
• 1 trial found • 26 patients HBO vs. non-HBO
• Conclusion – no evidence for or against
effectiveness of HBO for improving dental implant outcomes
Coulthard P et al. Eur J Oral Implantol 2008

Radiation induced Malignancies
Radiation induced Malignancies
• Soft tissue Sarcomas • Thyroid Carcinoma
