computed tomography in acute posterior fossa infarcts · cpa, and pm cisterns, hydrocephalus, cct:...
TRANSCRIPT

Fong Y. Tsai 1. 2
James S. Teal 1. 3
Grant B. Heishima4
Ch i-Shing Zee 1
Verity S. Grinnell 4
C. Mark Mehringer4
Hervey D. Sega l1 1
Received August 13. 1980; accepted after revision October 22, 1981.
' Department of Radiology. Los Ange les County-Universi ty of Southern Californi a Medica l Center , Los Ange les, CA 90033.
' Present address: Department of Radiology, University of Ca li forn ia Irvine Medica l Center , 10 1 City Dr. S., Orange, CA 92668. Add ress reprin t requests to F. Y. Tsai.
3Present address: Department of Rad iology, Howard University Hospital, Washington, DC 20060.
' Department of Rad iology, Harbor GeneralUniversity o f California at Los Angeles Medical Cen ter , Torrance, CA 90509.
AJNR 3:149- 156, March / April 1982 0 195-6108 / 82 / 0302-0149 $00.00 © American Roentgen Ray Society
Computed Tomography in Acute Posterior Fossa Infarcts
149
Thirty-one cases of acute posterior fossa infarcts are reported . CT evidence of obliterated posterior fossa cisterns and hydrocephalus indicates a grave prognosis due to brainstem compression . Progressive obliteration of posterior fossa cisterns may be used as an indicator for surgical decompression. Patients with intact posterior fossa cisterns had good recoveries without surgical treatment. CT can be used to diagnose the very early phase of an acute posterior fossa infarct and has prognostic value in predicting the outcome.
Acute infarcts involving the pons, medulla oblongata , and cerebellum are assoc iated with high mortali ty . Early diagnosis is essential [1-4], but has been difficult unti l the introduc tion of computed tomography (CT) . We reviewed literature on 'this entity [1-25] and carefully analyzed 3 1 cases seen over the past 3 years . CT plays an important role in the diagnostic and prognosti c implicati ons of acute posterior fossa infarcts.
Materials and Methods
Over a 3 year period, we have atlended at least 3 1 pat ients with acute infarcts in th e posterior fossa. Th e 1 8 men and 13 wo men were aged 23-73 years (average, 49.9 years). Almost all patients had dizziness , lethargy, and weakness on admission. Four had sudden onset of co ma without preceding symptoms. Nine had headache, and 1 4 had vom iting (table 1). The interval from onset of symptoms to initial CT scan was a few (4-6) hours to 2 weeks.
The 3 1 patients were divided into three groups according to age: (1 ) nine patients under 40 years old-three died , two became permanen tl y vege tative, and the other four had good recovery; (2) 1 3 patients aged 40- 59 years- fi ve died and eigh t had good recovery; and (3) nine patients aged 60 or older-four d ied and five had good recovery.
Results
Fi ve cases demonstrated isodense posterior fos sas by CT (Cases 1 , 2, 8, 14, and 16 ) a few hours to 2 - 3 days (case 2) after onset of symptoms. Twenty-five had hypodensity a few hours to 5 days (case 12) after the onset of symptoms. One of these 25 had mixed hyper- and hypodensities. One patient with mi xed hyper- and hypodensities was initiall y scanned about 2 weeks after the onset of symptoms.
There were 12 fata l cases (table 1). Among these, 10 showed complete obl iteration of the posterior fossa ciste rns, with a small or an absent fourth ventricl e. Nine of the 12 fatal cases had hydrocephalus related to swelling of the posterior fossa structures. Two had no hydrocephalus; in one of (case 5) those two , pontine and cerebellopontine ang le c istern s were maintained and the perimesencephalic c isterns were obliterated.
TA
BL
E 1
: S
um
mar
y o
f C
ase
s
Cas
e N
o.
(ag
e, g
en
de
r)
Die
d w
ith
ou
t su
rge
ry:
1 (3
9,F
)
2 (2
3,F
)
3 (4
9,F
)
4 (6
2,M
)
5 (6
4,M
)
6 (6
5,F
)
7 (4
6,F
)
8 (4
9,M
)
9 (5
3,M
)
10
(3
8,M
)
Clin
ical
Fin
din
gs
Le
tha
rgy
and
vom
itin
g,
1 d
ay
be
fore
ad
mis
sio
n,
Co
ma
tose
and
ap
ne
ic s
eve
ral
ho
urs
aft
er
ad
m
issi
on
, D
ow
nw
ard
nys
tag
mu
s, f
ixe
d a
nd d
ila
ted
pu
pils
, A
bse
nt
do
ll's
eye
mo
vem
en
t an
d co
rne
al
refl
exe
s,
He
ad
ac
he,
leth
arg
y,
and
vom
itin
g 2
-3
da
ys b
e
fore
ad
mis
sio
n,
Ob
tun
da
tio
n o
n a
dm
issi
on
, th
en
co
ma
tose
se
vera
l h
ou
rs l
ate
r, N
on
re
spo
nsi
ve,
fla
ccid
, a
bse
nt
corn
ea
l re
fle
x,
pu
pils
fix
ed
and
dila
ted
,
SLE
fo
r se
vera
l ye
ars
, L
eft
op
hth
alm
op
leg
ia,
he
ad
ach
e,
and
vom
itin
g;
the
n b
eca
me
co
ma
to
se o
ver
24
hr,
Pu
pil
s fix
ed
and
dila
ted
, F
lac
cid
an
d a
refl
exic
, L
on
g-t
erm
hyp
ert
en
sive
dia
be
tic,
Su
dd
en
on
set
of
com
a,
pin
po
int
pu
pils
, d
ecr
ea
sed
rig
ht
cor
nea
l re
fle
x, n
o s
po
nta
neo
us
resp
irat
ion
, in
cr
ea
sed
rig
ht
de
ep
te
nd
on
re
flex,
Ext
en
sor
ri
gid
ity,
Pro
gre
ssiv
ely
in
cre
asi
ng
we
akn
ess
2 d
ays
be
fo
re a
dm
iss
ion
, S
ud
de
n o
nse
t o
f co
ma
a f
ew
h
ou
rs b
efo
re a
dm
issi
on
, N
on
resp
on
sive
, fl
ac
cid
, a
nd
are
fle
xic
, N
o s
po
nta
ne
ou
s re
spir
ati
on
(i
ntu
ba
ted
),
Le
tha
rgy
an
d w
ea
kne
ss o
n d
ay
of
adm
issi
on
(f
ou
nd
un
resp
on
sive
at
ho
me
), R
esp
on
ded
to
pa
in b
y m
ovi
ng
le
ft s
ide
(rig
ht
he
mip
are
sis)
, V
ery
we
ak
corn
ea
l re
fle
xes,
Pu
pil
s 2
mm
, w
ea
kly
re
act
ive
, E
yes
de
via
ted
to r
igh
t.
Hyp
ert
en
sion
fo
r 6
yea
rs,
Su
dd
en
on
set
of
com
a
with
pre
ced
ing
in
cre
asi
ng
le
tha
rgy
and
we
ak
ne
ss,
Pin
po
int
pu
pils
, C
he
yne
-Sto
kes
resp
ira
tio
n (
intu
ba
ted
),
Su
dd
en
on
set
of
com
a w
ith
de
cere
bra
te p
ost
ur
ing
, P
up
ils 2
mm
, sl
ow
ly r
ea
ctiv
e,
Rig
ht
6th
cr
ani
al n
erv
e p
als
y, R
esp
on
de
d t
o p
ain
with
d
ece
reb
rate
po
stu
rin
g,
Su
dd
en
on
set
of
com
a,
No
nre
spo
nsi
ve t
o st
im
uli.
Are
fle
xic
, fla
ccid
, N
o sp
on
tan
eo
us
resp
ira
tion
, S
ynco
pa
l e
pis
od
e d
uri
ng
ca
rdia
c ca
the
teri
za
tion
, P
rog
ress
ive
ob
tun
da
tio
n w
ith s
ub
seq
ue
nt
com
a s
eve
ral
ho
urs
la
ter,
Re
spo
nsi
ve t
o d
ee
p
pa
in w
ith d
ece
reb
rate
po
stu
rin
g,
No
corn
ea
l o
r g
ag
re
fle
xes
or
do
ll's
eye
mo
vem
en
t. P
up
ils
fixe
d a
nd
dil
ate
d,
CT
an
d A
ng
iog
rap
hic
Fin
din
gs
NC
T:
Iso
de
ns
ity
in p
ost
eri
or
foss
a,
Ab
sen
ce o
f P
, C
PA
, a
nd P
M c
iste
rns,
Sm
all
fou
rth
ve
ntr
ic
le,
Hyd
roce
ph
alu
s,
CC
T:
No
no
pa
cifi
cati
on
of
ba
sila
r a
rte
ry,
An
gio
: O
cclu
sio
n o
f b
asi
lar
art
ery
pro
xim
al t
o A
ICA
, N
CT
: Is
od
en
sity
in p
ost
eri
or
foss
a,
Sm
all
fou
rth
ve
ntr
icle
, d
isp
lace
d t
o le
ft.
Ab
sen
ce o
f P
, C
PA
, an
d P
M c
iste
rns
, H
ydro
cep
ha
lus
, C
CT
: N
on
op
aci
fica
tio
n o
f ba
sila
r a
rte
ry,
An
gio
: P
art
ial o
cclu
sio
n o
f b
asi
lar,
su
pe
rio
r ce
re
be
llar,
an
d p
ost
eri
or
cere
bra
l a
rte
rie
s,
NC
T:
De
cre
ase
d d
en
sity
in b
rain
stem
and
ce
re
be
llum
, P
, C
PA
, a
nd P
M c
iste
rns
and
fou
rth
ve
ntr
icle
ob
lite
rate
d,
Hyd
roce
ph
alu
s,
CC
T:
No
ab
no
rma
l enh
an
cem
ent
. N
CT
: D
ec
rea
sed
de
nsi
ty in
up
pe
r p
on
s,
mid
b
rain
, a
nd
su
pe
rio
r ve
rmis
, P
and
CP
A c
is
tern
s a
nd
fou
rth
ven
tric
le n
orm
al.
PM
cis
tern
s p
art
ially
ob
lite
rate
d,
No
su
pra
ten
tori
al v
en
tric
ul
ar
dila
tati
on
, C
CT
: N
o a
bn
orm
al e
nh
an
cem
en
t.
NC
T:
Lo
w d
en
sity
in m
ed
ulla
, p
on
s,
and
mid
b
rain
, M
inim
al
he
mo
rrh
ag
ic d
en
sity
in b
rac
h
ium
po
ntis
, F
ou
rth
ve
ntr
icle
an
d p
ost
eri
or
foss
a c
i ste
rns
ob
lite
rate
d,
Hyd
roce
ph
alu
s,
NC
T:
De
cre
ase
d d
en
sity
in b
rain
ste
m a
nd c
ere
b
ellu
m,
Po
ste
rio
r fo
ssa
cis
tern
s a
nd
fo
urt
h
ven
tric
le c
om
ple
tely
ob
lite
rate
d,
Hyd
roce
ph
a
lus
,
NC
T:
De
cre
ase
d d
en
sity
in b
rain
ste
m a
nd
le
ft
an
d m
idlin
e c
ere
be
llum
an
d le
ft o
ccip
ital
lo
be
, P
ost
eri
or
foss
a c
iste
rns
an
d f
ou
rth
ve
ntr
icle
n
ot
visu
aliz
ed
, H
ydro
cep
ha
lus
, N
CT
: D
ec
rea
sed
de
ns
ity
in p
on
s a
nd
mid
bra
in,
Po
ste
rio
r fo
ssa
cis
tern
s an
d fo
urt
h v
entr
icle
n
ot
visu
aliz
ed,
Hyd
roce
ph
alu
s,
NC
T:
Iso
de
nsi
ty i
n p
ost
eri
or
foss
a,
Hyd
roce
ph
alu
s, P
ost
eri
or
foss
a c
iste
rns
and
fo
urt
h v
en
tri
cle
no
t vi
sua
lized
, N
CT
: D
ec
rea
sed
de
nsi
ty in
rig
ht
cere
be
llum
, O
b
lite
ratio
n o
f p
ost
eri
or
foss
a c
iste
rns
and
fou
rth
ve
ntr
icle
, H
ydro
cep
ha
lus,
C
CT
: N
on
op
aci
fica
tio
n o
f b
asi
lar
art
ery
,
Res
ult
s
Die
d 2
da
ys l
ate
r. B
asi
lar
art
ery
o
cclu
sio
n,
bila
tera
l ce
reb
ella
r in
fa
rcti
on
, an
d b
rain
ste
m c
om
pre
ssi
on a
t a
uto
psy
,
Die
d 1
wee
k la
ter.
Au
top
sy n
ot
pe
rfo
rme
d.
Die
d 4
da
ys l
ate
r, E
xte
nsi
ve c
ere
b
ella
r an
d p
ost
eri
or
po
nti
ne
in
fa
rcts
at
aut
op
sy,
Die
d 2
da
ys l
ate
r, A
uto
psy
no
t p
er
form
ed
,
Die
d 1
da
y la
ter,
Au
top
sy n
ot
pe
rfo
rme
d,
Die
d a
few
da
ys la
ter,
Die
d 4
da
ys l
ate
r,
Die
d 2
da
ys l
ate
r,
Die
d 2
da
ys l
ate
r,
Die
d sa
me
da
y,
(Jl o -i
(j) ~
m
-i
}>
r » ' Z
:IJ W
;::: '" Cl "::
J" " » ~
CD
CJ)
I\
)
11
(59
,M)
12
(7
3,M
)
Re
cove
red
wit
h s
urg
ery
: 1
3 (2
5,F
)
14
(4
2,F
)
15
(5
5,M
)
Re
cove
red
wit
ho
ut s
urg
ery
: 1
5 (
31
,F
)
17
(3
2,F
)
18
(5
5,M
)
19
(5
8,F
)
20
(5
3,F
)
Su
dd
en
on
set
of
diz
zin
ess
, ve
rtig
o,
and
he
ad
a
ch
e 1
da
y b
efo
re a
dm
issi
on
. U
nst
ea
dy
ga
it,
falli
ng
to r
igh
t. R
igh
t fa
cia
l w
ea
kne
ss a
nd
q
ua
dri
pa
resi
s. R
ema
ined
sta
ble
for
1 w
ee
k,
then
be
cam
e c
om
ato
se,
fla
ccid
, a
nd a
refl
ex
ic.
Fa
llin
g, w
ith
in
cre
as
ing
ly u
nst
ea
dy
ga
it fo
r 5
da
ys b
efo
re a
dm
iss
ion
. O
n a
rriv
al,
co
ma
tose
w
ith c
on
str
icte
d, n
on
rea
cti
ve p
up
ils.
Re
spo
n
sive
to
de
ep
pa
in w
ith
de
cere
bra
te p
ost
uri
ng
. L
eft
co
rne
al
refl
ex
ab
sent
.
Diz
zin
ess
, vo
mit
ing
, a
nd
fa
llin
g to
rig
ht.
Ro
tary
n
ysta
gm
us
, ri
ght
fac
ial
pa
lsy,
le
ft h
emip
are
sis
, d
ec
rea
sed
se
nsa
tion
in r
igh
t 5
th c
ran
ial
ne
rve
d
istr
ibu
tio
n.
Slig
htl
y d
ecr
ea
sed
he
ari
ng
in
rig
ht
ea
r. O
btu
nd
ati
on
2 d
ays
la
ter.
Acu
te o
nse
t o
f n
au
sea
, vo
mit
ing
, a
nd d
iplo
pia
. R
igh
t h
earin
g lo
ss a
nd
le
ft se
nso
ry d
efi
cit.
S
ub
seq
ue
nt
com
a,
left
he
mip
are
sis
, a
nd b
ila
te
ral
7th
cra
nia
l n
erv
e p
als
y 1
da
y la
ter.
S
ud
de
n o
nse
t o
f a
pn
ea
an
d co
ma
. O
n a
dm
is
sio
n,
no
t re
spo
nsi
ve t
o p
ain
; im
pro
ved
slig
htl
y a
fte
r N
arc
an
. G
lasg
ow
co
ma
sco
re 1
-4-1
(m
inim
al
wit
hd
raw
al)
. P
inp
oin
t p
up
ils,
left
con
ju
ga
te g
aze
pre
fere
nce
. R
igh
t h
em
ipa
resi
s,
eye
s tu
rnin
g l
eft
with
co
ld c
alo
ric
stim
ula
tion
.
Diff
icu
lty
spe
ak
ing
(su
dd
en
on
set)
. Q
ua
dri
pa
re
tic
, b
eca
me
qu
ad
rip
leg
ic.
De
cort
ica
te p
ost
ur
ing
la
ter.
Hea
d d
ev
iate
d t
o le
ft.
Do
ll's
eye
m
ove
me
nt
an
d c
orn
eal
refl
exe
s w
ea
k.
Dia
be
tes
me
llitu
s fo
r ye
ars
. O
ccip
ita
l h
ea
da
che
, le
tha
rgy,
an
d w
ea
kn
ess
1 d
ay
be
fore
ad
mis
si
on.
Rig
ht
ho
mo
nym
ou
s h
em
ian
op
sia
. D
is
con
jug
ate
ga
ze.
De
cre
ase
d l
eft
co
rne
al
refl
ex.
Le
ft f
aci
al
we
akn
ess
.
Occ
ipit
al
he
ad
ach
e r
ad
iati
ng t
o n
eck
fo
r 3
da
ys.
Ve
rtig
o,
diz
zin
ess
, a
nd
vom
itin
g 1
da
y b
efo
re
ad
mis
sio
n.
Wid
e-b
ase
d g
ait.
Fa
llin
g t
o ri
gh
t.
Nys
tag
mu
s,
left
la
tera
l ga
ze.
Diz
zy s
pe
lls,
un
ab
le t
o w
alk
fo
r 1
da
y. A
taxi
c,
falli
ng t
o le
ft.
Nys
tag
mu
s o
n ri
gh
t la
tera
l an
d
up
wa
rd g
aze
s. D
ec
rea
sed
se
nsa
tio
n i
n le
ft l
eg
and
tru
nk
. R
igh
t o
ph
tha
lmo
ple
gia
, h
ea
da
che
, d
izzi
ne
ss a
nd
vom
itin
g.
Be
cam
e c
om
ato
se 2
da
ys l
ate
r. C
or
neal
re
fle
xes
we
ak
. P
up
ils 4
mm
, re
act
ive
. D
oll'
s e
ve m
ove
me
nt
pre
sen
t.
NC
T:
De
cre
ase
d d
en
sity
in r
igh
t ce
reb
ellu
m w
ith
dis
pla
cem
en
t o
f sm
all
fou
rth
ven
tric
le t
o le
ft.
P,
rig
ht
CP
A,
an
d P
M c
iste
rns
no
t vi
sua
lize
d.
Le
ft C
PA
cis
tern
sm
all.
Mild
hyd
roce
ph
alu
s.
NC
T:
De
cre
ase
d d
en
sity
in v
erm
is,
mid
bra
in,
an
d u
pp
er
po
ns
. P
os
teri
or
foss
a c
iste
rns
ab
sen
t. S
ma
ll fo
urt
h v
en
tric
le.
No
hyd
roce
pha
lu
s.
NC
T:
De
cre
ase
d d
en
sity
in r
igh
t ce
reb
ellu
m.
Po
ste
rio
r fo
ssa
cis
tern
s vi
sua
lize
d.
Ven
tric
ula
r si
ze (
incl
ud
ing
fo
urt
h)
wit
hin
no
rma
l lim
its.
Re
pe
at
NC
T:
Sm
all
, co
mp
ress
ed
fo
urt
h v
en
tri
cle
. S
ma
ll P
and
PM
cis
tern
s. O
blit
era
tio
n o
f C
PA
cis
tern
s.
Hyd
roce
ph
alu
s.
An
gio
: O
cclu
sio
n o
f ri
ght
po
ste
roin
feri
or
cere
b
ella
r a
rte
ry.
NC
T:
Sm
all
are
a o
f h
ypo
de
nsi
ty in
rig
ht
cere
bel
lum
. F
ourt
h a
nd o
the
r ve
ntr
icle
s an
d p
ost
eri
or
foss
a c
iste
rns
wit
hin
no
rma
l lim
its.
NC
T:
Lo
w d
en
sit
y in
rig
ht
cere
be
llum
. F
ou
rth
ve
ntr
icle
co
mp
ress
ed
and
dis
pla
ced
to
left.
S
ma
ll P
cis
tern
. P
M a
nd C
PA
cis
tern
s o
blit
er
ate
d.
Hyd
roce
ph
alu
s.
NC
T:
Iso
de
nsi
ty i
n p
ost
eri
or
foss
a;
sma
ll fo
urt
h
ven
tric
le a
nd p
ost
eri
or
foss
a c
iste
rns.
No
hy
dro
cep
ha
lus
. A
ng
io:
Pa
rtia
l o
cc
lusi
on o
f b
asi
lar
and
left
sup
e
rio
r ce
reb
ella
r a
rte
ries
. R
ep
ea
t N
CT
: E
nh
an
cem
ent
in
po
ns
and
low
de
n
sity
in
left
cere
be
llum
.
NC
T:
De
cre
ase
d d
en
sity
in
left
in
feri
or
cere
be
llu
m,
righ
t ce
reb
ellu
m,
and
le
ft o
ccip
ital
lobe
. S
ma
ll fo
urt
h ve
ntr
icle
dis
pla
ced
to
rig
ht.
Mild
h
ydro
cep
ha
lus
. S
ma
ll P
an
d C
PA
cis
tern
s.
NC
T 1
da
y la
ter,
aft
er
on
set
of
com
a:
Co
mp
lete
o
blit
era
tion
of
po
ste
rio
r fo
ssa
cis
tern
s.
In
farc
ted
are
as
mo
re a
pp
are
nt.
Pro
gre
ssio
n o
f h
ydro
cep
ha
lus.
N
CT
: D
ecr
ea
sed
de
nsi
ty in
le
ft c
ere
be
llum
. F
ou
rth
ve
ntr
icle
dis
pla
ced
to
rig
ht.
No
hyd
ro
cep
ha
lus
.
NC
T:
De
cre
ase
d d
en
sity
in l
eft
ce
reb
ellu
m.
Po
ste
rio
r fo
ssa
cis
tern
s in
tac
t. F
ou
rth
ve
ntr
icle
co
mp
ress
ed
bu
t n
ot
dis
pla
ced
.
NC
T:
De
cre
ase
d d
en
sity
in l
eft
ce
reb
ellu
m a
nd
bra
chiu
m p
on
tis.
P,
left
CP
A,
an
d P
M c
iste
rns
visu
aliz
ed
. O
blit
era
tion
of
rig
ht
CP
A c
iste
rn.
No
hyd
roc
ep
ha
lus
.
Die
d 2
da
ys a
fte
r o
nse
t o
f co
ma
.
Die
d 2
mo
nth
s la
ter.
Bas
ila
r a
rte
ry
occ
lusi
on
and
in
farc
tio
n o
f b
rain
st
em
and
ce
reb
ellu
m a
t a
uto
psy
.
Su
rviv
ed a
fte
r su
rge
ry;
no
de
fici
t 5
mo
nth
s la
ter.
Su
rgic
al d
eco
mp
ress
ion
with
re
m
ova
l of
infa
rcte
d ri
gh
t ce
reb
el
lum
.
Su
rgic
al d
eco
mp
ress
ion
with
re
mo
val o
f h
ug
e in
farc
ted
rig
ht
cere
bellu
m.
Re
cove
red
with
out
si
gn
ifica
nt n
eu
rolo
gic
de
fici
t.
Su
rviv
ed
; sl
ow
ly i
mp
rove
d o
ver
2 m
on
ths
; q
ua
dri
pa
resi
s; o
be
yed
co
mm
an
ds
.
Su
rviv
ed
; n
od
de
d h
ead
and
mo
ved
ha
nd
s in
re
spo
nse
to
qu
est
ions
; ap
has
ia;
qu
ad
rip
are
sis
; h
om
o
nym
ou
s h
em
ian
op
sia
.
Re
cove
red;
no
de
fici
t 3
mo
nth
s la
ter.
Re
cove
red;
ab
le t
o w
alk
with
w
alk
er;
nys
tag
mu
s o
n ri
gh
t la
ter
al g
aze
1 m
on
th l
ate
r.
Su
rviv
ed
with
pe
rsis
ten
t q
ua
dri
pa
re
sis
. A
lert
and
aw
ake
1 m
on
th
late
r; d
isch
arg
ed
to
ho
me
.
» ' z :n .w ;:: '" (l :T
" » ~ to
(Xl '" o -I
o "Tl » o c -I
m
-U
o UJ
-I
m
JJ
(5
JJ
"Tl o UJ
UJ » Z
"Tl » JJ
o -I
UJ
(J1

Ta
ble
1 (
con
t'd
.)
Ca
se N
o.
(ag
e. g
end
er)
21
(54
,F)
22
(54
,M)
23
(25
,M)
24
(3
4,M
)
25
(4
5,M
)
26
(5
3,M
)
27
(6
4,M
)
28
(6
5,M
)
29
(7
0,F
)
30
(3
1,M
)
31
(59
,M)
Clin
ica
l Fi
nd
ing
s
He
ad
ac
he,
leth
arg
y,
an
d v
om
itin
g f
or
24
hr.
W
ea
kne
ss a
nd
lo
ss o
f b
ala
nc
e. C
ou
ld n
ot
wa
lk,
bu
t c
ou
ld m
ove
all
ext
rem
itie
s o
n c
om
m
an
d.
Lo
ss o
f b
ala
nce
an
d f
alli
ng
to
rig
ht
for
2 w
ee
ks.
Le
ft h
ea
rin
g l
oss
an
d d
ecr
ea
sed
le
ft c
orn
ea
l re
flex
. L
eft
5th
an
d 7
th c
ran
ial
ne
rve
pa
lsie
s.
Dip
lop
ia o
n le
ft l
ate
ral
an
d u
pw
ard
ga
zes
.
Le
tha
rgy
, vo
mit
ing
with
asp
ira
tio
n p
ne
um
on
ia.
Pu
pils
4 m
m,
rea
ctiv
e.
Dis
con
jug
ate
ga
ze w
ith
rig
ht
me
dia
l re
ctu
s p
als
y.
Su
dd
en
ly i
ncr
ea
sin
g le
tha
rgy
; su
bse
qu
en
t co
ma
an
d a
ton
ic b
rea
th
ing
2 d
ays
la
ter.
Wit
hd
raw
al
fro
m p
ain
. C
or
ne
al
refle
xes
pre
sen
t. P
upi
ls s
ma
ller
(2 m
m)
an
d w
ea
kly
re
act
ive
. D
izzi
ne
ss,
leth
arg
y, s
tag
ge
rin
g g
ait,
an
d v
om
it
ing
on
mo
rnin
g o
f ad
mis
sio
n.
Un
ab
le t
o s
tan
d
or
wa
lk.
Pu
pils
3 m
m,
rea
ctiv
e.
Co
rne
al
re
fle
xes
inta
ct.
Le
tha
rgy
, n
au
sea
, vo
mit
ing
, a
nd
in
ab
ility
to
wa
lk.
Fa
llin
g to
rig
ht.
Pu
pil
s 4
.5 m
m,
rea
ctiv
e.
Co
rn
eal
refl
exe
s in
tact
. S
ud
de
n o
nse
t o
f d
izzi
ne
ss.
Fe
ll; f
ou
nd h
avin
g
gra
nd
mal
se
izu
re.
Dis
ori
en
tati
on
, le
tha
rgy
, d
izzi
ne
ss,
and
we
ak
nes
s. N
eu
rolo
gic
exa
mi
na
tio
n o
the
rwis
e n
orm
al.
S
ud
den
on
set
of
vert
igo,
na
use
a,
an
d h
ea
da
ch
e,
wit
h o
cca
sio
na
l vo
mit
ing
. R
igh
t-s
ided
we
ak
ne
ss a
nd
ata
xia
. R
om
be
rg t
est
to
rig
ht.
Diz
zin
ess
, ve
rtig
o,
an
d l
eth
arg
y 2
da
ys b
efo
re
ad
mis
sio
n.
Un
ste
ad
y g
ait
with
le
ft-s
ide
d a
tax
ia.
Le
tha
rgy,
sh
ort
ne
ss o
f b
rea
th,
an
d v
om
itin
g 1
d
ay
be
fore
ad
mis
sio
n.
Aw
ake
an
d a
lert
, b
ut
diz
zy a
nd
qu
ad
rip
are
tic.
Rig
ht
faci
al
pa
lsy
and
p
tosi
s.
Le
tha
rgy
and
we
ak
ne
ss f
or
2 d
ays
. P
up
ils 4
mm
(r
igh
t) a
nd 2
mm
(le
ft),
we
akl
y re
ac
tive
. R
igh
t 3
d c
rani
al
ne
rve
pa
lsy.
Fa
llin
g to
rig
ht.
Dis
o
rie
nta
tio
n o
f tim
e a
nd p
lace
. S
eve
re h
ea
da
ch
e, n
au
sea
, vo
miti
ng,
an
d v
er
tig
o.
Le
ft-s
ide
d p
are
sth
esi
a a
nd w
ea
kne
ss;
falli
ng
to
left
. L
eft
-sid
ed
ata
xia
. D
ecr
ea
sed
re
sp
on
se t
o p
inp
rick
and
vib
ratio
n o
n r
igh
t si
de.
CT
an
d A
ng
iog
raph
ic F
ind
ing
s
NC
T:
De
cre
ase
d d
en
sity
in
verm
is.
Fo
urt
h v
en
tri
cle
co
mp
ress
ed
an
d d
isp
lace
d f
orw
ard
. N
o h
ydro
ce
ph
alu
s. P
ost
eri
or
foss
a c
iste
rns
pre
se
nt.
N
CT
: P
atc
hy
de
cre
ase
d d
en
sity
with
min
ima
l h
em
orr
ha
gic
de
nsi
ty i
n le
ft c
ere
be
llum
. F
ou
rth
ve
ntr
icle
dis
pla
ced
to
rig
ht.
CP
A c
iste
rns
sm
all.
PM
an
d P
cis
tern
s in
tact
. N
o h
ydro
ce
ph
alu
s.
NC
T:
De
cre
ase
d d
ens
ity
in m
idb
rain
wit
h o
blit
er
atio
n o
f P
M c
iste
rns
. F
ou
rth
ve
ntr
icle
an
d P
a
nd
CP
A c
iste
rns
inta
ct.
No
hyd
roce
ph
alu
s.
NC
T:
De
cre
ase
d d
en
sity
in
left
ce
reb
ellu
m a
nd
bra
chiu
m p
on
tis.
Fou
rth
ven
tric
le c
om
pre
sse
d
and
dis
pla
ced
to
rig
ht.
Pos
teri
or
foss
a c
iste
rns
int a
ct,
exc
ep
t ri
gh
t C
PA
cis
tern
. N
o h
ydro
ce
ph
alu
s.
NC
T:
De
cre
ase
d d
en
sity
in
rig
ht
cere
be
llum
. P
ost
eri
or
foss
a c
iste
rns
and
fo
urt
h v
en
tric
le
inta
ct.
No
hyd
roce
ph
alu
s.
NC
T:
De
cre
ase
d d
en
sity
in r
igh
t ce
reb
ellu
m.
Po
ste
rio
r fo
ssa
cis
tern
s a
nd f
ou
rth
ve
ntr
icle
in
tact
. N
o h
ydro
cep
ha
lus.
NC
T:
De
cre
ase
d d
en
sity
in r
igh
t ce
reb
ellu
m.
Fo
urt
h v
entr
icle
dis
pla
ced
to
left
. P
os
teri
or
fos
sa c
iste
rns
inta
ct.
No
hyd
roce
ph
alu
s.
CC
T:
No
ab
no
rma
l enh
an
cem
en
t.
NC
T:
De
cre
ase
d d
en
sity
in l
eft
ce
reb
ellu
m.
Fo
urt
h v
en
tric
le c
om
pre
sse
d b
ut
no
t d
is
pla
ced
. R
igh
t C
PA
cis
tern
ab
sent
; P
, P
M,
and
le
ft C
PA
cis
tern
s p
rese
nt.
No
hyd
roce
ph
alu
s.
NC
T:
De
cre
ase
d d
en
sity
in
left
cere
be
llum
. S
ma
ll fo
urt
h v
en
tric
le d
isp
lace
d t
o ri
gh
t. P
and
C
PA
cis
tern
s in
tac
t; P
M c
iste
rns
sm
all.
No
hy
dro
cep
ha
lus.
N
CT
: D
ecr
ea
sed
de
nsi
ty in
rig
ht
cere
be
llum
. N
o
dis
pla
cem
en
t o
f fo
urt
h v
en
tric
le.
Pos
teri
or
foss
a c
iste
rns
inta
ct.
l'Jo
hyd
roce
ph
alu
s.
NC
T:
De
cre
ase
d d
en
sity
in l
eft
cere
be
llum
. F
ou
rth
ve
ntr
icle
and
po
ste
rio
r fo
ssa
cis
tern
s n
orm
al.
No
hyd
roce
ph
alu
s.
Res
ult
s
Re
cove
red
; m
ild w
ea
kne
ss 2
w
ee
ks l
ate
r.
Re
cove
red
with
he
ari
ng
lo
ss.
Co
uld
w
alk
wit
h a
ssis
tan
ce
1 m
on
th
late
r.
Sl o
wly
re
cove
red
ove
r o
ne
mo
nth
w
ithou
t si
gn
ifica
nt
de
fici
t.
Re
cove
red
with
slu
rre
d s
pe
ec
h.
Ata
xia
, w
ea
kne
ss,
and
dys
me
tria
1
mo
nth
la
ter;
dis
cha
rge
d t
o c
hro
nic
ca
re f
aci
lity
.
Re
cove
red
wit
ho
ut
de
fic
it 3
we
eks
la
ter.
Re
cove
red
with
ou
t d
efi
cit
3 w
ee
ks
late
r.
Re
cove
red
1 m
onth
la
ter
with
mild
re
sid
ua
l w
ea
kne
ss.
Re
cove
red
with
min
ima
l ata
xia
3
we
eks
lat
er.
Re
cove
red
with
re
sid
ua
l d
izzi
ne
ss
and
we
akn
ess
2 w
ee
ks l
ate
r.
Dis
ch
arg
ed
to
ch
ron
ic c
are
fa
cil
it y.
Mild
ata
xia
and
slig
ht c
on
fusi
on
1 m
on
th l
ate
r.
Re
cove
red
with
mild
le
ft-s
ide
d
ata
xia
. A
ble
to w
alk
wit
h a
ssis
ta
nce
6 w
ee
ks l
ate
r.
No
le.-N
CT
= n
on
co
ntra
st
CT
; ee
T =
co
ntr
ast
CT
; P
= p
on
tin
e; P
M =
pe
rimes
en
ce
ph
alic
: C
PA
= c
ere
be
llop
on
tin
e a
ng
le:
AlG
A =
anl
ero
infe
rio
r c
ere
be
llar
art
ery
: S
LE
= s
yste
mic
lu
pu
s e
ryth
em
ato
su
s.
()l
t\) """ (f) » m
"""
» r }>
' Z
:D
w s: 0> " :::T
" }>
~
(!)
CO '"

AJNR :3, Marchi April 1982 CT OF ACUTE POSTERIOR FOSSA INFARCTS 153
Fig. 1.-Case 1. A , Conlrast CT. Forward displacement of small fourlh venIricle and complete obliterati on of ponline, ce rebellopontine angle, and peri mesencephalic c islern s; dilalalion of both temporal horns secondary 10 hydrocephalus. Posterior fossa structures were isodense. Nonopacification o f basilar artery. B, Left ve rtebral angiogram. Occ lusion o f basilar artery just distal to anteroinferior ce rebellar artery. Good filling of posteroinferior cerebellar artery.
A B
A
Fig. 2 .- Case 2. Contrast CT. Isodense posterior fossa structures, displacement of small fourth ventric le to left and anteriorly, dilatati on of both temporal horn s, obliterati on of posteri or fossa cistern s, and nonopaci ficat ion of basila r artery. Low densities within brainstem (B) were believed to be artifactual.
There were 19 survivors (table 1). One had nearly complete ob literation of the posterior fossa cisterns; another three had progressive ob literation of the posterior fossa cisterns plus hydrocephalus on the second CT examination . Three of these four patients had surgery resulting in better recovery than the one receiving nonsurgical treatment. The other 15 surviving cases had varying degrees of recovery with nonsurgical treatment. All of these 15 cases had visible posterior fossa cisterns and fourth ventricles .
The most common abnormality demonstrated by contrast CT was nonvisualization of the basilar artery.
In cases 1 - 3 (figs. 1 -3), the cause of the posterior fossa infarct was occlus ion of the basilar artery . In cases 1 and 2,
B
Fig . 3 .- Case 3. Noncontrast CT. Low density in center of posterior fossa with complete obliterati on of posterior fossa c istern s and fourth ventricle. Dilatal ion of both temporal horn s secondary to hydrocephalus.
CT demonstrated posteri or fossa isodensity; case 3 had hypodensity in the infarc ted pons and vermi s. In these cases there were some common features on CT, such as complete obliteration of the posterior fossa cisterns and hydrocephalus. These three pati ents, who were treated nonsurgicall y , died .
In cases 4, 5 , and 16 (figs. 4-6), the infarct was primarily in the brainstem , with less involvement of the cerebellum. In case 16, the posterior fossa structures were isodense on the first CT; an enhancing infarc t of the pons was demonstrated 5 days later after angiography . The posterior fossa cistern s and fourth ventri c le were not obliterated . In case 4 there were infarc ts in the pons, midbrain , and cerebellum . The perimesencephalic ciste rns were obliterated . The outcome in case 4 was far worse than in case 16, possibly due to more ex tensive invo lvement of the midbrain . In case 5 there was much more extensive infarcti on in the brainstem than in case 4 . The posterior fossa c istern s and fourth ventric le were completely obliterated , and hydrocephalus

154 TSAI ET AL. AJNR :3, Marchi April 19B2
A
A
Fig. 4.-Case 15. A, Contrast CT after angiography. Enhanc ing lesion in pons and low density in left cerebellum and brachium pontis. B, Reformatted sagittal CT. Posterior compression of fourth ventricle (arrow).
Fig. 5. -Case 4. Contrast CT. Low density in right side of brainstem and superior vermis, and partial obliteration of left ambient c istern .
B
Fig. 5. -Case 5. CT before (A) and after (B) contrast. Low density in brainstem, patchy hemorrhag ic density in left brachium pontis (arrow), and obliterat ion of posterior fossa c istern s.
was present. These three cases demonstrated that the larger the area of involved brainstem, the worse the prognosis.
In cases 13, 14, and 17 (figs. 7-9), the in itial CT showed
A B
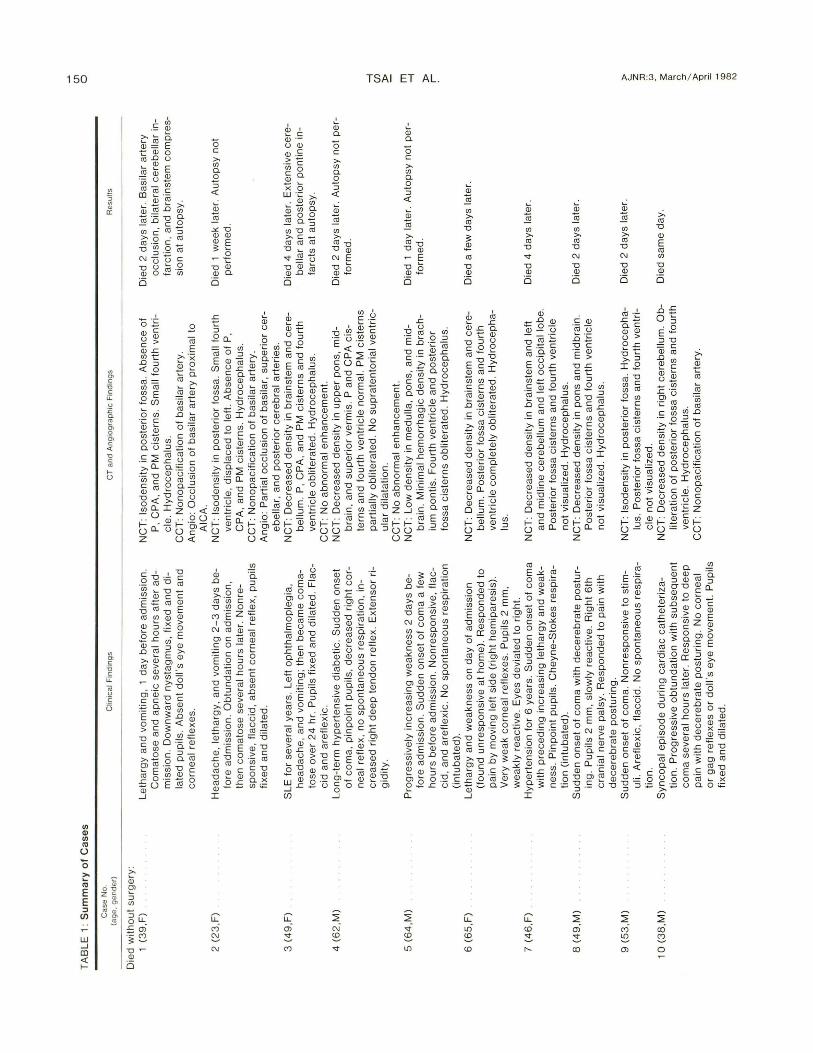
Fig . 7. -Case 17. Noncontrast CT. Displacement of small fourth ventric le to right , hypodensity of left cerebellar hemisphere, complete obliteration of peri mesencephalic cisterns, small pontine and cere bello pontine cistern s, and hydrocephalus.
c o Fig . B. - Case 13. Noncontrast CT. A and B, Slightly decreased density in
right cerebellum , slight displacement of fourth ventricle to left, intact posterior fossa c isterns , and absence of hydrocephalus. C and D, Repeat scans. Complete obliteration of posterior fossa cisterns and fourth ventric le, hydrocephalus, and more distinc t hypodensity in right cerebellum.
varying degrees of infarction in the posterior fossa. In case 17 there was also an occ ipital lobe infarct. Initially the posterior fossa cisterns were visualized and no hydroceph-
AJNR:3, March i April 1982 CT OF ACUTE POSTERIOR FOSSA INFARCTS 155
A B
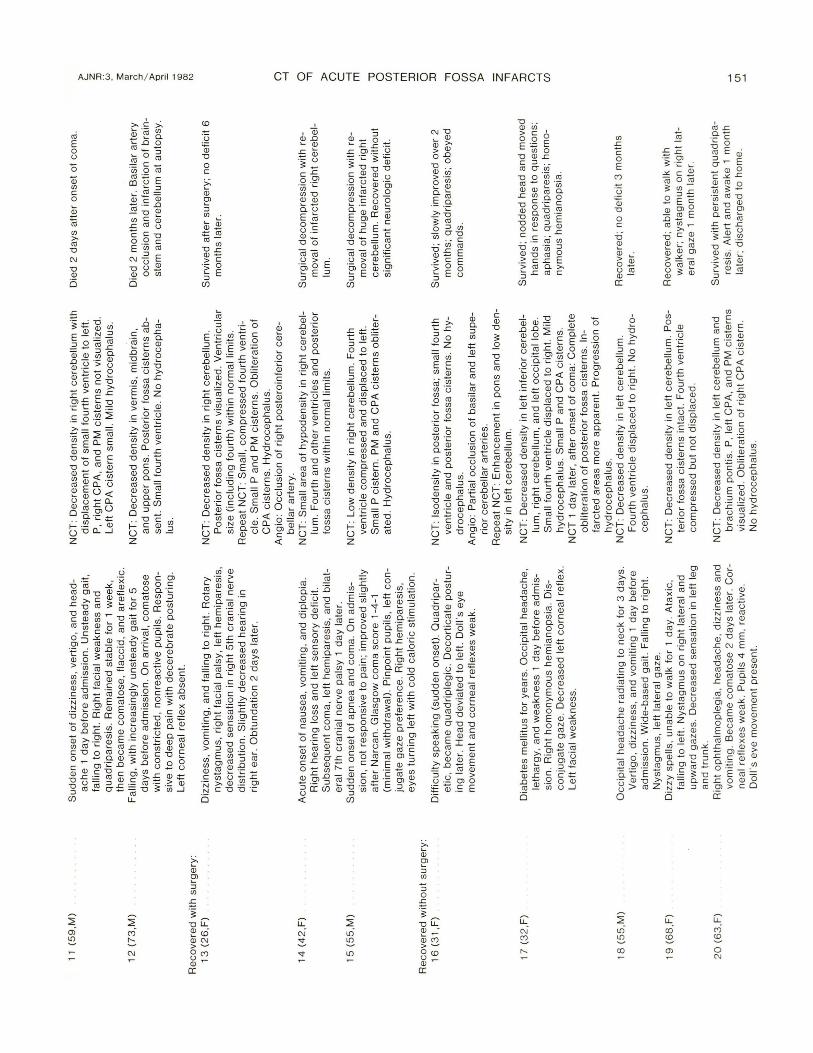
Fig. 9. - Case 14. Noncontrast CT. A , Small area of low density in right cerebellum , intact fourth ventri cle and c isterns, and absence of temporal horn dilatation. B , Repeat scan . Larger area of hypodensity in right cerebellum , displacement of fourth ven tric le to left. and dilatation of right temporal horn .
Fig . 1 D. - Case 18 . Noncontrast CT. Large area of low density in left cerebe llum , displacement of fourth ven tric le to right , and intact c istern s.
alus was demonstrated. However, when the posterior fossa cisterns became obliterated and hydrocephalus developed, the patient's condition deteriorated . Cases 13 and 14 had emergency surgical removal of infarcted brain in order to decompress the swelling and 'thus prevent brainstem compression . These patients recovered without neurologic deficit within 1 -6 months, Case 17 recovered with nonsurgical treatment, but had persistent severe neurologic deficits, In these three cases the cerebellar infarction was quite extensive; initial CT did not show cisternal or fourth ventricular obliteration or hydrocephalus. But follow-up CT did show obliteration of the cisterns and hydrocephalus that correlated with the progressive brainstem compression,
Surgical decompression is a life-saving procedure. Although case 17 showed survival without surgery, the result was a persistent vegetative state, In case 18 (fig . 10), the infarct in the cerebellum was also very extensive, compressing the fourth ventricle, Although there was very mild early brainstem compression, there was still enough space available for expansion of the infarcted cerebe llum , Injury to the
brainstem was not demonstrated . The outcome of this patient was excellent, with no surgical treatment required ,
Five patients (cases 1 , 2 , 13 , 14, and 16) had vertebral angiography, Occlusive changes were noted in each patient.
Discussion
Acute posterior fossa infarcts may result from occ lusion of the vertebrobasilar artery and / or its branches [2,3,6-9, 14-19]. The c linica l diagnosis of posterior fossa infarct may be difficu lt. Cerebellar infarcts are often associated with and complicated by infarcts of the lateral brainstem (which is supplied by the same arteri es), The manifestation of cerebellar disturbance has often been overshadowed by the more obvious brainstem dysfunction [3 , 7-9]. Angiographic diagnosis may also be difficult in the presence of isolated occlusion of a small arterial branch. Acute cerebe llar infarcts and accompanying cerebellar swelling may result in brainstem compression; a large cerebe llar infarct may require surgical decompression in order to reduce injury to the brainstem [4 , 7, 8 , 10-13, 20-25]. However, there are reports of good results after acute cerebellar infarcts without surgical intervention [2 , 14, 17]. Surgery is certain ly not indicated in acute brainstem infarction. Therefore, accurate diagnosis of the type and size of the posterior fossa infarct is essential for clinical management. In our experience, CT is often useful in differentiating cerebe llar from brainstem infarcts,
The mortality rate seems to increase only slightly with increasing age: 34% , group 1; 38.5% , group 2; and 44.5%, group 3 . However , the combined rate of mortality and poor recovery (persistent vegetative states) for group 1 was 56% , indicative of grave prognosis even for the younger patients. In reviewing the CT findings, the younger patients tended to have more associated mass effect than the older patients,
Although angiography is capab le of demonstrating vascular occlusions (cases 1, 2, 13, 14 , and 16) [6, 18], the precise site and the size of the infarct was often not c learly identified without CT. CT can demonstrate very early infarcts in the posterior fossa [5]. The fourth ventric le is a good landmark in locating a cerebellar infarct in those cases with isodense infarcts . In cases 1 and 2 , displacement of the fourth ventricle was the major finding of cerebellar infarction (other than the nonvisualization of the posterior fossa cisterns) . In case 17 there were infarcts on both sides, but the fourth ventri c le was sh ifted away from the larger infarct.
In cases of large or massive infarction , the posterior fossa c isterns and the fourth ventricle were obliterated , Nonvisualization of the posterior fossa c isterns may be correlated with clinical manifestations of brainstem compression [11, 13, 26-28]. Obliteration of the posterior fossa cisterns plus hydrocephalus were CT signs of a grave prognosis, (cases 1-3 and 5, table 1). Progressive obliteration of the posterior fossa ciste rns indicated that there was increasing brainstem compression (cases 13 , 14, and 17). This may be an indication for surgical intervention to prevent death or vegetative states from brainstem injury [4 , 21 , 22 , 26- 28].
In those cases with intact posterior fossa cisterns and no hydrocephalus by CT, there was good recovery with non-

156 TSAI ET AL. AJNR:3, March i April 1982
surgical treatment. These CT findings may be used in the c linical monitoring for nonsurgical management (table 1),
We believe that CT should be promptly used for the diagnosis of acute posterior fossa infarcts. These patients should be closely monitored by CT to assist in directing the c linical management in order to prevent grave complications.
REFERENCES
1. Burns J, Bisak R, Schut L , Silberbe rg D. Recovery following brainstem hemorrhage. Ann Neuro/ 1980;7: 183-1 84
2. Caplan LR . Occ lusion of the vertebral or basilar artery: fo llowup analysis of some patients with benign outcome. Stroke 1979;10 :277-282
3. Archer C, Horenstein S. Basi lar artery occlusion : c linical and radio logical correlation. Stroke 1977;8: 383-390
4 . Plum F, Posner JB. Subtentori al lesions causing coma. In : Diagnosis of stupor and coma, chap 3. Philadelphia, F. A. Davis, 1969:86- 101
5. Baker HL Jr, Houser OW. CT in diagnosis of posterior fossa lesions. Radiol C/in North Am 1976; 16 : 1 29-147
6. Caplan LR , Rosenbaum A. Role of cerebral angiog raphy in vertebrobasil ar occlusive disease. J Neurol Neurosurg Psychia try 1975;38: 601 - 612
7. Castaigne P, Lehermitle F, Gautier JC, et al. Arteria l occlusion in vertebrobasilar system: a stud y of 44 patients with postmortem data. Brain 1973;96: 133-154
8. Duncan GW, Parker SW, Fisher CM. Acute cerebellar infarct in th e PICA territory. Arch Neuro/ 1975; 32: 364-368
9. Fang HCH , Palmer JJ. Vascu lar phenomena involving brainstem structures: a c linical and pathologic correlation study. Neurology 1956;6 : 402-419
10. Fainburn 0 , Oliver LC. Cerebellar softening: a surgical emergency. Br Med J 1956;1 : 1335-1336
11 . Lehrich JR, Winkler GF, Ojemann RG . Cerebellar infarc tion with brainstem compression: diagnosis and surgical treatment. Arch Neuro/ 1970;22: 490-498
12. Fee ly MP. Cerebellar infarc tion. Neurosurgery 1979;4: 7 -11 13 . Greenburg J, Sku brick 0 , Shenkin H. Acute hydrocephalus
in cerebellar infarc t and hemorrhage. Neuro logy 1979;29: 409- 4 13
14. Mori K, Miwa S, Murata T, Okumura A, Handa H. Basilar artery occ lusion in childhood: report of a case. Arch Neurol 1979;36: 1 00-1 02
15. Kubrik CS, Adams RD. Occlusion of the basilar artery: a c linical and patholog ical study. Brain 1946;69 : 73-121
16. Fowler M. Two cases of basilar artery occ lusion in childhood. Arch Dis Child 1962;37: 78-81
17 . Field WS, Ratinov G, Weibel J, et al. Survival foll owing basi lar artery occ lusion . Arch Neuro/1965;15:463-471
18. Moscow NP, Newton TH . Angiog raphic implication in diagnosis and prognosis of basilar artery occlusion. AJR 1973; 11 9: 597-604
19. Drake CG. Ligation of the vertebral (unilateral or bilateral) or basilar artery in the treatment of large intrac ranial aneurysm. J Neurosurg 1975;43: 255- 274
20. Lindgren SO. Infarctions simulating brain tumors in the posterior fossa. J Neurosurg 1956;13: 575-581
21. Sypert GW, Alvord EC. Cerebellar infarction: a c linicopatholog ical stud y. Arch Neuro/1975; 32: 357 - 363
22. Norri s JW, Eisen AA , Branch CL. Problems in cerebellar hemorrh age and infarct ion. Neurology 1969; 19: 1 043- 1 050
23. Wood MW, Murphey F. Obstructive hydrocephalus due to infarction of a cerebellar hemisphere. J Neurosurg 1969 ; 30:260- 263
24 . Wolman L. Ischemic lesion in th e brainstem assoc iated wi th raised supratentorial pressure. Brain 1953;76: 364-377
25. Miki K. On the surgical treatmen t of cerebellar infarct ion. Neurol Surg (Tokyo) 1978;6: 707 -713
26. Tsai FY, Zee CS, Quinn MF, Teal JS, Segall HD. CT in brainstem disorders. Presen ted at the International Symposiu m and Course on Computed Tomography, Las Vegas, Apri l 1979
27. Tsai FY, Teal JS, Itabashi HH , Huprich JE, Heish ima GB, Segall HO. CT of posterior fossa trauma. J Comput Assist Tomogr 1980;4 : 291 - 305
28. Tsai FY, Teal JS, Quinn MF, et al. CT in brainstem injury . AJNR 1980; 1 : 23-29