concussion management s -return to play · • vestibular rehabilitation to improve function of the...
TRANSCRIPT

Concussion Management -Return to Plays
A.G. (Tony) SchneidersPhD MSc PGDipManipTh PGCertTerTch DipPhty
School of Health, Medical & Applied SciencesCentral Queensland University
5th Biennial Symposium: Tauranga 2019

Central Queensland University

Bundaberg
Killer sharks



Overview
• Conclusion….?
• Return to Play (RTP) considerations
• RTP after concussion: The 5+ “R’s” of concussion management
• How we used to RTP after concussion in the old days….
• How we do it now…………
• Management and RTP of acute concussion
• Factors to consider when RTP is based on symptomology
• Diagnosis, classification and management of post-concussive disorders
• Buffalo Concussion Treadmill Test (BCCT) and rehabilitation

Management of concussion?

Conclusion…..
Despite intense clinical and basic research into the pathophysiology and management of concussion, the
RTP decision remains one of the most difficult and
controversial in clinical sports medicine. The literature
is often unclear and contradictory regarding specific
diagnostic and therapeutic approaches
(Doolan et al 2011)

Is this the most effective treatment for concussion?

Return to Play after concussion 2019
Return to play (steps) after concussion
• Accurate assessment
• Differential diagnosis
• Appropriate and targeted management
• Relative Rest
• Graded rehabilitation (exercise)
• Optimal Loading (exercise)
• Monitoring of recovery (exercise)
• Risk reduction strategies (exercise)
• Appropriate education and counseling
• Medical clearance
• Athlete monitoring
RTP considerations
• Risk of subsequent concussions?
• Prolonged recovery from sequential concussions (post-concussion syndrome)?
• Chronic traumatic encephalopathy (CTE)?o Athletica Pugilistica
• “Second impact syndrome (SIS)”? o Diffuse Cerebral Swelling (DCS)/ Sub-dural haeamatoma (SDH)
o Benign Subarachnoid cyst?

Concussion Management: The 4-5+ “R”s
• Recognize
• Remove
• Referral
• Rest
• Return to Play
• Recognition
• Response
• Rehabilitation
• Return to play
Kissick & Johnston 2005
CISG’s 11 ‘R’s of SRC management


CISG’s 11 ‘R’s of SRC management
• Recognize
• Remove
• Re-evaluate
• Rest
• Rehabilitation
• Refer
• Recover
◼ Return to sport
• Reconsider
• Residual effects & sequelae
• Risk reduction

Return to Play after concussion (< 2000?)

LOC and amnesia to determine RTP (< 2001)
Grade I- No LOC and amnesia
Grade II- LOC < 1min, Amnesia < 30 min
Grade III- LOC > 1min, Amnesia < 24hr
E.g. Cantu system
Athletes with a Grade II concussion could RTP within 2 weeks if they were asymptomatic at rest and following exertion in the previous 7 days.
After a second Grade II concussion in the same season the athlete was not to return to play for 1 month.

Is this a punishment?


Neurometabolic cascade following concussion
K+, potassium; CMRglucose, cerebral metabolic rate of glucose utilization; Ca2+,
calcium; CBF, cerebral blood flow. With permission (Hovda et al., 1995)

Consensus StatementConcussion in Sport Group (CISG)

The cornerstone of concussion management is physical and cognitive rest until the acute symptoms resolve and then a graded programme of exertion prior to medical clearance
and RTP.
Concussion management

Athletes’ only rest occasionally…………

• Individuals randomised to rest reported higher symptoms over 10 days and had slower symptom resolution o (Thomas et al 2015)
• Greater activity level was associated with shorter symptom duration in one observational study (Howell et al 2016) and longer symptom duration in another (Brown et al 2015)
• Two retrospective studies did not find a significantassociation between recommended cognitive rest and time to symptom resolution (Gibson et al: Moor et al)

Leddy et al., 2019

So has the CISG group got it right?



RTP is based on symptomology
X
X
X
X
X
X
X

(Balasundaram, Schneiders et al., 2017)

Factors to consider when RTP is based
on symptomology
• Baselines need to be established
• Symptoms need to be diagnosed accurately
• RTP needs to be individualized
• Athlete “personalities” need to be considered
• External factors affecting symptoms are commono Sleep/alcohol/anxiety
o (Balasundaram, Schneiders et al. 2018)
Concussion Management

Post Concussion Syndrome & RTP
• The majority of athletes who sustain a concussion will reach full neurological recovery within 1–2 weeks
• However approx. 10–20% will demonstrate persistent signs and symptoms lasting greater than 3 weeks
• The cornerstone of management, physical and cognitive rest, is often not effective in resolving these symptoms

Post Concussion Syndrome & RTP
The management of athletes with sub-acute concussion and Post-Concussion syndrome remains controversial and
poorly established
(Ellis et al., 2015)

Post Concussion Disorder (PCD)
Characterized by persistent pathophysiological alterations in specific neurological sub-systems or global brain metabolism
(Ellis et al, 2015)
• Physiologic (global)
• Vestibulo-ocular (sub-system)
• Cervicogenic (sub-system)
While overlap between PCDs may exist the presence of each PCD has implications for patient prognosis and RTP
decision-making

Diagnosis Algorithm for PCD sub-types
(Ellis et al, 2015)

Vestibulo-ocular PCD
• Characterized by persistent concussion symptoms and impairments caused by dysfunction of the vestibulo-ocular system.o vestibular, oculomotor and somatosensory systems
• Vestibulo-ocular reflex (VOR)o regulates gaze stabilization during head acceleration
• Vestibulo-spinal reflex (VSR)o co-ordinates head, neck and trunk positioning during dynamic body movements
• Symptoms of dizziness, gait instability, fogginess, blurred vision and difficulty focusing are common
• Vertigo and dizziness can be due to post-traumatic benign paroxysmal positional vertigo (BPPV)

Vestibulo-ocular management
• Athletes with isolated vestibulo-ocular PCD are able to exercise to exhaustion during graded treadmill tests
• Vestibular therapy and repositioning techniques can be effective treatments to improve dizziness and vertigo
• Vestibular rehabilitation to improve function of the VOR, the cervico-ocular reflex (COR), depth perception, somatosensory retraining, dynamic gait and aerobic conditioning
• Athletes with benign paroxysmal positional vertigo (BPPV) have a high rate of responsiveness to canalith re-positioning manoeuvres


Cervicogenic PCD
• Cervicogenic PCD is characterized by persistent concussion symptoms and impairments caused by dysfunction of the cervical spine somatosensory system
• Athletes often describe impact mechanisms that involve rapid acceleration–deceleration forces to the head and cervical spine
• Athletes complain of neck pain, stiffness, fatigue, dizziness, headaches and postural instability
• On examination the cervical spine is implicated byhypomobile intervertebral segments, muscle spasm and tenderness of paraspinal structures.

Cervicogenic Management
• Cervical spine mobilisation
• Strengthening/stabilization
• Proprioceptive exercises
• Stretching soft-tissue
• Postural alignment/awareness/control
• Cervical retraction
• Gaze stabilisation

Physiologic PCD
• Characterized by persistent concussion symptoms and impairments caused by alterations in global cerebral metabolism.o Cell membrane permeability,
o Ion transport regulation,
o Neurotransmitter release
o Cellular metabolism
o Cerebral blood flow
• Athletes report mild persistent symptoms or are asymptomatic at rest but continue to have exacerbationof symptoms during cognitive activity and/or physical exercise
• The role of autonomic nervous system (ANS) regulation in concussion recovery is not clear but may be involved and mediated by effects on cerebrovascular reactivity.

Management of Physiologic PCD
• Exercise is emerging as strategy to promote ANS and concussion recoveryo Increase parasympathetic nervous system activity
o Decrease sympathetic nervous system activity
o Increase Cerebral Blood Flow (CBF)
• Animal models earlier suggested aerobic exercise 14-21 days post injury is most beneficial
• Sub-symptom threshold exercise training may hasten recovery and improve functional outcomes in adolescents and adults with concussion
• 80% HRmax of threshold, once daily, 5-6 days/weeko the rate of symptom improvement was highly correlated with the exercise
intensity achieved
(Leddy et al., 2010)
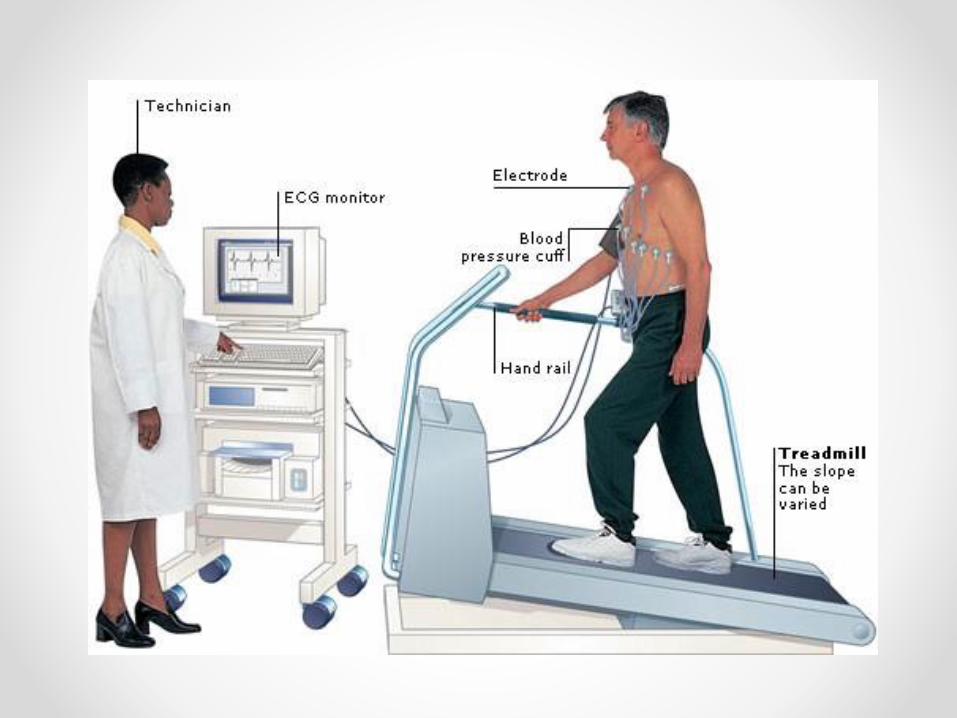

Buffalo Concussion Treadmill Test
• Based on the Balke cardiac treadmill test
• Contraindications same as cardiac stress testing
• Constant speed (5.2-5.8 km/hr), 1 degree incline each minute
• Once 12 degrees reached speed increased by 0.64km/hrto 20min max
• Borg RPE/Symptom response assessed each minute
• Cool down 4km/hr for 2 minutes

Terminating the Test
• Maximum exertion (RPE score of 19.5)
• Maximum Heart Rate reached (220 -age)
• Symptom exacerbation/new symptoms (increase of ≥3/10 points Likert scale)
• Continuing test constitutes significant health risk (faint/unsteady)
• Patient reports an inability to continue the test safely


Treatment/Return to Play
• On completion of the BCTT, exercise is prescribed as indicated (i.e. physiologic PCS)
• Exercise based on 80% MaxHR reached without symptom exacerbation.
• Instructed to exercise at this level for 20 minutes daily
• Exercise includes swimming, walking or stationary cycling: not resistance training.
• BCTT reviewed/recalibrated at weekly intervals
• If any symptoms return along the progression, athlete returns to the previous asymptomatic stage/maximum heart rate.
• When athlete can exercise to voluntary exhaustion on the BCTT without symptoms, begin the process of RTP using the five-step RTP program of the CISG Consensus Statement.

Summary
• Sports-related concussion is an inevitable consequence of sport participation
• All concussions should be treated as potentially serious injuries
• RTP consensus protocols based are available for acute, “simple” concussion
• RTP protocols are now emerging for Post-Concussion Disorders
• Exercise is emerging as the treatment of choice after relative rest
• Sports Physiotherapists should have a major role in returning athletes to play after concussion
• The evoultion of the CISG Consensus Statement and SCAT are tools that provide a best-practice approach to the evaluation of SRC and RTP protocols
Thank you for being part of SEPNZ 2019
5th Biennial Symposium: Tauranga 2019

References
• Child SCAT3 Br J Sports Med 2013;47:5 263.
• Marshall SW, Spencer RJ (2001) Concussion in rugby: the hidden epidemic. Journal of Athletic Training 36(3), 334.
• McCrory P, Meeuwisse WH, Aubry M, Cantu B, Dvořák J, Echemendia RJ,.. & Turner M (2013) Consensus statement on concussion in sport: the 4th International Conference on Concussion in Sport held in Zurich, November 2012. British Journal of Sports Medicine 47(5), 250-258.
• Pocket CRT Br J Sports Med 2013 47: 267.
• SCAT3 Br J Sports Med 2013 47: 259.
• Sye G, Sullivan SJ, McCrory P. (2006) High school rugby players' understanding of concussion and return to play guidelines. British Journal of Sports Medicine 40, 1003-5.
• Thurman DJ, Branche CM, Sniezek JE (1998) The epidemiology of sport-related traumatic brain injuries in the United States: Recent developments. J. Head Trauma Rehabil.13:1–8.