congenital hallux varus: how to deal with it?
TRANSCRIPT

CONGENITAL HALLUX VARUS (CHV):whow to deal with it?
R.Elbaum
CHIREC ORTHOPEDIC GROUP
Clinique Edith Cavell
Hôpital Universitaire Erasme
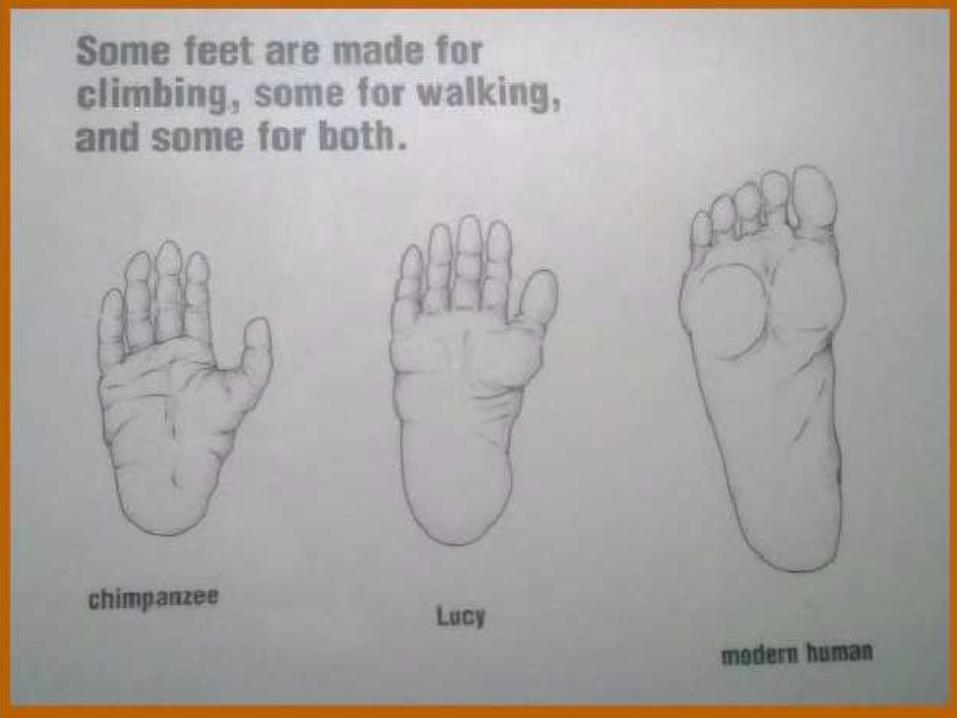

CHV: what it is?
• Congenital medial angulation of the greattoe at the metatarso-phalangealnjoint.
• Varus deformity vary from few degree to 90°
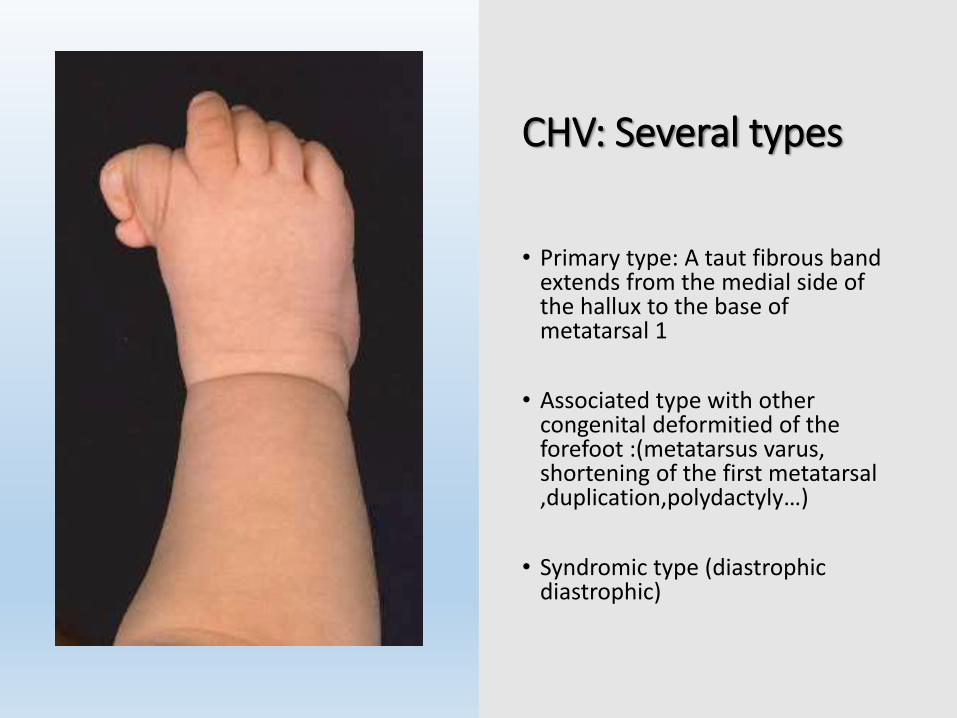
CHV: Several types
• Primary type: A taut fibrous band extends from the medial side of the hallux to the base of metatarsal 1
• Associated type with other congenital deformitied of the forefoot :(metatarsus varus, shortening of the first metatarsal ,duplication,polydactyly…)
• Syndromic type (diastrophic diastrophic)

CHV associated with longitudinal Epiphyseal bracket of Metatarsal 1th (LEB)
• Anomaly of growth plate formation on the MT1 on the medial side
• It extends as a continuous unit proximally and distally
• Abnormal growth with shortening and varus angulation

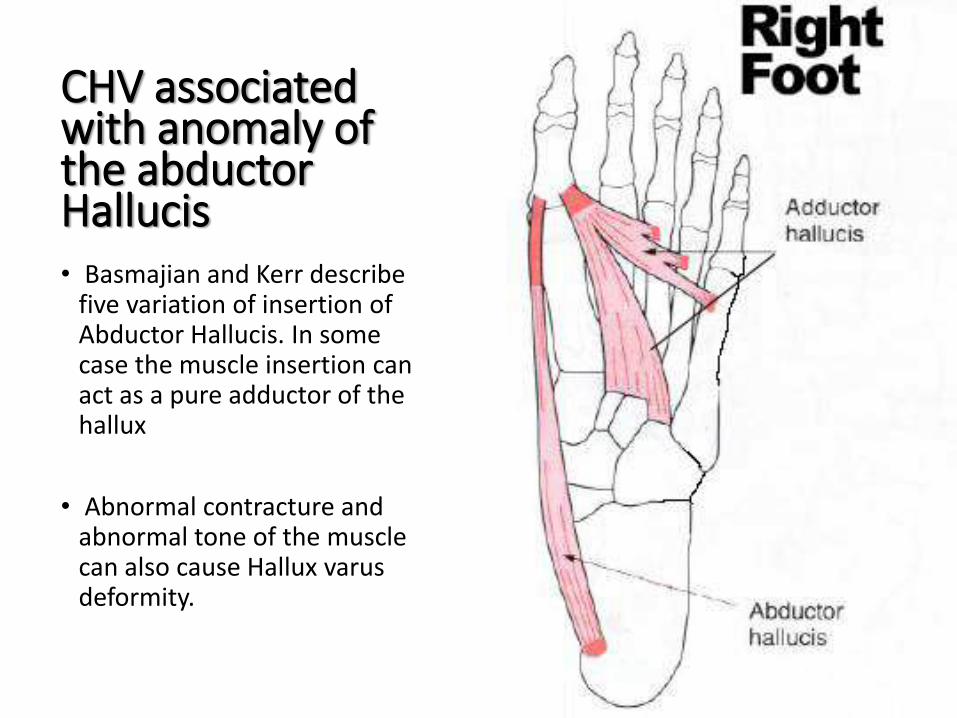
CHV associated with anomaly of the abductor Hallucis• Basmajian and Kerr describe five
variation of insertion of Abductor Hallucis. In some case the muscle insertion can act as a pure adductor of the hallux
• Abnormal contracture and abnormal tone of the muscle can also cause Hallux varus deformity.
CHV associated with anomaly of the abductor Hallucis• Basmajian and Kerr describe
five variation of insertion of Abductor Hallucis. In some case the muscle insertion can act as a pure adductor of the hallux
• Abnormal contracture and abnormal tone of the muscle can also cause Hallux varus deformity.

CHV is different from Adult Hallux Varus• Overcorrection of Hallux
Valgus (80%)
• Reumatoid arthritis
• Trauma
• Charcot-Marie –Tooth
• Avascular necrosis
• Contracture on burns
• ….
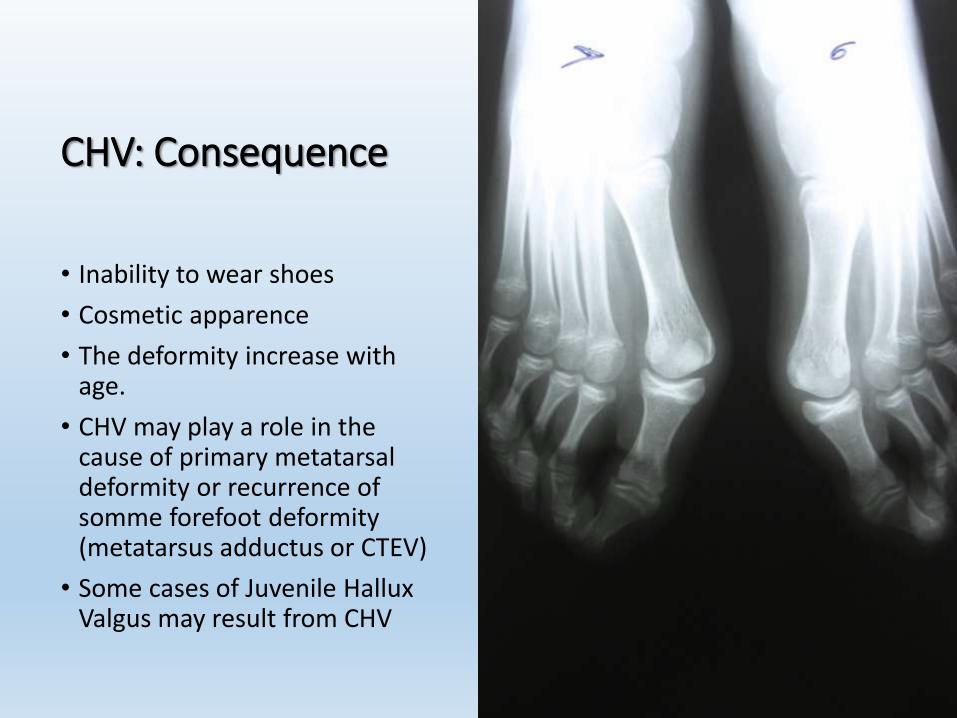
CHV: Consequence
• Inability to wear shoes
• Cosmetic apparence
• The deformity increase withage.
• CHV may play a role in the cause of primary metatarsaldeformity or recurrence of somme forefoot deformity(metatarsus adductus or CTEV)
• Some cases of Juvenile Hallux Valgus may result from CHV
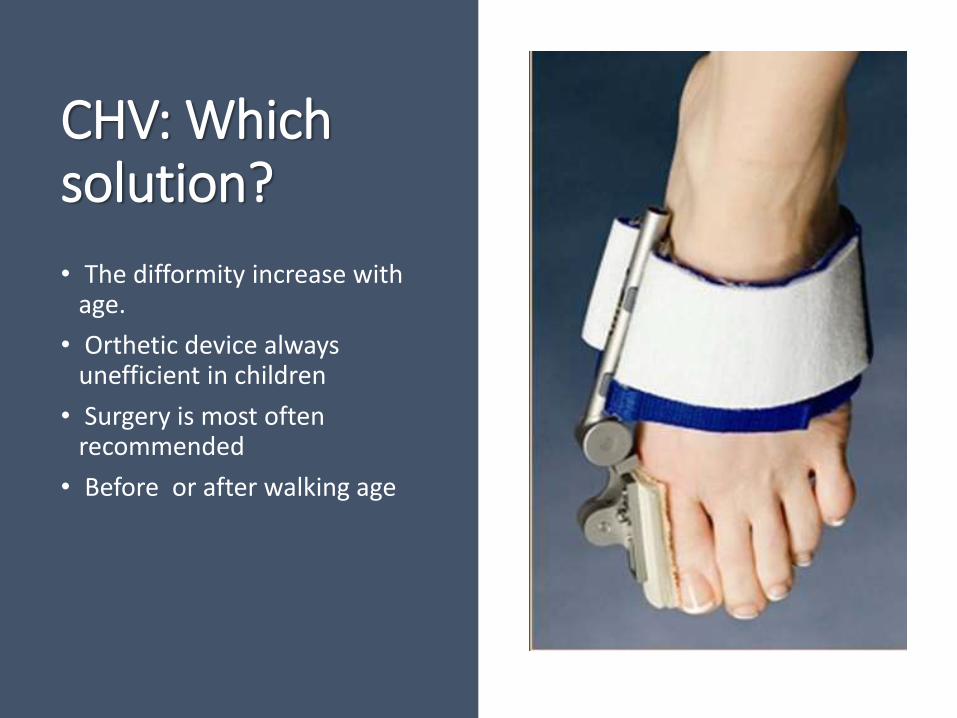
CHV: Which solution?
• The difformity increase with age.
• Orthetic device always unefficient in children
• Surgery is most often recommended
• Before or after walking age
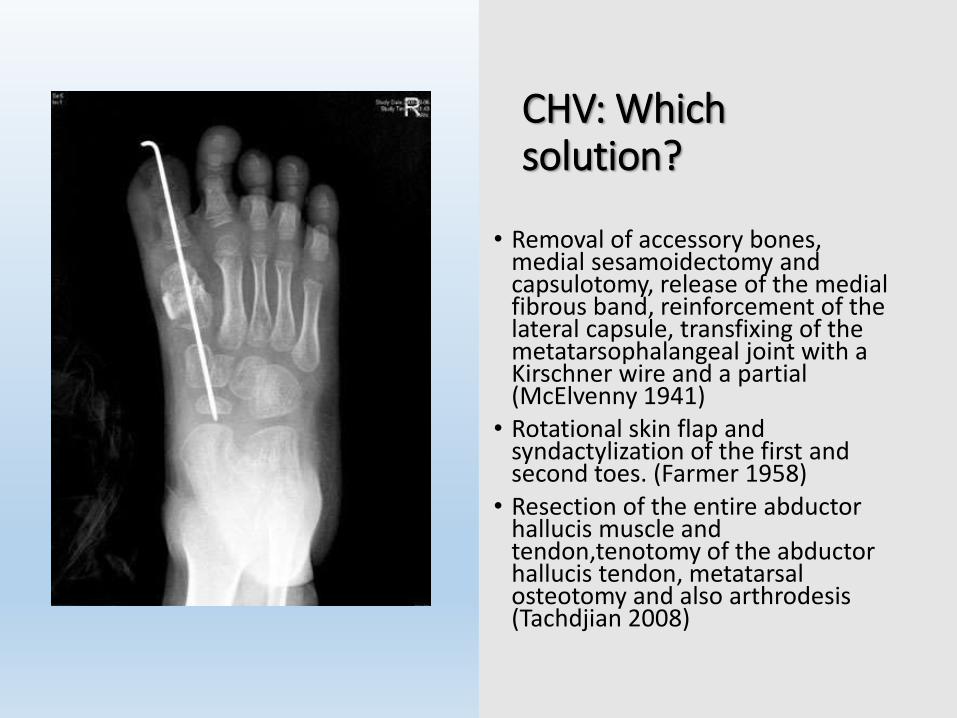
CHV: Whichsolution?
• Removal of accessory bones, medial sesamoidectomy and capsulotomy, release of the medial fibrous band, reinforcement of the lateral capsule, transfixing of the metatarsophalangeal joint with a Kirschner wire and a partial (McElvenny 1941)
• Rotational skin flap and syndactylization of the first and second toes. (Farmer 1958)
• Resection of the entire abductor hallucis muscle and tendon,tenotomy of the abductor hallucis tendon, metatarsal osteotomy and also arthrodesis (Tachdjian 2008)

Surgical technique: Farmer 1958
Which solution in case of LEB?
Bracket chondroosteotomy accompanied by fat interposition
Resection of the LEB with silicone polymer or polymethylmethacrylate interposition,
Simple bracket excision before ossification,
Distraction osteogenesis and metatarsal osteotomy after complete closure of the LEB
“The overall goal of any of these procedure is to eliminate the tethering
effect of the growth plate by removing the bar and therefore to
promotegrowth in a lengthwise fashion.”
• Mubarak SJ, O'Brien TJ, Davids JR. Metatarsal
epiphyseal bracket: treatment by central physiolysis.
J Pediatr Orthop.1993;13(1):5-8.
• Schreck MA. Pediatric longitudinal epiphyseal bracket:
reviewand case presentation. J Foot Ankle Surg.
2006;45(5):342-5.

Case presentation 1
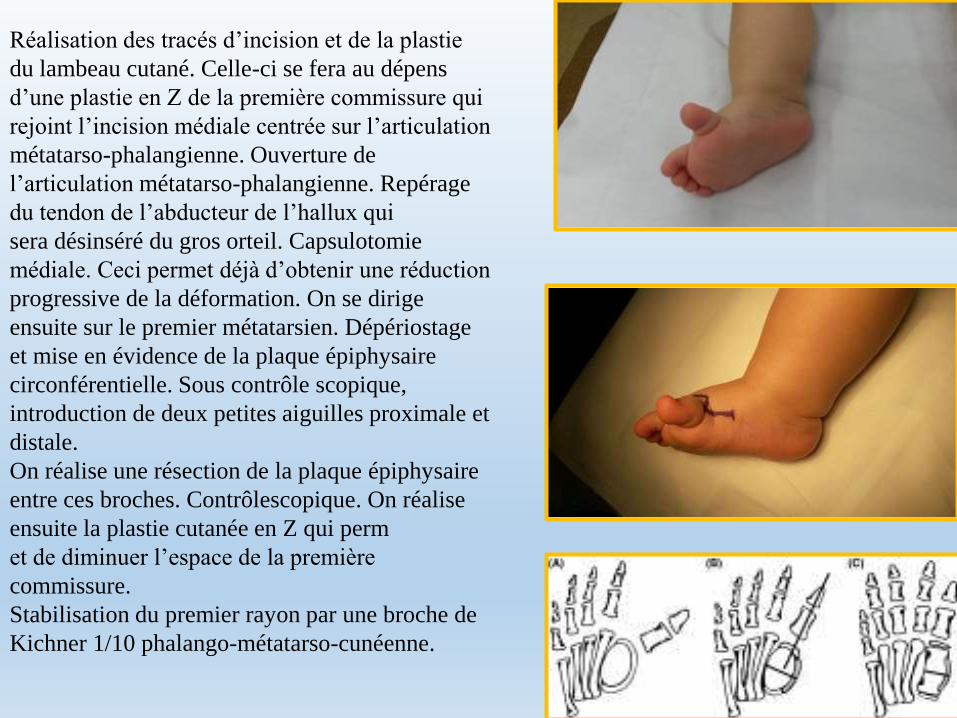
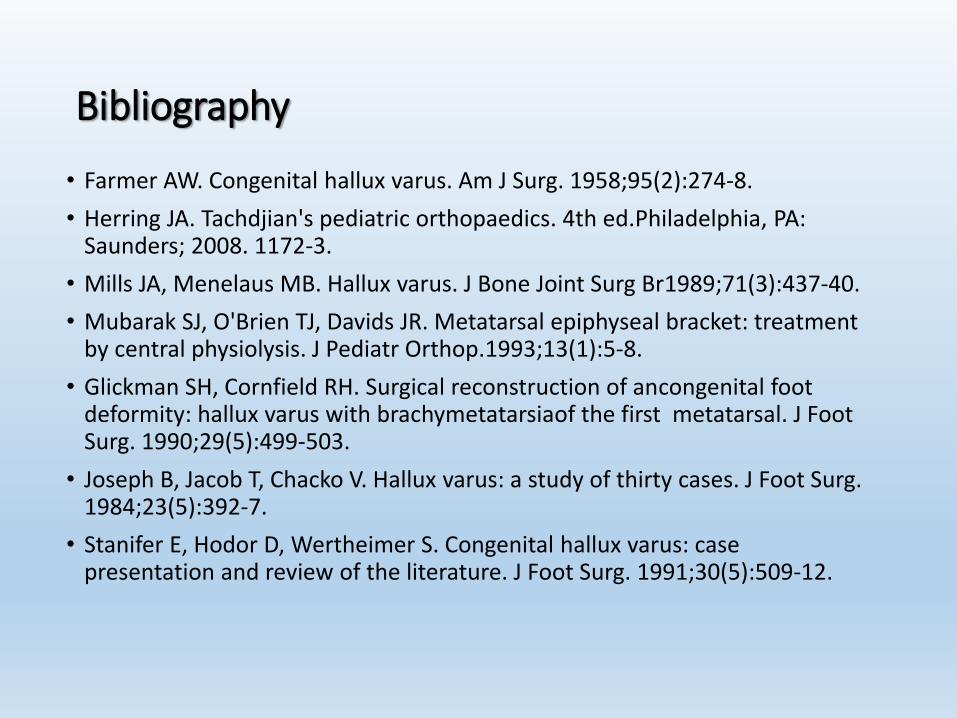
Réalisation des tracés d’incision et de la plastie
du lambeau cutané. Celle-ci se fera au dépens
d’une plastie en Z de la première commissure qui
rejoint l’incision médiale centrée sur l’articulation
métatarso-phalangienne. Ouverture de
l’articulation métatarso-phalangienne. Repérage
du tendon de l’abducteur de l’hallux qui
sera désinséré du gros orteil. Capsulotomie
médiale. Ceci permet déjà d’obtenir une réduction
progressive de la déformation. On se dirige
ensuite sur le premier métatarsien. Dépériostage
et mise en évidence de la plaque épiphysaire
circonférentielle. Sous contrôle scopique,
introduction de deux petites aiguilles proximale et
distale.
On réalise une résection de la plaque épiphysaire
entre ces broches. Contrôlescopique. On réalise
ensuite la plastie cutanée en Z qui perm
et de diminuer l’espace de la première
commissure.
Stabilisation du premier rayon par une broche de
Kichner 1/10 phalango-métatarso-cunéenne.



Case presentation 2



CHV:CONCLUSION
• CHV is a rare condition in neonate and children
• Surgical correction is generally recommended and various surgicaltechniques have been described
• Although the small size of series in litterature define a definitive conclusion on the optimal treatment strategy.
• Patient’s age is another factor that must be assessed whenconsidering surgery.
• Resection of a bracket epiphysis should be performed as with other procedures to prevent recurrent deformity.
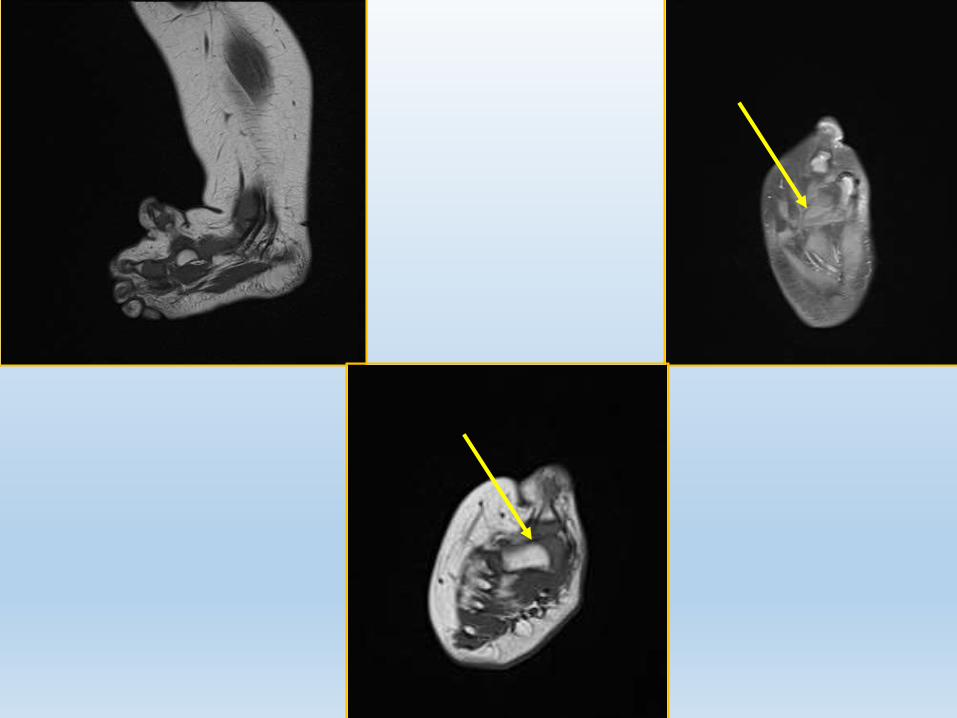
• Evaluation with MRI before surgery if the presence of a LEB is suspected.
Bibliography
• Farmer AW. Congenital hallux varus. Am J Surg. 1958;95(2):274-8.
• Herring JA. Tachdjian's pediatric orthopaedics. 4th ed.Philadelphia, PA: Saunders; 2008. 1172-3.
• Mills JA, Menelaus MB. Hallux varus. J Bone Joint Surg Br1989;71(3):437-40.
• Mubarak SJ, O'Brien TJ, Davids JR. Metatarsal epiphyseal bracket: treatment by central physiolysis. J Pediatr Orthop.1993;13(1):5-8.
• Glickman SH, Cornfield RH. Surgical reconstruction of ancongenital foot deformity: hallux varus with brachymetatarsiaof the first metatarsal. J Foot Surg. 1990;29(5):499-503.
• Joseph B, Jacob T, Chacko V. Hallux varus: a study of thirty cases. J Foot Surg. 1984;23(5):392-7.
• Stanifer E, Hodor D, Wertheimer S. Congenital hallux varus: case presentation and review of the literature. J Foot Surg. 1991;30(5):509-12.
THANK YOU