considerations for state obesity policy - women in … for state obesity policy scott kahan, md, mph...
TRANSCRIPT

Considerations for
State Obesity Policy
Scott Kahan, MD, MPH
Faculty, Johns Hopkins Bloomberg School of Public Health
Director, National Center for Weight & Wellness
Clinical Director, STOP Obesity Alliance,George Washington University School of Public Health/Health Services
Women In Government Annual Healthcare Summit – Washington, DC
November 13, 2014

Quiz
Which of the following results in significantly increased risk of morbidity (disease) and mortality (death)?
a. Diabetes (type 2)
b. Hypertension (chronic high blood pressure)
c. Heart disease
d. Obesity
e. All of the above

Quiz
Which of the following has significant genetic predispositions?
a. Diabetes (type 2)
b. Hypertension (chronic high blood pressure)
c. Heart disease
d. Obesity
e. All of the above

Quiz
Which of the following is governed by a complex system of biological factors (regulatory chemicals, hormones, etc)?
a. Diabetes (type 2)
b. Hypertension (chronic high blood pressure)
c. Heart disease
d. Obesity
e. All of the above

Quiz
Which of the following is associated with food intake and physical activity?
a. Diabetes (type 2)
b. Hypertension (chronic high blood pressure)
c. Heart disease
d. Obesity
e. All of the above

Quiz
Patients with which of the following are routinely regarded as lazy, irresponsible, and lacking self-control, and not given access to evidence-based treatments?
a. Diabetes (type 2)
b. Hypertension (chronic high blood pressure)
c. Heart disease
d. Obesity
e. All of the above

Clinical Obesity Prevalence, Adults, US
National Health and Nutrition Examination Survey, NCHS/CDC

Weight Gain is Normative

Severe Obesity Trends in Adults
Sturm R. Pub Health 2007;121:492-496.

Why Is It So Hard To Manage Weight?

Something Tells You to Breathe…
Because You’re Suffocating


Hypothalamic Appetite Regulation
Farooqi S. Cell Metab 2006;4:260-262

Valentino MA, et al. Clin Pharm & Therapeutics 2010; 87(6):652-62.
Endogenous Signaling of Appetite-regulating Hormones, Neuropeptides, and Neurotransmitters, and The Drugs That Target These Pathways
Why Is It So Hard To Manage Weight?

Hormone Changes and Hunger Persistently
Oppose Diet-Induced Weight Loss
Sumithran P, et al. NEJM 2011.

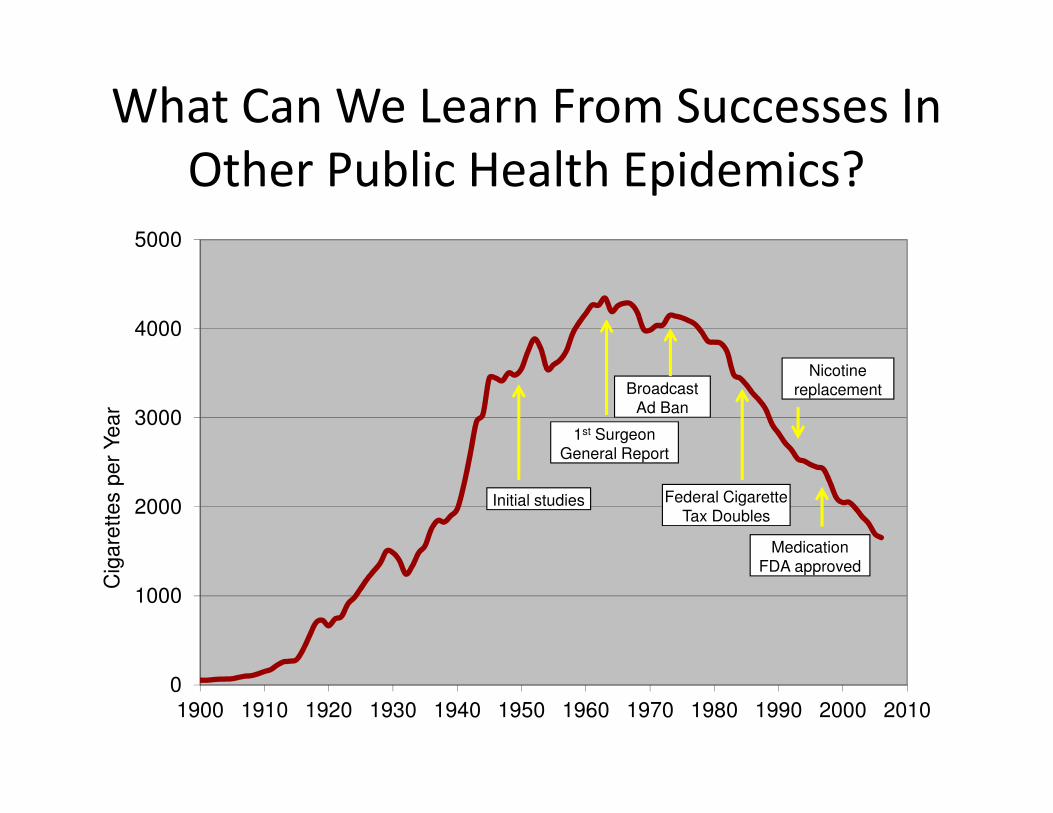
What Can We Learn From Successes In
Other Public Health Epidemics?
Armstrong GL et al, JAMA 1999.
0
1000
2000
3000
4000
5000
1900 1910 1920 1930 1940 1950 1960 1970 1980 1990 2000 2010
Cig
are
tte
s p
er
Ye
ar
Initial studies
1st Surgeon
General Report
Broadcast
Ad Ban
Federal Cigarette
Tax Doubles
Nicotine
replacement
Medication
FDA approved
What Can We Learn From Successes In
Other Public Health Epidemics?

What Can We Learn From Successes In Other Public Health Epidemics?
• Education is necessary, but insufficient
• Prevention and environmental change is
necessary, but insufficient
• Affected patients need access to evidence-
based treatments
• Long term focus
• Multiple parallel approaches

CDC Framework for Addressing Obesity
Individual Factors
Behavioral Settings
Social Norms and Policies
� Home and family
� School
� Community
� Work Site
� Healthcare
� Genetics
� Psychosocial
� Knowledge
� Motivation
� Treatment
� Food and beverage
industry
� Agriculture
� Education
� Media
� Government
� Public health
systems
� Healthcare industry
� Business and
workers
� Land use and
transportation
� Leisure and
recreation
Sectors of Influence

CDC Prevention Recommendations
For Local Governments
http://www.cdc.gov/nccdphp/DNPAO/publications/index.html
Strategies to: • Promote availability of affordable
healthy food• Support healthy food and
beverage choices• Encourage breastfeeding• Encourage physical activity • Encourage communities to
organize for change• Create safe communities that
support physical activity

Chronic Disease State Policies
http://apps.nccd.cdc.gov/CDPHPPolicySearch/Default.aspx#

Treatment Works
Knowler WC, et al. NEJM 2002.
3234 adults with obesity and “pre-diabetes”
Placebo Metformin Lifestyle

Treatment Works
Ann Intern Med, 2012. NEJM 2013.

Treatment Works
Garvey WT, et al. Am J Clin Nutr. 2012;95(2):297-308.
3.7%
1.7%
0.9%
0
0.5
1
1.5
2
2.5
3
3.5
4
Placebo Phn/TPM 7.5 Phn/TPM 15
Pro
gre
sso
rs p
er
year
(%)
76%54%
Annualized Incidence of DM

Combining Treatments Works Even Better
Adapted from Wadden, et al. NEJM, 2005.
Placebo alone
Medication alone
Lifestyle modification alone
Combined therapy

Treatment Works
New England Journal of Medicine, 2007.
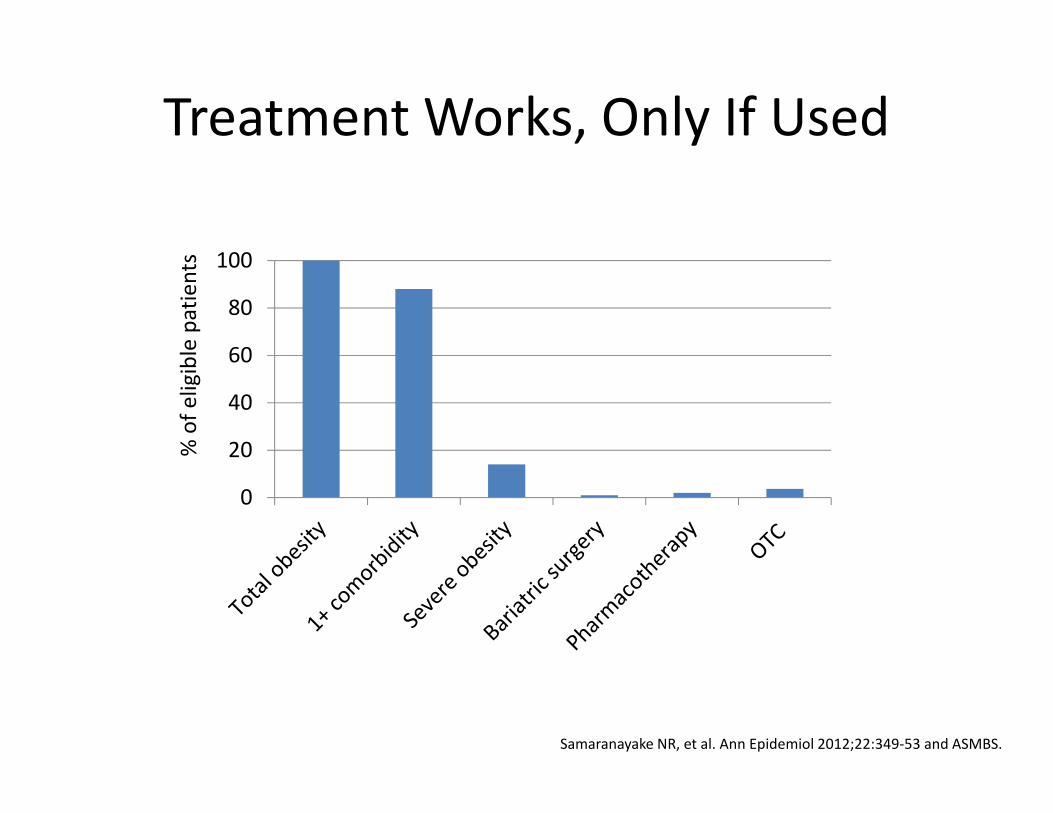
Treatment Works, Only If Used
0
20
40
60
80
100
% o
f e
lig
ible
pa
tie
nts
Samaranayake NR, et al. Ann Epidemiol 2012;22:349-53 and ASMBS.

Obesity Counseling in Medicare
Current CMS coverage in primary care settings:
• 1 face-to-face visit weekly for the first month
• 1 face-to-face visit biweekly for months 2-6
• 1 face-to-face visit monthly for months 7-12 (if 6.6 lb loss)
“Intensive behavioral therapy for obesity…is
reasonable and necessary for the prevention and early
detection of illness and disability and is appropriate for
individuals entitled to benefits [under Medicare].”
CMS. Decision memo for intensive behavioral therapy for obesity (CAG-00423N). November 29, 2011.

Medicaid Coverage of Obesity TreatmentNutrition: 6 states cover all obesity-related nutrition
counseling codes; 22 states cover none
Medicaid Coverage of Obesity-Related Nutrition Counseling Services
RI
WA
MT
ID
OR
CA
NVUT
NMAZ
KS
TX
CO
IA
AROK
ND
SD
NE
LA
WYWI
IL
TN
MS
MO
MN
AL
KY
OH
MI
IN
NC
VA
SC
GA
WV
NY
PA
FL
NJ
DE
MD
CT
MA
NHVT ME
HI
AK
Covers all obesity-related nutritional consult services
Covers some obesity-related nutritional consult services
Covers no obesity-related nutritional consult services
Undetermined/No Data Available
DC
Source: CPT Code Search of Provider Fee Schedules
Note: Common Nutritional Consult Services are defined as CPT codes S9452, 97802-97804, S9470
Kahan et al, 2014 (submitted).

Medicaid Coverage of Obesity TreatmentDisease Management: 0 states cover all obesity-
related disease mgmt CPT codes; 30 states cover none
RI
WA
MT
ID
OR
CA
NVUT
NMAZ
KS
TX
CO
IA
AROK
ND
SD
NE
LA
WYWI
IL
TN
MS
MO
MN
AL
KY
OH
MI
IN
NC
VA
SC
GA
WV
NY
PA
FL
NJ
DE
MD
CT
MA
NHVT ME
HI
AK
Covers all obesity-related disease management and
education services
Covers some obesity-related disease management and
education services
Covers no obesity-related disease management and
education services
Undetermined/No Data Available
DC
Source: CPT Code Search of Provider Fee Schedules
Note: Common Disease Management and Education Services are defined as CPT codes
99078, S0315-S0316, S9445-S9446, 98960-98962
Medicaid Coverage of Obesity-Related Disease Management and Education Services
Kahan et al, 2014 (submitted).

Medicaid Coverage of Obesity TreatmentBehavioral Counseling: 2 states cover all obesity-
related behavioral consult CPT codes; 23 states have
no coverage
RI
WA
MT
ID
OR
CA
NVUT
NMAZ
KS
TX
CO
IA
AROK
ND
SD
NE
LA
WYWI
IL
TN
MS
MO
MN
AL
KY
OH
MI
IN
NC
VA
SC
GA
WV
NY
PA
FL
NJ
DE
MD
CT
MA
NHVT ME
HI
AK
Covers all obesity-related behavioral consult and therapy
services
Covers some obesity-related behavioral consult and
therapy services
Covers no obesity-related behavioral consult and therapy
services
Undetermined/No Data Available
DC
Source: CPT Code Search of Provider Fee Schedules
Note: Common Behavioral Consult and Therapy Services are defined as CPT codes 96150-
96155, S9499, S9451
Medicaid Coverage of Obesity-Related Behavioral Consult and Therapy Services
Kahan et al, 2014 (submitted).

Medicaid Coverage of Obesity Treatment
Medications: 12 states cover obesity medication,
generally with restrictions and prior authorization;
34 states explicitly exclude
Medicaid Coverage of Obesity Pharmacotherapy
Kahan et al, 2014 (submitted).

Medicaid Coverage of Obesity Treatment Bariatric Surgery: 44 states cover bariatric surgery;
5 states explicitly exclude
RI
WA
MT
ID
OR
CA
NVUT
NMAZ
KS
TX
CO
IA
AROK
ND
SD
NE
LA
WYWI
IL
TN
MS
MO
MN
AL
KY
OH
MI
IN
NC
VA
SC
GA
WV
NY
PA
FL
NJ
DE
MD
CT
MA
NHVT ME
HI
AK
Covers bariatric surgery
Explicitly excludes bariatric surgery
Undetermined/No Data Available
DC
Source: State Medicaid Provider Manuals
Medicaid Coverage of Bariatric Surgery
Kahan et al, 2014 (submitted).

Coverage of Obesity-Related Services in
Essential Health Benefit Benchmark Plans
Kahan S, et al. STOP Obesity Alliance – Weight and the States, 2012.

Have you or anyone in your practice been specifically trained to deal with weight related issues? (n = 290)
Not sure: 4%
No answer: 3%
Most PCPs Report No Training in Obesity
Kahan, in preparation

Final Takeaways
• Health, not appearance– Obesity is no different from other chronic, behavior-
related health conditions
• Prevention and Intervention
• Treatment works, despite the aura of futility
• Think long term
• Need innovations– Access to care
– Health professional training
– Community-clinic partnerships
