constipation & diarrhea march 4, 2010. objectives 1. learn an approach to treating constipation...
TRANSCRIPT
Constipation & DiarrheaMarch 4, 2010

Objectives
1. Learn an approach to treating constipation in the Emergency Room and on discharge
2. Discuss when “constipation” needs further workup
3. Diarrhea-discuss the common and important ED presentations

True or False
1) Correction of constipation has been shown to diminish enuresis
2) Correction of constipation has been shown to decrease the frequency of UTI’s
3) Fecal soiling is associated with severe functional constipation
4) Constipation can be a cause of rectal prolapse
5) On digital rectal exam, no stool in the rectal vault is consistent with functional constipation
True or False
6) Vomiting can be a sign of Hirshsprung’s
7) Vomiting can be a sign of functional constipation
8) Celiac disease can present as constipation
9) Constipation is the first symptom of botulism
Few more quick facts
1) When is the 1st stool of a neonate normally passed?
2) Which chemotherapy agent causes constipation?

Definitions
Constipation
Functional Constipation
Definitions
ConstipationDelay or difficulty in defecation, present for
>2 weeks
Functional Constipation Constipation without objective evidence of a
pathologic condition

Case 1
2 month baby, term, formula fed Having 4-5 bowel movements/week Grandma thinks something is seriously
wrong because her other grandchild has 4-5 bowel movements/day
What do you do?
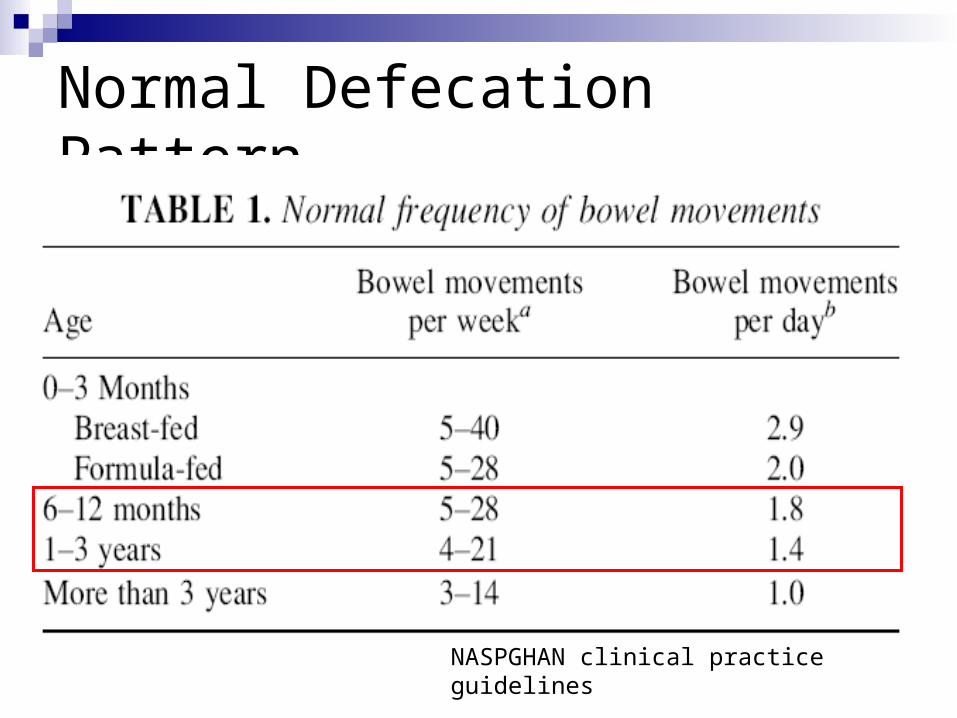
Normal Defecation Pattern

Normal Defecation Pattern
NASPGHAN clinical practice guidelines

Normal Defecation Pattern
NASPGHAN clinical practice guidelines

Approach to Constipation
What is your approach???

Approach to Constipation
Are there any red flags?
Approach to Constipation
Red flagsFeverEmesisBloody diarrheaFTTAnal stenosisTight empty rectumDelayed passage of meconium
If yes….need to investigate further

Approach to Constipation
No red flags=functional constipation Is there fecal impaction?
Yes: disimpact Oral or rectal meds Usually 2-3 days required
No: Treat as outpatient Education, diet, oral meds

Approach to constipation
Treatment effectiveYes: maintence therapy 4-6 monthsNo: Bloodwork
T4, TSH Celiac screen Lead Calcium
If above workup is negative, and child still constipated, refer to GI
But may want to refer for sweat chloride & rectal bx
What about abdominal x-rays?
Not needed if rectal exam reveals large amounts of stoolSens & PPV >80%
If child is obese or refuses the rectal exam, the AXR is reliable in determining fecal retention
If used in combination with DREsens 92% & PPV 94%
NASPGHAN clinical practice guidelines
Case 2
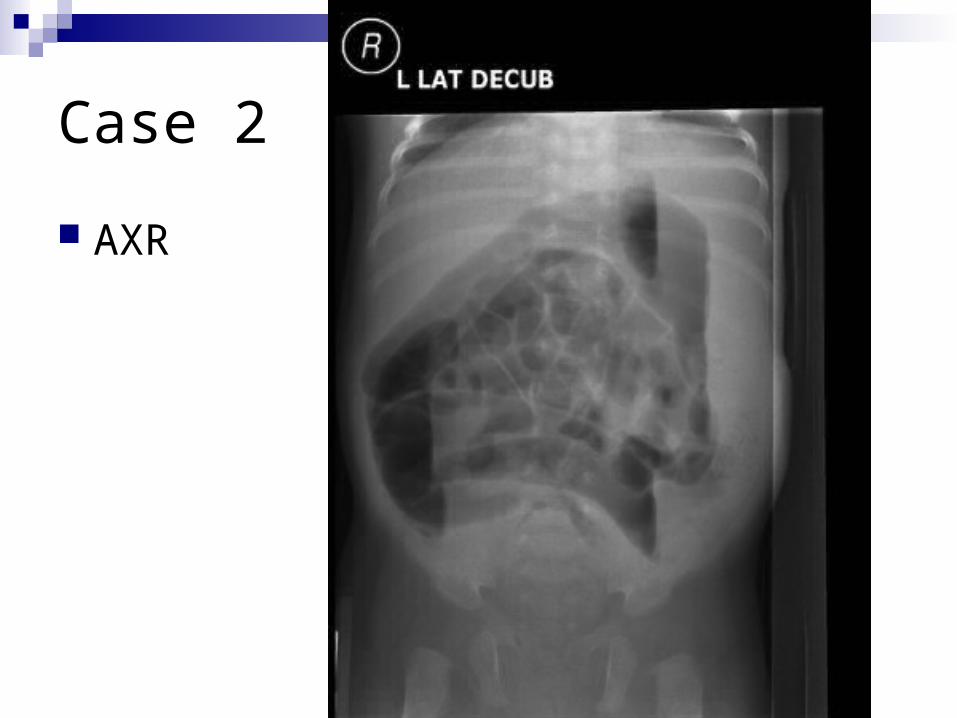
1 month asian male, term, with 12h hx of constipation Prior to presentation, had had 4-5 BM/day Breastfed, feeding less well at last 2 feeds No emesis Had passed meconium within first 24h Neonatal screen Neg for CF and hypothyroid O/E:
alert, slightly fussy, vitals stable distended abdo, +BS No anal fissure Palpable firm stool in rectum

Case 2
AXR
Case 2
AXR
Case 2
Glycerin supp-resulted in dry, crumbly stool in diaper
Attempted enema-came out immediately Manual disimpaction-able to remove dry hard
stool, with overflow liquid seepage After disimpaction, fed well, abdomen softer Arranged for F/U in Urgent Peds for further W/U
(hirshsprung, CF, hypothyroid)
Case 2
Returned to ED the following afternoon Tachypnic Repeat AXR

Case 2


Case 2
Intubated due to respiratory distress Went up to OR for laparotomy…..with pre-op
suspicion of volvulus
Post op dx: Inspissated stool
Workup all negative Sweat chloride, Hirshsprung’s, thyroid
Case 2: Take home message
Be cautious in diagnosing and discharging a 1 month old with constipation!

Case 3
3 month male with distended abdomen & poor feeding
No emesis Passing stool 2-3 times/day Febrile in ED (38.8) What do you want to do? NB question on history: is the stool liquid? (ie
overflow incontinence) NB finding on exam: tight anal sphincter with no
stool in rectum

Hirshsprung Disease
Most common cause of lower intestinal obstruction in neonates
Rare cause of intractable constipation in toddlers & school age childrenDiagnosed after age 3 in 8-20% of pts
Absence of ganglion cells in the myenteric & submucous plexuses of the distal colonSustained contraction of the aganglionic segment
Hirshsprung Disease
EnterocolitisFever, abdo distension, explosive bloody
diarrheaOccurs at age 2-3 months20% mortalityGreatest risk factor is delayed diagnosis of
Hirshsprung’s
The “don’t want to miss” causes of constipation Hirshsprung Disease Cystic Fibrosis Botulism Hypothyroid Imperforate anus Sacral teratoma Sexual abuse Celiac Disease

Botulism
Initial symptom of botulism is constipation Lethargy and feeding difficulties follow P/E:
Decreased DTR, decreased suck & gag Poorly reactive pupils & Ptosis Oculomotor palsies Facial weakness
Dx: Identify C. botulinum spores & toxin in stool* Tx: Admit! 50-77% require intubation
Baby BIG

Treatment of Constipation
Depends on age If <3 months, should have F/U with a
Pediatrician Consists of
“rescue therapy”maintenance therapy

Acute treatment (>1 year)
Fleet EnemaPediatric 66mL, Adult 133mL
Once >2 yrs, use adult enemaOnset 2-5 minutesSide effects:
Hyperphosphatemia Use with caution in renal failure
Osmotic effect in the small intestine draws water into the gut lumen, produces distension,
promotes peristalsis and evacuation

Maintenance Treatment(>1 year) PEG 3350
Osmotic Laxative Dose 1g/kg/d (Max 17g) Onset in 1-3 days Side effects (minimal):
bloating, cramping, diarrhea, flatulence, nausea
Contraindications GI obstruction, ileus, bowel perforation, toxic colitis,
megacolon

Evidence for PEG 3350
RCT, double blind 100 patients (aged 6 months-15 years) After fecal disimpaction, received either PEG or
Lactulose Primary outcomes:
defecation and encopresis frequency/weeksuccessful treatment after eight weeks
Secondary outcomes:Side effects after 8 weeks
Gut. 2004 Nov;53(11):1590-4.
Evidence for PEG 3350
Success defined as:defecation frequency > 3/weekencopresis < once every 2 weeks
ResultsSuccess was significantly higher in the PEG group
(56%) compared with the lactulose group (29%)PEG 3350 patients reported less abdominal pain,
straining, and pain at defecation than children using lactulose

Evidence for PEG 3350
CONCLUSIONS: PEG 3350 compared with lactulose
provided a higher success rate with fewer side effects
PEG 3350 should be the laxative of first choice in childhood constipation

Treatments to avoid
Mineral oil (if <1 yr, use with caution if <3)Lipoid pneumonia if aspirated
Phosphate enemas (if <1 year)Can use glycerine suppository
Stimulant laxatives (long term)SenekotDulcolax

Case 4
2 year female with 4 day hx of constipation & 8 cm rectal prolapse
Has just started toilet training What are you going to do?

Case 4
Other historyHas 2-3 BM/week with ++strainingFecal soiling presentTerm, passed meconium on day 2 of lifeWas admitted to hospital at 18 months with
pneumonia O/E
Weight & height at 5th percentile

Case 4
Other historyHas 2-3 BM/week with ++strainingFecal soiling presentTerm, passed meconium on day 2 of lifeWas admitted to hospital at 18 months with
pneumonia O/E
Weight & height at 5th percentile
Case 4
What is your immediate treatment?
What is the diagnosis? (top 3)
Case 4
What is your immediate treatment Reduce protrusion (pressure with warm compress) Start pt on stool softeners Surgery in refractive cases
What is the diagnosis? (top 3) Cystic Fibrosis Chronic constipation Meningocoele

True or False
Correction of constipation has been shown to diminish enuresis
TRUE

True or False
Correction of constipation has been shown to decrease the frequency of UTI’s
TRUE
True or False
Fecal soiling is associated with severe functional constipation
TRUE
True or False
Constipation can be a cause of rectal prolapse TRUE but….need to also consider other
etiologies Cystic Fibrosis Meningocoele Enterobius vermicularis (pinworm) Ehlers-Danlos Ulcerative colitis Pertussis
True or False
On digital rectal exam, no stool in the rectal vault is consistent with functional constipation
FALSE

True or False
Vomiting can be a sign of Hirshsprung’s TRUE
True or False
Vomiting can be a sign of functional constipation
FALSE
True or False
Constipation is the first symptom of botulism
TRUE
Quick Facts
When is the 1st stool of a neonate normally passed?
99% pass stool within 24 hours and 100% pass stool within 48 hoursPrems may be a little delayed (76% pass
within 24 hours and 98.8% pass within 48h)
Quick Facts
Which chemotherapy agent causes constipation?
Vincristine


Diarrhea

True or False
1) Salmonella enteritis can be safely treated as an outpatient
2) 40% of infants are colonized with C. diff3) Amoxicillin is responsible for most cases of
pseudomembranous colitis in children4) Switching to a lactose free formula is helpful
during an acute diarrheal illness5) Toddlers diarrhea is the most common cause of
chronic diarrhea in children between the ages of 12-36 months

Diarrhea
Definition
The “not to miss” diagnoses (4)
Diarrhea
Definition Softening in the consistency of the stool with or
without an increase in the number of stools
The not to miss diagnoses (5) Intussusception Pseudomembranous Colitis Hemolytic Uremic Syndrome Appendicits Salmonella enteritis with bacteremia
Diarrhea & Gastroenteritis
Usually no investigations are requiredwatery diarrhea in previously healthy children
Once diarrhea is bloody….do the testsBlood and stool cultures, U/A, CBC, BUN/Cr
Risk factors for bacteremia from gastroFever >5days and child <12 months
Remember to ask about reptiles in the house
HUS Initially mild gastroenteritis Hematochezia Pallor(microangiopathic hemolytic anemia) Purpura (Thrombocytopenia) Hematuria Renal Failure
If parents tell you that the kid hasn’t peed in 24 hours, take them seriously

HUS
Most often in kids <4 years E. coli 0157:H7
Avoid antibiotics in patients with acute enteritis presumed secondary to E.coli 0157
Take home pointDo CBC, Cr, urinalysis in kids with bloody
diarrhea (as well as stool & blood cultures)

Salmonella enteritis
Salmonella gastroenteritis is usually self-limited Fever generally resolves within 48 to 72 hours Diarrhea resolves within 4 to 10 days
BUT…in infants 5-40% will have +blood culture So….children <3 months (some say 1 year) with
symptomatic salmonellosis should be treated with antibiotics until blood cultures are negative Cefotax 100-200mg/kg/d div q6h Ceftriaxone 75mg/kg/d OD
Pseudomembranous colitis
Despite high carrier rates, illness is uncommon in neonates & infants
Abdominal distension, fever and bloody stools are the key physical findings
May occur several weeks after antibiotics Tx:
Discontinue current antibiotic Metronidazole 20-40 mg/kg/d div q6h PO 2nd line Vanco (if really severe, combine flagyl &
vanco) Admit to monitor for toxic megacolon

Case 5
4 month male with daily diarrhea (6x/d) Pretty bad eczema Admitted to hospital at 3 months of age
with pneumonia O/E: weight 4.5kg What are you going to do before sending
this child home?

Case 5
4 month male with daily diarrhea (6x/d) Pretty bad eczema Admitted to hospital at 3 months of age
with pneumonia O/E: weight 4.5kg (Failure to thrive) What are you going to do before sending
this child home?
Case 6
12 month female 5 loose stools/day Mom thinks that occasionally she is bloated Thriving No history of eczema 2 previous URTI’s What do you think the diagnosis is? Mom asks if this could be lactose
intolerance….what do you think?
Normal Defecation Pattern
NASPGHAN clinical practice guidelines
Toddler’s Diarrhea
Occurs at age 1-3 years History of excessive carbohydrate containing
beverages (specifically sorbital- found in apple, pear & prune juice)
Stools occur during the day (not at night) May contain undigested food particles
Limit sugar containing drinks and increase fat in the diet to 40%
Fluid restriction to <90ml/kg/d
Lactase Deficiency
Congenital lactase deficiency is RARE!<50 cases worldwideSo….when a parent is worried that their infant
is lactose intolerant and this is causing diarrhea….reassure that this is not the cause of their diarrhea (unless their child is #51 in the world)
Secondary Lactose Intolerance
Common Follows small bowel mucosal damage
Ie. Rotavirus, Celiac disease Transient & resolves with mucosal healing Treatment (classically)
Milk free diet or lactose-free formulaBut clinical trials haven't shown a benefit in
acute infectious diarrhea for the majority of infants
Use of Probiotics
Lactobacillus, Bifidobacterium, Saccharomyces
There are RCT’s supporting their use in acute infectious diarrhea and C. diff In rotavirus-diarrhea is briefer and milder
However, therapy is not yet standardized and the most effective organism has not been identified
True or False
Salmonella enteritis can be safely treated as an outpatient
TRUE IF >12 months (possible if >3mo)

True or False
40% of infants are colonized with C. diff TRUE
True or False
Amoxicillin is responsible for most cases of pseudomembranous colitis in children
TRUEBecause of the frequency it is prescribed

True or False
Switching to a lactose free formula is helpful during an acute diarrheal illness
FALSE
True or False
Toddlers diarrhea is the most common cause of chronic diarrhea in children between the ages of 12-36 months
TRUE

Objectives
1. Learn an approach to treating constipation in the Emergency Room and on discharge
2. Discuss when “constipation” needs further workup
3. Diarrhea-discuss the common and important ED presentations
Questions?