constraints with the avaliable immuno … · tdr results onto whole blood hôpital saint louis,...
TRANSCRIPT

CONSTRAINTS WITH THE AVALIABLE IMMUNO-SERO-VIROLOGICAL
DIAGNOSTIC TESTS IN RESSOURCE LIMITED COUNTRIES
François SimonCHU saint Louis – Lariboisière, Paris
• 1- Can we improve the HIV diagnosis strategy in POC ?
• 2- Can we move the viral load/resistance monitoring from Regional to District ?
HIV in RESSOURCE LIMITED COUNTRIES
HOW TO DO MORE WITH LESS !!

• HIV screening in UE
1- Test-and-Treat Strategy for HIV in Resource-Limited Settings ?
• in P O C
4th generation EIAAg & Ab detection
High sensitivity, similar to NAT
RDT on serumon capillary or whole blood
FDA approved 2010

- Large number of studies, including in P O C
- But no comparative studies between the different RDT assays
- Real time evaluation with oral fluid and capillary whole blood are difficult
- No primary infection with whole blood or OF , no reference panel for diversity
ARE THE RDT RELIABLE IN POC ?

> 80 RDT in 2010agressive marketing
HIV onto urineFDA labelled
in 2010
= number of RDT are commercialized by non- healthca re manufacturer with no visibility in quality assuranc e

TRANSACTION VOLUMES OF RAPID HIV TESTS (WHO 2009)
the overall RDT diagnostics sector has had sluggishgrowth but few major manufacturers involved

HIV RAPID DIAGNOSTIC TESTSARE THE RDT RELIABLE ?
Nucleic acid testing (NAT) in routine HIV in testing programs versus RDT , San Diego, California
• RDT : Oraquick
• 3151 persons tested
RDT missing 15 about 79 (19%) of the positive samples
Morris et al Ann Intern Med. 2010 Jun 15;152(12):I30

RDT IN A HEALTHCARE SETTING : A COMPARATIVE STUDY OF RDT SENSITIVITY
- Hôpital Saint Louis, Paris 2009
- 200 adults : HIV-1 (n=194) or HIV-2 infection (n=6)
- 5 HIV rapid tests using either oral fluid or finger-stick whole blood
Sensitivity ranged from 86.5% to 99%
Rapid HIV tests were -less sensitive on oral fluid than on whole blood- less sensitive on finger-stick whole blood than on serum
Pavie et al, PlosOne 2010
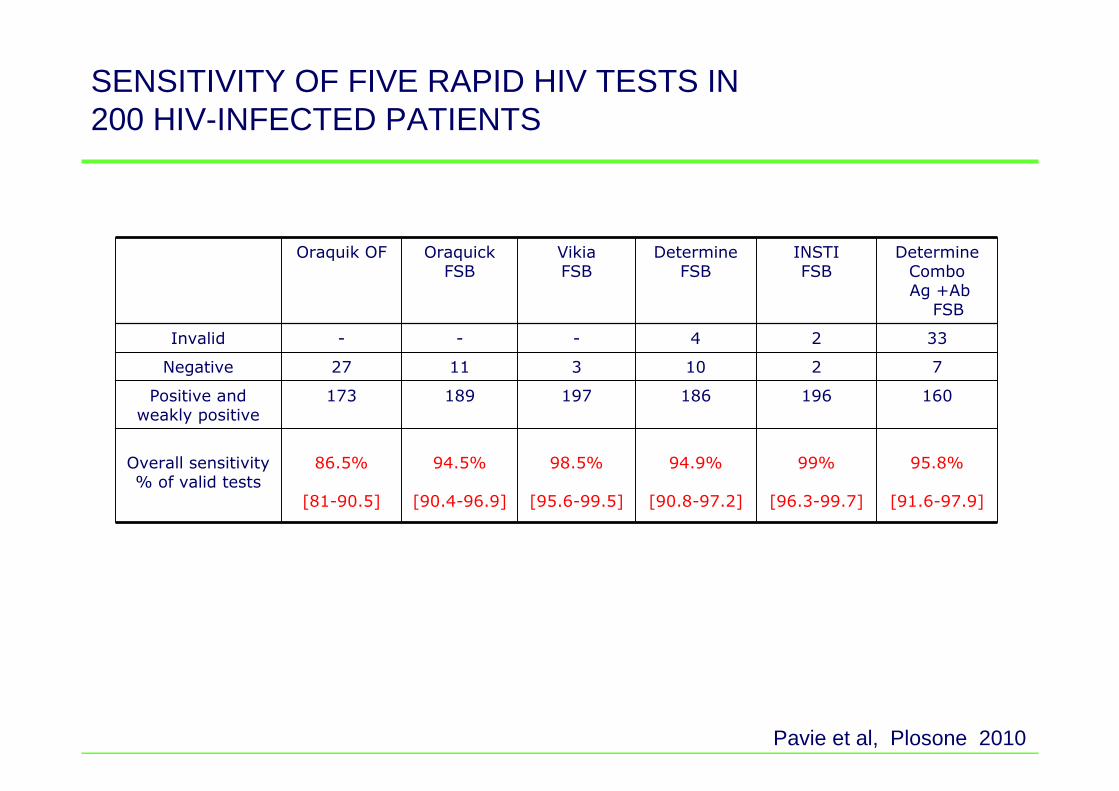
SENSITIVITY OF FIVE RAPID HIV TESTS IN 200 HIV-INFECTED PATIENTS
Oraquik OF Oraquick FSB
VikiaFSB
DetermineFSB
INSTIFSB
Determine ComboAg +Ab
FSB
Invalid - - - 4 2 33
Negative 27 11 3 10 2 7
Positive and weakly positive
173 189 197 186 196 160
Overall sensitivity % of valid tests
86.5%
[81-90.5]
94.5%
[90.4-96.9]
98.5%
[95.6-99.5]
94.9%
[90.8-97.2]
99%
[96.3-99.7]
95.8%
[91.6-97.9]
Pavie et al, Plosone 2010
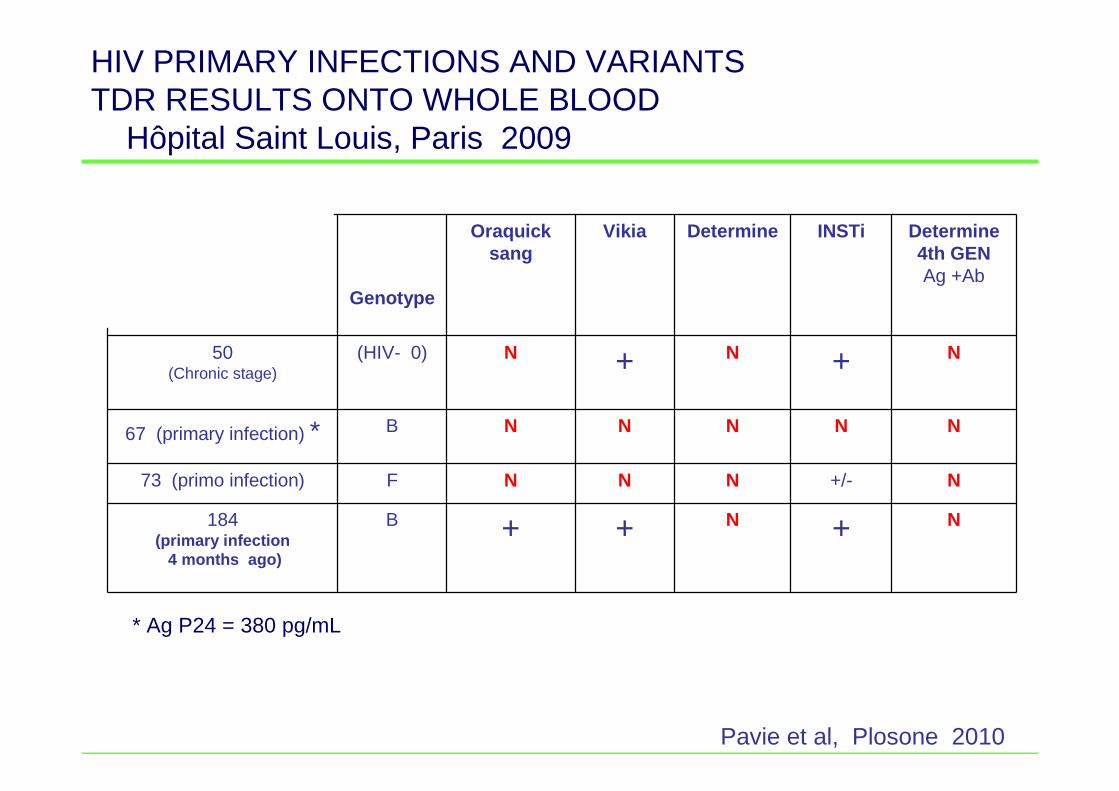
Genotype
Oraquick sang
Vikia Determine INSTi Determine 4th GENAg +Ab
50(Chronic stage)
(HIV- 0) N + N + N
67 (primary infection) * B N N N N N
73 (primo infection) F N N N +/- N
184 (primary infection
4 months ago)
B + + N + N
* Ag P24 = 380 pg/mL
Pavie et al, Plosone 2010
HIV PRIMARY INFECTIONS AND VARIANTS TDR RESULTS ONTO WHOLE BLOOD
Hôpital Saint Louis, Paris 2009

REVISED RECOMMANDATIONS FOR THE SELECTION AND USE OF HIV ANTIBODY TESTS
* WHO – Wkly Epidemiol Rec 1997, 72: 81-87
1°°°° screening assay Result2°°°° screening assay
Screening assay ResultConfirmatory assay
Conventional strategy
Alternative strategy

1892/09 780/09 133/08 130/08 1723/07 1946/09 1937/09 Determine 3G HIV1/2 + + + + - + +
Immuno HIV 1/2 - + - + + + +
Vikia HIV 1/2 + - - -
Retro check - - +
SD bioline + - -
Ag P24 - - - - -
CV Taqman V2.0 - -
EIA Architect Abbott - - - - - - -
Conclusion OMS P P P P P P P Conclusion SLS N N N N N N N
FAILURE IN WHO ALGORITHM : A ROUTINE SCREENING IN CAMEROON IN 2009
Tokombéré, JM Huraux, 2009
Failure in WHO strategy II leading to a false positivity reportFailure in western blot identification
WHO conclusion
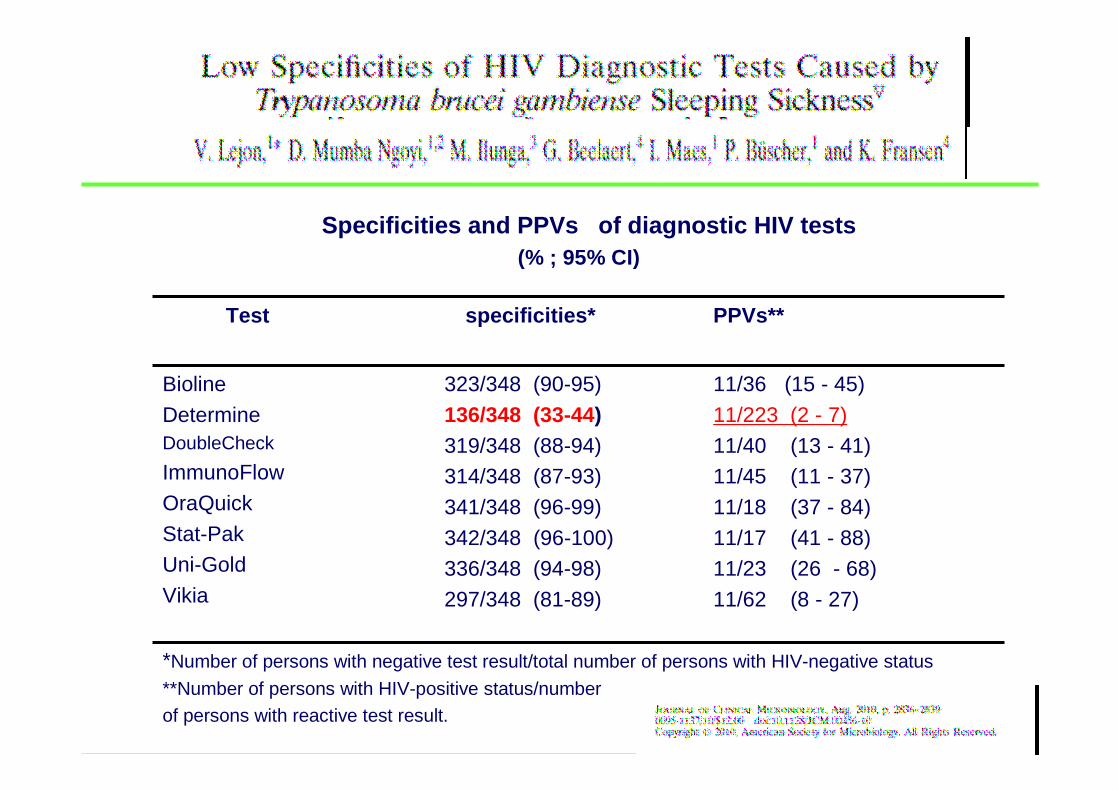
Specificities and PPVs of diagnostic HIV tests (% ; 95% CI)
Test specificities* PPVs**
Bioline
DetermineDoubleCheck
ImmunoFlow
OraQuick
Stat-PakUni-Gold
Vikia
323/348 (90-95)
136/348 (33-44)319/348 (88-94)314/348 (87-93)
341/348 (96-99)
342/348 (96-100)336/348 (94-98)
297/348 (81-89)
11/36 (15 - 45)
11/223 (2 - 7)
11/40 (13 - 41)11/45 (11 - 37)
11/18 (37 - 84)
11/17 (41 - 88)11/23 (26 - 68)
11/62 (8 - 27)
*Number of persons with negative test result/total number of persons with HIV-negative status
**Number of persons with HIV-positive status/number of persons with reactive test result.

RDT AND CONFIRMATORY STRATEGIESWHO RECOMMENDATIONS
The assumption that each test perform independently is the corner stoneof WHO 2 - tests strategy
11 % 89.6% 5 % 77.8% 2 % 57.6 %
Prevalence WHO 2-tests strategyPositive predictive value*
*

• Difficulties of conducting independent evaluations
• Lack of sensitivity and of specificity
• RDT and EIA serological assays are not independent , all being based onot gp41 reactivity
• WB is costly with an high rate undetermined samples
• A new algorithm is badly needed , based on the association of with a sensitive serological screening test and a specific molecularindependent assay
RDT : TO REDUCE THE COST BUT NOT AT ALL PRICE

HIV DIAGNOSIS IN AFRICA : PROPOSAL FOR A SERO-MOLECULAR ALGORITHM
RDTPOC
Whole bloodPlasma
HIV-1RNA NAT
VL on DBS
+
HIV-2 RDT
HIV-1 reportHIV-2 report
-
primaryinfection or variant
suspected
-
+
-New sample
andretest
RDT and Viral loadare both independent assays
Collect a new sample onto DBS
Refer tocentral lab
+
Persistance :Refer to Central for Blot
(LTNP) , peptides (Variant)

HIV MONITORING IN AFRICA
• Viral load alerts to non-adherence, treatment failure and HIV resistance
• HIV-1 diversity is now over-passed by the new assays
• Is Cost effective to Guide Switching Antiretroviral Therapy in Resource-limited Settings
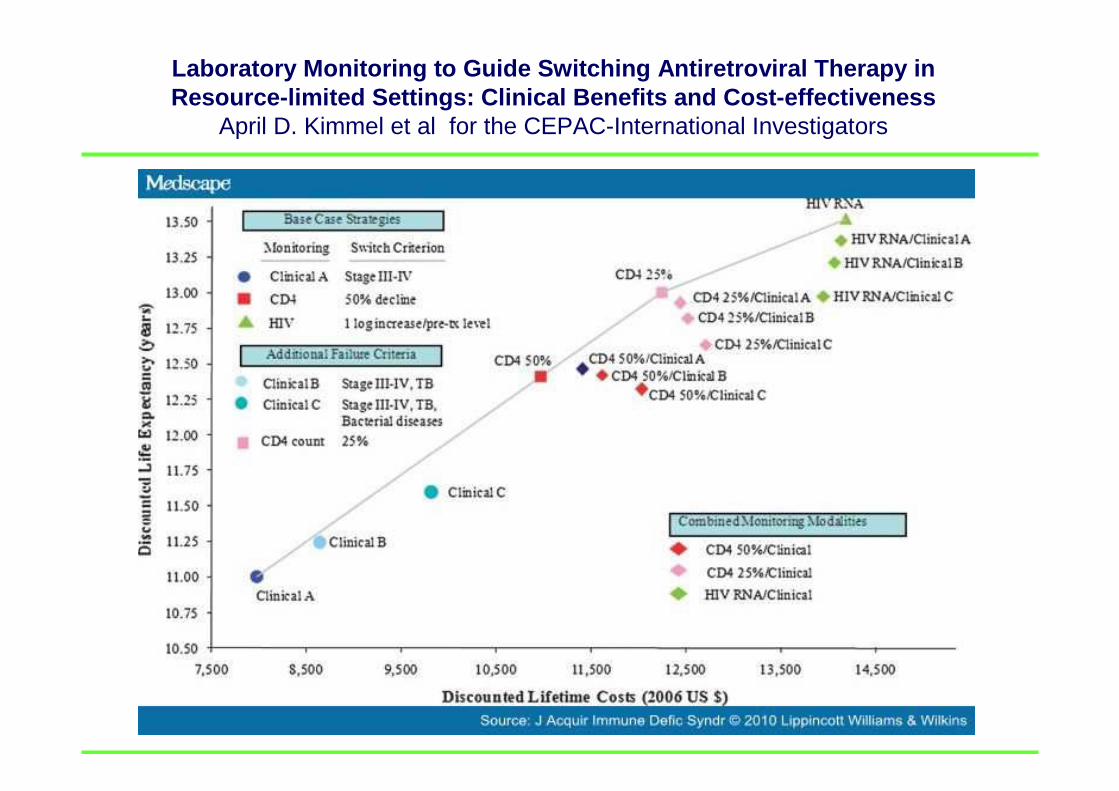
Laboratory Monitoring to Guide Switching Antiretrov iral Therapy in Resource-limited Settings: Clinical Benefits and Co st-effectiveness
April D. Kimmel et al for the CEPAC-International Investigators

Is a • Simple • Cheap • Reliable • Sensitive* • Individual • Disposable• No power• No cold chain, • no freezer, • no maintenance• Rapid
HIV VIRAL LOAD MONITORING IN RESOURCE-POOR SETTINGS LOCATIONS
* At least equivalent to 3 to 4 log equivalent RNA copies/mL
available in a near** future ?
•Cepheid, SAMBA, Inverness, CIGHT, Iquum Liat, Micronics DxBox, Wave 80 ESCAPE-20•Most are still in proof of concept•No field evaluations
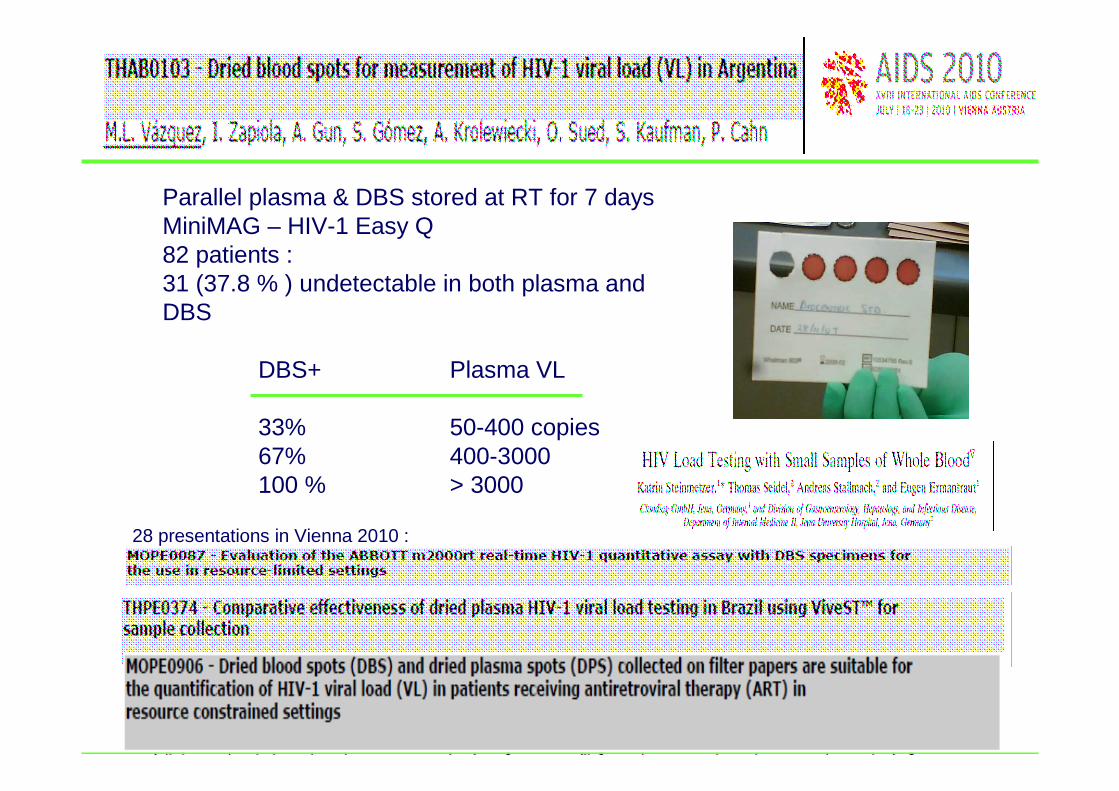
Parallel plasma & DBS stored at RT for 7 daysMiniMAG – HIV-1 Easy Q 82 patients :31 (37.8 % ) undetectable in both plasma and DBS
DBS+ Plasma VL
33% 50-400 copies67% 400-3000100 % > 3000
28 presentations in Vienna 2010 :

Plasma VL(Log
cop/ml)
DBS storage ( °°°°C) WO W2 W4 W8
< 1.6-20°°°°C
RT37
< 1.6 Not done< 1.6< 1.6< 1.6
< 1.6< 1.6< 1.6
1.8-20°°°°C
RT37
<1.6 Not done
< 1.6 < 1.6< 1.6
< 1.63.3
< 1.6
3.1-20°°°°C
RT37
3.63.63.73.6
3.63.53.7
3.53.73.8
3.5-20°°°°C
RT37
3.84.24.34.3
3.94.23.9
4.14.03.8
4.3-20°°°°C
RT37
4.6 Not done4.54.54.5
4.54.44.5
4.4-20°°°°C
RT37
4.64.95.35.2
4.64.94.9
4.54.94.7
4.5-20°°°°C
RT37
4.7 Not done4.64.84.8
4.14.44.5
Evaluation of VL and genotyping on DBS under different storage conditionsM Arredondo et Al

Dried Blood Spot HIV-1 RNA Quantification Using Open Real-Time Systems in South Africa and Burkina Faso
- 892 DBS HIV-1-positive pregnant women and their neonates
- For early infant diagnosis, the sensitivity and specificity were 100%
- DBS viral load kinetics were similar to those in plasma in treated patients
J Acquir Immune Defic Syndr. 2010 Aug 10. [Epub ahead of print]
Vilijoen et al, WHO-ANRS 1289 Kesho ora study group

IS ULTRA SENSITIVE P24 AG AN ALTERNATIVETO THE NAT IN POC ?
• The p 24 antigen or core antigen forms the conical core of the viral particle
• Interacts with Cyclophilin A, leading to its incorporation into the virion
• Complex crystal structure
• 13 potential antigenic sites with 2 major epitopes in the CypA binding loop and adjacent helices and at the end of the C-terminal domain.
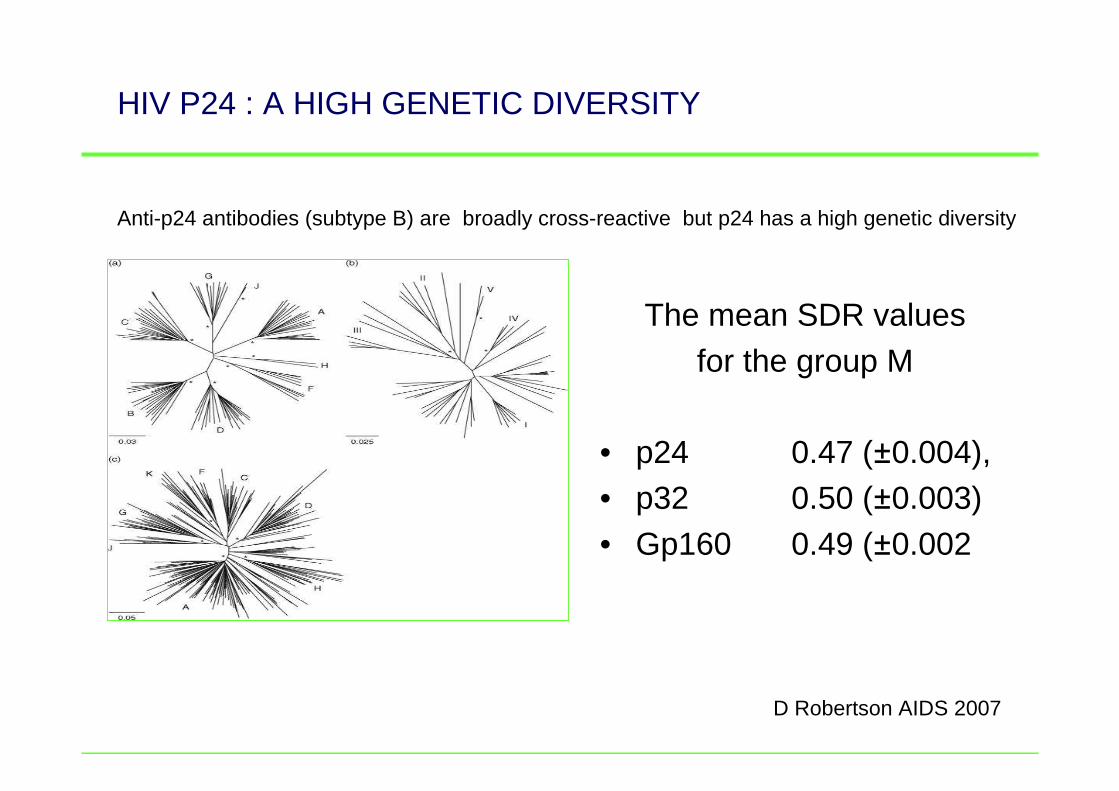
HIV P24 : A HIGH GENETIC DIVERSITY
The mean SDR values for the group M
• p24 0.47 (±0.004), • p32 0.50 (±0.003) • Gp160 0.49 (±0.002
D Robertson AIDS 2007
Anti-p24 antibodies (subtype B) are broadly cross-reactive but p24 has a high genetic diversity

HIV P24 : A HIGH GENETIC DIVERSITY SAINT LOUIS 2010
0,01
0,1
1
10
100
1 2 3 4 5 6 7 8 9 10 11 12 13 14
Série1
Série2
0,01
0,1
1
10
100
1 2 3 4 5 6 7 8 9 10 11 12 13 14
Série1
Série2
14 samples Subtype B 14 samples non-subtype B
Viral load Log
Viral load Log
Agp24 reactivity ratio Agp24 reactivity ratio
28 HIV- patients naives of HAART, chronically infectedR Nabias 2010
VL
Ag p24 Ag p24
VL
ULTRASENSITIVE HIV-1 P24 ANTIGEN & DBS ?
• 38 Tanzanian children
• DBS-p24, 32 (84%) of 38 (subtype D FN)
• DBS DNA, 30 (79%) of 38 ; – plasma-p24, 23 (85%) of 27 ;– plasma RNA, 30 (100%) of 30
– But is the p24 EIA more simple to perform than VL assay ??
SchSchüüpbach Jpbach J.. J Acquir Immune Defic Syndr. 2007 Mar 1;44(3):247-53
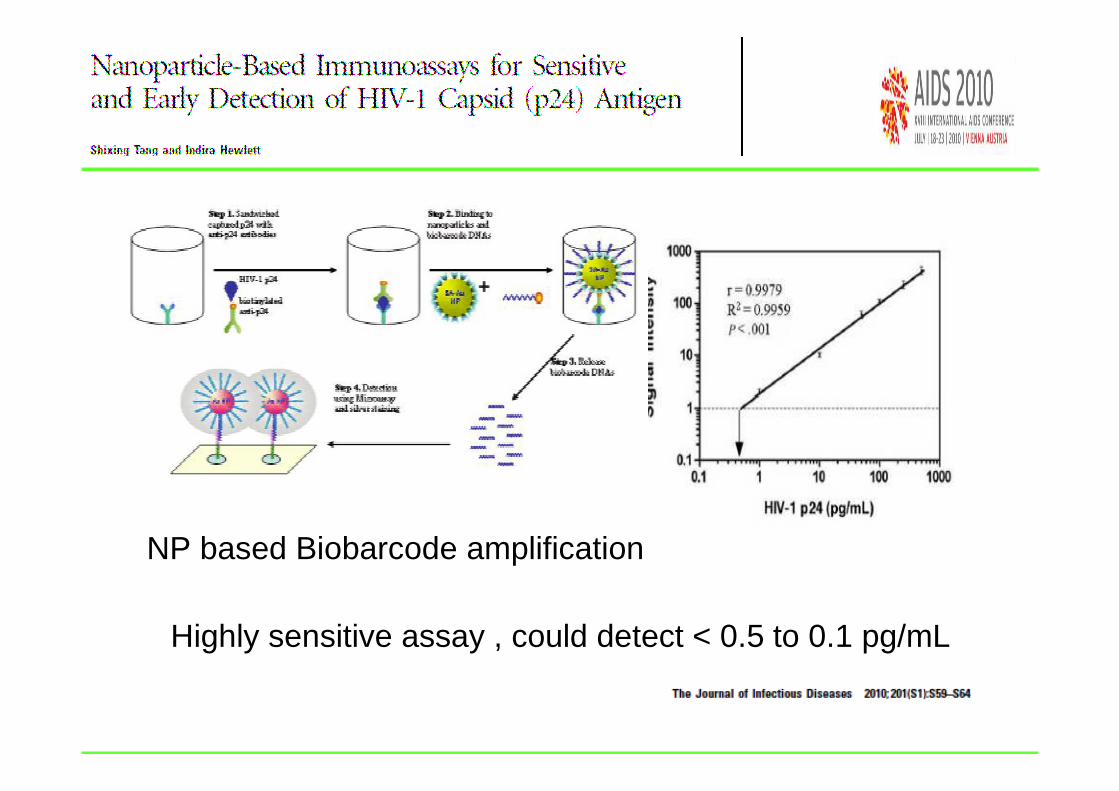
Highly sensitive assay , could detect < 0.5 to 0.1 pg/mL
NP based Biobarcode amplification

THE FIRST COMMERCIAL AG P24 RAPID TEST LACKS OF SENSITIVIY
AgP24(pg/ml)
> 400 400-100 100-50 50-5
Référence
EIA P24
VIDAS
6 4 5 17
Determine 4eme G
Ag POSITIF
4 3 1 0
JC Tardy , Lyon 2009
32 HIV-1 p24 positive sera by EIA
Competitive field and technical improvement will come soonWith and without decomplexation

development of a low-cost dipstick p24 antigen assay
Heat shock methods to disrupt immune complex
Analytical sensitivityof 50 pg/mL
Equivalent to4.6 log or RNA
Ag only Ab + Ag
A NEW ACADEMIC SIMPLE AND CHEAP DIPSTICK FOR AG P24 AND AB+AG DETECTION
Ab only
c

D. Glencross, MOPE0080 Wien 2010
CD38 on CD8 = correlate with CD4 & VLReliable marker of declining VL
73 pts, regular follow up 180 weeksin 62% successfully used : VL decreasing in 12% rises in CD38 : increased VLin 26% fluctuations with no matching
? Elevated CD38 -> VL monitoring ?
CD38 ACTIVATION AS ALTERNATIVE TO VIRAL LOAD FOR MONITORING
CONCLUSIONS :
• In a POC setting
– - RDT : new sensitive and specific RDT badly needed – DBS and new confirmatory strategy for diagnosis– - US p24 unitary RTD sensitive and cheap : in progress
• At the district level– new immunological follow up like CD38 – DBS and viral load– new VL technologies
PROJET PASCALPROJET PASCAL
PAPArtnership for SCSCaling up AAccess to viral LLoad testing in resource-constrainedsettings
CHU Saint Louis Paris
Laboratoire associéau Centre National de Référence du VIH
Faculté de Médecine-Pharmacie
Université de Rouen
J. Christophe PlantierMarie Gueudin
François SimonConstance Delaugerre
J. Michel Molina
PATIENTS, NURSES, TECHNICIANS AND ALL THOSE MAKING THESE STUDIES POSSIBLE
Eric Laforgerie
AKNOWLEDGMENTS
HIV IN LOW-RESOURCE SETTINGS: HOW TO DO MORE WITH LESS