consumer engagement in self management and prevention of...
TRANSCRIPT

Consumer Engagement in
Self Management and
Prevention of Diabetes
Global Snapshot
People living with diabetes:
- over 371 million world wide
- 63 million in India
- 92 million in China (* 114 million)
4 out of 5 cases are in low / middle income countries
Next 20 years - Africa will have the highest % increase
Diabetes killed 4.8million people in 2012 – more than
HIV and TB combined
Australian Perspective
More than 1.5 million Australians have diabetes
Over 1,100,000 Australians actually diagnosed
280 Australian’s diagnosed everyday
2 million at high risk (pre-diabetes)
32% of preventable hospital admissions are diabetes
related
Set to become No 1 burden of disease
Australian Perspective
Type 1 diabetes – 120,000
Type 2 diabetes – 950,000
Insulin treated – 202,000
Gestational diabetes – 25,000 per year
May be one person with silent, undiagnosed type 2
diabetes for every person diagnosed.
Prediabetes (high risk) – more than 2 million
The Seriousness
• 2-4 times more likely to develop cardiovascular disease
(heart attacks and strokes)
• Most common cause of blindness in adults
• Leading cause of kidney failure
• Limb amputation – four times the risk
• Depression and mental well being
• Erectile dysfunction
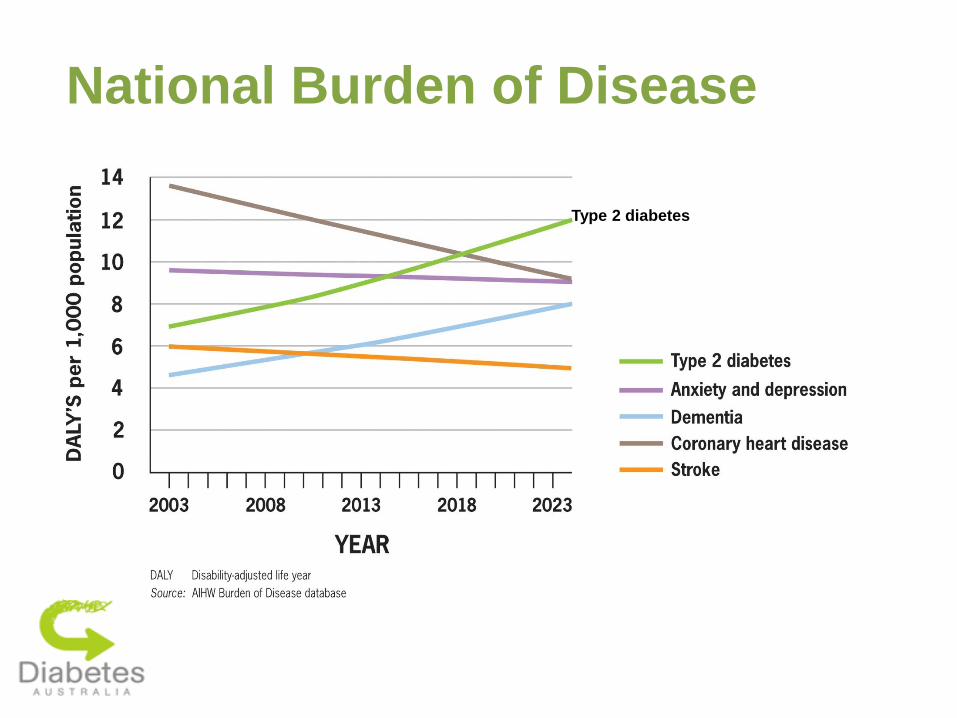
National Burden of Disease
Type 2 diabetes

HOMA=homeostasis model assessment.
Adapted from Holman RR. Diabetes Res Clin Pract 1998;40(suppl 1):S21―5.
Type 2 diabetes is a progressive condition
-c
ell f
uncti
on (
% o
f norm
al by H
OM
A)
Time (years)
0
20
40
60
80
100
―10 ―8 ―6 ―4 ―2 0 2 4 6
Time of diagnosis
?
Pancreatic function
= 50% of normal

Type 2 diabetes
• Insulin resistance
• Beta cell degradation leading to relative insulin deficiency
• 50% will require insulin therapy within 6-10yrs of
diagnosis. Some immediately on diagnosis.
• Serious and complex
• But….people blamed for getting type 2 diabetes!!
• Stigma and distress

Gradual loss of glycaemic control occurs despite various oral treatment regimens M
ed
ian
Hb
A 1
c (
%)
Lifestyle only (n = 200)
Chlorpropamide (n = 129)
Glibenclamide (n = 148)
Metformin (n = 181)
0 2 4 0
6
7
8
9
6 8 10
Years from randomisation
Upper limit of normal 6.2%
ADA goal 7%
Overweight Patients With T2DM in the UKPDS
ADA=American Diabetes Association.
Adapted from UK Prospective Diabetes Study (UKPDS) Group. Lancet. 1998;352:854-865.
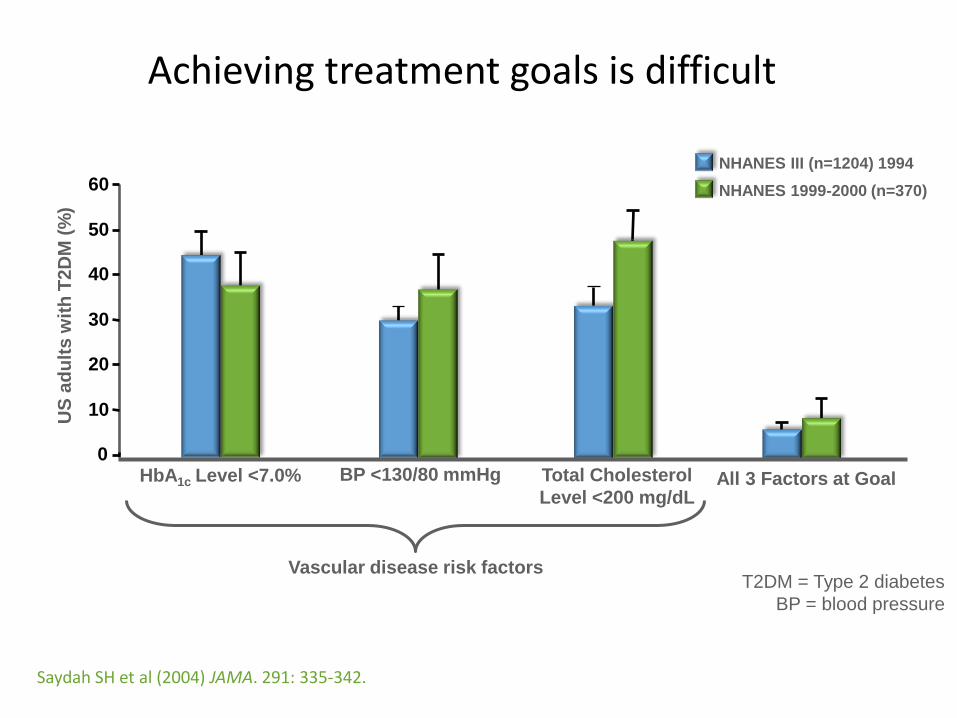
Saydah SH et al (2004) JAMA. 291: 335-342.
US
ad
ult
s w
ith
T2
DM
(%
)
Vascular disease risk factors
0
10
20
30
40
50
60
HbA1c Level <7.0% BP <130/80 mmHg Total Cholesterol
Level <200 mg/dL All 3 Factors at Goal
T2DM = Type 2 diabetes
BP = blood pressure
NHANES III (n=1204) 1994
NHANES 1999-2000 (n=370)
Achieving treatment goals is difficult

Improving self-management…
‘…will have a far greater impact on the health of the population than any improvement in specific medical treatments’
(World Health Organisation, 2003)

8,760 hours spent alone with diabetes

Looking beyond HbA1c, at the person
• 70-82% worry about complications
• 58-69% feel hopeless when they think about complications
• 51-66% feel diabetes controls their life
• 30-60% experience diabetes-related distress
• 10% experience clinical levels of depression
• In type 1, 20% have impaired awareness of hypoglycaemia
• In type 2, 28% unwilling to use insulin if prescribed
• On average, diabetes impacts negatively on quality of life

International guidelines recommend
• ‘Emotional well-being [as] part of
diabetes management’ (ADA, 2006)
• Routine monitoring of
psychological well-being
‘…should be integral part of
routine care’ (IDF, 2005)
• Structured education as an
‘…integral part of management’ (IDF, 2005)
International Diabetes Federation, 2005
Rationale for structured education
• Self-management = cornerstone of successful diabetes
outcomes
• Effective self-management often requires
a radical change in behaviour
• Health professionals perceive they are offering adequate
education
– Mostly 1:1; problem-focused; lacking theoretical basis
• Few people with diabetes feel they have the skills they
need and quality of life is impaired
• Structured education is equitable, effective, evidence-
based, scalable and cost-saving

CASE STUDY: DAFNE
What is DAFNE?
• structured self-management
education program for T1DM
– skills training to replace insulin by
matching it to CHO on a meal-by-meal
basis: “the end of the diabetic diet”
– adult education principles to facilitate
new learning
– emphasis on building confidence &
appropriate independence
– 5-day outpatient group program
(6-8 people) in secondary care
• Delivered by 2+ trained educators
(DSNs & dietitians)
dose adjustment for normal eating

OzDAFNE am
• Dose Adjustment For Normal Eating
• Evidence based 5-day intensive program for adults with type 1 diabetes
• Strong focus on carbohydrate counting and insulin dose adjustment
• Insulin is matched to lifestyle not the other way round
• Teaches self management skills regarding exercise, illness, alcohol, eating out, travel
• Principles are very similar to pump therapy
• Can self refer

CASE STUDY: DESMOND
What is DESMOND?
• structured self-management
education program for people
newly diagnosed with T2DM
• Underpinned by strong
philosophy of care and
psychological / educational
theory
• Delivered as 1 day or 2 ½ days
• Delivered by 2 trained
educators
• Delivered in Primary Care
Insulin pump therapy
• Type 1 diabetes
• Continuous rapid acting insulin infusion
• Cost involved around $8000 for pump, $15-20/month for consumables (NDSS)
• Can be updated after 4 years
• PHI will cover cost of pump, if member for over 1 year
• Advantages: more flexibility, stable control
• Be willing to test BGL frequently
• Worn for 24 hours but can be disconnected for up to two hours


A New National Diabetes Strategy
Prevention, Prevention, Prevention
Primary Prevention
Prevention of unhealthy food and physical activity
environments through public health initiatives, whole of
community programs, social marketing.
•Front of pack labelling
•Reducing marketing and promotion of junk food to kids
•Food reformulation
•Promote active living
•Active transport

- Nelson Mandela
“There can be no keener
revelation of a society's
soul than the way in
which it treats its
children.”
Knowledge
Motivation
How Best to Make Change?
Educate
Implore
Medicate
Operate
The
Individual Less Obesity?
Disastrous Defaults (examples)
• The economics of food
• Food marketing
• Portions
• Too much access
• Too little access


RWJF $100
million/yr vs.
Child
Marketing
January 4!

• Single greatest source of added sugar
• Poor calorie compensation
• Sugar may be addictive
• Gratuitous addition of caffeine
• Completely empty calories
Why Soft Drinks?
• Rock solid proof of harm
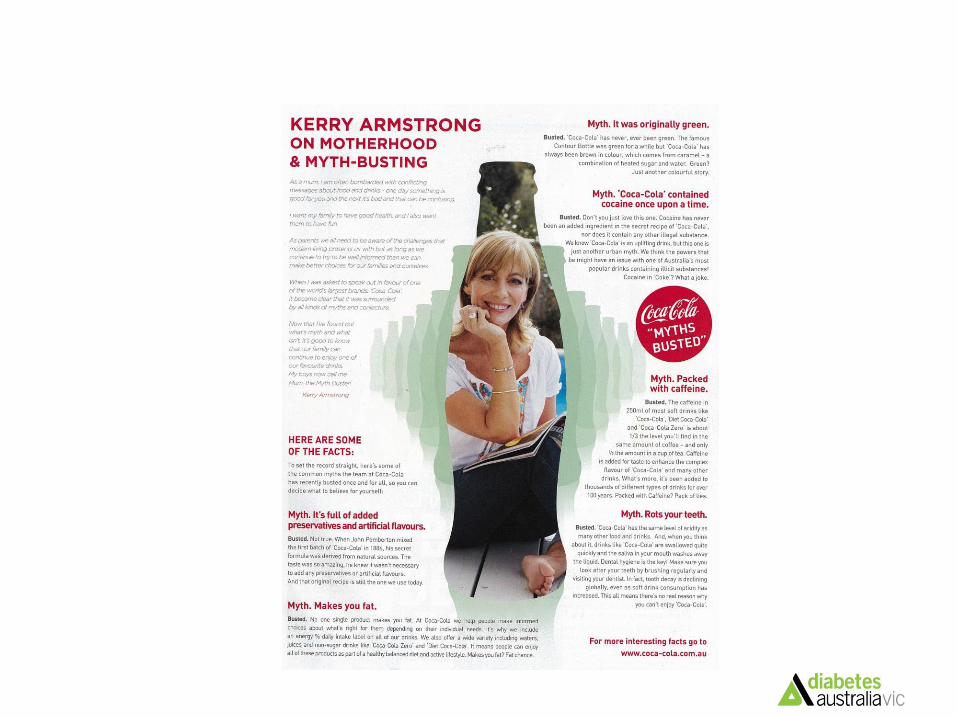
Coke and Kerry Armstrong

Coke Campaign
Coke campaign
Complaint re Misleading and
Deceptive Conduct
The campaign creates the overall impression that ‘Coca-Cola’ is not an unhealthy product. We consider these claims and this impression to be false and misleading. In fact, evidence shows that consumption of sugary soft drinks such as ‘Coca-Cola’ is associated with increased energy intake, weight gain, and risk of medical problems. Evidence also shows that consumption of black cola drinks like ‘Coca-Cola’ contributes to the development of dental caries.
Therefore, in our view, Coca-Cola’s conduct:
· is misleading and deceptive in breach of section 52 of the Trade Practices Act; and
· constitutes the making of false and misleading representations in breach of section 75AZC(1)(a) and (e) of the Act.
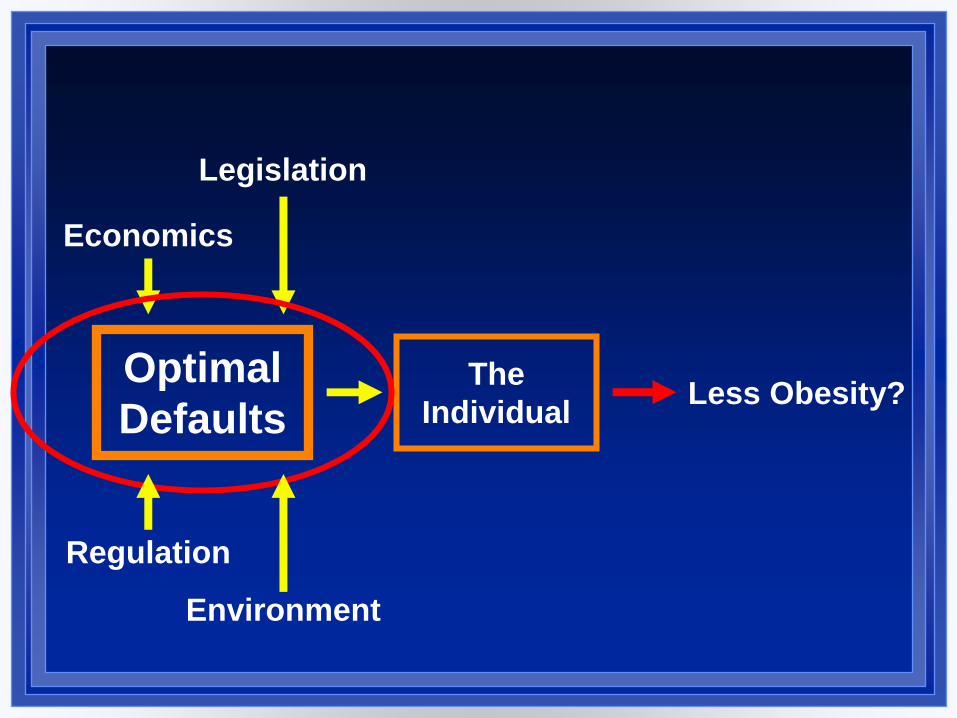
Optimal
Defaults
Economics
Legislation
Environment
Regulation
The
Individual Less Obesity?
Prevention – High Risk
Prevention for those at high risk (pre-diabetes) through
innovative national programs (and international links).
•2 million Australians with pre-diabetes
•Strong evidence base
•Life! Program in Victoria
•Loss of federal funding ($200m+over 4 years)
Prevention of Complications
Prevention of the serious complications and
hospitalisations related to diabetes (blindness, kidney
disease, heart attacks, strokes, amputations).
•32% of preventable hospital admissions
•Coordination of care ($449m program scrapped)
•Improved self management
•Quality of life and wellbeing

Creating national standards for structured education programs
• evidence-based, with specific aims and
objectives
• a structured, theory-driven curriculum with
effective supporting materials
• delivered by educators trained in education
theory
• quality assured, reviewed by independent
assessors and with outcomes regularly
audited

CASE STUDY: DAFNE
What is DAFNE?
• structured self-management education program for T1DM
– skills training to replace insulin by matching it to CHO on a meal-by-meal basis: “the end of the diabetic diet”
– adult education principles to facilitate new learning
– emphasis on building confidence & appropriate independence
– 5-day outpatient group program (6-8 people) in secondary care
• Delivered by 2+ trained educators (DSNs & dietitians)
dose adjustment for normal eating
CASE STUDY: DESMOND
What is DESMOND?
• structured self-management education program for people newly diagnosed with T2DM
• Underpinned by strong philosophy of care and psychological / educational theory
• Delivered as 1 day or 2 ½ days
• Delivered by 2 trained educators
• Delivered in Primary Care
Cost Effectiveness of Delivering
the DESMOND Intervention
(Diabetes Education and Self-
Management for Ongoing and
Newly Diagnosed) for People
Newly Diagnosed with Type 2
diabetes
BMJ on line 2010
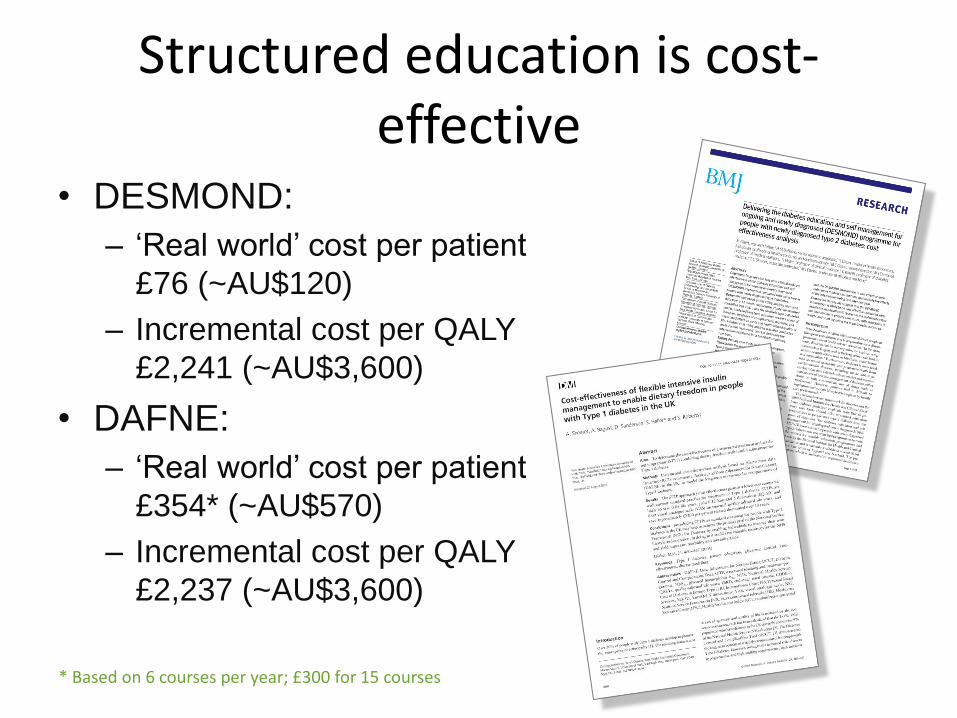
Structured education is cost-effective
• DESMOND:
– ‘Real world’ cost per patient
£76 (~AU$120)
– Incremental cost per QALY
£2,241 (~AU$3,600)
• DAFNE:
– ‘Real world’ cost per patient
£354* (~AU$570)
– Incremental cost per QALY
£2,237 (~AU$3,600)
* Based on 6 courses per year; £300 for 15 courses
National Diabetes Services
Scheme (NDSS)
National Self Management Support
• ATSI
• CALD
• Youth and Transition
• Diabetes in Pregnancy
• Mental Health and diabetes
• Older people and diabetes
• e-Health

Consumer Engagement in
Self Management and
Prevention of Diabetes