controlled trial of physical trainingin failure · coats et al physical trainingin heartfailure...
TRANSCRIPT
2119
Controlled Trial of Physical Training inChronic Heart Failure
Exercise Performance, Hemodynamics, Ventilation, andAutonomic Function
Andrew J.S. Coats, FRACP; Stamatis Adamopoulos, MD; Alberto Radaelli, MD;Alistair McCance, DM; Theo E. Meyer, FCP(SA); Luciano Bernardi, MD; Pier L. Solda, MD;
Patrick Davey, MRCP; Oliver Ormerod, MD; Colin Forfar, FRCP;James Conway, FRCP; and Peter Sleight, FRCP
Background. Many secondary abnormalities in chronic heart failure (CHF) may reflect physicaldeconditioning. There has been no prospective, controlled study of the effects of physical training on
hemodynamics and autonomic function in CHIF.Methods and Results. In a controlled crossover trial of 8 weeks of exercise training, 17 men with stable
moderate to severe CHF (age, 61.8±+1.5 years; left ventricular ejection fraction, 19.6±2.3%), increasedexercise tolerance (13.9±+1.0 to 16.5±+1.0 minutes, p<0.001), and peak oxygen uptake (13.2+0.9 to15.6± 1.0 mI/kg/min, p<0.01) significantly compared with controls. Training increased cardiac output atsubmaximal (5.9-6.7 1/min, p<0.05) and peak exercise (6.3-7.1 /min, p<0.05), with a significantreduction in systemic vascular resistance. Training reduced minute ventilation and the slope relatingminute ventilation to carbon dioxide production (-10.5%, p<0.05). Sympathovagal balance was alteredby physical training when assessed by three methods: 1) RR variability (+19.2%,p<0.05); 2) autoregres-sive power spectral analysis of the resting ECG divided into low-frequency (-21.2%, p<0.01) andhigh-frequency (+51.3%, p<0.05) components; and 3) whole-body radiolabeled norepinephrine spillover(-16%, p<0.05). These measurements all showed a significant shift away from sympathetic towardenhanced vagal activity after training.
Conclusions. Carefully selected patients with moderate to severe CHF can achieve significant,worthwhile improvements with exercise training. Physical deconditioning may be partly responsible forsome of the associated abnormalities and exercise limitation of CHF, including abnormalities inautonomic balance. (Circulation 1992;85:2119-2131)KEY WoRDs * heart failure * exercise training
heart rate * norepinephrine
P hysical training increases exercise tolerance innormal subjects and in patients with ischemicheart disease.1 Training has been shown to
improve exercise hemodynamics, blood lipid profiles,susceptibility to ventricular arrhythmias, and psycholog-ical status,2-4 all of which would be of considerablebenefit in chronic heart failure (CHF) if such patients
From the Department of Cardiac Medicine (A.J.S.C., S.A.),National Heart and Lung Institute, London; the Department ofCardiovascular Medicine (A.J.S.C., S.A., A.R., A.M., T.E.M.,P.D., 0.0., C.F., J.C., P.S.), John Radcliffe Hospital, Oxford,England; and the Department of Internal Medicine (A.R., L.B.,P.L.S.), First Medical Clinic, University of Pavia, Pavia, Italy.
Supported by the British Heart Foundation, a Squibb Cardio-vascular Fellowship, and an ICI Research Fellowship at PembrokeCollege, Oxford.
Presented in the final of the Melvin Marcus Young InvestigatorAward Competition of the American Heart Association Meeting,Dallas, Tex., November 1990.Address for correspondence: Dr. Andrew J.S. Coats, Depart-
ment of Cardiac Medicine, National Heart and Lung Institute,Dovehouse Street, London, SW3 6LY UK.
Received September 27, 1990; revision accepted March 4, 1992.
* hemodynamics * power spectral analysis v
could safely perform enough exercise to train. Patientswith moderate to severe heart failure in whom exerciseintolerance interferes most with daily life would havemost to gain from increased fitness,5,6 yet these patientshave often been routinely excluded from exerciseprograms.7,8We designed a controlled crossover trial comparing
home-based exercise training with activity restriction tolook at the effects of exercise training in stable CHF. Inaddition to conventional hemodynamic, exercise, venti-latory, and symptom measures, we used three methodsof assessing sympathovagal balance (heart rate variabil-ity, power spectral analysis of the ECG, and norepi-nephrine [NE] spillover) to critically assess whethershort-term physical training could modify the abnormal-ities of autonomic control seen in moderate to severeCHF. The present trial was designed to answer thefollowing questions. 1) Can patients with moderate tosevere CHF achieve a training effect with regular exer-cise? 2) Compared with a control period of normalactivity, does training improve exercise duration andmaximal oxygen consumption? 3) Are there associated
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

2120 Circulation Vol 85, No 6 June 1992
improvements in other known abnormalities of CHFincluding autonomic imbalance? The training protocoland exercise performance results of the first 11 patientshave been published in an interim report,9 but otherthan this preliminary report, this is the first controlled,prospective study of physical training in CHF.
MethodsStudy DesignThe study, which was approved by the Central Oxford
Research Ethics Committee, was a randomized cross-over comparison of 8 weeks of exercise training against8 weeks of restricted activity (rest). Two to threebaseline laboratory visits were used to familiarize thepatients to the exercise tests and other laboratory
See p 2323
procedures. The physician conducting the tests wasunaware of the training status of the patients. Habitu-ation to test procedures was avoided by the patients notattending the hospital during the 8 weeks of eitherphase of the study.
Study PopulationAll subjects gave informed consent for this trial.
Inclusion criteria were stable New York Heart Associ-ation class 11-III heart failure of at least 3 months'duration; ischemic etiology (as evidenced by docu-mented myocardial infarction and/or coronary arteriog-raphy and coronary bypass surgery); stable sinusrhythm; limitation of exercise by symptoms of dyspneaor fatigue only and ability to reach a respiratory ex-change ratio of at least unity; absence of Holter moni-toring evidence of sustained ventricular tachycardia orother serious arrhythmias; and absence of symptomaticangina or ECG evidence of ischemia limiting exercise.Radionuclide ventriculography was performed at base-line, but the results did not constitute part of the entrycriteria. This test was not repeated during the study anddid not constitute one of the tests of efficacy. This wasdecided because the trial was a crossover design requir-ing at least three assessment points, and it was not feltjustified to ask the subjects to undergo three scans forthis trial; therefore, no information is available on theeffects of physical training on ejection fraction.
Training ProgramThe patients were instructed on the use of a training
bicycle (Tunturi Professional Ergometer, Tunturi, Fin-land) that they kept for their use at home for 8 weeks.They were instructed to exercise at 50 rpm for 20minutes 5 days per week and to keep the resistancesetting of the bicycle so that their continuously moni-tored heart rate (Micro Sports Lab Computer, Triadco-lour, London) was kept in the range of 60-80% of theirpreviously determined maximum heart rate. Compli-ance was assessed as the percentage of expected bicyclewheel revolutions achieved over the training period.
Control Rest PhaseThe patients were asked to avoid exercise above their
normal prestudy routine and specifically to avoid exer-cise that would lead to feelings of dyspnea or exhaus-tion. No formal compliance assessment was made. The
patients did not have the exercise bicycle in their housesduring this phase of the trial.
Exercise TestingAt each visit, after overnight fasting and before
administration of medication, the patients performedan incremental (4-minute, 25-W stages) upright bicycleexercise test to exhaustion, with 1-minute average mea-surements of respiratory gas exchange. Inspiratory flow(Harvard Instruments Dry Gas Meter) and expiratoryoxygen and carbon dioxide concentrations (Servomex570A and PA404 meters, Servomex, Crowborough, Sus-sex, England) were measured, and oxygen consumptionand carbon dioxide production were calculated by stan-dard formulas. The gas meters were calibrated againstgases of known concentrations before each test.
Hemodynamic MeasurementsOn the same day after 1 hour's rest, a second exercise
test was performed (supine posture) during which he-modynamic measurements were made. Measurementswere made at rest and at the end of each 4-minute,25-W incremental stage of the supine bicycle exercisetest (Elema-Schonander, AM 368, Stockholm). Pulsed-wave Doppler ultrasonic measurements of ascendingaortic blood velocity from the suprasternal approachwere made using a Pedof Doppler ultrasound generator(Vingmed, Norway) and our own laboratory-made,computer-based, fast Fourier transform spectral analyz-er.10 We used the intensity-weighted mean frequency ineach 5-msec time bin (the integral of velocity and timefor the ejection period) to calculate stroke distance. Weused standard formulas and an echocardiographic mea-surement of aortic cross-sectional area (leading edge toleading edge, immediately distal to the sinus of Val-salva) to calculate stroke volume. Measurements ofvolume flow by this method in our laboratory have beenvalidated in a flow rig and in humans against thermodi-lution and electromagnetic catheter measurements andfound to be accurate (standard deviation of differencesbetween methods in estimate of stroke volume, 8.7%).11The accuracy of the Doppler cardiac output may be lessduring exercise because of the effects of body motionand increased respiratory excursion, but this is probablyalso a feature of other methods of measuring cardiacoutput. Dr. Coats12 reviewed the available validationstudies of Doppler-derived cardiac output during exer-cise and concluded that the standard deviations ofdifferences between Doppler-derived measurement andother techniques averaged 22%, significantly worse thanat rest but still an acceptable level of accuracy formeasurement during this difficult state. Blood pressurewas measured by a previously validated automaticsphygmomanometer (Copal UA 251, Takeda Medical,Tokyo).13 Peripheral vascular resistance was calculatedby the approximation of mean blood pressure divided bycardiac output.
ECG RecordingsDuring exercise. Heart rate was recorded at the end of
each stage of a bicycle exercise test and was derivedfrom the average of 20 beats. A three-lead ECG wasrecorded throughout exercise.
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

Coats et al Physical Training in Heart Failure 2121
Twenty-four-hour Holter monitoring. Twenty-four-hour ECG monitoring was performed using a two-channel (modified V, and V5 leads) recorder (OxfordMedilog II, Oxford Medical Instruments). Qualitativeand quantitative ECG analysis was performed using acomputerized nontriggered template system consistingof a Z8OA preprocessor and DEC-LSI master, whichwas developed and validated in our laboratory.14 Anal-ysis of the recordings was performed blind to thecurrent training status.
Tapes were analyzed to obtain the mean and stan-dard deviation of all RR intervals that had normalmorphology and cycle lengths within 80% and 120% ofthe preceding cycle duration. Results are presentedseparately for the whole 24 hours and separately fordaytime (14-20 hours) and nighttime (0-6 hours).These 6-hour periods were chosen as being unaffectedby the trip to the hospital and most likely to representdaytime and sleeping states. They are not, however, fullsummaries of waking and sleeping heart rate behavior.
Resting ECG recording in the laboratory. During su-pine rest in a quiet, darkened room, 640 consecutiveheartbeats were recorded on a Store 4 Racal-Thermi-onic FM tape recorder (Southampton, UK) at a tapespeed of 15/16 in./sec. Lead V5 was used for thisrecording. These recordings were used to performpower spectral analysis of variations in RR interval. Nospecial attempts were made to control or alter thepatient's respiratory pattern during this recording, butspecial care was taken that the patient was relaxed,stable, and undisturbed.
Power Spectral Analysis ofRR Interval VariabilityThe tape-recorded resting ECG signal from the lab-
oratory recording period was digitized off-line by a12-bit analog-to-digital converter (NB-MIO-16 board,National Instruments, Austin, Tex.) at a sampling rateof 500 samples per second. The converter was con-nected to a Macintosh IIcx computer (Apple Inc.,Cupertino, Calif.) equipped with a 5-Mb random accessmemory and a 60-Mb hard disk. A "C" languageprogram identified all the QRS complexes in eachsequence and located the peak of each R wave. Fromthese data, the RR intervals were obtained. For eachsequence, 256 heartbeats were analyzed. Trends wereremoved from each sequence by subtraction of thatsame sequence after a 124-lag window smoothing pro-cedure, following a previously described algorithm.15Premature beats were interactively identified and cor-rected by linear interpolation with the previous andfollowing beats.Power spectral analysis of the RR interval signal was
by an autoregressive model.16 Model coefficients wereevaluated according to a modification of the Burgalgorithm.'718 Model order was assessed by Akaikecriteria.1819 In most cases, a model order between 9 and13 was found to be adequate. Spectral components wereobtained by a previously described decomposition meth-od.16,19,20 This method was used to measure the areabelow each spectral peak.21 We expressed the variationin Hertz rather than in cycles per beat, assuming thatthe RR interval changes were small with respect to themean RR interval and considering the sampling timeequal to the mean RR interval. The power spectrum
shows two separate peaks: a higher-frequency peakrelated to respiration and a low-frequency peak unre-lated to any respiratory event.162'22 Occasionally, thelow-frequency peak is further subdivided into a low- anda very-low-frequency peak, but this was not done in thisstudy because the very-low-frequency peak can be dif-ficult to differentiate from low-frequency noise unlessthe recording period is very prolonged.Power spectral analysis is a relatively new technique,
and some explanation of its capabilities and limitationsmay be helpful. Spectral analysis is a mathematicaltechnique in which variations in heart rate are analyzedin the frequency domain. In other words, this analysiscan tell us how much of the variability of RR intervalsoccurs in a regular rhythmic fashion and how much of itoccurs at different frequencies. From experiments onparasympathetic and ,-blockade in dogs22 and hu-mans,21 it appears that the high-frequency rhythm isentrained by the respiratory frequency and, apart froma small residual (probably mechanical) respiratory com-ponent seen after cardiac transplantation,23 is carriedalmost entirely by vagal activity. The low-frequencyrhythm is mediated jointly by the vagus and the sympa-thetics but predominantly by the latter.16,2l,22We evaluated the power of the harmonic components
in the region between 0.03 and 0.14 Hz (low-frequencycomponent, LF) and those in the range between 0.18and 0.40 Hz (high-frequency component, HF).To simplify comparison between spectra, we consid-
ered the relative percentage of each spectral componentcompared with the total oscillatory power and ex-pressed it as normalized units (nu). In addition, weevaluated the absolute value of the HF area as anexpression of respiratory sinus arrhythmia (RSA).The relative amount of HF and the absolute amount
of RSA have been considered as indexes of parasympa-thetic activity, whereas the relative amount of LF hasbeen considered as an index of sympathetic activity.18'2'It must be stressed, however, that power spectral mea-surements are not strictly quantitative, because it isimpossible to assess absolute measurements of oscilla-tory power in different frequency ranges without takinginto account differences in heart rate variability. It hasnot been shown that power within a certain frequencyband can be used to quantify differences in sympatheticor parasympathetic tone between individuals. Mostly,the ratio between high- and low-frequency power isused, and this ratio does not lend itself to simplequantitative analysis. No gold standard measure ofautonomic balance exists. The power spectral techniquegives qualitative and semiquantitative information,which, when combined with other autonomic measures,can help describe autonomic nervous control of theintact circulation.
NE KineticsNE kinetics were measured according to the tech-
niques of Esler et a124 in seven subjects. 1-[2,5,6-3H]norepinephrine (New England Nuclear) was givenintravenously as a bolus (12 ,Ci, 0.44 MBq) followed byconstant infusion (0.7 ,Ci, 0.026 MBq min-1m-2) for upto 60 minutes. Blood samples were collected at rest andat submaximal (50-W) supine bicycle exercise in bothtraining and detraining phases of the study. Plasma NE
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

2122 Circulation Vol 85, No 6 June 1992
was measured by using high-performance liquid chro-matography. The normal range in our laboratory is120-300 pg/ml. Plasma [3H]NE was measured by liquidscintillation counting of alumina extracts with correc-tion for recovery of a nonradioactive internal standard(dihydroxybenzylamine). NE plasma clearance andwhole-body NE spillover were measured according tothe following relations, which hold under steady-stateconditions.
Infusion rate (dpm/min)Whole-body NE clearance=
Plasma [3H]NE (dpm/ml)
Infusion rate (dpmlmin)Whole-body NE spillover=-Ifsoat dmmn
Specific activity of [NE] (dpm/pg)
Symptom AssessmentPatients' completed scores from a modified Likert
symptom questionnaire were used to assess severity ofsymptoms relevant to CHF at the end of each phase ofthe trial. Questions were asked on breathlessness, fa-tigue, chest pain, daily activity, and ease of daily activ-ities, and the patients were asked to grade each on ascale of 1-7. Three questions were ordered with im-provement being indicated by a higher score and two bya lower score to lessen bias, but for simplicity ofpresentation in the "Results" section, the scores werecorrected so that for all questions, an improvement insymptoms is indicated by a higher score.
Statistical AnalysisThe trial was analyzed according to the recommen-
dations of Hills and Armitage25 for crossover trials andanalyzed for the presence of period or carry-over ef-fects, none of which were found. Analysis of variancefollowed by Student's t test was used for normallydistributed parameters, and Wilcoxon signed rank testwas used for nonnormally distributed parameters. Sig-nificance at the 5% level or lower is reported andcorrected where appropriate for multiple comparisontesting by the Scheffe procedure. Data are presented asmean+SEM.
ResultsPatients
Nineteen patients entered the trial, and two failed tocomplete the program. Both dropouts occurred in thefirst phase, which in both was the rest phase; in one,death followed progressive worsening of cardiac failureand the second underwent cardiac transplantation afteran admission with severe cardiac failure. The remaining17 patients completed the trial without adverse eventsand with no change in drug therapy. Patient character-istics are shown in Table 1 subdivided by the random-ization order of treatments. Individual patient details ofdrug therapy are given in Table 2.
Patients were aged 61.8+1.5 years (range, 47-74years). All had documented myocardial infarction (an-terior alone in 12, anterior and inferior in two, inferioralone in two, and inferolateral in one); six had under-gone coronary artery bypass grafting, and none hadlimiting angina pectoris. All subjects were taking diuret-ics (average furosemide dose, 77.6±10.0 mg), and 15 of
TABLE 1. Patient Characteristics at Baseline
Training first Rest first(n=8) (n=9)
Age (years) 65.1±+ 1.8 61.1+2.5LVEF 0.19+0.04 0.21±0.03NYHA class 11/III 5/3 5/4Peak Vo2 (ml/min/kg) 12.5±1.0 13.8±1.4Exercise time (minutes) 13.7±1.1 14.0±1.5Height (cm) 176.5±1.6 171.7±2.3Weight (kg) 85.2±3.9 79.7±4.8
Results are expressed as mean±SEM. LVEF, radionuclide leftventricular ejection fraction; NYHA, New York Heart Association.
17 were on ACE inhibitors. Mean radionuclide leftventriculographic ejection fraction was 19.6±2.3%.There was random allocation to rest or training first,and no significant differences were found in any of thebaseline variables between those allocated to exercisefirst and those to rest first.
General Training ResultsOverall compliance to the training program was good,
with a mean (range) compliance of 77.3% (26-116%).In one patient, the revolution counter broke during thetraining phase, so compliance data were available inonly 16 subjects. There were no adverse training-relatedside effects reported by the subjects other than mildfatigue after exercise. Pharmacological treatment re-mained stable for 3 months before the study and for theduration of the study in all 17 completed subjects. Therewas no consistent weight change produced by training.
Exercise Testing and Ventilatory FunctionCompared with the rest phase, training significantly
increased upright bicycle exercise time (13.9±1.0 to16.5± 1.0 minutes,p<0.001) and increased peak oxygenuptake (13.2±0.9 to 15.6± 1.0 ml/min/kg, p<0.01). In-dividual patient data on the change in exercise time areshown in Figure 1. There was no significant differencebetween the baseline and rest periods. Upright bicycleexercise was performed after training with lower heartrates at comparable work loads. After training, therewere significant reductions in submaximal heart rate at
25 -
S
.E
E0
>% cZ
o
Kw
20 -
15 -
10 -
5.-Baseline Training Rest
FIGURE 1. Graph of individual and mean±SEM patientupright exercise durations for baseline, training, and detrain-ing periods. Order has been sorted. * **p<0 001 for compar-ison between training and detraining periods, n=17.
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

Coats et al Physical Training in Heart Failure 2123
TABLE 2. Individual Patient Data
Patient Age (years) Diuretics ACE inhibitor (duration) Other agents
1 47 F 80, A 10 C 100 (10 months) Aspirin2 63 F 40, A S C 75 (12 months) Aspirin3 63 F 40, A 5 Aspirin, amiodarone4 66 B 2 E 10 (5 months) Aspirin, slow K5 65 F 40 C 75 (2 years) Fenbufen6 59 F 120, A 15 L 10 (18 months) Aspirin7 64 F 40 C 75 (12 months)8 62 B 1 C 75 (16 months) Aspirin, digoxin, ISDN9 53 B 4, A 10 E 10 (18 months) Warfarin, ranitidine10 68 B 2 C 75 (7 months) Warfarin, slow K11 58 B 2, A 20 Warfarin, digoxin12 73 F 40, A 5 C 37.5 (20 months) Diltiazem, dipyridamole13 74 F 240 C 37.5 (12 months) Warfarin14 60 F 160, S 100 C 37.5 (8 months)15 64 F 80, A 10 E 10 (9 months)16 67 F 160, A 10, S 50 C 50 (6 months)17 59 F 40 L 10 (7 months) Aspirin, amiodarone
F, furosemide; A, amiloride; S, spirinolactone; B, bumetanide; C, captopril; E, enalapril; L, lisinopril; ISDN,isosorbide dinitrate. All figures after drugs refer to daily dose in milligrams. All drugs were stable for 3 months beforeentering the trial and for the duration of the trial. For the ACE inhibitors, the duration of stable therapy before trialentry is given in parentheses.
25-W and 50-W exercise with no change in peak heartrate (see Figure 2). Resting heart rate was reducednonsignificantly from 84.6±3.5 to 81.0+4.2 (p=0.09),25-W heart rate from 101.0+3.9 to 92±4.1 (p<0.05),50-W heart rate from 111.1+4.1 to 103.2+4.6 (p<0.05),and peak heart rate unchanged (135.9±4.7 to133.4+6. 1, p=NS). The submaximal work load (50 W)rate-pressure product (- 11.8%, p<0.01) was also sig-nificantly reduced by training, indicating a more effi-cient exercise performance with respect to myocardialoxygen requirement.
Submaximal exercise performance was also improvedby training. Taking the point during exercise at whichthe respiratory exchange ratio equaled unity as an
approximate marker of when anaerobic muscular me-
tabolism is starting, this was achieved later in theexercise protocol after training (+ 1.8 minutes, p<0.01)and occurred at a higher oxygen uptake (13.7+±0.7compared with 11.9+0.8 ml/kg/min, p<0.001).To study the control of ventilation during exercise, we
looked at the relation between minute ventilation andthe rate of carbon dioxide production (V/Vco2 slope),which has been shown to parallel the severity of CHF.26The V/Vco2 slope was significantly reduced by physicaltraining (0.038+0.004 to 0.034±0.003, p<0.05). An ex-
ample in a single subject is shown in Figure 3. Overall,there was no significant change in the intercept of thisslope nor in peak ventilation achieved, but minute ven-tilation was significantly reduced at submaximal workloads by training. The relation between ventilation andwork load in Figure 4 shows a significant reduction in
0 25 50 75Load (Watts)
c
E
=1c
.e.0
0
100 125 c
m
FIGURE 2. Graph shows mean-+SEM values for heart rate(bpm, beats per minute) response at rest and different levels ofupright bicycle exercise for training (closed circles) and rest(open circles) periods. *p<0.05 for comparison of trainingversus rest; +++p<0.001 for comparison of peak loadachieved, n=17.
60 -
50 -
40 -
30 -
20 -
10 -
0 200 400 600 800 1000
V C02 (mil/min)
FIGURE 3. Graph of individual subject result showing rela-tion between minute ventilation and carbon dioxide produc-tion during exercise in rest (open circles) and training (closedcircles) phases.
130-
110-
90-
E
0
a-m
70 a1
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

2124 Circulation Vol 85, No 6 June 1992
c
E
0
a
a Res
E Training
Rest 25 W 50W Peak
Exercise Load
FIGURE 4. Bar graph shows relation between minute venti-lation and work load. Mean±SEM for training and restperiods. *p<0.05 for comparison of training versus rest,n=17.
submaximal minute ventilation at 25-W and 50-W exer-cise with no difference in resting or peak ventilation.
Hemodynamic Assessment During Supine ExerciseHemodynamic measurements were obtained at the
end of each 4-minute stage of a supine bicycle ergom-eter test as described in "Methods." In one of the 17subjects, the Doppler recordings during the trainingphase were corrupted by electrical interference andwere not usable. The exercise duration was increased bytraining from 10.7±0.7 to 12.3±0.7 minutes (p<0.001).The hemodynamic responses are shown in Figure 5.There was a significant systemic vasodilatation pro-duced by training at rest, submaximal (25-W), and peakexercise. This was associated with an increase in cardiacoutput at submaximal (25-W) and peak exercise, withno significant change in mean blood pressure. Theincreased cardiac output was largely due to increasedstroke volume at submaximal exercise with no change inheart rate, whereas at peak exercise there was also anincrease in peak heart rate.
ECG RecordingsTwenty-four-hour Holter monitoring. Training pro-
duced significant reductions in 24-hour mean heart rate
c
EC
0
C)
7
5.
4-
25
Load
50
(Watts)75 100
FIGURE 5. Graph ofmean +SEM values for cardiac outputduring exercise after training (closed circles) and rest (opencircles) periods. *p<0.05 for comparison of training versus
rest, n=16.
TABLE 3. Twenty-four-Hour Ambulatory ECG Recording
Training Rest p24-Hour HR (bpm) 77.0+2.8 79.1±3.0 <0.001Daytime* HR (bpm) 82.1±3.1 85.6±3.2 <0.05Night* HR (bpm) 70.1±2.2 72.3±3.1 <0.05VE rate (hr-1) 60.7±24.5 29.4±8.6 <0.05SD daytime (msec) 101.0±11.0 90.5±7.5 <0.05SD night (msec) 96.4±9.3 82.4±7.5 <0.05SD 24 hours (msec) 125.6±9.0 109.3±8.3 NS
24-Hour HR, mean heart rate on 24-hour Holter monitoring;bpm, beats per minute; Daytime HR, mean daytime heart rate;Night HR, nighttime mean heart rate from Holter monitor; VErate, hourly rate of ventricular ectopic beats from Holter monitor;SD, standard deviation of normal morphology RR intervals.Probability values refer to Student's t test comparison betweenrest and training phases. NS, not statistically significant.
*Daytime refers to 2 PM to 8 PM only and night refers to midnightto 6 AM only, so explaining how the reduction in heart rate over 24hours can be less than for either "day" or "night" separately.
(79.1+3.0 to 77.0+ 2.7 beats per minute,p<0.05) as wellas separately for both daytime and nighttime heart rateaverages (see Table 3). No serious or complex ventric-ular arrhythmias were detected on any of the record-ings, but there was a significant excess of ventricularectopic beats during the training phase (rest phase,29.4+8.6; training, 60.7+24.5 hour-l, p<0.05), whichmay have been related to the slower heart rate unmask-ing ventricular automaticity. There was no significantchange in the rate of early premature ventricular beats.
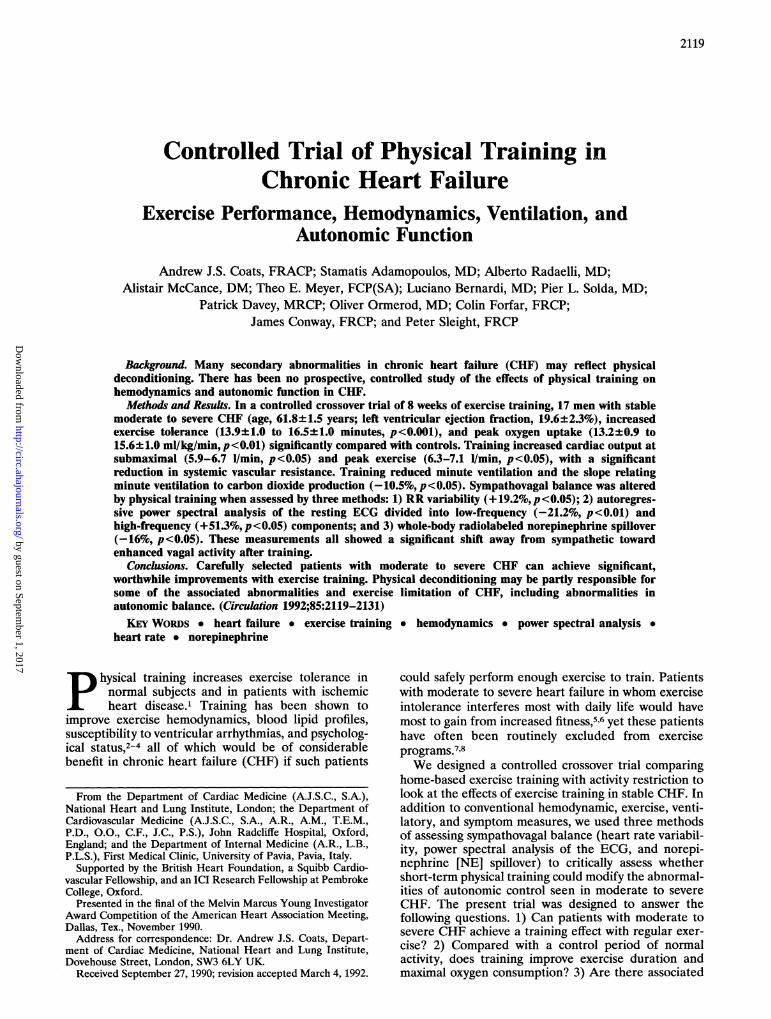
Twenty-four-hour heart rate variability, indicated bythe standard deviation of normal morphology RR inter-vals, was significantly higher after training (125.6+9.0versus 109.3+8.3 msec; n = 14, p<0.05). As shown forindividual subjects in Figure 6 (left panel), nocturnalheart rate variability was also higher after training(96.4+9.3 versus 82.4+7.5, p<0.05), but the daytimeheart rate variability was not significantly different(101.0+11.0 versus 90.5+7.5 NS) possibly because ofthe effects of different levels of physical activity betweenthe two phases of the trial.
Resting ECG recording in the laboratory. During su-pine rest in a quiet, darkened room, 640 consecutiveheartbeats were recorded as described in "Methods."Only normal morphology complexes with RR intervalsbetween 80% and 120% of the preceding RR intervalwere included in the calculation of heart rate variability
TABix 4. Effects of Physical Training on Autonomic Balance asDescribed by Power Spectral Analysis of RR Interval Variabilityand Norepinephrine Spillover at Rest and During Exercise
Training Rest pLF% (nu) 49.7±6.9 63.1±5.1 <0.01HF% (nu) 40.4±6.9 26.7±4.8 <0.05HF-sa (msec2) 343.9±201.3 192.7±146.0 <0.05NE rest (ng/min/m2) 320.8±49.0 381.3±51.2 <0.05NE 50 W (ng/min/m2) 592±152 648±102 NS
LF and HF, low-frequency and high-frequency components ofthe power spectral analysis of RR interval variability; nu, normal-ized units (percentage of the total oscillatory power); HF-sa,absolute measure of high-frequency respiratory sinus arrhythmia;NE, norepinephrine spillover at rest and during 50-W submaximalsupine bicycle exercise.
a ~
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from
Coats et al Physical Training in Heart Failure 2125
SaS.0
CqrCD
120 -
100-
c 80
2 E-i 0
c 40-
& 20-0
a 0CD Rest Training
FIGURE 6. Graphs show effects ofphysical training on nocturnal (0-6 AM) heart rate variability (left panel, n=14) and heartrate variability of 640 consecutive beats (right panel; laboratory recordings, n=15). For method of calculation, see text. *p<0.05for comparison rest versus training. SD, standard deviation.
to exclude an effect of increased ectopics on the mea-sure of heart rate variability. Resting heart rate vari-ability (standard deviation of all 640 consecutive beats)was significantly higher after training (40.9+6.1 versus
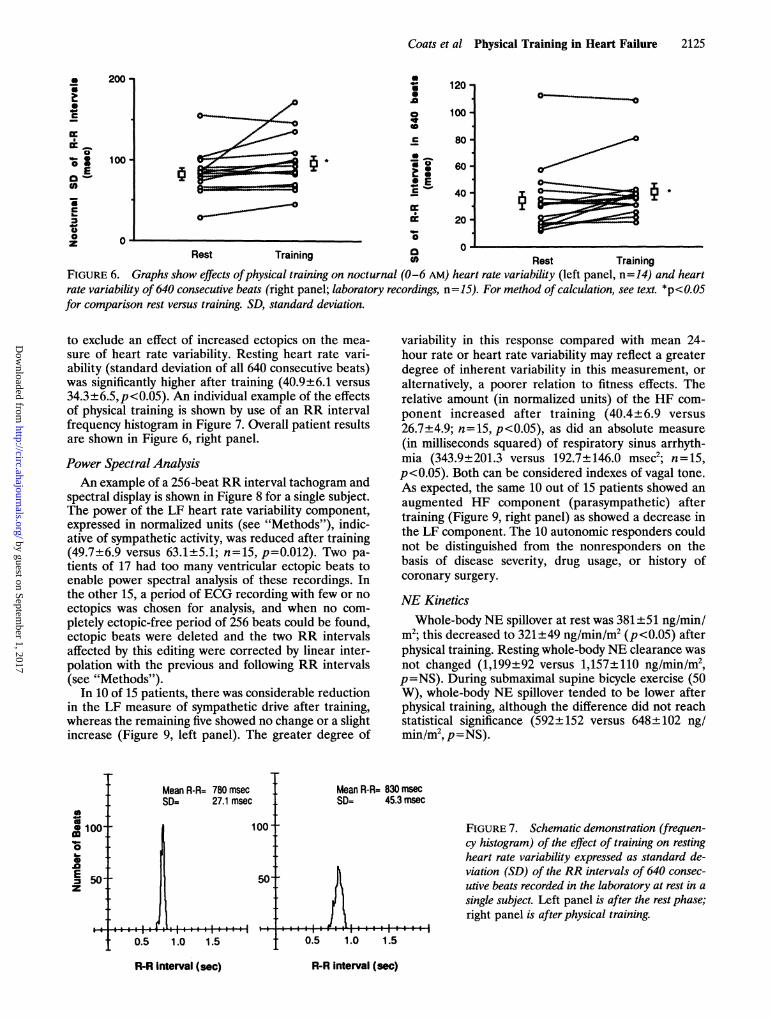
34.3±6.5,p<0.05). An individual example of the effectsof physical training is shown by use of an RR intervalfrequency histogram in Figure 7. Overall patient resultsare shown in Figure 6, right panel.
Power Spectral AnalysisAn example of a 256-beat RR interval tachogram and
spectral display is shown in Figure 8 for a single subject.The power of the LF heart rate variability component,expressed in normalized units (see "Methods"), indic-ative of sympathetic activity, was reduced after training(49.7±6.9 versus 63.1±5.1; n=15, p=0.012). Two pa-tients of 17 had too many ventricular ectopic beats toenable power spectral analysis of these recordings. Inthe other 15, a period of ECG recording with few or noectopics was chosen for analysis, and when no com-pletely ectopic-free period of 256 beats could be found,ectopic beats were deleted and the two RR intervalsaffected by this editing were corrected by linear inter-polation with the previous and following RR intervals(see "Methods").
In 10 of 15 patients, there was considerable reductionin the LF measure of sympathetic drive after training,whereas the remaining five showed no change or a slightincrease (Figure 9, left panel). The greater degree of
Mean R-R= 780 msec Mean R-RSD= 27.1 msec SD=
0m 100- 100-
o . .E50 50
0.5 1.0 1.5
1= 83045.:
variability in this response compared with mean 24-hour rate or heart rate variability may reflect a greaterdegree of inherent variability in this measurement, or
alternatively, a poorer relation to fitness effects. Therelative amount (in normalized units) of the HF com-
ponent increased after training (40.4±6.9 versus
26.7+4.9; n=15, p<0.05), as did an absolute measure
(in milliseconds squared) of respiratory sinus arrhyth-mia (343.9±201.3 versus 192.7±146.0 msec2; n=15,p<0.05). Both can be considered indexes of vagal tone.As expected, the same 10 out of 15 patients showed an
augmented HF component (parasympathetic) aftertraining (Figure 9, right panel) as showed a decrease inthe LF component. The 10 autonomic responders couldnot be distinguished from the nonresponders on thebasis of disease severity, drug usage, or history ofcoronary surgery.
NE KineticsWhole-body NE spillover at rest was 381±51 ng/min/
mi2; this decreased to 321±49 ng/min/im2 (p<0.05) afterphysical training. Resting whole-body NE clearance wasnot changed (1,199±92 versus 1,157+110 ng/min/m2,p=NS). During submaximal supine bicycle exercise (50W), whole-body NE spillover tended to be lower afterphysical training, although the difference did not reachstatistical significance (592±152 versus 648±102 ng/min/im2, p=NS).
msec3 msec
FIGURE 7. Schematic demonstration (frequen-cy histogram) of the effect of training on restingheart rate variability expressed as standard de-viation (SD) of the RR intervals of 640 consec-
utive beats recorded in the laboratory at rest in a
single subject. Left panel is after the rest phase;right panel is after physical training.
0.5 1.0 1.5
R-R Interval (sec)
200 -
100-
S6
SC
_*0
0
-
ECh%
n a
RAnt Tr..ininn
%P
R-R interval (sec)
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

2126 Circulation Vol 85, No 6 June 1992
De-training
100 -
(4E
RR INTERVALS 256
0
0 RR INTERVALS
HF
lit:
Hz
600
N
0Q)E
0.5 0 HzFIGURE 8. Tracings show effect ofphysical training on the RR interval tachogram (display of individual RR intervals) for 256consecutive beats (upper panels) and on the low- (0.08Hz) and high-frequency (0.25 Hz) spectral components afterpower spectralanalysis of RR variability (lower panels) in an individual patient. Note the higher variability after training and its morepredominant high-frequency pattern. This individual subject trained first and then entered the resting (detraining) phase.
Symptom AssessmentThere were significant improvements (higher scores
better) after training in patient-scored symptoms ofbreathlessness (2.5+0.3 to 3.9+0.4,p<0.01) and fatigue(2.4±0.4 to 4.6±0.4, p<0.001) but no change in theperception of chest pain. Significant improvements withtraining were also seen in the daily activity scores(1.4±0.5 to 4.6±0.4, p<0.01) and in the ease of theseactivities (2.6±0.3 to 4.0±0.4,p<0.01).
Correlates of Improved Exercise PerformanceTo elucidate the factors most likely to predict the
improvement in exercise capacity, simple and multiple
linear regression analysis was performed for baselineparameters against the percentage improvement in up-right exercise time or maximal oxygen uptake; these twowere very highly correlated, as expected, and eithercould substitute in the regression equations. None ofthe baseline characteristics significantly predicted im-provement; in particular, there was no evidence for themore severely affected patients with lower initial leftventricular ejection fractions or lower peak oxygenuptakes having a different response to training. Therewas, however, a strong correlation between improve-ment and the independently measured compliance tothe program (r=0.74,p<0.01); this relation is shown in
100-
c
0
c
05-
IL
-J
00
CB0
0
a.
100
80-
60 -
40 -
20 -
0
p c 0.05
Rest
ctC0
&L
a
CL
80 -
60
40-
201
0o
Training
1 5 4
1 4 c
1 34
1 115
7 - 5
1 012,041
p c 0.05
9
1 2a
3
TrainingRest
FIGURE 9. Graphs show effects ofphysical training on low-frequency (left panel) and high-frequency (right panel) oscillatorycomponents. Normalized units (nu), percentage ofeach spectral component of the total oscillatory power, both n=15. Individualsubjects are identified by number.
0
100
000E
0
140
N
cmJ00
E
0
256
0 0.5
.
9 1
r
Trailning
1
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

Coats et al Physical Training in Heart Failure 2127
duced by training were well correlated with improvedexercise tolerance.
Discussionr=0.74, p<0.01 There are many similarities between the abnormali-
ties associated with CHF and those seen in physicaldeconditioning. Both conditions are associated withexercise intolerance, sympathetic activation,27,28 re-duced heart rate variability,29,30 wasted skeletal mus-cle,31'32 and depleted skeletal muscle oxidative en-zymes.32,33 In CHF, acute pharmacologically ortransplant-induced improvements in hemodynamics are
20 40 60 80 100 120 not associated with immediate improvements in exerciseCompliance (%) performance, because the increased exercise tolerance
Graph shows relation between percentage inere- often takes several weeks to develop.3435 This may bedue to the need for increased activity to reverse some of
rcise tlrnagiscmlaetthtaig the secondary abnormalities of CHF, which may them-=16. selves have actually become the limiting factors toexercise. This study gives some insight into whether
trninob 2IlnpJ rnLn n2rtinlv rpvprQP. thLi f^ni'ir'cLFigure 10. There was no significant correlation betweenthe severity of heart failure (measured by either ejec-tion fraction or peak oxygen uptake) and compliance tothe program.We investigated whether other patient characteristics
were related to the extent of training-induced changesin the measures of autonomic function. There was nosignificant effect on these changes (either absolute orpercentage change) of the site of prior myocardialinfarction, the history of coronary bypass grafting, theduration of heart failure symptoms, or the taking of orduration of any particular cardiovascular medication.There were only two subjects taking digoxin, only one ona calcium antagonist, and only two not taking an ACEinhibitor; therefore, these numbers were too small todetermine whether these medications significantly af-fected the training response.We determined which training-induced change was
best correlated with the improvement in exercise per-formance as measured by the percentage increase inexercise duration. The percentage increase in heart ratevariability was the best correlate of improvement inexercise performance (r=0.79,p<0.01). The correlationbetween the increase in supine exercise tolerance andthe percentage reduction in NE spillover was also strong(r= -0.72, p<0.0l).
Using the increase in peak oxygen uptake as thedependent variable instead of exercise duration, verysimilar correlations were found. The percentage reduc-tion in submaximal exercise heart rate and the percent-age increase in nocturnal heart rate variability were thestrongest correlates of improvement (r= -0.70 andr=0.82, respectively). Other changes were not signifi-cant at the 1% level.
Correlations Between Baseline Measurements ofAutonomic Balance
At baseline, the different methods of estimatingautonomic balance correlated poorly and nonsignifi-cantly with each other, with the exception of the ex-
pected inverse correlation between LF and HF compo-nents of heart rate variability (r= -0.92, p<0.00l). Allmethods, however, showed an improvement in sym-pathovagal balance after training, and as described inthe previous section, the changes in each method pro-
WAsWoW[a11X11 1Ulaiuiv 1.all 61a117 1evelboW 119 iuaLulub
of deconditioning seen in CHF and thereby improvesymptoms and exercise performance.
General ConclusionsThe results show conclusively that in carefully se-
lected patients with ischemic heart failure of moderateto severe degree, an exercise training program at homeimproves exercise performance, hemodynamics, ventila-tion, autonomic function, and symptomatic status. Thishas been shown in the first prospective, controlled trialof training in this patient group and questions thecommonly held belief that avoidance of exercise isrequired in all forms and stages of heart failure.36 Thedegree of improvement shown here in a controlled trialis similar to that reported by Sullivan and colleagues37'38in retrospective, uncontrolled reports of rehabilitationin slightly less severely affected patients and also in earlyreports of training in patients with left ventriculardysfunction.9'39
Comparison With Training in Normal SubjectsThe percentage increase in exercise time or peak
oxygen consumption is similar to that seen in trainingprograms in normal subjects and patients with ischemicheart disease without heart failure.1 The features of thetraining response seen here are mostly consistent with anormal response to regular exercise training, includingreductions in 24-hour heart rate and blood pressure anda reduction in exercise heart rate and rate-pressureproduct. Two features are, however, not typical of thetraining response described in normal subjects. First,the reduction in heart rate during exercise seen in theupright posture is not duplicated in the supine exercisetest, and second, the increase in cardiac output we
found at submaximal work loads is not usually seen innormal subjects after training. The explanation of thesedifferences may be due to the fact that the supineposture was used in this study for exercise with hemo-dynamic measurements. A similar differential posture-dependent effect of training on heart rate has been seen
in studies that have looked at supine versus uprightexercise performance after bed rest and training.40'4' Thetraining-induced reduction in heart rate seen at restbefore the exercise test did not reach statistical signifi-
70
6c
5C
40
3c
2c
1a
I-~c
00
0E0 _
a.-0
FIGURE 10.ment in exeprogram; n
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

2128 Circulation Vol 85, No 6 June 1992
cance. This is probably due to chance, because day, night,and 24-hour average heart rates all showed significantreductions, as did the 256-beat period of ECG recordingtaken for the power spectral analysis. It may be thatanticipation of exercise causes an increased heart rate,which masks the training-induced bradycardia.The increased stroke volume we found after training
is consistent with the training response in normal sub-jects,3 the mechanism of which is not established. It mayrepresent enhanced diastolic recoil and/or a true in-crease in left ventricular mass and contractile perfor-mance. We have no data from our studies to determinewhich of these or other factors are operative, nor can wetell whether the enhanced stroke volume reponse wasdue to an increased end-diastolic volume, a decreasedend-systolic volume, or both. Athletes have been shownto use both mechanisms to increase stroke volumeduring exercise,42 a feature erroneously considered toindicate left ventricular dysfunction because it leads to areduced ejection fraction despite enhanced cardiacperformance.42
This study cannot tell us the precise mechanisms ofthe training-induced improvements in exercise capacity,but as the changes in ventilation, heart rate, and NEspillover would allow the same work load to be achievedat a lower sympathetic drive, heart rate, myocardialoxygen requirement, and minute ventilation, it is thenplausible that reserve exercise capacity could be en-hanced. It is not known whether these are direct effectsor whether they reflect reflex adaptations to enhancedskeletal muscle performance.
Training Effects on Autonomic BalanceAbnormalities in the autonomic control of the circu-
lation have been frequently described as part of thesyndrome of CHF.2843 Little is known of the mechanismof these changes in autonomic balance. Chronic activa-tion of the adrenergic system, decreased vagal activity,and impaired arterial baroreflex activity have all beendescribed in CHF.4344 Furthermore, these may be prog-nostically important abnormalities, as reduced heartrate variability and baroreflex sensitivity and increasedplasma NE levels have all been shown to be indepen-dent predictors of increased mortality in CHF.45-47Nonpharmacological approaches to reducing sympa-thetic activity (such as exercise training) could, there-fore, be of considerable importance, given the otherimprovements in risk factors that regular exercise canproduce.
Exercise training has been shown to enhance heartrate variability and baroreflex gain and reduce catechol-amines in subjects with normal left ventricular func-tion.27,29 Recent preliminary reports have suggested arestoration of the baroreflex gain and heart rate variabil-ity after pharmacological treatment48 or transplanta-tion,30 but the beneficial effects may take many weeks todevelop, raising the possibility that physical conditioningmay be contributing to the improvements described afterthese interventions. Nothing previously has been pub-lished on the effects of physical training on the abnor-malities of autonomic control of the circulation in CHF.In this study, physical training produced significant re-ductions in 24-hour, daytime, and nighttime heart rate aswell as increased heart rate variability in both waking and
sleep states. These findings may reflect beneficialchanges in central autonomic drive and/or baroreflex andcardiopulmonary reflex gains2949 and are in agreementwith the increased vagal tone described after enduranceexercise training in sedentary hypertensive men.29,50 Thesignificant correlations between improved exercise per-formance after training and the changes in various mea-sures of autonomic tone suggest that there may be abeneficial feedback between improvement in cardiovas-cular function and shifts in autonomic balance fromsympathetic to vagal predominance.A number of studies have been conducted51-53 using
power spectral analysis of heart rate variability as anoninvasive means of assessing "tonic" autonomic inputto the heart. This method has, however, been little usedto assess the autonomic balance in a controlled inter-vention trial in CHF. A reduced sympathetic activityafter training suggested by the changes in power spec-tral components was confirmed in this study by asignificant reduction in whole-body NE spillover. Eventhis method is not a direct measure of sympatheticactivity, as it cannot differentiate between differentcauses for the measured increase in the rate at whichNE spills over from the nerve terminals. This could bedue to increased presynaptic release of NE, decreaseduptake of NE by uptake1, or a combination of mecha-nisms. We have no information in this study on themechanisms of the apparently reduced sympatheticactivity.An increase in vagal tone was suggested by the
increase in both the relative and absolute oscillatorypowers of the HF power spectral component and therelative bradycardia both during exercise and on 24-hour ECG monitoring.We found no evidence for any differences in the
autonomic effects of training when the patients weresubdivided on the basis of disease severity and duration,pharmacological treatment, or history of coronary by-pass grafting. All except two of the patients were takingACE inhibitors (known to affect parasympathetic tone),so we can conclude that training has effects additive toACE inhibition, but we cannot determine whether thereis any significant interaction between training and ACEinhibition. This is the subject of a blinded trial currentlyunderway.The lack of significant intermethod correlations be-
tween the individual autonomic techniques at baselinein our patients may indicate that in CHF, individualmeasures of autonomic balance reflect different aspectsof circulatory control, and a comprehensive descriptionnecessitates more than one method. These results sug-gest that single techniques for estimating autonomicbalance may be inadequate to describe autonomic func-tion in CHF.
Significance of Training EffectsCardiac failure is associated with enhanced vasocon-
strictor activity caused by activation of the sympatheticnervous, renin-angiotensin, and arginine-vasopressinsystems.54 This endogenous release of vasoconstrictorneurohormones may eventually play a deleterious rolein the development of CHF, increasing the loadingconditions of the failing ventricle and favoring thedevelopment of complex ventricular arrhythmias. Rest-
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

Coats et al Physical Training in Heart Failure 2129
ing supine plasma NE is a significant independentpredictor of mortality among patients with moderate tosevere CHF.45 The results of this trial suggest thatphysical training may not only improve exercise toler-ance but may also improve prognosis because of reduc-tions in adverse prognostic features (e.g., increased NEspillover, reduced heart rate variability).55'56 Training inischemic heart disease without heart failure has beensuggested to have a beneficial effect on prognosis.57
Comparison With Other Therapeutic ApproachesPrevious reports have shown that the reduced heart
rate variability in heart failure is partially corrected bycardiac transplantation.30 Our values of heart rate vari-ability in the baseline phase are similar to those de-scribed by Smith et a130 before transplantation. Thechange in heart rate variability produced by trainingseen in our study is of similar magnitude to the in-creased variability described after transplantation. In-creased physical activity and training effects after trans-plantation may explain a large part of the improvedheart rate variability described by Smith and colleaguesand may also explain the delay in improvement seenafter cardiac transplantation.35 Similar delays are de-scribed after ACE inhibitor treatment and may similarlyreflect the need to undo some of the effects of physicaldeconditioning.34
Physical Deconditioning as a Complication of CHFProlonged inactivity is common in advanced heart
failure. This will lead to deconditioning of the skeletalmuscle and cardiovascular system, which may be partlyresponsible for the abnormalities of autonomic controlof heart rate described in heart failure. Future studiesshould control for conditioning status when assessingautonomic function in heart failure in either cross-sectional or intervention studies.The training-induced increase in cardiac output and
reduced peripheral resistance may be primarily a pe-ripheral adaptation either with reduced vasoconstrictorinfluences or with enhanced skeletal muscle bulk in-creasing effective limb vasodilatory capacity via anincreased muscle vascular network. It is known thatthere is a profound wasting of skeletal muscles in CHF(N. Buller and P. Poole-Wilson, personal communica-tion), and this may be partially reversed by exercisetraining of the leg muscles. In addition, there may be animprovement in left ventricular pumping capacity, per-haps resulting from a true positive inotropic effect oftraining as seen in animals.58 Thus, the increased sub-maximal and peak cardiac output produced by trainingcould be due to changes in the peripheral circulation,preload and afterload changes, or direct positive inotro-pic changes in ventricular muscle such as that describedin athletes.
Changes that have been proposed as important limi-tations to exercise in CHF such as skeletal musclehistological and metabolic changes may also be partlyattributable to muscle wasting secondary to prolongedinactivity. Further prospective trials early in the evolu-tion of heart failure would be necessary to show
Ventilatory EffectsBeneficial reductions are seen in minute ventilation
during exercise. The slope of the ventilation-to-carbondioxide production relation has been used as a markerof the severity of CHF,26 and this has been significantlyimproved by physical training. These findings may helpexplain the reduced sensation of breathlessness ob-served in this trial and may allow a greater respiratoryreserve during endurance exercise. Whether this bene-ficial effect on ventilation reflects more efficient muscu-lar performance, reduced pulmonary capillary wedgepressures, or an improved matching of ventilation toperfusion in the lung cannot be answered by this studybut could provide an interesting insight into the poorlyunderstood basis for the excessive ventilation seen inCHF.
LimitationsLimitations to the extension of this trial into treat-
ment of a wider patient group include the very strictentry criteria and the selection of a homogeneouspatient population. Only patients with an ischemicetiology were entered into this trial, and it remains a
possibility that some of the idiopathic cardiomyopathiesmay have an adverse response to the repetitive sympa-thetic stimulation of exercise (despite perhaps a reduc-tion in sympathetic activity throughout the rest of theday) or may not show the same benefits in exercisetolerance and autonomic balance. No patients withlimiting angina were recruited into this trial, but withthe known benefits of exercise training on anginathresholds59 and collateral development,60 it is likelythat training would be of benefit in the patients withmixed heart failure and angina. It may seem surprisingthat patients with an ischemic etiology did not haveECG evidence of myocardial ischemia, but some hadhad bypass grafting and all were highly selected so thatreversible myocardial ischemia was not a cause ofexercise limitation. In addition, no patients with seriousventricular arrythmias (e.g., ventricular tachycardia)were recruited; hence, it may be argued that thesepatients are for both these reasons not truly represen-tative of a general CHF population. The results remainvalid for this specific group, and similar studies indifferent groups of heart failure patients would clearlybe worthwhile.The methods for assessing autonomic function have
not been rigidly validated in CHF because no goldstandard exists that can be used in intact humans.Differences in a-receptor responsiveness will affectnerve traffic measures (e.g., NE spillover) differently toend-organ response measures (e.g., heart rate andpower spectral measures). No data exist on the effect ofphysical training on ,-receptor function in CHF. Thewide range of autonomic functional measures usedhere, all showing a similar trend, go some way toovercoming the lack of a truly representative and quan-titative measure of sympathetic and vagal control of thecirculation.
Safety and prognosis cannot be addressed in a small,intensive study of this nature, but an overview ofrehabilitation programs suggests an overall improve-
whether the secondary changes could be ameliorated byavoidance of physical deconditioning.
ment in prognosis in ischemic heart disease.57 Theincidence of potentially fatal exercise-induced arrhyth-
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

2130 Circulation Vol 85, No 6 June 1992
mias in rehabilitation programs or exercise testing inheart failure is very low61 and would add a negligibleextra risk, given the extremely poor prognosis of thesepatients. One hundred minutes of exercise per weekwould add very little to their risk of death based on theincidences of arrhythmias seen in rehabilitation pro-grams and in maximal exercise testing in heart failuretrials. There is also the possibility of improving progno-sis by reducing the susceptibility to ventricular arrhyth-mias and improving heart rate variability and perhapsother cardiovascular risk factors including blood lipidsand sympathetic activation.At what stage heart failure patients should be advised
to train cannot be definitively answered in this study.Training is beneficial after the early healing phase ofmyocardial infarction; provided that the patient is stablewith no evidence of exercise-induced ventricular ar-rhythmia and provided that diuretic treatment is opti-mized, training should be recommended down to theseverity of patients in this report, i.e., the ability toperform at least 50-W bicycle exercise for 3-4 minutes.The intensity of training should, however, be custom-ized for each patient and only recommended afterdetailed cardiac and cardiopulmonary evaluation.
ConclusionsTraining can improve the symptoms, exercise perfor-
mance, hemodynamics, ventilation, autonomic function,and symptoms in stable moderate to severe heart failurepatients. The possibility that exercise could lessen orreverse some of the secondary abnormalities of CHF israised, and recommendations of the use of training inCHF are proposed.
AcknowledgmentsWe are grateful to Dr. George Hart and Dr. Jim Holt for
permission to enter their patients in this trial.
References1. Clausen JP: Circulatory adjustments to dynamic exercise and effect
of physical training in normal subjects and in patients withcoronary artery disease. Prog Cardiovasc Dis 1976;18:459-495
2. Scheuer J, Tipton CM: Cardiovascular adaptations to physicaltraining. Ann Rev Physiol 1977;39:221-251
3. Blomqvist CG: Cardiovascular adaptations to physical training.Ann Rev Physiol 1983;45:169-189
4. Astrand P-O, Rodahl K: Textbook of Work Physiology: PhysiologicalBases of Exercise. New York, McGraw-Hill Book Co, 1986
5. Shabetai R: Beneficial effects of exercise training in compensatedheart failure. Circulation 1988;78:775-776
6. Mathes P: Physical training in patients with ventricular dysfunc-tion: Choice and dosage of physical exercise in patients with pumpdysfunction. Eur Heart J 1988;9(suppl F):67-69
7. McHenry MM: Medical screening of patients with coronary heartdisease: Criteria for entry into exercise conditioning programs.AmJ Cardiol 1974;33:752-756
8. Council on Scientific Affairs: Physician-supervised exercise pro-grams in rehabilitation of patients with coronary heart disease.JAMA 1981;245:1463-1466
9. Coats AJS, Adamopoulos S, Meyer TE, Conway J, Sleight P:Effects of physical training in chronic heart failure. Lancet 1990;335:63-66
10. Murphy C, Coats A, Conway J, Colditz P, Rolphe P: Dopplerultrasound signal analysis based on the TMS320 signal processor.J Biomed Eng 1988;10:127-129
11. Coats AJS, Murphy C, Conway J, Sleight P: Validation of the beatto beat measurement of ascending aortic blood velocity in manusing a new high temporal resolution Doppler ultrasound spectralanalyser. Br Heart J (in press)
12. Coats AJS: Doppler ultrasonic measurement of cardiac output:Validation and reproducibility. EurHeartJ 1990;11(suppl l):49-61
13. Coats AJS, Conway J, Somers VK, Isea JE, Sleight P: Ambulatorypressure monitoring in the assessment of antihypertensive therapy.Cardiovasc Drug Therapy 1989;3:303-311
14. Rossi PRF, Yusuf S, Ramsdale D, Furze L, Sleight P: Reduction ofventricular arrhythmias by early intravenous atenolol in suspectedacute myocardial infarction. Br Med J 1983;286:506-510
15. Press WH, Flannery BP, Teukolsky SA, Vetterling WT: NumericalRecipes: The Art of Scientific Computing. New York, CambridgeUniversity Press, 1986, pp 495-497
16. Kay SM, Marple SL Jr: Spectrum analysis: A modern perspective.Proc IEEE 1981;69:1380-1419
17. Ulrych TJ, Bishop TN: Maximum entropy spectral analysis andautoregressive decomposition. Rev Geophys Space Phys 1975;13:183-200
18. Pagani M, Lombardi F, Guzzetti S, Rimoldi 0, Furlan R, PizzinelliP, Sandrone G, Malfatto G, Dell'Orto S, Piccaluga E, Turiel M,Baselli G, Cerutti S, Malliani A: Power spectral analysis of heartrate and arterial pressure variabilities as a marker of sympatho-vagal interaction in man and conscious dog. Circ Res 1986;59:178-193
19. Zetterberg LH: Estimation of parameters for a linear differenceequation with application to EEG analysis. Math Biosci 1969;5:227-275
20. Isaksson A, Wennberg A, Zetterberg LH: Computer analysis ofEEG signals with parametric models. Proc IEEE 1981;69:451-461
21. Pomeranz B, Macaulay RJB, Caudill MA, Kutz I, Adam D,Gordon D, Kilborn KM, Barger AC, Shannon DC, Cohen RJ,Benson H: Assessment of autonomic function in humans by heartrate spectral analysis. Am J Physiol 1985;248:H151-H153
22. Akselrod S, Gordon D, Madwed JB, Snidman NC, Shannon DC,Cohen RJ: Hemodynamic regulation: Investigation by spectralanalysis. Am J Physiol 1985;249:H867-H875
23. Bernardi L, Keller F, Sanders M, Reddy PS, Griffith B, Meno F,Pinsky MR: Respiratory sinus arrhythmia in the denervatedhuman heart. JAppl Physiol 1989;67:1447-1455
24. Esler M, Jackman G, Bobik A, Kelleher D, Jennings G, Leonard P,Skews H, Korner P: Determination of norepinephrine apparentspillover rate and clearance in humans. Life Sci 1979;25:1461-1470
25. Hills M, Armitage P: The two-period cross-over clinical trial. Br JClin Pharmacol 1979;8:7-20
26. Buller NP, Poole-Wilson PA: Mechanism of the increased venti-latory response to exercise in patients with chronic heart failure. BrHeart J 1990;63:281-283
27. Cooksey JD, Reilly P, Brown S, Bomze H, Cryer PE: Exercisetraining and plasma catecholamines in patients with ischemic heartdisease. Am J Cardiol 1978;42:372-376
28. Leimbach WH, Wallin G, Victor RG, Aylward PE, Sundlof E,Mark A: Direct evidence from intraneural recordings for increasedcentral sympathetic outflow in patients with heart failure. Circula-tion 1986;73:913-919
29. Pagani M, Somers V, Furlan R, Dell'Orto S, Conway J, Baselli G,Cerutti S, Sleight P: Changes in autonomic regulation induced byphysical training in mild hypertension. Hypertension 1988;12:600-610
30. Smith ML, Ellenbogen KA, Eckberg DL, Szentpetery S, ThamesMD: Subnormal heart period variability in heart failure: Effect ofcardiac transplantation. JAm Coll Cardiol 1989;14:106-111
31. Buller NP, Jones D, Poole-Wilson PA: Direct measurement ofskeletal muscle fatigue in patients with chronic heart failure. BrHeart J 1991;65:20-24
32. Holloszy JO: Adaptations of muscular tissue to training. ProgCardiovasc Dis 1976;18:445-458
33. Sullivan MJ, Green HJ, Cobb FR: Skeletal muscle biochemistryand histology in ambulatory patients with long-term heart failure.Circulation 1990;81:518-527
34. Drexler H, Banhardt U, Meinertz T, Wollschlager H, Lehmann M,Just H: Contrasting peripheral short-term and long-term effects ofconverting enzyme inhibition in patients with congestive heartfailure: A double-blind, placebo-controlled trial. Circulation 1989;79:491-502
35. Sinoway L, Minotti JR, Davis D, Pennock JL, Burg JE, Musch TI:Delayed reversal of impaired vasodilatation in congestive heartfailure after heart transplantation. Am J Cardiol 1988;61:1076-1079
36. Smith TW, Braunwald E, Kelly RA: The management of heartfailure, in Braunwald E (ed): Heart Disease. Philadelphia, WBSaunders Co, 1988, pp 485-543
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from

Coats et al Physical Training in Heart Failure 2131
37. Sullivan MJ, Higginbotham MB, Cobb FR: Exercise training inpatients with chronic heart failure delays ventilatory anaerobicthreshold and improves submaximal exercise performance. Circu-lation 1989;79:324-329
38. Sullivan MJ, Higginbotham MB, Cobb FR: Exercise training inpatients with severe left ventricular dysfunction: Hemodynamicand metabolic effects. Circulation 1988;78:506-515
39. Conn EH, Williams RS, Wallace AG: Exercise responses beforeand after physical conditioning in patients with severely depressedleft ventricular function. Am J Cardiol 1982;49:296-300
40. Convertino V, Hung J, Goldwater D, DeBusk RF: Cardiovascularresponses to exercise in middle-aged men after 10 days of bed rest.Circulation 1982;65:134-140
41. Saltin B, Blomqvist G, Mitchell JH, Johnson RL Jr, Wildenthal K,Chapman CB: Response to exercise after bed rest and aftertraining. Circulation 1968;38(suppl VII):VII-1-VII-78
42. Fisman EZ, Frank AG, Ben-Ari E, Kessler G, Pines A, Drory Y,Kellermann JJ: Altered left ventricular volume and ejection frac-tion responses to supine dynamic exercise in athletes. JAm CollCardiol 1990;15:582-585
43. Eckberg DL, Drabinsky M, Braunwald E: Defective cardiac para-sympathetic control in patients with heart disease. N Engl J Med1971;285:877-883
44. Olivari MT, Levine TB, Cohn JT: Abnormal neurohumoralresponse to nitroprusside infusion in congestive heart failure.JAmCoil Cardiol 1983;2:411-417
45. Cohn JN, Levine TB, Olivari MT, Garberg V, Lura D, Francis GS,Simon AB, Rector T: Plasma norepinephrine as a guide toprognosis in patients with chronic congestive heart failure. N EnglJ Med 1984;311:819-823
46. Saul JP, Arai Y, Berger RD, Lilly LS, Colucci WS, Cohen RJ:Assessment of autonomic regulation in chronic congestive heartfailure by heart rate spectral analysis. Am J Cardiol 1988;61:1292-1299
47. Kleiger RE, Miller PJ, Bigger TJ, Moss AJ, Multicenter Post-Infarction Research Group: Decreased heart rate variability andits association with increased mortality after acute myocardialinfarction. Am J Cardiol 1987;59:256-262
48. Marin-Neto JA, Pintya AO, Gallo L, Maciel BC: Reversibility ofimpaired heart rate reflex control in congestive heart failure.(abstract) Circulation 1988;36:299A
49. Seals DR, Chase P: Influence of physical training on heart ratevariability and baroreflex circulatory control. J Appi Physiol 1989;66:1886-1895
50. Somers VK, Conway J, Sleight P: The effect of physical training onhome blood pressure measurements in normal subjects.JHypertens 1986;4(suppl 6):S657-S658
51. Akselrod S, Gordon D, Ubel FA, Shannon DC, Barger AC, CohenRJ: Power spectrum analysis of heart rate fluctuation: A quanti-tative probe of beat-to-beat cardiovascular control. Science 1981;213:220-222
52. Lombardi F, Sandrone G, Pempruner S, Salari R, Garimoldi M,Cerutti S, Baselli G, Pagani M, Malliani A: Heart rate variability asan index of sympathovagal interaction after acute myocardialinfarction. Am J Cardiol 1987;60:1239-1245
53. Sands KEF, Appel ML, Lilly LS, Schoen FJ, Mudge GH, CohenRJ: Power spectrum analysis of heart rate variability in humancardiac transplant recipients. Circulation 1989;79:76-82
54. Francis GS: Neurohumoral mechanisms involved in congestiveheart failure. Am J Cardiol 1985;55:15A-21A
55. Szlachic J, Massie BM, Kramer BL, Topic N, Tubau J: Correlatesand prognostic implication of exercise capacity in chronic conges-tive heart failure. Am J Cardiol 1985;55:1037-1042
56. Myers GA, Martin GJ, Magid NM, Barnett PS, Schaad JW, WeissJS, Lesch M, Singer DH: Power spectral analysis of heart ratevariability in sudden cardiac death: Comparison to other methods.IEEE Trans Biomed Eng 1986;33:1149-1156
57. O'Connor GT, Buring JE, Yusuf S, Goldhaber SZ, Olmstead EM,Paffenbarger RS Jr, Hennekens CH: An overview of randomizedtrials of rehabilitation with exercise after myocardial infarction.Circulation 1989;80:234-244
58. Crews J, Aldinger EE: Effect of chronic exercise on myocardialfunction. Am Heart J 1967;74:536-542
59. Todd IC, Ballantyne D: Antianginal efficacy of exercise training: Acomparison with 3-blockade. Br Heart J 1990;64:14-19
60. Eckstein RW: Effect of exercise and coronary artery narrowing oncoronary collateral circulation. Circ Res 1957;5:230-235
61. Von Camp SP, Peterson RA: Cardiovascular complications ofoutpatient cardiac rehabilitation programs. JAMA 1986;256:1160-1163 by guest on Septem
ber 1, 2017http://circ.ahajournals.org/
Dow
nloaded from

Davey, O Ormerod and C ForfarA J Coats, S Adamopoulos, A Radaelli, A McCance, T E Meyer, L Bernardi, P L Solda, P
hemodynamics, ventilation, and autonomic function.Controlled trial of physical training in chronic heart failure. Exercise performance,
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1992 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.85.6.2119
1992;85:2119-2131Circulation.
http://circ.ahajournals.org/content/85/6/2119the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on September 1, 2017
http://circ.ahajournals.org/D
ownloaded from