copyright © 2013 wolters kluwer health | lippincott williams & wilkins cervical and thoracic...
TRANSCRIPT

Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Cervical and Thoracic Spinal Conditions
Cervical and Thoracic Spinal Conditions
Chapter 11
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
AnatomyAnatomy
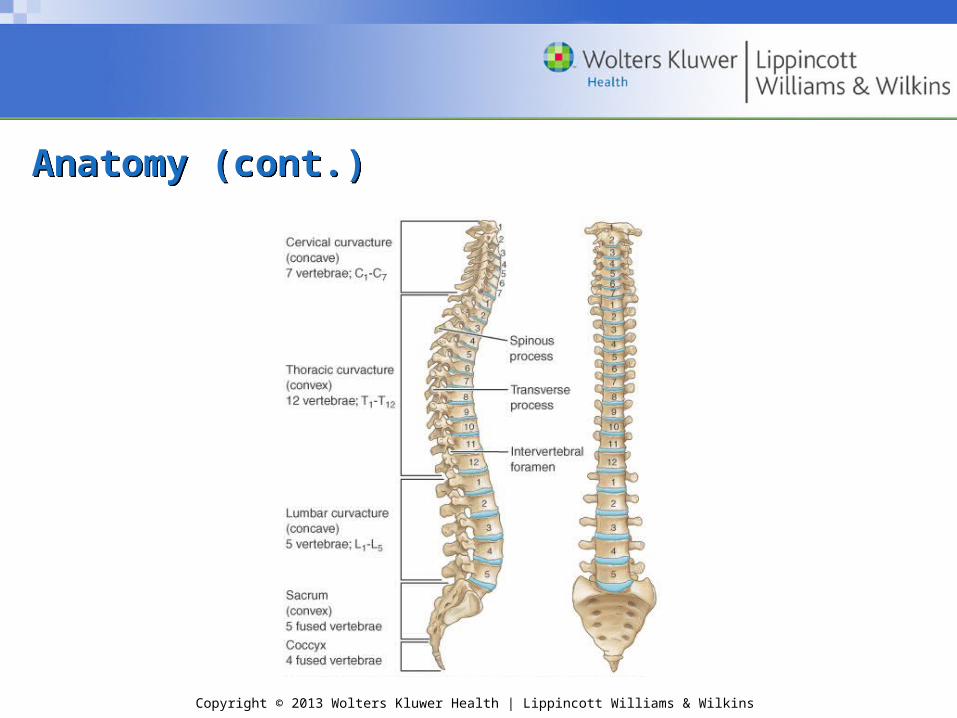
• Spinal column– Vertebrae
• Cervical (7)convex anteriorly
• Thoracic (12)concave anteriorly
• Lumbar (5)convex anteriorly
• Sacral (5 fused)concave anteriorly
• Coccyx (4 fused)
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Anatomy (cont.)Anatomy (cont.)
– Structure• Rigid enough to support body and protect
spinal cord• Flexible enough to produce a
variety of movements
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Anatomy (cont.)Anatomy (cont.)
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Anatomy (cont.)Anatomy (cont.)

Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Anatomy (cont.)Anatomy (cont.)
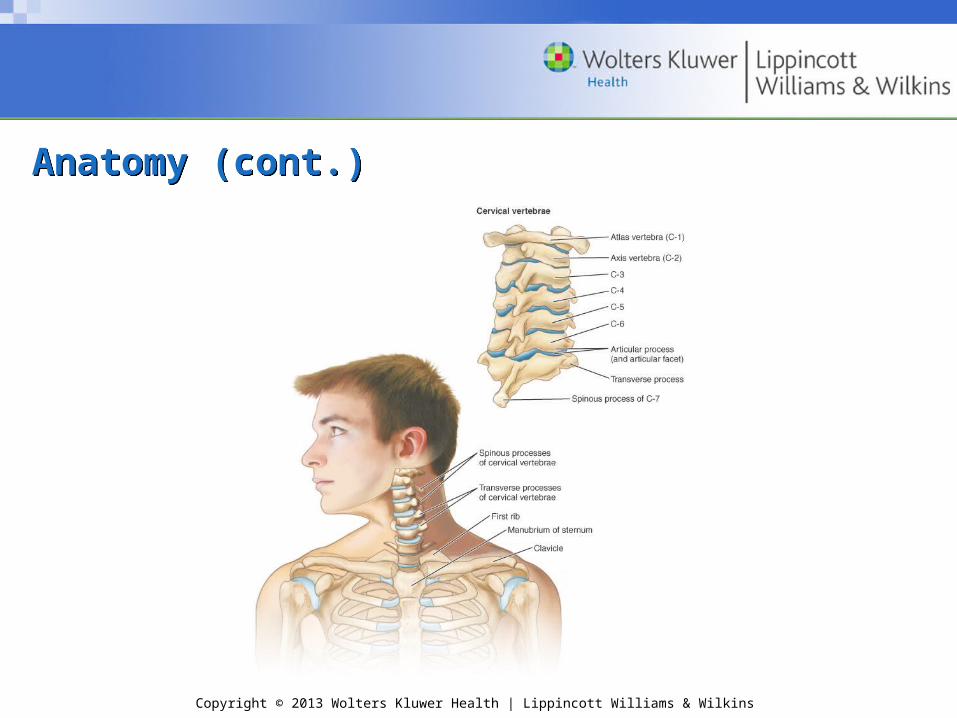
• Cervical– 7 vertebrae form curve – convex anteriorly– Atlas
• 1st vertebra• No body – filled with odontoid process• Function: support the head
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Anatomy (cont.)Anatomy (cont.)
– Axis• 2nd vertebra• Odontoid process – tooth-like• Allows head to rotate
• Thoracic– 12 vertebrae form curve – concave anteriorly – Extra facets for articulation with ribs

Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Anatomy (cont.)Anatomy (cont.)

Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Anatomy (cont.)Anatomy (cont.)• Vertebral structure
– Body
– Vertebral arch
– Superior and inferior articular processes
• Facet joints
– Spinous process
– Transverse processes
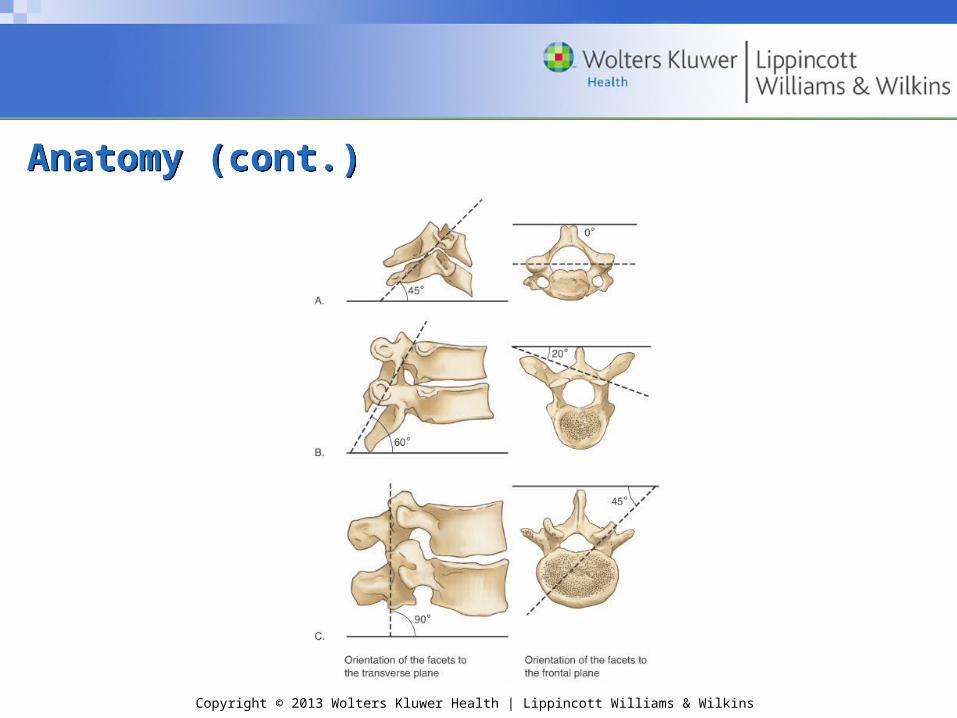
• Progressive increase in vertebral size
• Change in angulation
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Anatomy (cont.)Anatomy (cont.)
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Anatomy (cont.)Anatomy (cont.)
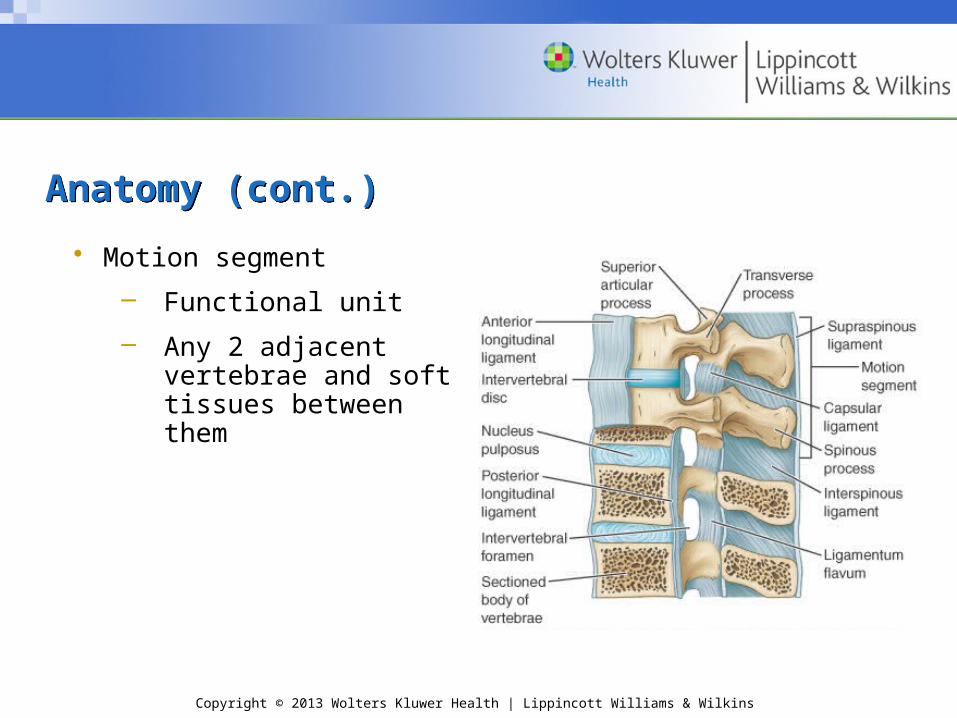
• Motion segment
– Functional unit
– Any 2 adjacent vertebrae and soft tissues between them

Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Anatomy (cont.)Anatomy (cont.)
• Intervertebral discs
– Components
• Annulus fibrosus
Thick fibrous ring
• Nucleus pulposus
Gelatinous interior
– Function
• Shock absorption
• Allow spine to bend

Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Anatomy (cont.)Anatomy (cont.)
• Ligaments
– Anterior longitudinal
– Posterior longitudinal
– Ligamentum flavum
– Interspinous
– Supraspinous
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Anatomy (cont.)Anatomy (cont.)
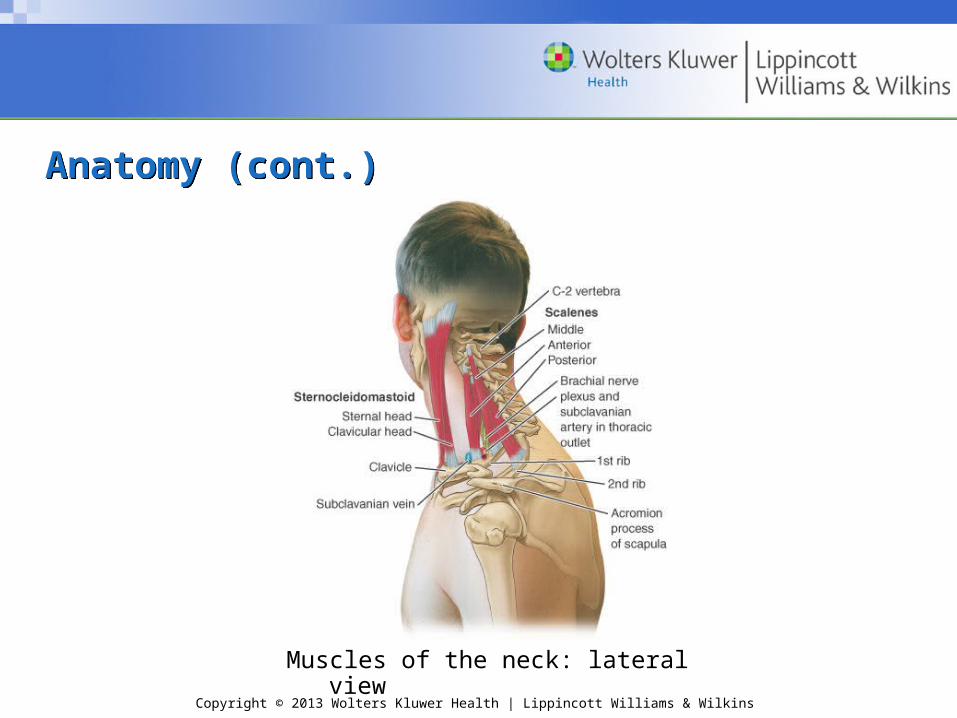
Muscles of the neck: lateral view
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
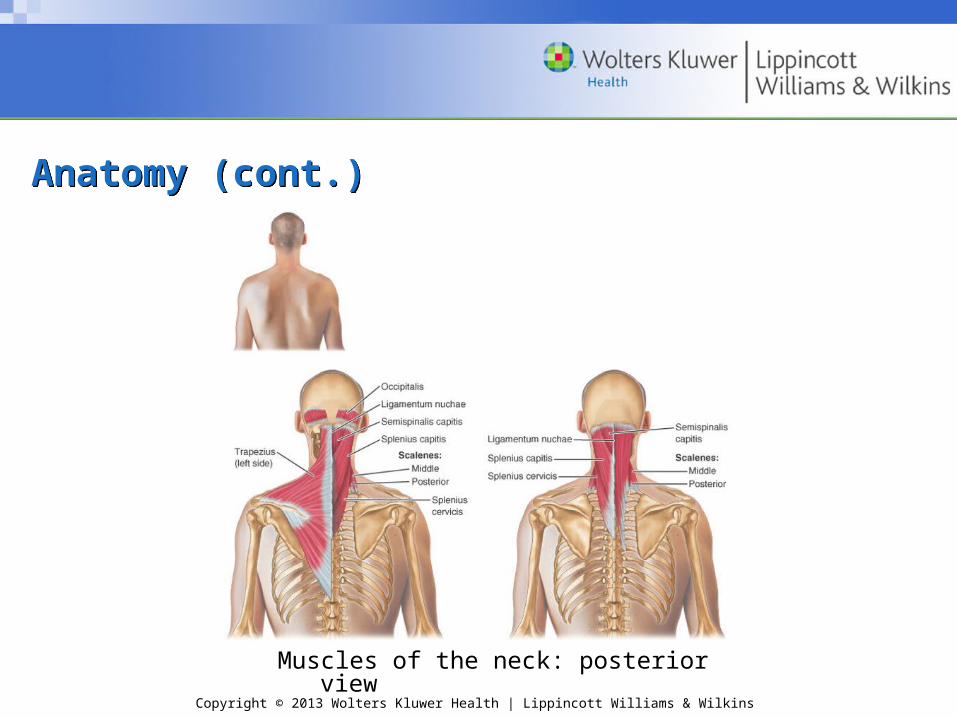
Anatomy (cont.)Anatomy (cont.)
Muscles of the neck: posterior view
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
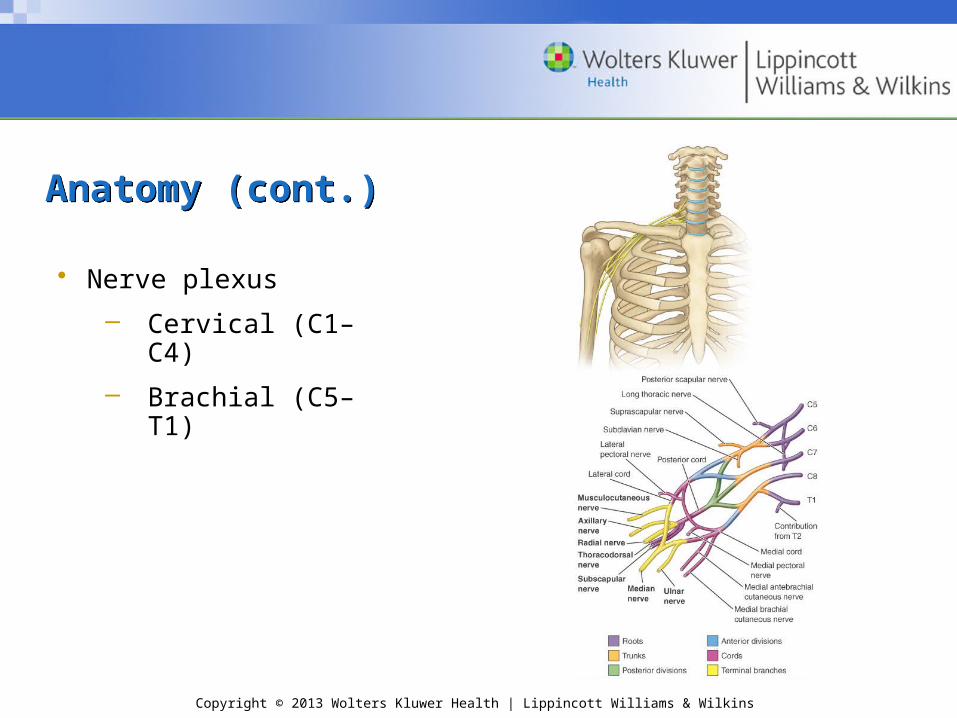
Anatomy (cont.)Anatomy (cont.)
• Nerve plexus
– Cervical (C1–C4)
– Brachial (C5–T1)

Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Anatomy (cont.)Anatomy (cont.)
• Blood supply
– Common carotid
– Vertebral
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
KinematicsKinematics
• Movements involve a number of motion segments– Flexion/extension/ hyperextension– Lateral flexion– Lateral rotation
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
KineticsKinetics• Effects of loading
– Primary load
• Cervical spine: weight of head
• Thoracic: weight of body above and any load in hands
• Effects of impact forces
– High speed and collision → risk
– Cervical flexion (large bending moment) + axial compression load = danger

Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Kinetics (cont.)Kinetics (cont.)
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
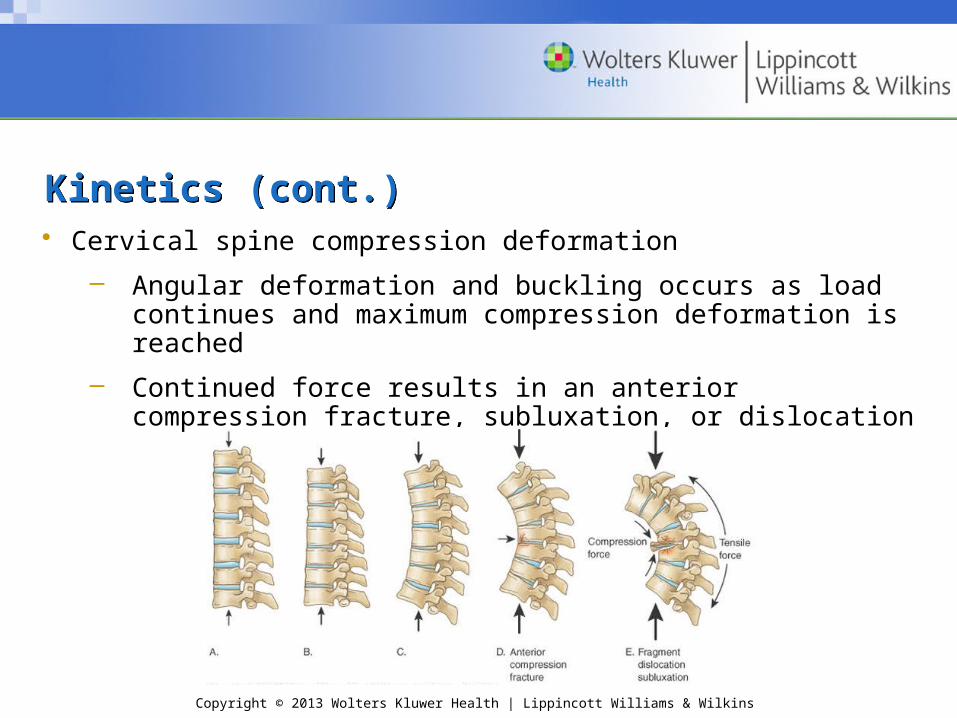
Kinetics (cont.)Kinetics (cont.)• Cervical spine compression deformation
– Angular deformation and buckling occurs as load continues and maximum compression deformation is reached
– Continued force results in an anterior compression fracture, subluxation, or dislocation
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Anatomic Variations: Injury PotentialAnatomic Variations: Injury Potential• Kyphosis
– Excessive curve of thoracic spine– Congenital – deficits in vertebral bodies– Idiopathic
• Scheuermann’s disease– Secondary to osteoporosis

Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Anatomic Variations: Injury Potential (cont.)Anatomic Variations: Injury Potential (cont.)• Scoliosis
– Lateral curvature of spine; “C” or “S” curve– Structural
• Inflexible curve, persists with lateral bending
– Nonstructural• Flexible, corrected with lateral bending
– Commonly idiopathic
– Symptoms vary with severity• Mild 20 and moderate = 20–45
Treated with exercise• Severe

Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Anatomic Variations: Injury Potential (cont.)Anatomic Variations: Injury Potential (cont.)
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Prevention of Spinal InjuriesPrevention of Spinal Injuries
• Protective equipment
– Neck roll
– Rib protectors
• Physical conditioning
– Strength and flexibility
• Proper technique
– Spearing
– Proper lifting
– Posture

Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Cervical Spine ConditionsCervical Spine Conditions• Cervical sprain
– Extreme motions or violent mechanism
– S&S
• Pain, stiffness, restricted ROM
• Pain can persist for several days
– Management: standard acute; cervical collar; consult physician
– No return to competition until pain free and ROM is normal

Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Cervical Spine Conditions (cont.)Cervical Spine Conditions (cont.)• Cervical strain
– Usually, sternocleidomastoid or upper trapezius
– Same mechanism as sprain; injuries often simultaneous
– S&S
• Pain, stiffness, spasm, restricted ROM
• pain with active contraction or passive stretch of involved muscle
– Management: standard acute; cervical collar; consult physician
– No return to competition until pain free and ROM is normal

Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Cervical Spine Conditions (cont.)Cervical Spine Conditions (cont.)
• Cervical spinal stenosis
– Structural
• Torg ratio
– Functional
• Loss of CSF around the cord → cord’s ability to decompress
– Asymptomatic until external force to head

Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Cervical Spine Conditions (cont.)Cervical Spine Conditions (cont.)
– S&S
• On impact, may develop immediate quadriplegia with sensory changes or motor deficits in both arms, both legs, or all 4 extremities
• Transient with full recovery in 10–15 minutes (or 36–48 hrs)
– Management: activate EMS
– Continued participation

Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Cervical Spine Conditions (cont.)Cervical Spine Conditions (cont.)
• Spear tackler’s spine
– Mechanism: cervical flexion + axial loading
– S&S
• Immediate pain with sensory changes and motor deficits distal to injury site
– Management: activate EMS
– Criteria to return to play—controversial
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Cervical Spine Conditions (cont.)Cervical Spine Conditions (cont.)
• Cervical disc injuries
– Soft disc herniation
• Nucleus pulposus herniates through posterior annulus
• Acute mechanism: uncontrolled lateral bending of neck
– Hard disc disease
• Chronic, degenerative
• Diminished disc height and formation of marginal osteophytes
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Cervical Spine Conditions (cont.)Cervical Spine Conditions (cont.)
– S&S
• Varying degrees of neck or arm pain, may radiate
• Pain exacerbated by Valsalva maneuvers and neck movement
• + Spurling’s maneuver
• + Babinski’s sign
• Severe cases—potential loss of motor function below injury level
– Management: rest, activity modification, NSAIDs
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Cervical Spine Conditions (cont.)Cervical Spine Conditions (cont.)
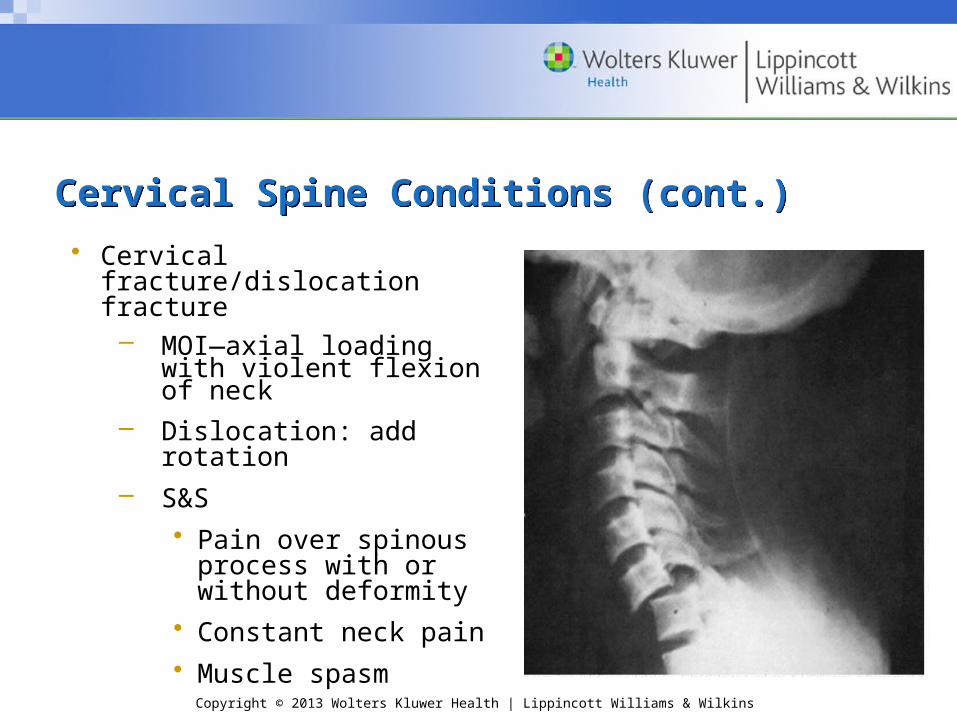
• Cervical fracture/dislocation fracture– MOI—axial loading with
violent flexion of neck– Dislocation: add rotation– S&S
• Pain over spinous process with or without deformity
• Constant neck pain • Muscle spasm

Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Cervical Spine Conditions (cont.)Cervical Spine Conditions (cont.)
• Signs of neural damage Muscle weakness in extremities; inability to
move Abnormal sensations in extremities Absent or weak reflexes Loss of bladder or bowel control
• Suspect injury with violent mechanism– Management: activate EMS
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Cervical Spine Conditions (cont.)Cervical Spine Conditions (cont.)
• “Red flags” indicating a possible cervical spine injury: refer to Box 11.1
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Brachial Plexus InjuriesBrachial Plexus Injuries
• Mechanism– Tension (stretching)
• Violent lateral movement of head and neck• Arm forced into excessive external rotation,
abduction, and extension– Compression
• Location where plexus is most superficial (Erb’s point) • Forced lateral flexion, causing increased
pressure between shoulder pad and superior medial scapula

Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Brachial Plexus Injuries (cont.)Brachial Plexus Injuries (cont.)
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Brachial Plexus Injuries (cont.)Brachial Plexus Injuries (cont.)
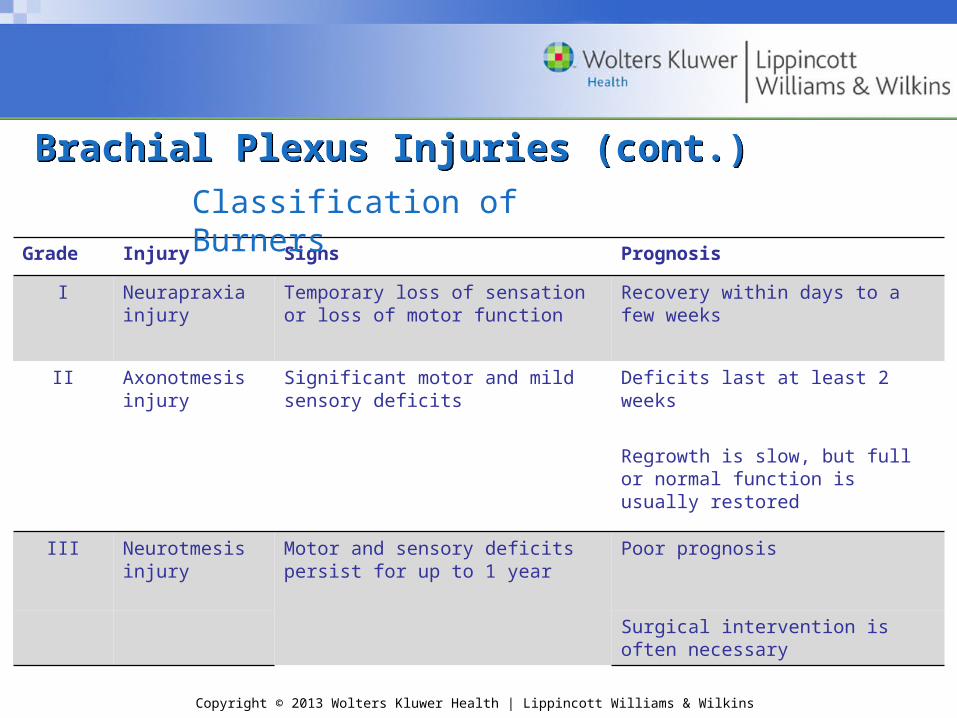
Grade Injury Signs Prognosis
I Neurapraxia injury
Temporary loss of sensation or loss of motor function
Recovery within days to a few weeks
II Axonotmesis injury
Significant motor and mild sensory deficits
Deficits last at least 2 weeks
Regrowth is slow, but full or normal function is usually restored
III Neurotmesis injury
Motor and sensory deficits persist for up to 1 year
Poor prognosis
Surgical intervention is often necessary
Classification of Burners
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Brachial Plexus Injuries (cont.)Brachial Plexus Injuries (cont.)
• Acute burners– S&S
• Immediate, severe, burning pain and prickly paresthesia radiates into hand
• Pain transient; subsides in 5–10 minutes• Weakness in abduction and external rotation
– Management: return to play—full strength, ROM, & sensation; cryotherapy
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Brachial Plexus Injuries (cont.)Brachial Plexus Injuries (cont.)
• Chronic burner syndrome– S&S
• Frequent acute episodes that may not produce areas of numbness
• Muscle weakness may develop hours or days after initial injury; dropped shoulder or visible atrophy in shoulder muscles
– Management: same parameters as acute; frequent re-examination

Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Brachial Plexus Injuries (cont.)Brachial Plexus Injuries (cont.)
• Suprascapular nerve injury
– Innervates the supraspinatus, infraspinatus, and glenohumeral joint capsule
– Same mechanism
– S&S
• Muscles weak and atrophied
• Improper functioning of muscles → other problems (e.g., rotator cuff tendinitis, impingement syndrome, bicipital tenosynovitis, or bursitis)
– Management: standard treatment; refer to physician
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Thoracic Spine ConditionsThoracic Spine Conditions• Sprains/strains
– MOI: overload; overstretch
– S&S
• Painful spasms of back muscles
May develop as a sympathetic response to sprains
Presence of spasms makes it difficult to determine sprain or strain
• Sprain—dramatic improvement in 24–48 hours; severe strains—3–4 weeks to heal
– Management: standard acute care

Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Thoracic Spine Conditions (cont.)Thoracic Spine Conditions (cont.)
• Thoracic spinal fractures and apophysitis
– Wedge fracture
• Fracture of vertebral end plates
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Thoracic Spine Conditions (cont’d)Thoracic Spine Conditions (cont’d)
• Mechanism
Large compressive loads or landing on the buttock area
Compressive stress during small, repetitive loads
• S&S: standard fracture; pain and muscle guarding
• Management: physician referral

Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Thoracic Spine Conditions (cont.)Thoracic Spine Conditions (cont.)
– Scheuermann’s disease
• Leading cause of fractures among adolescents
• Osteochondrosis of the spine
• Abnormal epiphyseal plate behavior allows herniation of disc into vertebral body
• After physician referral, treatment: activity modification, stretching (shoulder, neck, and back muscles), and strengthening (abdominal and spinal extensor muscles)

Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Thoracic Spine Conditions (cont.)Thoracic Spine Conditions (cont.)
– Apophysitis
• Repeated flexion–extension of thoracic spine
• Progressive condition characterized by local pain and tenderness
• After physician referral, treatment: eliminate flexion–extension stress; strengthening of abdominal and other trunk muscles
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Assessment of Spinal ConditionsAssessment of Spinal Conditions
• Traumatic episode– When in doubt, always assume a severe spinal
injury and activate emergency care plan– Do not move head, neck, or spine (or helmet)

Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Assessment of Spinal Conditions (cont.)Assessment of Spinal Conditions (cont.)
• “Red flags”—warrant immobilization and immediate referral– Severe pain, point tenderness, or deformity along
vertebral column– Loss or change in sensation anywhere in the body– Paralysis or inability to move a body part– Diminished or absent reflexes– Muscle weakness in a myotome– Pain radiating into the extremities– Trunk or abdominal pain referred from visceral organs– Any injury involving uncertainty about severity or nature
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Spinal Assessment—Conscious IndividualSpinal Assessment—Conscious Individual• History
– Important to ask questions about:• Pain
Location (i.e., localized or radiating) Type (i.e., dull, aching, sharp, burning)
• Sensory changes (i.e., numbness, tingling, or absence of sensation)
• Muscle weakness or paralysis– Neck injury – Determine both long- and short-term memory loss that
may indicate an associated brain injury

Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Spinal Assessment—Conscious Individual (cont.)Spinal Assessment—Conscious Individual (cont.)
• Observation/inspection– Postural assessment– Scan exam– Gait analysis– Inspection of injury site– Gross neuromuscular assessment
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Spinal Assessment—Conscious Individual (cont.)Spinal Assessment—Conscious Individual (cont.)
• Palpation
– Seated, standing, supine, or prone position
– Relax the neck and spinal muscles—lying position
– Posterior neck structures
• Patient supine
– Thoracic region
• Patient prone
• Pillow under the hip region to tilt the pelvis back and relax the lumbar curvature
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Spinal Assessment—Conscious Individual (cont.)Spinal Assessment—Conscious Individual (cont.)
• Physical examination testing
– If, at anytime, movement leads to increased acute pain or change in sensation or the individual resists moving the spine, a significant injury should be assumed and EMS activated
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Range of Motion (ROM)Range of Motion (ROM)
• Active range of motion (AROM)
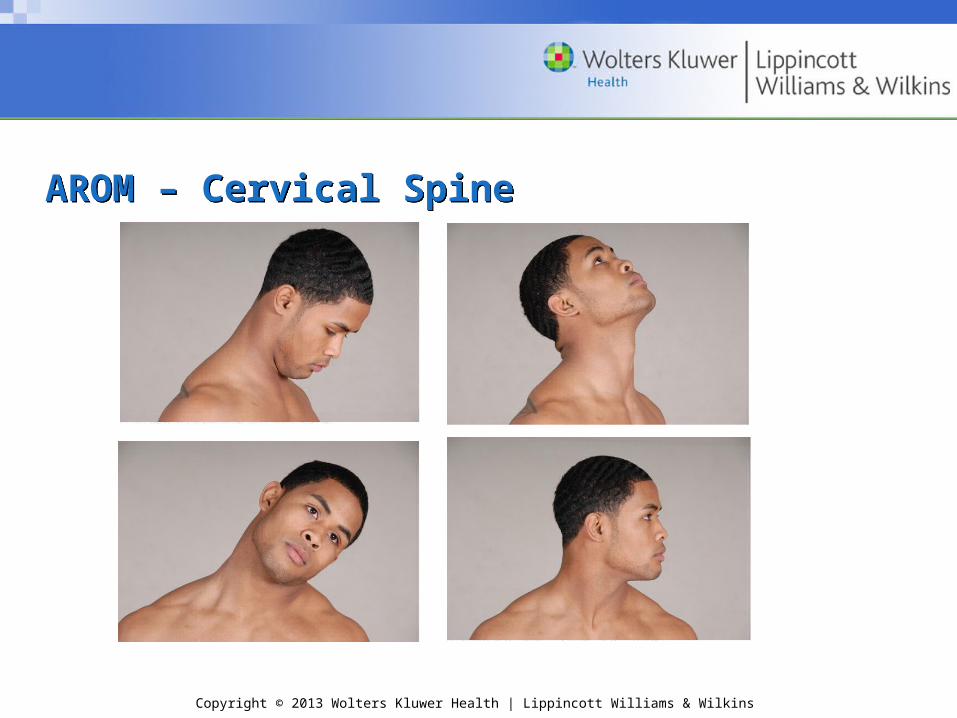
– Cervical flexion
– Cervical extension
– Lateral cervical flexion (left and right)
– Cervical rotation (left and right)
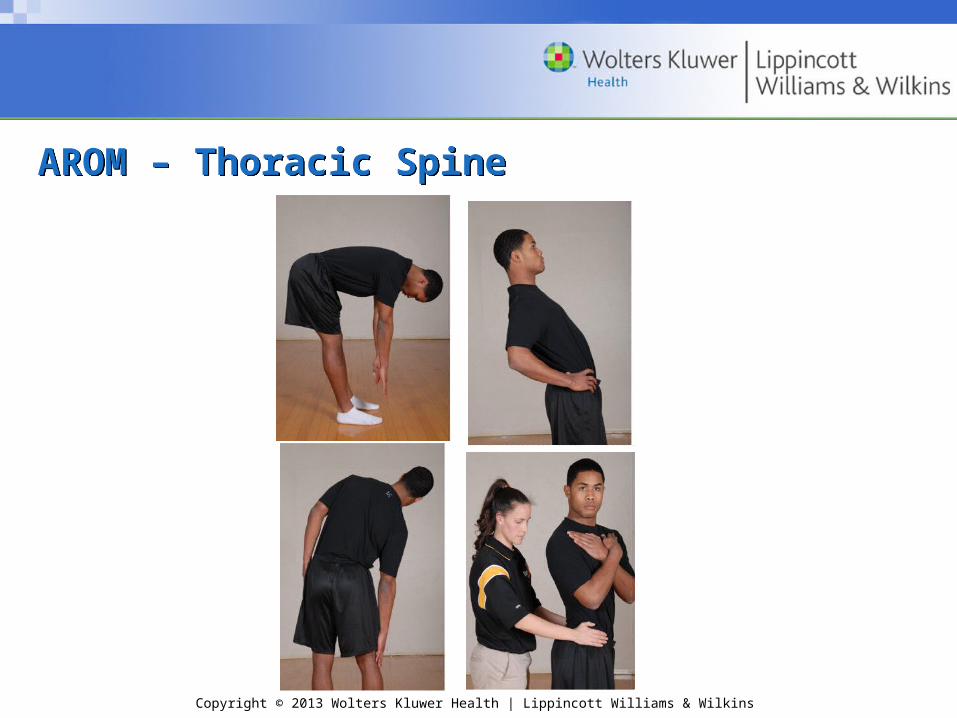
– Forward trunk flexion
– Trunk extension
– Lateral trunk flexion (left and right)
– Trunk rotation
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
AROM – Cervical SpineAROM – Cervical Spine
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
AROM – Thoracic SpineAROM – Thoracic Spine
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
ROM (cont.)ROM (cont.)• Normal ranges
– Cervical flexion—80–90°
– Cervical extension—70°
– Lateral cervical flexion (left and right)—20–45°
– Cervical rotation (left and right)—70–90°
– Forward trunk flexion—40–60°
– Trunk extension—20–35°
– Lateral trunk flexion (left and right)—15–20°
– Trunk rotation—35–50°
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
ROM (cont.)ROM (cont.)
• Passive ROM– Cervical spine
• Do not perform if motor and sensory deficits are present
• Normal end feel—tissue stretch – Thoracic is seldom performed
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
ROM (cont.)ROM (cont.)
• Resisted ROM– Cervical spine
• Stabilize the hip and trunk to avoid muscle substitution
• Patient seated; one hand stabilizes the shoulder or thorax while other hand applies manual overpressure
– Thoracic region• Weight of the trunk will stabilize the hips

Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Stress and Functional TestsStress and Functional Tests
• Brachial plexus traction
Cervical Spine TestsCervical Spine Tests

Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Cervical Spine Tests (cont.)Cervical Spine Tests (cont.)• Brachial plexus tension test
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
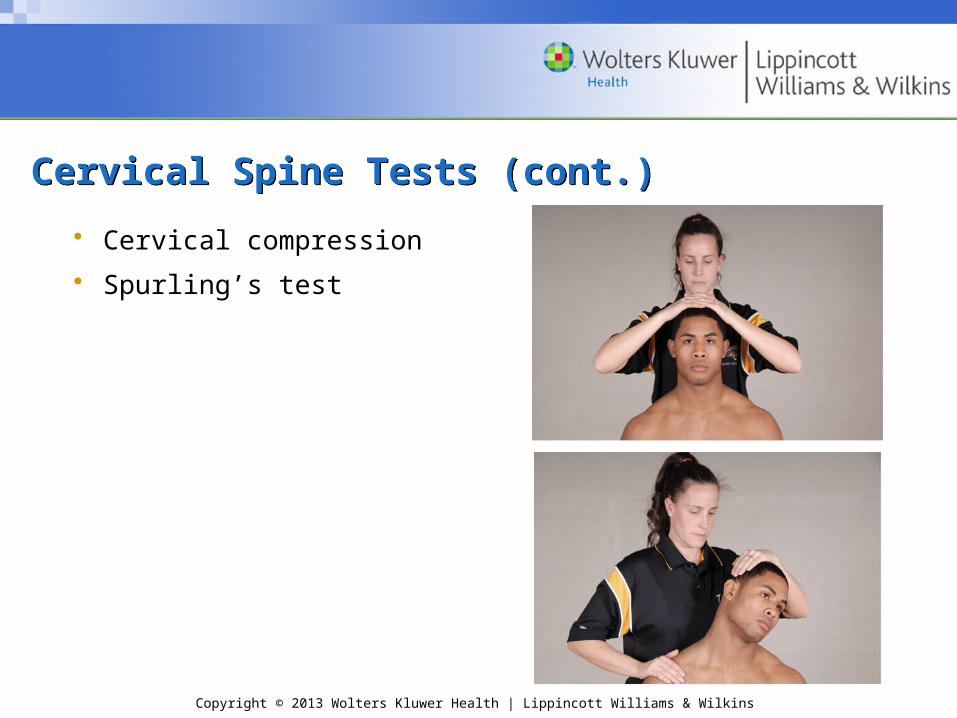
Cervical Spine Tests (cont.)Cervical Spine Tests (cont.)
• Cervical compression
• Spurling’s test

Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Cervical Spine Tests (cont.)Cervical Spine Tests (cont.)• Cervical distraction
• Shoulder abduction

Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Facet Joint MobilityFacet Joint Mobility
• Spring Test

Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Nerve Root ImpingementNerve Root Impingement
• Valsalva Test
• First thoracic nerve root stretch

Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Neurologic TestsNeurologic Tests
• Oppenheim
• Babinski
• Hoffman
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
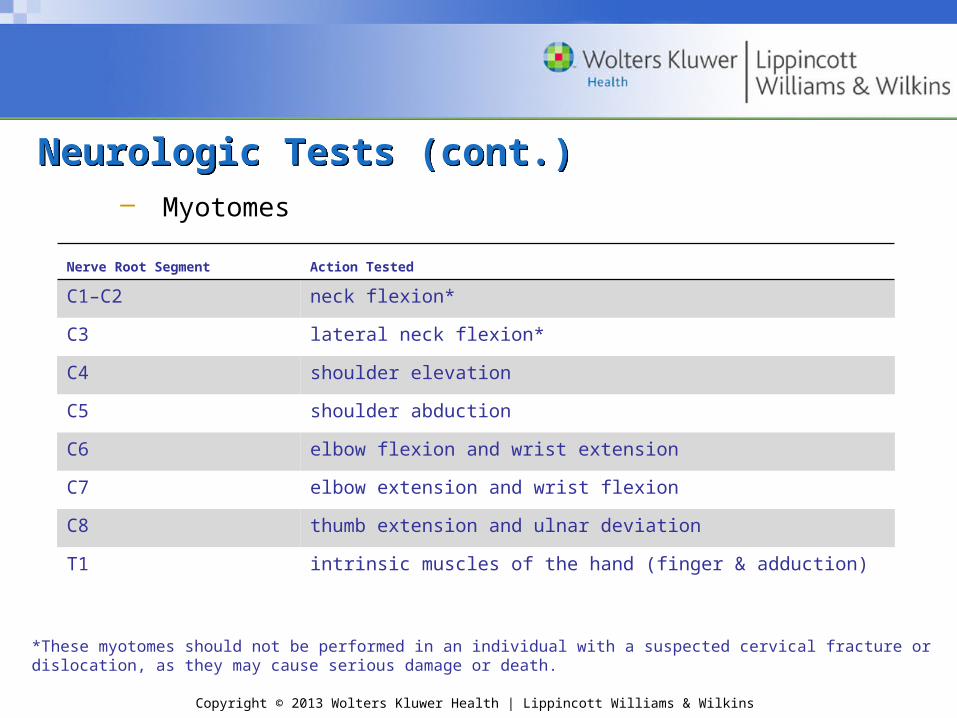
Neurologic Tests (cont.)Neurologic Tests (cont.)– Myotomes
Nerve Root Segment Action Tested
C1–C2 neck flexion*
C3 lateral neck flexion*
C4 shoulder elevation
C5 shoulder abduction
C6 elbow flexion and wrist extension
C7 elbow extension and wrist flexion
C8 thumb extension and ulnar deviation
T1 intrinsic muscles of the hand (finger & adduction)
*These myotomes should not be performed in an individual with a suspected cervical fracture or dislocation, as they may cause serious damage or death.

Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Neurologic Tests (cont.)Neurologic Tests (cont.)
– Reflexes
Reflex Segmental Levels
Biceps C5, C6
Brachioradialis C5, C6
Triceps C7, C8

Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Neurologic Tests (cont.)Neurologic Tests (cont.)
• Cutaneous patterns
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
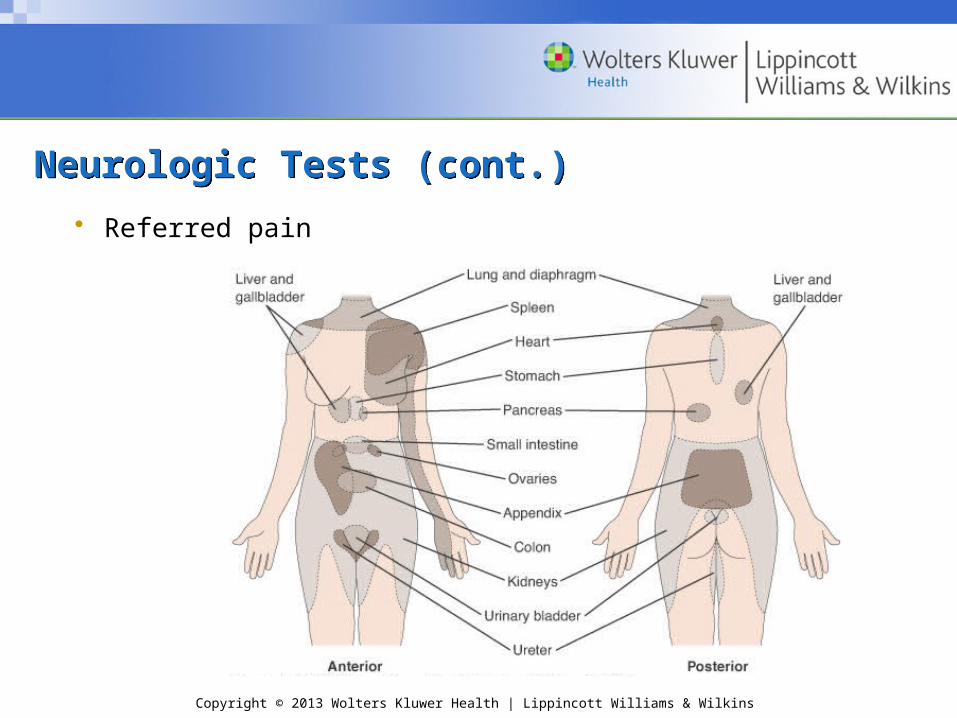
Neurologic Tests (cont.)Neurologic Tests (cont.)
• Referred pain

Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
Activity-Specific Functional TestingActivity-Specific Functional Testing
• Normal parameters
• Pain free and unlimited movement
Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
RehabilitationRehabilitation
• Relief of Pain and Muscle Tension
• Restoration of motion
• Restoration of Proprioception and Balance
• Muscular strength and endurance
• Cardiovascular fitness