core competencies for psychiatric practice what clinicians need to know
TRANSCRIPT


Core Competencies for Psychiatric Practice
What Clinicians Need to Know
A Report of the American Board of Psychiatry and Neurology, Inc.

This page intentionally left blank

Washington, DCLondon, England
Core Competencies for Psychiatric Practice
What Clinicians Need to Know
A Report of the American Board of Psychiatry and Neurology, Inc.
Edited by
Stephen C. Scheiber, M.D.
Thomas A. M. Kramer, M.D.
Susan E. Adamowski, Ed.D.

Note: The authors have worked to ensure that all information in this book is ac-curate at the time of publication and consistent with general psychiatric and med-ical standards, and that information concerning drug dosages, schedules, androutes of administration is accurate at the time of publication and consistent withstandards set by the U. S. Food and Drug Administration and the general medicalcommunity. As medical research and practice continue to advance, however,therapeutic standards may change. Moreover, specific situations may require aspecific therapeutic response not included in this book. For these reasons and be-cause human and mechanical errors sometimes occur, we recommend that read-ers follow the advice of physicians directly involved in their care or the care of amember of their family.
Books published by American Psychiatric Publishing, Inc., represent the viewsand opinions of the individual authors and do not necessarily represent the poli-cies and opinions of APPI or the American Psychiatric Association.
Copyright © 2003 American Board of Psychiatry and Neurology, Inc.ALL RIGHTS RESERVED
Manufactured in the United States of America on acid-free paper07 06 05 5 4 3 2First Edition
Typeset in Adobe’s Berling Roman and Frutiger 55 Roman
American Psychiatric Publishing, Inc.1000 Wilson Blvd.Arlington, VA 22209-3901www.appi.org
Library of Congress Cataloging-in-Publication DataCore competencies for psychiatric practice : what clinicians need to know : a report of the American Board of Psychiatry and Neurology / edited by Stephen C. Scheiber, Thomas A. M. Kramer, Susan E. Adamowski.—1st ed.
p. ; cm.Includes bibliographical references and index.ISBN 1-58562-112-9 (alk. paper)1. Psychiatry. 2. Core competencies. 3. Clinical competence. I. Scheiber,
Stephen C. II. Kramer, Thomas A. M., 1957– III. Adamowski, Susan E., 1944– IV. American Board of Psychiatry and Neurology.
[DNLM: 1. Clinical Competence—standards. 2. Psychiatry—standards. 3. Mental Disorders—therapy. WM 21 C793 2003]RC454.4 .C667 2003616.89′002′1873—dc21
2002027691
British Library Cataloguing in Publication DataA CIP record is available from the British Library.

ContentsContributors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .ix
Foreword . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .xiDavid C. Leach, M.D.
Preface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .xiiiStephen C. Scheiber, M.D., Thomas A. M. Kramer, M.D., and Susan E. Adamowski, Ed.D.
Abbreviations. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . xv
Part IAn Introduction to Core Competencies
1 What Core Competencies Mean to Psychiatrists and Trainees . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3Stephen C. Scheiber, M.D., and Thomas A. M. Kramer, M.D.
2 The Evolving Concept of Clinical Competence in Psychiatric Practice. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Stephen C. Scheiber, M.D., and Thomas A. M. Kramer, M.D.
Part IIOrigins of Core Competencies: Canadian Groundbreaking and American Development
3 Advance Standards: The Canadian Concept of Specialty Competencies as Delineated by Physician Roles . . . . . . . . . . 23Nadia Z. Mikhael, M.D.
4 The ACGME and ABMS Initiatives: Toward the Development of Core Competencies . . . . . . . . . . . . . . . . . . . 43Susan E. Adamowski, Ed.D.

Part IIICore Competencies and the Practice of Psychiatry Today: The ABPN Initiative
5 General and Psychiatry-Specific Patient Care Core Competencies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59Glenn C. Davis, M.D.
6 General and Psychiatry-Specific Medical Knowledge Core Competencies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69Daniel K. Winstead, M.D.
7 Interpersonal and Communications Skills Core Competencies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 79Michael H. Ebert, M.D.
8 Practice-Based Learning and Improvement Core Competencies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 91Larry R. Faulkner, M.D.
9 Professionalism Core Competencies . . . . . . . . . . . . . . . . . . . 103Elizabeth B. Weller, M.D.
10 Systems-Based Practice Core Competencies . . . . . . . . . . . . . 109Pedro Ruiz, M.D.
11 Cross Competencies: What Psychiatrists Should Know About Neurology . . . . . . . . . . . . . . . . . . . . . . . . . . . . 119Glenn C. Davis, M.D., Daniel K. Winstead, M.D., and Thomas A. M. Kramer, M.D.
Part IVThe Impact of Core Competencies
12 Implications of the Core Competencies on ABPN Certification and Maintenance ofCertification for Psychiatric Practitioners . . . . . . . . . . . . . . . 125Stephen C. Scheiber, M.D., and Susan E. Adamowski, Ed.D.
13 Implications of the Core Competencies on the Full Spectrum of Psychiatric Medical Education for Clinical Psychiatric Practice: From Medical School Through Continuing Medical Education . . . . . . . . . . . . . . . 133Thomas A. M. Kramer, M.D.

14 A Forward View: Core Competencies in Future Psychiatric Practice. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 139Stephen C. Scheiber, M.D., and Thomas A. M. Kramer, M.D.
Appendix A: Psychiatry Quadrad Core Competencies Outline . . . . . . . . . . . . . . . . . . . . . . . . . 143
Index . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 153

This page intentionally left blank

ix
ContributorsSusan E. Adamowski, Ed.D.Director, New Assessment Initiatives, American Board of Psychiatry andNeurology, Inc., Deerfield, Illinois
Glenn C. Davis, M.D.Dean, College of Human Medicine, Michigan State University, East Lan-sing, Michigan
Michael H. Ebert, M.D.Professor and Chair, Department of Psychiatry, Vanderbilt UniversitySchool of Medicine, Nashville, Tennessee
Larry R. Faulkner, M.D.Vice President for Medical Affairs and Dean, University of South Caro-lina School of Medicine, Columbia, South Carolina
Thomas A. M. Kramer, M.D.Director, Student Counseling and Resource Service, The University ofChicago, Chicago, Illinois
David C. Leach, M.D.Executive Director, Accreditation Council for Graduate Medical Educa-tion, Chicago, Illinois
Nadia Z. Mikhael, M.D.Director of Education, Royal College of Physicians and Surgeons of Can-ada, Ottawa, Ontario, Canada

x Core Competencies for Psychiatric Practice
Pedro Ruiz, M.D.Professor and Vice Chair, Department of Psychiatry and BehavioralSciences, The University of Texas Medical School at Houston, Houston,Texas
Stephen C. Scheiber, M.D.Clinical Professor of Psychiatry, Northwestern University Medical School,Evanston, Illinois; Clinical Professor of Psychiatry, Medical College ofWisconsin, Milwaukee, Wisconsin; Executive Vice President, AmericanBoard of Psychiatry and Neurology, Inc., Deerfield, Illinois
Elizabeth B. Weller, M.D.Professor of Psychiatry and Pediatrics, University of Pennsylvania, Chil-dren’s Hospital of Philadelphia, Philadelphia, Pennsylvania
Daniel K. Winstead, M.D.Heath Professor and Chair, Department of Psychiatry and Neurology,Tulane University School of Medicine, New Orleans, Louisiana
xi
Foreword
David C. Leach, M.D.
Success follows those adept at preserving the substance of thepast by clothing it in the forms of the future. Preserve sub-stance; modify form; know the difference.
Dee Hock The Birth of the Chaordic Age
The substance of medicine is professional competence demonstratedthrough compassionate care. The Institute of Medicine recognizes thisprinciple in its report Crossing the Quality Chasm: A New Health Systemfor the Twenty-First Century (2000), wherein it proposes 10 simple rulesfor the twenty-first century healthcare system. The first of these rules isthis: Care is based on continuous healing relationships. For us physicians,the delivery of competent patient care to enable healing is the essence ofour professional responsibility. Continuity of that care depends to a largeextent on our ability to maintain compassionate relationships with ourpatients. Preserving this substance is the mission of medical education.
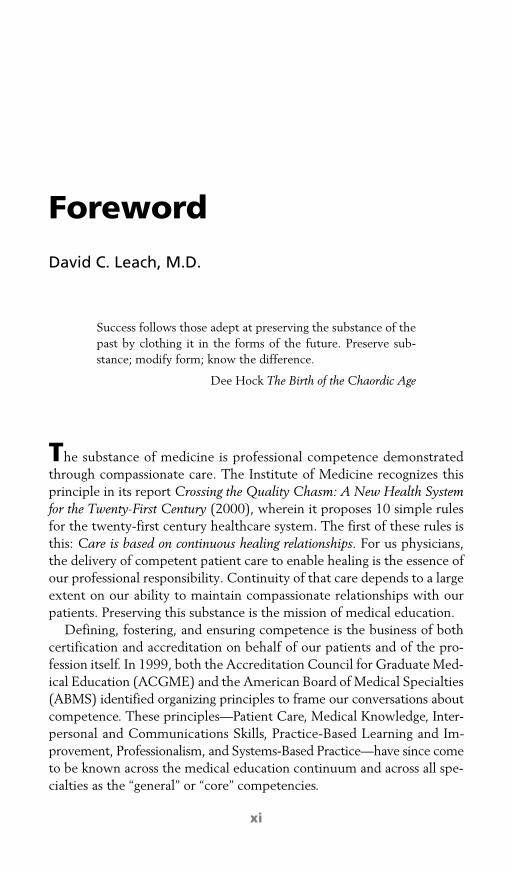
Defining, fostering, and ensuring competence is the business of bothcertification and accreditation on behalf of our patients and of the pro-fession itself. In 1999, both the Accreditation Council for Graduate Med-ical Education (ACGME) and the American Board of Medical Specialties(ABMS) identified organizing principles to frame our conversations aboutcompetence. These principles—Patient Care, Medical Knowledge, Inter-personal and Communications Skills, Practice-Based Learning and Im-provement, Professionalism, and Systems-Based Practice—have since cometo be known across the medical education continuum and across all spe-cialties as the “general” or “core” competencies.

xii Core Competencies for Psychiatric Practice
The recent report of the Commonwealth Fund, Training Tomorrow’sDoctors: The Medical Education Mission of Academic Health Centers(2002), recommends that “accrediting agencies and medical professionalorganizations . . . take a leadership role in assisting [academic health cen-ters] to develop the needs and methods to train physicians to be lifelonglearners and should develop new capabilities to measure the . . . qualityof the medical education mission.” Both the ACGME and ABMS arecurrently engaged in identifying and developing assessment methods andtools for the competencies. We believe that this approach to the form ofmedical education—namely, focusing on how residents and practicingphysicians demonstrate the competencies—ultimately will contribute topreserving the substance of medicine.
Nothing less than the quality of the medical education mission and, ul-timately, of excellent patient care is at stake. This volume and the corecompetencies outlined herein provide evidence that the community ofpsychiatrists rises to this challenge.
References
Commonwealth Fund: Training Tomorrow’s Doctors: The Medical EducationMission of Academic Health Centers. New York, Commonwealth Fund,2002
Institute of Medicine: Crossing the Quality Chasm: A New Health System for theTwenty-First Century. Washington, DC, National Academy Press, 2000

xiii
Preface
Stephen C. Scheiber, M.D.Thomas A. M. Kramer, M.D.Susan E. Adamowski, Ed.D.
This book reports on the psychiatric core competencies as they were dis-cussed at the Invitational Core Competencies Conference sponsored bythe American Board of Psychiatry and Neurology, Inc. (ABPN) in June2001. It attempts to document for the field of psychiatry what was dis-cussed at that time in order to follow future evolutions of the core com-petencies. As the ABPN is the only certification board that representstwo primary specialties, we thought it appropriate to write a comparablebook on core competencies for the field of neurology. This “sister publi-cation” contains essentially the same material on the history of the corecompetency movement and on predictions for the future, but the pri-mary content section of each book will relate directly to the specialty athand.
It is important to note that whatever is written about core competen-cies is current as of its writing but that, just as knowledge changes andgrows, the listing of core competencies is in constant evolution. For thepurposes of training, evaluation, and certification, particular core compe-tencies need to be agreed on, but core competencies as a concept have tobe fluid.
During the time of the writing of this book, the core competenciesoutline has undergone many refinements— each after much thought anddiscussion. This process is expected to continue but to become more at-tenuated.

xiv Core Competencies for Psychiatric Practice
Acknowledgments
Just as core competencies are not defined or assessed by any one organi-zation or agency, the authors of this book realize that this book is the re-sult of collaborative efforts of many individuals. As this book is primarilya report of the work of the ABPN-sponsored Invitational Core Compe-tencies Conference held in June 2001, primary appreciation is due allthose who attended the conference.
Chief among those to be acknowledged for their contributions to thisbook is Dr. Nadia Z. Mikhael, the Director of Education of the RoyalCollege of Physicians and Surgeons of Canada. Dr. Mikhael served as theconference keynote speaker and a member of the reactor panel at the endof the conference. Dr. Mikhael also contributed Chapter 3 to this vol-ume. In this chapter, she summarizes her keynote speech, outlines theCanMEDS 2000 Report, and provides a basic conceptual framework fororganizing physician competencies.
The authors also acknowledge the others who participated in the corecompetencies conference, especially Stanley Fahn, M.D., President of theAmerican Academy of Neurology; Melvyn Haas, M.D., Associate Di-rector for Medical Affairs, Substance Abuse and Medical ServicesAdministration; David Leach, M.D., Executive Director, AccreditationCouncil for Graduate Medical Education (ACGME); and David Nahr-wold, M.D., then President-Elect of the American Board of MedicalSpecialties (ABMS)—all of whom served, along with Dr. Mikhael, asmembers of a reactor panel at the end of the conference.
All of the conference participants are thanked for their enthusiasm forthinking “out of the box” and for their insightful comments regarding thedeveloping concept of core competencies.
The authors also owe a debt of gratitude to the many who contributedto and supported the beginning work on core competencies through theACGME and the ABMS. Special thanks go to the writers of the psychia-try quadrad outline.
The authors would also like to acknowledge the contributions andsupport of all the directors of the ABPN, without whom none of ourwork would be possible.
Last, but certainly not least, the authors wish to thank Shel Cappel-lano and Megan Thiede, the patient administrative assistants who cheer-fully worked through iteration after iteration of this manuscript.
Just as the core competencies are (and will continue to be) the resultof the collaborative efforts of many, this book also represents the thoughts,discussions, and writings of many others. To all of these persons, the au-thors are extremely grateful.

xv
Abbreviations
360-degreeevaluations
Evaluations done by multiple people in a person’s sphere of influence, usually superiors, peers, subordinates, and patients and their families
ABMS American Board of Medical Specialties
ABPN American Board of Psychiatry and Neurology, Inc.
ABPN certificationexamination
Part I Written certification examination
Part II Oral certification examination
ACGME Accreditation Council for Graduate Medical Education
AMA American Medical Association
ANA American Neurological Association
APA American Psychiatric Association
CanMEDS 2000Report
Skills for the New Millennium: Report of the Societal Needs Working Group—The CanMEDS 2000 Project
CME continuing medical education
CSA clinical skills assessment
CT computed tomography
D.O. Doctor of Osteopathy
DSM Diagnostic and Statistical Manual of Mental Disorders
ECFMG Educational Commission for Foreign Medical Graduates
ECT electroconvulsive therapy
Ed.D. Doctor of Education

xvi Core Competencies for Psychiatric Practice
FITER Final In-Training Evaluation Report
ICU intensive care unit
IMG international medical graduate
M.D. Doctor of Medicine
MCQ multiple choice question
MOC Maintenance of Certification
MRI magnetic resonance imaging
MRS magnetic resonance spectroscopy
MRV magnetic resonance venography
NBME National Board of Medical Examiners
OSCE objective-structured clinical examination
PET positron emission tomography
PSM phenomenology, diagnosis, and management of a competency
Royal College Royal College of Physicians and Surgeons of Canada
SAQ short-answer questions
SPECT single photon emission computed tomography

1
Part I
An Introduction to Core Competencies
The term core competencies is self-explanatory: core competencies arethose skills and abilities that are central to, or “at the core” of, a givenfield. In a medical specialty, core competencies represent what physicianspecialists should be able to do in order to be considered minimally com-petent in their fields. By their very nature, core competencies are nonne-gotiable.
Core competencies grew out of the focus on educational outcomesspearheaded by the U.S. Department of Education in the 1980s. The de-partment mandated outcome measures for all educational projects, in-cluding those involving accreditation. Heavily funded medical educationsystems were a prime target of this initiative and were called on to pro-vide evidence of responsible stewardship in preparing competent physi-cians to meet public healthcare needs.
From the 1980s to the present time, the interest in assessing compe-tence has increased, and medical leaders clearly understand that unlessthey begin a comprehensive assessment of their own field, an outsideagency is likely to conduct the assessment for them. Pressure from insur-ance carriers and other third parties has also intensified the effort to de-termine medical competence according to an objective standard.

2 An Introduction to Core Competencies
Efforts in the United States to determine the core competencies of med-ical specialty fields have been led by the Accreditation Council for Grad-uate Medical Education and the American Board of Medical Specialties.Their efforts will have an impact on medical residents and medical spe-cialists in all fields.
This book is an attempt to explain what is happening in the field withpsychiatry core competencies and how the competencies will affect psy-chiatry residents and practicing psychiatrists. Chapter 1 of this partspeaks directly to that issue, underscoring the fact that both educationaland practice arenas are changing rapidly. Chapter 2 provides a historicalcontext for the core competencies by tracing the evolving concept ofmedical competence in psychiatry practice from the beginning of themovement of specialty education in the late 1920s and early 1930s to thepresent.
Medical competence is not a new concept, but its current iteration inthe form of core competencies will change both medical education andmedical practice. It is imperative that those who work as and with psy-chiatrists understand core competencies in their broadest context andtheir most narrow application.

3
Chapter 1
What Core Competencies Mean to Psychiatrists and Trainees
Stephen C. Scheiber, M.D.Thomas A. M. Kramer, M.D.
The practice of medicine has changed dramatically in the last few de-cades. Not only have medical advances altered patient care, but the societalframework of which medical care is a part has changed drastically. Alongwith the growth in the sheer quantity of medical knowledge has been thepopularization of that knowledge through a variety of sources. Medicaltelevision programs have always been popular. Television has more recentlyprovided behind-the-scenes looks at physicians as real people and notmedical gods.
Patients today are more aware of health and healthcare issues thantheir parents and grandparents were. They are more likely to ask theirphysicians perceptive questions after having read about medical topicsand procedures in the popular press and on the Internet. Patients demandmore of their physicians today. No longer are physicians revered. Today’sphysician is no longer the total decision-maker when it comes to medicalissues. He or she is often seen as the primary expert in terms of medicalknowledge, but also as a partner with the patient and the patient’s familyin making healthcare decisions.
With the growth of medical knowledge and the increasing astutenessof patients, demands for specialty medical services have escalated. Insur-ance companies and other third-party payers have not been pleased with

4 An Introduction to Core Competencies
this. To stem the rising tide of insurance claims, managed care companiesare making healthcare decisions, often serving as gatekeepers for those invarious insurance programs. Decisions made in the managed care officeoften determine what medical care a patient will ultimately receive. Notonly do managed care companies determine the type and level of care forwhich insurance will pay, but they often determine who can deliver thatcare. Very often physicians who are not board certified are dismissed asbeing inadequate providers of care. Today more than ever, medical cre-dentials, and not just the medical degree, determine how busy a physicianis and what his or her income will be.
These changes in the medical care scene could be positive. Patientsshould be receiving the best care available, according to their needs, from themost qualified physicians. In practice, this is not always the case. Whatcan be said with assurance, however, is that physicians today are beingheld more accountable than ever for their knowledge, skills, and atti-tudes. Medical competence, once assumed because a physician had anM.D. or a D.O. after his or her name, has been called into question.
Competence is not an all-or-nothing proposition. Competence is mea-sured along a sliding scale through demonstrated knowledge and per-formed tasks. Competence is assessed by degrees. The measuring ofmedical competence has been a difficult activity. Just how much and ex-actly what must a physician know and be able to do to be judged “com-petent”?
Different groups have tackled these questions and listed the knowl-edge, skills, and attitudes that must be demonstrated by physicians todemonstrate competence. These groups include
• American Board of Medical Specialties (ABMS) Task Force on Com-petence
• Accreditation Council for Graduate Medical Education (ACGME)Outcome Project Advisory Group
• Association of American Medical Colleges’ Medical School ObjectivesProject Group
• Federated Council for Internal Medicine Task Force on the InternalMedicine Residency Curriculum
• National Association for Competency Assurance• The Pew Health Professions Commission
Various groups have recently gotten together to agree on categories ofcore competencies. Core competencies are just what their name implies.They are “competencies” or abilities that are “core” or central to medicalpractice. Core competencies are nonnegotiable. Some core competencies

What Core Competencies Mean to Psychiatrists 5
are essentially uniform across specialties and subspecialties; others are, bynecessity, specialty specific.
This book lays out in some detail what the core competencies mightbe for the field of psychiatry, how they came into being, and, most im-portantly, how they might affect practicing psychiatrists and those whohope to become such. The first part of the book sets the stage for the cur-rent concept of physician “competence” by explaining the logic of the de-velopment of the current thought. Part II provides two different views ofhow to look at core competencies: what the leaders in Canada have doneand, based on some of their work, what is currently being done in theUnited States.
Part III discusses specific core competencies as currently delineated forpsychiatrists across the six core competency categories agreed on by theACGME and the ABMS. These categories include Patient Care, MedicalKnowledge, Interpersonal and Communications Skills, Practice-BasedLearning and Improvement, Professionalism, and Systems-Based Prac-tice. Part III also includes discussions of when in a physician’s career thesecompetencies should be assessed and what methodologies would be ap-propriate for that assessment. Throughout this portion of the book, it willbe clear that core competencies are “living entities”; they will constantlybe in development and under refinement. These development and refine-ment processes will not be the purview of any one organization or agency,but rather will reflect the input of medical school faculty, residency train-ing directors, practitioners in the field, individual specialty boards, spe-cialty societies, the ACGME, the ABMS, and others with an interest inthe field.
Part IV concludes the book by discussing how the psychiatry corecompetencies are changing board certification and recertification. Thisportion also addresses changes that medical school faculty and residencytraining directors will likely have to make and discusses how practicingpsychiatrists will likely have to change behaviors to maintain their boardcertification.

This page intentionally left blank

7
Chapter 2
The Evolving Concept of Clinical Competence in Psychiatric Practice
Stephen C. Scheiber, M.D.Thomas A. M. Kramer, M.D.
Today, with the American Board of Medical Specialties (ABMS) servingas the umbrella organization of 24 separate specialty boards, one hears ofmedical competence discussed in terms of certification, recertification,and, most recently, maintenance of certification. It is helpful to rememberthat these aspects of competence—becoming certified initially, gettingcertified again or repeatedly, and continuously maintaining certification—are evolving views of the same basic idea—namely, that medical special-ists should be held to certain educational and performance standards inorder to practice their specialties.
The practice of medical specialties can be documented to before thetwentieth century, but it was not until the late 1920s and early 1930s thatthe specialty movement gained real momentum in the United States. Thescientific and technical advances behind the growth in the movementbrought attendant increases in specialized medical knowledge. In addition,independent departments of psychiatry were beginning to be formed inmedical schools, which were greatly expanded after World War II. Aspart of the independent departments, there was an increasing emphasison research and how it applied to the expanding knowledge base for thespecialties. This led to greater differentiation among the specialties. De-veloping urban areas also provided concentrations of people who could

8 An Introduction to Core Competencies
support medical specialists. Perhaps the greatest impetus to the develop-ment of psychiatry as a separate medical specialty was the formation ofthe National Institute of Mental Health as part of the National Institutesof Health following World War II.
The issue for psychiatrists and neurologists, as well as for all other med-ical specialists, was to gain public recognition for their specialties. Thisrecognition was based on both altruistic reasons and professional survival.The patient, or in aggregate “the public,” deserved the best medical carepossible. Providing such care is the undeniable altruistic aim of all medi-cal practitioners, including medical specialists.
Specialists, however, sensed that both professional and financial gainscould be achieved if their professions were regulated from within. It wouldbenefit the competent, well-trained specialists to have themselves iden-tified as such and keep those with lesser capabilities outside their medicalspecialty field. Thus, specialty boards began organizing formally: theAmerican Board of Ophthalmology in 1916, the American Board of Oto-laryngology in 1924, the American Board of Obstetrics and Gynecologyin 1930, and the forerunner of today’s American Board of Dermatologyin 1930.
Formation of the American Board of Psychiatry and Neurology
Adolf Meyer, M.D., first called for educational standards within the fieldof psychiatry in his presidential address to the American Psychiatric As-sociation (APA) in 1928 (Meyer 1928). Meyer’s voice was joined by oth-ers over the years. The impetus for increased zeal to form a certificationbody was fueled by both professional and practical concerns. There wasa desire for professional recognition of the specialties, but there was alsogrowing concern that if the professions did not regulate themselves fromwithin, external agencies would step in to handle that task. There was gen-eralized concern that the American Medical Association (AMA), the statemedical societies, the National Board of Medical Examiners (NBME), orsome combination of these groups would define competence in psychia-try. J. V. May, M.D., in his presidential address to the APA in 1933,stated:
It will at least be conceded, I think, that if we are to maintain a positionof supremacy in our own field, we must establish standards fully equiva-lent to those already erected by the surgeons, internists, ophthalmologists,otolaryngologists, obstetricians and gynecologists, dermatologists, and pe-diatrists. (May 1933, p. 14)

The Evolving Concept of Clinical Competence 9
In June 1933, the Section on Nervous and Mental Diseases of theAMA resolved that it would cooperate with the APA and other con-cerned national organizations in forming a certification board to certifycompetence in the practice of psychiatry. Representatives of the Ameri-can Neurological Association were invited to join with representatives ofthe AMA and the APA to discuss the formation of a joint certificationboard. “The inclusion of neurology was in keeping with the stand takenby the Council on Medical Education and Hospitals of the AMA, a standthat favored a single board when fields overlap to the extent that neurol-ogy and psychiatry overlap” (Hollender 1991b, p. 4). Ground rules wereagreed on at this first meeting that are still basically in effect today. Theserules had to do with representation on the board, separate qualificationsbeing required for each specialty, and the fact that a candidate whowished to be certified in both specialties had to demonstrate high profi-ciency in both areas.
The second meeting of the combined group on April 14, 1934, withAdolf Meyer, M.D., presiding, yielded agreement on the outline of pre-requisites for examination and certification. These prerequisites includedthat all prospective candidates should 1) be graduates of approved med-ical schools and possess a license to practice medicine, 2) have served ageneral internship, 3) be recognized as ethical practitioners in their com-munities, and 4) be members of the AMA (with exceptions made for Ca-nadians). Experiential prerequisites varied by specialty.
In 1934, Regulations for the Guidance of the Board of Certification inPsychiatry and Neurology in Establishing the Requirement for Such Certifi-cates discussed separate certifying examinations for psychiatry and neu-rology. The document1 stated that
[t]he examinations both written and practical are proposed to test theability of the candidates to meet the situations to which they might at anytime be subjected. They [the examinations] will be of such a type that noadequately trained individual will fail to pass, and they will be sufficientlysearching so that the specialist in fact may be separated from the specialistin name. They will be held one or more times a year.
The document further stated that
[p]ractical examinations will include the examination of patients underthe supervision of an examiner, the identification of specimens in the lab-oratory of anatomy and pathology and the interpretation of roentgeno-
1The full document can be found in Hollender 1991b.

10 An Introduction to Core Competencies
grams, but will not require the performance of diagnostic tests properlyin the field of laboratory medicine. The manner of examining both neu-rological and psychiatric cases and the reasoning and deductions there-from constitute the most important part of the whole examination.
Of the first organizational meeting of the board being held on October20, 1934, with Adolf Meyer, M.D., as chairman, it can be said that thefirst official core competencies for certification in psychiatry and neurol-ogy became operationalized. The board offered three types of certifica-tion: in psychiatry, in neurology, or in both. Physicians desiring to be“double-boarded” had to meet the requirements for and pass the exami-nation in both specialties. The first certification examination was admin-istered in Philadelphia on June 7, 1935.
Although psychiatry and neurology were to be seen as distinct special-ties, all candidates took the same examination from 1935 through 1946.The difference between the two specialties was evidenced by differentscoring standards. These scoring differences came to be known as the“major” and the “minor” examinations. Physicians seeking “double-board-ing” had to meet the requirements for major examinations in bothspecialties.
From its inception, the American Board of Psychiatry and Neurology(ABPN) focused almost exclusively on the development and adminis-tration of certifying examinations to denote competence within the spe-cialties of psychiatry and neurology. Part of the issue of competenceinvolved setting standards to determine who would be allowed to take thecertification examination. Qualifications for examination eligibility inthe early days of the exam included graduation from medical school and1 year of internship training, plus specialty training and clinical experi-ence for specified amounts of time. The board also attempted to establishethical and professional standards of conduct as examination prerequi-sites, but these proved to be unworkable. Thus, early board certificationcommunicated to the public that the successful candidate had fulfillededucational and experiential requirements and had passed an examina-tion, but it was essentially silent on issues of ethics and professional con-duct.
Issues of Being a Dual Board
Certification within a dual board raises many questions. One of the mainreasons that psychiatry and neurology formed one board for certificationpurposes had to do with the politics of the time. The AMA Council onMedical Education and Hospitals and the Advisory Board of Medical

The Evolving Concept of Clinical Competence 11
Specialties (the forerunner of the ABMS) encouraged complementaryspecialties to unite as one board simply to stem the proliferation ofboards. Such unification was done, for example, with obstetrics and gyn-ecology, which formed one board in 1930, and with dermatology andsyphilology, which formed one board in 1932. When differences be-tween two areas could not be overcome, two separate boards were cre-ated. This was the case with the formation of the American Board ofOphthalmology in 1916 and the American Board of Otolaryngology in1924.
Besides the push of politics to incorporate as one board, the practicalmatter of the number of neurologists had to be considered. “At the time ofthe inception of the ABPN, there were not enough neurologists to justifythe establishment of an examining board in neurology” (F.M. Forster, M.D.,personal correspondence to M. Hollender, M.D., 1960). Thus, for both po-litical and practical reasons, the medical fields of psychiatry and neurologydecided to unite under one board. In December 1933, egalitarian mindsprevailed in deciding, despite the preponderance in terms of numbers ofpsychiatrists over neurologists, that there should be equal representation ofboth specialties on the board. At the same time, however, decisions weremade that qualifications, examinations, and certifications would be separatefor the two medical specialties. Those wishing to be certified in both spe-cialties would have to qualify for both examinations. While the board didencourage dual certification, no concessions were made in reducing thenumber of years of education and experience in each field to make this amore manageable accomplishment. In addition, physicians desiring double-boarding had to achieve qualifying scores for the major areas in each exam;there was no major-minor difference for these candidates.
Through the years, there have been many points of contention betweenpsychiatrists and neurologists, even over such things as the name of theboard. The neurologists claimed the name should have been the Ameri-can Board of Neurology and Psychiatry, with the names of the two spe-cialties in alphabetical order. The psychiatrists claimed that their greaternumbers should give their specialty first berth in the board’s name. In theend, the psychiatrists prevailed, and the American Board of Psychiatryand Neurology was incorporated in 1934.
The primary work of the ABPN has been and continues to be to estab-lish standards of competence for the medical fields of psychiatry and neu-rology. In the ensuing years, changes in the qualifications for and natureof the examinations separated the two fields even more than they hadbeen separated initially. This separation can be documented by studyingchanges in the Information for Applicants booklets, which were revised al-most annually over the years.

12 An Introduction to Core Competencies
The earliest available Information for Applicants booklet is the fourthedition, from 1939.2 The fourth edition of the booklet stated that theABPN was created “in response to a widespread desire among specialistsin psychiatry and neurology for some means of distinguishing the fullyqualified specialist from the would-be specialist of inferior training andinadequate training.” This statement was later emended to read, “This ac-tion [of creating the ABPN] was taken as a method of identifying thequalified specialists in Psychiatry and Neurology” (quoted in Hollender1991b, p. 29). In every edition of the Information for Applicants booklet,it was stressed that the main goal of the ABPN was to separate the com-petent from the incompetent in the practice of psychiatry and neurology.
The fourth edition of the Information for Applicants booklet describedin some detail how competence was judged:
The same examination is given whether a candidate applies for certifica-tion in psychiatry or in neurology or in both psychiatry and neurology.The Board requires some proficiency in neurology on the part of those itcertifies in psychiatry and vice versa, but judges the candidate in accor-dance with the certificate he seeks. (quoted in Hollender 1991b, p. 30)
It is interesting to note that the early certification examinations werealmost entirely oral. According to the 1939 Information for Applicantsbooklet, in addition to identification and discussion of the functions ofthe more important anatomic structures of the brain and spinal cord, dis-cussion of gross and microscopic pathologic specimens, and interpreta-tion of roentgenograms dealing with neurological disorders, 2 hours weredevoted to an oral examination on the subjects of psychobiology and psy-chopathology. The candidate was also required to examine four patients,two with neurological disorders and two with psychiatric disorders, andto discuss his or her findings with the examiners. The Information forApplicants booklet clearly stated that the patient examinations, each ofwhich lasted about an hour, were the most important parts of the exam-ination. In addition, the 1939 edition states that “some acquaintance withthe history of psychiatry and neurology, with the body of the doctrine,and with recent advances is presupposed.” These areas of knowledgewere also addressed on the oral examination.
Not all practicing psychiatrists and neurologists of the time wererequired to take the certification examination to demonstrate their com-
2Unfortunately, the early editions of the booklet (the first three editions) are notavailable.

The Evolving Concept of Clinical Competence 13
petence. Some more senior members of the professions were “grand-fathered” into certification. To be considered for grandfathering, a candidatehad to have graduated from medical school in or before 1919, have spe-cialized in neurology and/or psychiatry for at least 15 years, and havemaintained a satisfactory professional record.
The first cohort of examinees sat for the certification examination atPhiladelphia General Hospital on June 7, 1935. Of the 31 candidates, 21passed the examination (10 in psychiatry alone, 2 in neurology alone, and9 in both psychiatry and neurology). Essay-type questions piloted withthis examination were judged unsuccessful and thus eliminated.
The ABPN certification examination continued in the above formatuntil 1946. The only notable change was the introduction of true-falsequestions in 1943, but like the earlier essay questions, these were deemedunsatisfactory.
Changes in the 1946 examination highlighted changes in the certifica-tion process that have continued and increased during the years. Not onlywere separate examinations for psychiatry and neurology given in 1946,but the emphasis in each exam shifted. Previously, the joint examinationhad devoted approximately 3 hours each to psychiatry and to neurology.In 1946, the emphasis was shifted to devote 4 hours to the major spe-cialty of the candidate and 2 hours to the minor specialty.
Perhaps even more importantly, the 1946 Information for Applicantsbooklet stressed that competence in dealing with patients, and not justfactual knowledge, was the main objective in the examination process.This emphasis is clearly shown in the expanded section on requirementsfor training as a prerequisite for the examination. The 1946 edition of theInformation for Applicants booklet explicitly stated for the first time:“Oral and practical examinations will be given in the basic sciences withspecial regard to their clinical implications.” This statement was repeatedyear after year. In 1949, a new sentence was added following the state-ment above: “Written examinations may be given at the discretion of theBoard”; in 1966, that statement was amended to read: “Written exami-nations will be given at the discretion of the Board” (emphasis added inboth statements).
Development of the Written Portion of the Certification Examination
In 1949, according to the minutes of a policy meeting, the directors ofthe ABPN also began in earnest to develop a written examination. Eachdirector was to send 10 suitable multiple-choice questions for use in the

14 An Introduction to Core Competencies
development of separate written psychiatry and neurology examinations.Not enough usable questions were received, however, and discussion ofthe creation of a written competency examination occurred at the nextthree policy meetings. Then “the whole idea was dropped because the di-rectors could not agree on the questions, to say nothing of the answers”(Hollender 1991a, p. 32).
The potential written examination was seen alternately as a screeningdevice to deselect unqualified candidates and as a part of the examinationitself. Efforts to create a written examination in each of the medical spe-cialties occurred sporadically during the 1950s and early 1960s. By 1963,the need for a written examination seemed to become a practical neces-sity. A written examination would serve two major purposes: 1) it mighteliminate or at least lessen reliability problems with the oral examina-tions, and 2) it could help to cope with the ever-increasing number ofcandidates seeking to take the examination. Consensus now seemed tofavor using the written examination as a screening tool for admittingqualified candidates to the oral examinations.
Having been unsuccessful in creating a written examination them-selves, the directors of the ABPN turned to the NBME for assistance, andin 1966, the first written examination was given. Initially, it was thoughtthat the written examination could be administered immediately preced-ing the oral examination, but for test security purposes, several differentversions of the examination would be required. These examination ver-sions would require a substantially larger test item pool than was cur-rently available, and so it was decided that the written portion of thecertification examination would be administered separately from the oralexamination and only one time per year. The written examination was in-creased in length from 2 to 3 hours and came to be known as Part I of thetwo-part ABPN certification examination. This written examination wasadministered for the first time in 1967, and only those successful on thisexamination could register for the oral examination. Labeling the writtenexamination as Part I and the oral examination as Part II legitimized theformer as a required part of the certification examination and not merelya screening tool. It continued to provide a screening function, however,in that its successful completion was a prerequisite for the oral (Part II)examination.
From the beginning of the administration of the written examination,the directors of the ABPN took this part of competency testing veryseriously. Instead of merely relying on the NBME to create the writtenexamination, the ABPN recruited practicing specialists to develop ques-tions for their own question pool.
The ABPN Annual Report for 1969 stated that

The Evolving Concept of Clinical Competence 15
[t]he written examination is considered to be essentially a method to de-termine the candidate’s fund of knowledge. The principal purpose of theoral examination is to provide the candidate with the opportunity to ap-ply his knowledge and thereby demonstrate his clinical competence.
Besides being used as a prerequisite for admission to the oral examina-tion, the written examination also prompted changes in the format of theoral examination. Since the written examination could adequately assessthe general knowledge of the basic sciences, the oral examination was re-duced in time and was devoted to the clinical application of basic knowl-edge. Oral examination sections in basic neurology for psychiatrists andin basic psychiatry for neurologists were also eliminated.
For a time, a bridging committee was established to identify basicsciences common to both psychiatry and neurology. After a few years,however, it was determined that two separate committees, one for basicsciences in psychiatry and one for basic sciences in neurology, needed tobe established. These committees focused their efforts on the written ex-aminations.
The written portion of the ABPN certification examination first usedpictorial material in 1970, and this was seen as a major step forward inthe developing sophistication of the examination.
In 1975, the section of the Part I examination that tested both basicpsychiatry and basic neurology, the only common portion of the examina-tion for the two specialties, was replaced by two separate examinations.Thus, the psychiatry and neurology certification examinations could beseen as completely different entities.
Further Evolution of the ABPN Certification Examination
Increasing numbers of candidates to be examined for Part II of the exam-ination called for increasing numbers of patients and examiners and in-creasing numbers of clinical sites for testing. Clearly, a new venue had tobe found to accomplish the same competency testing purposes.
The use of motion pictures for some sessions of patient contact was dis-cussed but never pursued because of the costs involved. When lower-costaudiovisual tapes became available, they were assessed for use in the late1970s. Studies showed a high level of concurrence on the part of the can-didates between the use of live patients and their videotaped counter-parts (Greenblatt 1977, as reported in Hollender 1991a). By the begin-ning of the 1982 examination cycle, the Part II examination in psychiatrycomprised a 1-hour interview of a live patient (including 30 minutes of

16 An Introduction to Core Competencies
discussion about the candidate’s examination of the patient) and a 1-hourvideotaped presentation of a patient (including 30 minutes of discussionof the candidate’s analysis of the videotape). Both the live patient inter-view and its videotaped counterpart were deemed more effective at test-ing complex interpersonal skills than any written examination could be(Small 1980). With the live patient interview, these skills included assess-ing how the candidate related to the patient, how the clinical interviewwas conducted, and how well the candidate was able to organize and pre-sent data in the form of a differential diagnosis and medical treatmentplan. The videotaped portion of the examination focused on the synthe-sis of the data presented, the differential diagnosis, and the formulationof a treatment plan.
At the same time, the neurology oral examination became a 3-hourprocess, with 1 hour devoted to a patient examination and 2 hours de-voted to vignettes.
The ABPN examinations in psychiatry and neurology, which had be-gun as a single examination, were now two completely separate exami-nations. Although each examination tested for competency in bothsubject areas, each focused clearly on its own “major” area. By the 1980s,not only were the examinations completely separate, but the grading ses-sions for them were also separate.
Conclusion
From its inception, the ABPN has been devoted to assessing the compe-tence of psychiatrists and neurologists for the ultimate benefits of the pa-tients they serve. Various testing formats were used over the years. Thesebecame increasingly specialty-specific and matured through evolutionsoften dictated by the number of candidates needing to be served.
The commitment of the ABPN to use the six categories of core compe-tencies adopted by the Accreditation Council for Graduate Medical Edu-cation and the ABMS represents a continued step in the evolution ofsophistication in the measurement of physician competence. This step, likethe many that preceded it, will provide challenges in its implementationbut will ultimately enhance the assessment of physician competence.
References
Greenblatt M: History of Significance of Recent Rulings of the ABPN. Paper pre-sented at the annual meeting of the American Psychiatric Association, Tor-onto, Ontario, Canada, May 2–6, 1977

The Evolving Concept of Clinical Competence 17
Hollender MH: The examination in psychiatry, in The American Board of Psychi-atry and Neurology: The First Fifty Years. Edited by Hollender MH. Deer-field, IL, American Board of Psychiatry and Neurology, 1991a, pp 29–42
Hollender MH: The founding of the ABPN, in The American Board of Psychiatryand Neurology: The First Fifty Years. Edited by Hollender MH. Deerfield,IL, American Board of Psychiatry and Neurology, 1991b, pp 1–14
May JV: The establishment of psychiatric standards by the association. Am J Psy-chiatry 90:1–15, 1933
Meyer A: Presidential address: thirty-five years of psychiatry in the United Statesand our present outlook. Am J Psychiatry 85:1–31, 1928
Small SM: Role of objective examinations in psychiatry, in Comprehensive Text-book of Psychiatry/III, 3rd Edition. Edited by Kaplan HI, Freedman AM,Sadock BJ. Baltimore, MD, Williams & Wilkins, 1980, pp 2974–2975

This page intentionally left blank

19
Part II
Origins of Core Competencies
Canadian Groundbreaking and American Development
As Part I of this book has shown, the concept of medical competencehas evolved over time. Just as with other professions, those who per-formed various professional tasks in the past have found their fields be-coming increasingly regimented. Educational requirements are generallythe first to be applied to a profession, and only much later are practiceparameters established as assessment measures.
A simple example of this involves the profession of school teaching.From the time America was first settled by Europeans until the early1900s, the teacher in each village was generally the one who had learnedto read and to compute and who was not needed for other life-maintain-ing chores on the farm or in the home. These “standards,” such as theywere, sufficed and even worked well. As the general population becameboth more literate and numerate, many more people could have qualifiedto serve as teachers, except for the simple fact that other, generally more

20 Origins of Core Competencies
subsistence-related work was required of them; they were required to tillthe fields or to weave cloth for the family’s clothing.
As farm production methods required fewer workers and industrialmethods reduced backbreaking housekeeping chores, one might haveexpected a market glut of those qualified to serve as their communities’teachers. However, an interesting change came about. Educational stan-dards for teachers were introduced, and only those with a high school di-ploma—and later some college training, and still later, a 2-year collegedegree—were judged to be qualified to teach. During this time in theUnited States, normal or teacher-training colleges abounded in order tokeep pace with the need for more and more teachers as children werefreed from full-time chores to be able to attend school.
Because this system seemed to work well, it became more sophisticated.Longer schooling, the mandatory 4-year college diploma, was required forpublic school teachers. About this same time, teacher training also becamemore specialized. Someone desiring to become a teacher had to decide atthe beginning of training if she or he wanted to teach young children orolder children and then, in the case of the older children, what particularsubjects would be taught. Teacher certification was granted based on thefiling of an appropriate diploma, which came to require a certain minimalamount of coursework in the methods of teaching.
Not until fairly recently have teachers been required to take minimumskills competency tests. These tests focus on acquired knowledge, but noton the ability to communicate that knowledge. If the content was mas-tered and the neophyte teachers survived a period of “practice teaching”with a more senior teacher, that person was judged to be a teacher forever-more.
When these requirements were judged to be insufficient, teacherswere forced to receive successful evaluations from their supervisors fortheir first 2 or 3 years of teaching in order to be granted tenure, or life-time certification. Even with lifetime tenure, some more sophisticatedschool districts have required continuing education credits. These creditshave been generally earned through colleges and universities, and theteachers involved in these programs generally have only had to present agrade report for continued employment and, in many cases, salary ad-vancement. Only very recently has there been talk about higher-level andongoing competency testing, and the focus here is, again, on knowledgeacquisition, not knowledge sharing, which is really what teaching is.
Physicians have run a track parallel with that of the teachers in manyrespects, but as the body of knowledge required of a physician is so muchlarger than that required for an elementary or high school teacher, the re-quirements for physicians have been both more numerous and more

Canadian Groundbreaking and American Development 21
stringent. Increasing demands have been placed on physicians in the ed-ucational arena, and certification requirements for specialized fields inmedicine have been developed.
As with teachers, physician competence has focused more on the ac-quisition of knowledge and less on the skills that demonstrate the im-plementation of that knowledge. With greater consumer awareness andincreasing problems funding medical care through third parties, the com-petence of physicians is under scrutiny in a way that it never before hasbeen. With ever-increasing amounts of specialized medical knowledge—and access to that information—acquired knowledge is almost a given forany board-certified medical specialist. While keeping up to date academ-ically in one’s specialty field is a mark of competence, new standards ofcompetence for physicians have begun to be implemented.
Chapter 3 discusses these standards of physician competence in termsof the roles a physician specialist must play. This concept of physiciancompetence was developed by the Royal College of Physicians and Sur-geons of Canada and includes the seven roles played by each physician:medical expert (or clinical decision-maker), communicator, collaborator,manager, health advocate, scholar, and professional. The premise on whichthis work rests is that while the role of being a medical expert (or clinicaldecision-maker) is central to being a specialist, competence in the othersix roles is essential to success in the primary role.
Chapter 4 discusses how the Accreditation Council for GraduateMedical Education (ACGME) and the American Board of Medical Spe-cialties (ABMS) have approached the subject of competency for physi-cian specialists. The ACGME and ABMS have looked not at the roles aphysician specialist plays, but rather at six broad areas of competencethat must be mastered: Patient Care, Medical Knowledge, Interpersonaland Communications Skills, Practice-Based Learning and Improvement,Professionalism, and Systems-Based Practice. Competencies in each areahave been delineated through a study of medical education and practiceas represented by a member of the area’s specialty board, a representativeof the Residency Review Committee of the ACGME, a residency pro-gram director, and a resident. These six categories of core competenciesare discussed in detail in the chapters of Part III.

This page intentionally left blank

23
Chapter 3
Advance Standards
The Canadian Concept of Specialty Competencies as Delineated by Physician Roles
Nadia Z. Mikhael, M.D.
Some of the earliest work done to delineate the necessary competenciesfor medical specialists was carried out in Canada through the efforts ofthe Royal College of Physicians and Surgeons. As the keynote speaker forthe Invitational Core Competencies Conference sponsored by the Amer-ican Board of Psychiatry and Neurology (ABPN) held in Toronto in June2001, I was pleased to share our pioneering work with my Americanpeers. I assured the American medical leaders gathered for the confer-ence that they were on the right track in listing medical specialty compe-tencies for assessment.
Background of the CanMEDS
The beginning work of the core competencies in Canada is best delin-eated in the CanMEDS 2000 Project Report, a 1996 publication. The fulltitle of the part of the CanMEDS 2000 Project Report that concerns corecompetencies is “Skills for the New Millennium: Report of the SocietalNeeds Working Group.” This report describes our attempt at the RoyalCollege to establish guidelines for optimal specialty medical care throughan analysis of the competencies needed by physicians practicing in differ-

24 Origins of Core Competencies
ent medical specialties.1 The framework for our listing of core competen-cies is divided according to the seven roles played by each physician:medical expert (or clinical decision-maker), communicator, collaborator,manager, health advocate, scholar, and professional.
The premise on which our work rests is that while the role of being a“medical expert” or “clinical decision-maker” is central to being a special-ist, competence in the other six roles is essential to success in the primarycare role. All 16 medical schools in Canada have agreed with this frame-work and are working to make certain that by the end of residency train-ing, all specialists have a grounding in each role plus the background todevelop expertise as needed in their future careers.
In addition, work through the Royal College in the areas of accredita-tion, specialty-specific objectives, and evaluation has incorporated the“role framework” into all aspects of postgraduate medical education.Consequently, in Canada all stages of medical education, from residencythrough professional practice, are operating under the same set of expec-tations—one set of core competencies divided into the tasks of the sevendifferent roles a specialist plays.2
Our CanMEDS 2000 Project began in 1993 as an initiative of theHealth and Public Policy Committee of the Royal College. The overallgoal of this project was to ensure that postgraduate specialty training pro-grams in Canada be fully responsive to societal needs. The main organiz-ing principle of our project was to better meet the specialty medicalneeds of the Canadian public by changing from a supply-side (focusing
1Copies of this report are available from the Royal College of Physicians andSurgeons of Canada, through the Educational Research and Development Unitof the Office of Education, 774 Echo Drive, Ottawa, Ontario, Canada K1S 5N8(telephone: 1-800-668-3740/613-730-6276). The report is also available on theRoyal College Web site (http://rcpsc.medical.org); refer to Publications andDocuments, Special Projects and Reports.2In addition, the Royal College Office of Education is responsible for recognitionof specialties, accreditation of residency programs, credentialing of candidates,all specialty examinations, educational research, and faculty development. Cur-rently, the Royal College recognizes 58 specialties and subspecialties. Each disci-pline has its own Royal College specialty committee. The role of a specialtycommittee is to develop specialty-specific objectives of training and specialtytraining requirements and to develop and update the specific standards ofaccreditation. Each committee is also involved in all matters relating to the disci-pline, including review of accreditation status of programs and specialty-specifictraining requirements.

Advance Standards: The Canadian Concept of Specialty Competencies 25
on the interests of those providing medical education) to a demand-side(focusing on the needs of individual patients in the context of the Cana-dian population at large) orientation.
One component of the CanMEDS 2000 Project was the SocietalNeeds Working Group (SNWG). The charge given to the SNWG was tooutline the objectives and the educational and evaluation strategies forvarious competencies and to make recommendations for their imple-mentation, including how these new program measures would impact ac-creditation of postgraduate programs and the certification of residents.
Framework of Roles That a Physician Plays
Our concept of the delineation of physician competencies according toroles originated with the Educating Future Physicians for Ontario Project(EFPO). The SNWG realized that it had to broaden the Ontario focus ofthe EFPO to consider the medical needs of creating competencies for phy-sician roles that would serve the people of the entire country. Using bothpublished and unpublished literature, including that of consumer surveysand focus groups, the SNWG collected information on general physiciancompetencies and then organized this information into the roles a physi-cian plays. These roles, as listed earlier, are medical expert (or clinicaldecision-maker), communicator, collaborator, manager, health advocate,scholar, and professional, with the medical expert role being key to all.
Different task forces focused on the different roles and defined keycompetencies for each. To implement the role framework of physiciancompetencies, the SNWG broadened our list of the competencies to in-clude specific educational objectives, relevant learning points, effectiveevaluation measures, and pertinent faculty development issues for eachrole. The framework of our CanMEDS 2000 Project is therefore theproduct of many months’ work involving medical education expertsacross Canada. It reflects overlapping clusters of the generic knowledge,attitudes, and skills set required of all specialists while allowing for theunique competencies of our 58 different medical specialties.
Two cohorts of Royal College Fellows and all Canadian specialty pro-gram directors were selected to validate the work of the SNWG. Surveyrespondents were asked to rate each of the competencies from twoperspectives: 1) how important that competency was to their clinicalpractice, and 2) how well they felt they had been prepared for operation-alizing that competency during their training programs. Overall, it ap-peared that new fellows and program directors identified with each ofthe roles listed, but that in certain key areas training was deemed poor.

26 Origins of Core Competencies
Role Delineation for Specialty Physicians
Table 3–1 lists the essential roles and key competencies of specialty phy-sicians identified in the CanMEDS 2000 Project Report. In what follows,I provide a more complete description of each role a physician specialistmust play in order to be deemed competent.
The Role of Medical Expert
The role of medical expert is the central role a physician plays and drawson the competencies of all the other roles. As delineated in the CanMEDS2000 Project Report, as a medical expert, a specialist should be able todemonstrate the following competencies:
• Demonstrate diagnostic and therapeutic skills to effectively and ethicallymanage a spectrum of patient care problems within the boundaries of hisor her specialty. This includes the ability to do the following:
■ Elicit a relevant, concise, and accurate history.■ Conduct an effective physical examination.■ Carry out relevant procedures to collect, analyze, and interpret
data.■ Reach a diagnosis.■ Perform appropriate therapeutic procedures to help resolve a pa-
tient’s problem.
• Access and apply relevant information and therapeutic options to clinicalpractice. This includes the ability to do the following:
■ Pose an appropriate patient-related question.■ Execute a systematic search for evidence.■ Critically evaluate medical literature and other evidence in order to
optimize clinical decision making.
• Demonstrate medical expertise in situations other than in direct patientcare. This includes the ability to do the following:
■ Provide testimony as an expert witness.■ Give presentations.
• Recognize personal limits of expertise. This includes the ability to do thefollowing:
■ Decide if and when other professionals are needed to contribute toa patient’s care.
■ Implement a personal program to maintain and upgrade profes-sional medical competence.

Advance Standards: The Canadian Concept of Specialty Competencies 27
Table 3–1. Essential roles and key competencies of specialty physicians
Roles Key competencies
The physician must be able to:
Medical expert Demonstrate diagnostic and therapeutic skills for ethical and effective patient care.
Access and apply relevant information and therapeutic options to clinical practice.
Demonstrate medical expertise in situations other than in direct patient care.
Recognize personal limits of experience.Demonstrate effective consultation skills (with respect to
patient care, education, and legal opinions).
Communicator Establish therapeutic relationships with patients and their families.
Elicit and synthesize relevant information from patients, their families, and their communities about patients’ problems.
Listen effectively.Discuss appropriate information with patients, their families,
and other healthcare providers to facilitate optimal healthcare of patients.
Collaborator Consult effectively with other physicians and healthcare professionals.
Contribute effectively to other interdisciplinary team activities.
Manager Utilize time and resources effectively to balance patient care, learning needs, outside activities, and personal life.
Allocate finite healthcare and health education resources effectively.
Work effectively and efficiently in a healthcare organization.Utilize information technology effectively to optimize
patient care, continued (lifelong) self-learning, and other activities.
Health advocate Identify the determinants of health that affect patients to effectively contribute to improving individual and societal health.
Recognize and respond to those issues, settings, circum-stances, or situations in which advocacy on behalf of patients, professions, or society is appropriate.
Scholar Develop, implement, and document a personal continuing education strategy.
Critically appraise sources of medical information.Serve as an educator by facilitating the learning of patients,
students, residents, and other health professionals.Contribute to the development of new knowledge.

28 Origins of Core Competencies
• Demonstrate effective consultation skills. This includes the ability to dothe following:
■ Present well-documented patient assessments and recommenda-tions in both verbal and written form in response to a request fromanother health professional.
The Role of Communicator
As a communicator, a specialist must be able to obtain information fromand convey information to patients, their families, and other healthcareprofessionals concerned about the patients. Because obtaining and con-veying such information is essential to ensure humane, high-quality careof patients, the role of communicator is integral to the functioning of amedical expert. As delineated in the CanMEDS 2000 Project Report, as acommunicator, a specialist should be able to demonstrate the followingcompetencies:
• Establish therapeutic relationships with patients. This includes the abilityto do the following:
■ Establish and maintain rapport.■ Foster an environment characterized by understanding, trust, em-
pathy, and confidentiality.
• Elicit and synthesize relevant information from patients, their families,and/or their communities about patients’ problems. This includes theability to do the following:
■ Explore patients’ beliefs, concerns, and expectations about the ori-gin, nature, and management of their illnesses.
■ Assess the impact of factors such as age, gender, ethnocultural back-ground, social support, and emotional influences on patients’ illnesses.
Professional Deliver the highest quality care with integrity, honesty, and compassion.
Exhibit appropriate personal and interpersonal professional behaviors.
Practice medicine in an ethically responsible manner that respects the medical, legal, and professional obligations of belonging to a self-regulating body.
Table 3–1. Essential roles and key competencies of specialty physicians (continued)
Roles Key competencies

Advance Standards: The Canadian Concept of Specialty Competencies 29
• Discuss appropriate information with patients, their families, and otherhealthcare providers to facilitate optimal healthcare of patients. This in-cludes the ability to do the following:
■ Inform and counsel patients in a sensitive and respectful manner.■ Foster understanding, discussion, and patients’ active participation
in decisions about their care.■ Listen to patients.■ Communicate effectively with other healthcare providers to ensure
optimal and consistent care of patients and their families.■ Maintain clear, accurate, and appropriate records.
The Role of Collaborator
A medical expert does not work in isolation; he or she works as a partnerwithin a coordinated team involved in the care of a particular patient orgroup of patients. As a collaborator, a specialist must function well as apart of this team to ensure optimal patient care. Collaboration occurs inhospitals, practice settings, committee work, research, teaching, andlearning. As delineated in the CanMEDS 2000 Project Report, as a collab-orator, a specialist should be able to demonstrate the following compe-tencies:
• Consult effectively with other physicians and healthcare professionals.This includes the ability to do the following:
■ Develop investigations, treatments, and continuing care plans in part-nership with patients and their other healthcare providers.
■ Recognize the limits of personal expertise.■ Understand the roles and expertise of the other members of the
healthcare team.■ Inform and involve patients and their families in decision making.■ Integrate the opinions of patients and their caregivers into manage-
ment plans.
• Contribute effectively to other interdisciplinary team activities. This in-cludes the ability to do the following:
■ Recognize team members’ areas of expertise.■ Respect the opinions and roles of individual team members.■ Contribute to healthy team development and conflict resolution.■ Contribute personal expertise to the team’s tasks.

30 Origins of Core Competencies
The Role of Manager
Managers allocate finite healthcare and other resources in their dailypractice of making decisions about time, staff, tasks, policies, and theirpersonal lives. This role involves the ability to prioritize effectively andassume the role of leader, when necessary, to execute tasks within thehealthcare team. In the role of manager, a medical expert often findshimself or herself as the formal or informal leader of the healthcare team.As delineated in the CanMEDS 2000 Project Report, as a manager, a spe-cialist should be able to demonstrate the following competencies:
• Utilize time and resources effectively in order to balance patient care,learning needs, outside activities, and personal life. This includes the abil-ity to do the following:
■ Employ effective time management and self-assessment skills toformulate realistic expectations and a balanced lifestyle.
• Allocate finite healthcare and health education resources effectively. Thisincludes the ability to do the following:
■ Make sound judgments on resource allocation based on evidence ofthe benefit to individual patients and the population served.
• Work effectively and efficiently in a healthcare organization. This includesthe ability to do the following:
■ Understand the roles and responsibilities of specialists in Canada.■ Understand the organizations and functions of the Canadian health-
care system.■ Understand the forces of change.■ Work effectively within teams of colleagues.■ Manage a medical practice while simultaneously functioning within
broader organizational management systems (e.g., hospital com-mittees).
• Utilize information technology effectively to optimize patient care, contin-ued self-learning, and other activities. This includes the ability to do thefollowing:
■ Use patient-related databases.■ Access computer-based information.■ Understand the fundamentals of medical informatics.
The Role of Health Advocate
A health advocate responds to challenges represented by those social, en-vironmental, and biological factors that determine the health of patients

Advance Standards: The Canadian Concept of Specialty Competencies 31
and society. Advocacy is an essential and fundamental component ofhealth promotion that occurs at the level of the individual patient, thepractice population, and the broader community. As a health advocate,a specialist responds both individually and collectively in influencingpublic health and policy. As delineated in the CanMEDS 2000 Project Re-port, as a health advocate, a specialist should be able to demonstrate thefollowing competencies:
• Identify the determinants of health that affect patients in order to be ableto effectively contribute to improving individual and societal health inCanada. This includes the ability to do the following:
■ Recognize, assess, and respond to the psychosocial, economic, andbiological factors influencing the health of those served.
■ Incorporate information on health determinants into personal prac-tice behaviors, both with individual patients and with their commu-nities.
■ Adapt patient management and education to promote health,enhance understanding, foster coping abilities, and enhance activeparticipation in informed decision making.
• Recognize and respond to those issues, settings, circumstances, or situationsin which advocacy on behalf of patients, professions, or society is appropri-ate. This includes the ability to do the following:
■ Identify populations at risk.■ Identify current policies that affect health.■ Recognize the fundamental role of epidemiologic research in in-
forming practice.■ Describe how public policy is developed.■ Employ methods of influencing the development of health and so-
cial policy.
The Role of Scholar
In the role of scholar, a specialist engages in the lifelong pursuit of mas-tery of his or her domain of professional expertise. Recognizing his or herown need to learn continually, the specialist models lifelong learning forothers. As a scholar, the specialist contributes to the appraisal, collection,and understanding of healthcare knowledge and facilitates the educationof students, patients, and others. As delineated in the CanMEDS 2000Project Report, as a scholar, a specialist should be able to demonstrate thefollowing competencies:

32 Origins of Core Competencies
• Develop, implement, and document a personal continuing education strat-egy. This includes the ability to do the following:
■ Accept responsibility for personal learning needs:
• Assess personal learning needs.• Select appropriate learning methods and materials.• Evaluate the outcome of learning to optimize practice.
• Apply the principles of critical appraisal to sources of medical information.This includes the ability to do the following:
■ Incorporate a spirit of scientific inquiry and use of evidence intoclinical decision making:
• Select appropriate inquiry questions.• Efficiently search for and assess the quality of evidence in litera-
ture.• Keep up-to-date with the evidence-based standard of care for
the conditions most commonly seen in patients.
• Serve as an educator by facilitating the learning of patients, students, resi-dents, and other health professionals. This includes the ability to do thefollowing:
■ Help others define learning needs and directions for development.■ Provide constructive feedback to peers and other learners.■ Apply the principles of adult learning in interactions with patients,
students, residents, colleagues, and others.
• Contribute to the development of new knowledge. This includes the abil-ity to do the following:
■ Possess the skills necessary to participate in collaborative researchprojects, quality assurance, or guideline development relevant tothe practice of a specialist.
The Role of Professional
Medical specialists have unique societal roles as professionals with a dis-tinct body of knowledge, skills, and attitudes relevant to improving thehealth and well-being of others. In the role of professional, the specialistis committed to the highest standards of excellence in clinical care andethical conduct, continually perfecting mastery of his or her medicalspecialty. As delineated in the CanMEDS 2000 Project Report, as a pro-fessional, a specialist should be able to demonstrate the following com-petencies:

Advance Standards: The Canadian Concept of Specialty Competencies 33
• Deliver the highest quality care with integrity, honesty, and compassion.This includes the ability to do the following:
■ Demonstrate an awareness of racial, cultural, and societal issues thatimpact the delivery of care to patients.
■ Demonstrate an ability to maintain and enhance appropriate knowl-edge, skills, and professional behaviors.
• Exhibit appropriate personal and interpersonal professional behaviors.This includes the ability to do the following:
■ Assume responsibility for personal actions.■ Demonstrate a high degree of self-awareness.■ Maintain an appropriate balance between personal and professional
roles.■ Address interpersonal differences in professional relations.
• Practice medicine in an ethically responsible manner that respects the med-ical, legal, and professional obligations of belonging to a self-regulatingbody. This includes the ability to do the following:
■ Demonstrate an understanding of and adherence to legal and ethi-cal codes of practice.
■ Recognize ethical dilemmas and the need to help resolve them.■ Demonstrate the ability to recognize and respond to unprofessional
behaviors in clinical practice, taking into account local and provin-cial regulations.
Implementing the Role Framework
Besides delineating the roles a competent specialist must play, the RoyalCollege of Physicians and Surgeons has developed and continues to de-velop tools to implement the role framework. These tools are meant toassist in learning, teaching, evaluating, and developing faculty. A delinea-tion of these tools as listed in the CanMEDS 2000 Project Report is foundin Table 3–2.
Directions for Faculty Development
The CanMEDS 2000 Project Report stresses that the success of any edu-cational program is greatly influenced by the effectiveness of the faculty.Faculty members must have the knowledge, skills, and attitudes appro-priate to their medical specialty in addition to the knowledge, skills, andattitudes to design, implement, and evaluate a course of study. They

34
Orig
ins
of
Co
reC
om
pe
ten
cies
Table 3–2. Educational strategies for implementation of roles: an overview
Roles Learning environment Bedside teachingStructure: cognitive instructiona Workshops
Medical expert Self-directed learningIndividual mentorship
Apprenticeship model Problem-based learningClinical reasoning
Effective consultationsPresentation skillsEvidence-based medicineInformation access/
retrievalBioethics
Communicator Empathy, respect (reflects how patient should be treated)
Individual and groupReflection of experiences
Role modelingEffective patient and
family communications
Conceptual framework of patient-M.D. communication
Communication skills, special topics (e.g., racial/cultural issues, bad news)
Communications skills Constructive feedbackRole playing, +/�
videotape
Collaborator Interdisciplinary organization/staffing
Seamless healthcare delivery unit (inpatient/ambulatory)
Role modeling Relevant governance structuresInterdisciplinary teaching
sessions
Team-building exercises
Manager Role modeling, managing time and resources among different priorities
Allocation of healthcare resources
Practice managementLeadership skills
Health advocate Individual patient and patient population advocacy issues
Relevant governance structuresInterdisciplinary teaching
sessions
Effective intervention/ assistance in patient and population problems

Ad
vance Stan
dard
s: The C
anad
ian C
on
cept o
f Specialty C
om
peten
cies3
5
Scholar Self-directed learningEvidence-based practiceLifelong learningPractice reflection
Learning from clinical problems
Clinical standard settingQuality assurance/managementHealth economics
Reflection on practiceCritical appraisal skills
Professional Direct observation and feedback
Learner prescriptions
Role modeling of professional attitudes and behaviors
Case-based discussionsMedicolegal roundsMedical ethics rounds
Awareness of professional responsibilities
aCase discussions, half-day rounds, etc.
Table 3–2. Educational strategies for implementation of roles: an overview (continued)
Roles Learning environment Bedside teachingStructure: cognitive instructiona Workshops

36 Origins of Core Competencies
must also be able to evaluate their students’ learning and their own effec-tiveness as teachers. Within the scholar role, the CanMEDS 2000 ProjectReport discusses functioning as an educator in facilitating learning. Sucha role is multidimensional, as the physician as educator will likely need tofunction as teacher, professional within the subject area field, researcher,educational design specialist, communicator, performer, coach, advocate,mentor, judge, and remediator. The CanMEDS 2000 Project Reportclearly points out that faculty development is extremely important in theprocess of curriculum change. It is all the more important in a projectsuch as the CanMEDS 2000 Project, given that professional attitudes, be-haviors, and patterns of practice are more firmly established during post-graduate training than at any other time in the medical life cycle.
The Royal College emphasizes that our commitment to faculty devel-opment not only is structured and long-term but also places faculty de-velopment within the lifelong learning plans of the faculty themselves.
Just as the role of medical expert was central among all the roles a spe-cialist must play, so the role of mentor is central among all of the roles aphysician educator must play. As the CanMEDS Project Report pointsout, students implicitly model themselves after their mentors, incorpo-rating in themselves similar concepts, approaches, and attitudes, as wellas specific knowledge and skills. It is often through the implicit influencesof such role models that students determine their values, priorities, andbehaviors. Faculty must not only be knowledgeable about the CanMEDSrole framework of competencies but also exemplify the very behaviorsthat need to be instilled in students and actively support and promotetheir application.
The CanMEDS 2000 Project Report also stresses the support that thefaculty must have in order to do their task. Faculty require the sustainedleadership of senior staff, fair and consistent evaluation, and appropriatecareer advancement, including financial rewards. The faculty must seethe faculty development program as an integral part of their own con-tinuing education programs.
Implications of the CanMEDS 2000 Project for American Medical Systems
Size and Scope
The Royal College of Physicians and Surgeons is an organization of med-ical specialists dedicated to ensuring the highest standards and quality ofhealthcare. Our college is uniquely structured to cover the full spectrumof postgraduate medical education for all 58 medical, surgical, and labo-

Advance Standards: The Canadian Concept of Specialty Competencies 37
ratory specialties recognized in Canada. In other words, the Royal Col-lege combines the functions of the Accreditation Council for GraduateMedical Education (ACGME), with its oversight for the residency pro-grams and the resident review councils, and the American Board of Med-ical Specialties, with its coordination of medical specialty boards withina single organization. Having one organization that is totally responsiblefor medical specialties allows the implementation of a program of com-petencies a unified approach. The Royal College is the Canadian institu-tion responsible for all standard setting and monitoring of specialtymedical education; the college fulfills this responsibility by using specialty-specific committees. To achieve agreement on a body of core competen-cies and to fully implement them, medical institutions in the UnitedStates would require both the consensus and the complicity of various or-ganizations, a task that could be both time-consuming and tedious, if notimpossible. Our Canadian system is far more streamlined than what ex-ists in the United States.
Also, all Royal College–accredited programs are university sponsored.There are 16 medical schools in Canada with university-based programs,16 psychiatry residencies, and 15 neurology residencies. This againcontrasts greatly with the situation in the United States, which has 125medical schools, which are sponsored both publicly and privately. In ad-dition, in the United States, there are 179 psychiatry residencies and 117neurology residencies. The size, scope, and varying governing bodies ofU.S. institutions again provide a challenge for the uniform implementa-tion of even the very best programs.
Implementation Procedures
Once the generic competencies were identified, the Royal College em-barked on a period of experimentation and development of the CanMEDSroles. This was done through the provision of seed grants to workinggroups with the overall goal of developing pilot projects on how to teachand evaluate the CanMEDS.
The next phase of implementation for the CanMEDS 2000 Projectwas to incorporate the CanMEDS competencies into the standards andinfrastructure of the Royal College. Research and development grantswere created, and an Educational Research and Development Unit of theOffice of Education was formed. After that unit was formed, the CanMEDScompetencies were incorporated into the specialty-specific objectives oftraining; examination blueprints, final in-training evaluation reports, andstandards of accreditation are well under way. The specialty-specific ob-jectives of training define each discipline and state the general as well as

38 Origins of Core Competencies
the specialty-specific objectives under each CanMEDS competency. Asample of these specialty-specific objectives is shown in Table 3–3.
As in the unified approach to medical specialties described in the pre-vious section, the monolithic structure of the Royal College has permit-ted a uniform implementation plan of the roles concept that can reachand affect all areas of medical specialty education while taking into ac-count the uniqueness of specialty-specific competencies. With the diver-sity of medical specialty training venues in the United States, such animplementation plan would be impossible.
Evaluation Measures on the Residency Level
A new template has been developed for the Final In-Training (residency)Evaluation Reports (FITER) of all specialties and subspecialties recognizedby the Royal College. This FITER template incorporates the competenciesfrom each of the seven CanMEDS physician roles (Figure 3–1). The tem-plate identifies the generic competencies required of all specialists, andeach specialty committee defines specialty-specific competencies as nec-essary for its FITER.
Once each of the disciplines has incorporated its specialty-specific ob-jectives into the FITER, a successful FITER becomes one of the require-ments for eligibility to sit for the examinations leading to certification aswell as for successful completion of subspecialties without examination.
The Canadian FITER template could prove useful to medical resi-dency programs in the United States as a model for evaluating residentson the agreed-on competencies for a given specialty. Given that the med-ical competencies for each specialty are in the process of being defined,it is possible that the residency review committees would have the re-
Table 3–3. Objectives of training for psychiatry under the health advocate role
General requirementsIdentify the important determinants of health affecting patients.Contribute effectively to improved health of patients and communities.Recognize and respond to those issues where advocacy is appropriate.
Specific requirementsDemonstrate awareness of structures of governance in mental healthcare.Demonstrate awareness of the major regional, national, and international
advocacy groups that are active in mental health matters.

Ad
vance Stan
dard
s: The C
anad
ian C
on
cept o
f Specialty C
om
peten
cies3
9Expectations
A rationale must be provided to support ratings with asterisks.
Rare
ly m
eets
*
Inco
nsi
sten
tly*
Gen
era
lly
So
meti
mes
Co
nsi
sten
tly*
MEDICAL EXPERT
a) Demonstrates a good understanding of the basic scientific and clinical knowledge relevant to the specialty.
b) Conducts complete, accurate, and well-organized history and physical examinations.
c) Uses all of the pertinent information to arrive at complete and accurate clinical decisions.
d) Recognizes and manages emergency conditions (extremely ill patient), resulting in prompt and appropriate treatment. Remains calm, acts in a timely manner, and prioritizes correctly.
Please define other competencies as necessary.
Please comment on the strengths and weaknesses of the candidate and provide a rationale for your ratings.
Figure 3–1. FITER (Final In-Training Evaluation Report) template using the medical expert role.

40 Origins of Core Competencies
sponsibility for developing a FITER-like tool to assess residents. A pro-gram director’s attestation of the completion of a FITER, in combinationwith other criteria, could serve as a final tool to be required for eligibilityfor the certification examination.
Examination Blueprints
The Canadian system provides for the initial certification of medical spe-cialists, stressing a comprehensive examination at the end of the trainingperiod. The Royal College examination blueprints are based on the Can-MEDS competencies as well as on the objectives of training developedby each specialty. An examination blueprint defines the content andcompetencies that are to be measured by examination.
Blueprints promote content validity (the concept that the examina-tion is designed to test the material it should test), ensure stability of testcontent and competencies over time, and help in examining the relation-ship between examination components. Blueprints are used to choose theappropriate measurement technique to evaluate each competency and toweigh the value of the examination components, content, and competen-cies.
Figure 3–2 provides sample examination blueprints for the general rolesof health advocate and scholar. Examination methodologies listed in thefigure include multiple-choice questions, short-answer questions, oral ex-aminations, and a composite evaluation of the phenomenology, diagnosis,and management of the competency. In the last-mentioned methodology,technical skills are both tabulated and rated. For competencies for whichnone of the cited evaluation methodologies would be appropriate, otherevaluative measures must be determined.
This template may prove useful to the medical specialty boards in theUnited States if the six categories of core competencies compose the firstcolumn, a listing of all of the competencies makes up the second column,and the sections of the certification and recertification examinations—rather than the evaluation methodologies, as described earlier—are listed.Perhaps this listing for certification examinations given by the ABPNcould include the Part I (written) examinations and each of the compo-nents of the Part II (oral) examination (e.g., patient examination, audio-visual tapes, vignettes) as appropriate.
Summary
The CanMEDS Program represents one way of approaching the use ofcompetencies for training and evaluation purposes. The fact that Can-

Ad
vance
Stand
ards:Th
eC
anad
ianC
on
cept
of
Specialty
Co
mp
etencies
41
Role Competencies MCQ SAQ Oral PDM
Health advocate Ability to engage in advocacy activities in responding to the challenges represented by social, environmental, and biological factors
Ability to recognize advocacy concept as it relates to the individual patient, the practice population, and the broader community
Y Y Y
Awareness of the major regional, national, and international advocacy groups active in mental health matters
Y Y
Scholar Ability, motivation, and desire to maintain competence through involvement in independent learning and continuing medical education activities
Ability to access and critically appraise sources of medical information Y Y Y
Ability to facilitate learning of patients, students, residents, and other health professionals
Y
Skills necessary to participate in collaborative research projects, quality management, or guidelines development relevant to the practice
Figure 3–2. Sample competencies examination blueprints for the roles of health advocate and scholar.Note. MCQ = multiple-choice questions; Oral = oral examinations; PDM = phenomenology, diagnosis, and management of a competency (a composite eval-uation); SAQ = short-answer questions.

42 Origins of Core Competencies
ada’s core competencies are broken out by the roles a physician plays, asopposed to categories of skills, and the fact that Canada’s medical systemis structured very differently from the medical system of the United Statesare irrelevant. The Canadian experience is similar enough in purpose tothe core competency movement within the United States that perhaps agreat deal of the competency work we have already struggled throughcan be helpful to our southern neighbors.
Reference
Royal College of Physicians and Surgeons of Canada: Skills for the New Millen-nium: Report of the Societal Needs Working Group, CanMEDS 2000Project Report. Ottawa, Ontario, The Royal College of Physicians and Sur-geons of Canada, 1996

43
Chapter 4
The ACGME and ABMS Initiatives
Toward the Development of Core Competencies
Susan E. Adamowski, Ed.D.
The Push for Definition of Medical Competencies
The field of education was heavily influenced in the late 1960s and early1970s by a focus on educational outcomes. According to Ralph Tyler, aprofessor at the University of Chicago, educational activities should beguided by objectives written in behavioral terms that describe measur-able outcomes. The success of the educational activities should be judgedon how well the students achieve the measurable outcomes (Tyler 1949).The concept of core competencies grew out of this focus on educationaloutcomes and received a major thrust in the 1980s when the U.S. De-partment of Education mandated outcome measures for all educationalprojects, including those involving accreditation.
I am indebted to Dr. David Leach, Executive Director of the AccreditationCouncil for Graduate Medical Education, and Dr. Sheldon D. Horowitz, Associ-ate Vice President of the American Board of Medical Specialties, for their assis-tance in the preparation of this chapter.

44 Origins of Core Competencies
Heavily funded medical education systems, having greatly expandedduring the 1970s, were a prime target of this initiative and were called onto provide evidence of responsible stewardship in preparing competentphysicians to meet public healthcare needs. Various groups, meetingthrough the 1990s, developed objectives to assess or measure these edu-cational outcomes within medicine. Some groups concentrated on attri-butes of competence, while others focused more on performance issues.These outcomes eventually came to be referred to as necessary, or “core,”competencies. Among the groups in the United States working on defi-nitions or delineations of competence were the following:
• American Board of Medical Specialties (ABMS) Task Force on Com-petence
• Accreditation Council for Graduate Medical Education (ACGME)Outcome Project Advisory Group
• Association of American Medical Colleges Medical School ObjectivesProject Group
• Federated Council for Internal Medicine Task Force on the Internal Med-icine Residency Curriculum
• National Association for Competency Assurance• The Pew Health Professions Commission
The work of these various groups was remarkably similar. For example,the core components of competence, as listed by the ABMS in draft formfor discussion at its meeting of the Task Force on Competence, heldMarch 16–17, 1999, are presented in Table 4–1.
Essentially at the same time these core components were being dis-cussed by the ABMS, the ACGME asked its Outcome Project AdvisoryGroup to research work on competencies and to develop a list of neces-sary competencies. The group eventually settled on 86 competencies forphysicians, and that list was pared to fall within six general areas:
• Patient Care• Medical Knowledge (originally Clinical Science)• Interpersonal and Communications Skills• Practice-Based Learning and Improvement• Professionalism• Systems-Based Practice
Within these six major categories, the ACGME’s Outcome ProjectAdvisory Group listed competencies in a manner similar to the way theABMS had listed the components of its necessary attributes of compe-tency as shown in Table 4–1. A major step forward occurred in Septem-

The
AC
GM
Ean
dA
BM
SIn
itiatives4
5Table 4–1. American Board of Medical Specialties example components of competence
Attributes Example components
Medical knowledge Possess up-to-date knowledge needed to evaluate and manage patients.
Clinical skills Demonstrate proficiency in history taking.Conduct physical examinations effectively.Lead and manage diagnostic studies.Demonstrate practice skills.Show proficiency in technical skills.
Clinical judgment Demonstrate clinical reasoning.Make sound diagnostic and therapeutic decisions.Understand the limits of one’s knowledge.Incorporate the considerations of cost-awareness and risk-benefit analysis for the patient.
Interpersonal skills Communicate and work effectively with patients, families, physicians, other health professionals, and health-related agencies.
Professional attitudes and behavior AccountabilityAccept responsibility.Maintain comprehensive, timely, and legible medical records.Be available in a consultative role to other physicians and health professionals when needed.Seek continuous improvement in the quality of care provided.Facilitate learning of patients, students, house staff, and other health professionals.
Lifelong learningEvaluate critically new medical and scientific information relevant to the practice of medicine and apply
it to patient care.Possess skills and experience in self-assessment of medical knowledge and clinical skills.
46
Orig
ins o
f Co
re C
om
pe
ten
cies
Professional attitudes and behavior(continued)
Humanistic qualitiesDemonstrate integrity and honesty.Demonstrate compassion/empathy.Show respect for patients’ privacy.Show respect for the dignity of patients as persons, including their culture, gender, and age.
Ethical behaviorConsistently demonstrate high standards of moral and ethical behavior.
Managerial skills Work effectively and efficiently in a healthcare organization.Utilize information technology to optimize patient care, lifelong learning, and other activities.Possess basic business skills important for effective practice management.
Health advocacy Promote health and prevention of disease of individuals and populations.Advocate in the interest of one’s patients.
Source. Adapted from American Board of Medical Specialties Task Force on Competence Agenda Book (pp. 91–92), from a meeting of the task force held inChicago, Illinois, March 16–17, 1999.
Table 4–1. American Board of Medical Specialties example components of competence (continued)
Attributes Example components

The ACGME and ABMS Initiatives 47
ber 1999 when the ABMS Assembly agreed to adopt the ACGME’s sixareas of competencies. This meant that for the first time there was agree-ment on the areas of core competencies among the governing body of res-idency programs and the umbrella organization for medical specialtyboards.
The chart in Table 4–2 lists the competencies in the six categories aswritten by the ACGME and correlates those with the ABMS compo-nents listed in Table 4–1 and the seven roles a physician plays as delin-eated by the CanMEDS 2000 Project of the Royal College of Physiciansand Surgeons of Canada as described in Chapter 3.
Concurrent with implementation of core competencies at the resi-dency level according to ACGME mandate, the ABMS announced thatit expected specialty boards to determine which components of eachcompetency are relevant to the initial certification and maintenance ofcertification programs. Later, in March 2002, the ABMS Assembly ap-proved, as part of the Maintenance of Certification©, “Guidelines for theAssessment of Physician Practice Performance.” The guidelines statedthat, initially, each of the six general competencies should be assessed atleast once during a board’s repeating Maintenance of Certification cycle.
ACGME/ABMS Quadrads
To complete these tasks, the ACGME Outcome Project and the ABMS,through a joint initiative, established quadrads composed of a specialtyboard representative, an ACGME Residency Review Committee (RRC)representative, a program director, and a resident. Each quadrad devel-oped a specialty-specific version and an assessment plan for each of thecompetencies.
The Psychiatry Quadrad
The psychiatry quadrad members were Dr. Glenn C. Davis, representingthe American Board of Psychiatry and Neurology (ABPN); Dr. AndrewRussell, representing the Psychiatry RRC; Dr. John Herman, the psychi-atry program director at Massachusetts General/McLean Hospital; andDr. Mara Goldstein, representing psychiatry residents.
The outline of the six general categories of core competencies as de-veloped by the psychiatry quadrad can be found in Appendix A in thisvolume.
The quadrads for the different medical specialties came up with a va-riety of approaches to their outline task. All quadrad outlines, however,

48
Orig
ins
of
Co
reC
om
pe
ten
cies
Table 4–2. General competencies core components
Categories ACGME ABMSCanMEDS2000 Project
Patient Care Communicate effectively and demonstrate caring and respectful behaviors when interacting with patients.
Gather essential and accurate information about the patient and use it, together with up-to-date scientific evidence, to make decisions about diagnostic and therapeutic interventions.
Develop and carry out patient management plans.Perform competently all medical and invasive
procedures considered essential for the area of practice.
Provide healthcare services aimed at preventing health problems or maintaining health.
Work with other healthcare professionals to provide patient-focused care that maximizes the likelihood of a positive health outcome.
Demonstrate proficiency in history taking.Conduct physical examinations effectively.Lead and manage diagnostic studies.Demonstrate clinical reasoning.Make sound diagnostic and therapeutic
decisions.Understand the limits of one’s knowledge.Demonstrate practice skills.Show proficiency in technical skills.Promote heath and prevention of disease of
individuals and populations.Advocate in the interest of one’s patients.Utilize information technology to optimize
patient care, lifelong learning, and other activities.
Medical expertCommunicator
Medical Knowledge (Clinical Science)
Demonstrate rigor in thinking about clinical situations.
Know and apply the basic and clinically supportive sciences that are appropriate to the discipline.
Possess up-to-date knowledge needed to evaluate and manage patients.
Medical expert

The A
CG
ME an
d A
BM
S Initiatives
49
Interpersonal and Communications Skills
Create and sustain a therapeutic relationship with patients.
Engage in active listening, provide information using appropriate language, ask clear questions, and provide an opportunity for input and questions.
Work effectively as a member or leader of a healthcare team or other professional group.
Communicate and work effectively with patients, families, physicians, other health professionals, and health-related agencies.
Be available in a consultative role to other physicians and health professionals when needed.
Maintain comprehensive, timely, and legible medical records.
CommunicatorCollaborator
Practice-Based Learning and Improvement
Analyze practice experience and perform practice-based improvement activities using a systematic methodology.
Locate, appraise, and assimilate “best practices” related to patients’ health problems.
Apply knowledge of study designs and statistical methods to the appraisal of clinical studies and other information on diagnostic and therapeutic effectiveness.
Use the computer to manage information, access on-line medical information, and support clinical care and patient education.
Evaluate critically new medical and scientific information relevant to the practice of medicine and apply it to patient care.
Utilize information technology to optimize patient care, lifelong learning, and other activities.
Possess skills and experience in self-assessment of medical knowledge and clinical skills.
Facilitate learning of patients, students, house staff, and other health professionals.
ScholarManager
Table 4–2. General competencies core components (continued)
Categories ACGME ABMSCanMEDS2000 Project

50
Orig
ins o
f Co
re C
om
pe
ten
cies
Professionalism Demonstrate respect, regard, integrity, and a responsiveness to the needs of patients and society that supersedes self-interest; assume responsibility and act responsibly; demonstrate a commitment to excellence.
Demonstrate a commitment to ethical principles pertaining to provision or withholding of clinical care, confidentiality of patient information, informed consent, and business practices.
Demonstrate sensitivity and responsiveness to cultural differences, including awareness of one’s own and one’s patients’ cultural perspectives.
Accept responsibility.Demonstrate integrity and honesty.Demonstrate compassion/empathy.Show respect for patients’ privacy.Consistently demonstrate high standards
of moral and ethical behavior.Show respect for the dignity of patients as
persons, including their culture, gender, and age.
ProfessionalScholarHealth advocate
Table 4–2. General competencies core components (continued)
Categories ACGME ABMSCanMEDS2000 Project

The A
CG
ME an
d A
BM
S Initiatives
51
Systems-Based Practice Understand how patient care practices and related actions impact component units of the healthcare delivery system and the total delivery system, and how delivery systems impact the provision of healthcare.
Know systems-based approaches to controlling healthcare costs and allocating resources; practice cost-effective healthcare and resource allocating that does not compromise quality of care.
Advocate for quality patient care and assist patients dealing with system complexities.
Know how to partner with healthcare managers and healthcare providers to assess, coordinate, and improve healthcare; know how these activities can impact system performance.
Incorporate the considerations of cost-awareness and risk-benefit analysis for the patient.
Advocate in the interest of one’s patients.Work effectively and efficiently in a
healthcare organization.Possess basic business skills important for
effective practice management.Seek continuous improvement in the
quality of care provided.
Health advocate
Note. ABMS = American Board of Medical Specialties; ACGME = Accreditation Council for Graduate Medical Education.Source. The first three columns of this table are from the American Board of Medical Specialties Task Force on Competence Agenda Book (pp. 93–96) from ameeting in Chicago, IL, March 16–17, 1999. The fourth column is adapted from the same source, p. 107.
Table 4–2. General competencies core components (continued)
Categories ACGME ABMSCanMEDS2000 Project

52 Origins of Core Competencies
were set up in essentially the same way, as they had to relate to the sixareas of core competencies as agreed on by the ACGME and the ABMS.
Comparison of the Psychiatry and Neurology Quadrad Outlines
The difference between the psychiatry and neurology quadrad outlinesbecame a cause for concern for the ABPN, since the board is unique inrepresenting two specialties. The history of this merger goes back to theinception of the ABPN in 1934. Because the ABPN represents two spe-cialties, the Task Force on Core Competencies, the body established bythe ABPN to consider the ACGME/ABMS mandate regarding core com-petencies, suggested that the two quadrad outlines be merged so that theABPN would have one core competency outline for which to be respon-sible to the ABMS.
Generally speaking, the psychiatry quadrad outline was more specificthan the neurology quadrad outline. In addition, the psychiatry quadradoutline offered suggestions for evaluative tools at the end of each outlinesection. The neurology quadrad included its evaluation suggestions in atable attached to the end of its outline.
Although the approaches to content in the various sections of the out-line required discussion, the discrepancy between the two medicalknowledge sections was the most dichotomous. The neurology quadradbasically said through its outline that neurology residents must be com-petent in two areas:
Neurology residents must know the areas of medical knowledge as pro-vided in the content outlines of the examinations given by the ABPN.1
Neurology residents must have the ability to reference and utilize elec-tronic information systems to access new information.
The neurology quadrad’s attaching the ABPN examination contentoutline as essentially its complete medical knowledge section of the corecompetencies outline raised an interesting question: Should the medicalknowledge section of the core competency outline be exactly the same asthe board’s examination content outline in that specialty? The neurologyquadrad thought that it should, but the psychiatry quadrad differed and
1This section of the neurology quadrad outline attaches the content outline forthe ABPN written certification (Part I) examination in neurology.

The ACGME and ABMS Initiatives 53
wrote its own list of core competencies for the medical knowledge cate-gory. An examination of other specialty quadrad outlines shows that a va-riety of approaches were taken in this and other areas.
In dealing with the six different subject areas of the outline (PatientCare, Medical Knowledge, Interpersonal and Communications Skills,Practice-Based Learning and Improvement, Professionalism, and Systems-Based Practice), a dichotomy emerged. It appeared that while the firsttwo content sections of the outline (Patient Care and Medical Knowl-edge) were divergent, the content of the last four sections of the outline(Interpersonal and Communications Skills, Practice-Based Learning andImprovement, Professionalism, and Systems-Based Practice) was more sim-ilar than divergent. Thus, it appeared that the latter four sections of theoutlines would be easier to merge than would the first two.
Reflection suggested the logic behind this observation. Physicians’skills in the last four areas of the outline could be thought of as beingmore uniform across specialties than specific to a specialty. The first twoareas of the outline—Patient Care and Medical Knowledge—would be,logically, more specialty specific. In dealing with this dichotomy, it wasdecided to merge the first two sections of the neurology competency out-line with the psychiatry competency outline as far as possible. Thesecommon areas would be referred to as “General Patient Care” and “Gen-eral Medical Knowledge.” The specialty-specific areas of Patient Care andMedical Knowledge would be kept separate and labeled “Neurology” and“Psychiatry” as appropriate.
It was further decided that the last four sections of the competency out-lines (Interpersonal and Communications Skills, Practice-Based Learningand Improvement, Professionalism, and Systems-Based Practice) would bemerged into one with a uniform format. Rather than use the statements/bulleted points format of the neurology outline or the numbered state-ments/bulleted points of the psychiatry outline, a regular Roman nu-meral outline format was selected for this merger.
The Merged Core Competency Outline
Through the process of merging the psychiatry and neurology quadradoutlines, it became abundantly clear that core competencies, in concept,are fluid and responsive to new knowledge in the medical field and to ad-vances in technology among other things. Thus, the task of arriving at a“final” core competency outline was abandoned. Any iteration of a corecompetency outline can only be current as of its writing. Amendmentsand revisions will always need to be made, and all those who use the corecompetency outlines (e.g., medical school faculty, program residency di-

54 Origins of Core Competencies
rectors, medical certification examination writers) will need to take thisprinciple into account. Clear communication among core competencyconstituent groups regarding major changes in the core competenciesoutline would be absolutely necessary, but most variations would be as-sumed to be minor.
A “final version” of the core competency outline was prepared afterhaving taken into account input from all of the ABPN directors. This“final version” of the core competency outline was final only in the sensethat it was the outline that was printed for use at the ABPN InvitationalCore Competencies Conference, which is discussed in Part III of thisbook. Changes to the outline were anticipated and accepted during thework of that conference.
Reference
Tyler RW: Basic Principles of Curriculum and Instruction: Syllabus for Education360. Chicago, IL, University of Chicago Press, 1949

55
Part III
Core Competencies and the Practice of Psychiatry Today
The ABPN Initiative
This part of the book will focus on the key points that emerged from thediscussions conducted at the American Board of Psychiatry and Neurology(ABPN) Invitational Core Competencies Conference held June 22–23,2001, in Toronto, Ontario, Canada. For this conference, the ABPN invitedsome of the key leaders in the medical fields of psychiatry and neurologyto come together to discuss the six categories of core competencies agreedon by the Accreditation Council on Graduate Medical Education and theAmerican Board of Medical Specialties. Approximately 50 of the inviteeswere able to attend. The primary goal of the conference was for thethought leaders in medical education to dialogue about how best to imple-ment the core competencies as written for certification purposes.
Representatives from the following groups were initially invited to theABPN Core Competencies Conference:

56 Core Competencies and the Practice of Psychiatry Today
• Accreditation Council for Continuing Medical Education• Accreditation Council for Graduate Medical Education• American Academy of Child and Adolescent Psychiatry• American Academy of Neurology• American Association of Chairpersons of Departments of Psychiatry• American Association of Directors of Psychiatric Residency Training• American Association of Medical Colleges• American Board of Medical Specialties• American College of Psychiatrists• American Medical Association• American Neurological Association• American Psychiatric Association• Association of University Professors of Neurology• Child Neurology Society• National Institute of Mental Health• National Institute of Neurological Disorders and Stroke• Professors of Child Neurology• Royal College of Physicians and Surgeons of Canada• Substance Abuse and Mental Health Services Administration
The working objectives presented for the ABPN Invitational CoreCompetencies Conference were as follows:
1. Determine what core competencies for psychiatry and neurologyshould be assessed for certification purposes.
2. Determine who should carry out the assessment. (If not ABPN, who?)3. Determine how this should be done. (Which methodologies should
be used for which competencies?)4. Determine where in the medical education track this should be done.
(If by ABPN, at which assessment?)5. Determine how to collect data to validate the core competencies.
In addition to the questions in the objectives above, two other key issuesneeded attention:
1. Is the core competency outline as currently conceived adequate forABPN purposes? If not, what needs to be changed, and how?
2. Are there core competencies about neurology that psychiatrists needto know (and about psychiatry that neurologists need to know) to bejudged competent? If so, what must be added to the outline?
Nadia Z. Mikhael, M.D., Director of Education for the Royal Collegeof Physicians and Surgeons of Canada, delivered a keynote address to the

The ABPN Initiative 57
conference participants. Her topic was the pioneering work done by theRoyal College regarding core competencies. Specifically, Dr. Mikhael fo-cused on the following:
1. Listing the competencies the CanMEDS 2000 Project identified asbeing needed by physician specialists.
2. Explaining how the Royal College went about working with programdirectors and curriculum committees to ensure that the necessary ma-terial covering these competencies was taught in residency.
Dr. Mikhael’s presentation at the conference is the basis for her chap-ter in the preceding part (Chapter 3, “Advance Standards”).
The chapters in Part III present in some detail the discussions that oc-curred as breakout groups of conference participants attempted to ac-complish the tasks set by the conference objectives. Each breakout groupwas assigned to one of the six general areas of core competencies. Discus-sion was structured by applying the objectives to each individual compe-tency within each of the six general core competency areas. Although thediscussion groups did come to some specific conclusions, discussiontended to be global rather than specific. Chapters 5 through 10 discusseach of the core competency areas as it applies to the field of psychiatry.Chapter 11 discusses which neurology competencies are necessary forpsychiatrists to know.
Following the small-group work, the conference attendees reconvenedas a large group for reports on the general core competency areas. Ques-tions and answers followed each small-group presentation. The confer-ence concluded with remarks from a selected panel of reactors. Theremarks included subjective evaluations of the conference and variousanswers to the unspoken question “Where do we go from here with thecore competencies?” Part IV of this book will discuss these issues.

This page intentionally left blank

59
Chapter 5
General and Psychiatry-Specific Patient Care Core Competencies
Glenn C. Davis, M.D.
Assumptions Regarding the Patient Care Core Competencies
The group discussing the Patient Care Core Competency Section of thepsychiatry quadrad outline (see Chapter 4: “The ACGME and ABMS In-itiatives”) debated several initial assumptions. First, they assumed thatevery competency listed for them to consider was already being assessedby the American Board of Psychiatry and Neurology (ABPN) written cer-tification (Part I) examination, by the ABPN oral certification (Part II)examination, or by both. Second, they also assumed that the Patient CareCore Competencies should all be of the highest priority for both trainingand assessment purposes. Both of these assumptions were supported af-ter debate, but much discussion ensued regarding the first assumption.
The Patient Care Core Competencies Outline is divided into threesections: general, psychiatry, and neurology. The competencies in thegeneral section apply to both psychiatrists and neurologists, while the lat-ter two sections are specialty specific. For the purposes of this chapter,the neurology section will not be discussed, but it will be referenced in adiscussion of cross competencies in Chapter 11 (“Cross Competencies”).
The outline as presented to the conference participants was dividedinto parts, with each part representing essentially one core competency.

60 Core Competencies and the Practice of Psychiatry Today
This division into parts was made by the staff in order to create logicalsections of the outline for discussion purposes. It was recognized that thediscussion group might want to make changes if it deemed them neces-sary. This information was communicated to the discussion group leadersin their training, but no changes for the Patient Care Core Competencieswere thought to be necessary; thus, each section of the outline discussedin what follows will be assumed, for current purposes, to be one corecompetency.
The General Patient Care Core Competencies
The First General Patient Care Core Competency
The physician shall demonstrate the ability to perform and document a relevant history and examination on culturally diverse patients1 to include as appropriate:
A. Chief complaintB. History of present illnessC. Past medical historyD. Review of systemsE. Family historyF. Sociocultural history2
G. Developmental history (especially for children)
The discussants clearly saw this core competency as being assessed pri-marily through clinical examinations, such as the current ABPN oral cer-tification (Part II) examination. Discussion centered on the difficultysome candidates have with this examination. Indeed, the demonstrationof this competency (and some of the following related core competencies)has proven to be such a stumbling block that some candidates have been
1Cultural diversity includes issues of race, gender, language, age, country of ori-gin, sexual orientation, religious/spiritual beliefs, sociocultural class, education/intellectual levels, and physical disability. Working with a culturally diverse pop-ulation requires knowledge about cultural factors in the delivery of healthcare.For the purposes of this document, all patient and peer populations are to be con-sidered culturally diverse.2Regarding sociocultural issues, for the purposes of this document, “family” isdefined as those having a biological or otherwise meaningful relationship with thepatient. Such “significant others” are to be defined from the patient’s point ofview.

Patient Care Core Competencies 61
unable to pass the patient portion of the Part II examination in spite ofmultiple attempts.
Discussion led to the idea that if this core competency is such a basicskill, it should be formally assessed early in candidates’ educational ca-reers. That way, if remediation were needed, it could be provided whilecandidates were still in training. If remediation proved ineffective, a candi-date could be redirected in terms of career decisions. How this assessmenttask could be accomplished led to more discussion, with one conclusionbeing that the residency program directors could be the primary assessorsof this core competency. The ABPN could work with the program direc-tors to make certain that the assessment was done according to the board’scurrent standard.
Further discussion included the necessity for including this core com-petency in the Practice Assessment Component of the Maintenance ofCertification (MOC) Program. The MOC Program will affect all prac-ticing psychiatrists who do not have lifetime certification—that is, thosewho were certified after October 1, 1994. Psychiatrists holding lifetimecertification will also be able to apply for the ABPN MOC Program todemonstrate their continued competence in practice.
As the ABPN MOC Program is just beginning to be implemented ac-cording to the mandate of the American Board of Medical Specialties(ABMS), the discussion directions provided to the group encouraged par-ticipants to think about using the four components of the MOC Program(Licensure, Lifelong Learning, Recertification Examination, and PracticeAssessment) as assessment opportunities for core competencies when ap-propriate for recertification purposes. Conference participants were toldthat they need not be concerned at this time as to how the LifelongLearning and Practice Assessment Components of the ABPN MOC Pro-gram were going to be implemented. Decisions regarding these two com-ponents of the MOC Program would be made later by the ABPN, mostlikely with direction from the ABMS. The main issue for discussion atthis conference was to see what core competencies might be delegated tothe MOC Program.
Thus, for this first Patient Care Core Competency, the group recordedthat this competency is being assessed on the ABPN oral certification(Part II) examination, but that this competency should at least initially beassessed much earlier in the candidates’ careers. Program directors, withinvolvement at some level by the ABPN, could carry out this assessment,and their evaluation would be sufficient for the early part of the candi-dates’ careers. Program directors would also have the responsibility toprovide remediation for candidates who did not perform up to standardon this measure of competence. This core competency was also assigned

62 Core Competencies and the Practice of Psychiatry Today
to the Practice Assessment Component of the MOC Program for psychi-atrists seeking recertification.
Possible methodologies suggested for assessing this core competencyincluded the following:
• Oral examinations with actual patients, similar to what is currently be-ing done in the ABPN oral certification (Part II) examination
• Oral examinations using standardized patients• Vignettes, which could be presented at various points during the can-
didates’ educational journey• Objective-structured clinical examinations
Some conference participants spoke of program directors having aconflict of interest in trying to assess the competence of their own resi-dents. Program directors, because of their involvement with their resi-dents and their need for their program to be seen in a good light, mightnot be able to rate their residents objectively. It was concluded that theprogram directors could provide initial assessment in this area, but thatsomeone outside the training program would need to certify that a phy-sician had the particular skill. The assessment provided by the programdirectors would be especially helpful for those residents needing remedi-ation, as such could easily be provided during residency. There was noconsensus on when this competency should be assessed for certificationpurposes.
To validate that this core competency is indeed a required competencyfor the practice of psychiatry, the perceptions of both public and profes-sional groups could be referenced and documented. A given patient canrepresent the public sector and certainly report his or her perceptions ofthe encounter with the physician. Although the patient could not judgethe clinical effectiveness of a physician’s work involved with this com-petency, he or she could report whether or not different portions of theexamination had, in fact, been done. In most cases, during a patient-physi-cian encounter, no one else is present. Thus, the patient is in a unique po-sition to assess the completeness of the tasks listed within the first corecompetency. Perceptions of other professionals (general physicians, otherspecialists, and nurses, for example) as to how well the physician accom-plishes this core competency would also be important. These could bemeasured on the basis of feedback given to a referring physician, infor-mation provided to a nurse, and discussion about the patient with otherspecialist colleagues in psychiatry and/or other fields.

Patient Care Core Competencies 63
The Second General Patient Care Core Competency
The physician shall demonstrate the ability to delineate appropriate differential diagnoses.
After the extensive discussion of the first Patient Care Core Compe-tency, this second one was handled quickly. In general, everything thatwas said regarding the first Patient Care Core Competency could applyto this one as well. The only addition was that the group thought that thiscore competency could also be assessed on cognitive examinations, likethe ABPN written certification (Part I) examination.
During discussion of all that needed to be assessed on the written andoral sections of the ABPN certification examination, it was pointed outthat all examinations, no matter what their form, are samplings of repre-sentative knowledge, skills, and attitudes. No examination can ever testevery situation that a professional might encounter in practice. There-fore, for its written certification (Part I) examination, the ABPN wouldneed to be committed to having a question pool that covered all of thecore competencies that could be assessed in a multiple-choice question(MCQ) format. Not all questions would have to be asked—or even couldbe asked—but that is not the goal of an examination. The examination ismeant to sample representative knowledge. Similarly with the ABPN oralcertification (Part II) examination, only a sampling of possible patientscan be considered. Methods of validation could include both public andprofessional perception.
The Third General Patient Care Core Competency
The physician shall demonstrate the ability to evaluate, assess, and recommend effective management of patients.
As with the second general Patient Care Core Competency, for thisthird core competency, it was assumed that the ABPN written certification(Part I) and oral certification (Part II) examinations, along with the Prac-tice Assessment Component of the MOC Program, could be the timesthis competency would be assessed. Specific suggested methodologies forassessment here included oral interviews, audits, and portfolio reviews.Methods of validation could include outcome studies and both public andprofessional perception.

64 Core Competencies and the Practice of Psychiatry Today
In general, the conference participants discussing the Patient CareCore Competencies agreed that the outline lacked sufficient detail, butwith the exception of two minor examples, no suggestions for specificitywere made.
The Psychiatry Patient Care Core Competencies
The second section of the core competency outline represents psychia-try-specific core competencies.
The First Psychiatry Patient Care Core Competency
Based on a relevant psychiatric assessment, the physician shall demonstrate the ability to develop and document the following:
A. A complete multiaxial differential diagnosisB. An evaluation plan, including appropriate medical, laboratory,
radiological, and psychological examinationsC. A comprehensive treatment plan addressing biological, psychological,
and sociocultural domains
This core competency is currently evaluated most completely on theABPN oral certification (Part II) examination. It was also thought thatthis core competency could be assessed on the ABPN written certifica-tion (Part I) examination, but such an assessment would not involve “de-veloping and documenting” the specified DSM differential diagnosis, careformulation and evaluation plan, and comprehensive treatment plan. Nocognitive examination would be able to assess development and docu-mentation, but it could test about these issues. Well-written MCQs couldbe presented after a description of a case and followed by answers fromwhich the candidate would be directed to select the best alternative. GoodMCQs are difficult to write under the best circumstances, and MCQs forthis core competency could prove especially challenging.
To prepare candidates for the ABPN assessment of this psychiatry corecompetency, program directors could work on the “developing and doc-umenting” portion of this core competency. If candidates became adeptat those skills, answering MCQs about them should not be overly diffi-cult.
Assessment of this core competency was also thought necessary forthe MOC Program as well as for initial certification. While the LicensureComponent of the MOC Program would not apply to this core compe-tency, it was thought that all of the other three components (Lifelong

Patient Care Core Competencies 65
Learning, Recertification Examination, and Practice Assessment) would.Testing for this competency on the recertification examination would bea variation of testing for it on the written certification (Part I) examina-tion, probably again with MCQs. Exactly how this competency would beevaluated in the Lifelong Learning and Practice Assessment Componentsof the MOC Program was not discussed.
Methodologies for assessing this core competency, in addition to in-cluding the MCQs of the written certification (Part I) and recertificationexaminations and the patient encounters and videotapes of the oral cer-tification (Part II) examination, could include the development of a port-folio. Validation of this core competency could be done through bothpublic and professional perception, as discussed earlier.
The Second Psychiatry Patient Care Core Competency
Based on a comprehensive psychiatric assessment, the physician shall demonstrate the ability to comprehensively assess and document patient’s potential for self-harm or harm to others. This shall include the following:
A. An assessment of riskB. Knowledge of involuntary treatment standards and proceduresC. Ability to intervene effectively to minimize riskD. Ability to implement prevention methods against self-harm and harm
to others
This core competency, like the first psychiatry Patient Care Core Com-petency, is currently assessed most completely on oral/clinical examina-tions such as the ABPN oral certification (Part II) examination. As withthe first psychiatry-specific core competency, it was also thought that theABPN written certification (Part I) examination could use MCQs to testabout this core competency. The oral interviews, however, would providethe only opportunity in which the candidate could fully demonstrate thiscompetency. Again, as with the first psychiatry-specific core compe-tency, it was thought that this core competency should be assessed underthree parts of the MOC Program, namely, the Lifelong Learning (perhapswith portfolio evaluation), Recertification Examination (most likely withMCQs), and Practice Assessment Components.
Program directors could coach their residents on the skills needed todemonstrate this core competency and provide initial assessment feed-back. Candidates needing remediation could receive assistance throughtheir residency programs. This core competency could also be validatedwith measures of public and professional perception.

66 Core Competencies and the Practice of Psychiatry Today
The Third Psychiatry Patient Care Core Competency
Based on a comprehensive psychiatric assessment, the physician shall demonstrate the following abilities:
A. To conduct therapeutic interviews, e.g., enhance the ability to collect and use clinically relevant material through the conduct of supportive interventions, exploratory interventions, and clarifications
B. To conduct a range of individual, group, and family therapies, using standard, accepted models, and to integrate these psychotherapies in multimodal treatment, including biological and sociocultural interventions
In theory, this core competency could be assessed during the patientportion of the ABPN oral certification (Part II) examination, but that isnot currently being done. What is currently used is an initial diagnosticinterview, not a therapeutic one. Interviews for therapeutic purposescould be designed with the use of standardized patients. In theory, suchinterviews could also be designed for the candidate to meet individuals,groups, or families (either live or simulated patient), but such interviewswould probably be cost- and time-prohibitive. Portfolio assessment couldpossibly help here, as candidates could showcase their best examples ofvarious kinds of their clinical work. Exactly what form these portfolioswould take and who would assess them was not discussed.
Program directors could work with their residents to develop skills todemonstrate this core competency, and public and professional percep-tion could be used to validate it.
The Fourth Psychiatry Patient Care Core Competency
Based on a comprehensive psychiatric assessment, the physician shall demonstrate the ability to recognize and treat psychiatric disorders.
Discussion about this core competency was essentially the same as forthe previous three. This competency is currently being assessed on theABPN written certification (Part I) and oral certification (Part II) exami-nations. It lends itself better to MCQ analysis than do the three previouspsychiatry-specific core competencies and is clearly covered on the oralexamination.
It was also agreed that this core competency should be assessed on theLifelong Learning (perhaps with portfolio reviews), Recertification Ex-

Patient Care Core Competencies 67
amination (most likely through MCQs), and Practice Assessment Com-ponents.
Again, program directors could do a great deal in teaching their resi-dents to be competent in this area, and public and professional percep-tions could be used for validation.
Summary
The Patient Care Category of the core competency outline is divided intothree sections: a general section, a psychiatry-specific section, and a neu-rology-specific section. Only the first two sections have been discussedhere (see Table 5–1 for summary). Neurology Patient Care Core Compe-tencies are covered in Chapter 11 (“Cross Competencies”) of this book,which deals with what psychiatrists need to know about neurology fortheir clinical practice.
All of the core competencies in the Patient Care Category of the out-line were judged to be of highest priority in terms of assessment. Most ofthem are currently being assessed by the ABPN written certification (Part I)or oral certification (Part II) examinations, but some topics lend them-selves more easily than others to an MCQ format. All of the core com-petencies could be assessed using the ABPN oral certification (Part II)examination, but the competency involving therapeutic skills (the thirdpsychiatry-specific core competency) could prove both cost- and time-prohibitive.
For all Patient Care Core Competencies, it was agreed that the resi-dency program faculty would be key teachers in assisting residents inmastering these core competencies. Feedback during the learning processwould be important so that remediation, when needed, could occur. Ini-tial assessments by program directors could also serve to hone and perfectskills. It is possible that at some point these core competencies could beassessed during residency, but for certification purposes this would haveto be done with the use of an outside evaluator to eliminate conflict-of-interest issues that program directors might have.
Portfolio development, currently in use in some programs to a minorextent, could serve as a possible means of evaluation as long as the focusis on the content of the portfolio and not on its format or facade.
All of the Patient Care Core Competencies could be validated by mea-surements of perception of the public (singularly represented in each pa-tient) and various professions with which psychiatrists interact (generalphysicians, other psychiatrists, nurses, social workers, etc.).

68 Core Competencies and the Practice of Psychiatry Today
Table 5–1. Summary of Patient Care Core Competencies
General Core Competencies1. The physician shall demonstrate the ability to perform and document a
relevant history and examination on culturally diverse patients1 to include as appropriate:A. Chief complaintB. History of present illnessC. Past medical historyD. Review of systemsE. Family historyF. Sociocultural history2
G. Developmental history (especially for children)
2. The physician shall demonstrate the ability to delineate appropriate differential diagnoses.
3. The physician shall demonstrate the ability to evaluate, assess, and recommend effective management of patients.
Psychiatry-Specific Core Competencies1. Based on a relevant psychiatric assessment, the physician shall demonstrate
the ability to develop and document the following:A. A complete multiaxial differential diagnosisB. An evaluation plan, including appropriate medical, laboratory,
radiological, and psychological examinationsC. A comprehensive treatment plan addressing biological, psychological,
and sociocultural domains
2. Based on a comprehensive psychiatric assessment, the physician shall demonstrate the ability to comprehensively assess and document patient’s potential for self-harm or harm to others. This shall include the following:A. An assessment of riskB. Knowledge of involuntary treatment standards and proceduresC. Ability to intervene effectively to minimize riskD. Ability to implement prevention methods against self-harm and harm to
others
3. Based on a comprehensive psychiatric assessment, the physician shall demonstrate the following abilities:A. To conduct therapeutic interviews, e.g., enhance the ability to collect
and use clinically relevant material through the conduct of supportive interventions, exploratory interventions, and clarifications
B. To conduct a range of individual, group, and family therapies, using stan-dard, accepted models, and to integrate these psychotherapies in multi-modal treatment, including biological and sociocultural interventions
4. Based on a comprehensive psychiatric assessment, the physician shall demonstrate the ability to recognize and treat psychiatric disorders.
1See footnote 1, p. 60, this chapter. 2See footnote 2, p. 60, this chapter.

69
Chapter 6
General and Psychiatry-Specific Medical Knowledge Core Competencies
Daniel K. Winstead, M.D.
Assumptions Regarding the Medical Knowledge Core Competencies
The group discussing the Medical Knowledge Core Competency Cate-gory of the outline made several initial assumptions, just as the group dis-cussing the Patient Care Core Competencies had done (see Chapter 5:“General and Psychiatry-Specific Patient Care Core Competencies”):
• Every competency listed for them to consider was already being as-sessed by cognitive examinations, such as the American Board ofPsychiatry and Neurology (ABPN) written certification (Part I) exam-ination; by clinical examinations such as the ABPN oral certification(Part II) examination; or by both. For the purposes of discussion here,all Medical Knowledge Core Competencies are, in fact, represented insome way on both the ABPN written examination and oral examina-tions; two minor variants from this will be discussed separately.
• All of the Medical Knowledge Core Competencies would be of the high-est priority for both training and assessment purposes. Minor variationsfrom this general statement will be discussed as they arise in the text.

70 Core Competencies and the Practice of Psychiatry Today
• All of the Medical Knowledge Core Competencies could be validatedas core competencies through use of surveys of the field. This assump-tion proved valid throughout the Medical Knowledge Category of theoutline.
The General Medical Knowledge Core Competencies
The First General Medical KnowledgeCore Competency
The physician shall demonstrate knowledge of the major disorders, including the following:
A. The epidemiology of the disorderB. The etiology of the disorder, including medical, genetic, and
sociocultural factorsC. The phenomenology of the disorderD. Diagnostic criteriaE. Effective treatment strategiesF. Course and prognosis
The discussants clearly saw this core competency as currently beingassessed through cognitive examinations, such as the ABPN written cer-tification (Part I) examination, and clinical examinations, such as the cur-rent ABPN oral certification (Part II) examination. In addition, the groupclearly thought that this competency should be assessed on recertifica-tion examinations and possibly also as part of the Practice AssessmentComponent of the ABPN Maintenance of Certification (MOC) Program.
Methodologies for assessing this competency included in-training eval-uations, cognitive examinations, and portfolio development. In-trainingevaluations could take a variety of forms but would be administered byprogram directors. The primary goal in this context would be to identifyand assist residents who need remediation. Cognitive examinationswould include the multiple-choice questions (MCQs) of the ABPN writ-ten certification (Part I) examination and recertification examinations.Portfolio assessment would most likely be used when actual practice is as-sessed as part of the MOC Program.

Medical Knowledge Core Competencies 71
The Second General Medical Knowledge Core Competency
The physician shall demonstrate knowledge of healthcare delivery systems, including patient and family counseling.
Discussants saw this competency as being evaluated through cognitiveand oral examinations and through the Practice Assessment Componentof the MOC Program. Examinations could be part of the training pro-gram and/or part of the ABPN certification process. This competencywas one of the very few in the Medical Knowledge Category that did notassume a place of first priority among the competencies needing to be as-sessed. It was ranked, in fact, among the lowest priorities for assessment.
The Third General Medical Knowledge Core Competency
The physician shall demonstrate knowledge of ethics in psychiatry/neurology.
Ethics can be difficult to assess, but the discussion group thought thatcognitive ethical questions could be formulated for MCQ examinationsand for clinical testing situations. The group also thought that this com-petency could be evaluated through the Practice Assessment Componentof the MOC Program. Assessment of this competency could take placein training and/or at the time of certification. It was also thought thatstate licensing bodies would be involved with the assessment of ethicsthrough their licensure programs.
The Fourth General Medical Knowledge Core Competency
The physician shall demonstrate the ability to reference and utilize electronic systems to access medical, scientific, and patient information.
The group believed that although this core competency did not war-rant assessment at this time, it should be considered soon for implemen-tation.

72 Core Competencies and the Practice of Psychiatry Today
Psychiatry-Specific Medical Knowledge Core Competencies
The First Psychiatry-Specific Medical Knowledge Core Competency
The physician shall demonstrate knowledge of human growth and development, including normal biological, cognitive, and psychosexual development, including sociocultural factors.
The discussants felt that this competency could be assessed withMCQs, in-training evaluations, patient interviews, and portfolio reviews.Regarding certification, they saw this competency as being assessedthrough the ABPN written certification (Part I), and oral certification(Part II) examinations and the recertification examinations.
The Second Psychiatry-Specific Medical Knowledge Core Competency
The physician shall demonstrate knowledge of behavioral science and social psychiatry, including
A. Learning theoryB. Theories of normal family organization, dynamics, and communicationC. Theories of group dynamics and processD. Anthropology, sociology, and theology as they pertain to clinical
psychiatryE. Transcultural psychiatryF. Community mental healthG. EpidemiologyH. Research methodology and statisticsI. Psychodynamic theory
For discussion purposes, the listing of knowledge areas was divided inhalf, and with very different results. Areas A through D were thought tobe worthy of assessment through in-training evaluations, MCQs, oral ex-aminations, and portfolios. The discussion group clearly thought thatthese points should be covered on the ABPN written certification (Part I)and oral certification (Part II) examinations for initial certification and onthe recertification examinations as a part of the MOC Program.
Areas E through I were debated; consensus was that these items shouldnot be assessed as core competencies at this time but that future discus-sion would dictate how and when these skills should be assessed.

Medical Knowledge Core Competencies 73
The Third Psychiatry-Specific Medical Knowledge Core Competency
The physician shall demonstrate knowledge of patient evaluation and treatment selection, including
A. Psychological testingB. Laboratory testingC. Mental status examinationD. Diagnostic interviewingE. Treatment comparison and selectionF. Psychosocial therapies, including
1. All forms of psychotherapies
a. Brief therapyb. Cognitive-behavioral therapyc. Psychodynamic therapyd. Psychotherapy combined with psychopharmacologye. Supportive therapy
2. All delivery systems of psychotherapies
a. Individualb. Groupc. Family
3. Treatments of psychosexual dysfunctions4. Doctor-patient relationships
G. Somatic treatments, including
1. Pharmacotherapy, including the antidepressants, antipsychotics, anxiolytics, mood stabilizers, hypnotics, and stimulants, including their
a. Pharmacological actionsb. Clinical indicationsc. Side effectsd. Drug interactionse. Toxicitiesf. Appropriate prescribing practicesg. Cost-effectiveness
2. Electroconvulsive therapy3. Light therapy
H. Emergency psychiatry, including
1. Suicide2. Crisis interventions3. Differential diagnoses in emergency situations4. Treatment methods in emergency situations5. Homicide, rape, and other violent behavior

74 Core Competencies and the Practice of Psychiatry Today
I. Substances of abuse, including
1. Pharmacological actions of substances of abuse
2. Signs and symptoms of toxicity3. Signs and symptoms of withdrawal4. Management of toxicity and withdrawal5. Epidemiology, including sociocultural factors
J. Child and adolescent psychiatry, including
1. Assessment and treatment of children and adolescents2. Disorders usually first diagnosed in infancy, childhood, or
adolescence3. Mental retardation and other developmental disabilities
K. Geriatric psychiatry
L. Forensic psychiatry
M. Consultation-liaison psychiatry, including
1. Specific syndromes, e.g., stress reactions, postpartum disorders, pain syndromes, postsurgical and ICU reactions, etc.
2. The psychiatric and neurological aspects of nonpsychiatric illness
3. The psychiatric and neurological complications of nonpsychiatric treatments
4. Psychosomatic and somatopsychic disorders5. Models of consultation psychiatry6. Coping strategies for patients with chronic illnesses, terminal
illnesses, etc.7. Ethical issues regarding consent to treatment in medical
settings8. Evaluating and treating difficult medical patients
This very long list of Medical Knowledge Competencies was not dis-cussed in total, but rather it was broken into nine small discussion areas,with points A through E being discussed together and each other letteredsection being discussed separately.
For this entire listing, the discussion group felt that these knowledgecompetencies could be assessed on cognitive and oral examinations. Thediscussants also concluded that, with the exception of points A throughF, evaluation on the Practice Assessment Component of the MOC Pro-gram would also be appropriate.
All of the items above, with the exception of child and adolescent psy-chiatry (point J) and forensic psychiatry (point L), were held to be of thehighest priority for assessment purposes. Child and adolescent psychiatryand forensic psychiatry, being subspecialty certification areas, were thoughtto be of a lesser, but not a low, priority. Geriatric psychiatry (point K),

Medical Knowledge Core Competencies 75
also a subspecialty certification area, was considered to be mainstreamenough to be of highest priority.1
The discussion group felt that all of the knowledge competencies inthis area should be assessed on in-training, initial certification, and re-certification examinations. Most could also be assessed through thedevelopment of a portfolio reporting clinical cases seen by the candidate.In addition, the group thought that psychosocial therapies (point F)could be assessed with standardized psychotherapy vignettes, somatictreatments (point G) could be assessed during training through patientlogs, and emergency psychiatry (point H) could be assessed by peer re-view.
Summary
The Medical Knowledge Category of the core competency outline as dis-cussed at the Core Competencies Conference is divided into three sec-tions: a general section, a psychiatry-specific section, and a neurology-specific section. Only the first two sections are discussed here (see Table6–1 for summary). Neurology Medical Knowledge Core Competenciesare covered in Chapter 11 (“Cross Competencies”) of this book, whichdeals with what psychiatrists need to know about neurology for theirclinical practice.
All of the core competencies in the Medical Knowledge Category ofthe outline were judged to be of highest priority in terms of assessment,with the exception of the following:
• Knowledge of administrative medicine and healthcare delivery sys-tems (the second core competency in the general section), which wasjudged to be of low priority for assessment purposes
• Certain aspects of behavioral science and social psychiatry (transculturalpsychiatry, community mental health, epidemiology, and researchmethodology and statistics, all part of the second psychiatry-specificcore competency), which were not to be assessed as core competenciesat this time
1Discussion after the conference separated points J (child and adolescent psychi-atry), K (geriatric psychiatry), L (forensic psychiatry), and M (consultation-liaison psychiatry) from the third psychiatry-specific competency into a sectionentitled “Psychiatric Subspecialties and Other Areas of Psychiatric Endeavor.”Addiction psychiatry was also added to this section. This section became thefourth psychiatry-specific core competency area.

76 Core Competencies and the Practice of Psychiatry Today
Table 6–1. Summary of Medical Knowledge Core Competencies
General Core Competencies1. The physician shall demonstrate knowledge of the major disorders, including
A. The epidemiology of the disorderB. The etiology of the disorder, including medical, genetic, and
sociocultural factorsC. The phenomenology of the disorderD. Diagnostic criteriaE. Effective treatment strategiesF. Course and prognosis
2. The physician shall demonstrate knowledge of healthcare delivery systems, including patient and family counseling.
3. The physician shall demonstrate knowledge of ethics in psychiatry/neurology.
4. The physician shall demonstrate the ability to reference and utilize electronic systems to access medical, scientific, and patient information.
Psychiatry-Specific Core Competencies1. The physician shall demonstrate knowledge of human growth and
development, including normal biological, cognitive, and psychosexual development, including sociocultural factors.
2. The physician shall demonstrate knowledge of behavioral science and social psychiatry, including
A. Learning theoryB. Theories of normal family organization, dynamics, and communicationC. Theories of group dynamics and processD. Anthropology, sociology, and theology as they pertain to clinical
psychiatryE. Transcultural psychiatryF. Community mental healthG. EpidemiologyH. Research methodology and statisticsI. Psychodynamic theory
3. The physician shall demonstrate knowledge of patient evaluation and treatment selection, includingA. Psychological testingB. Laboratory testingC. Mental status examinationD. Diagnostic interviewingE. Treatment comparison and selection

Medical Knowledge Core Competencies 77
Psychiatry-Specific Core Competencies (continued)F. Psychosocial therapies, including
1. All forms of psychotherapiesa. Brief therapyb. Cognitive-behavioral therapyc. Psychodynamic therapyd. Psychotherapy combined with psychopharmacologye. Supportive therapy
2. All delivery systems of psychotherapiesa. Individualb. Groupc. Family
3. Treatments of psychosexual dysfunctions4. Doctor-patient relationships
G. Somatic treatments, including
1. Pharmacotherapy, including the antidepressants, antipsychotics, anxiolytics, mood stabilizers, hypnotics, and stimulants, including theira. Pharmacological actionsb. Clinical indicationsc. Side effectsd. Drug interactionse. Toxicitiesf. Appropriate prescribing practicesg. Cost-effectiveness
2. Electroconvulsive therapy3. Light therapy
H. Emergency psychiatry, including
1. Suicide2. Crisis interventions3. Differential diagnoses in emergency situations4. Treatment methods in emergency situations5. Homicide, rape, and other violent behavior
I. Substances of abuse, including
1. Pharmacological actions of substances of abuse2. Signs and symptoms of toxicity3. Signs and symptoms of withdrawal4. Management of toxicity and withdrawal5. Epidemiology, including sociocultural factors
Table 6–1. Summary of Medical Knowledge Core Competencies (continued)

78 Core Competencies and the Practice of Psychiatry Today
• Child and adolescent psychiatry and forensic psychiatry (both part ofthe third psychiatry-specific core competency), which were judged tobe of secondary importance for assessment purposes
Formal assessment of these competencies would be done by the ABPNfor initial certification and on the recertification examinations. In addi-tion, most of these competencies could also be evaluated under the Prac-tice Assessment Component of the MOC Program. Portfolio assessmentof most of these competencies could serve as a possible means of evalua-tion.
For all Medical Knowledge Core Competencies, it was agreed that theresidency program faculty would be key teachers in assisting their resi-dents in mastering these core competencies. As with any educational set-ting, feedback during the learning process would be important so thatremediation, when needed, could occur.
All of the Medical Knowledge Core Competencies could be validatedby surveys of the field to determine that they are, in fact, core competen-cies for psychiatrists.
Psychiatry-Specific Core Competencies (continued)J. Child and adolescent psychiatry, including
1. Assessment and treatment of children and adolescents2. Disorders usually first diagnosed in infancy, childhood, or
adolescence
3. Mental retardation and other developmental disabilitiesK. Geriatric psychiatryL. Forensic psychiatryM. Consultation-liaison psychiatry, including
1. Specific syndromes, e.g., stress reactions, postpartum disorders, pain syndromes, postsurgical and ICU reactions, etc.
2. The psychiatric and neurological aspects of nonpsychiatric illness3. The psychiatric and neurological complications of nonpsychiatric
treatments4. Psychosomatic and somatopsychic disorders5. Models of consultation psychiatry6. Coping strategies for patients with chronic illnesses, terminal
illnesses, etc.7. Ethical issues regarding consent to treatment in medical settings8. Evaluating and treating difficult medical patients
Table 6–1. Summary of Medical Knowledge Core Competencies (continued)

79
Chapter 7
Interpersonal and Communications Skills Core Competencies
Michael H. Ebert, M.D.
Assumptions Regarding the Six Categories of Core Competencies
The core competencies under discussion in this book are divided into sixcategories:
• Patient Care• Medical Knowledge• Interpersonal and Communications Skills• Practice-Based Learning and Improvement• Professionalism• Systems-Based Practice
The first two categories of core competencies, Patient Care (discussedin Chapter 5: “General and Psychiatry-Specific Patient Care Core Com-petencies”) and Medical Knowledge (discussed in Chapter 6: “Generaland Psychiatry-Specific Medical Knowledge Core Competencies”) arealike in that they are each divided into three sections: general, psychiatryspecific, and neurology specific. In each of the preceding two chapters,only the general and psychiatry-specific sections were discussed. To theextent necessary, the core competencies that are neurology specific willbe discussed in the chapter on cross competencies (Chapter 11). The fo-cus therein will be on what psychiatrists need to know about neurology.

80 Core Competencies and the Practice of Psychiatry Today
At the American Board of Psychiatry and Neurology (ABPN) Invita-tional Conference on Core Competencies, there was consensus that thefirst two categories of core competencies (Patient Care and Medical Knowl-edge) would need to have specialty-specific components in addition to ageneral category. Unlike for those two categories of core competencies,the consensus was also that it was likely that the next three categories ofcore competencies (Interpersonal and Communications Skills, Practice-Based Learning and Improvement, and Professionalism) would probablycontain competencies that would be (or could be) applicable to mostmedical specialties. The last category of core competencies, Systems-Based Practice, could most likely be common for most medical specialtiesbut may need special sections for psychiatry.
If it turns out that the last four categories of core competencies are ei-ther the same or similar for most medical specialties, the American Boardof Medical Specialties (ABMS) could assist the 24 specialty boards in co-ordinating efforts to define the specific competencies for these areas.With this possible future endeavor, it is anticipated that the ABMS willwork closely with its member boards that have already attempted delin-eation of these categories.
With this rationale, this chapter on Interpersonal and Communica-tions Skills and the two following it (Chapter 8: “Practice-Based Learningand Improvement Core Competencies” and Chapter 9: “ProfessionalismCore Competencies”) will assume less of a psychiatry-specific view andmore of a global view of medical core competencies.
Assumptions Regarding the Interpersonal and Communications Skills Core Competencies
As the physician-patient relationship is central to any healthcare pro-gram, it is logical that the core competencies in the Interpersonal andCommunication Skills Section are of great importance. Therefore, it wasassumed that the majority of competencies listed in this category wouldbe of highest priority for assessment purposes. Those rated differentlywill be discussed as they appear in the listing below.
It was generally assumed that almost all of these competencies shouldbe assessed through oral examinations with either actual or simulatedpatients; it was also assumed that the majority of these competenciesshould be evaluated under the Practice Assessment Component of theABPN Maintenance of Certification (MOC) Program.

Interpersonal and Communications Skills Core Competencies 81
The Interpersonal and Communications Skills Core Competencies
The First Interpersonal and Communications Skills Core Competency1
Points A Through C
The physician shall demonstrate the following abilities:
A. Listen to and understand patients and attend to nonverbal communicationB. Communicate effectively with patients, using verbal, nonverbal, and
written skills as appropriateC. Develop and maintain a therapeutic alliance with patients by instilling
feelings of trust, honesty, openness, rapport, and comfort in the relationship with the physician
This grouping of core competencies could be evaluated on oral exam-inations that use points similar to those of the ABPN oral certification(Part II) examination. The discussion group decided that this was alreadybeing done adequately for points A and B (see above) but inadequatelyfor point C. It was also thought that all three points should be evaluatedunder the Practice Assessment Component of the MOC Program.
Generally, in an oral examination with an actual or simulated patient,the patient is not asked to rate the physician (resident or ABPN certifica-tion candidate). Gathering information from the patient, however, couldbe a viable option for the future as long as what the patient was asked torate was under the patient’s purview. Thus, it would be logical that pa-tients could rate residents or ABPN certification candidates on points Aand B. Patients could express their opinions as to whether or not the phy-sician seemed to listen to and understand them and if the physician com-municated effectively (from the patient’s point of view). In fact, no oneother than the patient can rate what the patient thought about these twoissues. An external rater, such as a program director or an examiner, couldalso rate the physician-patient encounter, but the best judge of these twopoints would probably be the patient himself or herself.
1During the discussion of the first interpersonal and communications skills sec-tion of the core competency outline, essentially every point and subpoint werediscussed separately. For the sake of presentation here, points that follow oneanother will be discussed together when the discussion of them is either thesame or similar. Important differences will be noted.

82 Core Competencies and the Practice of Psychiatry Today
This situation is, however, not true for point C. The patient could notbe logically asked to ascertain if a therapeutic alliance with him or herhad been developed and maintained. A patient could report on the estab-lishment of rapport but not on the creation of a therapeutic alliance. Thisevaluation would have to be done by a medically qualified external per-son, most likely a physician observer.
The discussion group thought that an external reviewer could validatethese three related competencies.
Points D Through F
(Continued) The physician shall demonstrate the following abilities:
D. Partner with patients to develop an agreed-on healthcare management plan with patients
E. Transmit information to patients in a clear, meaningful fashionF. Understand the impact of the physician’s own feelings and behavior on
treatment
Point D above was judged to be of less importance than the precedingthree Points (A, B, and C) or points E and F listed above. Also, the dis-cussion group decided that point D, the physician’s skill in negotiating ahealthcare management plan with patients, could be assessed using mul-tiple-choice questions (MCQs), especially those of the branching variety.Such MCQs would have to be very carefully worded. Oral examinationscould also be used to assess negotiation skills.
The discussion group decided that points E and F, the physician’s abil-ities to transmit information to patients and to understand the impact ofhis or her own feelings and behavior on the treatment, could be best as-sessed in some type of oral interview or patient observation process, mostlikely one that used vignettes or objective-structured clinical exami-nations (OSCEs). It was decided that points D, E, and F all could andshould be evaluated under the Practice Assessment Component of theMOC Program. This evaluation would also serve as the validation forthese skills.
Consistent with the discussion above, the group decided that the ne-gotiating skills of a physician (point D) could be assessed with branchinglogic questions, for example, on an MCQ examination. Points E and Fwould be better assessed using vignettes or OSCEs. Testing the extent towhich a physician understands the impact of his or her own feelings andbehavior on treatment for the patient could also be assessed in an oral ex-amination.

Interpersonal and Communications Skills Core Competencies 83
Points G and H
(Continued) The physician shall demonstrate the following abilities:
G. Communicate effectively and work collaboratively with allied healthcare professionals and with other professionals involved in the lives of patients
H. Educate patients, professionals, and the public about medical, psychosocial, and behavioral issues
Of these two points, the first listed above, the physician’s ability towork collaboratively with a healthcare team of professionals, was thoughtto be of higher priority than the second point.
In discussion, the group saw that point G would require some type oforal assessment for initial certification purposes and would also requireevaluation under the Practice Assessment Component of the MOC Pro-gram. The group also thought both vignettes and OSCEs would be suit-able methodologies for assessing competence for this skill.
Point H, the physician’s ability to educate patients, professionals, andthe public about medical, psychological, and social issues, was clearlyseen as a skill that develops slowly over the individual professional’s lifefrom residency into and through practice. A physician in residency train-ing or even in early practice could not be expected to have this skill toany measurable level. This is clearly a skill that develops with experienceand maturity. The discussion group believed that the physician should beheld accountable under the Lifelong Learning Component of the MOCProgram to show evidence of study to have the current information to beable to communicate to patients and others. The process of communicat-ing that information or of educating others could be assessed through oralexaminations, vignettes, and OSCEs. The group decided that this partic-ular skill should be documented under both the Lifelong Learning Com-ponent and the Practice Assessment Component of the MOC Program.
The Second Interpersonal and Communications Skills Core Competency
The physician shall demonstrate the ability to elicit important diagnostic data and data affecting treatment from individuals from the full spectrum of ethnic, racial, gender, and educational backgrounds. This will include skills in tolerating and managing highly charged affect in patients.

84 Core Competencies and the Practice of Psychiatry Today
This competency, rated at the highest priority, clearly has training im-plications that can be assessed almost continuously throughout residency.Assessment of this multifaceted competency could be done through MCQs,oral interviews with either actual or standardized patients, vignettes, andOSCEs. The discussion group clearly saw this competency as needingevaluation under the Practice Assessment Component of the MOC Pro-gram.
The Third Interpersonal and Communications Skills Core Competency
The physician shall demonstrate the ability to obtain, interpret, and evaluate consultations from other medical specialties. This shall include
A. Knowing when to solicit consultation and being sensitive to one’s resistance to the need for consultation
B. Discussing the consultation findings with patients and their familiesC. Evaluating the consultation findings
The three skills listed as parts of this competency are clearly related,and the group saw them as being of the highest importance. All skillscould be assessed through simple MCQs and oral interviews. Other meth-odologies suggested for use in evaluating these skills included branchinglogic questions, vignettes, and OSCEs. All skills could be validatedthrough the Practice Assessment Component of the MOC Program.
The Fourth Interpersonal and Communications Skills Core Competency
The physician shall serve as an effective consultant to other medical specialists, mental health professionals, and community agencies. The physician shall demonstrate the ability to
A. Communicate effectively with the requesting party to refine the consultation question
B. Maintain the role of consultantC. Communicate clear and specific recommendationsD. Respect the knowledge and expertise of the requesting professional
The related skills of this competency were judged to be of the highestpriority for assessment purposes. They could be assessed with MCQs,oral interviews, vignettes, OSCEs, and branching logic questions. The dis-

Interpersonal and Communications Skills Core Competencies 85
cussion group saw these skills as needing evaluation under the PracticeAssessment Component of the MOC Program.
The Fifth Interpersonal and Communications Skills Core Competency
The physician shall demonstrate the ability to communicate effectively with patients and their families by
A. Gearing all communication to the educational/intellectual levels of patients and their families
B. Demonstrating sociocultural sensitivity to patients and their familiesC. Providing explanations of psychiatric and neurological disorders and
treatment that are jargon-free and geared to the educational/intellectual level of patients and their families
D. Providing preventive education that is understandable and practicalE. Respecting patients’ cultural, ethnic, religious, and economic
backgroundsF. Developing and enhancing rapport and a working alliance with patients
and their families
These related skills were thought, much as were most others in thiscategory, to be of the highest priority for assessment purposes. The dis-cussion group saw these skills as being assessed through MCQs, oral ex-aminations, OSCEs, and branching logic questions. They also saw theseskills as being able to be validated through the Practice Assessment Com-ponent of the MOC Program.
The Sixth Interpersonal and Communications Skills Core Competency
The physician shall maintain medical records and written prescriptions that are legible and up-to-date. These records must capture essential informa-tion while simultaneously respecting patient privacy and be useful to health professionals outside psychiatry and neurology.
This core competency is unlike most of the other competencies dis-cussed in this and other sections of the outline in that it is clearly a prac-tice issue. Although residents can be taught to create records that arelegible, it takes an ongoing practice to assess how current the records are,how well the records respect patients’ privacy, and if the records are use-ful to other medical professionals. Thus, this competency, judged to be of

86 Core Competencies and the Practice of Psychiatry Today
priority importance, can be evaluated only as part of the Practice Assess-ment Component of the MOC Program.
The Seventh Interpersonal and Communications Skills Core Competency
The physician shall demonstrate the ability to effectively lead a multidisci-plinary treatment team, including being able to
A. Listen effectivelyB. Elicit needed information from team membersC. Integrate information from different disciplinesD. Manage conflictE. Clearly communicate an integrated treatment plan
This competency represents a skill set of secondary importance; effec-tively leading a multidisciplinary team is clearly secondary to practicingexcellent medicine. It is, nonetheless, an important skill, one that resi-dents can learn and practice during training and one that mature, well-established physicians in some specialties practice daily. Like the corecompetency immediately preceding it, this skill can be evaluated only aspart of the Practice Assessment Component of the MOC Program.
The Eighth Interpersonal and Communications Skills Core Competency
The physician shall demonstrate the ability to communicate effectively with patients and their families while respecting confidentiality. Such communi-cation may include
A. The results of the assessmentB. Use of informed consent when considering investigative proceduresC. Genetic counseling and palliative care when appropriateD. Consideration and compassion for the patient in providing accurate
medical information and prognosisE. The risks and benefits of the proposed treatment plan, including
possible side effects of medications and/or treatmentsF. Alternatives (if any) to the proposed treatment planG. Appropriate education concerning the disorder, its prognosis, and
prevention strategies
This important communications skill was judged to be of the highestpriority. The discussion group saw this competency as needing to be eval-

Interpersonal and Communications Skills Core Competencies 87
uated at multiple points in a physician’s training and career. They decidedthat this skill set could be assessed through well-written MCQs, oral ex-aminations, vignettes, and OSCEs. The discussion group also saw thisskills set as being assessed under three components of the MOC Program:Lifelong Learning, Recertification Examinations, and Practice Assess-ment.
Validation of the skills composing this core competency could be val-idated through the Practice Assessment Component of the MOC Pro-gram, through outcome studies (for points A through D listed above),and by self-report (for points E through G listed above).
Summary
The Interpersonal and Communications Skills Core Competency Cate-gory of the outline represents the first to be described that could be saidto be essentially common across all specialties (see Table 7–1 for sum-mary). Although the items described in this chapter came from the workof specific specialty groups, it is anticipated that other specialty groupswould come up with essentially the same list of competencies.
All of the skills making up the competencies in this section were judgedto be of highest importance, except for those skills that involved negoti-ating healthcare maintenance plans, educating patients and others, andworking as part of or leading a team of other health professionals. It is notthat these skills are not important; these skills are of secondary im-portance and can be assessed after the more essential skills have beenaddressed. A more valid assessment of these skills may also be possibleonly after the physician has had some time to develop them in practice.
Although the discussion group suggested MCQs as evaluation tools formany of the skills within this section of competencies, it must be remem-bered that MCQs that assess interpersonal and communications skills aredifficult to write. Far more logical for the evaluation of these skills wouldbe oral examinations, observations of physician-patient interactions, vi-gnettes, and OSCEs. For a limited number of these skills, assessmentcould be handled by consulting with the person receiving the communi-cation, whether that be a patient, a nurse, another physician, or anotherhealth professional.
The core competencies listed in this area are worthy of constant assess-ment from residency training and all through practice.

88 Core Competencies and the Practice of Psychiatry Today
Table 7–1. Summary of Interpersonal and Communications Skills Core Competencies
1. The physician shall demonstrate the following abilities:A. Listen to and understand patients and attend to nonverbal
communicationB. Communicate effectively with patients, using verbal, nonverbal, and
written skills as appropriateC. Develop and maintain a therapeutic alliance with patients by instilling
feelings of trust, honesty, openness, rapport, and comfort in the relationship with the physician
D. Partner with patients to develop an agreed-on healthcare management plan with patients
E. Transmit information to patients in a clear, meaningful fashionF. Understand the impact of the physician’s own feelings and behavior on
treatmentG. Communicate effectively and work collaboratively with allied
healthcare professionals and with other professionals involved in the lives of patients
H. Educate patients, professionals, and the public about medical, psychosocial, and behavioral issues
2. The physician shall demonstrate the ability to elicit important diagnostic data and data affecting treatment from individuals from the full spectrum of ethnic, racial, gender, and educational backgrounds. This will include skills in tolerating and managing highly charged affect in patients.
3. The physician shall demonstrate the ability to obtain, interpret, and evaluate consultations from other medical specialties. This shall includeA. Knowing when to solicit consultation and being sensitive to one’s
resistance to the need for consultationB. Discussing the consultation findings with patients and their familiesC. Evaluating the consultation findings
4. The physician shall serve as an effective consultant to other medical specialists, mental health professionals, and community agencies. The physician shall demonstrate the ability toA. Communicate effectively with the requesting party to refine the
consultation questionB. Maintain the role of consultantC. Communicate clear and specific recommendationsD. Respect the knowledge and expertise of the requesting professional

Interpersonal and Communications Skills Core Competencies 89
5. The physician shall demonstrate the ability to communicate effectively with patients and their families byA. Gearing all communication to the educational/intellectual levels of
patients and their familiesB. Demonstrating sociocultural sensitivity to patients and their familiesC. Providing explanations of psychiatric and neurological disorders and
treatment that are jargon-free and geared to the educational/intellectual level of patients and their families
D. Providing preventive education that is understandable and practicalE. Respecting patients’ cultural, ethnic, religious, and economic
backgroundsF. Developing and enhancing rapport and a working alliance with patients
and their families
6. The physician shall maintain medical records and written prescriptions that are legible and up-to-date. These records must capture essential information while simultaneously respecting patient privacy and be useful to health professionals outside psychiatry and neurology.
7. The physician shall demonstrate the ability to effectively lead a multidisciplinary treatment team, including being able toA Listen effectivelyB. Elicit needed information from team membersC. Integrate information from different disciplinesD. Manage conflictE. Clearly communicate an integrated treatment plan
8. The physician shall demonstrate the ability to communicate effectively with patients and their families while respecting confidentiality. Such communication may includeA. The results of the assessmentB. Use of informed consent when considering investigative proceduresC. Genetic counseling and palliative care when appropriateD. Consideration and compassion for the patient in providing accurate
medical information and prognosisE. The risks and benefits of the proposed treatment plan, including possible
side effects of medications and/or treatmentsF. Alternatives (if any) to the proposed treatment planG. Appropriate education concerning the disorder, its prognosis, and
prevention strategies
Table 7–1. Summary of Interpersonal and Communications Skills Core Competencies (continued)

This page intentionally left blank

91
Chapter 8
Practice-Based Learning and Improvement Core Competencies
Larry R. Faulkner, M.D.
Discussion of the Practice-Based Learning and Improvement Core Competencies in Relation to Other Core Competency Categories
The Practice-Based Learning and Improvement Core Competency Cate-gory is different from the three previous sections. The focus of thiscompetency area is the practicing physician, and more specifically thelearning and improvement that comes to the physician through practice.The goal of this section is to stress planned, purposeful learning withoutdiscounting natural or serendipitous learning. This section of core com-petencies attempts to capitalize on all learning and structure it into a for-mal pattern that will benefit the individual physician and the patientpopulation being served.
This section of core competencies relates directly to the Maintenanceof Certification (MOC) Program©, which the American Board of Medi-cal Specialties (ABMS) is proposing to take the place of just a recertifica-tion examination. Not very many years ago, board certification was seenas the ultimate achievement for a physician. There was no formal planfor continuing the physician’s education after certification; it was as-sumed that a physician would learn what he or she needed to know whenhe or she needed to know it and would do so by choice.

92 Core Competencies and the Practice of Psychiatry Today
Medicine has always been a dynamic field, but never more so thanright now. Medical knowledge is expanding at such a phenomenal ratethat it is humanly impossible to keep up with all of the latest develop-ments. Yet it is imperative that physicians stay up-to-date with new knowl-edge. The ABMS, working through its specialty boards, has taken steps toguarantee medical learning after physician practice has begun.
Specialty boards, at the urging of the ABMS, are all moving to “time-limited certification,” which means that a physician, once initially board-certified, will remain certified only for a specified number of years. Forpsychiatrists, this period is 10 years. After the initial 10-year period ofcertification, the psychiatrist will have to become certified again (“recer-tified”) by taking a cognitive examination similar to the initial certi-fication examination. This new development was not necessarily wellreceived by younger physicians, who claimed that they were beingdiscriminated against compared with what had been allowed for moresenior physicians. For better or for worse, the senior physicians’ certifica-tion could not be changed after their having earned “lifetime certifica-tion”; rules cannot be changed after the fact.
The cry of unfair treatment became louder when the ABMS mandatedthat not only was a recertification examination to be required, but the ex-amination would have to be a secure, proctored examination as opposed toa take-home recertification examination to be completed at leisure. Thismandate for a secure, proctored examination was made at the request ofthe state licensing boards and institutions, which demanded assurance thatthe person taking the examination was the person he or she claimed to be.
After reflection, the ABMS decided that a cognitive examination, oc-cupying perhaps 4 hours each decade, did not seem to be enough to guar-antee that physicians’ knowledge and skill were up-to-date. They opinedthat the recertification examination needed to be a part of a larger pro-gram; thus, the MOC Program© was designed.
As envisioned by the ABMS, the MOC Program© would have four com-ponents, with the second listed here being directly related to the Practice-Based Learning and Improvement Core Competency Category being dis-cussed in this chapter:
1. Evidence of professional standing2. Evidence of lifelong learning and periodic self-assessment3. Evidence of cognitive expertise4. Evidence of evaluation of practice performance
The first requirement of the MOC Program©, evidence of professionalstanding, is neither new nor surprising. The American Board of Psychiatry

Practice-Based Learning and Improvement Core Competencies 93
and Neurology (ABPN) has always had this requirement of evidence ofprofessional standing. Evidence has taken the form of the requirement ofa full, unrestricted medical license, with documentation to be provided atthe time of registration for a certification examination. This requirementhas been in effect since 1935 for initial certification examinations andsince 2000, when the first recertification examinations were offered. Thereis currently no plan for the ABPN to change this requirement.
The second requirement of the MOC Program©, evidence of LifelongLearning and Periodic Self-Assessment, relates directly to the Practice-Based Learning and Improvement Core Competency Category of theoutline. While the rest of the chapter will explore this relationship, it isof value now to look at the component parts of this section of the MOCProgram©. ABMS guidelines specify that evidence of Lifelong Learningand Periodic Self-Assessment will require the following:
• Documentation of participation in specialty-specific educational ac-tivities
• Documentation of participation in specialty-specific self-assessmentactivities
• A relationship between the lifelong learning activities and perfor-mance standards
This section contains some interesting aspects. Among them are thefollowing:
• This section of the MOC Program© speaks of lifelong learning. Thus, itis assumed that the physician, simply by his or her status as a physi-cian, will be committed to some form of learning throughout his orher life.
• This section of the MOC Program© speaks of documentation of par-ticipation in educational activities. This implies that the learning aphysician will undertake while in practice cannot be serendipitous, hap-hazard, or left to chance. The learning must constitute some form oforganized activity, which of its nature implies both structure and goals.The discussion group indicated that it would be most beneficial if sucheducational activities were structured into some type of program.
• The use of the word participation is interesting, in that for most con-tinuing medical education (CME) programs, participation is generallyjudged by simply being present in the room where the activity is tak-ing place. (Sometimes not even that is required. The signing in at thebeginning of the activity or the payment of a registration fee sufficesfor enough participation to earn a CME certificate in some cases.) It ispossible that the ABPN and its sister boards may choose to define par-

94 Core Competencies and the Practice of Psychiatry Today
ticipation in terms of some form of assessment that demonstrates thatlearning has actually occurred. Pre- and posttests can measure cogni-tive gain, but generally the documentation of participation in the ed-ucational activity is in no way tied to the achievement on the posttest.
• The MOC Program© notes that the educational activities must be spe-cialty specific. This indicates that participation in a serendipitous arrayof activities will not suffice. Most of the lifelong learning required herewould probably emanate from relevant specialty societies. Some ABMSboards already require that a stated number of specialty-specific CMEhours be documented prior to a diplomate’s taking a recertification ex-amination.
• Besides specialty-specific, the discussion group also thought that theeducational activities should be relevant. “Specialty specific” is cer-tainly clear, but “relevant” is more ambiguous, as one must determinerelevance in relationship to what? Certainly, the CME should be rele-vant to the specialty, but relevance also relates to the physician partic-ipating in the activity. Most likely, relevance would be determined byuse of self-assessment examinations, as discussed below.
• Linking self-assessment programs to member board certification re-quirements appears to provide the clarity needed for determining anddesigning a specialty-specific and relevant CME program. This means, ofcourse, that member boards must have a self-assessment program linkedto their certification requirements. As most ABMS member boards arenot and do not want to be involved in education, even at the self-assessment level, this requirement also seems to offer an opportunityfor the member boards to partner with their appropriate specialty so-cieties to meet this requirement.
The third requirement of the MOC Program©, the recertification ex-amination, has been discussed earlier. This cognitive examination, in amultiple-choice question (MCQ) format for psychiatrists, is meant to as-certain (to the degree such an examination can do so) that the physicianis practicing medicine consistent with current medical knowledge andup-to-date treatment practices. Although the recertification examinationcould certainly retest basic science and other topics covered on the initialcertification examination, the ABPN plans for its specialty and sub-specialty recertification examinations to focus on practice issues. This isconsistent with the specifications of the ABMS that the recertificationexamination focus on current knowledge of clinical science and that it berelevant to maintenance of certification.
The fourth requirement of the MOC Program©, assessment of prac-tice-based performance, is the specialty board’s commitment to ensuring

Practice-Based Learning and Improvement Core Competencies 95
that the physicians’ patterns of practice meet acceptable standards. Thespecialty boards, with the support of the ABMS, are currently undertak-ing measures to determine how and when this assessment should takeplace and what its exact nature or form will be. This part of the ABPNMOC Program will probably not be available for implementation untillater in this decade.
Assumptions Regarding the Practice-Based Learning and Improvement Core Competencies
As explained by its title and in the discussion above, it is logical to assumethat core competencies in the Practice-Based Learning and ImprovementCategory of the core competency outline will be assessed at specifiedpoints during a physician’s practice as part of the mandated MOC Pro-gram. Thus, it can also be assumed that most, if not all, of the core com-petencies of this section will not have relevance for assessment purposesduring residency or at the time of initial certification. Residency training,done well, would lay an excellent groundwork for these competencies tobe established and maintained during practice.
A second assumption is that because the focus of the Practice-BasedLearning and Improvement Core Competencies is on the period of prac-tice (as opposed to the period of residency), the assessment of these corecompetencies would most aptly be part of the Lifelong Learning andPractice Assessment Components of the MOC Program.
The Practice-Based Learning and Improvement Core Competencies
During the core competencies conference, each subpoint of the sectionsof the Practice-Based Learning and Improvement Category was discussedseparately. That is how the points will be presented here, with groupingsoccurring only when discussion of them was essentially similar. Sub-points of the competencies listed for discussion below do not imply thatthey are of lesser importance than other main points.
The First Practice-Based Learning and Improvement Core Competency
The physician shall recognize and accept limitations in his or her own knowledge base and clinical skills and understand and address the need for lifelong learning.

96 Core Competencies and the Practice of Psychiatry Today
The discussion group concurred that in addition to recognizing andaccepting the limitations of his or her own knowledge, a physician mustalso acknowledge the need for continued learning and the importance ofconferring with other specialists and healthcare providers when the situ-ation warrants. This is critical for optimum patient care. For this reasonespecially, this competency was seen to be of highest priority.
The discussion group believed that this competency could initially beassessed during oral interviews, such as are held in residency and as partof the ABPN oral certification (Part II) examination. Special vignettescould be written for this purpose.
This competency should also receive additional assessment as part ofthe Lifelong Learning and Practice Assessment Components of theABPN MOC Program. Exactly how this competency would be assessedat those times was not discussed at length, but it would be logical to as-sume that a physician’s lack of knowledge in a given area would be themotivating force of his or her CME program. A database of CME activi-ties and of patient practice would be helpful for this assessment.
It is also logical to assume that an analysis of practice patterns wouldindicate where a physician decided that his or her knowledge, skills, orspecialty would be insufficient to treat a given patient; that would thenbe the point at which other specialists or healthcare providers would becalled in. Assessment of this practice component might be handled with360-degree evaluations (evaluations done by multiple people in a per-son’s sphere of influence, usually superiors, peers, subordinates, and pa-tients and their families).
The Second Practice-Based Learning and Improvement Core Competency
The physician shall demonstrate appropriate skills for obtaining and evaluating up-to-date information from scientific and practice literature and other sources to assist in the quality care of patients. This shall include, but not be limited to, the following:
A. Use of information technology, including Internet-based searches and literature databases (e.g., Medline); medical libraries; and drug information databases
B. Active participation, as appropriate, in educational courses, conferences, and other organized educational activities at both the local and national levels
This competency would be of critical importance to the Lifelong Learn-ing Component of the ABPN MOC Program. Within point A above, the

Practice-Based Learning and Improvement Core Competencies 97
discussion group agreed that the ability to use information technologylike the Internet is critical for today’s physician, as that it is through thatmedium that most new knowledge is first communicated. And, while itis likely that specialists, especially those in large practices, would not haveto perform literature searches on their own, they should always have theknowledge of how such searches are done in order to direct the work ofthose doing the Internet work. The discussion group decided that usingcase-based vignettes that would require library, Internet, or other re-search would be an excellent methodology for assessing point A of thiscompetency.
Point B of this competency also ties directly into the Lifelong LearningComponent of the ABPN MOC Program. It is, in fact, the basis for thecurrent CME infrastructure, that is, of a physician attending and par-ticipating actively in educational programs. In discussion, there were anumber of criticisms of the current CME situation. These included thefollowing:
• A physician self-selects his or her own CME activities. It is assumedthat the selection is based on need, but currently there is no way tolink attendance and participation at CME events to any type of indi-vidual physician needs assessment. For the learning from these educa-tional programs to be meaningful for the purposes of this competency,the learning must answer a specific need. This need could be real orperceived but would require being measured and documented. Vari-ous needs assessment processes could be used; these might include,but not be limited to, specialty-specific self-assessments, normed as-sessments, and mentor-assisted assessments.
• Left to one’s own devices, most people will choose to learn moreabout favorite subjects or participate in activities in which they al-ready have some degree of proficiency. Thus, areas in which a deficitof knowledge, a lack of skills, or a troublesome attitude is present maybe those areas specifically not selected for CME or other educationalactivities. In that case, the learning that comes about because of the se-lection of a particular educational activity is really an enhancement ofan already adequate area, not the meeting of a true need.
• CME activities are currently measured in credit hours. A physicianearns one CME credit hour for each 60 minutes spent attending an ed-ucational program. Thus, the currency is “seat-time,” not a measure oflearning. While seat-time might still be the currency used for measure-ment, this core competency demands that the change in knowledge,skills, or attitudes based on the educational activity be measured anddocumented.

98 Core Competencies and the Practice of Psychiatry Today
• The discussion group especially recommended that CME be specialty-specific to ensure that meaningful learning is taking place.
The Third Practice-Based Learning and Improvement Core Competency
The physician shall evaluate caseload and practice experience in a systematic manner. This may include, but not be limited to, the following:
A. Obtaining appropriate supervision and consultationB. Use of best practices through practice guidelines or clinical pathwaysC. Case-based learningD. Review of patient records and outcomesE. Obtaining evaluations from patients (e.g., their opinion of outcomes
and patient satisfaction)F. Maintaining a system for examining errors in practice and initiating
improvements to eliminate or reduce errors
This core competency asks the physician to evaluate himself or herself ac-cording to various parameters. The wording of this competency promptedsome discussion. Questions asked included the following:
• Will the evaluation be accomplished by the physician doing a self-assessment, or by an outside agent or group?
• What should be done with the results of that assessment? • If there is no follow-up from the assessment, what is the point of doing
it?• How can or should such an evaluation (and follow-up measures) be
documented?• What does “systematic” mean in this core competency? Who estab-
lishes the system? The physician? The specialty? Another agency? • If this core competency is to be considered as part of the MOC Program,
wouldn’t that imply that someone other than the physician himself orherself should be doing the assessment? And, if another does the assess-ment of the physician, the questions in the other bullets still remain tobe answered.
While these questions were not specifically answered, the fact thatthey were raised at all speaks to how difficult assessing the core compe-tencies in this section of the outline will be. It also points out the samedifficulties for standards to be set to address the Lifelong Learning andPractice Assessment Components of a MOC Program, to which thiscompetency clearly relates.

Practice-Based Learning and Improvement Core Competencies 99
Regarding point A above, the discussion group suggested that the useof best practices through practice guidelines or clinical pathways couldinitially be evaluated during oral interviews, such as the ABPN oral certi-fication (Part II) examination, using specially designed case vignettes andthen continued through a MOC Program.
The discussion group agreed that evidence would be needed demon-strating physician participation in some type of certified case-based qualityassurance program. They suggested further that it might be the specialtysocieties, such as the American Psychiatric Association, that should un-dertake this task.
The discussion group further suggested that specialty societies mightfind meaningful ways to assist with the assessment of the review of pa-tient records and outcomes and obtaining evaluations from patients.
Unlike most of the core competencies in the Practice-Based Learningand Improvement Category of the outline, which were deemed to be inthe middle range of priority for assessment, both points E and F of thiscore competency were rated as being of highest priority. Both pointscould be evaluated under the Lifelong Learning and Self-AssessmentComponent of a MOC Program, but could probably be evaluated morecompletely under the Practice Assessment Component of a MOC Pro-gram. The discussion group suggested a third-party evaluation for bothpoints E and F, with benchmarks being established by the ABPN.
The Fourth Practice-Based Learning and Improvement Core Competency
The physician shall demonstrate an ability to critically evaluate relevant medical literature. This ability may include, but not be limited to, the following:
A. Using knowledge of common methodologies employed in psychiatric and neurological research
B. Conducting and presenting reviews of current research in such formats as journal clubs, grand rounds, and/or original publications
C. Researching and summarizing a particular problem that derives from the physician’s caseload
The discussion group believed that point A of this core competency isevaluated on MCQ examinations, such as the ABPN written certification(Part I) examination, but that it could be evaluated in a more sophisti-cated manner than is being done currently. Besides on cognitive exami-nations, this core competency could also be assessed using vignettes and

100 Core Competencies and the Practice of Psychiatry Today
under the Lifelong Learning and Self-Assessment Component of a MOCProgram.
Point B of this core competency was one of the few in the entire corecompetency outline that was thought to be at a low priority level for as-sessment. The discussion group clearly saw this as being evaluated underthe Lifelong Learning Component of a MOC Program, perhaps throughdocumentation of the number of reviews submitted.
Point C of this core competency was seen as being evaluated under theLifelong Learning and Practice Assessment Components of a MOC Pro-gram. The methodology used for assessment could be the submission ofcase-based reports demonstrating the use of medical literature. The dis-cussion group decided that this assessment should most probably be doneby the ABPN.
The Fifth Practice-Based Learning and Improvement Core Competency
The physician shall demonstrate the ability to do the following:
A. Review and critically assess scientific literature to determine how quality of care can be improved in relation to one’s practice (e.g., reliable and valid assessment techniques, treatment approaches with established effectiveness, practice parameter adherence). Within this aim, the physician shall be able to assess the generalizability or applicability of research findings to one’s patients in relation to their sociodemographic and clinical characteristics.
B. Develop and pursue effective remediation strategies that are based on critical review of scientific literature
C. Learn from one’s own and other specialties
The discussion group saw the three points of this core competency asbeing of highest priority for assessment. They concurred that these pointscould be assessed under the Lifelong Learning and Practice AssessmentComponents of a MOC Program, most likely by having diplomates pre-sent cases they had handled.
Validation of the Practice-Based Learning and Improvement Core Competencies
The discussion group agreed that to validate these core competencies, asurvey of the field would be needed, with benchmarks and data out-comes, especially with functional measures for outcomes in psychiatry.

Practice-Based Learning and Improvement Core Competencies 101
A minor examination of the data needed would be that of how many pa-tients a physician has cared for and how those patients have progressedto date.
Summary
This section of the full core competency outline was unlike the three pre-ceding sections in that most of the core competencies herein could andshould be assessed only after the physician has been in practice (see Table8–1 for summary). The Lifelong Learning and Practice Assessment Com-ponents of a MOC Program seemed to be almost perfectly designed forthis purpose.
Although most of the core competencies of this section were placedin the middle range of priority in terms of assessment, the core compe-tencies that related to a physician’s understanding his or her own limitsof knowledge and how and when to search for answers for his or herpatient were judged of highest priority. Also in this category of highestpriority for assessment was the physician’s maintenance of a system forexamining errors in practice and initiating improvements to eliminate orreduce those errors.
In terms of assessment methodologies for these core competencies, thediscussion group decided that while some current methodologies, such asthe use of cognitive examinations and vignettes, might be appropriate,they stressed that such cognitive examination questions and such vi-gnettes would have to be carefully constructed to assess what was neededhere. Case-based problems might often involve the presentation of re-search, and there appeared to be great leeway in deciding where the re-sponsibility for the assessments of these core competencies should rest.In some cases, specialty societies were suggested as the agents of assess-ment, but in other cases, the responsibility was clearly seen as that of theABPN. In all cases, however, a critical step before any assessment couldbegin would be the establishment of benchmarks.

102 Core Competencies and the Practice of Psychiatry Today
Table 8–1. Summary of Practice-Based Learning and Improvement Core Competencies
1. The physician shall recognize and accept limitations in his or her own knowledge base and clinical skills and understand and address the need for lifelong learning.
2. The physician shall demonstrate appropriate skills for obtaining and evaluating up-to-date information from scientific and practice literature and other sources to assist in the quality care of patients. This shall include, but not be limited to, the following:A. Use of information technology, including Internet-based searches and
literature databases (e.g., Medline); medical libraries; and drug information databases
B. Active participation, as appropriate, in educational courses, conferences, and other organized educational activities at both the local and national levels
3. The physician shall evaluate caseload and practice experience in a systematic manner. This may include, but not be limited to, the following:A. Obtaining appropriate supervision and consultationB. Use of best practices through practice guidelines or clinical pathwaysC. Case-based learningD. Review of patient records and outcomesE. Obtaining evaluations from patients (e.g., their opinion of outcomes and
patient satisfaction)F. Maintaining a system for examining errors in practice and initiating
improvements to eliminate or reduce errors4. The physician shall demonstrate an ability to critically evaluate relevant
medical literature. This ability may include, but not be limited to, the following:A. Using knowledge of common methodologies employed in psychiatric
and neurological researchB. Conducting and presenting reviews of current research in such formats
as journal clubs, grand rounds, and/or original publicationsC. Researching and summarizing a particular problem that derives from the
physician’s caseload5. The physician shall demonstrate the ability to do the following:
A. Review and critically assess scientific literature to determine how quality of care can be improved in relation to one’s practice (e.g., reliable and valid assessment techniques, treatment approaches with established effectiveness, practice parameter adherence). Within this aim, the physician shall be able to assess the generalizability or applicability of research findings to one’s patients in relation to their sociodemographic and clinical characteristics.
B. Develop and pursue effective remediation strategies that are based on critical review of scientific literature.
C. Learn from one’s own and other specialties.

103
Chapter 9
Professionalism Core Competencies
Elizabeth B. Weller, M.D.
Assumptions Regarding the Professionalism Core Competencies
The Professionalism Core Competencies, like the Interpersonal and Com-munications Skills Core Competencies (discussed in Chapter 7) and thePractice-Based Learning and Improvement Core Competencies (dis-cussed in Chapter 8), are regarded as core competencies that may benon–specialty specific, or “generic,” for most medical specialties. Thesegeneric core competencies stand in sharp contrast to the core competen-cies in the Patient Care, Medical Knowledge, and Systems-Based PracticeCategories that, by their nature, must have specialty-specific compo-nents for psychiatry.
As discussed in Chapter 4 (“The ACGME and ABMS Initiatives To-ward the Development of Core Competencies”), during the AmericanBoard of Psychiatry and Neurology (ABPN) Invitational Core Compe-tencies Conference, six working groups were identified, and each wasassigned the task of discussing one of the six sections of the core compe-tency outline. The original outline of core competencies was the result ofthe merging of the outlines of the six areas written by the psychiatry andneurology quadrads as convened by the American Board of MedicalSpecialties (ABMS) and the Accreditation Council for Graduate MedicalEducation (ACGME). The instructions to each working group includedthe recommendation to accept the basic outline unless serious changes

104 Core Competencies and the Practice of Psychiatry Today
needed to be made. Of the six working groups, only the group discussingthe core competencies on Professionalism found it necessary to make ma-jor changes to the outline provided. The basis for making these changeswas the elimination of redundancies in the Professionalism Core Com-petencies. The following summary represents the conclusions drawnregarding their amended outline. Sections deleted from the outline pro-vided will not be discussed, as they are repetitious of the material pre-sented here.
As the demeanor and attitudes of a physician are important in all as-pects of his or her professional life, the working group believed that thecore competencies in the Professionalism Category of the outline were ofhighest priority for evaluation in almost all instances.
The Professionalism Core Competencies
The First Professionalism Core Competency
The physician shall demonstrate responsibility for his or her patients’ care, including responding to communication from patients and other health professionals in a timely manner.
The discussion group decided that this core competency could be eval-uated in training and throughout practice (and especially as part of thePractice Assessment Component of the ABPN Maintenance of Certifi-cation [MOC] Progam). The evaluation of this competency could bebased on an established policy for optimal physician-patient communica-tions and on patient satisfaction surveys.
The Second Professionalism Core Competency
The physician shall demonstrate responsibility for his or her patients’ care, including
A. Using medical records for appropriate documentation of the course of illness and its treatment
B. Coordinating care with other members of the medical and/or multidisciplinary team
C. Providing coverage if unavailable, e.g. , out of town, on vacationD. Providing for continuity of care, including appropriate consultation,
transfer, or referral if necessary

Professionalism Core Competencies 105
The discussion group again concluded that the points of this core com-petency could begin to be assessed in training and continue to be assessedthrough residency and practice, the latter as part of a MOC Program.Samples of medical records and the peer review process were suggestedas assessment methodologies. In addition, point B could be evaluated byoral examinations and point D by oral and cognitive examinations. Alsorelated to point D, evaluating how well a physician provides for appro-priate referral or transfer when necessary could be accomplished by ex-amining office records, medical charts, and patient satisfaction surveys.Data obtained from the sources listed above could validate this compe-tency.
The Third Professionalism Core Competency
The physician shall demonstrate ethical behavior, integrity, honesty, compassion, and confidentiality in the delivery of care, including matters of informed consent/assent, professional conduct, and conflict of interest.
The medical licensing bodies of each state have primary responsibility formonitoring ethical behavior in physicians. The ABPN and other ABMSmember boards rely on that measure, requiring individuals to have full,unrestricted medical licenses in order to sit for certification and recerti-fication examinations. The discussion group also decided that ethicalbehavior and personal and professional attitudes of integrity, honesty,and compassion should be assessed in training and throughout practice.This assessment could be achieved through written and oral examina-tions such as the ABPN written certification (Part I) and oral certification(Part II) examinations and the recertification examinations, and as part ofthe Practice Assessment Component of the ABPN MOC Program. Pa-tient surveys and peer reviews were suggested as methodologies of as-sessment. Data from such sources could also be used to validate thiscompetency.
The Fourth Professionalism Core Competency
The physician shall demonstrate respect for patients and their families, and his or her colleagues as persons, including their ages, cultures, disabilities, ethnicities, genders, socioeconomic backgrounds, religious beliefs, political leanings, and sexual orientations.

106 Core Competencies and the Practice of Psychiatry Today
The discussants decided that this core competency could be assessed intraining and through both written and oral examinations, such as the ABPNwritten certification (Part I) and oral certification (Part II) examinations,and the ABPN recertification examinations. For this assessment to takeplace as part of the current ABPN oral certification (Part II) examination,examiners would have to be trained to ensure that this area would beevaluated effectively.
Again, patient surveys and peer reviews were suggested as assessmentmethodologies. Data from such sources could also be used to validate thecompetency.
The Fifth Professionalism Core Competency
The physician shall demonstrate understanding of and sensitivity to end-of-life care and issues regarding provision of care.
The discussion group thought that this core competency could be as-sessed using both written and oral examinations. Criteria for successfulevaluation of this core competency could include examination perfor-mance, peer reviews, and assessment of how well advance directives wereobtained and followed. Medical record review could aid in this assess-ment. Validation for this core competency could come through variousoutcome measures.
The Sixth, Seventh, and Eighth Professionalism Core Competencies
The sixth, seventh, and eighth Professionalism Core Competencies, be-ing closely related, can be discussed together. They are as follows:
The physician shall review his or her professional conduct and remediate when appropriate.
The physician shall participate in the review of the professional conduct of his or her colleagues.
The physician shall acknowledge and remediate medical errors should they occur.

Professionalism Core Competencies 107
These core competencies speak to the accountability to which anyprofessional should hold himself or herself. These competencies as theyrelate to medical professionalism should be developed beginning in med-ical school, furthered in residency, and continued throughout practicelife. Evaluation of these competencies can begin with faculty, program di-rector, and peer review in medical school and residency, but their mostmeaningful evaluation will come as part of the Practice Assessment Com-ponent of a MOC Program.
Summary
Discussion of the Professionalism Core Competencies at the ABPN Invi-tational Core Competencies Conference involved crystallizing key pointsof the outline and eliminating repetitious language. For all of the compe-tencies listed in this chapter (see Table 9–1 for summary), the generalconsensus was that the development of professionalism is begun in medicalschool, continued during residency, and must be maintained throughoutpractice life. Thus, it is important to begin instilling professional attitudesand behaviors early in medical education and to provide coaching andcorrective behavior to ensure that adequate standards are acquired andmaintained. Initial assessment of professional behaviors and attitudescould come through specially designed questions on the written examina-tions, but would more easily be handled through the oral examinations,such as the ABPN oral certification (Part II) examination. Cognitivequestions similar to those that might be used on the ABPN written cer-tification (Part I) examination could also be included in the recertifi-cation examinations. For ongoing practice, however, the logical point ofevaluation would be under the Practice Assessment Component of theABPN MOC Program.
As the skills that form this section of the core competency outline per-meate all other sections of the outline, it would be logical that Profession-alism Core Competencies be evaluated in tandem with other skills. Forexample, when the Interpersonal and Communications Skills (discussedin Chapter 7: “Interpersonal and Communications Skills Core Compe-tencies”) are assessed, part of that assessment could include the profes-sionalism of the encounters. The most meaningful evaluation would takeplace when the Professionalism Core Competencies are evaluated as anintegral part of the other competencies.

108 Core Competencies and the Practice of Psychiatry Today
Table 9–1. Summary of Professionalism Core Competencies
1. The physician shall demonstrate responsibility for his or her patients’ care, including responding to communication from patients and other health professionals in a timely manner.
2. The physician shall demonstrate responsibility for his or her patients’ care, includingA. Using medical records for appropriate documentation of the course of
illness and its treatmentB. Coordinating care with other members of the medical and/or
multidisciplinary teamC. Providing coverage if unavailable, e.g. , out of town, on vacationD. Providing for continuity of care, including appropriate consultation,
transfer, or referral if necessary3. The physician shall demonstrate ethical behavior, integrity, honesty,
compassion, and confidentiality in the delivery of care, including matters of informed consent/assent, professional conduct, and conflict of interest.
4. The physician shall demonstrate respect for patients and their families, and his or her colleagues as persons, including their ages, cultures, disabilities, ethnicities, genders, socioeconomic backgrounds, religious beliefs, political leanings, and sexual orientations.
5. The physician shall demonstrate understanding of and sensitivity to end-of-life care and issues regarding provision of care.
6. The physician shall review his or her professional conduct and remediate when appropriate.
7. The physician shall participate in the review of the professional conduct of his or her colleagues.
8. The physician shall acknowledge and remediate medical errors should they occur.

109
Chapter 10
Systems-Based Practice Core Competencies
Pedro Ruiz, M.D.
Defining the Category of Systems-Based Practice Core Competencies
The Systems-Based Practice Core Competency Category is unlike any ofthe preceding five categories of core competencies. Physicians and lay-people alike have no trouble understanding what the terms patient care,medical knowledge, practice-based learning and improvement, interpersonaland communications skills, and professionalism mean. Applying these wordsas labels to categories of core competencies, listing the specific compe-tencies within each category, and then deciding how and when to assessthese competencies is more challenging, but generally, consensus on mostpoints can be achieved.
The physicians who were in the Systems-Based Practice Core Compe-tency discussion group at the core competencies conference sponsoredby the American Board of Psychiatry and Neurology (ABPN) in June2001 spent a great deal of their time defining this category. Their conclu-sion mirrored what James E. Youker, MD, the twenty-eighth president ofthe American Board of Medical Specialties (ABMS), said in his Presi-dent’s Column of the Summer 2001 The ABMS Record:
A system, as universally defined, is a set of interdependent componentsor elements, which interact to achieve a common purpose or goal. Physi-cians are familiar with the concept of scientific systems such as organ

110 Core Competencies and the Practice of Psychiatry Today
systems, but the generic meaning of the word is much broader. It encom-passes the concepts of distinct entities, which function together toachieve a desired goal. Not a difficult concept, [but] why then do we findit so difficult to accept when applied to the practice of medicine as op-posed to the science of medicine?
Youker explains that part of the concern may stem from the confusionbetween the terms systems-based practice and managed care systems. Hestates that “although managed care systems are inherently encompassedwithin the concept, the competency [category] should be envisioned ina broader context to reflect the complexities of current healthcare deliv-ery in the United States” (Youker 2001).
The need for serious consideration of the systems of medical practiceprobably stems from the 1999 Institute of Medicine report on medicalerrors, To Err Is Human: Building a Safer Health System, which lists med-ical mistakes as the eighth leading cause of death in the United States,ahead of deaths caused by traffic accidents, breast cancer, and AIDS. Thereport stresses that no one entity is to blame for the high rate of mistakes;the failure stems from multiple sources. An emerging body of researchexists that suggests that more often than not, “medical errors are oftendue to the failure of health systems rather than individual deficiencies”(Epstein and Hundert 2002). It is primarily by improving the systemsthat the medical edict that promises first and foremost to “do no harm”can be actualized.
These systems of medical care are perhaps best understood as a webof interconnected services comprising physicians and other healthcareworkers, hospitals and medical centers, governmental agencies, industrysettings, consumers and watchdog agencies, and more. The main point tounderstand in regard to the Systems-Based Practice Core Competenciesis that medical care is not provided in a vacuum. Most physicians do notpractice alone (Randolph 1997), and even individual physicians in solopractice are enmeshed in a network of healthcare and health-related agen-cies and entities (Frankford et al. 2000).
For example, an individual psychiatrist working only with outpatientsin private practice may or may not have involvement with a hospital set-ting, but even the independent, non–hospital-based psychiatrist wouldneed an excellent working knowledge of the full realm of services avail-able on an inpatient basis should any of his or her patients need referralto such an inpatient setting. When such a psychiatrist refers a patient forinpatient care, he or she may refer the patient to the care of a hospital-based psychiatrist. The independent psychiatrist in effect transfers the re-sponsibility and authority for that patient to the hospital-based psychia-

Systems-Based Practice Core Competencies 111
trist, who accepts that individual as his or her own patient.1 When thepatient is released from the hospital, he or she may choose to again be-come a patient of the independent psychiatrist, at which time the inde-pendent psychiatrist again assumes responsibility for that patient.
The example cited above is a very narrow example of what a systemcan be said to be: namely, the cooperation between an independent prac-titioner (in the case of our example above, a non–hospital-based psychi-atrist in private practice) and a parallel department in a hospital. Thisnarrow example can be broadened to include the private practitioner (orindependent psychiatrist) and the full array of programs and services thatare available for all types of medical care through local community hos-pitals, university-based teaching hospitals, and national centers knownfor specialized care. To make a responsible referral, the private practitio-ner must have a working knowledge of other related medical “systems.”
The system can be broadened again when one considers that a psychi-atrist in private practice must also have a full, working knowledge ofcommunity-based services for low-cost or no-cost medical care for thosepatients who no longer have insurance or any other means of paying forprivate medical care. These community-based services include far morethan just medical care or even mental healthcare. These services may in-clude housing and other social services information, addiction treatmentprograms such as Alcoholics Anonymous or other 12-step programs, ap-propriate counseling sources such as family service agencies, and the like.
To reiterate, the idea behind Systems-Based Practice Core Competen-cies is that a psychiatrist never practices in a vacuum. He or she is part ofa network of programs and services available to the patient. To provideoptimum psychiatric care, the psychiatrist must understand the full spec-trum of services available. A responsible private or systems-based practi-tioner (e.g., a hospital-based psychiatrist) will always make available tothe patient the best and most appropriate services to meet the needs ofthat person.
The conference group working with Systems-Based Practice Core Com-petencies discussed at length the longitudinal responsibility for assessingcompetence in this area. Competencies in this category, perhaps morethan in some of the others, need to be developed incrementally over timebeginning in residency and continued throughout practice. As a corollaryof their longitudinal development, longitudinal assessment is needed.
1Note that the referral might not necessarily be to a psychiatrist. It could be to aphysician in another specialty, depending on the medical need of the patient. Forpurposes of our discussion here, we will stay with the psychiatry example.

112 Core Competencies and the Practice of Psychiatry Today
The discussion group suggested that some type of mutually beneficialconsortium between the residency training directors and the ABPNmight be the optimum means of actualizing this for the competency as-sessment process.
The Systems-Based Practice Core Competencies
The First Systems-Based Practice Core Competency
The physician shall be able to articulate the basic concepts of systems theory and how it is used in psychiatry. The physician should have a working knowledge of the diverse systems involved in treating patients of all ages and understand how to use the systems as part of a comprehensive system of care, in general, and as part of a comprehensive, individualized treatment plan. This will include the following:
A. Development of awareness leading to use of practice guidelines plus community, national, and allied health professional resources that may enhance the quality of life of patients with chronic psychiatric illnesses
B. Development of the ability to lead and delegate authority to healthcare teams needed to provide comprehensive care for patients with psychiatric diseases
C. Development of skills for the practice of ambulatory medicine, including time management, clinic scheduling, and efficient communication with referring physicians
D. Utilization of appropriate consultation and referral for the optimal clinical management of patients with complicated illnesses
E. Demonstration of the awareness of the importance of adequate cross coverage
F. Demonstration of the awareness of the importance of accurate medical data in the communication with and effective management of patients
The wording of the first Systems-Based Practice Core Competency isan excellent example of the comprehensiveness in wording the confer-ence discussion group deemed necessary for each core competency inthis group. The two introductory statements provide the systems-basedpractice context for this particular core competency. The specific detailsof the competency are not introduced until the subpoints. This contex-tualization of the core competency itself into a description of what ismeant by “systems” was thought to be important for the wording of thesecore competencies.
Point A above, the development of awareness leading to use of practiceguidelines plus community, national, and allied health professional re-

Systems-Based Practice Core Competencies 113
sources, is an excellent example of the longitudinal aspect of Systems-Based Practice Core Competencies. The “development of awareness” is,of necessity, a longitudinal process. This process should begin in residency(or before) and continue throughout the physician’s practice life. Thetopics mentioned within this core competency are dynamic, not static, andit is imperative that the practicing physician remain current with the re-sources available in his or her medical field and systems realm.
For this reason, the discussion group suggested that assessment of thiscore competency begin in residency, be addressed at the time of initialcertification, and be addressed again through the ABPN Maintenance ofCertification (MOC) Program. Residency evaluation could be donethrough a variety of means, depending on the interests of and the resourcesavailable to the various residency training directors. Specific assessmentmethodologies during residency and practice include multiple-choicequestions (MCQs), objective-structured clinical examinations (OSCEs),record reviews, chart-stimulated recalls, portfolio reviews, and documen-tation of involvement in community organizations.
Point B above, involving the leading of healthcare teams, is much lessbroad in scope than Point A. Point B was judged by the discussion groupto be at a lower level in terms of priority for assessment than Point A. Thediscussion group also saw a more narrow focus of assessment for this corecompetency—namely, that it be assessed only through the LifelongLearning and Practice Assessment Components of a MOC Program. Sug-gested evaluation methodologies included record reviews, chart-stimulatedrecalls, portfolio reviews, and 360-degree evaluations (evaluations done bymultiple people in a person’s sphere of influence, usually superiors, peers,subordinates, and patients and their families).
Like point B, point C, which focuses on ambulatory medicine, has anarrow focus for evaluation. The discussion group thought that the skillsneeded for the practice of ambulatory medicine—namely, such skills astime management, clinic scheduling, and effective communication withreferring physicians—should be both taught and evaluated in residency.These same skills should then be evaluated during the Practice Assess-ment Component of a MOC Program.
Besides the variety of residency evaluations possible, the discussiongroup suggested record reviews, chart-stimulated recalls, portfolio re-views, and patient surveys as methodologies for evaluating point C of thiscore competency. The group also saw this point of the core competencyas being of higher priority for assessment than either of the previouspoints.
Similar to point A (the development of awareness leading to the useof practice guidelines and professional resources), point D, which dis-

114 Core Competencies and the Practice of Psychiatry Today
cusses the role of consultation and referral, is a broad one. The discussiongroup suggested a wide-ranging assessment for this competency, includ-ing during residency, through cognitive examinations like the ABPNwritten certification (Part I) and recertification examinations, throughoral interviews, and through the Lifelong Learning and Practice Assess-ment Components of a MOC Program.
Points E and F of this core competency directly address the systems-based nature of practicing medicine. Point E, regarding cross coverage,and point F, regarding communication with and about patients, by theirvery nature stress that the physician does not practice alone. Assessmentof these competencies would need to be both wide-ranging and longitu-dinal.
Again, similar to what had been suggested for point A, the discussiongroup suggested the following methodologies for assessment purposes ofall of the other points within this competency: residency directors’ attes-tations of competence, MCQs, oral examinations, OSCEs, record re-views, chart-stimulated recalls, and portfolio reviews.
The Second Systems-Based Practice Core Competency
In the community system, the physician shall demonstrate the ability to recognize the limitation of healthcare resources and demonstrate the ability to act as an advocate for patients within their social and financial constraints.
The discussion group saw the second Systems-Based Practice CoreCompetency as being evaluated during residency and as part of the Prac-tice Assessment Component of a MOC Program. Suggested methodol-ogies included residency training directors’ attestations, record reviews,chart-stimulated recalls, and portfolio reviews.
The Third Systems-Based Practice Core Competency
In the community system, the physician shall demonstrate knowledge of the resources available both publicly and privately for the treatment of psychiatric problems impacting a patient’s ability to enjoy relationships and gain employment.
The discussion group saw this Systems-Based Practice Core Compe-tency as another with longitudinal parameters. Residents should begin

Systems-Based Practice Core Competencies 115
learning about the community resources, both public and private, duringtheir training and then be able to transfer this ability to find and keep cur-rent with that information throughout their practice. Evaluation of thiscore competency for psychiatrists should be done during residency, dur-ing the ABPN oral certification (Part II) examination as part of initial cer-tification, and through the Practice Assessment Component of a MOCProgram.
Suggested methodologies for this core competency included residencytraining directors’ attestations, oral examinations, OSCEs, record re-views, chart-stimulated recalls, and portfolio reviews.
The Fourth Systems-Based Practice Core Competency
In the community system, the physician shall demonstrate the ability to utilize knowledge of the legal aspects of psychiatric diseases as they impact patients and their families.
Of primary importance for psychiatrists, this Systems-Based PracticeCore Competency must be developed both longitudinally and incremen-tally. Residents should begin to understand the impact of the legal systemon patients and their families, and on entering practice, these physiciansmust keep current with both the changing laws and their changing appli-cations and implications.
This core competency should be assessed during residency, at the timeof initial certification, and through a MOC Program. Suggested method-ologies include residency training directors’ attestations; MCQs, such asthe ABPN written certification (Part I) and recertification examinations;oral examinations, such as the ABPN oral certification (Part II) examina-tion; OSCEs; and practice assessments.
The Fifth Systems-Based Practice Core Competency
The physician shall demonstrate knowledge of and interact with managed care systems, including the following:
A. Participating in utilization review communications and, when appropriate, advocating for quality patient care
B. Educating patients concerning such systems of care
This Systems-Based Practice Core Competency was judged to be oflesser importance than the other core competencies in this category for

116 Core Competencies and the Practice of Psychiatry Today
the assessment of psychiatrists because many psychiatrists, being in pri-vate practice, do not interact with managed care health systems or partic-ipate in utilization review. The skills relating to this core competencyshould be developed in residency and assessed through the residencytraining directors’ attestations of competency. The assessment of practic-ing psychiatrists should be accomplished through the Lifelong Learningand Practice Assessment Components of a MOC Program, as appropriateto the individual psychiatrist.
The Sixth Systems-Based Practice Core Competency
The physician shall demonstrate knowledge of community systems of care and assist patients in accessing appropriate care and other support services. This requires knowledge of treatment settings in the community, which include ambulatory, consulting, acute care, partial hospital, skilled care, rehabilitation, and substance abuse facilities; halfway houses; nursing homes; and home care and hospice organizations. The physician should demonstrate knowledge of the organization of care in each relevant delivery setting and the ability to integrate the care of patients across such settings.
This Systems-Based Practice Core Competency, like some of the oth-ers discussed earlier in this chapter, is both broad and longitudinal. Ofprimary importance for psychiatrists, the core competencies describedherein can be developed only incrementally and must constantly be keptcurrent. Training for these competencies should begin in residency, andtheir maintenance should be continued throughout the entire practice ca-reer. Formal assessment of this core competency should come throughresidency training directors’ attestations and OSCEs during residency;through the use of MCQs on the cognitive examinations of the ABPNwritten certification (Part I) and recertification examinations; throughoral examinations of the ABPN oral certification (Part II) examination;and through record reviews, chart-stimulated recalls, and portfolio re-views for the Lifelong Learning and Practice Assessment Components ofa MOC Program.
Validation of the Systems-Based Practice Core Competencies
The discussion group decided that all of the Systems-Based Practice CoreCompetencies could be validated by surveying the public, evaluating pa-

Systems-Based Practice Core Competencies 117
tient complaints, and reviewing legal records. As every core competencyin this section was suggested for evaluation through the Practice Assess-ment Component of a MOC Program, it might become the responsibilityof the ABPN to validate all of the Systems-Based Practice Core Compe-tencies.
Summary
More than any of the five previous core competency sections discussed(Patient Care in Chapter 5, Medical Knowledge in Chapter 6, Interper-sonal and Communications Skills in Chapter 7, Practice-Based Learningand Improvement in Chapter 8, and Professionalism in Chapter 9), thissection of the core competencies outline, Systems-Based Practice (seeTable 10–1 for summary), demonstrates the longitudinal character ofboth the development of competence and the necessity of ongoing assess-ment.
References
Epstein RM, Hundert EM: Defining and assessing professional competence.JAMA 287:226, 2002
Frankford DM, Patterson MA, Konrad TR: Transforming practice organizations tofoster lifelong learning and commitment to medical professionalism. AcadMed 75:708–717, 2000
Institute of Medicine: To Err Is Human: Building a Safer Health System. Wash-ington, DC, National Academy Press, 1999
Randolph L: Physician Characteristics and Distribution in the U.S.: 1997–98 Edi-tion. Chicago, IL, Department of Data Survey and Planning. Division of Sur-vey and Data Resources, American Medical Association, 1997
Youker JE: What is systems-based practice? The ABMS Record, X3 (Summer),2001, p 2

118 Core Competencies and the Practice of Psychiatry Today
Table 10–1. Summary of Systems-Based Practice Core Competencies
1. The physician shall be able to articulate the basic concepts of systems theory and how it is used in psychiatry. The physician should have a working knowledge of the diverse systems involved in treating patients of all ages and understand how to use the systems as part of a comprehensive system of care, in general, and as part of a comprehensive, individualized treatment plan. This will includeA. Development of awareness leading to use of practice guidelines plus
community, national, and allied health professional resources that may enhance the quality of life of patients with chronic psychiatric illnesses
B. Development of the ability to lead and delegate authority to healthcare teams needed to provide comprehensive care for patients with psychiatric diseases
C. Development of skills for the practice of ambulatory medicine, including time management, clinic scheduling, and efficient communication with referring physicians
D. Utilization of appropriate consultation and referral for the optimal clinical management of patients with complicated illnesses
E. Demonstration of the awareness of the importance of adequate cross coverage
F. Demonstration of the awareness of the importance of accurate medical data in the communication with and effective management of patients
2. In the community system, the physician shall demonstrate the ability to recognize the limitation of healthcare resources and demonstrate the ability to act as an advocate for patients within their social and financial constraints.
3. In the community system, the physician shall demonstrate knowledge of the resources available both publicly and privately for the treatment of psychiatric problems impacting a patient’s ability to enjoy relationships and gain employment.
4. In the community system, the physician shall demonstrate the ability to utilize knowledge of the legal aspects of psychiatric diseases as they impact patients and their families.
5. The physician shall demonstrate knowledge of and interact with managed care systems, including the following:A. Participating in utilization review communications and, when
appropriate, advocating for quality patient careB. Educating patients concerning such systems of care
6. The physician shall demonstrate knowledge of community systems of care and assist patients in accessing appropriate care and other support services. This requires knowledge of treatment settings in the community, which include ambulatory, consulting, acute care, partial hospital, skilled care, rehabilitation, and substance abuse facilities; halfway houses; nursing homes; and home care and hospice organizations. The physician should demonstrate knowledge of the organization of care in each relevant delivery setting and the ability to integrate the care of patients across such settings.

119
Chapter 11
Cross Competencies
What Psychiatrists Should Know About Neurology
Glenn C. Davis, M.D.Daniel K. Winstead, M.D.Thomas A. M. Kramer, M.D.
Cross Competency Considerations for Psychiatrists
It was clear from the very beginning of the development of the AmericanBoard of Psychiatry and Neurology (ABPN) core competency outlinethat there would be three distinct sections for some categories of corecompetencies: a general section, which would discuss core competenciesthat both psychiatrists and neurologists would need to possess, and bothpsychiatry-specific and neurology-specific competency sections. A basicassumption was that these specific areas would affect only the PatientCare and Medical Knowledge Core Competency Categories. However,discussion also showed a dichotomy in practice (and therefore an assess-ment needed) in the area of Systems-Based Practice Core Competencies.This book focuses only on the psychiatric aspects of core competencies,but one area that cannot be excluded is what the Toronto discussiongroups concurred that psychiatrists needed to know about neurology interms of basic core competencies.

120 Core Competencies and the Practice of Psychiatry Today
Historically, psychiatry and neurology were often thought of together,especially as both were represented from the beginning in the Section onNervous and Mental Diseases of the American Medical Association(AMA) and in some of the medical schools of the 1920s and 1930s, asingle department represented both specialties. And, as Hollender (1991,p. 24) noted, “many clinicians, belonging to one specialty, practiced theother to a limited extent either by choice or out of economic necessity.”Even though the specialties of psychiatry and neurology were, to someextent, complementary and therefore linked, the practitioners of eachspecialty chose to see their own specialty as separate and distinct fromthe other.
There were two practical reasons the specialties of psychiatry and neu-rology, while electing to remain separate, still came together to form onespecialty board, the ABPN. The first was that the AMA Council on Med-ical Education and Hospitals and, later, the Advisory Board of MedicalSpecialties (now, the American Board of Medical Specialties) were activelyworking to restrict the number of specialty boards being formed and en-couraging the partnering of disciplines where possible and practical. Theother reason, according to a historian of the ABPN, is that “at the time ofthe inception of the ABPN, there were not enough neurologists to justifythe establishment of an examining board in neurology” (F.M. Forster, M.D.,personal correspondence to M. Hollender, M.D., 1960).
From the inception of the ABPN, examination and certification inpsychiatry and neurology recognized the complementary natures of thedisciplines. Initially, the same examination was given for both psychia-trists and neurologists. The examination was graded differently for thetwo groups of specialists, however, on the basis of whether the physiciandeclared himself or herself to be a psychiatrist or a neurologist. Passingstandards were set higher for the subject area for which one claimed profes-sional membership than for the complementary field. Those seeking certi-fication in both psychiatry and neurology had to meet the higher standardfor both subjects on each examination.
Thus, each examination had a “major” and a “minor” section, the majorsection being the specialty in which certification was sought and the mi-nor being the other specialty. These major and minor sections of the cer-tification examinations came to be known as, respectively, the Part A andPart B of the ABPN Part I certification examination. Thus, every certifiedpsychiatrist has taken and passed a Part B examination in neurology. (Thecorollary is also true: every certified neurologist has taken and passed aPart B examination in psychiatry.)
Thus, the ABPN Invitational Core Competencies Conference held inToronto, having representatives of both specialties present, offered a unique

Cross Competencies 121
opportunity to document the core competencies in neurology for whicha psychiatrist should be held accountable (and in psychiatry a neurologistshould be held accountable for).
Basically, the psychiatrists and neurologists attending the ABPN Invi-tational Core Competencies Conference agreed that psychiatrists mustunderstand that the neurology competencies, whether they relate to an-atomical pathways, neurotransmitters, medications, or basic neurophysi-ology, are all related to central nervous systems as opposed to peripheralnervous systems.
Neurology-Specific Core Competencies for Psychiatrists
Patient Care
The Patient Care Core Competency discussion group felt that psychia-trists should be held accountable for demonstrating a comprehensiveknowledge of the active and inert chemicals in neurological drugs, in-cluding their uses, side effects, and drug-drug interactions. The discus-sion group also felt that psychiatrists should be conversant with and havethe clinical skills to elicit signs and symptoms of neurological origin andimportance to be able to interpret their meaning and weigh them ap-propriately when forming differential diagnoses. Assessment for thesecompetencies should begin in residency training and continue through-out practice life. Depending on when the assessment would take place,methodologies might include multiple-choice questions (MCQs) oncognitive examinations, in-training evaluations, portfolio reviews, andsupervisor/peer attestations. Validation of the Patient Care Core Com-petencies could be done through surveys of the field.
Medical Knowledge
The Medical Knowledge Core Competency discussion group was veryspecific in terms of items from the neurology core competency outlinefor which psychiatrists should be held accountable. All of the followingwere listed and judged to be of the highest priority for psychiatrists to un-derstand fully:
• Basic neuroscience that would be critical to the practice of neurology• Pathophysiology of major neurological disorders and familiarity with
the scientific basis of neurological diseases, including knowledge of thefollowing:

122 Core Competencies and the Practice of Psychiatry Today
1. Neuroanatomy, especially that of the cerebral cortex, basal ganglia/thalamus, vascular system, autonomic nervous system, and painpathways
2. Neurochemistry, especially that of neurotransmitters, the blood-brain barrier, neuronal excitation, vitamins, and neurotoxins
3. Basic neurophysiology, especially membrane physiology; synaptictransmission; the reticular system and mechanisms of sleep andarousal, consciousness, and circadian rhythms; the rhinencephalon,limbic system, and visceral brain; learning and memory; cortical or-ganizers and functions; and the blood-brain barrier
4. Clinical neurophysiology, especially electroencephalograms, evokedresponses, and sleep studies
5. Neuropharmacology, especially that of anticonvulsants, antidys-kinesia drugs (including antiparkinsonian agents), vitamins (clini-cal aspects), analgesics (narcotic, nonnarcotic, and other centrallyactive agents), hormones, anticholinesterase drugs, and the neuro-logical side effects of systemic drugs
6. Neurogenetics/molecular neurology and neuroepidemiology, espe-cially of Mendelian-inherited diseases, trinucleotide repeat disor-ders, and risk factors for neurological disease
7. Neuroimaging, including MRI, MRV/MRS, CT, and SPECT/PET8. Neuro-ophthalmology, including vision and visual pathways, visual
fields, pupils, ocular motility, and fundi, retina, and optic nerve func-tion and disorders
9. Movement disorders
As with the neurology Patient Care Core Competencies for which psy-chiatrists should be held accountable, assessment for these MedicalKnowledge Core Competencies should begin in residency training andcontinue throughout practice life. Depending on when the assessmentwould take place, methodologies might include MCQs on cognitive ex-aminations, in-training evaluations, portfolio reviews, and supervisor/peer attestations. Validation of the Medical Knowledge Core Competen-cies could be done through surveys of the field.
It is significant to note that during the discussion, both psychiatristsand neurologists were able to agree on the neurology competencies thatare necessary to the basic practice of psychiatry.
Reference
Hollender MH: Neurology and psychiatry, in The American Board of Psychiatryand Neurology: The First Fifty Years. Edited by Hollender MH. Deerfield,IL, American Board of Psychiatry and Neurology, 1991, pp 23–27

123
Part IV
The Impact of Core Competencies
Part I of this book has shown how the concept of medical competencein psychiatry has evolved. Part II focused on two different methods of de-lineating core competencies: the Canadian approach of defining the rolesphysician specialists play and the American approach as developed by theAccreditation Council for Graduate Medical Education and the Ameri-can Board of Medical Specialties. Part III expanded on the latter ap-proach and discussed each of the six categories of core competencies insome detail. Part IV of this book will take the concept of core competen-cies from the present time into the future and attempt to predict howcore competencies will affect practicing psychiatrists and those in train-ing for that profession.
Chapter 12 focuses on the implications of core competencies for thepurposes of initial certification through the American Board of Psychia-try and Neurology and on the evolving concept of maintenance of certi-fication. Chapter 13 focuses on the impact the core competencies arelikely to have on the full spectrum of medical education, from medicalschool through continuing medical education. Special emphasis is placedon the possible role of the core competencies vis-à-vis the Lifelong Learn-ing Component of the Maintenance of Certification Program. Chapter 14

124 The Impact of Core Competencies
concludes this book with some educated guesses about how core compe-tencies will affect future psychiatric practice.
Throughout this book, core competencies have been presented as fluid,living, evolving concepts, not hard and fast rules carved in stone. While itis likely that for residency education and certification examinations, somecompetencies will be made quite specific for assessment purposes, it isalso likely that the methods used for assessing these core competencieswill provide great latitude.
The ultimate goal of the core competencies is to provide real and re-alistic means for physicians to display their skills, all of which are to beused for the benefit of the patients they serve.

125
Chapter 12
Implications of the Core Competencies on ABPN Certification and Maintenance ofCertification for Psychiatric Practitioners
Stephen C. Scheiber, M.D.Susan E. Adamowski, Ed.D.
ABPN Certification and Recertification
From its inception, the American Board of Psychiatry and Neurology(ABPN) had as its goal the creation and administration of fair, valid, andreliable certification examinations in psychiatry, neurology, child neurol-ogy, and the subspecialties. The mission of the ABPN specifies that theultimate goal of this endeavor is to serve the public interest. The creationand administration of fair, valid, and reliable examinations is an arduousprocess that the ABPN approaches with appropriate determination. Nec-essary resources of the board have always been allocated for the accom-plishment of this task.
The mission of the board expanded with the inception of time-limitedcertification. The ABPN, along with its sister boards, answered the man-date of the American Board of Medical Specialties (ABMS) by instituting

126 The Impact of Core Competencies
certificates that expire after a given time period. Depending on the par-ticular member board, certificates are active for a period of 6–10 years.For the ABPN, this period is 10 years. As of October 1, 1994, all physi-cians receiving board certification from the ABPN are issued 10-year,time-limited certificates. Certificates issued in the subspecialties of ad-diction psychiatry, clinical neurophysiology, forensic psychiatry, geriatricpsychiatry, neurodevelopmental disabilities, and pain medicine, includ-ing those issued before October 1, 1994, are also 10-year, time-limitedcertificates.1 What this means is that every certificate, whether for a spe-cialty or subspecialty, issued by the ABPN as a time-limited certificate isactive for 10 years from December 31 of its year of issuance. For example,a physician who was certified in the subspecialty of addiction psychiatryon January 20, 1995, would need to recertify in addiction psychiatry be-fore December 31, 2005 in order to have continuous certification in thatsubspecialty. In addition, for the physician to be able to recertify in ad-diction psychiatry, his or her certification in general psychiatry must becurrent. With the exception of child and adolescent psychiatry, recertifi-cation in the relevant specialty is a prerequisite for recertification in thesubspecialty.
The Core Competencies and the ABPN Examinations in Psychiatry
The ABPN Written Certification (Part I) Examination in Psychiatry
The development of the written certification examination in psychiatryand in subspecialties begins with the examination committees’ writingcontent outlines. One major criterion for selecting committee membersis their content expertise.
Content outlines are comprehensive subject area lists of topics thatmay be covered on the examination. The pool of examination questionscovers all areas of the content outlines, but questions in all areas of thecontent outlines will not necessarily be on all examinations.
Of the six core competency areas (Patient Care, Medical Knowledge,Interpersonal and Communications Skills, Practice-Based Learning andImprovement, Professionalism, and Systems-Based Practice), it is proper
1Ten-year, time-limited certification for child and adolescent psychiatry began in1995.

Core Competencies and ABPN Certification and Recertification 127
to say that the current ABPN written certification (Part I) examinationcovers primarily the second competency area, Medical Knowledge, and,to some degree, the first competency area, Patient Care.
The physicians who attended the ABPN Invitational Core Competen-cies Conference in June 2001 discussed all six areas of core competenciesand ascertained that while the focus of the current ABPN written certi-fication (Part I) examination is on Medical Knowledge, multiple-choicequestions (MCQs) could be written for the other core competency areasas well. It is important to note that while conference attendees stated thatMCQs could be written for the five other core competency areas, writingvalid and reliable questions in most of these subject areas could be bothdifficult and time-consuming. The exception here might be writingMCQs for the Systems-Based Practice Core Competency area. Evenmore importantly, conference attendees stressed that assessment, partic-ularly in the last four mentioned core competency categories, may bemore effectively and efficiently accomplished through use of measuresother than MCQs. Suggested alternative assessment measures included oralexaminations, such as objective-structured clinical examinations (OSCEs);portfolio review; chart-stimulated recall; peer reviews; and supervisor at-testation.
The ABPN Oral Certification (Part II) Examination in Psychiatry
From its inception, the ABPN realized that a written examination, nomatter how comprehensive and well written, could never completely testfor skills necessary for certification. To that end, an oral examination hasalways been required for certification in psychiatry. For psychiatry, theoral examination consists of an interview with an actual psychiatricpatient and the viewing of a videotape of a psychiatrist interviewing anactual psychiatric patient. The patient interview is observed by twoboard-certified psychiatrists who are under the supervision of a seniorboard-certified psychiatrist. The primary examiners assess the candi-date’s skills of interacting with the patient and then have the candidatediscuss his or her findings, including chief complaint, history of presentillness and life circumstance, significant past history, review of systems, andmental status examination, followed by a summary of the pertinent clin-ical findings. This discussion is followed by a formulation of the case andthen a differential diagnosis, a working diagnosis, prognosis, and a treat-ment and management plan.
The audiovisual component of the Part II examination is similar to thepatient encounter, except that a videotaped interview of a patient takes

128 The Impact of Core Competencies
the place of the examination of the actual patient. Thus, obviously, thenature of the physician-patient interaction cannot be judged. Grading forthe patient portion of the Part II examination includes an evaluation ofthe physician-patient relationship, and the conduct of the interview.Grading for the audiovisual portion of the Part II examination is based onthe organization and presentation of data, phenomenology, diagnosis andprognosis, and etiologic, pathogenic, and therapeutic issues. The two ex-aminers discuss their observations of each candidate and must agree on apass or fail determination.
Although the primary content emphasis on the ABPN oral certification(Part II) examination is on Medical Knowledge (and to a lesser extent, Pa-tient Care), significant emphasis is also placed on communications skillsin the patient interview and on Professionalism in both the patient and au-diovisual sections of the examination. Thus, it is accurate to say that boththe core competency areas of Interpersonal and Communications Skills(discussed in Chapter 7) and Professionalism (discussed in Chapter 9) arebeing assessed globally with the ABPN Part II examination.
The ABPN Core Competency Committee may decide to develop andrecommend to the board a specific checklist of criteria for these two corecompetency areas to more formally evaluate specific competencies ratherthan continuing with the holistic approach.
The core competency areas of Practice-Based Learning and Improve-ment (discussed in Chapter 8) and Systems-Based Practice (discussed inChapter 10) are not currently a primary focus of the ABPN oral certi-fication (Part II) examination. It is possible that the Core CompetencyCommittee will recommend to the board that the Part II ExaminationCommittee develop specific questions and/or vignettes to cover thesecompetency areas.
It has been recognized, however, that the ABPN Part I and Part II cer-tification examinations cannot, by their very nature, comprehensivelyevaluate all six core competency areas. One of the main conclusions ofthe ABPN 2001 Invitational Core Competencies Conference was thatthe assessment of many of the core competencies should begin early inthe physician’s medical education career rather than at the time of initialcertification. This process would have many benefits, among which maylikely be the following:
• Skills, such as the manner in which a physician establishes rapportwith a patient, are developed incrementally through a physician’s ed-ucational and practice career. Thus, it might be appropriate to beginthe assessment of such skills on an incremental basis as well. Certainlevels of skills in this communications area are developed (and there-

Core Competencies and ABPN Certification and Recertification 129
fore assessable) in medical school and other levels of skills during med-ical residency.
• If the assessment of designated skills occurred during medical schooland in residency, those not meeting criteria of success would have anexcellent opportunity for remediation with the assistance of their fac-ulty and program directors.
• Early assessment of specific competencies would allow more emphasisto be placed on the assessment of other competencies especially dur-ing the ABPN Part II certification examination. This emphasis mightbe placed on competencies in the Practice-Based Learning and Im-provement and the Systems-Based Practice Categories.
Implications of the Core Competencies on the ABPN Certification Examinations
The ABPN written (Part I) and oral (Part II) certification examinationshave always attempted to measure competencies necessary for successfulpsychiatric practice. The mandate of the ABMS to focus on the corecompetencies formalized this practice by designating six categories ofcompetencies to be considered. The Accreditation Council for GraduateMedical Education and the ABMS facilitated the development of listingof competencies in each of the six competency areas through the work ofthe medical specialty quadrads (discussed in Chapter 4: “The ACGME andABMS Initiatives Toward the Development of Core Competencies”). Thework of the ABPN Invitational Core Competencies Conference in June2001 examined those categories especially pertinent to psychiatry andneurology, revised and added competencies as deemed necessary, and be-gan discussion of competency assessment issues. The ABPN Core Com-petency Committee, appointed late in 2001, held its first meeting inJanuary 2002.
This committee was charged with
a. Developing an infrastructure for surveying the field, reviewing, andvalidating core psychiatry and neurology competencies on an ongoingbasis.
b. Determining which core competencies should be assessed throughtraditional ABPN certification processes and which through the ABPNMaintenance of Certification (MOC) Program.
The board will assist the committee with the integration of the core com-petencies into the field by having discussions with appropriate institu-tions and organizations.

130 The Impact of Core Competencies
Thus, it is both correct and appropriate to say that the introduction ofcore competencies into the certification work of the ABPN has not sub-stantially changed the vision of the board, but instead the core compe-tencies have provided a structured format for achieving its mission. Theultimate goal, serving the American public by providing the means ofcertifying psychiatrists, has become more structured and more formal-ized.
The core competencies, when fully integrated into the course of med-ical education and residency and when correlated with the ABPN writtenand oral certification examinations, should provide a comprehensive struc-ture for the initial assessments of physician competencies.
The core competencies structure, especially by delineating competen-cies in the area of Practice-Based Learning and Improvement and in thearea of Systems-Based Practice, points out the necessity for more thaninitial certification.
The Core Competencies and the Maintenance of Certification© Program
Recertification’s Evolution Into a Maintenance of Certification© Program
Chronologically parallel with the development of the core competenciesstructure came the realization on the part of the ABMS that even the re-certification of physicians on a periodic basis was not sufficient to main-tain the public trust. The public both demanded and deserved to knowthat their physicians maintained a level of competence that was morethan what could be shown by the successful completion of a daylongwritten examination in psychiatry every 10 years.
To this end, the ABMS developed its four-part Maintenance of Certi-fication© program, into which the written recertification examination hassince been subsumed. The four parts of the MOC program are
1. Evidence of Professional Standing2. Evidence of Lifelong Learning and Periodic Self-Assessment3. Evidence of Cognitive Expertise4. Evidence of Evaluation of Practice Performance
All 24 member boards of the ABMS were directed to implement a MOCprogram suitable for their diplomates.

Core Competencies and ABPN Certification and Recertification 131
The Core Competencies and the ABPN Maintenance of Certification Program
Core competencies clearly relate to all four elements of the ABPN MOCprogram. In some cases, one category of core competencies clearly and/or primarily relates to one of the elements of the ABPN MOC Program.For example, the requirement for licensure, handled by state licensingbodies and not the ABPN, clearly relates to the category of Professional-ism Core Competencies. While it would not be correct to say that everylicensed physician has met all of the competencies within the Profession-alism category, it would be correct to assume that an unlicensed physi-cian is seriously deficient enough in the area of Professionalism that he orshe does not merit continued certification.
The second element of the ABPN MOC Program, Lifelong Learningand Periodic Self-Assessment, relates most directly to the Practice-BasedLearning and Improvement Core Competency Category. The relation-ship between this element of the ABPN MOC Program and the above-named core competency category will be developed from recommenda-tions the ABPN MOC Committee makes to the full ABPN board. TheABMS has directed its member boards that this component of eachboard’s MOC Program must be satisfied according to the dictates of theindividual member boards before physicians can be admitted to sit forthe recertification examination.
Various ABMS member boards have begun delineating requirementsto document lifelong learning. Physician learning after residency has tra-ditionally been measured in units of continuing medical education(CME) credits. Although some ABMS member boards will continue touse CME credits as a measure of lifelong learning, it is anticipated that abetter system—one that reflects educational efforts that will improve prac-tice—will be developed for those wishing to recertify through the ABPN.As this process is developed and formalized, it will be communicated bytraditional methods, such as the ABPN Annual Report published in theAmerican Journal of Psychiatry, as well as newer means, such as the ABPNDiplomate newsletter and on the ABPN Web site (www.abpn.com).
The third element of the ABPN MOC Program, cognitive expertise,will be handled for psychiatrists through the ABPN recertification ex-aminations. The ABMS mandates that these examinations be secure andproctored, and, as stated earlier, evidence of lifelong learning and self-assessment must be documented prior to the administration of such exam-inations. It is anticipated that recertification examinations will be closelymodeled on the ABPN written certification (Part I) examinations, but withprimary focus on applications to practice rather than on basic sciences.

132 The Impact of Core Competencies
The ABPN Board of Directors has instructed the ABPN MOC Com-mittee to focus their initial efforts on the first three elements of the MOCprogram as discussed above. The fourth element of the ABPN MOC pro-gram, the assessment of practice performance, will be implemented last.As this assessment becomes formalized, details will be communicatedthrough the various media described above.
Implications of the Core Competencies on the ABPN Maintenance of Certification Program
The ABPN supports the mandate of the ABMS to evolve the recertifica-tion examination into a MOC program. Regarding the ABPN’s progresstoward implementing the four elements of the MOC program, the fol-lowing can be said:
1. Regarding evidence of professional standing, the ABPN foresees nomajor change in its current procedure of requiring a full, unrestrictedmedical license at the time of registration for the administration of therecertification examination.
2. The ABPN MOC Committee will establish acceptable procedures forthe documentation of lifelong learning and self-assessment on the partof individual physicians prior to their registration for the recertifica-tion examination. It is likely that this effort will be carried out in co-operation with relevant professional specialty societies.
3. The ABPN will model its recertification examinations on the MCQformat of the ABPN written certification (Part I) examination. Therecertification examination will focus on the core competencies asthey apply to physicians in practice. Only physicians who have metthe two criteria listed above will be able to register for the recertifica-tion examination. All recertification examinations will be given oncomputer.
4. The last part of the ABPN MOC program to be implemented will bethe assessment of performance in practice. The MOC Committee willbe responsible for this procedure and making recommendations to theboard.
All aspects of the ABPN MOC program will be discussed in the ABPNDiplomate newsletter and on the ABPN Web site (www.abpn.com).

133
Chapter 13
Implications of the Core Competencies on the Full Spectrum of Psychiatric Medical Education for Clinical Psychiatric Practice
From Medical School Through Continuing Medical Education
Thomas A. M. Kramer, M.D.
From Time-Based to Competency-Based Medical Education
It would be difficult to overstate the potential impact on medical educa-tion in general, and psychiatric education in particular, of the core com-petency movement. The shift toward basing education on the acquisitionof specific competencies as opposed to time-limited rotations representsa sea change the likes of which probably has not been seen since the in-stitution of the Flexner Report, which precipitated the transition fromapprentice-based medical training to curriculum-based medical training.

134 The Impact of Core Competencies
Medical education as a whole remains a time-driven enterprise. Ittakes 4 full-time years to graduate from an American medical school.Graduate medical education has specific lengths of residency trainingranging from 3 to 7 years, depending on the specialty selected. Contin-uing medical education (CME) is measured in hours. Even the mostintriguing educational experiment in medicine is done by altering the se-quence of events still within prescribed time frames, or, at most, combin-ing and condensing time frames while providing the opportunity forcontinuity experiences in the case of combined training programs. It isonly with the core competency movement that the possibility exists thatendurance for a specific period of time will not be the primary criterionfor the completion of medical training.
This is not to say that there are not already some competency mea-sures in place within the medical education system as it currently exists.Medical students are graded with at least pass/fail grades, if not lettergrades, in their preclinical courses and their clinical rotations. They mustpass these if they are to proceed. They also have examinations, such as theUnited States Medical Licensing Examination Steps, that most schools re-quire for promotion and graduation. Graduate medical education hasfewer competency-based assessments required for its completion, andthese vary from specialty to specialty and from program to program.More than those in medical school, these assessments remain driven pri-marily by spending the requisite number of months and years doing re-quired rotations. CME in its current form is driven almost exclusively bytime. Although much CME has pre- and postassessments of the materialpresented, these assessments usually have little to do with the granting ofcredit. If physicians sit through the program, they earn the CME credit.Thus, there is a spectrum in which competency is assessed somewhat inmedical school, less so in graduate medical education, and even less so inCME.
Implications of the Core Competencies for Medical Schools
In medical schools, the impact of core competencies has already begunto be felt to a certain extent. Since many schools have comprehensive ex-aminations, particularly between preclinical and postclinical training,and students cannot proceed to the next phase unless they pass the exam,there is already some sense that at least this part of medical education re-quires some documentation of competency. Still, most clinical rotationsare time-driven, and successful completion of training is not competency-

Core Competencies and Psychiatric Medical Education 135
based in most institutions. Medical school, however, remains the only in-stitution within the sequence of medical education that seems to, at themoment, routinely require the demonstration of competency for promo-tion. It is also the institution that, in a functional sense, is most likely toadapt smoothly to the competency paradigm.
With the diminution, if not the elimination, of time as the importantcriterion for medical education, the question is then begged whether dif-ferent students can proceed through training at different rates of speed,thus making the length of medical school variable. If one achieves com-petency in all the things necessary to complete a program sooner ratherthan later, could he or she graduate sooner rather than later? Since medicalstudents pay tuition to attend school, it is perhaps possible that someonewho attains all the core competencies early could graduate early and thussave some tuition fees. Conversely, it would also be possible that thosestudents who are unable to attain all competencies within the prescribedtime could attend school longer, continuing to pay tuition for the privi-lege, until they have achieved competence in all things necessary for grad-uation. Medical students offset their cost to the institution, at least to acertain extent, and for the most part are not required members of thehealthcare team.
For all these reasons, shorter or longer courses of training are easier fora medical school to adapt to, and, as such, medical student education maybe the most flexible of the different medical education institutions in thetransition to a core competencies model.
Implications of the Core Competencies for Residency Programs
The application of core competencies to the graduate medical educationsystem, however, initially appears to be considerably more problematic.Although one can make the argument that the acquisition of competen-cies is even more crucial for a resident in specialty training, residents un-der the current system are funded for a specific number of years and areneeded by many of the hospitals that employ them to perform specifictasks for given periods of time. Rotations within a residency-training pro-gram are similar to a musical chairs game, with the same number of chairsat all times. When someone moves from one chair to another, there mustbe someone to fill the vacant chair and someone must give up a chair forthe first person to sit in. If residents take longer or shorter periods of timeto finish their training, funding formulas and clinical coverage at the train-ing institution will be affected. For residents who require a longer period

136 The Impact of Core Competencies
to attain the core competencies, there may not be funding, at least underthe current system, for them to train for a longer period of time. Simi-larly, if residents are able to attain the required competencies in a shorterperiod of time, the program may still need them present for the originallyagreed-on duration to be able to cover clinical service with the requisitenumber of physicians.
Implications of the Core Competencies for Continuing Medical Education
Continuing medical education will also be changed dramatically by corecompetencies. There has been a great deal of criticism of the currentCME system in terms of conflicts of interest by providers funded bypharmaceutical companies, the lack of meaningful assessment of theprograms and the physicians participating in them, and the relevance topractice of program content. Since all members of the American Boardof Medical Specialties are moving to time-limited certificates, physicianswill be required in some way to demonstrate competency at least sporad-ically. The institution of a Maintenance of Certification program by theABPN dovetails well with the core competency movement, in that it willrequire physicians on an ongoing basis to educate themselves, documentthe efficacy of that education, and demonstrate in some way that they areapplying that education in the form of competent practice. There is verylittle controversy that physicians need ongoing education in order tomaintain and increase their knowledge and skills. Core competencies,when promulgated and assessed, will hopefully make this process morestructured and more meaningful.
Additional Issues, Possible Solutions
The general issue of time versus competency in the completion of anymedical training program remains to be resolved. It is probably true thatit will be necessary for training programs to have a combination ofcompetency assessment and prescribed lengths of time at least withinguidelines. This may be necessary not just for smooth functioning of thetraining programs but also for the utility of requiring at least a minimumof time in training services to get a sense of the culture of those servicesbeyond the acquisition of core competencies.
Most of the current discussion concerning the transition to a core com-petency–driven educational system has centered on what the core com-petencies will be, who will write them, and what kind of latitude the

Core Competencies and Psychiatric Medical Education 137
various training programs will have with them. These concerns may be,to a certain extent, missing the point. Change is fundamental to the prac-tice of quality medicine. Treatments are continuously improving. The un-derstanding of health and disease issues continues to expand. Any kind ofrigidity in the determination of what core competencies are threatens tobe a regressive force that will lead to progressively obsolete competen-cies. Infrastructures need to be developed under which core competen-cies can be continually modified to stay current with the field. Thesechanges need to occur throughout the entire spectrum of medical educa-tion, as medical students need to be given the most current informationand skills, residents need to be taught to practice using the most recentlydeveloped treatments, and practicing physicians need to be kept up-to-date with the constant changes. The challenge will be for the accreditingbodies to develop a mechanism to revise the required competencies insome ongoing fashion, perhaps in ways similar to the manner in whichcertification boards continually update their exams.
Far and away the most difficult challenge of the institution of core com-petencies to the medical education infrastructure is the development ofappropriate assessment methodologies for all the competencies. Medicaleducation has been traditionally dependent on multiple-choice question(MCQ) examinations. While these exams are enormously effective inassessing medical knowledge and somewhat effective in determiningabilities in patient care, there are many parts of the six general categoriesof core competencies that cannot be assessed with such examinations.For example, the efficacy of communication, the establishment of rap-port with a patient, and issues of professionalism do not lend themselveseasily to assessment through MCQs.
Many certification boards give oral examinations to increase their as-sessment abilities, and medical schools are moving toward both actualpatient examinations and oral examinations as a way to assess their stu-dents. Other evaluation methodologies, such as computer-based testingwith vignettes and MCQs, portfolio reviews, and other standardized clin-ical scenarios, are in various phases of development. It is relatively easyto develop a list of competencies one would want a particular physicianto have. It is considerably more difficult to find reliable and valid methodsto assess whether that physician is indeed competent in those areas. Theextent to which the medical education establishment rises to this partic-ular challenge will, for the most part, determine the success or failure ofcore competencies in medical education.

This page intentionally left blank

139
Chapter 14
A Forward View
Core Competencies in Future Psychiatric Practice
Stephen C. Scheiber, M.D.Thomas A. M. Kramer, M.D.
Predicting the future is always an impossible task. Any discussion of thefuture impact of core competencies on clinical practice in psychiatryshould be intended only to provoke discussion, thought, and flexibility.Very few authors, if any, have had any success in predicting the directionthat healthcare in general will go. The many variables involved and themany unforeseen influences that have had a profound impact on the pro-vision of healthcare create overwhelming odds that any predictions madein this chapter will probably seem short-sighted in the years to come.
There are, however, some current general trends in healthcare. The fu-ture of these trends will probably be the primary determinants of theimpact of core competencies on clinical practice. One current trend is amove toward more competition among healthcare providers, probablyon the institutional level and perhaps even on the individual practitionerlevel. This appears to be where the managed care revolution is leading. Ifhealthcare decision making is going to be increasingly driven by market-ing issues, there will be a push toward concrete aspects that can be adver-tised as positive aspects of care. One can, for instance, easily note theincreased number of commercials on television and in print describinghospital systems or healthcare organizations as places where consumerswould receive optimum care.

140 The Impact of Core Competencies
As a result of this marketing, board certification of the physicianswithin given systems may become increasingly common. As a corollaryto hospitals advertising their board-certified psychiatrists, psychiatrists inprivate practice might market themselves as being board-certified. One pos-sible outcome of this trend is that there will be increased public aware-ness of the meaning of board certification. In 1999, the American Boardof Psychiatry and Neurology did a series of focus groups with consumersof psychiatric and neurological care. Focus group participants had virtu-ally no knowledge of the meaning of the term board certification. Onemight anticipate the meaning and the importance of board certificationincreasing through marketing enterprises already under way.
If public awareness of board certification increases and board certifica-tion becomes associated with the satisfactory demonstration of core com-petencies as described earlier in this book, then core competencies asdefined and assessed have at least the potential to become the central is-sue in healthcare. Practitioners will need to be able to demonstrate com-petency in order to attract and retain patients. The competition amongproviders will create marketing that will educate consumers so that theywill demand proficiency in core competencies in the physicians whomthey consult for healthcare.
Core competencies, as they are integrated into graduate medical edu-cation, have been described as hurdles for the physician-in-training to getpast. The transition, as described previously, between spending a certainamount of time in training as the primary determinant of competencyand actually demonstrating identified competencies should more appro-priately be described as a series of “checkpoints” in training. Some physi-cians-in-training will proceed easily through these training checkpoints,and others will be held back until they obtain the specified competency.This process may initially reduce the flow of physicians-in-training frombecoming full practitioners.
One example of this phenomenon is occurring now with the Educa-tional Commission for Foreign Medical Graduates (ECFMG) clinical skillsassessment examination. International medical graduates (IMGs) consti-tute a large group of physicians practicing in this country; in particular,they constitute a large group of the graduate medical education popu-lation. The ECFMG is now requiring that IMGs pass a clinical skills as-sessment (CSA) examination that uses standardized patients before theIMGs can enter approved residency training programs in this country.The CSA exam provides IMGs with the opportunity to demonstratetheir ability to interact with patients and make basic clinical decisions.Preliminary data from the ECFMG indicate that the CSA exam serves asan excellent means of ensuring that IMGs have skill levels that will allow

A Forward View 141
them to compete in the American medical residency program. The CSAexamination effectively creates a set of core competencies for IMGs. Thosewho do not demonstrate that they have achieved the necessary competen-cies are unable to enter into the U.S. medical education system. As morecore competencies are integrated into medical education and assessmentsare developed for them, it is likely that the CSA exam will mirror thesechanges.
The major impact of core competencies on clinical practice for the fu-ture is likely to be enormously positive. The reason for this is that corecompetencies can provide the healthcare system with a level of qualitycontrol it has never had, at least as far as physician competence is con-cerned. Currently, most people locate doctors by consulting lists in healthinsurance books or by having doctors recommended to them by a friendor another physician. There is currently no objective way to ascertain if aphysician is professionally competent. The core competency system hasthe potential to allow patients to approach the healthcare system with agreat deal more confidence that their doctors are competent and able toperform their duties. The trend toward demedicalizing a great deal ofhealthcare may also reverse itself as physician’s assistants, nurse practitio-ners, and psychologists are unable to demonstrate the delineated physi-cian core competencies. Core competencies, as defined, would make itvery clear exactly what physicians are trained to do and which tasks areinappropriate for nonphysicians.
One major problem in current healthcare is the limited extent to whichpracticing physicians are monitored. With core competencies integratedinto Maintenance of Certification© programs, physicians who are unableor unwilling to keep up with their fields will not be able to demonstrateongoing competency and will be eliminated from practice. In medicine,the wisdom of age is often counterbalanced by the lack of new knowl-edge. Core competencies would reassure patients that their senior physi-cians are keeping up-to-date and also counteract the trend that youngerdoctors tend to be more current than older ones. It is easy to say that alldoctors should keep up with their field. Core competencies provide a sys-tem, an infrastructure, to ensure that.
To reiterate, it is very difficult to predict the future. The impact of corecompetencies on clinical practice very much remains to be seen. It is safeto predict, however, that the effect of core competencies on future prac-tice will be both profound and positive. Implementation of core compe-tencies into physician training and into Maintenance of Certification©
programs should lead to the overall improvement of healthcare.

This page intentionally left blank

143
Appendix A
Psychiatry Quadrad Core Competencies Outline
Appendix A presents the first draft of psychiatric core competencies.This draft was developed by a “quadrad” (group of four) that was namedby the Accreditation Council for Graduate Medical Education (ACGME)and the American Board of Medical Specialties (ABMS). The ACGMEand ABMS named a quadrad for each recognized medical specialtyboard, with two quadrads being named for the American Board of Psy-chiatry and Neurology (ABPN), as the ABPN represents two major med-ical specialties.
The list of psychiatric competencies in Appendix A was developed byDr. Glenn C. Davis representing the ABPN; Dr. Andrew Russell repre-senting the Psychiatry RRC; Dr. John Herman, the psychiatry programdirector at Massachusetts General/McLean Hospital; and Dr. Mara Gold-stein, representing psychiatry residents.
This work product of the psychiatry quadrad was merged with a sim-ilar outline developed by the neurology quadrad for use at the ABPNInvitational Core Competency Conference. Organizers of the conferencethought a merged outline appropriate for a group representing both spe-cialties. This merged outline served as the basis for the psychiatric corecompetencies developed at the conference and discussed in this book.

144 Core Competencies for Psychiatric Practice
Patient Care
1. The resident shall demonstrate the ability to perform and documenta comprehensive psychiatric history and examination in adult, geriat-ric, and child/adolescent patients to include
• Complete present and past psychiatric history• Social and educational history• Family history• Substance abuse history• Medical history and review of systems• Physical and neurological examination• Comprehensive mental status examination, including the assess-
ment of cognitive functioning
2. Based on a comprehensive psychiatric assessment (see no. 1), the res-ident shall demonstrate the ability to develop and document the fol-lowing:
• Complete DSM multiaxial differential diagnosis• Evaluation plan, including appropriate laboratory, medical, and
psychological examinations• Comprehensive treatment plan addressing biological, psychologi-
cal, and social domains
3. The resident shall demonstrate the ability to comprehensively assess,discuss, and document the patient’s potential for self-harm or harm toothers and intervene. This shall include
• Assessment of risk based on known risk factors• Knowledge of involuntary treatment standards and procedures• Effectively intervening to minimize risk
4. The resident shall demonstrate the ability to conduct therapeutic in-terviews, i.e., psychotherapy appropriate to the conduct of supportiveinterventions and exploratory interventions and clarifications. Theuse of this skill should further enhance the ability to collect and useclinically relevant material.
5. Evaluation of patient care may be measured by
• Caring and respectful behavior (standardized patients, patient ques-tionnaire)
• Interviewing (checklist, objective-structured clinical examination[OSCE])
• Informed decision making (chart-stimulated recall [CSR])• Patient management (CSR)

Psychiatry Quadrad Core Competencies Outline 145
• Counseling patients, families (standardized patients, OSCE, pa-tient questionnaire)
• Routine physical examinations (standardized patients, OSCE)• Medical procedures (checklist, simulations, models)• Preventive health services (record review, OSCE)• Working within a team (global rating [“360”])
Medical Knowledge
1. The resident shall demonstrate knowledge of the major psychiatricdisorders, based on the scientific literature and standards of practice.This knowledge shall include
• Epidemiology of the disorder• Etiology of the disorder, including (when known) medical, genetic,
and social factors• Phenomenology of the disorder• DSM diagnostic criteria• Effective treatment strategies• Course and prognosis
2. The resident shall demonstrate knowledge of psychotropic medica-tions including the antidepressants, antipsychotics, anxiolytics, moodstabilizers, hypnotics, and stimulants. The knowledge shall include
• Pharmacological action• Clinical indications• Side effects• Drug interactions• Toxicity• Appropriate prescribing practices
3. The resident shall demonstrate knowledge of substances of abuse.This knowledge shall include
• Pharmacological action• Signs and symptoms of toxicity• Signs and symptoms of withdrawal• Management of toxicity and withdrawal• Epidemiology, including social factors
4. The resident shall demonstrate relevant medical knowledge about med-ical conditions masquerading as psychiatric conditions, medicationsthat cause behavioral and cognitive change, and the management ofpsychiatric disorders in the setting of other medical illnesses.

146 Core Competencies for Psychiatric Practice
5. The resident shall demonstrate the ability to use information. Thiswill include skills in organizing the elicited information in order to di-agnose and treat patients from the full spectrum of ethnic, racial, gen-der, and education backgrounds. This will include skills in conductingtherapeutic interviews.
6. Medical knowledge may be measured by
• Analytic thinking (CSR, oral examinations)• Knowledge, basic science (multiple-choice questions [MCQs], oral
examinations)
Interpersonal and Communications Skills
1. Interpersonal skills refer to the ability of the psychiatrist to developand maintain therapeutic relationships with patients and work col-laboratively with professionals and the public.
2. Interpersonal skills require an underlying attitude of respect for oth-ers, even those with differing points of view or from different back-grounds; the desire to gain understanding of another’s position andreasoning; a belief in the intrinsic worth of other human beings; thewish to build collaboration; the desire to share information in aconsultative rather than dogmatic fashion; and the willingness tocontinuously self-observe and confront one’s own biases and trans-ferences.
3. Interpersonal skills are defined as the specific techniques and meth-ods that facilitate effective and empathic communication betweenthe psychiatrist, patients, colleagues, staff, and system.
4. The competent resident is able to demonstrate the following abili-ties:
• Listen to and understand patients• Communicate effectively with patients, using verbal, nonverbal,
and writing skills as appropriate• Foster a therapeutic alliance with patients, as indicated by instill-
ing feelings of trust, openness, rapport, and comfort in the rela-tionship with the physician
• Use negotiation to develop an agreed-on healthcare managementplan with patients
• Transmit information to patients in a clear, meaningful fashion• Understand the impact of the physician’s feelings and behavior
on psychiatric treatment• Communicate effectively with allied healthcare professionals and
with other professionals involved in the life of patients

Psychiatry Quadrad Core Competencies Outline 147
• Educate patients and professionals about medical, psychological,and behavioral issues
• Work effectively within multidisciplinary team structures as mem-ber, consultant, or leader
• Form relationships with patients and professionals in a culturallysensitive fashion
• Exhibit professional, ethically sound behavior and attitudes in allpatient and professional interactions
5. The resident shall demonstrate the ability to elicit information. Thiswill include skills in eliciting important diagnostic data and data af-fecting treatment from individuals from the full spectrum of ethnic,racial, gender, and education background. This will include skills intolerating and managing high levels of affect in the patients.
6. The resident shall demonstrate the ability to obtain, interpret, andevaluate consultations from other medical specialties. This shall include
• Formulating and clearly communicating the consultation question• Discussing the consultation findings with the consultant• Evaluating the consultation findings
7. The resident shall serve as an effective consultant to other medicalspecialists, mental health professionals, and community agencies.The resident should demonstrate the ability to
• Communicate effectively with the requesting party to refine theconsultation question
• Maintain the role of consultant• Communicate clear and specific recommendations• Respect the knowledge and expertise of the requesting party
8. The resident shall demonstrate the ability to communicate effec-tively with patients and their families by
• Providing explanations of psychiatric disorders and treatment(both verbally and in written form) that are jargon-free and gearedto the educational/intellectual level of the patient
• Providing preventive education that is understandable and prac-tical
• Respecting the patient’s cultural, ethnic, and economic back-ground
• Demonstrating the ability to develop and enhance rapport and aworking alliance with patients
9. The resident shall demonstrate the ability to manage his or her ownaffects and countertransference.

148 Core Competencies for Psychiatric Practice
10. The resident shall maintain psychiatric medical records that are
• Legible• Timely• Capturing essential information while simultaneously respecting
patient privacy• Useful to nonpsychiatric health professionals
11. The resident shall demonstrate the ability to effectively lead a multi-disciplinary treatment team. This skill includes the ability to
• Listen effectively• Elicit needed information from team members• Integrate information from different disciplines• Manage conflict• Clearly communicate an integrated treatment plan
12. The resident shall demonstrate the ability to effectively communi-cate with the patient and his or her family (while respecting confi-dentiality). Communications may include
• Results of the assessment• Risks and benefits of the proposed treatment plan, including pos-
sible side effects of psychotropic medications• Alternatives (if any) to the proposed treatment plan• Education concerning the disorder, its prognosis, and prevention
strategies
13. Skills would be rated by clinical supervisors using a Likert scale, withsuggestions for improvement. Interactions used to evaluate interper-sonal skills include direct observation in both clinical and examina-tion settings, videotape observation, and supervisory evaluationsfrom clinical rotations. Identified deficiencies should be followed upby suggestions for improvement and specific objectives and timeline for evaluation of successful remediation.
• Create therapeutic relationship (standardized patients, OSCE,patient questionnaire)
• Listening skills (standardized patients, OSCE, patient question-naire)
Practice-Based Learning and Improvement
1. Psychiatrists must recognize and accept limitations in one’s knowl-edge base and clinical skills and understand the need for lifelong learn-ing.

Psychiatry Quadrad Core Competencies Outline 149
2. The resident will have appropriate skills and demonstrate obtainingup-to-date information from the scientific and practice literature andother sources to assist in the quality care of patients. This shall includebut not be limited to
• Use of medical libraries• Use of information technology, including Internet-based searches
and literature databases (e.g., Medline)• Use of drug information databases
3. The resident shall evaluate caseload and practice experience in a sys-tematic manner. This may include
• Maintaining patient logs• Reviewing patient records and outcomes• Obtaining evaluations from patients (e.g., outcomes and patient
satisfaction)• Obtaining appropriate supervision• Maintaining a system for examining errors in practice and initiating
improvements to eliminate or reduce errors
4. The resident shall demonstrate the ability to critically evaluate psy-chiatric literature. This may include
• Using knowledge of common methodologies employed in psychi-atric research to evaluate studies, particularly drug treatment trials
• Conducting and presenting reviews of current research in such for-mats as journal clubs, grand rounds, and/or original publications
• Researching and summarizing a particular problem that derivesfrom the resident’s caseload.
5. The resident shall be able to
• Review and critically assess scientific literature to determine howquality of care can be improved in relation to one’s practice (i.e.,reliable and valid assessment techniques, treatment approaches withestablished effectiveness, practice parameter adherence) (Withinthis aim, the resident should be able to assess the generalizabilityor applicability of research findings to one’s patients in relation totheir sociodemographic and clinical characteristics.)
• Develop and pursue effective remediation strategies that are basedon critical review of scientific literature
6. Practice-based learning and improvement may be measured throughthe following:
• Analysis of one’s own practice (portfolio)• Evidence from science studies (record review, CSR, MCQs, oral

150 Core Competencies for Psychiatric Practice
examination, portfolio)• Application of research and statistics (portfolio)• Use of information technology (global rating, portfolio)• Facilitating the learning of others (global rating)
Professionalism
1. The resident will respond to communications from patients andhealth professionals in a timely manner. If unavailable, the residentwill establish and communicate backup arrangements. The residentcommunicates clearly to patients concerning how to seek emergent andurgent care when necessary.
2. The resident shall demonstrate ethical behavior, as defined in the Prin-ciples of Medical Ethics With Special Annotations for Psychiatry (Amer-ican Psychiatric Association).
3. The resident shall demonstrate respect for patients and colleagues aspersons, including their age, culture, disabilities, ethnicity, gender, andsexual orientation.
4. The resident shall ensure continuity of care for patients and when itis appropriate to terminate care, doing so appropriately and not “aban-doning” patients.
5. Professionalism may be measured by behavior that is
• Respectful, altruistic (OSCE, patient questionnaire)• Ethically sound (global rating)• Sensitive to culture (OSCE, global rating)
Systems-Based Practice
1. The resident shall be able to articulate the basic concepts of systemstheory and how it is used in psychiatry. The resident should have aworking knowledge of the diverse systems involved in treating chil-dren and adolescents, and understand how to use the systems as partof a comprehensive system of care in general and as part of a compre-hensive, individualized treatment plan.
2. In the community system, the resident shall have
• Knowledge of the resources available both publicly and privatelyfor the treatment of psychiatric/behavioral problems impacting apatient’s ability to enjoy relationships and gain employment
• Knowledge of the legal aspects of mental health as they impact pa-tients (and their families) with psychiatric problems

Psychiatry Quadrad Core Competencies Outline 151
3. The resident should demonstrate knowledge of and interact withmanaged behavioral health systems. This shall include
• Participating in utilization review communications and, when ap-propriate, advocating for quality patient care
• Educating patients concerning such systems of care
4. Demonstrate knowledge of community systems of care and assistpatients in accessing appropriate psychiatric care and other mentalhealth support services. This requires a knowledge of psychiatric treat-ment settings in the community that include ambulatory, consulting,inpatient, partial hospital, and substance abuse facilities; halfwayhouses; nursing homes; and hospices. The resident should demon-strate knowledge of the organization of care in each relevant deliverysetting and the ability to integrate the care of patients across such set-tings.
5. Systems-based practice skills may be measured by the following:
• Understanding of interactions with system (global rating)• Knowledge of practice and delivery system (MCQs)• Practicing cost-effective care (checklist)• Advocating for patients (global rating, patient questionnaire)

This page intentionally left blank

153
Index
Page numbers printed in boldface type refer to tables or figures.
ABMS. See American Board of Medical Specialties
ABPN. See American Board of Psychiatry and Neurology
ABPN Annual Report, 131ABPN Diplomate, 131, 132Accountability, 104–107Accreditation Council for Graduate
Medical Education (ACGME), 2. See also ACGME/ABMS quadrads
and ABPN certification examination, 129
and core competencies, 44–47, 48–51
functions of, 37ACGME. See Accreditation Council
for Graduate Medical EducationACGME/ABMS quadrads, 47–54
in neurologycomparison with psychiatry,
47–52merged with psychiatry, 53–54
in psychiatry, 47–52, 143–151comparison with neurology,
47–52merged with neurology, 53–54
Addiction psychiatry, 75Advance standards, 23–42
Advisory Board of Medical Specialties, and American Board of Psychiatry and Neurology, 10–11
Advocacy. See Health advocacy; Health advocate
AMA. See American Medical Association
American Board of Dermatology, formation of, 8
American Board of Medical Specialties (ABMS), 2. See alsoACGME/ABMS quadrads
and ABPN certification examination, 129
and core competencies, 44, 45–46,47, 48–51, 80
functions of, 37on lifelong learning, 91–95and Maintenance of Certification
Program, 47, 61and time-limited certification,
125–126as umbrella organization, 7
American Board of Obstetrics and Gynecology, formation of, 8
American Board of Ophthalmology, formation of, 8, 11

154 Core Competencies for Psychiatric Practice
American Board of Otolaryngology, formation of, 8, 11
American Board of Psychiatry and Neurology (ABPN)
and ACGME/ABMS quadrads, 52certification examination of
(See Certification examina-tion, of American Board of Psychiatry and Neurology)
Core Competency Committee of, 129
dual board issues of, 10–13formation of, 8–11, 120Information for Applicants of, 11–13Invitational Core Competencies
Conference of, 23, 55–57, 103–104, 120–121, 127, 128, 129, 143
and Maintenance of Certification Program, 61
mission of, 125–126name of, 11Task Force on Core Competencies
of, 52American Journal of Psychiatry, 131American Medical Association
(AMA)and American Board of Psychiatry
and Neurology formation, 8–9Council on Medical Education and
Hospitals of, 10–11Section on Nervous and Mental
Diseases of, 9, 120American Neurological Association,
and American Board of Psychiatry and Neurology formation, 9
American Psychiatric Association (APA), and American Board of Psychiatry and Neurology formation, 8–9
ANA. See American Neurological Association
APA. See American Psychiatric Association
Behavioral science, knowledge of, 72Board certification, public awareness
of, 140
Canada. See also CanMEDS 2000 Project
medical schools in, 37specialty competencies in, role
framework of, 23–42CanMEDS 2000 Project
background of, 23–25core competencies of, 48–51examination blueprints of, 40, 41implementation of, 37–38implications for American medical
system, 36–40at residency level, 38–40, 39role framework of, 25–33, 27–28
and faculty development, 33–36implementation of, 33, 34–35
Societal Needs Working Group and, 25
specialty-specific objectives of, 37–38, 38
CanMEDS 2000 Project Report, 23–25Caseload, evaluation of, 98–99Certification
dual board, 10–13grandfathering in, 13lifetime, 91maintenance of (See Maintenance
of Certification Program)medical competence and, 7time-limited, 91, 125–126
Certification examinationsof American Board of Psychiatry
and Neurology, 10–16clinical section of, 13, 15–16,
127–128core competencies and,
125–130medical knowledge section of,
52–53oral section of, 12, 14, 15,
127–129

Index 155
prerequisites for, 9–10qualifications for, 10structure of, changes in, 12–13videotape section of, 15–16written section of, 13–15,
126–127in neurology, 120oral section of, 137in psychiatry, 120question pool in, 63of Royal College of Physicians and
Surgeons, blueprints of, 40, 41scope of, 63
Child and adolescent psychiatry, 74Clinical competence, in psychiatric
practice, 7–16Clinical interview, in ABPN
certification examination, 13, 15–16, 127–128
Clinical judgment, as ABMS core competency, 45
Clinical practice, in CanMEDS 2000 Project, 26
Clinical science. See Medical Knowledge Core Competencies
Clinical skills, as ABMS core competency, 45
Clinical skills assessment (CSA) examination, 140–141
CME. See Continuing Medical Education
Cognitive expertise, in Maintenance of Certification Program, 131, 132
Collaboration, as Interpersonal and Communications Skills Core Competency, 83
Collaborator, physician as, 27, 29, 49
implementation of, 34Communication Skills. See Inter-
personal and Communications Skills Core Competencies
Communicator, physician as, 27,28–29, 48, 49
implementation of, 34
Community-based services, 111, 114–116
Compassion, 105Competence
and certification, 7measurement of, 4
Confidentiality, 86–87, 105Conflicts of interest, 105Consultation-liaison psychiatry, 74Consultation skills, in CanMEDS
2000 Project, 28Consultations
from other physicians, 84to other physicians, 84–85
Continuing education, 32Continuing medical education
(CME), 131, 134core competencies and, 136criticisms of, 97–98
Core competencies. See also specificcore competencies
Accreditation Council for Graduate Medical Education and, 48–51
American Board of Medical Specialists and, 48–51
American Board of Psychiatry and Neurology certification and, 125–130
assessment methodologies for, development of, 137
in Canada, role framework of, 23–42
of CanMEDS 2000 Project, 48–51categories of, assumptions
regarding, 79–80and continuing medical education,
136definition of, 1, 4–5development of, 19–21, 43
groups involved in, 44future of, 139–141impact of, 123–124and Maintenance of Certification
Program, 130–132, 141

156 Core Competencies for Psychiatric Practice
Core competencies (continued)and medical education, 133–137outlines of,
Patient Care, 68Medical Knowledge, 76–78Interpersonal and Communica-
tions Skills, 88–89Practice-Based Learning and
Improvement, 102Professionalism, 108Systems-Based Practice, 118
and recertification, 125–126and residency programs, 135–136,
140Counseling, knowledge of, 71Cross competencies, 119–122CSA examination. See Clinical skills
assessment examinationCulturally diverse patients, 60–62
Diagnostic data, 83–84Diagnostic skills, in CanMEDS 2000
Project, 26Differential diagnoses
as General Patient Care Core Competency, 63
as Psychiatry Patient Care Core Competency, 64–65
Disorders, knowledge of, 70–71
ECFMG. See Educational Commis-sion for Foreign Medical Graduates
Educating Future Physicians for Ontario Project (EFPO), 25
Educational Commission for Foreign Medical Graduates (ECFMG), 140–141
Educational outcomes, 1, 43EFPO. See Educating Future
Physicians for Ontario ProjectEmergency psychiatry, 73Ethics, 33, 71, 105Evaluation, as Psychiatry Patient Care
Core Competency, 64–65
Examination blueprints, of CanMEDS 2000 Project, 40, 41
Faculty development, in CanMEDS 2000 Project, 33–36
Familiescommunication with, 85counseling of, 71respect for, 105–106
Final In-Training Evaluation Reports (FITER), 38–40, 39
FITER. See Final In-Training Evaluation Reports
Flexner Report, 133Forensic psychiatry, 74
General Medical Knowledge Core Competencies, 70–71, 76
first, 70–71second, 71third, 71fourth, 71
General Patient Care Core Competencies, 68
first, 60–62, 68second, 63, 68third, 63–64, 68
Geriatric psychiatry, 74–75Graduate medical education, 134,
135–136, 140Grandfathering, in certification, 13
Harm to others, assessment of, 65Health advocacy, as ABMS core
competency, 46Health advocate, physician as, 27,
30–31, 50examination blueprints for, 41implementation of, 34training objectives for, 38
Healthcare, future of, 139–140Healthcare delivery systems,
knowledge of, 71Healthcare providers, competition
among, 139–140

Index 157
Honesty, 105Human growth and development,
knowledge of, 72
Illnesses, knowledge of, 70–71IMGs. See International medical
graduatesImprovement. See Practice-Based
Learning and Improvement Core Competencies
Information for Applicants, 11–13Information technology, 30, 71,
96–98Informed consent, 105Institute of Medicine, 110Insurance carriers
and core competencies development, 1
and specialty medical services, 3–4
Integrity, 105Interdisciplinary teams, in CanMEDS
2000 Project, 29International medical graduates
(IMGs), 140–141Interpersonal and Communications
Skills Core Competencies, 79–87, 88–89, 146–148
first, 81–83second, 83–84third, 84fourth, 84–85fifth, 85sixth, 85–86seventh, 86eighth, 86–87assumptions regarding, 80in certification examination, 128
Interpersonal skills, as ABMS core competency, 45, 49
Invitational Core Competencies Conference, of American Board of Psychiatry and Neurology, 23, 55–57, 103–104, 120–121, 127, 128, 129, 143
Legal issues, 115Licensure, and Maintenance of
Certification Program, 131, 132Lifelong Learning and Periodic Self-
Assessment, in Maintenance of Certification Program, 61, 93–94, 131, 132
Maintenance of Certification (MOC) Program, 47, 61
cognitive expertise in, 131, 132components of, 92–95, 130and continuing medical education,
136core competencies and, 130–132,
141Lifelong Learning and Periodic
Self-Assessment in, 61, 93–94, 131, 132
practice-based assessment in, 94–95, 132
and Practice-Based Learning and Improvement Core Competencies, 91–95
professional standing in, 131, 132
and recertification, 94Managed care, 4, 115–116Manager, physician as, 27, 30, 49
implementation of, 34Managerial skills, as ABMS core
competency, 46Marketing, of healthcare, 139–140MCQs. See Multiple choice questionsMedical care
changes in, 3–4patient involvement in, 3specialty services in, 3–4
Medical care systems, interconnections of, 110–111
Medical credentials, 4Medical education
in Canada, 37core competencies and, 133–137graduate, 134, 135–136, 140
158 Core Competencies for Psychiatric Practice
Medical education (continued)time-based vs. competency-based,
133–134tuition in, 135in United States, 37
Medical errors, 106Medical expert, physician as, 26–28,
27, 48Final In-Training Evaluation
Reports for, 39implementation of, 34
Medical expertise, in CanMEDS 2000 Project, 26
Medical information, critical appraisal of, 32
Medical knowledgeas ABMS core competency, 45, 48access to, 3growth of, 92personal limitations and, 95–96
Medical Knowledge Core Competencies, 48, 69–78
assumptions regarding, 69–70in certification examination
oral section, 128written section, 127
and cross competencies, 119General, 70–71, 76
first, 70–71second, 71third, 71fourth, 71
Neurology-Specific, 75, 121–122Psychiatry-Specific, 72–75, 76–78,
145–146first, 72second, 72third, 73–75
Medical literature, critical evaluation of, 99–100
Medical records, maintenance of, 85–86
Medical science, changing nature of, 137
Meyer, Adolf, 8, 9, 10
Mikhael, Nadia Z., 56–57MOC Program. See Maintenance of
Certification ProgramMultidisciplinary teams, 86Multiple-choice questions (MCQs),
64, 127, 137
National Board of Medical Examiners (NBME), and American Board of Psychiatry and Neurology certification examination, 14
National Institute of Mental Health, formation of, 8
NBME. See National Board of Medical Examiners
Neurologists, representation of, on American Board of Psychiatry and Neurology, 11
NeurologyACGME/ABMS quadrad of
comparison with psychiatry, 52–53
merged with psychiatry, 53–54certification examination in, 16,
120 (See also American Board of Psychiatry and Neurology, certification examination of)
cross competencies with psychiatry, 119–122
double board with psychiatry (See American Board of Psychiatry and Neurology)
ethics in, 71Neurology-Specific Core Competen-
cies for Psychiatrists, 121–122Neurology-Specific Medical
Knowledge Core Competencies, 75, 121–122
Neurology-Specific Patient Care Core Competencies, 67, 121
Nonverbal communication, 81
Patient(s)autonomy of, 114–115communication with, 85

Index 159
culturally diverse, 60–62evaluation of, 73–75involvement in medical care, 3respect for, 105–106selection of physician by, 141
Patient Care Core Competencies, 48,59–67
assumptions regarding, 59–60in certification examination
oral section, 128written section, 127
and cross competencies, 119General, 60–64, 68
first, 60–62, 68second, 63, 68third, 63–64, 68
in Maintenance of Certification Program, 61, 62
Neurology-Specific, 67, 121outline of, 59–60Psychiatry-Specific, 64–67, 68,
144–145first, 64–65, 68second, 65, 68third, 66, 68fourth, 66–67, 68
Physician(s)accountability of, 104–105,
106–107in Canada, role framework of,
23–42as collaborator, 27, 29, 34,
49as communicator, 27, 28–29, 34,
48, 49as health advocate, 27, 30–31, 34,
38, 41as manager, 27, 30, 34, 49as medical expert, 26–28, 27, 34,
39, 48patient selection of, 141personal feelings/beliefs/behavior
of, as Interpersonal and Communications Skills Core Competency, 82
as professional, 28, 32–33, 35, 50and research, 32roles of, in CanMEDS framework,
24, 25, 26–33, 27–28as scholar, 27, 31–32, 35, 41, 49,
50as teacher, 32, 83
Portfolio development, for assessment, 67
Practice Assessment Component, of Maintenance of Certification Program, 61, 94–95, 132
Practice-Based Learning and Improvement Core Competen-cies, 49, 91–101, 102, 148–150
first, 95–96second, 96–98third, 98–99fourth, 99–100assumptions regarding, 95in certification examination, oral
section, 128and Maintenance of Certification
Program, 91–95, 131relation to other core
competencies, 91–95validation of, 100–101
Practice experience, evaluation of, 98–99
Private practice, 110, 111Professional, physician as, 28, 32–33,
50implementation of, 35
Professional attitudes and behavior, as ABMS core competency, 45–46
Professional conduct, 105of colleagues, 106self-assessment of, 106
Professional standingevidence of, 93in Maintenance of Certification
Program, 131, 132Professionalism Core Competencies,
50, 103–107, 108, 150first, 104

160 Core Competencies for Psychiatric Practice
Professionalism Core Competencies (continued)
second, 104–105third, 105fourth, 105–106fifth, 106sixth, 106–107seventh, 106–107eighth, 106–107assumptions regarding, 103–104in certification examination, oral
section, 128and Maintenance of Certification
Program, 131Program directors, and Patient Care
Core Competencies, 62, 64, 65, 66, 67
Psychiatric assessment, 65Psychiatrists, representation of, on
American Board of Psychiatry and Neurology, 11
PsychiatryACGME/ABMS quadrad of,
47–52, 143–151comparison with neurology,
52–53merged with neurology, 53–54
certification examination in, 120, 126–130 (See also American Board of Psychiatry and Neurology, certification examination of)
oral section of, 127–129written section of, 126–127
cross competencies with neurology, 119–122
double board with neurology (SeeAmerican Board of Psychiatry and Neurology)
ethics in, 71as medical specialty, development
of, 7–8Psychiatry Patient Care Core
Competencies, 64–67first, 64–65
second, 65third, 66fourth, 66–67
Psychiatry-Specific Medical Knowledge Core Competencies, 72–75, 76–78, 145–146
first, 72second, 72third, 73–75
Psychiatry-Specific Patient Care Core Competencies, 68, 144–145
first, 68second, 68third, 68fourth, 68
Psychosocial therapies, 73
Quality assurance program, 98–99
Recertification, 94core competencies and, 125–126Maintenance of Certification
Program and, 130–132Referrals, 110, 111Regulations for the Guidance of the
Board in Certification in Psychiatry and Neurology in Establishing the Requirement for Such Certificates, 9–10
Researchapplicability of, 100critical evaluation of, 99–100physician involvement in, 32
Residency programsassessment in, 134
in CanMEDS 2000 Project, 38–40, 39
core competencies and, 135–136, 140
Resource management, in CanMEDS 2000 Project, 30
Resources, 114–115Royal College of Physicians and
Surgeons of Canada, 23–42examination blueprints of, 40, 41

Index 161
Health and Public Policy Committee of, 24
Office of Education of, 24Educational Research and
Development Unit of, 37
size and scope of, 36–37specialty committees of, 24
Scholar, physician as, 27, 31–32, 49,50
examination blueprints for, 41implementation of, 35
Scientific literature, critical evaluation of, 99–100
Self-harm, assessment of, 65SNWG. See Societal Needs Working
GroupSocial constraints, 114Social psychiatry, knowledge of, 72Societal Needs Working Group
(SNWG)and CanMEDS 2000 Project, 25and Educating Future Physicians
for Ontario Project, 25Sociocultural issues, 60Somatic treatments, 73Specialty medical services
in Canada, role framework of, 23–42
historical development of, 7–8patient demands for, 3–4physician roles in, 26–33, 27–28
Standards of conduct, attempts to establish, 10
Substance abuse, 74Systems-Based Practice Core
Competencies, 51, 109–117, 118
first, 112–114second, 114third, 114–115fourth, 115fifth, 115–116sixth, 116
in certification examinationoral section, 128written section, 127
and cross competencies, 119defining, 109–112validation of, 116–117
Systems theory, working knowledge of, 112–114
SNWG. See Societal Needs Working Group
Teacher(s)physician as, 32, 83standards for, 19–20
Teamsinterdisciplinary, 29multidisciplinary, 86
Therapeutic alliance, 81Therapeutic interviews, 66Therapeutic relationship, in
CanMEDS 2000 Project, 28Therapeutic skills, in CanMEDS 2000
Project, 26Third-party payers
and core competencies, 1and specialty medical services, 3–4
Time management, in CanMEDS 2000 Project, 30
To Err Is Human: Building a Safer Health System, 110
Treatment of patientsas General Patient Care Core
Competency, 63–64as Interpersonal and Communica-
tions Skills Core Competency, 82
as Psychiatry-Specific Medical Knowledge Core Competency, 73–75
as Psychiatry-Specific Patient Care Core Competency, 64–65, 66–67
as Systems-Based Practice Core Competency, 112–114
Tyler, Ralph, 43

162 Core Competencies for Psychiatric Practice
United Statesinternational medical graduates in,
140–141medical schools in, 37medical systems in, implications of
CanMEDS for, 36–40U.S. Department of Education, and
core competencies development, 1, 43
Videotape section, of ABPN certification examination, 15–16, 127–128
Youker, James E., 109–110

“A serious effort by the American Board of Psychiatry and Neurology, Inc.,to define and evaluate the core competencies thought to be both neces-sary and sufficient for certified psychiatrists to possess. The competenciesare modeled after the six competencies recommended by the Accredita-tion Council for Graduate Medical Education (ACGME) and the Amer-ican Board of Medical Specialties (ABMS). While the major focus of thebook is the processes leading to initial certification, the competencies andtheir evaluation in practicing psychiatrists as they participate in the Main-tenance of Certification© Program of the American Board of Psychiatryand Neurology are also discussed in detail.”—Stephen H. Miller, M.D.,M.P.H., Executive Vice President, American Board of Medical Specialties,Adjutant Professor of Surgery, Northwestern University
“Stephen C. Scheiber, M.D., and colleagues have provided the psychiatriccommunity with a comprehensive review of the core competencies ini-tiative. This volume reviews the process by which the competencies weredeveloped, the nature of each of the competencies, and possible methodsof assessment. This will be a useful guide for program directors, residents,academic faculty, and practitioners of psychiatry as they prepare for con-tinued maintenance of certification. To the larger medical community,this volume also provides an exemplar of how a specialty can respondproductively to the competency initiative toward the aim of enhancingpatient care and physician formation.”—David C. Leach, M.D., ExecutiveDirector, Accreditation Council for Graduate Medical Education, Chicago,Illinois
“If you have heard the words ‘core competencies’ and aren’t quite surewhat they mean, help is on the way. Most psychiatric educators have al-ready been grappling with the issues of determining competency in theirresidents, since the Accreditation Council for Graduate Medical Educa-tion introduced competency requirements for residencies in 2000. Yetmany questions remain. This timely book describes the history, the presentstate, and future directions of the core competency movement in medi-cine, with particular attention to psychiatry. Several chapters cover whathas already been accomplished in the defining and assessing of core com-petencies in psychiatric residency training. Dr. Nadia Mikhael’s chapteron the Canadian approach to competency is particularly instructive andthought provoking, since the Canadians began working on competencyguidelines in 1993. This book is essential reading for all psychiatric edu-cators and those concerned with the future of psychiatric education inthe United States.”—Deborah J. Hales, M.D., Director, Division of Educa-tion, Minority and National Affairs, American Psychiatric Association,Washington, D.C.

“This text is an outstanding, comprehensive review of the historical per-spective, evolution and development, proposed details of implementa-tion, and the possible impact of the core competencies on the field ofpsychiatry. In addition, it challenges every educator to ponder the ques-tions What do we want the next generation of psychiatrists to learn? andHow will we evaluate if we are achieving our goals?”—Bruce R. Levy,M.D., President, American Association of Directors of Psychiatric ResidencyTraining; Director, Education and Training, Department of Psychiatry, LongIsland Jewish Medical Center; Associate Professor of Clinical Psychiatry, Al-bert Einstein College of Medicine, Bronx, New York
“As psychiatry program directors and residents struggle with defining, im-plementing, assessing and remediating core competencies in psychiatry,this book’s publication could not be more timely. The book is an out-standing compilation of the history of the evolution of the competencymovement (Part I); the delineation of core competencies from both theCanadian and the ACGME perspectives (Part II); detailed discussion of theACGME competencies, with chapters addressing each of the six compe-tencies as defined by the psychiatry and neurology quadrads (Part III);culminating in Part IV, which addresses how these competencies mayimpact psychiatric trainees and practicing psychiatrists in the future, par-ticularly related to the certification and maintenance of certification pro-cesses as well as medical education in general. The book’s organization issuch that it can easily be used both as a book to read front to back and asa reference book for specific questions that may come up in the day-to-day work on competencies. This book will undoubtedly be a highly valu-able asset for the psychiatric educator and the trainee as psychiatric train-ing—and, indeed, all of medical training—in the United States movestoward competency-based curricula and assessment. Recognizing thatthe competency movement is a work in progress, the authors have pro-vided a template from which educators can move toward the ‘ultimategoal.. .[of providing] real and realistic means for physicians to displaytheir skills, all of which are to be used for the benefit of the patients theyserve.’”—Sandra B. Sexson, M.D., Associate Professor, Psychiatry and Pedi-atrics, Emory University School of Medicine, Atlanta, Georgia, President-Elect, American Association of Directors of Psychiatric Residency Training