corporate presentation - · pdf file10.07.2016 · pathway to us market •...
TRANSCRIPT

Corporate Presentation
July 2016

Forward Looking Statements
This document does not constitute or form part of any offer or invitation to sell or issue, or any solicitation
of any offer to purchase or subscribe for, any shares in the Company, nor shall any part of it nor the fact of
its distribution form part of or be relied on in connection with any contract or investment decision relating
thereto, nor does it constitute a recommendation regarding the securities of the Company.
This document may contain forward-looking statements and estimates made by the Company, including
with respect to the anticipated future performance of TiGenix and the market in which it operates. They
include all matters that are not historical facts. Such statements, forecasts and estimates are based on
various assumptions and assessments of known and unknown risks, uncertainties and other factors,
which were deemed reasonable when made but may or may not prove to be correct. Actual events are
difficult to predict and may depend upon factors that are beyond the Company's control. Therefore, actual
results, the financial condition, performance or achievements of TiGenix, or industry results, may turn out
to be materially different from any future results, performance or achievements expressed or implied by
such statements, forecasts and estimates. Forward-looking statements, forecasts and estimates only
speak as of the date of this document and no representations are made as to the accuracy or fairness of
such forward-looking statements, forecasts and estimates. TiGenix disclaims any obligation to update any
such forward-looking statement, forecast or estimates to reflect any change in the Company’s
expectations with regard thereto, or any change in events, conditions or circumstances on which any such
statement, forecast or estimate is based.
2

Management Team With Proven Track Record of Success
Managing Director and CEO: Eduardo Bravo, MBA
• More than 25 years experience in the pharma and biotech industries at Sanofi-Aventis, Recordati,
Cephalon and SmithKline Beecham. With company since: July 2005
CFO: Claudia D’Augusta, PhD
• More than 15 years experience in equity and debt financing at Aquanima (Santander Group), Apax
Corporate Finance and Deloitte Corporate Finance. With company since: April 2004
CTO: Wilfried Dalemans, PhD
• More than 25 years experience in the pharma and biotech industries; previous engagements at GSK
Biologicals and Transgène. With company since: April 2007
CMO: Marie Paule Richard, MD
• More than 25 years experience in the global pharma and biotech industries at Bristol-Myers Squibb,
Sanofi Aventis, GSK, Sanofi Pasteur, Crucell and AiCuris. With company since: September 2014
VP Regulatory Affairs & Corporate Quality: María Pascual, PhD
• More than 10 years experience in cell therapy companies; specialized in regulatory affairs for
advanced therapies; external adviser to EMA. With company since: July 2003
VP Medical Affairs & New Product Commercialisation: Mary Carmen Diez, MD
• More than 20 years experience in the biopharmaceutical industry at Meda Pharma, Asta Médica,
Pfizer and Dupont Pharma. With company since: September 2014
3

Key Facts About TiGenix
Headquarters / Operations Leuven, Belgium / Madrid, Spain
Employees Approximately 75 employees
Stock Exchange Euronext Brussels. Ticker: TIG
Market Capitalization Approx. USD 190M June 27, 2016
Reference Shareholders ~20% held by Grifols and BNP Paribas
Liquidity ~80% free-float, of which ~30% held by institutional investors
Analyst Coverage 5 analysts covering the stock
Cash and Cash Equiv. USD 19.78M at December 31st, 2015
Last Capital Increase USD 26.1M raised from US and EU investors in March 2016
4
Note: Numbers reflect EUR/USD = 1.10 as of 06/27/16

Compelling Investment Case
Cx601: Global
Agreement Ex-US
with Takeda
• Complex perianal fistulas in Crohn’s disease patients in United States & EU is a multi-billion
dollar opportunity
• Pivotal Phase III (local administration of a single dose of allogeneic adipose derived stem cells)
• Primary endpoint met. Cx601 statistically superior to placebo in achieving combined remission
at week 24 (p=0.024)
• Long term efficacy sustained at week 52 on same endpoint (p=0.019)
• MAA submitted to EMA in 1Q16. Launch expected 2H17
• GMP process approved for commercial manufacturing by Spanish Agency in 1Q16.Takeda will
co-invest in the expansion of the Madrid facility to secure supply for the initial few years
• Up to €380M agreement with Takeda for the exclusive ex-US rights to Cx601 for the treatment of
complex perianal fistulas in Crohn’s disease patients
• Use of data from positive pivotal Phase III trial in EU to support a BLA in the US
• FDA’s agreement on SPA obtained for pivotal phase III trial in the US
• Same primary endpoint as positive EU Phase III trial
• US Phase III to start 1H17
• Fully-owned asset; granted patent valid until 2030
• Lonza selected as contract manufacturing organization for Cx601 in the US
Cx601: Clear
pathway to US
market
• AlloCSC-01: intra-coronary administered allogeneic cardiac stem cells, being developed for acute
myocardial infarction
• Randomized, double blind, placebo controlled Phase II trial ongoing
• Interim 6 months data confirmed safety. Final one-year follow up data expected 1H17
• Cx611: Intravenously-administered allogeneic adipose derived stem cell product for severe sepsis
• Phase I study completed
• Severe sepsis Phase I/ll trial design has been finalized; expected to enroll first patient in 2H16
Valuable Pipeline
Opportunities:
AlloCSC-01 and
Cx611
1 Advanced Therapy Medicinal Product 5

Multiple Product Candidates with Significant Upcoming Milestones
Product1 Indication Preclinical Phase I Phase II Phase III Market
Allogeneic Adipose-Derived Stem Cells
Cx601
(local)
Complex Perianal
Fistulas in Crohn’s
Disease
Cx611
(intravenous) Severe Sepsis
Allogeneic Cardiac Stem Cells
AlloCSC-01
(intracoronary) Acute Myocardial
Infarction
Characterized Autologous Chondrocytes
ChondroCelect Knee Cartilage Lesions
Ex-US rights licensed to Takeda
Withdrawal of MA requested at European Commission2
SPA agreed to by FDA
1 Covered by 29 patent families
2 Implementation of withdrawal of Marketing Authorization (pending EC confirmation) and termination of all CC related agreements anticipated by December 31, 2016
6
Launch EU 2H17
Pivotal US starts 1H17
Ph I/II starts 2H16
Final results 1H17

Cx601 Local injection of expanded Adipose-derived Stem Cells
(“eASCs) for the treatment of complex perianal fistulas in Crohn’s disease patients
7

Cx601 Inhibits Pro-inflammatory Cytokines Mechanism of Action (“MoA”) is IDO1-Mediated
8
1 IDO: Indoleamine 2,3-dioxygenase 2 PBMC: Peripheral Blood Mononuclear Cells
Source: De la Rosa et al. Tissue Engineering 2009
Inhibition of Immune Cell Proliferation
* p<0.05 relative to activated PBMCs without ASCs
Source: Tigenix data IDO Mediated
Inhibits pro-inflammation
Activated PBMC + Cx601
Inhibition of pro-inflammatory cytokines
* p<0.05 relative to supernatant from activated PBMCs
PBMCs
Activated PBMCs
PBMCs+Cx601
Actiivated PBMCs+Cx601
Cx601
0 5 10 15 20
IFN- (ng/ml)
0 1 2 3 4 5
TNF- (ng/ml)
* *
• Cx601 has the ability to balance an inflammatory
milieu, through the reduction of PBMC2 mediated
secretion of pro-inflammatory cytokines among
other immunological processes
Key Characteristics of Cx601
• IDO is key to the immunomodulatory properties of
Cx601, as shown here by its effect on PBMC
proliferation

9
GMP Facility in Madrid Approved for Commercial Manufacturing Takeda1 Will Endeavor to Take Over Manufacturing ex-US
1 Liposuction
2,400 Finished Products (Cx601)
Consistent and Robust Process
• Production facility in Madrid approved for
commercial manufacturing
• Current capacity is about 400 patient lots of
finished product per year
• TiGenix will initially supply Cx601 to Takeda
at cost for the EEA2 and Switzerland (CH)
• Takeda will co-fund the expansion of the
Madrid facility to secure supply for the initial
few years
• Takeda will endeavor to take over
manufacturing asap to leverage on a global
supply network
• Outside of the EEA and CH, Takeda is
responsible for manufacturing from July
2016
• Takeda will be fully responsible for
distribution and logistics in the whole
Territory
Manufacturing Capabilities
1 In July 2016 TiGenix and Takeda entered into an exclusive Ex-US Licensing Agreement for Cx601 2 EEA stands for European Economic Area, it includes all 28 states currently part of the European Economic
Area as well as the three states Iceland, Lichtenstein and Norway

A Common and Severe Complication of Crohn’s Disease Complex Perianal Fistulas Affect 1 in 12 Adult Crohn’s Disease Patients
• Complex fistulas are sores or
ulcers that tunnel through the
affected area into surrounding
tissues, and that:
• Affect anal sphincters
• Present multiple tracts
• Are recurrent
• Are often associated with
perianal abscess
• Complex fistulas cause
compromised Quality of Life
(QoL), pain, depression and risk
of anal epithelial carcinoma
120,000 adult patients in Europe and the US alone
10
Fistula
Fistula

Treatments Lack Long Term Efficacy and Present Safety Issues
11
• Optimal management remains challenging
• Little progress due to limited trials and poorly validated endpoints
• Clear gap for a clinically validated treatment with long term efficacy
1 L.J. Brandt et al. Metronidazole Therapy for Perineal Crohn’s Disease: a Follow-Up Study, 83 GASTROENTEROLOGY 383-7 (1982) 2 E.S. Goldstein et al., 6 - Mercaptopurine Is Effective in Crohn’s Disease Without Concomitant Steroids, 10 INFLAMM BOWEL DIS 79-84 (2004) 3 B.I. Korelitz et al., Favorable Effect of 6-Mercaptopurine on Fistulae of Crohn’s Disease, 30 DIGEST DIS SCI 58-64 (1985) 4 B.E. Sands et al., Infliximab Maintenance Therapy for Fistulizing Crohn’s Disease, 350 N ENGL J MED 876-85 (2004) 5 E. Domenech et al., Clinical Evolution of Luminal and Perianal Crohn’s Disease after Inducing Remission with Infliximab, 22 ALIMENT PHARMACOL THER 1107-13 (2005) 6 J.F. Colombel et al., Adalimumab for Maintenance of Clinical Response and Remission in Patients with Crohn’s Disease: The CHARM Trial, 132 GASTROENTEROLOGY
52-65 (2007) 7 C.B. Geltzeiler et al., Recent Developments in the Surgical Management of Perianal Fistula for Crohn’s Disease, 27 ANN GASTROENTEROL 1-11 (2014) 8 T. Sonoda et al., Outcomes of Primary Repair of Anorectal and Rectovaginal Fistulas Using the Endorectal Advancement Flap, 45 DIS COLON RECTUM 1622-28 (2002) 9 A. Soltani and A. Kaiser, Endorectal Advancement Flap for Crypto Glandular or Crohn’s Fistula-in-Ano, 53 DIS COLON RECTUM 486-495 (2010)
Treatment options
• High relapse on cessation1
• Safety concern with prolonged use
Benefit Shortfall
Antibiotics
Anti-TNFs Infliximab- Remicade®
Adalimumab - Humira®
Immunosuppressants
Surgery
• Improve symptoms and short term healing
• High relapse on cessation2,3
• Risk of infectious complications
• Moderate benefit reported
• Limited clinical trial data
• Low remission4,6 and high relapse4,5
• Safety concern with long term use and systemic immunosuppression
• Moderate benefit in clinical trials
• Conservative surgery risks recurrence
• Risk of complications (incontinence, non healing wounds, abscesses)8,9
• Eliminating risk of recurrence is possible with radical, mutilating surgery7,8

Product description
Four (4) vials of 6ml suspension, each with
30 million cells (total dose 120 million cells)
12
Cx601: A Completely Different Approach; A Single Dosage Suspension of Expanded Adipose-derived Stem Cells (“eASC)
Injection sites: Injection sites:
a. Fistula internal opening b. Fistula tract
Mode of Administration
• Fistula curettage and closure of internal
opening (sutured)
• Half of Cx601 dose (2 vials) injected into
tissue around internal opening (small blebs)
• Other 2 vials injected along the walls of the
fistula tracts (several small blebs)

Trial Summary
Study design
• Randomized, double-blind, placebo-controlled trial
• All tracts treated. Single procedure2
Number of
sites 47 active sites in 8 countries
Enrollment 289 patients recruited
Primary
endpoint
Combined Remission3 at week 24
with α<0.025 for all existing
fistulas
Secondary
endpoints at
Weeks 24
and 52
• Combined Remission at week 52 • Clinical Remission4 • Response5 • Time to Clinical Remission / to
Response • PDAI6 and other scores • Safety and tolerability
1 Adipose Derived Mesenchymal Stem Cells for Induction of Remission in Perianal Fistulising Crohn’s Disease 2 120 million cells 3 Closure of all treated external openings draining at baseline despite gentle finger compression, and absence of collections > 2cm by MRI (Magnetic Resonance Imaging) 4 Closure of all treated external openings draining at baseline despite gentle finger compression 5 Closure of at least 50% of all treated external openings draining at baseline despite gentle finger compression 6 Perianal Disease Activity Index 13
• Men and women aged 18 years or older
• Non active or mildly active luminal Crohn’s
disease (CDAI ≤ 220) diagnosed for ≥ 6
months
• Patients with complex perianal fistulas with
≤ 2 internal openings and ≤ 3 external
openings
• Fistula draining ≥ 6 weeks prior to inclusion
• Patients with inadequate response to at
least one of the following: antibiotics,
immunosuppressants or anti-TNFs
• Medical standard of care was allowed to
continue without modification of treatment
dose or regimen
Patients selected to ensure clear cut-off results
Phase III ADMIRE-CD1 Trial Double-Blind, Placebo-Controlled, Designed to Qualify as a Single Pivotal Study

Treatment
W24
Primary Endpoint
W52
Preparation Screening
D0
Follow-Up
W6 W12 W18 W36 W-3 W-5
Baseline
MRI
W52
MRI
W24
MRI
MRI: Magnetic Resonance Imaging
week
Randomization Clinical Assessment
Clinical and MRI Combined Primary Endpoint at Week 24 Long Term Follow-Up for Persistence (Week 52) and Safety (up to Week 104)
14
W104

15
1 ITT: Intention To Treat i.e. patients randomized 2 Safety Set: patients randomized and treated 3 Surgical procedures for other reasons than fistulas; Fistulas not healing/worsening of fistula symptoms; No tract found or additional blind tract found by the surgeon
during preparation visit; Impossibility to administer 12 ml into the tract or to identify the primary opening; Fistula closed, etc
Cx601 Phase III Patient Populations Largest Ever Study in Complex Perianal Fistulas
• 1 Reoccurrence of
Crohn’s Disease
• 1 Deep Vein
Thrombosis
• 1 Informed Consent
Withdrawn
• 1 Missing Data
Screened n=289
Screening Failures
n=77
Randomized n=212
Cx601 n=107
Placebo n=105
Not Treated
n=4
Treated n=103
Treated n=102
Not treated
n=3
ITT 1 set n=212
Safety Set 2 n=205
• 1 Informed Consent
Withdrawn
• 1 No Longer Met
Inclusion Criteria
• 1 Did Not Have Post-
baseline Efficiency
Evaluation
• 43 Wrong Inclusion /
Exclusion criteria
• 20 Other3
• 12 Informed Consent
Withdrawn
• 2 (Serious) Adverse
Events

Demographics (ITT) Cx601
n= 107
Placebo
n= 105
Age (years) mean (SD) 39.0 (13.1) 37.6 (13.1)
Men (%) 60 (56.1) 56 (53.3)
Caucasian (%) 100 (93.5) 96 (91.4)
Weight (kg) mean (SD) 73.9 (15.0) 71.3 (14.9)
PDAI (ITT)
Mean (SD) 68 (2.5) 6.6 (2.9)
Topography of Internal &
External Openings (%) (ITT) 2
One-tract fistula 51.4 67.7
Multiple-tract fistula* 44.8 29.6
Good Balance Among Groups Except for Topography of Fistulas Cx601 Group Contained More Difficult to Treat Patients
• Similar demographics and PDAI1 score between arms
• Higher proportion of multiple-tract fistulas in Cx601 group
16
* Primary endpoint measured combined remission on all tracts 1 Perianal Disease Activity Index 2 Fistula topography not available in seven (7) patients

75.0%
55.9%
0
20
40
60
80
Cx601 Placebo
Primary endpoint met at week 24 Benefit Sustained at Week 52
1 ITT: Intention To Treat i.e. patients randomized. Efficacy results are consistent across all statistical populations 17
54.2%
37.1%
0
20
40
60
Sustained Remission at W52
49.5%
34.3%
0
20
40
60
% Combined Remission at W24
(ITT1 Population n= 212)
p = 0.024
• 75.0% of Cx601 treated patients who achieved combined
remission at week 24 remained in combined remission at
week 52 compared to only 55.9% in the placebo arm
• Primary endpoint met: Combined remission at W24 was
44.3% higher in treated patients versus placebo (p=0.024)
• Benefit maintained at W52: Combined remission was 46%
higher in treated group versus placebo (p=0.012)
p = 0.012
Combined Remission at W52
(ITT1 Population n= 212)

Faster Time to Remission Cx601 Achieves Remission Twice as Fast as Placebo
1 ITT: Intention To Treat i.e. patients randomized
• Cx601-treated patients achieved Clinical Remission after 6.7 weeks 50% sooner that
placebo-treated patients
• The placebo-treated patients achieved Clinical Remission after 14.6 weeks (HR 1.75, 95%
CI (1.27-2.44))
18
ITT Population1 n=212

Safety Profile Maintained Over the Long Term Product is Free From Serious Side Effects of Biologic Treatments
19
Number of Patients with (%) Cx601
n= 103
Placebo
n=102
W24 W52 W24 W52
*TEAEs 68 (66.0) 79 (76.7) 66 (64.7) 74 (72.5)
Related TEAEs 18 (17.5) 21 (20.4) 301 (29.4) 271 (26.5)
Withdrawn due to a TEAEs 5 (4.9) 9 (8.7) 6 (5.9) 9 (8.8)
**TESAEs 18 (17.5) 25 (24.3) 14 (13.7) 21 (20.6)
Related TESAEs 5 (4.9) 7 (6.8) 7 (6.9) 7 (6.9)
Withdrawn due to TESAEs 4 (3.9) 6 (5.8) 4 (3.9) 7 (6.9)
Note: If a patient has multiple events of the same severity, relationship or outcome, then they are counted only once in that severity, relationship or outcome. However, patients can be counted more than once overall.
Overview of TEAEs up to Week 24 & Week 52 (Safety population n= 205)
*Most common TEAEs: Anal Abscess; Proctalgia; Nasopharyngitis; Diarrhoea; Abdominal pain; Pyrexia
**TE(S)AE: Treatment-Emergent (Serious) Adverse Events 1 Figures are cumulative; however prior AEs reevaluated at W52 as non-related are not adjusted retroactively.

Oral presentation in Plenary Session by
Dr. Panés (March 17, 2016)
Satellite Symposium chaired by
Dr. Van Assche (March 18, 2016)
Cx601: Communication of ADMIRE-CD Results ECCO1 2016 (Amsterdam, 16-19th March 2016)
20 1European Crohn’s and Colitis Organization

Cx601: Communication of ADMIRE-CD Results ECCO 2016 (Amsterdam, 16-19th March 2016)
21

Cx601’s Approach to the US Market Leveraging EU Data With Approved Phase III Protocol
Preparing for US BLA1 Filing with clear pathway to US Market
Solid regulatory and clinical development strategy
• Type B meeting with FDA2 confirmed:
• Adequacy of existing non-clinical package to support an IND3 filing
• Acceptability of using data from the ADMIRE-CD trial to support BLA
• SPA4 for US Phase III protocol agreed with FDA:
• Primary end-point identical to ADMIRE-CD trial
• p-value < 0.05 (vs. p-value <0.025 in ADMIRE-CD trial)
US Phase III trial scheduled to start by 1H17
Lonza selected as contract manufacturing organization for Cx601 in the US,
technology transfer ongoing
1 BLA: Biological License Application 2 FDA: Food and Drug Administration 3 IND: Investigational New Drug 4 SPA: Special Protocol Assessment
22

25% 75%15,18
Simple fistulas
# of cases = 39,404 Complex fistulas
# of cases = 118,211
Perianal fistulas = 157,615
Crohn’s Disease Patients *1-9 = 1.540.710
11% 10-17
93% 7,8
Adult Crohn’s Disease Patients = 1,432,860
Non-Perianal fistulas = 109,529 (41% of fistulas are not perianal 13,14)
Cx601: Estimated Potential Patient Population (EU & US) An Attractive Commercial Opportunity
66%19
Non-Controlled luminal CD
# of cases = 40,192
Refractory fistulas
# of cases = 70,217
90%19, 20
34%
10%
Non-refractory fistulas
# of cases = 7,802 (Further details on references provided in Appendix )
1 Stone MA et al. 2013 2 Hein R et al. 2014 3 Lucendo AJ et al. 2014 4 Dal Pont E et al. 2010 5 Cottone M et al. 2006 6 Herrinton LJ et al. 2007 7 Kappelman MD et al. 2007
8 Kappelman MD et al. 2013 9 Molodecky NA et al. 2012 10 SEESGCD.19
11 Gibson PR et al. 2007 12 Dranga M et al. 2015 13 Schwartz DA et al. 2002 14 Bell SJ et al. 2003
23
• A total of 267,144 CD patients experience fistulas
• 34-61% of CD patients with fistulas experience ≥ 2
fistulizing episodes13,14 or 90,829 - 162,958 patients
• 33% of CD patients with perianal fistulas experience
≥ 2 fistulizing episodes13 or 52,013 patients
Controlled luminal CD
# of cases = 78,019
* Estimated prevalence in US: 190/100,000
(average from US nationwide studies comprising study periods post year 2000) 6-9
Estimated average prevalence in EU: 180/100,000
(no nationwide studies available; average of regional studies conducted in EU5
comprising study periods post year 2000, weighed by country populations) 1-5, 9
15 Eglinton TW et al. 2012 16 Gray BK et al. 1965 17 Galandiuk S et al. 2005 18 Molendijk I et al. 2014 19 Sands BE et al. 2004 20 Domènech E et al. 2005

Prevalence per 10,000 patients vs. prices for selected drugs
Cx601: Pricing Considerations Lower Prevalence Would Suggest Higher Price
24
€0
€50
€100
€150
€200
€250
€300
€350
€400
€450
€500
0 1 2 3 4 5 6 7 8 9 10
1 Ex-manufacturer prices per patient per year, including mandatory published discounts, obtained from CMS, L’Assurance Maladie, G-BA, Gazzetta
Ufficiale, Spanish MoH, British National Formulary. $1 = €0.90. Indications for select products: Kalydeco, G551D-mutation cystic fibrosis; Kuvan,
Phenylketonuria; Adempas, Chronic thromboembolic pulmonary hypertension; Revolade, Low blood platelet count in adults with chronic immune
thrombocytopenic purpura; Esbriet, idiopathic pulmonary fibrosis. Full list of references provided at back.
Ka
lyd
eco
Kuvan
Re
vo
lad
e
Ad
em
pas
Esb
rie
t
Ex
-ma
nu
fac
ture
pri
ce
per
ye
ar
(00
0)
1
Non-orphan drugs Orphan drugs
Solir
is
Za
ve
sca
Xyre
m
Tysabri
Sa
msca

Takeda exclusive Ex-US Licensing Agreement for Cx601

26
1 BioCentury, 30th May 2016
• Global pharmaceutical company, with a focus on GI, Oncology and CNS
• Market presence in over 70 countries and regions; with more than 30,000 employees
• Total sales in FY 2015 (as of March 2016) amounted to €15Bn.
• Major regions by sales are Japan (38%), the US (29%) and Europe (17%)
• In 2015, Takeda formed a GI drug discovery unit. The aim of this unit is to further develop
internal GI projects as well as execute deals which will complement Takeda’s GI franchise
• FY 2015 sales for Takeda’s GI franchise amounted to €720M. Takeda recently disclosed that
Entyvio is the company's No. 4 selling drug targeting sales >$2Bn by 2018
• Takeda is already among the top 10 companies by sales in GI space1
Takeda Pharmaceutical The Partner of Choice in the GI Space
Cx601 is the perfect fit with Takeda’s GI focus, with
clear synergies with Entyvio

27
Licensing Agreement with Takeda Summary of Key Terms
• Takeda acquires the exclusive ex-US rights to Cx601 for the treatment of complex
perianal fistulas in Crohn’s disease patients
• TiGenix retains 100% rights to the US market, estimated at 50% of Cx601 global
market and the rights to develop Cx601 in new GI indications
• Upfront payment of € 25 million and € 10 million of equity investment
• Regulatory and sales milestones payment for up to a potential total of € 355 million, of
which € 15 million at marketing approval of Cx601 in Europe expected in 2H17
• Following Marketing Authorization in the European Union, Takeda will become the
marketing authorization holder (MAH) and will be responsible for all commercialization
and regulatory activities
• Takeda will also be responsible for additional development activities of Cx601 for the
indication of complex perianal fistulas in Crohn’s disease and will eventually take over
manufacturing for Cx601 within the licensed territory
A deal for a potential total of € 380 million (excluding US)
the best partner to secure Cx601 commercial success

28
Cell Therapy Product Deals to Date The Largest “Product” Licensing Deal in Cell Therapy
Deal Indication/ Phase Territory Upfront Total deal Comments
TiGenix licenses Ex-US
rights of Cx601 to
Takeda (2016)
Complex Perianal
Fistulas in Crohn’s
disease patients; MAA
submitted to EMA
Worldwide
Ex-US
€25M
€10M in
equity
Up to
€380M
TiGenix maintains 100% rights
to US market, (≈50% market)
and full rights to develop Cx601
in other indications
Mesoblasts acquires
MSC business from
Osiris (2013)
Prochymal: Acute
GvHD in children
(approved in
Canada and NZ)
Worldwide $20M $100M > 50% potentially payable in
stock
Janssen options rights
to CAP-1002 from
Capricor (2014)
Large myocardial
infarction (in Ph. II)
Worldwide $12.5M Up to
$337.5M
Exclusive right to license CAP-
1002 at any time until 60 days
post 6-month follow-up data
from Phase II
Chugai licenses
Multistem from
Athersys (2015)
Ischemic stroke (in
Ph. II)
Japan $10M Up to
$205M
United Therapeutics
licenses PLX-PAD
from Pluristem (2011)
Pulmonary
hypertension
(in Ph. I)
Worldwide $7M $55M Agreement ended by UT
December 2015

29
• Cx601 addresses a severe and common unmet need in Crohn’s Disease
• Current treatment options lack long term efficacy and present safety concerns
• European Phase III clinical trial results show clear superiority in efficacy vs. standard of
care with just one single treatment
• Clinical effect is significantly quicker and efficacy persists at 52 weeks
• Product has good safety profile and is easy to administer
• Approval and launch in Europe expected 2H17
• US Pivotal Phase III trial agreed with FDA (SPA) to start 1H17
Cx601 a Major Breakthrough Clear Plan to Secure Even Further Upside

AlloCSC-01: Phase ll Data To Be Announced 1H 17
Intracoronary administration of allogeneic cardiac stem cells for the
treatment of acute ischaemic heart disease
30

AlloCSC-01: Preventing Chronic Heart Failure Myocardial Repair May Be The Only Feasible Alternative
• 1.9M Acute Myocardial Infarctions (US+EU)1 occur annually, mostly treated by PCI2 and stent
implantation
• Successful treatment of Acute Myocardial Infarctions (“AMI”) has increased short term survival
but contributed to a Chronic Heart Failure (CHF) epidemic (26M patients worldwide3)
• CHF post-AMI is a terminal disease with an annual mortality rate of ~5% after the first
episode, for which no curative treatment exists with the exception of heart transplantation
31
1 Datamonitor: Stakeholder Insight: Acute coronary syndromes, DMHC2347, 2007 2 PCI: Percutaneous Coronary Intervention 3 Ambrosy PA et al., J Am Coll Cardiol. 2014;63:1123-1133.
Myocardial repair is the only
feasible treatment to
address the post-acute
phase of the disease and
prevent the onset of CHF
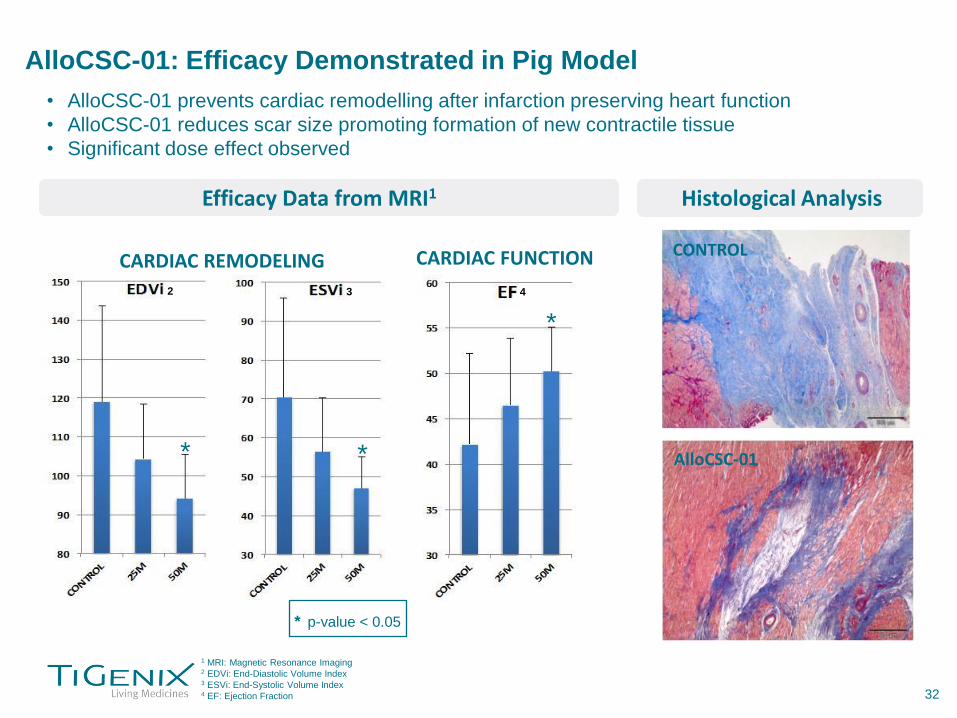
AlloCSC-01: Efficacy Demonstrated in Pig Model
1 MRI: Magnetic Resonance Imaging 2 EDVi: End-Diastolic Volume Index 3 ESVi: End-Systolic Volume Index 4 EF: Ejection Fraction
• AlloCSC-01 prevents cardiac remodelling after infarction preserving heart function
• AlloCSC-01 reduces scar size promoting formation of new contractile tissue
• Significant dose effect observed
32
CARDIAC REMODELING CARDIAC FUNCTION
Efficacy Data from MRI1 Histological Analysis
CONTROL
AlloCSC-01 * *
*
* p-value < 0.05
2 3 4

CAREMI Phase I/II Trial Final Results Expected 1H17 Safety and Efficacy of Intracoronary Infusion of Allogeneic Cardiac Stem Cells in
Patients with Acute Myocardial Infarction (“AMI”)
TRIAL SUMMARY
Condition Acute Myocardial Infarction
Study design
AlloCSC-01 administered 5-7 days after PCI4
• Phase 1. Open label dose escalation in 6 patients
• Phase 2: Placebo controlled, 49 patients randomized 2:1 (35M cell dose in active arm)
Recruitment
• Phase 1: Completed
• Phase 2: Completed recruitment in 4Q15
# of centers 8 sites
Primary endpoint Mortality and MACE5 from any cause at
30 days
Secondary
endpoints (6 and
12 months)
Safety: Mortality and MACE
Efficacy: evolution of infarct size, biomechanical parameters by MRI
Clinical parameters: 6m walk test, NYHA6 scale
Completion 1H17 (Interim data announced June 16)
PATIENT SELECTION
Initial clinical pre-screening:
• Males, females ≥18 years and ≤80 years
• Patients who present a STEMI1
• Killip ≤ 2 on admission
• Successful revascularization by PCI (TIMI2 = 3)
within 12h after the onset of symptoms
• EF≤50% by echocardiography (day 2 after infarct
symptoms)
• EF≤45% by MRI on D3-5 post-STEMI
• Infarct size (1st MRI) >25% in LV3
• Bare-metal stents or second generation drug
eluting stent at PCI
• The infarct culprit coronary artery is adequate for
treatment administration and the procedure is
technically feasible
• The patient is stable and in adequate clinical
condition to undergo the procedure
1 STEMI: ST-Segment-Elevation Myocardial Infarction 2 TIMI: Thrombolysis In Myocardial Infarction 3 LV: Left Ventricle 4 PCI: Percutaneous Coronary Intervention 5 MACE: Major Adverse Cardiac Events 6 NYHA: New York Heart Association 33

• In the dose-escalation open-label phase, 6 patients were treated and 5 of them were followed up for 6 months
• Patients received a single injection of 11 million (M), 22M or 35M cells of AlloCSC-01 (n=2 each) by intracoronary infusion 5 to 7 days after Percutaneous Coronary Intervention (PCI)
• Data presented at the European Society of Cardiology meeting in London, showed that AlloCSC-01 has a good safety profile as no adverse events or Major Adverse Cardiac Events (MACE) were observed during the 6 month follow-up period
• Preliminary data from this treated group showed a reduction in infarct size, and a LVEF improvement on MRI, over the 6-month follow-up period (n=54; p<0.05 for both parameters)
* p-value < 0.1
** p-value < 0.05
34
CAREMI Phase I/II Trial Positive Preliminary Results from Phase I Presented at ESC
1 3 2
1 LVEF (%): Left Ventricular Ejection Fraction % change versus screening MRI 2 IS (mL): Infarct Size 3 IS (% of LV): Infarct Size as % of Left Ventricular mass 4 The patient lost to follow-up received the 11 million dose
• 51 patients were evaluated: 34 patients received AlloCSC-01 (35 M cells) and 17 patients received placebo
• Primary endpoint met: No mortality of any cause within one month was recorded for both placebo and AlloCSC-01 groups
• No major adverse cardiac event (MACE) was recorded within one month in either group
• Importantly for the long term safety evaluation, no mortality of any cause nor MACE was recorded in either group at six months
• Preliminary secondary efficacy data at six months was limited to infarct size evolution, defined as a percent of the left ventricular mass measured by magnetic resonance imaging. The mean absolute change in infarct size from baseline to six months was similar in both groups
• The final full set of safety and efficacy study results at twelve months will be reported in first half of 2017
35
CAREMI Phase I/II Trial Interim Results at 6 Months Confirm Safety Profile of AlloCSC-01

Cx611: Phase lI Ready
Intravenous injection of eASCs for the treatment of severe sepsis
36
1 The Lancet Infectious Diseases; Volume 12; issue 2; page 89; February 2012 2 Martin GS Expert Rev Anti Infect Ther. 2012 June ; 10(6): 701–706. 3 Torio et al. National inpatient hospital costs: the most expensive conditions by payer. AHRQ, Healthcare Cost Brief No. 160 August 2013. 4 Adapted from Lagu, T., et al. Critical Care Medicine, 40(3):754-761; 2012 5 Adapted from: Elixhauser et al. Septicemia in U.S. Hospitals 2009, AHRQ, Healthcare Cost Brief No. 122 October 2011
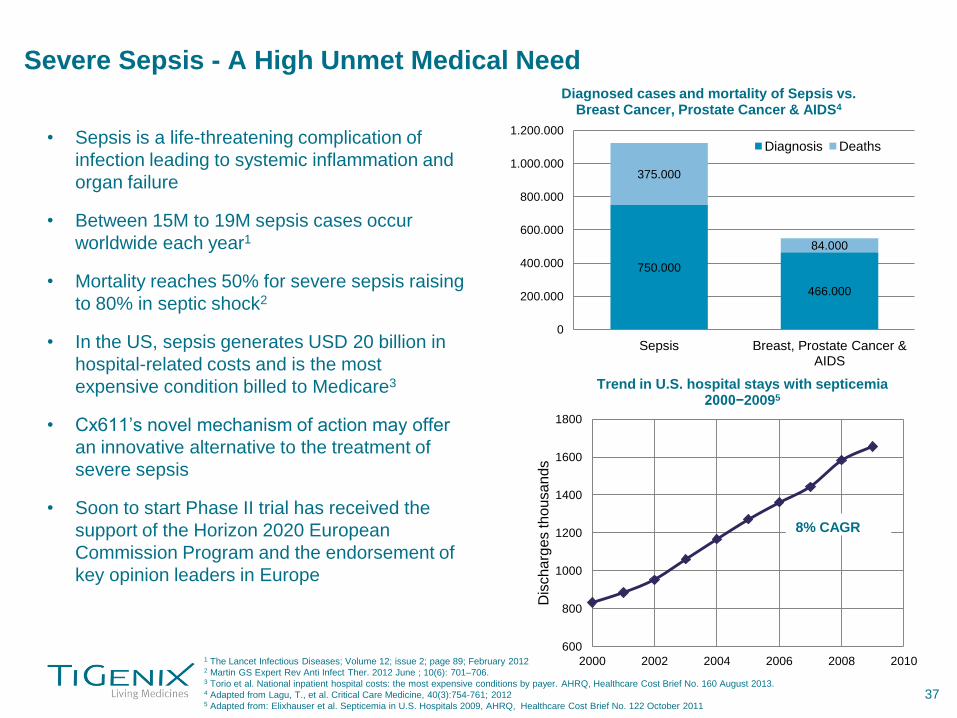
Severe Sepsis - A High Unmet Medical Need
• Sepsis is a life-threatening complication of
infection leading to systemic inflammation and
organ failure
• Between 15M to 19M sepsis cases occur
worldwide each year1
• Mortality reaches 50% for severe sepsis raising
to 80% in septic shock2
• In the US, sepsis generates USD 20 billion in
hospital-related costs and is the most
expensive condition billed to Medicare3
• Cx611’s novel mechanism of action may offer
an innovative alternative to the treatment of
severe sepsis
• Soon to start Phase II trial has received the
support of the Horizon 2020 European
Commission Program and the endorsement of
key opinion leaders in Europe
37
600
800
1000
1200
1400
1600
1800
2000 2002 2004 2006 2008 2010
Dis
ch
arg
es th
ou
san
ds
Trend in U.S. hospital stays with septicemia 2000−20095
8% CAGR
750.000
466.000
375.000
84.000
0
200.000
400.000
600.000
800.000
1.000.000
1.200.000
Sepsis Breast, Prostate Cancer & AIDS
Diagnosed cases and mortality of Sepsis vs. Breast Cancer, Prostate Cancer & AIDS4
Diagnosis Deaths

Cx611 Reduces Mortality in Animal Models of Sepsis
• This effect is due to a combination of reducing pro-inflammatory and increasing anti-
inflammatory mediators, production of anti-microbial effectors, and increased
phagocytosis
Source: Gonzalez-Rey, 2009 * p < 0.001
LPS1 Model CLP2 Model
38
1 LPS: lipopolysaccharide. LPS model is based on endotoxemia induced by high-dose of endotoxin 2 CLP: cecal ligation and puncture. This model mimics the clinical situation of patients with colonic leakage following surgical procedures or diffused peritonitis

CL
P m
od
el • ↓ of pro-inflammatory mediators
• of anti-inflammatory mediator
• ↓ of inflammatory cells
LP
S m
od
el
* p<0.001
Source: Gonzalez-Rey et al. Gut. 2009 Jul;58(7):929-39
Cx611 Has an Effect at Cytokine and Cellular Level
39

Cx611: Phase I/II in Severe Sepsis Expected to Start 2H16
CELLULA Phase I trial results
• 250k, 1M, 4M eASC/kg and placebo administered to 32 healthy volunteers (8 per group)
• Favorable safety and tolerability profile of Cx611, consistent with Phase I/IIa in refractory RA1
patients
SEPCELL Phase I/II study in severe sepsis to start 2H16
• Randomized, double blind, parallel groups, placebo controlled, multicenter study
• 180 patients (90 per group) with sCABP2 requiring mechanical ventilation and/or vasopressors,
admitted to the ICU. At least 50 centers in at least 4 countries
• 160M eASC or placebo on days 1 and 3 (320M in total) in addition to standard of care therapy.
90 days follow up
• Primary endpoint: Adverse event and potential immunological host responses against the
administered cells
• Secondary endpoint: Reduction in the duration of mechanical ventilation and/or vasopressors
needed and/or improved survival, and/or clinical cure of the CAPB, and other infection-related
endpoints
• Partially funded with EUR 5.4 million from the European Commission through its Horizon 2020
Program
40
1 Rheumatoid Arthritis 2 Severe community-acquired bacterial pneumonia

41
IP, Key Milestones and
Compelling Investment Case

Key Intellectual Property Patent Portfolio in Cell Therapy
• 29 patent families related to cell therapy products
• Pending & granted patents in over 20 jurisdictions including the US; expiry dates
2024 onwards for the products in development
• Patent covering eASC population and therapeutic uses granted in EU recently
• Key patent for Cx601 (PCX007) granted in US, AU, RU, MX, IL and NZ
• Patent protects use of ASCs in treatment of fistula
• Complementary protection possible through additional patents under review
• Portfolio covers key features of TiGenix’s stem cell and chondrocyte platforms
• Expanded cell compositions and preparations
• Use of expanded cells in treatment of broad range of indications
• Cell preparation methods & delivery systems
• FTO for indications in clinical development reviewed by external counsel
• US: Morrison & Foerster
• Europe: Carpmaels & Ransford
42

Product 2014 2015 2016 2017
Cx601
(local)
Europe
US
AlloCSC-01 (intracoronary)
acute
myocardial
infarction
Cx611
(IV)
severe
sepsis
ChondroCelect
Key Milestones
3Q15 Phase 3 primary endpoint met (24 weeks)
1Q16 study results (1 year follow-up)
1Q16 EMA filing
3Q14 CMO selection
2H16 tech transfer finalized
4Q14 SPA submission
4Q14 Phase 3 enrollment completed
1H17 start US Phase 3
Takeda Deal
3Q15 positive SPA
1Q14 manufacturing facility sold
2Q14 licensed to SOBI
2H16 Phase 2 interim analysis
1H17 Phase 2 study results
1Q15 Phase 2 enrollment initiated
4Q15 Phase 2 enrollment completed
1Q17 IND filing
4Q14 Phase 1 initiated
2Q15 Phase 1 study results
2H16 Phase 2 enrollment initiated
43
2H17 EMA approval
2H17 launch
Termination of agreement with SOBI
Withdrawal of MAA requested

Compelling Investment Case
Cx601: Global
Agreement Ex-US
with Takeda
• Complex perianal fistulas in Crohn’s disease patients in United States & EU is a multi-billion
dollar opportunity
• Pivotal Phase III (local administration of a single dose of allogeneic adipose derived stem cells)
• Primary endpoint met. Cx601 statistically superior to placebo in achieving combined remission
at week 24 (p=0.024)
• Long term efficacy sustained at week 52 on same endpoint (p=0.019)
• MAA submitted to EMA in 1Q16. Launch expected 2H17
• GMP process approved for commercial manufacturing by Spanish Agency in 1Q16.Takeda will
co-invest in the expantion of the Madrid facility to secure supply for the initial few years
• Up to €380M agreement with Takeda for the exclusive ex-US rights to Cx601 for the treatment of
complex perianal fistulas in Crohn’s disease patients
• Use of data from positive pivotal Phase III trial in EU to support a BLA in the US
• FDA’s agreement on SPA obtained for pivotal phase III trial in the US
• Same primary endpoint as positive EU Phase III trial
• US Phase III to start 1H17
• Fully-owned asset; granted patent valid until 2030
• Lonza selected as contract manufacturing organization for Cx601 in the US
Cx601: Clear
pathway to US
market
• AlloCSC-01: intra-coronary administered allogeneic cardiac stem cells, being developed for acute
myocardial infarction
• Randomized, double blind, placebo controlled Phase II trial ongoing
• Interim 6 months data confirmed safety. Final one-year follow up data expected 1H17
• Cx611: Intravenously-administered allogeneic adipose derived stem cell product for severe sepsis
• Phase I study completed
• Severe sepsis Phase I/ll trial design has been finalized; expected to enroll first patient in 2H16
Valuable Pipeline
Opportunities:
AlloCSC-01 and
Cx611
1 Advanced Therapy Medicinal Product 44

45
References

46
References
1. Stone MA et al. Prevalence and management of inflammatory bowel disease: A cross-sectional study from central England. European Journal of Gastroenterology
& Hepatology 2013; 15:1275-1280.
2. Hein R et al. Prevalence of inflammatory bowel disease: estimates for 2010 and trends in Germany from a large insurance-based regional cohort. Scandinavian
Journal of Gastroenterology 2014; 49:1325-1335.
3. Lucendo AJ et al. Epidemiology and temporal trends (2000-2012) of inflammatory bowel disease in adult patients in a central region of Spain. European Journal of
Gastroenterology & Hepatology 2014; 26:1399-1407.
4. Dal Pont E et al. Inflammatory bowel diseases (IBD) incidence and prevalence in a North East limited area of Italy. Digestive Liver Disease 2010; S180.
5. Cottone M et al. Incidence of Crohn’s disease and CARD 15 mutation in a small town in Sicily. European Journal of Epidemiology 2006; 21:887-892.
6. Herrinton LJ et al. Estimation of the period prevalence of inflammatory bowel disease among nine health plans using computerized diagnoses and outpatients
pharmacy dispensings. Inflammatory Bowel Disease 2007; 13:451-661.
7. Kappelman MD et al. The prevalence and geographic distribution of Crohn’s disease and ulcerative colitis in the United States. Clinical Gastroenterology &
Hepatology 2007; 5:1424-1429.
8. Kappelman MD et al. Recent trends in the prevalence of Crohn’s disease and ulcerative colitis in a commercially insured US population. Digestive Diseases &
Sciences 2013; 58:519-525.
9. Molodecky NA et al. Increasing incidence and prevalence of inflammatory bowel diseases with time, based on systematic review. Gastroenterology 2012; 142:46-
54.
10. Spanish Epidemiological and Economic Study Group on Crohn’s disease. Epidemiological and clinical features of Spanish patients with Crohn’s disease. European
Journal of Gastroenterology & Hepatology 1999; 11:1121-1127.
11. Gibson PR et al. Relationship between disease severity, quality of life and health care resource use in a cross-section of Australian patients with Crohn’s disease.
Journal of Gastroenterology & Hepatology 2007; 22:1306-1312.
12. Dranga M et al. Are there any particularities in Crohn’s disease in North-Eastern Romania? Revista Medico-Chirurgicala a Societatii de Medici si Naturalisti din Iasi
2015; 119:334-339.
13. Schwartz DA et al. The natural history of fistulizing Crohn’s disease in Olmsted county, Minnesota. Gastroenterology 2002; 122:875-880.
14. Bell SJ et al. The clinical course of fistulating Crohn’s disease. Alimentary Pharmacology & Therapeutics 2003; 17:1145-1151.
15. Eglinton TW et al. The spectrum of perianal Crohn’s disease in a population-based cohort. Diseases of the Colon & Rectum 2012; 55: 773-777.
16. Gray BK et al. Crohn’s disease of the anal region. Gut 1965; 6:515-524.
17. Galandiuk S. Perianal Crohn’s disease. Predictors of need for permanent diversion. Annals of Surgery 2005; 241:796-802.
18. Molendijk I et al. Disappointing durable remission rates in complex Crohn’s disease fistula. Inflammatory Bowel Disease 2014; 20:2022-2028.
19. Sands BE et al. Infliximab maintenance therapy for fistulizing Crohn’s disease. The New England Journal of Medicine 2004; 350:876-85.
20. Domènech E et al. Clinical evolution of luminal and perianal Crohn’s disease after inducing remission with infliximab: how long should patients be treated?
Alimentary Pharmacology & Therapeutics 2005; 22:1107-1113.
21. Gammie T et al. Comprehensive Review of Legislations, Regulations and Policies in 35 Countries. PLoS One. 2015;10(10):e0140002, 2015.

Corporate Presentation
July 2016
47