cortical capillary angiopathy in the stroke-like episodes ...10.1007... · web viewan eeg on day...
TRANSCRIPT

MS ID#: JOON-D-17-01709 Page
Supplementary Data
These data provide supplementary Tables 1 and 2, Figure 1, and additional clinical information of 11 patients
shown in Tables 1 and 2.
Online Resource 1. Supplementary Table 1
Online Resource 2. Supplementary Table 2
Online Resource 3. Supplementary Figure 1
Online Resource 4. Case Description: Patients 1-6 who were antibody-negative but fulfilled the probable
criteria
Online Resource 5. Case Description: Patients 7-11 who were antibody-positive but not fulfilled the probable
criteria
Abbreviations: ADEM: acute disseminated encephalomyelitis; AEDs: anti-epileptic drugs; AQP4: aquaporin-4;
CBA: cell-based assay; CSF; cerebrospinal fluid; DWI: diffuse-weighted imaging; EEG: electroencephalogram;
EMG: electromyogram examination; FLAIR: fluid-attenuated inversion recovery; GAD: glutamic acid
decarboxylase; HSV: herpes simplex virus; IHC: immunohistochemistry; IVIg: intravenous high-dose
immunoglobulin; IVMP: intravenous high-dose methylprednisolone; MBP: myelin basic protein; MOG: myelin
oligodendrocyte glycoprotein; mono: mononuclear cells; MPO-ANCA: myeloperoxidase antineutrophil
cytoplasmic antibodies; mRS: modified Rankin Scale; NMDAR: NMDA receptor; NMOSD: neuromyelitis
optica spectrum disorder; NSA: neuronal cell surface antigens and synaptic proteins; OCBs: oligoclonal bands;
PD: paroxysmal discharge; PMH: past medical history; probable criteria: diagnostic criteria for probable anti-
NMDAR encephalitis; sIL-2R: soluble IL-2 receptor; Tg: thyroglobulin; TPO: peroxidase; WBCs: white blood
cells.
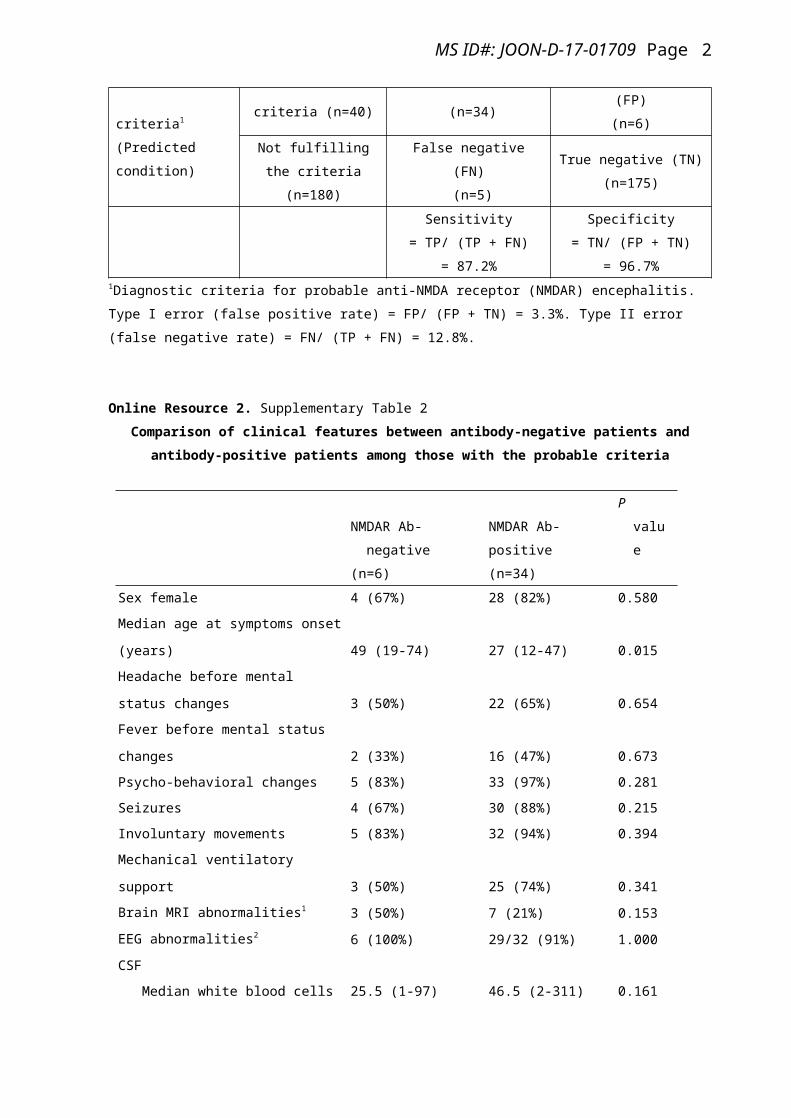
Online Resource 1. Supplementary Table 1: Table for sensitivity, specificity, type I and type II error.
Patients with clinically-suspected autoimmune
neurological disorders (n=220)
Patients with anti-NMDAR encephalitis
confirmed by antibody testing (True condition)
NMDAR-antibody
positive (n=39)
NMDAR-antibody
negative (n=181)
Probable criteria1
(Predicted condition)
Fulfilling the criteria
(n=40)
True positive (TP)
(n=34)
False positive (FP)
(n=6)
Not fulfilling the criteria
(n=180)
False negative (FN)
(n=5)
True negative (TN)
(n=175)
Sensitivity
= TP/ (TP + FN)
= 87.2%
Specificity
= TN/ (FP + TN)
= 96.7%
1
MS ID#: JOON-D-17-01709 Page
1Diagnostic criteria for probable anti-NMDA receptor (NMDAR) encephalitis. Type I error (false positive rate) =
FP/ (FP + TN) = 3.3%. Type II error (false negative rate) = FN/ (TP + FN) = 12.8%.
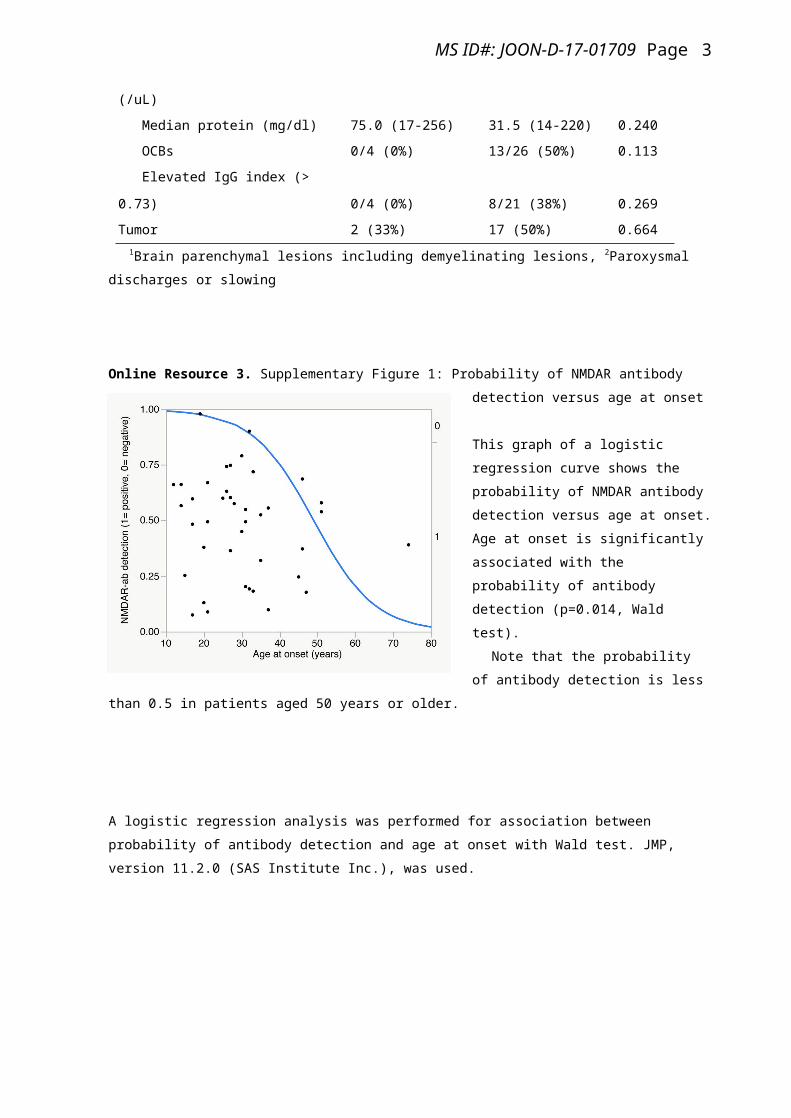
Online Resource 2. Supplementary Table 2
Comparison of clinical features between antibody-negative patients and antibody-positive patients among
those with the probable criteria
NMDAR Ab-negative
(n=6)
NMDAR Ab-positive
(n=34)
P value
Sex female 4 (67%) 28 (82%) 0.580
Median age at symptoms onset (years) 49 (19-74) 27 (12-47) 0.015
Headache before mental status changes 3 (50%) 22 (65%) 0.654
Fever before mental status changes 2 (33%) 16 (47%) 0.673
Psycho-behavioral changes 5 (83%) 33 (97%) 0.281
Seizures 4 (67%) 30 (88%) 0.215
Involuntary movements 5 (83%) 32 (94%) 0.394
Mechanical ventilatory support 3 (50%) 25 (74%) 0.341
Brain MRI abnormalities1 3 (50%) 7 (21%) 0.153
EEG abnormalities2 6 (100%) 29/32 (91%) 1.000
CSF
Median white blood cells (/uL) 25.5 (1-97) 46.5 (2-311) 0.161
Median protein (mg/dl) 75.0 (17-256) 31.5 (14-220) 0.240
OCBs 0/4 (0%) 13/26 (50%) 0.113
Elevated IgG index (> 0.73) 0/4 (0%) 8/21 (38%) 0.269
Tumor 2 (33%) 17 (50%) 0.664
1Brain parenchymal lesions including demyelinating lesions, 2Paroxysmal discharges or slowing
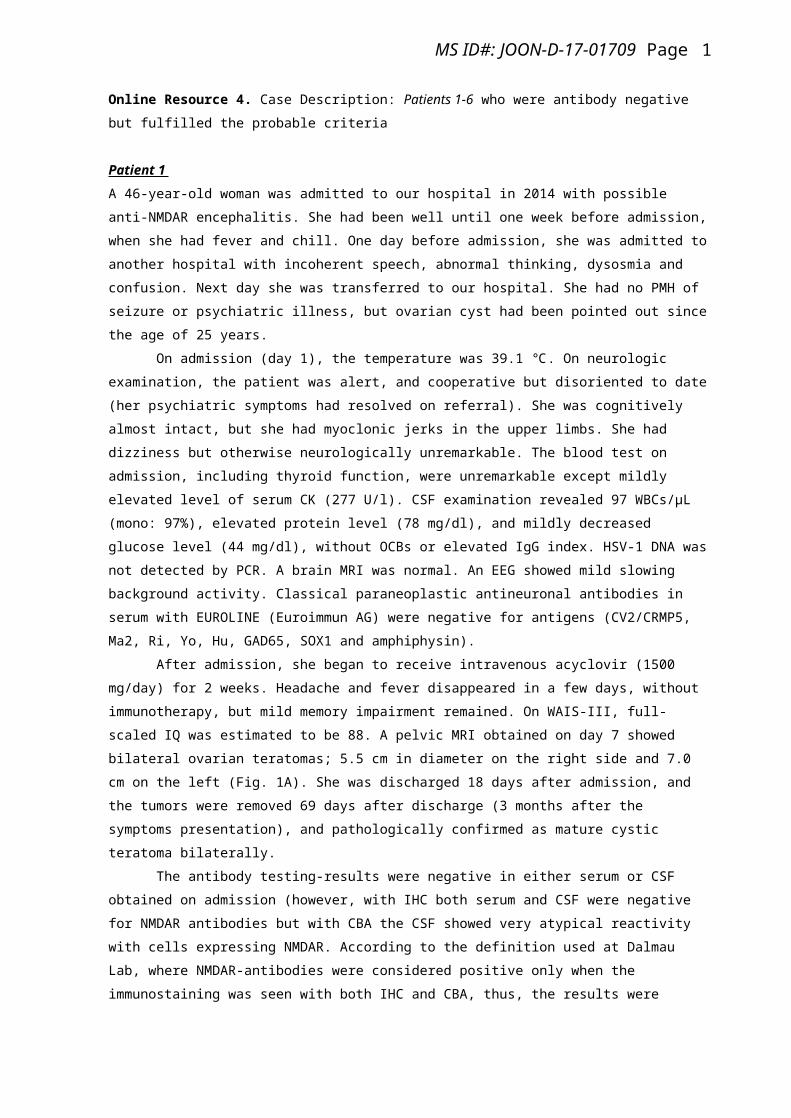
Online Resource 3. Supplementary Figure 1: Probability of NMDAR antibody detection versus age at onset
This graph of a logistic regression curve
shows the probability of NMDAR antibody
2
MS ID#: JOON-D-17-01709 Page
detection versus age at onset. Age at onset is significantly associated with the probability of antibody detection
(p=0.014, Wald test).
Note that the probability of antibody detection is less
than 0.5 in patients aged 50 years or older.
A logistic regression analysis was performed for association between probability of antibody detection and age at
onset with Wald test. JMP, version 11.2.0 (SAS Institute Inc.), was used.
3
MS ID#: JOON-D-17-01709 Page
Online Resource 4. Case Description: Patients 1-6 who were antibody negative but fulfilled the probable
criteria
Patient 1
A 46-year-old woman was admitted to our hospital in 2014 with possible anti-NMDAR encephalitis. She had
been well until one week before admission, when she had fever and chill. One day before admission, she was
admitted to another hospital with incoherent speech, abnormal thinking, dysosmia and confusion. Next day she
was transferred to our hospital. She had no PMH of seizure or psychiatric illness, but ovarian cyst had been
pointed out since the age of 25 years.
On admission (day 1), the temperature was 39.1 ℃. On neurologic examination, the patient was alert,
and cooperative but disoriented to date (her psychiatric symptoms had resolved on referral). She was cognitively
almost intact, but she had myoclonic jerks in the upper limbs. She had dizziness but otherwise neurologically
unremarkable. The blood test on admission, including thyroid function, were unremarkable except mildly
elevated level of serum CK (277 U/l). CSF examination revealed 97 WBCs/µL (mono: 97%), elevated protein
level (78 mg/dl), and mildly decreased glucose level (44 mg/dl), without OCBs or elevated IgG index. HSV-1
DNA was not detected by PCR. A brain MRI was normal. An EEG showed mild slowing background activity.
Classical paraneoplastic antineuronal antibodies in serum with EUROLINE (Euroimmun AG) were negative for
antigens (CV2/CRMP5, Ma2, Ri, Yo, Hu, GAD65, SOX1 and amphiphysin).
After admission, she began to receive intravenous acyclovir (1500 mg/day) for 2 weeks. Headache and
fever disappeared in a few days, without immunotherapy, but mild memory impairment remained. On WAIS-III,
full-scaled IQ was estimated to be 88. A pelvic MRI obtained on day 7 showed bilateral ovarian teratomas; 5.5
cm in diameter on the right side and 7.0 cm on the left (Fig. 1A). She was discharged 18 days after admission,
and the tumors were removed 69 days after discharge (3 months after the symptoms presentation), and
pathologically confirmed as mature cystic teratoma bilaterally.
The antibody testing-results were negative in either serum or CSF obtained on admission (however,
with IHC both serum and CSF were negative for NMDAR antibodies but with CBA the CSF showed very
atypical reactivity with cells expressing NMDAR. According to the definition used at Dalmau Lab, where
NMDAR-antibodies were considered positive only when the immunostaining was seen with both IHC and CBA,
thus, the results were considered to be negative, but the results did not exclude the possibility that the patient
may have extreme low titers of NMDAR-antibodies against different epitopes of the receptor). The follow-up
CSF examination obtained 3 months later was normal (4 WBCs/µL, protein 39 mg/dl). NMDAR-antibodies were
negative. At the last follow-up (approximate 6 months after the symptoms onset), the mRS was scored 0, without
any relapse of symptoms.
Patient 2
A 19-year-old woman was admitted to our associated hospital in 2016 with possible encephalitis. She had been
well until 5 days before admission, when fever and headache developed. One day before admission she was seen
at another hospital, where ceftriaxone was administered intravenously. On the day of admission, she underwent a
brain MRI, which showed increased DWI/FLAIR signals in the splenium (not shown), and then she was referred
1

MS ID#: JOON-D-17-01709 Page
to our associated hospital. Her PMH included atopic dermatitis since childhood but otherwise unremarkable. Her
family history was unremarkable. She had no habits of smoking, drinking, or the use of illicit drugs.
On admission (day 1), the temperature was 39.9°C. On neurologic examination the patient was awake,
well oriented to time and place, but not completely alert. She reported photophobia but no cognitive dysfunction
or psychiatric symptom was seen. The deep tendon reflexes were exaggerated in the upper limbs but normal in
the lower limbs. She had no limb ataxia but her walking was slightly unsteady. She had no bladder or bowel
dysfunction. She had neck stiffness. The blood test on admission were unremarkable, including thyroid function,
tumor markers, ANA and autoantibodies against GAD, Tg, TPO, GQ1b, GM1, AQP4, SS-A/Ro, or SS-B/La.
CSF examination on admission revealed 81 WBCs/μL (mono: 99%), elevated protein level (89 mg/dl), and
decreased glucose level (40 mg/dl), without OCBs or elevated IgG index. The MBP level was markedly elevated
(3210 pg/ml, normal < 102). Cytological examination was negative. An EEG showed mild slowing activity
without PD.
She was empirically treated with intravenous acyclovir (1500 mg/day) but PCR testing for HSV-1 was
negative. On day 3 she developed myoclonic jerks in all limbs, diplopia, dysarthria, left hemi-ataxia, startle
reaction, bladder and bowel dysfunction, and decreased level of consciousness. A brain MRI obtained on day 3
showed increased DWI/T2/FLAIR signals in the splenium (Fig. 1B, C) with abnormal restricted diffusion on
apparent diffusion coefficient maps (not shown). She was treated with IVMP (1000 mg/day, 3 days); however,
hyponatremia developed. On day 5 the level of consciousness further deteriorated, and she vomited, causing
aspiration pneumonia. The serum level of sodium was 115 mEq/L. On day 6 she was intubated and sedated under
mechanical ventilation support. A brain CT showed brain edema, which was treated with intravenous glycerol
and intravenous infusion of barbiturate. Central hypoventilation and hypersalivation developed. She also
received additional IVMP. A pelvic CT showed a tumor of the left ovary. On day 19 she underwent a
laparoscopic left oophorectomy (pathologically confirmed as a mature teratoma). She also received the 3rd cycle
of IVMP. After that, her neurologic symptoms became markedly improved, but persistent hypersalivation and
nocturnal apnea persisted. The follow-up MRI on day 28 showed mildly increased T2 signal in the mid-brain and
pons. The level of consciousness had gradually improved. On Day 77 she was discharged. During her
hospitalization, no convulsive seizure or apparent orofacial-limb dyskinesias developed, but transient episodes of
perioral muscle twitching or myoclonic jerks developed.
Both serum and CSF were confirmed to be negative for antibodies against NSA including NMDAR or
Glycine receptor. MOG and AQP4 antibodies were also examined and negative. At the last follow-up (3 months
after presentation), the m RS was scored 2, without relapse of symptoms.
Patient 3
A 32-year-old woman was transferred to our hospital in 2012 with possible anti-NMDAR encephalitis. She had
been in her usual state of health until 7 months before transfer, when she began to complain of depressive
symptoms, anorexia and weight loss. Since 5 weeks before transfer, she had insomnia and then visited a local
hospital where antidepressant was prescribed but did not work. She began to have delusional thinking, and
hallucination, and show abnormal behaviors. Four weeks before transfer, she was first admitted to the other
psychiatric hospital. After admission, schizophrenia-like symptoms had been getting worse with low-grade fever
2

MS ID#: JOON-D-17-01709 Page
and tachycardia. Two weeks before transfer, she became bed-ridden due to catatonic stupor with speech
dysfunction, increased muscle tone and abnormal posture. Four days before transfer, convulsive seizures
developed, and then she was transferred to our hospital. She had a 2-year history of lung tuberculosis, for which
she had been treated with anti-tuberculosis drugs. Her family history was unremarkable except her mother who
had schizophrenia. She had no habits of drinking or smoking.
On admission (day 1) the temperature was 37.9℃. Physical examination showed dehydration and
emaciation (163 cm, 40 kg). On neurologic examination, the patient was awake with the eyes opened, but she
continued speaking incomprehensible words; she was not able to follow simple commands. Her facial expression
was masked face, with twitching in the peri-oral muscles. The eyes were tended to deviate to the left, but no
nystagmus was seen. She was in a bed-ridden state with abnormal posture; she was able to raise the right upper
extremity, but the left upper extremity was being bended at the elbow, and both lower extremities were extended.
The muscle tone was rigid and paratonic in all extremities. Myoclonic jerks and tremulous movements were
occasionally seen in the right upper extremity. The deep tendon reflexes were hyperactive on both sides without
Babinski sign. The neck was rigid in all directions. The blood tests on admission, were normal or unremarkable
except serum CK (372 U/L), CRP (6.19 mg/dl, normal < 0.30), FDP (17.5 μg/ml, normal <5.0), and D-dimer
(6.43 μg/ml, normal <0.72). CSF examination on admission showed 1 WBC/μL, without elevated IgG index or
OCBs. A brain MRI was unremarkable. An EEG showed mild slowing activities without PD. A whole body CT
showed no evidence of tumor including ovarian teratoma. She was treated with 1 cycle IVMP (1000 mg/day, 3
days) and 2 cycles of IVIg (0.4 g/kg/day, 5 days), without apparent clinical improvement.
Both serum and CSF were negative for NSA including NMDAR. She was transferred to the referring
hospital on day 26; on discharge the mRS remained 5. The cause of encephalopathy remained unknown.
Patient 4
A 51-year-old woman was admitted to our associated hospital in 2016 with possible anti-NMDAR encephalitis.
She had been in her usual state of health until 11 days before admission, when she began to complain of not
feeling well and having dizzy on walking without prodromal headache or fever. She visited a local clinic and she
was diagnosed with depression. On the day of admission, prominent psychiatric symptoms developed; she was
brought in by ambulance to the emergency room of our associated hospital. On referral, the temperature was
36.7°C. She was in delirious state with prominent psychiatric symptoms and incoherent speech. She was initially
admitted to the department of psychiatry. Her PMH included epileptic seizure at 12 years of age, but no clinical
seizure developed after initiation of the treatment with carbamazepine 200 mg and clonazepam 2 mg. She also
had chronic alcoholism since the age of 30 years, for which she required a 2-month hospitalization at the age of
37 years. Her family history was unremarkable. She had a habit of drinking of beer 2000 ml, daily.
On admission (day 1) the patient was in delirious state with incoherent speech. She was treated with
risperidone 2 mg and nitrazepam 5 mg for acute psychosis, but next day she became unresponsive with her eyes
opened with increased muscle tone showing a catatonic stupor. On day 3 she developed apneic spells with right
gaze preference. On day 4 orofacial-limb dyskinesias developed. On day 5 she was transferred to the department
of neurology. On referral, the temperature was 36.7°C, the blood pressure 160/100 mmHg, and oxygen
saturation was 97% while she was breathing ambient air. On neurologic examination the patient was awake but
3

MS ID#: JOON-D-17-01709 Page
mute and unresponsive to noxious stimuli, without withdrawal response; she had orofacial-limb dyskinesias with
irrhythmic myoclonic jerks in her extremities, with increased muscle tone in all extremities. The neck was rigid
in all directions.
Blood test including thyroid function were unremarkable, except mildly elevated level of serum CK
(279 U/L). Additional testing for ANA, and autoantibodies to DNA, SS-A/Ro, SS-B/La, Tg, TPO, MPO-ANCA
or GAD was unremarkable. CSF examination on day 5 revealed 1 WBC/μL, with normal protein level (25
mg/d), and normal glucose level (80 mg/dl). On day 6, apneic spells frequently developed, with hypersalivation
and fever, resulting in aspiration pneumonia. On day 7 she remained unresponsive, with right gaze preference,
and marked rigidity on the left side, but involuntary movements subsided. CSF examination on day 7 was
unremarkable; HSV-PCR was negative, but IL-6 level was slightly elevated (545 pg/ml). Classical
paraneoplastic antineuronal antibodies in serum were also negative for antigens including CV2/CRMP5, Ma2,
Ri, Yo, Hu, GAD65, SOX1, and amphiphysin. A brain MRI obtained on day 7 showed symmetric increased
DWI signals in the basal ganglia, insula, opercular cortex, and temporal and parietal lobes (not shown). A whole
body CT showed the right ovarian cyst, but an ultrasonography did not confirm solid tissue in the ovarian cyst.
The trachea was intubated and she was assisted by ventilator support with continuous infusion of midazolam.
She was treated with intravenous acyclovir (1500 mg/day) and levetiracetam. She also received IVMP
(1000 mg/day, 5 days) from day 12. On day 14 an EEG showed diffuse delta slowing but no PD were seen. On
day 19, she was transferred to the other associated hospital. A brain MRI showed multifocal but almost
symmetric increased DWI/FLAIR signals in the insular cortex, peri-Sylvian opercular cortex, and temporo-
parieto-occipital cortex (Fig. 1D-F). She received the second cycle of IVMP on day 33, and underwent a
laparoscopic right oophorectomy on day 58 (pathologically confirmed as a paraovarian cyst but not teratoma).
The serum and CSF obtained on day 7 at the initial hospital were confirmed to be negative for NSA
antibodies including NMDAR. She was then back to the initial hospital 10 weeks later, and transferred to a care
hospital 11 months after the symptoms presentation. At the last follow-up, the mRS was scored 4, with
psychiatric symptoms.
Patient 5
A 51-year-old man was admitted to our associated hospital in 2017 with possible encephalitis. Ten days before
admission, he began to complain of headache. Three days before admission, leg weakness developed. One day
before admission at night he complained of visual and auditory hallucinations, and followed by involuntary
movements. Next day he was referred to the emergency room, and he was admitted to the hospital. His PMH was
unremarkable, but he had a family history of dementia in his father, suicide in his mother, and schizophrenia in
his younger sister. He had a 20-pack-year history of smoking but quit at the age of 40 years. He consumed large
amounts of alcohol only at weekend.
On admission (day 1), the temperature was 36.5°C. On neurologic examination, the patient was agitated
with incoherent speech. He was able to raise his upper extremities but not his lower extremities. He had
excessive eye blinking, perioral twitching, startle reaction in all extremities to external stimuli, myoclonic jerks,
and tremulous head movements. He had hyperreflexia but the plantar response was flexor. He had neck stiffness.
4
MS ID#: JOON-D-17-01709 Page
The blood tests on admission were unremarkable except hyponatremia (Na 129 mEq/L), and mildly
elevated level of NH3 (76 μg/dl). Testing for ANA and autoantibodies against GAD, SS-A/Ro, SS-B/La, Tg,
TPO, MPO-ANCA, were all negative. Classical paraneoplastic antineuronal antibodies measured in serum with
EUROLINE (Euroimmun AG) were negative for antigens including CV2/CRMP5, Ma2, Ri, Yo, Hu, GAD65,
SOX1, and amphiphysin. CSF examination obtained on admission revealed 43 WBCs/μL (mono 99%), with
marked elevated protein level (256 mg/dl), and slightly decreased level of glucose (47 mg/dl), without OCBs or
elevated IgG index. The CSF level of sIL-2R was elevated (1340 U/ml). Cytological examination was negative.
HSV-1 PCR was negative. A whole body CT showed no evidence of malignancy. A brain MRI obtained on day
4 showed sulcus FLAIR hyperintensity in the parieto-occipital lobes, probably reflecting edema and protein
leakage. (Fig. 1G-I).
On admission (day 1), he was intubated and sedated with continuous infusion of anesthetic drugs. He
was empirically treated with antibiotics, acyclovir (1500 mg/day), fosphenytoin, and IVMP (1000 mg/day, 3
days). Myoclonic jerks resolved. An EEG obtained on day 2 showed diffuse slowing without PD. Follow-up
CSF examination on day 6 showed reduction in inflammatory changes; WBCs were 12/μL (mono 100%), with
elevated protein level (144 mg/dl), decreased level of glucose (29 mg/dl; serum glucose 90 mg/dl), and elevated
sIL2R level (533 U/ml). Latex agglutination test for cryptococcus antigens, and nested PCR for mycobacteria
tuberculosis were negative. Cytological examination did not show any evidence of tumor. On day 9 he received
additional IVMP. On day 10 the trachea was extubated. Follow-up CSF examination on day 16 revealed 3 WBCs
/μL, with elevated protein level (99 mg/dl), and decreased level of glucose (40 mg/dl; serum glucose 90 mg/dl).
On day 20, he received the third cycle of IVMP, resulting in gradual recovery of the symptoms.
Both serum and CSF obtained on admission were confirmed to be negative for NSA including
NMDAR. He was discharged on day 54. At the last follow-up (8 months after initial symptoms presentation) the
mRS was scored 2, with mild emotional symptoms.
Patient 6
A 74-year-old man was transferred to our associated hospital in 2017 with possible status epilepticus. He had
been in his usual state of health until approximately 3 months before transfer, when behavioral changes
developed, without apparent preceding headache or fever. He began to show nocturnal wandering behavior. Ten
weeks before admission he was seen at the emergency room at another hospital, but his behavioral alterations
were supposed to be due to fatigue, and he returned home. Afterwards, disorganized thinking and delusion
developed. He was given aripiprazole by the other hospital. Nine weeks before admission, he was admitted to the
hospital with hyponatremia (125 mEq/L). After admission hyponatremia was corrected, but the level of
consciousness fluctuated. One day before transfer, wandering behaviors developed again. Next day, he had fever
and seizure-mimicking involuntary movements in both upper extremities, and peri-oral twitching also repeatedly
developed. After receiving intravenous fosphenytoin and levetiracetam, and he was transferred to our associated
hospital. He had a PMH of hypertension, and benign prostate hypertrophy. His family history was unremarkable.
He had no habits of smoking, drinking, or the use of illicit drugs.
On admission (day 1), the temperature was 37.5°C, the blood pressure 137/78 mmHg, and the pulse 81
beats per minute, regular, and the oxygen saturation 100% while he was breathing oxygen at 2 L/min through the
5
MS ID#: JOON-D-17-01709 Page
nasal cannula. On neurologic examination he was awake but mute and not able to follow verbal commands or
answer to questions. The function of the cranial nerves was grossly normal, but both eyes tended to deviate to the
left. He was able to move all extremities spontaneously. He had a tendency to show catalepsy-like posture. The
deep tendon reflexes were normal in the upper extremities but decreased in the lower extremities; the plantar
response was flexor. The neck was rigid in all direction.
The blood tests on admission showed mild anemia (Hb 10.6 g/dl) and mild leukocytosis (WBC
10,000/μL), elevated serum CK level (1,324 U/L), and mild liver dysfunction, but serum sodium level was
normal (137 mEq/L). The serum CRP was 3.34 mg/dl, and serum BNP level was elevated (211.1 pg/ml).
Thyroid function was normal. Testing for autoantibodies for Tg, TPO, ANA, SS-A/Ro, SS-B/La, ds-DNA, Sm,
MPO-ANCA, PR3-ANCA, and cardiolipin were all unremarkable or negative. CSF examination obtained on
admission revealed 8 WBCs/μL (mono 4%) with mildly elevated protein level (46 mg/dl), and normal glucose
level (61 mg/dl); IgG index and OCBs were not available. A brain CT was unremarkable. A whole-body CT did
not show evidence of tumor. An EEG on day 2 showed generalized slowing activity at 5-7 Hz, without PD.
He was treated with 2 cycles of IVMP (1000 mg/day, 3 days) from day 3 and day 14, respectively
resulting in gradual improvement in cognitive and motor disability. A brain MRIs on day 6 and day 20 were
unremarkable. Classical paraneoplastic antineuronal antibodies measured in serum with EUROLINE
(Euroimmun AG) were negative for antigens including CV2/CRMP5, Ma2, Ri, Yo, Hu, GAD65, SOX1, and
amphiphysin. He initially had some peri-oral twitching movements but no apparent faciobrachial dystonic
seizure developed; oral dyskinesia and catalepsy-mimicking postural abnormality developed transiently, but
quickly disappeared following IVMP. No autonomic symptoms, or central hypoventilation developed. He
became able to walk without assistance, and talk and eat by himself. On day 38 he was transferred to a
rehabilitation hospital.
The CSF and serum obtained on admission are confirmed to be negative for NSA antibodies, including
NMDAR. At the last follow-up (7 months after initial symptoms presentation) the mRS was scored 0.
6

MS ID#: JOON-D-17-01709 Page
Online Resource 5. Case Description: Patients 7-11 who were antibody positive but not fulfilled the probable
criteria. A pat of the clinical information of Patients 7-9 were previously reported elsewhere1.
Patient 7
A 21-year-old man was admitted to our hospital in 2012 with generalized seizure. Two weeks before admission
he began to have dysesthesia in the lateral surface of the left leg and difficulty in moving the left lower
extremity, which was gradually accompanied by pain. He also complained of some memory loss. Six days before
admission he was seen at our hospital. On examination he had hyperreflexia in the left lower extremity, but
otherwise unremarkable. Brain MRI and EMG examination were normal. On the day of admission, from the
morning he had multiple attacks of painful tonic spasms in the left leg, and at 11 pm he had secondarily
generalized tonic seizure starting as focal painful tonic spasm in the left lower extremity, and then he was
brought to our hospital. He had a PMH of second degree AV block. His family history was unremarkable.
On arrival, the temperature was 37.0°C, the blood pressure 139/73 mmHg, and the pulse 67 beats per
minutes. He had multiple seizures, which began with a short-lasting painful tonic seizure of the left lower
extremity with extension of the knee and planter flexion of the foot, followed by generalized tonic seizure with
head extension and loss of consciousness. Cyanosis and sinus bradycardia developed transiently associated with
breath holding during the attack. After receiving intravenous injection of diazepam, the patient regained his
consciousness and he was admitted to our hospital.
On admission (day 1) the patient was alert, cooperative, and well oriented to time and place. No
psychiatric symptom was seen, but he had decreased attention span and short-term memory loss. He also had
numbness and mild weakness in the left lower extremity, and he occasionally had tonic spasm in the left leg. The
deep tendon reflexes were exaggerated in all extremities, more marked in the left lower extremity with Babinski
sign. The coordination was normal but he couldn’t stand or walk without assistance. The neck was supple. The
results of the blood tests on admission, including ANA, antibodies against dsDNA, MPO-ANCA, SSA/Ro, SS-
B/La, and GAD, were normal, except elevated level of CK (380 U/L), uric acid (9.7 mg/dl), and lactate (38.8
mg/dl). CSF examination on admission showed 12 WBCs/μL (mono 100%), with normal protein level (35
mg/dl) and normal glucose level (57 mg/dl). The IgG index was normal, and OCBs were not detected. The result
of PCR for HSV-1 was negative. A brain MRI was normal. An EEG showed mild slowing activities in the right
cerebral hemisphere.
The patient was initially treated with intravenous administration of phenytoin and oral levetiracetam,
but began to receive IVMP (1000 mg/day, 5 days) twice from day 6, and day 21, respectively. On day 28
NMDAR antibodies were confirmed in CSF obtained on admission (negative in serum). Based on the result, the
patient also received IVIg (0.4g/kg/day, 5 days) with gradual taper of prednisolone. After these immunotherapies
with antiepileptic agents, all symptoms improved, and he was discharged 2.5 months later. After this he had no
recurrence of seizure. He had full recovery without any neurological deficit at the last follow-up (mRS 0 at 84
months).
Patient 8
1

MS ID#: JOON-D-17-01709 Page
A 18-year-old boy was admitted to our hospital in 2010 with status epilepticus partialis continua. He had been in
his usual state of health until 22 months before admission (at 16 years of age), when he had the first attack of
generalized convulsive seizure. After that he had twice attacks of seizure, 2 months, and 3 months later,
respectively. However, he refused taking AED until the fourth attack. After taking valproate (400 mg/day) he
had no seizure. One day before admission he complained of fatigue. Next morning, convulsive seizure developed
in his left side of the body, which repeated intermittently, and he was brought in by ambulance to our hospital.
He had a PMH of ADEM at the age of 8 years, which presented with fever, left hemiparesis and
bilateral visual impairment. He was admitted to our hospital and treated with IVMP resulting in resolution of
symptoms, however one week later right hemiparesis developed. A brain MRI showed multiple demyelinating
lesions with multifocal enhancements (not shown). He was treated with multiple courses of IVMP, resulting in
resolution of symptoms. A family history was unremarkable.
On admission (day 1), the temperature was 37.4°C. The patient was alert without neurological deficits.
The blood tests were normal, including ANA, LAC, SS-A/Ro, and SS-B/La. CSF examination revealed 9
WBCs/μL, and normal protein level; however, IL6 was elevated (427 pg/ml). An EEG showed irregular frontal
slow activity without PD. Enhanced FLAIR image on day 4 showed gadolinium enhancement along bilateral
medial frontal cortex (not shown). After admission he was treated with phenytoin, carbamazepine, lamotrigine,
or clobazam, but fever persisted. The follow-up MRI on day 13 (Fig. 2A, B) showed more extensive enhancing
lesions, for which he received IVMP, resulting in rapid decline in temperature, but the temperature rose up again,
and he received additional IVMP, followed by oral prednisolone. Follow-up MRI on day 27 revealed resolution
of abnormal enhancement. He was discharged on prednisolone 40 mg/day with AEDs (clobazam 10 mg/day, and
valproate 800 mg/day) on day 33. Prednisolone was subsequently gradually tapered-off approximately 4 months
later. AEDs were discontinued 5 years after discharge.
Both NMDAR and MOG antibodies were detected in serum and CSF obtained on admission. The
patient became symptom free for 5-year observation period. At the last follow-up (62 months after discharge); he
was free of symptoms, with mRS of 0.
Patient 9
A 17-year-old girl was admitted to our hospital in 2011 with progressive right hemiplegia. She had been well
until 3 weeks before admission, when she noticed dysesthesia in the right hand, after that progressive weakness
in the right upper and lower extremities gradually developed. Eight days before admission the weakness rapidly
developed, and she was admitted to our hospital. She had a PMH of Kawasaki disease in her childhood.
On admission (day 1), the temperature was 36.6°C. On neurologic examination she the patient had
moderate weakness in the right upper and lower extremities, with a grip power of 2.5 kg on the right side and 16
kg on the left. She had mild sensory loss in the right side of the body. The blood tests were normal. CSF
examination obtained on day 2 revealed 2 WBCs/μL, and slightly elevated protein level (58 mg/dl) without
OCBs. The IgG index was normal, but the MBP level was elevated (355 pg/mL, normal < 102). CSF JC virus
DNA was not detected. A brain MRI on day 2 showed multifocal increased T2/FLAIR signals in the cerebral
white matter (Fig. 2C-F) with subtle patchy enhancement mimicking “cloud-like enhancement”.
2

MS ID#: JOON-D-17-01709 Page
She was treated with IVMP (1000 mg/day, 5 days) from day 2, followed by gradual tapering of
prednisolone. Despite the treatment with IVMP, she developed complete right hemiplegia on day 3. Then she
was treated with IVIg (0.4g/kg/day, 5 days) from day 3, and plasma exchanges from day 9. Following the
immunotherapies, the motor weakness began to improve since day 16. After that, the weakness gradually
improved and she was discharged on day 61 with mild weakness in the right side. On day 62, NMDAR
antibodies were confirmed in both serum and CSF obtained on admission (but AQP4 or MOG antibodies were
not detected in either serum or CSF). She was also treated with azathiopurine (50 mg/day). The motor function
gradually recovered over years and the mRS became 1. Three years after discharge, azathiopurine was
discontinued. The follow-up MRI showed gradual improvement of initial lesions.
Five years after the symptoms presentation, she was re-admitted to our hospital in 2016 with a relapse
of symptoms. One day before admission she noticed numbness in the right posterior neck to the shoulder and
followed by right arm weakness in the evening. Next day she was seen at the emergency room and admitted to
our hospital. A cervical MRI on admission showed increased T2 signal in the C1-C2 with mild enhancement.
CSF examination revealed 2 WBCs/μL (mono 100%), with normal level of protein and normal glucose. OCBs
are negative. She began to receive IVMP (1000 mg/day, 5 days), resulting in improvement. The CSF and serum
obtained on re-admission were negative for antibodies to NSA including NMDA, AMPA, GABA(B), LGI1 or
Caspr2. MOG and AQP4 were also determined to be negative. At the last follow-up (75 months after the initial
symptoms presentation) the mRS was scored 1.
Patient 10
A 33-year-old previously healthy woman was admitted to our hospital in 2016 with HSV encephalitis. Two
weeks before admission, she had abdominal pain, vomiting, and fever. She gradually became ill due to persistent
fever. She was transferred from another hospital and admitted to our hospital for possible encephalitis. Her PMH
and family history were unremarkable.
On admission (day 1), the temperature was 38.3°C, the blood pressure 93/50 mmHg, and the pulse 69
beats per minute, the respiratory rate 18 breaths per minute, and the oxygen saturation 98% while she was
breathing ambient air. On neurologic examination, she appeared ill, and she was somnolent, disoriented to time
or place, and apathetic, but no aphasia was seen. She had hyperreflexia, neck stiffness, and urinary retention. The
blood test on admission were unremarkable, except elevated level of serum CK (461 U/L). CSF examination on
admission revealed 118 WBCs/μL (mono 100%) with elevated protein level (77 mg/dl) and normal glucose level
(68 mg/dl). The IgG index was elevated (0.92) and 3 OCBs were detected; HSV-1 DNA was detected. A brain
MRI on admission showed right-side predominant T2/FLAIR signals in the temporal lobe, insular cortex, and
inferior-medial frontal and medial-dorsal frontal lobe, compatible with HSV encephalitis (Fig. 2G-I). An EEG
showed right frontal predominant slowing without periodic discharges.
She was treated with IV acyclovir (1500 mg/day, 14 days) with one cycle of IVMP (1000 mg/day, 5
days), resulting in clinical improvement. The follow-up brain MRI on day 17 showed intensive enhancement
along the gyrus of the affected cortex. CSF examination on day 28 revealed improved pleocytosis; WBCs were
25/μL, and the protein level was 116 mg/dl, with elevated IgG index (2.30) and OCBs. The mini-mental status
examination was scored 30 on day 36. On day 39 she underwent WAIS-III; verbal IQ, performance IQ, and full-
3

MS ID#: JOON-D-17-01709 Page
scale IQ were reported to be 97, 76, and 87, respectively. It was subsequently reported that the CSF obtained on
day 28 were positive for NMDAR antibodies with CBA but negative with IHC, while the serum was negative
with both techniques; the results of NMDAR antibodies were considered to be questionable, and on day 54 she
returned home.
After discharge, she was followed-up at the outpatient clinic. On day 78, when she came to our clinic,
she appeared slightly depressed and emotionally unstable because she was aware of slow thinking and difficulty
in performing daily activity. CSF examination on day 78 revealed further decline in WBC counts; WBC was
only 6/μL, the protein level was 90 mg/dl, with OCBs and sustained elevated IgG index (2.18) (however, it was
subsequently reported that the CSF obtained on day 78 was clearly positive for NMDAR antibodies with both
CBA and IHC, but the serum was very mild positive in only one of the two techniques). She returned home, but
after day 112 (16 weeks after the onset of HSV encephalitis) she became unable to manage her daily activity due
to depression, and she also began to have suicidal ideation. On day 133, at the outpatient clinic, she was much
depressed, but had no aphasia, apraxia or agnosia. CSF examination obtained on day 133 revealed 5 WBCs/μL,
and elevated protein level 72 mg/dl, with OCBs and elevated IgG index (1.07); NMDAR antibodies were again
positive in both serum and CSF. On day 147 (21 weeks after the initial symptoms presentation) she was re-
admitted to our hospital. A brain MRI showed no new lesions.
Under the diagnosis of autoimmune post-HSV encephalitis, she was treated with 2 cycles of IVMP
(1000 mg/day, 3 days), and 1 cycle of IVIg (0.4g/kg/day, 5 days) and followed by oral prednisolone 30 mg/day,
resulting in clinical improvement. On day 178, she was referred to another hospital; on discharge, she still
required her parents’ support to perform daily activity for residual depression, insomnia, anxiety, and apathy; the
mRS was scored 3 at the last follow-up (7 months after the symptoms presentation).
Patient 11
A 51-year-old woman was admitted to our associated hospital in 2016 with prominent psychiatric symptoms.
She had a PMH of acute myelitis of unknown causes at 26 years of age; she was admitted to another hospital
with paraparesis and sensory loss, and treated with IVMP, resulting improvement but left leg weakness and
bladder and bowel dysfunction remained. At 48 years of age, she had seizure beginning with visual field defect
and incoherent speech, and followed by generalized convulsive seizures. She was suspected to have complex
partial seizure at the other hospital but no AED was started. Fifteen months before admission (at 50 years of age)
she was re-admitted to the hospital with decreased level of consciousness associated with hyponatremia (111
mEq/L). She also had left optic neuritis and extraocular movement abnormalities in the left eye (no detailed
information is available). A brain MRI showed increased T2/FLAIR signals in the left thalamus and pons. She
was diagnosed with NMOSD associated with AQP4 antibodies, and treated with IVMP (1000 mg/day, 5 days),
followed by short-term use of prednisolone and she was discharged.
Ten months before admission, she began to complain of general fatigue, nausea, vomiting, and diarrhea.
Nine months before admission, psycho-behavioral and cognitive dysfunction gradually develop and she became
difficult to perform her daily activities. She was often absentminded in the daytime, and her psycho-behavioral
changes including depression had further deteriorated. Four months before admission, she became apathetic and
indifferent to her daily activity. Six days before admission she became agitated and incoherent. One day before
4
MS ID#: JOON-D-17-01709 Page
admission, she was referred to the department of psychiatry at our associated hospital. A brain MRI showed
increased FLAIR signals in the left medial temporal subcortical area, extreme capsule, posterior external capsule,
posteromedial part of the left thalamus, and bilateral medial frontal cortex (Fig. 2J-L). Next day she was
admitted to the hospital. She had a PMH of hepatitis B and hepatitis C virus infection.
On admission (day 1), the temperature was 36.2°C. Physical examination was unremarkable. On
neurologic examination she was able to follow simple commands, or make simple gesture with her fingers, but
she was mute and indifferent to the surroundings; once she was agitated, she kept shouting loudly
incomprehensible words. She did not show withdrawal response to noxious stimuli despite the ability of moving
all extremities. The deep tendon reflexes were exaggerated in the lower extremities, with Babinski sign on the
right side. The blood tests were unremarkable, including antibodies against human immunodeficiency virus, Tg,
TPO, SS-A/Ro, SS-B/La, MPO-ANCA. CSF examination on day 1 revealed 6 WBCs/μL (mono 100%), with
normal protein level (27 mg/dl), and normal glucose level (55 mg/dl); OCBs were negative but IgG index was
elevated (0.90). The MBP level was < 40 pg/ml (normal < 102). Classical paraneoplastic antineuronal antibodies
measured in serum with EUROLINE (Euroimmun AG) were negative for intracellular antigens (CV2/CRMP5,
Ma2, Ri, Yo, Hu, GAD65, and amphiphysin). An EEG recorded on day 2 showed diffuse alpha slowing with
mild attenuation of alpha activity in the left temporal area, without PD. A thoracic MRI obtained on day 5
showed faint T2 hyperintensities in the mid thoracic cord. On day 6 an enhanced brain MRI showed only faint
enhancement in the lesion (not shown).
After admission, the psychiatric symptoms had subsided spontaneously over a week, but subsequently
she fell into catatonic stupor with gradual development of orofacial dyskinesias on day 4. On day 10 athetoid-
dystonic movements also developed. These involuntary movements were refractory to intermittent injection of
diazepam, phenytoin or levetiracetam leading to continuous infusion of midazolam or propofol. She was treated
with IVMP (1000 mg/day, 3 days) from day 14, followed by prednisolone (20 mg/day); however, on day 14
generalized seizure developed beginning with focal seizure of the right arm with right gaze preference. On day
20 she was started on levetiracetam (1000 mg/day), but seizures repeated with transient reduction in blood
pressure and increased salivation. On day 21 she was started on plasma exchange; however, seizures persisted
and bulbar palsies developed. On day 22, she developed central hypoventilation with decreased level of
consciousness requiring mechanical ventilation support. A pelvic MRI did not show any evidence of ovarian
teratoma. Following 7 cycles of plasma exchanges over 2 weeks, the level of consciousness began to improve
gradually. On day 42 she was weaned off the ventilator. On day 61 she was transferred to another hospital. On
discharge the mRS was scored 5, but at the last follow-up (13 months after admission to our hospital) the mRS
was scored 2. NMDAR antibodies were detected in both serum and CSF.
References
1. Iizuka T, Kaneko J, Tominaga N, et al. Association of progressive cerebellar atrophy with long-term
outcome in patients with anti-n-methyl-d-aspartate receptor encephalitis. JAMA Neurol. 2016;73(6):706-13.
doi: 10.1001/jamaneurol.2016.0232.
5