counselling skills for medical termination of pregnancy · counselling skills for medical...
TRANSCRIPT
1
Counselling Skills forMedical Termination
of Pregnancy
Acknowledgements
This dissertation is the result of undertaking self-imposed formal study in form ofthe “Edexcel Professional development Diploma in Counselling”. This part-timeevening study has only been possible with the full support of my family, all of mycolleagues in the imaging department, Sister N Cline and staff on the MTOP Unit,Rev John Fisher, the Gynaecologists, my employers and Pam Martin from “NorthLindsey College”.
I gratefully acknowledge all the help I have received.
2
Dissertation: Counselling skills for Medical Termination of Pregnancy.
Subject of the Dissertation:Issues relating to the counselling of females attending the ultrasound department for a gestationalscan prior to a medical termination of pregnancy (MTOP) are considered.
Introduction.
Definition of Medical Termination of Pregnancy:
“Medical Termination of Pregnancy using mifespristone and misoprostol has enabled women toundergo termination of pregnancy without a surgical procedure”The procedure is very similar to a woman experiencing a miscarriage (Slade et al, 1998).
Aims of the dissertation.By undertaking this research, I would like to find out about the anxiety levels associated withfemales who are attending the ultrasound department. The scan will assess the age of thepregnancy prior to having a termination. This is important because the treatment, which will beoffered, depends on the accurate age of the pregnancy. Many of these ladies would have gone togreat lengths to evaluate why a pregnancy at this particular time is unwelcome.The clients are normally referred to hospital by their General Practitioners (GPs) for consultationto end their pregnancy. They see coming to the ultrasound department as a great hurdle, whichthey will have to face. Majority of the clients have a high anxiety levels at this very critical time intheir lives. I would like to find to find out how this anxiety can be reduced during the waiting andexamination before returning back to the MTOP unit. Although all this is undertaken on the sameday, it is an event, which may affect the rest of their lives. Indeed it is often perceived as anegative life event.
Relationship to previous workLiterature search.CINHAL, Medline, and the Obstetric and Gynaecologist Journals were used for the initial search.The literature survey found that there was no specific published research on counselling skillsrelating to scanning patients prior to terminating their pregnancy.Following the location of some general articles referring to termination of pregnancy, furtherpapers were obtained from the references given.I had found information relating to ultrasound examinations and the anxiety levels associated with:• Comparison of high feedback during the ultrasound examination to one where there is low
feedback and how this affects the anxiety levels of the patient. This is researched where thepregnancy leads to a live birth. (Zlotogoriski et al, 1996).
• There is some research on comparison of medical and surgical termination of pregnancy, butthere is no mention of specific counselling skills, which are required whilst waiting for andduring a gestational scan. (Slade et al, 1998).
• The process of grieving following termination for abnormalities (Bewley (1993), Kenyon,1985)).
• The process of grief following termination of pregnancy (Adler (1975), Adler (1992),Lazarus (1985), Peppers (1987), Tentoni (1995)).
3
• Dealing with unplanned pregnancy (Wright, 1991).
Setting:A survey of patients was undertaken at a termination of pregnancy unit in a District GeneralHospital.This was a prospective study where participants were patients who attended the MTOP unit forending their pregnancy during a six-week period, which commenced 29th March 1999 and endedon 21st May 1999.
Background.There is an increasing demand for termination of pregnancies. The service has been developed toprovide a fast-track diagnostic and therapeutic care for the clients in an environment, which isinformative, empathetic, and non-judgmental. Staff grade medical staff supports this with theback- up from a consultant. The central lead professional is the specialist nurse and her staff. Allthe stakeholders felt that the previous service was inappropriate to the patient’s emotional needs.By changing the environment and re-focussing the service, these needs were to be met. From anagency’s view there is increased efficiency and effectiveness of the service. In line with the MTOPunit’s consultation session, an ultrasound session is carried out at the same time, once a week. Thisis to confirm and date the pregnancy before any medical intervention is taken.
Permission from the Ethics Board.Before proceeding with this piece of research, permission was sought from the Director of Nursingwho is also on the Ethics Board. On obtaining permission from the Director of Nursing, supportfrom the Obstetric and Gynaecology Consultants was also necessary since I was surveying theirpatients. This was obtained verbally from one Consultant (who was also on the ethics board) whoassured me that he will inform his colleagues of my research during their departmental meetings.The Consultant offered support when necessary.Formal notification of the research was also submitted to the Department of Effective Healthcare.The purpose of this was to add my research and eventual results to the Trust’s database

4
Materials and Methodology
MaterialsPC with 64 megabytes capacity / printer /keyboard, using:• Microsoft Word 97.• Microsoft Excel 97.• Radiology Information System for confirming the number of clients who were examined prior
to ending their pregnancy.• Internet, Medline and CINHAL access.• Reports generated on the “Reality” reporting system• Acuson Aspen ultrasound system + accessories.• Hard copy ultrasound imaging on thermal paper.• Information from the Trust’s Management Information Systems on the number of deliveries
(births) at the hospital.
MethodologyA questionnaire was designed to elicit general and specific information on relating to counsellingissues and a pilot study was performed. Before implementation, there was a little hesitation fromone of the Consultants as to whether I could cause emotional damage by researching this group ofladies. Following reassurance the pilot study commenced.Seven participants (staff) were selected at random from my agency; a verbal explanation and acovering letter were included outlining the purpose of the questionnaire and asking for commentson the content and presentation of the questionnaire. This was to assess whether the questionnairewas appropriate and valid in a culturally emotive area.Following the pilot study, and advice from one of the consultants, some suggestions led toamendments being introduced to the questionnaire.Although the Sister on the MTOP unit had not seen the questionnaire she and her staff appeared tobe supportive. The questionnaires were left in her keeping on Friday 26.03.99 and were to bedistributed by the unit staff from Monday 29.03.99.A phone call on the first day (Monday) led to the distribution of the questionnaires being halted.The sister was unhappy with some of the questions and their inappropriateness of being asked.After negotiation it was agreed that the questionnaire could remain unchanged.The questionnaires were then distributed in the MTOP unit, week commencing 29.03.99 and tofinish collating the data week ending 21.05.99.During the six-week period, there were sixty-eight clients who attended the unit. There were forty-two questionnaires (61.8%) returned either to the MTOP clinic or directly to myself in the self-addressed envelopes provided. Twenty-six (38.2%) women declined to take part.
5
Results
Edited results relevant to this report are as follows:
Question 1: Age group of patients.For the purposes of data entry, the upper age from each category was entered on the database.19 patients were in the 15-24 years of age. This represents 54.76% of the service users.8 patients in the 30-34 age group. This represents the next biggest (19.05%) service user group.
Question 2: The residential area the client lives in.52% of the users are from the Scunthorpe area.
Question 3: Patient’s ethnicity.41 patients (97.62%) specified ethnicity as white.1 (2.38%) is unspecified. The respondent stated “American”.
Question 4: The patient’s relationship.22 patients (52.38%) are from a stable relationship.10 patients (23.81%) are from a recent break-up of a relationship.9 patients (21.43%) are single.1 patient (2.38%) did not respond.
Question 5: Is the pregnancy a result of contraceptive failure?28 patients (66.67%) stated that the pregnancy was the result of failed contraception.11 patients (26.19%) stated No.
Question 6: Has the patient told anyone about the pregnancy?39 patients (93%) had told someone about the pregnancy.3 (7%) had not informed anyone.
Question 6b: To whom does the patient confide in?13 patients (30.95%) confided in their partner.4 patients (9.52%) confided in a close friend.1 patient (2.38%) confided in a relative.4 patients (9.52%) confided in their parent.Most of the other responses were a combination of the above social support.1 patient (2.38%) did not respond.
Question 7a: Has the patient been exposed to any infectious diseases?38 patients (90.48%) stated No.1 patient (2.38%) stated Yes.2 patients (4.76%) didn’t know1 patient (2.38%) did not respond.
Question 7b: Which infectious disease they have been exposed to?41 patients (97.62%) did not respond.
6
1 patient (2.38%) stated Yes• The patient wrote “NSU” which is an abbreviation which stands for “non-specific urethritis”
This is an infection of the lower urinary system, which could be sexually transmitted.
Question 8: Has the client taken any medication during pregnancy?28 patients (66.7%) had not taken any medication.14 patients (33.3%) had taken medication.
Question 9: Was the medication prescribed?11 patients (26.19%) state that the medication was prescribed.5 patients (11.90%) indicate that it wasn’t prescribed.
Question 10: What worries does the patient have concerning the pregnancy?1 patient (2.38%) stated:• “couldn’t go through with pregnancy, Husband used to beat me and didn’t want any further
ties with him.”1 patient (2.38%) stated• “ Taking drugs”.28 patients (66.67%) did not respond.11 patients (26.19%) had no concerns.
Questions 11a and 11b were to elicit how we can help the patient through this difficult time.
Question11a: Can we help the patient with their concerns?31 patients ( 73.81 %) stated that we couldn’t help them.1 patient ( 2.38%) stated Yes.
Question 11b: How can we help?1 patient (2.38%) indicated No.40 patients (95.24%) did not respond.1 patient (2.38%) stated:• “To be caring and understanding of every individuals reasons, needs, especially to those who
don’t fully understand what will happen i.e. People who haven’t been through childbirth asthey won’t understand the level of pain involved”.
Please note:Questions 12, 13, 14 and 16 are the patient’s perception of the professional they came into contactwith.Question 15 was to elicit whether all agency staff have good communication skills.For this and the following questions, sympathy and not empathy was selected because it was feltthat the client would have a better understanding of this word in the context it was put in.
7
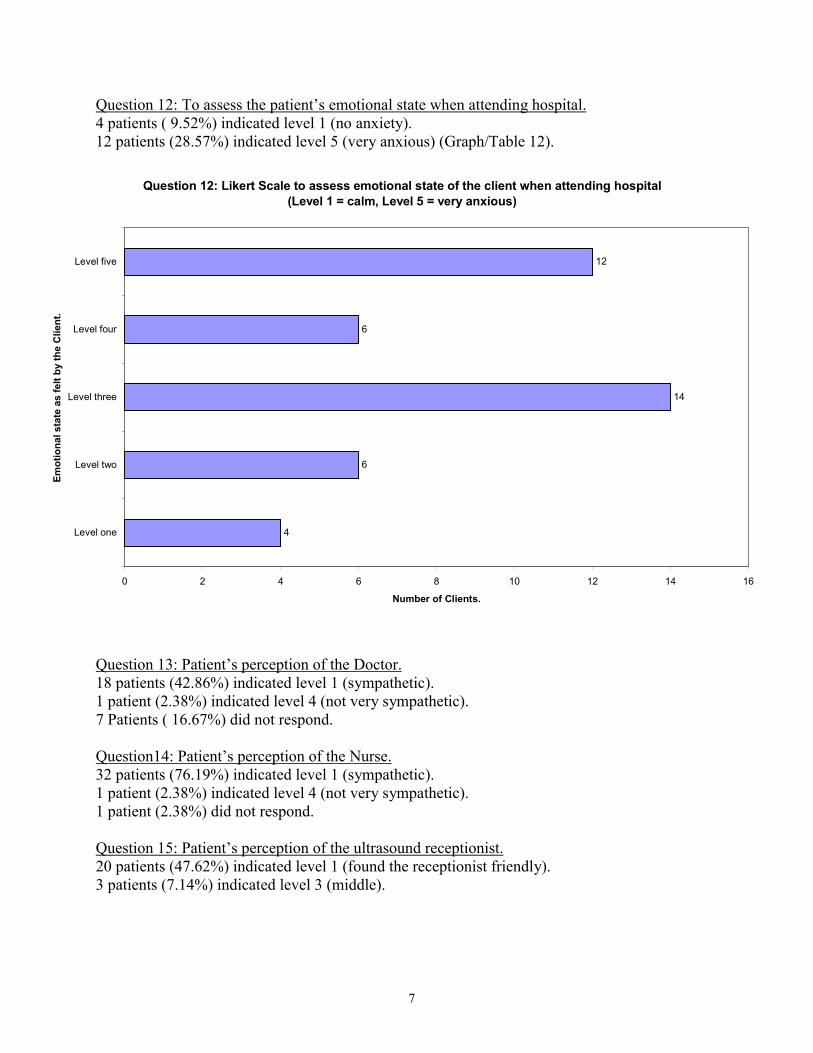
Question 12: To assess the patient’s emotional state when attending hospital.4 patients ( 9.52%) indicated level 1 (no anxiety).12 patients (28.57%) indicated level 5 (very anxious) (Graph/Table 12).
Question 13: Patient’s perception of the Doctor.18 patients (42.86%) indicated level 1 (sympathetic).1 patient (2.38%) indicated level 4 (not very sympathetic).7 Patients ( 16.67%) did not respond.
Question14: Patient’s perception of the Nurse.32 patients (76.19%) indicated level 1 (sympathetic).1 patient (2.38%) indicated level 4 (not very sympathetic).1 patient (2.38%) did not respond.
Question 15: Patient’s perception of the ultrasound receptionist.20 patients (47.62%) indicated level 1 (found the receptionist friendly).3 patients (7.14%) indicated level 3 (middle).
Question 12: Likert Scale to assess emotional state of the client when attending hospital (Level 1 = calm, Level 5 = very anxious)
4
6
14
6
12
0 2 4 6 8 10 12 14 16
Level one
Level two
Level three
Level four
Level five
Emot
iona
l sta
te a
s fe
lt by
the
Clie
nt.
Number of Clients.
8
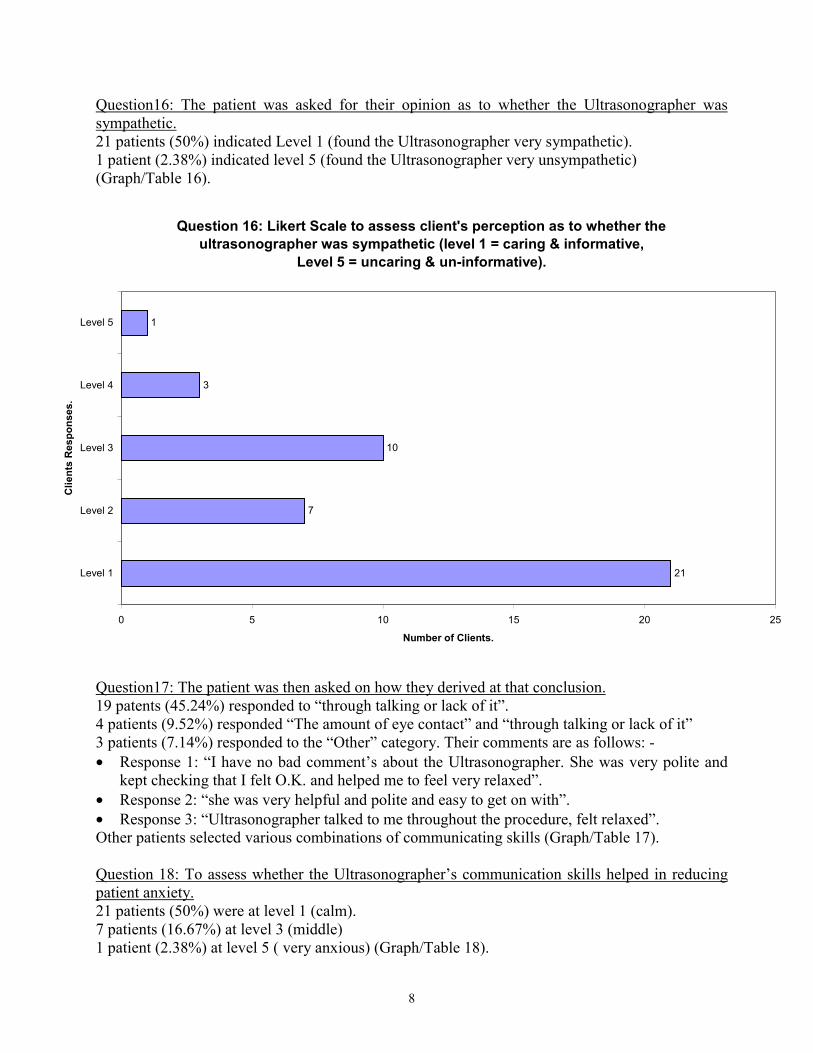
Question16: The patient was asked for their opinion as to whether the Ultrasonographer wassympathetic.21 patients (50%) indicated Level 1 (found the Ultrasonographer very sympathetic).1 patient (2.38%) indicated level 5 (found the Ultrasonographer very unsympathetic)(Graph/Table 16).
Question17: The patient was then asked on how they derived at that conclusion.19 patents (45.24%) responded to “through talking or lack of it”.4 patients (9.52%) responded “The amount of eye contact” and “through talking or lack of it”3 patients (7.14%) responded to the “Other” category. Their comments are as follows: -• Response 1: “I have no bad comment’s about the Ultrasonographer. She was very polite and
kept checking that I felt O.K. and helped me to feel very relaxed”.• Response 2: “she was very helpful and polite and easy to get on with”.• Response 3: “Ultrasonographer talked to me throughout the procedure, felt relaxed”.Other patients selected various combinations of communicating skills (Graph/Table 17).
Question 18: To assess whether the Ultrasonographer’s communication skills helped in reducingpatient anxiety.21 patients (50%) were at level 1 (calm).7 patients (16.67%) at level 3 (middle)1 patient (2.38%) at level 5 ( very anxious) (Graph/Table 18).
Question 16: Likert Scale to assess client's perception as to whether the ultrasonographer was sympathetic (level 1 = caring & informative,
Level 5 = uncaring & un-informative).
21
7
10
3
1
0 5 10 15 20 25
Level 1
Level 2
Level 3
Level 4
Level 5
Clie
nts
Res
pons
es.
Number of Clients.
9
Question 19: Would the patient like to have seen the scan being performed?32 patients (76.19%) did not wish to see the scan.8 patients (19.05%) did wish to see the scan.2 patients (4.76%) did not respond (Graph/Table 19).There were two comments.• Response 1: “Yes, did”.• Response 2: “No I was offered the chance but refused”.
Question 20: How does having a scan being performed, before an elective abortion makes theclient feel?The results indicate the following responses:3 patients (7.14%) indicated level 1 (calm during the scan).9 patients (21.43%) indicated level 4 (becoming increasingly anxious).7 patients (16.67%) indicated they were very anxious (see Graph/Table 20).
Question 21a: The patient was asked if they had any questions, were these answered satisfactorilyby the Ultrasonographer?32 patients (76.19%) were satisfied with their answers.3 patients (7.14%) were not satisfied with the response.7 patients (16.67%) did not respond.
Question 21b: The patient had an opportunity to comment on their response from Q21a.38 patients (90.48%) did not respond.2 patients (4.76%) didn’t ask any questions.There were 3 comments.• 1 patient (2.38%) commented as follows:“Asked for a photograph but it was explained to me that under the circumstances it was policy thatone couldn’t be given”• 1 patient (2.38%) responded by saying:“I asked if my dates were correct with those from the scan and was expecting to be told shecouldn’t tell me but she was very helpful”• 1 patient (2.38%) gave the following response:“had no need for questions as all had been answered in counselling”
Question 23 The patient had the opportunity to comment on their experience in the UltrasoundDepartment.11 patients (23.19%) found the experience very relaxing.13 patients (30.95%) found the experience relaxing.13 patients ( 30.95%) found the experience acceptable.5 patients (11.9%) did not respond.
Question 24a. The patient was asked whether we can improve the experience of their visit to theultrasound department.31 patients (73.81%) responded No.9 patients (21.43%) gave no response.1 patient (2.38%) responded Yes.
10
Question 24b. The patient was asked for their opinion on how we can improve the experience oftheir visit to the ultrasound department.39 patients (92.86%) did not respond.
There were 3 patients who gave the following responses:• Response 1: “Nurse didn’t know how to use the machine, said it was a new computer”.• Response 2: “Ask each person if they would like to see the scan as everyone is different.• Response 3: “I was nervous before attending my appointment, that I may be treated badly, and
judged. But during my appointments everyone that dealt with me were genuinely nice. Whichmade me feel a lot more comfortable”.
Question 25: The patient was asked for comments on how we could improve the experience in theultrasound department.32 patients (76.19%) did not respond.5 patients (11.90%) indicated No.2 patients (4.76%) indicated “No applicable”.
There were 3 comments.• Response 1: “Everyone as a whole has been wonderful”• Response 2: “I don’t think you should have a scan if you are terminating. It does not help”.• Response 3: “Keep up the good work”
11
Discussion
Discovery of an unwanted pregnancyFor too many patients the confirmation of an unwanted or unplanned for pregnancy can be seen asa negative life event. Each decision on what to do about pregnancy gives rise to different conflictsand choices to be made. Lazarus (1985) believes that this choice may have a major impact on herfuture personal development depending on how the choice is managed.He states that women have more favorable psychological outcomes since abortion has beinglegalized. Also he considers that we have moved away from the psychological scarring imposedby furtive or illegal abortion.
Legalized abortionAbortion has been legalized in England since 1967 in line with many western countries. Prior toand following legalization, it was available to certain restrictive groups of patients for medical andtherapeutic reasons. The grounds for abortion included if it was proven to be a risk to the mother’smental (Peppers, 1987) or physical health or in cases where major structural abnormalities weredetected e.g. anencephaly and spina bifida. It was also allowable for “mothers” who were exposedto environmental factors such as rubella. Since abortion has been legalized, the demand for thisservice has been steadily increasing. The present view is that abortion is available almost ondemand. This point is well illustrated in Graph 27 where locally one in four pregnancies isterminated.
What choices do the women have today?In simplified terms, the options for women are:(1) To continue pregnancy with all the financial and rearing responsibilities of a parent(2) Undergo an abortion and continue with their present lifestyle.(3) To continue with the pregnancy and at birth give the baby up for adoption.
Complications and choices for women before they attend clinic.Many women who have unprotected sexual intercourse have the added complications ofcontracting sexually transmitted diseases (Waterhouse, 1999). One of the respondents to question7 stated she had NSU (non-specific urethritis). Sexually transmitted diseases (STD) are on theincrease, NSU is believed to be one of them.The women who have unplanned sexual intercourse can have access to the “morning after pill”from their General Practitioners (GP), Family Planning Clinics (FPA) or even Accident andEmergency departments of many hospitals. Other women will present themselves when theysuspect a pregnancy, or they have missed a period.Many brands of pregnancy testing kits are available over the counter to confirm the client’ssuspicions.
12
ContraceptionThe response to question 5 indicated that 28 patients (67%) of requests for termination ofpregnancy are as a direct result of contraceptive failure. To reduce the number of MTOPs, there isa need for the prescribers of contraceptives to inform the patients in every day language on theavailability of contraception and their effectiveness in preventing pregnancy and STDs. There hasto be continuing advice and education on contraception from other areas rather than the standardGeneral Practitioners, Family Planning Association etc. For teenagers, Martin (1999) suggestsusing peers to educate their colleagues. This is the case for teenagers in the Bronx, America.
What stage does the woman present herself to clinic?Literature suggests that there are a small group of women who are late presenters to the unit. Thisgroup includes the very young teenagers or older women. The reason behind late presentation isthought to be due to either a lack of social support, or possibly their acknowledgement and desireto keep the pregnancy; a potential life growing inside them. At the same time external (possiblyfamily) pressures dictate otherwise (Peppers, 1987, Lazarus, 1985). Research has also shown thata small minority of women who appear to use this procedure as a means of birth control (Tentoni,1995).
Dilemmas the women have to face.Women are challenging male dominated views on the topic of termination. It has been recentlydocumented that women make their moral and ethical judgments differently to men. Wright(1991) is of the opinion that women base their judgement on their relationships with their partner,family and friends. Female therapists from the Stone Centre in Boston (Wright, 1991) call this“relational perspectives”. The client bases her judgement on how the chosen option would affecther relationships to those who are close to them. The outcome may be either harmony or conflict.If the client opts for total privacy because of either secrecy, or not having a person to confide; thismay lead them into isolation. The role of the Counsellor may be to direct the individual to a self-help group if they are unable to provide such support themselves.Although there is some discrepancy in the responses to question 6b and 7a, the survey shows thatone (2.38%) respondent did not confide in anyone. We can only speculate as to the reasons why.It could it be due to secrecy, emotional security or self-reliance on making a decision forthemselves. For making such a difficult decision, Gilligan, (1982) believes their personal valueswill be upheld.• Although societal values may have changed, there is still a stigma of being single and
pregnant.• Personal religious beliefs which are reinforced by their families and GPs who are unwilling to
support termination.• Family Pressures by imposing their wishes or possibly demands on the client.• Cultural: This may not be seen to be a barrier to the “white” patients but is a major hurdle for
single ethnic clients. The client is in a no-win situation because of the condition they findthemselves in. If they continue with their pregnancy, it would be dishonorable for herself andher family. At the same time it is dishonorable to have an intimate relationship outsidemarriage.
• Financial and Social support if the client decides to keep the baby. Allowing time for thepatient to reflect and seek advice from the health professionals who may be able to help them.
• The importance of “professionals” reserving their judgements and opinions when a request for

13
abortion is received. It isn’t just because of failed contraception, the research has highlightedother issues which contribute to the need for termination. The Abortion Act Compendium(1995) states that an opportunity is given to the clients to: -
“make a reasoned assessment of her own wishes and circumstances to obtain any advice she mayneed in reaching her own decision …and also to secure the necessary aftercare facilities”.
AttitudesThis aspect can be divided into three areas:• Their own beliefs, values and perception of morality.• Attitude of family, friends and society.• The attitude of the staff they come into contact with.(Gilligan, 1982).
Role of the CounsellorThe aim of counselling in these situations is to try to remove, or minimize the external pressuresfrom the client, who can then come to a decision. The counsellor helps by getting the woman tofocus on her present and deep-rooted feelings about the pregnancy. This is during a privateconsultation where family pressures have been removed. Irrespective of the age, a contract is madewith her and that what is discussed will be confidential. From Brien’s experience (1996) thisstatement can contribute towards the client becoming cathartic and allowing her to focus on herfeelings towards abortion and the implications of her choice. The counsellor does not influence theclient’s decision.
Counselling RelationshipThis is defined as a formal relationship between the client (who may be in a state of crisis) and thecounsellor (who has received specific training). The relationship between the Ultrasonographer,the client and her partner are important in how the service is perceived by the service user.
Counselling SkillsThese are “tools” developed by the Ultrasonographer, which can be used on formal or spontaneousbasis. Application includes reducing the anxiety levels client experiences in a hospital setting.(Smith, J & Smith A.P.M, 1995).
SupportResearch has shown that women who make a decision to terminate their pregnancy do so with alot of personal probing. The results show that 22 patients (52.38%) of the patients are from astable relationship. The availability of a supportive partner/relative/friend can help the patient tofocus on how her “pregnancy” will affect her as well as the relationships, which are close to her.Wright (1991) states that the decision of how to deal with an unplanned pregnancy will help thewoman to reflect and examine her relationships and financial support. The decision may confirmher self-independence and at the same time maybe in opposition to her support.
14
“A State of Crisis” for the patientWhen patients attend hospital, their anxiety levels increase (Smith, J & Smith A.P.M,1995) tosuch a degree that some of them experience physical symptoms (such as sweating and palpitationsAtwal, 1999). It must be acknowledged that it takes a lot of personal courage for a client to turn upin the ultrasound department, which confirms their pregnancy, a potential for life, which they havedecided to end.Their normal communications skills may be absent. During the short contact time with theUltrasonographer, some clients may wish to reply with closed answers. They avoid conversation,eye contact and gaze away as much as possible often preferring to turn their head away from theexamining Ultrasonographer.It may make the Ultrasonographer and the client feel that they are invading each other’s space.Even though the client has consented for the examination to proceed, physical touch during theexamination may be seen as unwelcome. To the inexperienced this may make both parties feeluncomfortable.
Practical Skills in the Ultrasound Department
There are many factors to reflect on when considering what skills the Ultrasonographer needs todevelop for helping MTOP clients. Areas to consider include the following:• The patient’s “maturity” as to how the Ultrasonographer approaches her during their short
contact.• Is the patient showing signs of underlying guilt and anger at ending the pregnancy?• Is the patient grieving?• Is the patient very matter of fact?• If they request to view their "live scan" during the examination, will the imaging reaffirm their
thoughts and feelings on the action they are about to take.
Discussion:Under normal circumstances (wanted pregnancies) the ultrasound monitor is positioned so that thepatient and the Ultrasonographer can view the examination together. If the mother requests, a printof the “baby” is given. If the MTOP patient requests, the monitor can be positioned in the sameway so that they can see the scan. Results show that 8 patients (19.05%) did wish to see the scanand probably requested to do so (Graph/Table19). To some the visual image can be upsetting andconfusing. Normally this would be considered a time of joy but the reality for this group ofpatients is that they are “ending the life of their baby”. It can be a very emotive time for the clientsand there are many opinions as to why the MTOP patients request (or do not) to see their scans: -1) Personal curiosity.2) Image of the fetus on the screen is seen as something, which is not real.3) Indecisiveness can lead to maternal-fetal bonding to occur and the patient may change her
mind about the abortion (Peppers, 1987).4) Viewing the examination can make the patient associate the experience with future unwanted
intrusive thoughts. The inevitable fate of the pregnancy leading to pain and death of a fetus canfurther increase the stress and anxiety. Literature suggests that intrusive experiences may be away for the subconscious to deal with the experience more positively so as to allow adjustmentin the long run (Slade et al 1998). The unwanted imagery can be related to Post TraumaticStress Disorder. The long-term outcome may lead to depression (Atwal, 1999).
15
5) Personal circumstances can dictate termination of even a wanted pregnancy. One of thepatients requested a print. Unfortunately on this occasion, due to policy unawareness her wishwasn’t full filled. This request may have been to help her with her thought process ofinevitability, acceptance and grieving. Although Slade et al (1998) states that the emotionaldistress is no greater than the community norms. The necessity of having to undergo a scan isseen to be a very anxious time for this group of ladies. Following the scan, there may be a needto allow the patient more space to acknowledge the feelings on their own.
Ultrasonographer’s practical helping skills.• A warm friendly greeting right from the beginning. Making the patient feel valued and that
you have time for them.• Psychoanalytical room setting is appropriate for this group. Comfortable room with sub-dued
lighting and privacy ensures the appropriate setting for sharing confidences (Smith, J & SmithA.P.M, 1995).
• The importance of listening to what the client is saying. This includes developing skills at ahigher level in receiving, de-coding and returning messages either verbally or non-verbally.
• To be sincere. It is important to give clear verbal and non-verbal signals to the client, whichcannot be mis-interpreted by the client.
• When greeting the patient, the Ultrasonographer’s body language and voice messages need tobe coherent. Nelson-Jones (1998) states that the voice needs to be at the correct level ofvolume, articulation, pitch, emphasis and rate.
• He also recommends that the Ultrasonographer’s (Counsellor’s) body posture should mirrorthat of the client. Unfortunately while the patient is being examined, this isn’t possible becausethe client is lying down. A sitting position at a similar height would be acceptable.
• To indicate interest in the patient, the Ultrasonographer has to rely on intermittent eye contactand gaze skills. Important facial messages are sent and received during these few moments.
• The response to question 19 indicated that 76.19% of the clients did not wish to see the scan. Itis also noted that during the examination a number of our women tend to turn their head awayfrom the Ultrasonographer. To ensure continuing communication during the examination, thepatient’s other senses such as hearing needs to be awakened by using the messages we send inour voices more effectively.
• Avoid generalizing and stereotyping clients. Their basic psychological and support needs willbe similar. Any personal barriers should be acknowledged and worked upon so as to removethem.
• Developing thinking and action skills to positively challenge any unreasonable behaviours anddemands (Nelson-Jones 1998).
• To have an open mind, avoiding tunnel vision and possible negativeness towards this group ofwomen.
The Patient’s Perception of the ServiceLiterature shows that the post abortion adjustment is based partially on the treatment the clientreceives (Lazarus, 1985). This is from the time she goes onto the MTOP unit, pregnant andfollowing abortion.Clients who see the service positively also evaluate the elective abortion in the same light. Thereverse is true where clients are unable to resolve their decision on abortion are also dissatisfiedwith the service that they have used.
16
To illustrate this point the following responses are taken from the questionnaire survey:Positive Perceptions• “1 was nervous before attending my appointment, that I may be treated badly, and judged. But
during my appointments everyone that dealt with me was genuinely nice. Which made me feela lot more comfortable”.
• “I have no bad comments about the Ultrasonographer. She was very polite and kept checkingthat I felt O.K. and helped me feel very relaxed”.
Negative Perceptions• “Nurse didn’t know how to use the machine, said it was a new computer”.• “I don’t think you should have a scan if you are terminating. It does not help”.In agreement with other literature, a sympathetic approach aids in reducing post abortiondissatisfaction and enhancing the overall effect of personal development from the abortion.
Ultrasound EnvironmentAt present the ultrasound examinations are performed in our main ultrasound / CT suite. Althoughdemand on the ultrasound department is high from all users from within and outside the agency,one separate session once a week is used for the MTOP clients. The aim is to provide asympathetic environment. Although we cannot control the work of the adjacent rooms, the contactwith “normal pregnancy” clients is minimized.This is seen as a vast improvement from the days of the conveyor belt system where patients withdiffering needs were in the same waiting area. This included normal pregnancies, the assistedreproduction clients as well as those requesting terminations.It was felt that we as Ultrasonographers need to ensure that the clients who attend the departmentfor a gestational scan, are treated with empathy and without judgement.In the final week of the data collection a second temporary ultrasound room was set up in the“Social Workers” area which is adjacent to the ultrasound department. The driving forces were thetwo bank holidays and additional demands on the service. It was visibly obvious that the patientswho attended this scanning session felt their psychological needs were being met.
Purpose of the scan.This is to confirm that a pregnancy is present and it is in the right place as well as an accurategestational age. This is a requirement as set aside in the Department of Health’s Abortion ActCompendium 1995.It is good practice to confirm a pregnancy with the following diagnostic tests:• Urine test on all patients of eight weeks or under.• Either a urine test or an ultrasound scan in patients of more than 8 weeks.
In our unit, routine scans are now requested on all patients attending the MTOP unit. Clinically ascan is more accurate method for confirming and providing an accurate gestational age of thepregnancy than a client’s last menstrual period (LMP). Over time we have had cases where:• Patient’s scan dates do not agreed with the LMP. This could be more or less than anticipated
gestational age. The client may have to reassess the situation.• There is no pregnancy. These clients are normally so relieved that they do not have to be the
“executioner”.• Multiple pregnancies diagnosed. This may cause additional dilemmas for the client. They may
re-evaluate and reassess their strategy. As one client said, “it was a hard decision to end one
17
pregnancy, but to end two is unthinkable”.• Pregnancy has failed to progress. These clients may experience mixed emotions, which may
include sadness, guilt, anger and possibly remorse.The clients’ anxiety may be further heightened by the impending visit to the ultrasounddepartment. They may even perceive this as a potential threat.
Case study:A client was referred to the MTOP unit through the normal channels. Following her scan it wasevident that she was around 24 weeks gestation, a point where a pregnancy can be “viable” andnot “early” as she had suspected. In this case a termination was refused. A clinical decision wasmade because of the limitations of the scan at this gestation to accurately give a gestational age.Allowing for a variation of +/- 10days, this meant that the pregnancy might actually be more thanthe 24 weeks stated. The Abortion Act Compendium categorically states:
“that no abortion should be carried out after the expiration of 24 weeks (168days) of gestation”.
Unfortunately the client found this totally unacceptable and demanded an abortion. In this case thestaff were unable to resolve the situation, and the patient was visibly upset when she left the clinic.
18
Conclusions
This project has highlighted the lack of specific research on anxiety levels for women having ascan prior to a termination of pregnancy.
Patient’s anxiety levels were found to have increased following scan (Graph 26 and 28). Researchhas shown that there is a real barrier to the patients’ having the scan as one of them hadcommented that “I don’t think you should have a scan if you are terminating. It does not help”.Unfortunately for providing an accurate dating of the pregnancy there is no alternative method atthe present. The majority of the patients (76.19%) did not want to see the scan. To address thisissue the Ultrasonographers should ask individual patients whether they wish to view the scan ornot during the examination.
The main reason given by patients for terminating their pregnancy was failed contraception. Otherreasons included physical abuse of one patient by her partner and abuse of drugs by another. Thestaff with whom this group of clients comes into contact with will need to be impartial, empatheticand non-judgmental. There is a need to provide “true counselling” rather than just impartinginformation prior to the scan. This approach would allow the patient to explore their thoughts andfeelings prior to undergoing an ultrasound examination.
One in four pregnancies are terminated (Graph27). Two-thirds of the women in the surveyindicated that their pregnancy was the result of a contraceptive failure. To reduce or eliminate thistrend, there needs to be a strategy, which focuses on peer and team approach towards educationand prevention of unwanted pregnancy.
The present view is that abortion is available “on demand” and the increasing acceptance of thisintervention by society devalues human life. There is a need to change the attitude of societytowards termination of pregnancy through education. Promotion of saying “No” is the easiest butunrealistic option. Contraception, infection control, education and advice should be made easilyavailable in more accessible areas other than the traditional health centres, family planning clinics,and chemists. “Drop-In” clinics in schools, places of work, places of leisure, nightclubs, towncentres or supermarkets seem to be attractive alternatives.
In conclusion there was a high level of satisfaction in the MTOP unit specialist nursing staff. Thepatients’ anxiety levels were reduced during their contact with them. The change in servicedelivery has helped in addressing some of the emotional needs of women who attend the MTOPUnit and the Ultrasound Department before ending their pregnancy.
19
Further Research.
Following an extensive literature search, there is a noticeable lack of specific knowledge in thefield of women having scans prior to the termination of unwanted pregnancies.There is a need for further research into the emotional distress and anxiety induced in femaleshaving a scan prior to a MTOP.Face to face interviews with patients before and following scan should be considered. Withfollow-ups at intervals of e.g. 2 weeks, 3 months and 12 months following termination.Research using more advanced anxiety measures for quantifying anxiety and distress would be ofvalue. These could include the following well-established measures: -1. Hospital Anxiety and Depression Scale.2. Positive and Negative Affect Scale.3. Impact of Event Scale.4. Satisfaction with Care.(Slade, et al 1998).
The patient’s anxiety and stress changes from believing that she was having a termination towhere the ultrasound results indicate a miscarriage should be explored.
The anxiety levels of patients who view their scan compared to those who do not should beexplored.
Studies to examine whether viewing the scan can help the patient to cope psychologically withhaving the termination in the long term should be carried out.
20
Recommendations
The increasing ease with which MTOP can be requested and performed does not appear toconsider the emotional implications of the intervention. It is worthwhile for the agency to explorea number options on how to manage the psychological needs of this group of women. There is aneed to give the patient a sense of meaning for what they have undergone clinically andpsychologically. The following issues are worth consideration:
Ultrasound Department.• Although Ultrasonographers do have good communication skills, there is room for further
development to a higher counselling level. This can be undertaken in the form of informal in-house training workshops on a regular basis exploring issues, which are relevant to this groupof patients. Clinical Psychologist or a Psychiatrist should lead the workshops. The workshopscan then be extended to other fields where communication and understanding behaviour is alsoan essential part of delivering the service.
• Ultrasonographers to develop helping skills (such as active listening skills) to a higher level.• Sufficient time to allow Ultrasonographers to undertake counselling prior to the patient having
a scan. Aspects may include:1. Helping patients to become more aware of their thoughts before, during and after theexamination.2. Helping the patient to relax through positive thought and actions.3. Relaxation statements which can help the patient to stay in control.4. To set up a scanning session in the MTOP unit where all women are in a continuingsympathetic, non-judgmental environment.5. The patient may need to validate their loss in the future. Taking an extra scan print and leavingthis in the patients notes. This can be retrieved at a later date if the patient requests. This may helpthem to come to terms with the pregnancy loss.6. It is noted that Ultrasonographers experience an increase in stress levels following a MTOPscanning session. Supervision on its own is felt to be insufficient. Other methods of stressmanagement need to be implemented.
Other Areas.• Should patients’ request, involvement of them in the planning and participation of the funeral
and service may be emotionally valuable. Many professionals and lay persons may disagreewith this hypocritical view, but Tentoni (1995) believes that this provision is of value to thepatient. Although this facility is available at the hospital, patients do not take up theopportunity. It could be due to lack of awareness by the patient. The availability of this serviceshould be highlighted on the MTOP unit.
• A sacred site within the MTOP unit for clients to visit because of the intense emotionalfeelings experienced by the client. Tentoni (1995) suggests that this will allow Gestaltdialogue with the fetus acknowledging their short but unforgettable relationship. A way ofsaying goodbye and validate the loss of the pregnancy.
• Setting up of a self-help group where patients can help each other through their experiences.• There is a need to collect management data on the number of patients who:(I) Fall pregnant soon after the elective abortion because there are unable to resolve theiremotions following termination and
21
(2) Who suffer from anxiety and depression following the termination. The provision of BriefTherapy to be made available to this group of women.• Improved contraceptive advice and education within the agency and the community.• Encourage multi-disciplinary team working to provide a seamless service.• Accept limitations of intervention when helping the clients to resolve their guilt.• Audit the service in 12 months time.
22
Bibliography.
Adler, NE, (1975). Emotional Responses of Women Following Therapeutic Abortion.American Journal Orthopsychiatric., volume 45(3), pages 446-454. April 1975.
Adler, NE; David HP et al (1992). Psychological Factors in Abortion. American Psychology,Volume 47, pages 1194-1204. 1992.
Atwal, BK (1999). Module 1 Essay: Crisis Intervention and Therapy. Edexel ProfessionalDevelopment Diploma in Counselling. North Lindsey College.
Bell, K, (1996). The establishment of a gynaecology assessment unit. Nursing Times, volume 922,Number 10. March 6, 1996.
Bewley, C (1993). The midwife’s role in pregnancy. Nursing Standard, volume 8, number 12. 8th
December 1993.
Brien, J, (1996). Finding out for themselves. Nursing Standard, Volume 10, Number 15, page 43.January 1996.
Brooks, C (1997). The importance of the group when teaching counselling skills in the breaking ofbad news. UKAS Reverberations, March 1997, pages 12-15.
Department of Health (1995). Abortion Act 1967. Key extracts from the Compendium ofGuidance on procedures for approval of Private Sector places for termination of pregnancy undersection 1(3) of the Abortion Act 1967, as amended.
Gilligan, C (1982). In a Different Voice. Published by Harvard University Press, Cambridge,Massachusetts, and London, England.
Green, V (1997). Communication and Counselling Skills training for Sonographers: An AcademicInstitution’s Perspective. UKAS Reverberations, March 1997, pages 10-12.
Kenyon, S, (1985?). No grave, no photograph, no baby.
Lazarus, A (1985). Psychiatric Sequelae of Legalised Elective First Trimester Abortion.Journal of Psychosomatic Obstetrics and Gynaecology, Volume 4, pages 141-150. 1985.
Martin, N, (19990. Why some mothers do have babies by chance. Newspaper Article: The DailyTelegraph, Wednesday, March 24,1999, page 11.
Nelson-Jones, R (1998). Practical Counselling & Helping Skills. Third Reprint. Published byCassell, London, England.
23
Peppers, LG (1987). Grief and Elective Abortion: Breaking The Emotional Bond.Journal Death & Dying, Volume 18, pages 1-12. 1987.
Slade, P., Heke, S, et al (1998). A comparison of medical and surgical termination of pregnancy:choice, emotional impact and satisfaction with care. British Journal of Obstetrics andGynaecology, volume 105, pages 1288-1295. December 1998.
Smith, J & Smith A.P.M, (1995). Obstetric Ultrasound: Psychological Dimensions.BMUS Bulletin, Volume 3, No. 4, pages 25-26. November 1995.
Tentoni, SC (1995). A Therapeutic Approach to Reduce Postabortion Grief in University Women.Journal of American College Health, Volume 44, Part 1, pages 35-37. 1995.
The College of Physicians & Surgeons of Manitoba (1998). Guidelines and Statements.Counselling and Assessment prior to Therapeutic Abortion. College on The Web,http:/www.umanitoba.ca/cgi-bin/colleges/cps/college.cgi/633.html
Waterhouse, R., Fraser, L (1999). Sex diseases soar among teenagers. Newspaper article: TheMail on Sunday, page 25, February 28th,1999.
Wright, J (1991). Dealing With Unplanned Pregnancy.The Canadian Nurse, pages 20-22. October 1991.
Zlotogoriski, Z., Tadmor, O et al (1996). The Effect Of The Amount Of Feedback On AnxietyLevels During Ultrasound Scanning. Clinical Ultrasound, Volume 24, pages 21-24. January 1996.