counties manukau district health board board meeting agenda · counties manukau district health...
TRANSCRIPT

Counties Manukau District Health Board Agenda
Counties Manukau District Health Board Board Meeting Agenda Wednesday, 15 June 2016 at 1.30 – 4.30pm, Room 101, Ko Awatea, Middlemore Hospital, Hospital Road, Otahuhu, Auckland Time Item
1.00 – 1.30pm Board Only Session
1. Welcome
1.30 – 1.35pm 2. Governance
2.1. Attendance & Apologies – Wendy Lai 2.2. Conflicts of Interest/Specific Interests 2.3. Confirmation of Public Minutes – 4 May 2016 2.4. Action Items Register
1.35 – 1.45pm 1.45 – 1.55pm 1.55 – 2.00pm
3. Strategy
3.1. Chair’s Report (Verbal Update) 3.2. Chief Executive’s Report
3.2.1. Health & Safety Quarterly Report (Bev Stone)
4. General Business
2.00 – 2.05pm 5. Resolution to Exclude the Public
2.05 – 2.10pm 2.10 – 2.15pm 2.15 – 2.45pm
2.45 – 3.05pm
6. Confidential
6.1. Confirmation of Confidential Minutes – 4 May 2016 6.2. Action Items Register 6.3. Maternity Review Panel Update (Prof Ron Paterson & Panel Members/Margie Apa
& Carmel Ellis) 6.4. System Level Measures/Quality Improvement Case Study Report – Dr Robin Gauld
& Dr Mataroria Lyndon
Afternoon Tea Break
3.10 – 3.20pm 3.20 – 3.40pm 3.40 – 4.00pm 4.00 – 4.10pm 4.10 – 4.20pm 4.20 – 4.25pm
4.25 – 4.30pm 4.30 – 4.35pm 4.35 – 4.45pm
6.5. Investor Confidence Rating – Verbal Update (Louise Zacest) 6.6. Draft Long Term Investment Plan (Marianne Scott) 6.7. Future Land Use for Manukau Site (Louise Zacest) 6.8. Botany Letter of Intent (Louise Zacest) 6.9. Healthy Together 2020 - Technology Update (Sarah Thirlwall) 6.10. Healthy Together 2020 – Technology – Clinical Portal Upgrade Regional Initiative
Business Case (Sarah Thirlwall/Phillip Balmer) 6.11. Extension of Blood Culture Supply Agreement (Phillip Balmer) 6.12. IS Projects Update (Leanne Elder) 6.13. Second Draft Pacific Health Plan 2016/17 (Margie Apa/Elizabeth Powell)
1

Counties Manukau District Health Board Agenda
4.45 – 4.55pm 4.55 – 5.00pm 5.00 – 5.05pm 5.05 – 5.10pm 5.10 – 5.15pm 5.15 – 5.20pm
6.14. Second Draft Asian Health Plan 2016/17 (Margie Apa/Marianne Scott) 6.15. Workforce Development – Tindall Foundation (Margie Apa) 6.16. HWNZ Health Workforce Workshop Verbal Update (Beth Bundy) 6.17. Confirmation of NRA Directors (Lee Mathias) 6.18. IHI Special General Meeting (Lee Mathias) 6.19. Updated Board & Board Committee Terms of Reference (Lee Mathias)
Next Meeting: 27 July 2016 Room 101, Ko Awatea, Middlemore Hospital, Otahuhu
2

Counties Manukau District Health Board Agenda 15 June 2016
Board Member Attendance Schedule 2016
Name
Jan 10 Feb 23 Mar 4 May 15 June 27 July 7 Sept 19 Oct 30 Nov
Lee Mathias (Chair)
No
Mee
ting
Wendy Lai (Deputy Chair)
Arthur Anae
Colleen Brown
Sandra Alofivae
Lyn Murphy
David Collings
*
Kathy Maxwell
George Ngatai
Dianne Glenn
Reece Autagavaia
* Attended part meeting only
3

Counties Manukau District Health Board Agenda 15 June 2016
BOARD MEMBERS’ DISCLOSURE OF INTERESTS
June 2016 Member Disclosure of Interest
Dr Lee Mathias, Chair • Chair, Health Promotion Agency
• Chairman, Unitec • Deputy Chair, Auckland District Health Board • Acting Chair, New Zealand Health Innovation Hub • Director, healthAlliance NZ Ltd • Director, New Zealand Health Partners Ltd • External Advisor, National Health Committee • Director, Pictor Limited • Director, John Seabrook Holdings Limited • MD, Lee Mathias Limited • Trustee, Lee Mathias Family Trust • Trustee, Awamoana Family Trust • Trustee, Mathias Martin Family Trust
Wendy Lai, Deputy Chair • Partner, Deloitte
• Board Member Te Papa Tongarewa, the Museum of New Zealand
• Chair, Ziera Shoes • Board Member, Avanti Finance
Arthur Anae
• Councillor, Auckland Council • Member, The John Walker ‘Find Your Field of
Dreams’
Colleen Brown • Chair, Disability Connect (Auckland Metropolitan Area)
• Member, Advisory Committee for Disability Programme Manukau Institute of Technology
• Member, NZ Down Syndrome Association • Husband, Determination Referee for Department of
Building and Housing • Chair, IIMuch Trust • Director, Charlie Starling Production Ltd • Member, Auckland Council Disability Advisory Panel • Member, NZ Disability Strategy Reference Group
4

Counties Manukau District Health Board Agenda 15 June 2016
Dr Lyn Murphy • Member, ACT NZ • Director, Bizness Synergy Training Ltd • Director, Synergex Holdings Ltd • Trustee, Synergex Trust • Member, International Society of
Pharmacoeconomics and Outcome Research (ISPOR NZ)
• Member, New Zealand Association of Clinical Research (NZACRes)
• Member, Franklin Local Board • Senior Lecturer, AUT University School of Inter
professional Health Studies
Sandra Alofivae
• Member, Fonua Ola Board • Board Member, Pasifika Futures Ltd • Director, Housing New Zealand • Member, Ministerial Advisory Council for Pacific
Island Affairs
David Collings
• Chair, Howick Local Board of Auckland Council • Member, Auckland Council Southern Initiative
Kathy Maxwell • Director, Kathy the Chemist Ltd
• Regional Pharmacy Advisory Group, Propharma (Pharmacy Retailing (NZ) Ltd)
• Editorial Advisory Board, New Zealand Formulary • Member, Pharmaceutical Society of NZ • Trustee, Maxwell Family Trust • Member, Manukau Locality Leadership Group,
CMDHB • Board Member, Pharmacy Guild of New Zealand
Dianne Glenn • Member, NZ Institute of Directors
• Member, District Licensing Committee of Auckland Council
• Life Member, Business and Professional Women Franklin
• Member, UN Women Aotearoa/NZ • President, Friends of Auckland Botanic Gardens and
Chair of the Friends Trust • Life Member, Ambury Park Centre for Riding
Therapy Inc. • Vice President, National Council of Women of New
Zealand • Justice of the Peace • Member, Pacific Women’s Watch (NZ) • Member, Auckland Disabled Women’s Group
5

Counties Manukau District Health Board Agenda 15 June 2016
George Ngatai • Chair, Safer Aotearoa Family Violence Prevention Network
• Director, Transitioning Out Aotearoa • Director, BDO Marketing • Board Member, Manurewa Marae • Conservation Volunteers New Zealand • Maori Gout Action Group • Nga Ngaru Rautahi o Aotearoa Board • Transitioning out Aotearoa provides services and
back office support to Huakina Development Trust and also provide GP Services to their people
• Chair, Restorative Practices NZ
Reece Autagavaia • Member, Pacific Lawyers’ Association • Member, Labour Party • Member, Auckland Council Pacific People’s Advisory
Panel • Member, Tangata o le Moana Steering Group • Employed by Tamaki Legal • Board Member, Governance Board, Fatugatiti Aoga
Amata Preschool • Trustee, Epiphany Pacific Trust
6

Counties Manukau District Health Board Agenda 15 June 2016
BOARD MEMBERS’ REGISTER OF DISCLOSURE OF SPECIFIC INTERESTS
Specific disclosures (to be regarded as having a specific interest in the following transactions) as at June 2016 Director having interest
Interest in Particulars of interest Disclosure date Board Action
David Collings Innovation Hub Mr David Collings has a conflict of interest in regard to ATEED (being a member of the Local Community Board, which is part of the Auckland Council) and will be involved in the Innovation Hub.
5 October 2011 The Board notes that Mr Collings has a conflict of interest in regard to the Innovation Hub. He may participate in the deliberations of the Board in relation to this matter because he is able to assist the Board with relevant information, but is not permitted to participate in decision making.
David Collings
Potential Botany Land Development
Mr Collings declared a specific interest in relation to the Potential Botany Land Development, being a member of the Howick Local Board.
4 September 2013 That Mr Collings’ specific interest be noted and that the Board agree that he may remain in the room and participate in any deliberations or decisions.
Wendy Lai
HBL – Food & Laundry & FPSC Programme
Ms Lai declared a specific interest in regard to Deloitte providing support to HBL in the food and laundry and FPSC Programme. Deloitte has mainly been providing Oracle implementation resources to FPSC. Ms Lai is not directly involved with this work.
12 February 2014 That Ms Lai’s specific interest be noted and that the Board agree that she may remain in the room and participate in any deliberations, but be excluded from any voting.
George Ngatai Community Services Pharmacy Funding Policy
Mr Ngatai declared a specific interest in terms of their GP Service being like to use a local Pharmacy.
13 August 2014 That Mr Ngatai’s specific interest be noted and that the Board agree that he may remain in the room and participate in any deliberations, but be excluded from any voting.
7

Counties Manukau District Health Board Agenda 15 June 2016
Wendy Lai HBL Business Cases Ms Lai declared a specific
interest in regard to Deloitte’s involvement with HBL on this work.
13 August 2014 That Ms Lai’s specific interest be noted and that she may not participate in either the deliberations or determination of the Board in relation to this matter and is asked to leave the room.
Wendy Lai Ko Awatea Panel Advisory Services
Ms Lai advised that Deloitte have been shortlisted to provide Panel Advisory Services to Ko Awatea. This work does not have any involvement with the APAC Business Case
5 November 2014 Noted. Ms Lai advised on the 3 December 2014 that Deloitte have now been selected to work with the Ko Awatea team to improve commercial awareness and increase income levels.
Lee Mathias Otahuhu Boundary Change The Chair noted her Specific Conflict of Interest, being Deputy Chair at ADHB.
25 March 2015
That Dr Mathias’ specific interest be noted and that the Board agree that she may remain in the room and participate in any deliberations, but be excluded from any voting.
Lee Mathias Northern Region Electronic Health Record (NEHR) Project & Regional Information Strategy (RIS 10-20) Refresh
The Chair declared her specific interest as a Director of HealthAlliance.
25 March 2015 That Dr Mathias’ specific interest be noted and that the Board agree that she may remain in the room and participate in any deliberations, but be excluded from any voting.
Wendy Lai
FPSC Ms Lai advised that Deloitte is involved with FPSC, but confirmed that she personally does not have any involvement.
6 May 2015 That Ms Lai’s specific interest be noted and that the Board agree that she may remain in the room and participate in any deliberations, but be excluded from any voting.
Wendy Lai
EPIC Ms Lai noted that a Deloitte colleague worked with EPIC in the US. Mr Pearson and Mrs Zacest have met with him for his independent expertise on EPIC.
6 May 2015 That Ms Lai’s specific interest be noted and that the Board agree that she may remain in the room and participate in any deliberations, but be excluded from any voting.
8

Counties Manukau District Health Board Agenda 15 June 2016
Wendy Lai Botany Land Discussions Ms Lai advised that Deloitte
has been appointed by the three parties involved in the Botany Land discussions (CMDHB, BUPA & East Health). She is not personally involved in this work.
17 June 2015 That Ms Lai’s specific interest be noted and that the Board agree that she may remain in the room and participate in any deliberations, but be excluded from any voting.
David Collings Fencing of Swimming Pools Legislation
Mr Collings advised that he is the Chair of the Howick Local Advisory Board Swimming Pool Fencing Exemption Committee.
9 September 2015 That Mr Collings’ specific interest be noted and that the Board agree that he may remain in the room and participate in any deliberations, but be excluded from any voting.
Lyn Murphy Fencing of Swimming Pools Legislation
Mrs Murphy advised that she is the Deputy Chair of the Swimming Pool Fencing Exemption Committee for Franklin Local Board.
9 September 2015 That Mrs Murphy’s specific interest be noted and that the Board agree that she may remain in the room and participate in any deliberations, but be excluded from any voting.
Lyn Murphy MIT Nursing Programme Report
Mrs Murphy is a Lecturer in the Faculty of Business & Information Technology at MIT.
9 September 2015 That Mrs Murphy’s specific interest be noted and that the Board agree that she may remain in the room and participate in any deliberations, but be excluded from any voting.
9

Counties Manukau District Health Board Agenda 15 June 2016
Minutes of Counties Manukau District Health Board Held on Wednesday, 4 May 2016 at 1.30 – 4.30pm Room 101, Ko Awatea, Middlemore Hospital, Hospital Road, Otahuhu, Auckland Present: Dr Lee Mathias (Chair), Mrs Dianne Glenn, Dr Lyn Murphy, Mrs Sandra Alofivae,
Mrs Kathy Maxwell, Mrs Colleen Brown, Ms Wendy Lai, Anae Arthur Anae, Mr George Ngatai
In attendance: Mr Geraint Martin (Chief Executive), Mr Ron Pearson (Deputy CEO), Mrs Lyn
Butler (Board Secretary) Apologies: Apulu Reece Autagavaia, Mr David Collings 1. Welcome
The Chair welcomed everyone to the meeting.
2. Governance 2.1 Attendance & Apologies
Noted.
2.2 Conflicts of Interest/Specific Interests Noted. The Chair advised that she is currently Acting Chair, NZHIH.
2.3 Confirmation of Public Minutes – 23 March 2016 Resolution That the public Minutes of the Board Meeting held on Wednesday, 23 March 2016, were taken as read and confirmed as a true and correct record. Moved: Dianne Glenn Seconded: Lyn Murphy Carried: Unanimously
2.4 Action Items Register None currently listed.
3. Strategy
3.1 Chair’s Report - verbal update (Lee Mathias) The Chair provided an update on progress on NZHIH and NZHP. PHARMAC announced today that they will receive at extra $39M over two years in this year’s budget.
10

Counties Manukau District Health Board Agenda 15 June 2016
3.2 Chief Executive’s Report (Geraint Martin) The report was taken as read. Mr Martin advised that the Annual Plan for 2016/17 is close to being finalised. The budget is showing the small surplus required, without any reduction in services. Savings need to be found before prioritisation, and ‘one offs’ have been reduced to achieve a system of sustainability. Mr David Lenihan, Director Healthy Together 2020 starts in his new role in early June, although he is already assisting on some projects, including the Investor Confidence Rating. A rebalance of portfolio of services will see some changes take place for Mr Phillip Balmer, Mr Benedict Hefford and Mrs Margie Apa. The SPMO will report to Mr David Lenihan, Mrs Apa will work on the Social Investment Board, and Ambulatory Care will report to Mr Hefford, which will help balance services between hospital and community. The management of Patient Care, Experience and Professional standards is being reviewed to ensure we are fit for purpose with the Transformation Strategy. The Terms of Reference will be added to the Diligent Resource Centre. Ms Alofivae asked if the Social Investment Board would provide updates to CPHAC. Mr Martin advised that he will be on the SIB Board, so would cover this off, and ensure a clear reporting path to the Board. Mrs Brown referred to the Deep Dive on Population Health, and the desire to improve peoples’ wellness and engage with people to be part of the solution. The Chair said this refers to early preventative issues, but has not taken the step before about what good health is. The Minister has approved funding for the NZHPA Blue Zone customisation, which is a national programme with standardised collateral based on evidence from the Blue Zone, which will be customised for NZ. Mrs Brown said that local communities have seen a large amount of people involved in their communities over many years, and there are often no outcomes or continuation of services. People need to be able to trust the services on offer, plus the services need to be more sophisticated. Mr Martin advised that this is the purpose of the SIB work, plus the Localities work already in place. Mr Ngatai agreed in that most people often have no experience in the communities they are trying to help. They need to have an indigenous lens rather than pakeha. Mr Anae asked where this work fits in with the Whanau Ora Programme. Mr Martin said that the Whanau Ora work was very small, with only approximately 400 people signed up, and subsequently had a low impact in the community. Mrs Alofivae said that she is on the Pasifika Future Board and over 3,000 are involved nationally, with over 1,000 families in Auckland. Resolution That the Chief Executive’s Report be received. Moved: Lee Mathias Seconded: Lyn Murphy Carried: Unanimously
11

Counties Manukau District Health Board Agenda 15 June 2016
4. General Business
5. Resolution to Exclude the Public
Resolution That in accordance with the provisions of Schedule 3, Clause 32 and Sections 6, 7 and 9 of the NZ Public Health & Disability Act 2000, that the public now be excluded from the meeting as detailed in the above paper. Moved: Colleen Brown Seconded: Dianne Glenn Carried: Unanimously
The meeting was re-opened to the public. The meeting closed at 4.10pm. The next meeting of the Board will be Wednesday, 15 June 2016 at Ko Awatea, Middlemore Hospital. The Minutes of the meeting of the Counties Manukau District Health Board of 4 May 2016 are approved. Signed as a true and correct record on 15 June 2016. Chair ……………………………… Dr Lee Mathias (Chair)
12
Counties Manukau District Health Board Agenda 15 June 2016
Counties Manukau District Health Board Action Items Register (Public)
DATE ITEM ACTION DUE DATE RESPONSIBILITY COMMENTS/UPDATES COMPLETE
4 May CE Report - The management of Patient Care, Experience
and Professional standards is being reviewed to ensure we are fit for purpose with the Transformation Strategy. The Terms of Reference will be added to the Diligent Resource Centre when available.
July Geraint Martin
13

Counties Manukau District Health Board Agenda 15 June 2016
Counties Manukau District Health Board Chief Executive’s Report
Recommendation It is recommended that the Board receive the Chief Executive’s Report. Prepared and submitted by: Geraint Martin, Chief Executive 1.0 Introduction
1.1 As routine, my report is set out in three sections: - Strategic – with a special focus on planning for 2016/17. - Operational – including the reports from the Director of Strategic Development,
Director of Corporate & Business Services and Director of Ko Awatea. - Compliance – included is an update on Health & Safety.
2.0 Strategic 2.1 Last month I reported on a Deep Dive on the key issues facing us in Population
Health. This month, I include one for Primary & Integrated Care. The second of our three key ‘battlefields’ is Healthy Together 2020.
2.2 It is important to note that David Lenihan, Director Healthy Together 2020 delivery is joining the DHB on the 13 June. This is a key appointment, which will see a significant quickening of the transformational agenda.
Over the last three months, we have been reviewing how well geared we are to deliver at pace. There are six special areas of focus: - The development of System Level Measures (repeated elsewhere on the
Agenda).
- The review of our operational management structure has proposed the transfer of Outpatient & Ambulatory Care to the Director Primary Health & Community Services. This is currently out to staff consultation.
- The current configuration of Patient Care & Professional Standards management
and leadership has been reviewed, and a report is currently awaited.
- The Strategic Project Management Office will transfer to the Director Healthy Together Delivery on his arrival.
- The Investor Confidence Rating work has proven exceptionally useful in
identifying where we as an organisation need to go from individually good to systematically great.
- Ensuring that the 2016-17 budget has focussed enough resources in the right
areas to ensure adequate capacity for change.
14

Counties Manukau District Health Board Agenda 15 June 2016
2.3 ELT recently considered progress with Integrated Care implementation. This
programme of work includes: • Localities and the development of clusters • A model of care for planned, proactive care (At Risk programme) • Community Integration Programme including reablement; integrated home based
support services; community central; and development of community hubs. • Enhanced Primary Care
Significant milestones have recently been reached within this programme including: Development of 11 clusters across the localities: Clinicians across the system including specialist, community based and primary care have identified specific opportunities to progress integration. This has resulted in this strategy moving to a further level of granularity – the development of clusters within each locality. There are 11 clusters now functioning across the four localities – providing a network of providers who work collaboratively to care for their enrolled population. These clusters span across PHO boundaries and enable strong working relationships between providers to be formed at a local level, including multi-disciplinary case conferencing to share learning and identifying how patients’ needs can be met by drawing on resources from across the health, social and voluntary sectors. Embedding an approach for planned, proactive care: We have developed an innovative approach to long term condition care, which recognises the complex health and social needs of our patients. Following the launch of the At Risk programme in July 2014, 20,119 patients have now benefited from the programme. These patients have a named care co-ordinator within their general practice; a common assessment; a summary of the primary care information available within the secondary care system; and a goal based electronic shared care plan shared by the patients with their multidisciplinary care team. Early outcome data for those patients enrolled in the programme is also encouraging, both at a system level and at a patient level. Patients enrolled in the programme are showing reduced utilisation of Emergency Care following enrolment in the At Risk programme, and similarly reduced levels of inpatient episodes.
15

Counties Manukau District Health Board Agenda 15 June 2016
We are currently working on a solution to enable NHI level data from primary, community and secondary data sources to be securely analysed in order to perform quality and population health monitoring. Until this solution is in place, we are currently unable to analyse the clinical outcome indicators for the programme at a district level. However, ProCare have performed some initial analysis for their practices within the region (c. 50% of Counties enrolled population) which indicates an overall improvement in glycaemic control across the district (2% improvement). However, for those diabetics enrolled in the ARI programme, there is a threefold improvement in glycaemic control (6% improvement) when compared to control groups from other regional DHBs. ProCare have also identified improvements in the patient level measures which indicates that patients feel more engaged, and have greater knowledge of their condition – supporting their journey to self management.
16

Counties Manukau District Health Board Agenda 15 June 2016
Within this model of care, a quality improvement initiative has been developed. As a result, all 99 practices operating the At Risk model of care have a quality improvement plan which they have developed as a practice and are implementing improvements to facilitate improved care planning for patients in the programme. The excellent engagement from Primary Care in implementing this model of care has identified the opportunities to expand this approach to other patient cohorts. Launch of the Enhanced Primary Care programme: Our Alliance has formed a collaborative between the DHB, our PHO partners and 11 general practices across the district to support practices to redesign their model of care to operate in a more integrated and interdisciplinary way. This collaborative has launched, with all 11 practices now working on identifying their vision for the change and currently analysing data regarding their enrolled population. Technology will be a key enabler for this new way of working - particularly in enabling improved access to primary and specialist care through virtual consultations; accessing a comprehensive patient record, across the system at point of care; and remote monitoring for patients. Business requirements for these elements have been gathered, and in conjunction with healthAlliance, a delivery plan is currently being developed. Implementation of our Community Health programme: The reablement pathway provides intense support of functional home based assistance and community-based rehabilitation for individuals with moderate to complex needs. Over 250 patients have been enrolled on the pathway – with 188 now transitioned to self-care. Feedback from both a community clinician and patient perspective is very positive with improvements in both quality of life and independence scores at completion.
Implementation of the Community Central service continues, which will provide a centralised intake and interdisciplinary triage, scheduling and rostering for our community teams. The demonstration version of this service is due to launch on 1 August 2016, and a procurement process has been initiated to secure a technology partner to provide a long term development of the service. Within this, our community staff are being mobility enabled – tablets have been provided to community based clinicians in the Locality Community Health teams with excellent feedback. This enables staff to communicate securely, complete progress notes at point of care, access Concerto based notes from previous visits and effectively plan their route to maximise patient contact time. All locality community Health staff will be mobility enabled by 31 July 2016. In additional to the work within Locality Community Health teams, planning is underway to develop six community hubs across the district by 2020. These hubs will be a magnet for services to enable a greater range and scope of services delivered closer to where people live. The Department of Medicine are contributing significantly to the planning for services which can be carried out within Community Hubs, with detailed planning now underway within Mangere.
17

Counties Manukau District Health Board Agenda 15 June 2016
Next steps The below visual outlines the roadmap for continued implementation of the integration agenda to support our goal of Healthy Together 2020. Key initiatives to progress over this time will include: • Outpatient redesign • Development of Community hubs • Urgent & unplanned care redesign • Embed clusters • Extension of community central • Development of a model of care for planned, proactive care for children
18

Counties Manukau District Health Board Agenda 15 June 2016
Functioning clusters
- Provision of primary care for an enrolled population independent of employer- Integrated model fo care- Improvement network- MDT case conferencing- Services organised & delivered on a cluster/locality basis e.g. urgent care, palliative care, minor surgery.
Scale up of Community Central
Child healthMental Health
Self managementTransparency of
quality indicators
Unplanned, urgent care redesign
Community Hubs Implementation
6 hubs across the district enabling a greater range and scope of services delivered closer to where people live
Sporadic clinical integration
e.g individual hospital based specialists, nurse specialists, GPs etc
MOVE TO SCALE UP AND SYSTEMATISE
Community Health Integration launched
- Community based staff support clusters- Reablement model of care launched- Increased transparency of clinical information & patient flow via Community Central- Increased focus on cluster level relationships and patient co-ordination within clusters
Integrated Mental Health & Addictions
- Teams of specialist services & NGO providers supporting general practice clusters
ARI model launched- Implementation of model of care for planned, proactive care for patients with LTCs (adult focus)- Flexible funding model for general practice- Electronic shared care planning tool implemented
Safety in Practice LaunchedQuality improvement
methodology developed an implemented in cohort of
practices increasing improvement capability
20,000 Days Campaign launchedImprovement programme to anticipate and prevent acute health problems, respond quickly and effectively in the community, and provide timely and safe care to people admitted to hospital.
Ambulatory Care Redesign
Localities launched - Local networks- Provider & community engagement- Planning & implementation based on ‘place’
Enhanced Primary Care launched
- Development of new model of care in general practice - Increased ability to respond to patient demand
New model of care for diabetes
Implementation of a diabetes care bundle
Manaaki Hauora Campaign launched
- Development of approaches for engaging patients with self-management support
Integrated Care 2020 Roadmap
Existing historical relationships
Informal networks increasingly forming based on common interests (e.g diabetes, complex social issues)
MDTs form & start of cluster development
Clear cluster based relationships across all localities
NETWORKS
20,000 patients
through ARI
18 community MDTs held per
month
7,921 views of summary
health records
781 ARI patients
graduated to self
management
11 clusters established Single point of
contract for all locality
community requests
50,000 patients supported to self manage 240,000 patients through ARI
11 clusters operating500 local pathways
10,000 pathway views per year50% capacity release within locality community
teams11,000 patients through reablement
70% of population belong to ‘Enhanced’ Practice30% of consultations in general practice are
virtual670 community staff mobility enabled10% fewer admissions than expected
10,000 hits on clinical
pathways site
602 secondary clinicians using
shared care
150 community
staff mobility enabled
2012 2014 2016 2017 2018 2020WE ARE HERE!
X virtual patient reviews
X mental health
patients shared with primary care
X DNS phone consults with
practice nurses
23,060 bed days saved
through 20,000 days
25,000 kids through
ManaKIdz X face to face
reviews between
specialist and primary care
53% reduction in rheumatic fever rates
250 patients through
reablement
19

Counties Manukau District Health Board Agenda 15 June 2016
3.0 Operational
Health Target Summary Target Current Results Status by 30
June 2016 Emergency Departments
95% of patients will be admitted, discharged, or transferred from an Emergency Department (ED) within six hours May result: 96%
ACHIEVE
Elective Surgery
Elective surgery will increase by an average of 4,000 discharger per year March result: 105% WIES: 97% Ministry agreed target of 95%
ACHIEVE
ESPI 2: 82 FSA breaches for March, expected to be slightly less for April. ESPI 5: 12 breaches for treatment in March, expected to be similar for April (Ministry data not released at time of reporting) ACTION: Detailed production planning underway, including opening theatres on Saturday to meet ESPI targets by June 2016.
Faster Cancer Treatment
85% of patients receive their first treatment within 62 days of being referred with a high suspicion of cancer April result: 80% (internal result) A 10% increase from March result. The increase is beginning to reflect improvements made two months prior due to the 62 day lead-in time. Retrospective reporting reflects work done up to 8 months ago given the 6 month reporting cycle. ACTION: Continue to micro-manage with weekly case reviews, tumour stream reporting, CanTrack system monitoring patient pathways, understanding patient DNAs and analysis of breaches.
ON COURSE
Immunisation
95% of eight month olds will have had their primary course of immunisation on time May result: 94% ACTION: 1% equals 20 extra babies to meet target, these babies are being targeted.
ON COURSE
Heart & Diabetes Checks*
90% of eligible population have had their CVD risk assessed in the last five years March result: 92%
ACHIEVE
Tobacco*
Primary 90% of enrolled patients who smoke and were seen by a health practitioner in general practice and were offered brief advice and support to quit smoking March result: 89% ACTION: Targeted support for lower performing PHOs.
ON COURSE
Secondary 95% of hospitalised patients who smoke and were seen by a health practitioner in a public hospital were offered brief advice and support to quit smoking May result: 96%
ACHIEVE
Maternity 90% of pregnant women how identify as smokers, at the time of confirmation of pregnancy in general prate or booking with a LMC is offered advice and support to quit smoking March result: 100%
ACHIEVE
ACHIEVE: Already meeting target / will meet target by 30 June 2016 ON COURSE: Includes actions to meet target; expected to meet target by 30 June 2016 *PHOs concentrate on quarterly reporting resulting in lower, inaccurate mid-quarter results. For this reason quarterly results are only provided.
20

Counties Manukau District Health Board Agenda 15 June 2016
4.0 Strategic Development
Deep Dive – Hazardous Use of Alcohol: Action Plan Strengthening our focus on reducing the burden of hazardous alcohol use and alcohol-related harm is one of the sub-population health goals that will contribute substantially to achieving the strategic goal of the ‘Healthy Together’, CM Health Strategic Plan: “Together, the Counties Manukau health system will work with others to achieve equity in key health indicators for Maaori, Pacific and communities with health disparities by 2020”. Hazardous use of alcohol is one of six recommended areas for focus and identification of key indicators to track progress towards health equity. As described in more detail in the accompanying Discussion Paper (Appendix 1), hazardous alcohol use and alcohol-related harm cause large health, social, and economic burdens in Counties Manukau. There is an inequitable burden of harm on Maaori, males, youth, and socio-economically deprived populations. CM district also has a high prevalence of hazardous drinking among working-aged adults. Harms from other’s drinking are not well described, however populations at risk are likely to be children and whaanau/families. There is clear evidence and direction about which strategies effectively prevent and reduce the harmful use of alcohol. A broad and comprehensive public health approach is required, which includes strategies such as increased alcohol price, restrictions on the physical availability of alcohol, drink-driving countermeasures, brief interventions with hazardous alcohol users, and treatment of drinkers with alcohol dependence. The figure below shows the pyramid of alcohol use problems, displayed against the prevention spectrum (on the right) and response to problems using the Screening, Brief Intervention, and Referral to treatment (SBIRT) model (also known to as ABC Alcohol Approach).
Figure 1: Alcohol use pyramid
1.6%
Dependence
Hazardous orharmful use
13% (~50,000 people)
Low risk use
Abstinence
Screening
Secondary prevention
Tertiary prevention
Primary prevention
Brief interventions
Treatment in primary care or referral for specialist treatment
~8,000 people (2% of adult CM population) accessed AOD or
CADS services in 2014
~50,000 people (13% of adult CM population) have
hazardous, harmful, or dependent alcohol patterns
Categories of alcohol misuse: Hazardous drinking is a pattern of alcohol use that increases the risk of harmful consequences for the user; hazardous drinkers will not usually be seeking treatment for an alcohol problem; AUDIT score 8-15. Harmful drinking is a pattern of alcohol use that is already causing damage to health; harmful drinkers may or may not be seeking treatment; AUDIT score 16-19. Dependent drinking is alcohol use with an
21

Counties Manukau District Health Board Agenda 15 June 2016
established moderate or severe level of dependence on alcohol; people usually have damage to their health and may seek treatment and help for the dependence itself, or associated health, interpersonal and social problems; AUDIT score 20-40.
ELT agreed an Alcohol Action Plan and a budget of $990,000 ($560,000 one-off implementation costs and $430,000 ongoing costs). The plan takes a primary prevention (i.e. prevention of problem before it develops) and secondary prevention (i.e. early detection of problem) approach. Implementation or further development (depending on the setting) of SBIRT is key element of the proposed plan. In the first year, it is proposed that the focus of SBIRT development be on three key health settings. In subsequent years, in a phased approach, SBIRT could be extended to other important settings, including antental care, secondary schools, and inpatient services (e.g. trauma services). The goal, focus areas, objectives and planned actions are summarised in Table 1. A more detailed discussion paper providing background can be found in Diligent Resource Centre. Table 1: Overview of Proposed Alcohol Action Plan Goal Together, the Counties Manukau health system will work with others to achieve
equity in hazardous alcohol use and alcohol-related harm for Maaori, Pacific and communities with health disparities by 2020.
Focus Areas 1. Pursuing equity in access to high quality and culturally-appropriate healthcare services, specifically:
a. Screening for hazardous alcohol use, brief intervention, and referral to treatment when indicated (SBIRT),
b. Diagnosis and treatment of alcohol-related conditions with adequate service volumes to meet the increased demand likely to be generated by systematic SBIRT.
2. Working with communities and intersectoral partners to influence the social determinants of hazardous drinking and alcohol-related harm.
Objectives To be achieved by 30th June 2017
1. In three key health settings (general practices, Middlemore Emergency Department, locality-based community providers):
i. Implement or further develop a systematic, sustainable, and equitable SBIRT system
ii. Build the capacity and capability of those working in these settings to be able to provide equitable access to high quality and culturally appropriate SBIRT.
iii. Develop a system for data collection, recording, and output of key indicators to monitor the SBIRT system.
2. Strengthen integration between SBIRT system and Mental Health & Addiction services, including Alcohol & Other Drug (AOD) providers.
3. Support and enable communities/groups to take actions on alcohol harm reduction.
4. Support and enable inter- and intra-sectoral collaborative work aimed at alcohol harm reduction.
SBIRT=Screening, Brief Intervention, and Referral to Treatment. Directorate Highlights There are 7 teams that provide “corporate services” and two direct patient support services (Maaori and Pacific cultural support) in the Strategic Development Directorate. Risk Management is reported through the Finance and Audit Committee. The table below summarises Directorate highlights as at end April. Highlights Strategic Planning • 2016/17 Second Draft Pacific and Asian Health Annual Plans submitted to Board 15 June for final
approval to publish. • Q3 report on 15/16 approved at ELT for submission to the Ministry of Health.
22

Counties Manukau District Health Board Agenda 15 June 2016
Maaori Health Development • Integrated Service Agreement (ISA) contracts are aligned to a robust Whaanau Ora Outcomes
Framework for implementation from 1 July. National Hauora Coalition is due to complete their contract by 30 June 2016. This will end any further work from NHC in Maaori provider services.
• Maaori Workforce Development: Strengthened regional commitment to Maaori workforce development has been supported by the Regional Clinical Leaders Group for implementation in 2016/17. Scholarship process implemented for 2016/17 and Cadet programme successfully implemented. A calendar of organisational events, seminars, symposiums and learning activity is in progress to expose the CM Health workforce to indigenous and Maaori health excellence. The Hui Kaikookiri (internal Maaori workforce network meeting) was held in April and focussed on the barriers and enablers to Maaori leadership development. The next suite of events is planned for Matariki (June).
• Manawhenua: The Letter of Agreement is with MWiTM for signing that will implement the agreed Board to Board work programme. This enables a joint approach and builds on the collaborative workshop implemented in 2015.
• Healthy Together 2020 Implementation: Two teams in the Maaori Health Development group will be under review during May – June: Maaori Workforce Development Team and Te Kaahui Ora to progress its translation to a Whaanau Ora service. Both changes in teams are to align the services to the Healthy Together 2020 strategy.
Pacific Health Development • 2016/17 Pacific Health Plan – this plan is being submitted to 15 June Board for approval to publish.
The plan describes activities that will be undertaken and measures we will use to show improvement in health outcomes for Pacific people living in Counties Manukau. In line with the Healthy Together 2020 Strategy and the goal of achieving health equity, the plan recommends priority action areas and activities for accelerating Pacific health gains and achieving health equity.
• Regional Pacific: Cook Islands – Partnering with MOH to deliver targeted development for radiology. Samoa – ILP discussions with Samoa completed by MFAT consultant in preparation for next 5 years. Activity Design Document will be completed by 31 May 2016 and contract in place by 1 July 2016. Kiribati – Further contract received from MFAT for Radiology support. Further programme of support unlikely to be tendered until September 2016. Niue - Proposal for MFAT on the Community Ambulance Programme - partnering with St John NZ submitted. Approved to seek funding by Niue parliament and communication with MFAT in place. Fiji - NZMAT response to TC Winston was very successful. 23 person clinical and support team were in Fiji for 3.5 weeks in total. Further programme support unlikely to be tendered until September 2016. MFAT – RFP for 5 other Pacific countries scheduled for September 2016.
• Healthy Together 2020 Implementation: The Fanau Ola team will be implementing a change to increase the clinical capability to enable a focus on high need and vulnerable fanau with complex health and social household issues. A Pacific Health Gain team will also be established with 2 FTEs including an analyst. This change is to be implemented from 1 July and completed by end of September. Both changes in teams are to align the services to the Healthy Together 2020 strategy.
Communications Highlights of campaigns in progress: • Suburban Newspapers promoting a smoke free campus for MSC and MMH has been extended
through to May. • New Hand Hygiene campaign for staff launched in March and will run through to May. • Communications in planning for following activities: New retail and food precinct at
Middlemore, ongoing promotion of Integrated Care, Enhanced Primary Care to reflect business case sign off,
• Healthy Together 2020: Technology – developing interim comms plan & project plan support. • Be Well this Winter – increased activity to promote alternative options to Emergency Care this
winter. • Social media: growth in followers and engagement across Healthy Together, corporate Facebook,
Twitter and LinkedIn - CEO Twitter now has 1,594 followers; Connect+ - now in digital format with 3,200+ readers.
23
Counties Manukau District Health Board Agenda 15 June 2016
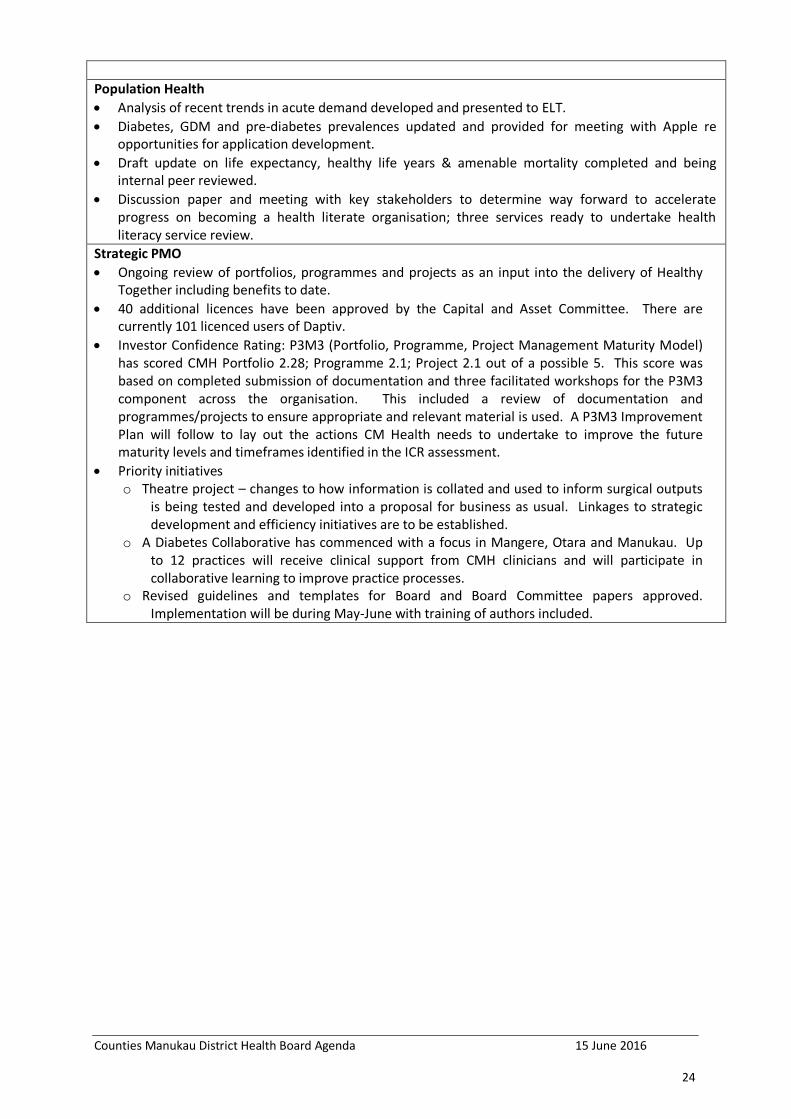
Population Health • Analysis of recent trends in acute demand developed and presented to ELT. • Diabetes, GDM and pre-diabetes prevalences updated and provided for meeting with Apple re
opportunities for application development. • Draft update on life expectancy, healthy life years & amenable mortality completed and being
internal peer reviewed. • Discussion paper and meeting with key stakeholders to determine way forward to accelerate
progress on becoming a health literate organisation; three services ready to undertake health literacy service review.
Strategic PMO • Ongoing review of portfolios, programmes and projects as an input into the delivery of Healthy
Together including benefits to date. • 40 additional licences have been approved by the Capital and Asset Committee. There are
currently 101 licenced users of Daptiv. • Investor Confidence Rating: P3M3 (Portfolio, Programme, Project Management Maturity Model)
has scored CMH Portfolio 2.28; Programme 2.1; Project 2.1 out of a possible 5. This score was based on completed submission of documentation and three facilitated workshops for the P3M3 component across the organisation. This included a review of documentation and programmes/projects to ensure appropriate and relevant material is used. A P3M3 Improvement Plan will follow to lay out the actions CM Health needs to undertake to improve the future maturity levels and timeframes identified in the ICR assessment.
• Priority initiatives o Theatre project – changes to how information is collated and used to inform surgical outputs
is being tested and developed into a proposal for business as usual. Linkages to strategic development and efficiency initiatives are to be established.
o A Diabetes Collaborative has commenced with a focus in Mangere, Otara and Manukau. Up to 12 practices will receive clinical support from CMH clinicians and will participate in collaborative learning to improve practice processes.
o Revised guidelines and templates for Board and Board Committee papers approved. Implementation will be during May-June with training of authors included.
24

Counties Manukau District Health Board Agenda 15 June 2016
5.0 Finance
Key Issues (April): 1. Monthly results continues the very tight pattern of the past, but we remain
marginally ahead of budget overall with no new material concerns arising or evident currently. However, the level of “one off” benefits is very high relative to the underlying operational performance.
2. Key operational issues are primarily hospital based. Despite a very mild entry towards winter, hospital attendances are at all-time highs for this time of the year with multiple “Dot” (i.e. well in excess of 100% bed capacity) days. Being well managed by the team, but causing increasing stress as this continues. Elective WIES numbers remain behind budget despite being well over discharge budget levels. A presentation from Phillip Balmer was presented to the Audit, Risk and Finance Committee reflecting the agreed plan to correct this by year end. Note, nearly 40% of the shortfall is generated by the national change in WIES calculation which has been accepted by MoH. The balance, however, will be recovered primarily through third party provisions contracts now being enacted.
3. Forecast year end position reaffirmed at the budget level. While it has been stated previously many times, the operating position remains extremely tight requiring intense management on all fronts. This tightening position is well reflected already in the worsening health sector position, particularly the hospital arms, which suggest an underlying structural funding problem.
4. Steady, but very positive progress, towards breakeven has been made on the Annual Plan/Budget 16/17. This is now achieved, but has required and received enormous organisation wide commitment. The next challenge is now identifying further savings to fund implementation of key additional priority initiatives. Approximately $10M is sought, on top of the significant money required for other priority initiatives that have already been approved and occurring currently.
5. Current year capital budget is being finalised. Still outstanding is regional discussion/resolution of hA IT capital funding both in terms of core infrastructure replacement/upgrade and new investment. The greater challenge is the consequent related higher depreciation and operating costs against continuing under investment and the consequences of such.
6. Huge effort organisation wide is being put into the initial Treasury Investor Confidence Rating (ICR) requirement, given both its accepted process improvement, but equally the critical impact the rating will have on the DHB’s future flexibility around freedom to operate both from a capital investment and operating perspective. Despite CMDHB’s generally high Treasury and National reputation around this, the new requirements are a significant step up on existing health sector standards, particularly around very much more formalised, documented processes than currently exist. Very positive, supportive and helpful meetings have been held recently with Treasury to assist us, but are clear and Treasury re-affirmed this, that it is likely to be a transition process to optimise rating levels given the complexities of health vs. say the IRD. Louise Zacest will update the Board separately on progress to date.
25

Counties Manukau District Health Board Agenda 15 June 2016
Of more immediate concern is the indication by Treasury of an imminent change in Debt to Equity policy requirement. Ron Pearson is now on the MoH Technical Group covering this and will update the Board regularly. This needs much more discussion as the potential impact on the State Sector and Health in particular, without permanent compensating changes to our capital structural flexibility could be enormously costly.
7. Good progress being made by Kerry Bakkerus, our new Risk Manager. She will be reviewing Facilities Risk Management soon. No concerns here as they have well proven successful processes, but important to understand and review given importance of the Mental Health rebuild and other Facilities projects such as Laboratories relocation.
26

Counties Manukau District Health Board Agenda 15 June 2016
SECTOR FINANCIAL POSITION at March 2016 The Sector Forecast Year end position continues to deteriorate as the Year to date result slips particularly in Provider arms. Note the rate of deterioration in the Provider Arms is now significantly greater than the offsetting Funder under spending. The last three months remaining in this year are, based on the results below, going to be a challenge for all DHBs.
Sector Loss Statement Sector CMDHB $m Actual Budget Var %Var Var % Var
Total Revenue 11,150 11,081 69 0.6 % 0.2 -
Personnel 4,223.0 4,201.0 (22.0) (0.5)% 2.0 0.4 % Outsourced Personnel 129.0 86.0 (43.0) (50.0)% (6.7) 100.3 % Total Personnel 1 4,352.0 4,287.0 (65.0) (1.5)% (4.7) (1.0)% Outsourced Services 325.0 313.0 (12.0) (3.8)% (0.6) (1.4)% Clinical Supplies 2 1,006.0 981.0 (25.0) (2.5)% (3.4) (3.6)% Infrastructure/ Other Suppliers 1,011.0 1,015.0 4.0 0.4 % 0.3 0.3 % Total Operating Costs 6,694.0 6,596.0 (98.0) (1.5)% (8.4) (1.2)% Personal Health 3,060.0 3,054.0 (6.0) (0.2)% 4.2 1.1 % Mental Health 329.0 341.0 12.0 3.5 % 6.1 11.1 % Public Health 19.0 19.0 - - 0.3 (1.9)% Disability Support Services 1,077.0 1,080.0 3.0 0.3 % (1.7) 17.5 % Maori Health 32.0 34.0 2.0 5.9 % - 3.3 % Total Payments to Other Providers 4,517.0 4,528.0 11.0 0.2 % 8.9 1.6 % Total Expenditure 11,211.0 11,124.0 (87.0) (0.8)% 0.5 - Net Result (61.0) (43.0) (18.0) (41.9)% 0.7 28.4 %
1. Total Personnel
Var. $m YTD
March
Var. $m YTD Feb
Change 2. Clinical Supplies
Var. $m YTD
March
Var. $m YTD Feb
Change
Bay of Plenty $(8.9) $(7.5) $(1.4) Auckland $(4.3) $(2.4) $(1.9) Canterbury $(7.3) $ 0.1 $(7.4) Capital and
Coast $(7.7) $(6.0) $(1.7)
Northland $(6.3) $(4.9) $(1.4) Waitemata $(6.0) $(5.1) $(0.9) Waitemata $(8.3) $(6.4) $(1.9)
27

Counties Manukau District Health Board Agenda 15 June 2016
Sector Performance By DHB YTD Full Year
Actual Budget Variance Forecast at Mar
Variance to budget
Budget (with
$25m)*
Auckland DHB 1,722 1,489 234 2,398 19 2,379 Counties Manukau DHB 3,069 2,428 641 2,741 39 2,702 Northland DHB (997) 1,776 (2,773) 255 (869) 1,124 Waitemata DHB (937) (1,584) 647 4,395 1,584 2,811 Northern Region Total 2,857 4,109 (1,251) 9,789 773 9,016 Bay of Plenty DHB (1,150) (1,136) (14) 1,388 - 1,388 Lakes DHB (1,538) 374 (1,912) (2,128) (2,747) 619 Tairawhiti DHB (2,496) 488 (2,984) (1,176) (1,492) 316 Taranaki DHB (2,512) (1,852) (660) (3,580) (4,317) 737 Waikato DHB (12,023) (10,908) (1,115) 2,226 - 2,226 Midland Region Total (19,720) (13,034) (6,686) (3,270) (8,556) 5,286
Capital & Coast DHB (9,556) (1,562) (7,994) (10,552) (11,992) 1,440 Hawke’s Bay DHB (4,111) (4,299) 187 3,990 - 3,990 Hutt Valley DHB (4,628) (4,906) 278 (7,750) (1,025) (6,725) MidCentral DHB (4,246) 1,383 (5,629) (2,011) (4,121) 2,110 Wairarapa DHB (1,480) (2,324) 845 (3,593) (1,633) (1,960) Whanganui DHB (466) (248) (218) (498) (498) - Central Region Total (24,487) (11,957) (12,531) (20,414) (19,270) (1,144) Canterbury DHB (2,676) (2,228) (448) (53) (53) - Nelson Marlborough DHB 2,042 4,045 (2,003) 1,500 (2,356) 3,856 South Canterbury DHB 605 354 251 430 2 428 Southern DHB (18,159) (23,957) 5,798 (34,372) 1,583 (35,955) West Coast DHB (983) (825) (158) (991) (113) (878) Southern Region Total (19,171) (22,611) 3,440 (33,486) (937) (32,549)
All DHBs (60,521) (43,493) (17,028) (47,381) (27,990) (19,391)
* This refers to MOH additional funding of $25m to the Sector which is required to “pass through” to the net result.
28
Counties Manukau District Health Board Agenda 15 June 2016
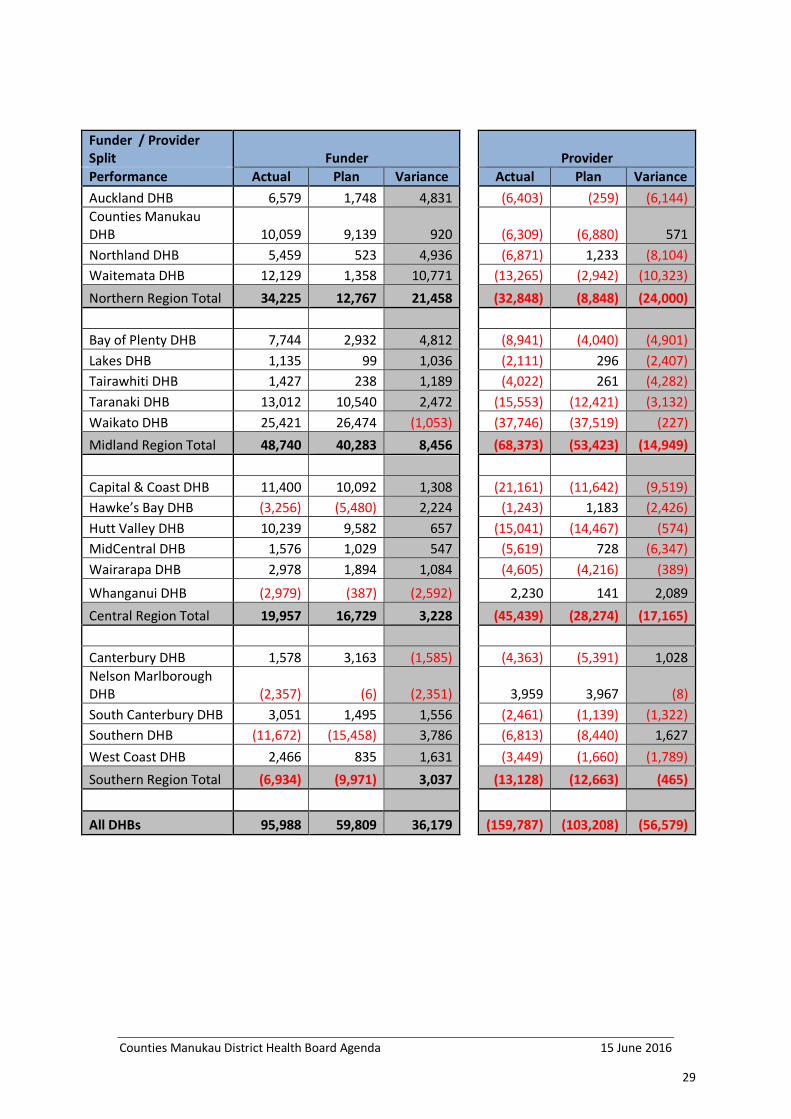
Funder / Provider Split Funder
Provider
Performance Actual Plan Variance
Actual Plan Variance Auckland DHB 6,579 1,748 4,831
(6,403) (259) (6,144)
Counties Manukau DHB 10,059 9,139 920
(6,309) (6,880) 571
Northland DHB 5,459 523 4,936
(6,871) 1,233 (8,104) Waitemata DHB 12,129 1,358 10,771
(13,265) (2,942) (10,323)
Northern Region Total 34,225 12,767 21,458
(32,848) (8,848) (24,000)
Bay of Plenty DHB 7,744 2,932 4,812
(8,941) (4,040) (4,901) Lakes DHB 1,135 99 1,036
(2,111) 296 (2,407)
Tairawhiti DHB 1,427 238 1,189
(4,022) 261 (4,282) Taranaki DHB 13,012 10,540 2,472
(15,553) (12,421) (3,132)
Waikato DHB 25,421 26,474 (1,053)
(37,746) (37,519) (227) Midland Region Total 48,740 40,283 8,456
(68,373) (53,423) (14,949)
Capital & Coast DHB 11,400 10,092 1,308
(21,161) (11,642) (9,519)
Hawke’s Bay DHB (3,256) (5,480) 2,224
(1,243) 1,183 (2,426) Hutt Valley DHB 10,239 9,582 657
(15,041) (14,467) (574)
MidCentral DHB 1,576 1,029 547
(5,619) 728 (6,347) Wairarapa DHB 2,978 1,894 1,084
(4,605) (4,216) (389)
Whanganui DHB (2,979) (387) (2,592)
2,230 141 2,089 Central Region Total 19,957 16,729 3,228
(45,439) (28,274) (17,165)
Canterbury DHB 1,578 3,163 (1,585)
(4,363) (5,391) 1,028
Nelson Marlborough DHB (2,357) (6) (2,351)
3,959 3,967 (8)
South Canterbury DHB 3,051 1,495 1,556
(2,461) (1,139) (1,322) Southern DHB (11,672) (15,458) 3,786
(6,813) (8,440) 1,627
West Coast DHB 2,466 835 1,631
(3,449) (1,660) (1,789) Southern Region Total (6,934) (9,971) 3,037
(13,128) (12,663) (465)
All DHBs 95,988 59,809 36,179
(159,787) (103,208) (56,579)
29

Counties Manukau District Health Board Agenda 15 June 2016
FINANCIAL POSITION at April 2016 Statement of Performance by Operating Arm
Month April 2016
Net Result YTD April 2016
Full year
Act Var. $000 Act Bud Var. st year Bud orecast
2,097 2,121 (24) Hospital Provider 24,847 25,253 (406) 13,781 10,744 10,744
(1,977) (2,001) 24 Integrated Care (20,076) (20,615) 539 (7,428) (9,665) (9,665)
(1,394) (1,226) (168) Ko Awatea (12,354) (12,624) 270 (10,772) (13,500) (13,500)
(1,274) (1,106) (168) Provider (7,583) (7,986) 403 (4,419) (12,421) (12,421)
1,533 1,016 517 Funder 11,592 10,155 1,437 8,467 14,893 15,593
(299) 21 (320) Governance (980) 190 (1,170) (2,566) 230 (470
(40) (69) 29 Surplus (deficit) 3,029 2,359 670 1,482 2,702 2,702
30

Counties Manukau District Health Board Agenda 15 June 2016
Volume Summary April 2016 Total WIES
Month Year to date Act Bud Var. % Last.
Yr. Act Bud Var. % Last. Yr.
5,543 5,605 (62) (1.1)% 5,548 Acute 58,451 56,626 1,825 3.2% 56,784
1,345 1,530 (185) (12.1)% 1,594 Elective 13,797 14,914 (1,117) (7.5)% 15,343
6,888 7,135 (247) (3.5)% 7,142 Total 72,248 71,539 708 1.0% 72,126
Counties DHB of Domicile elective discharges As at 31 March 2016, the achieved results were (April results not yet confirmed by MOH): • 105.1% of the Health Target for Elective Discharges • 97.1% of the target for Elective WIES • Third Party contracts /outsourcing committed to achieving Elective WIES targets by June 2016 This will be discussed more fully at the next HAC meeting.
Month
Act Last Yr. Var. %
8,675 8,204 471 5.7%
1,628 2,126 (498) (23.4)%
10,303 10,330 (27) (0.3)%
0.67 0.69 (0.02)
* The drop between years is caused by the change in Medical Electives, which have moved from elective inpatients to outpatients. Hence a drop in volumes and an increase in Average Length of Stay - these very short stay cases have been removed, so the remaining elective volumes have a (relatively) long length of stay
Volumes Other
Month Year to date
Act Last Yr. Var. % Act Last Yr. Var. %
594 600 (6) (1.0)% Birth Numbers 6,017 6,065 (48) (0.8)%
9,019 8,656 363 4.2% ED Volumes 95,799 91,225 4,574 5.0%
Data not available Renal Dialysis Data not available
52,656 50,674 1,982 3.9% Outpatient Summary 542,966 548,721 (5,755) (1.0)%
2.9 2.6 (0.3) (11.5)% ALOS 2.8 2.6 (0.2) (7.7)%
31
Counties Manukau District Health Board Agenda 15 June 2016
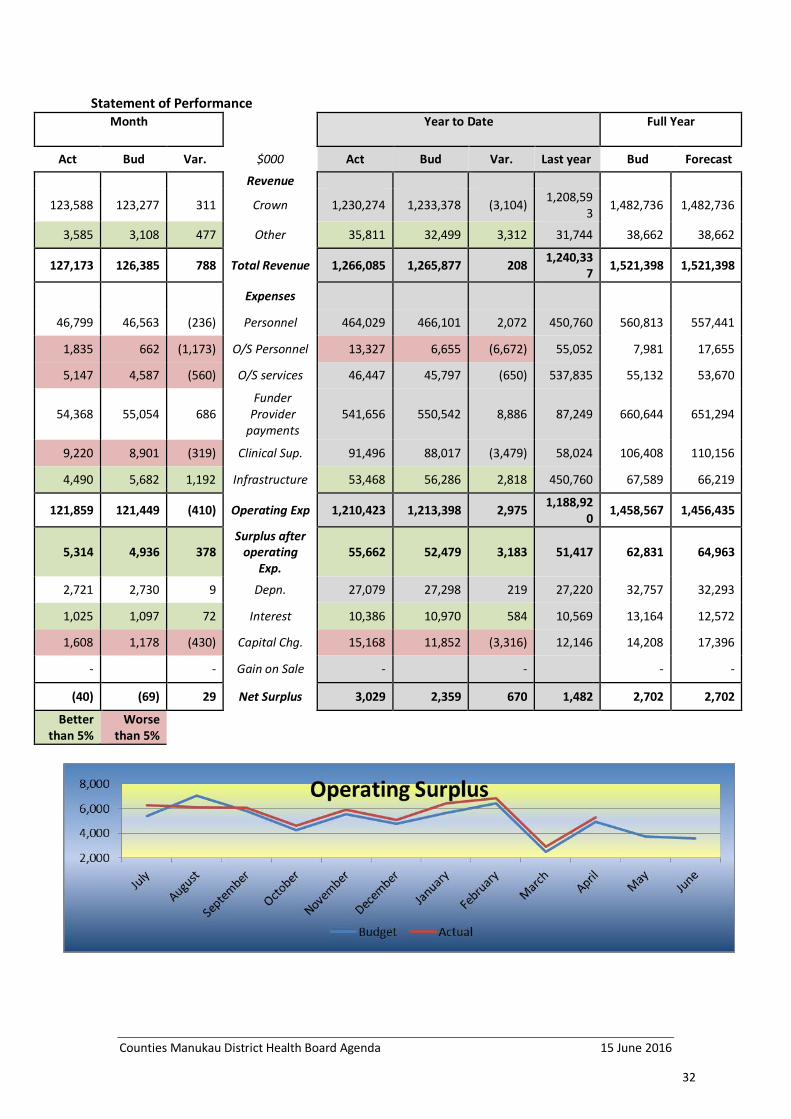
Statement of Performance Month
Year to Date
Full Year
Act Bud Var. $000 Act Bud Var. Last year Bud Forecast
Revenue
123,588 123,277 311 Crown 1,230,274 1,233,378 (3,104) 1,208,593 1,482,736 1,482,736
3,585 3,108 477 Other 35,811 32,499 3,312 31,744 38,662 38,662
127,173 126,385 788 Total Revenue 1,266,085 1,265,877 208 1,240,337 1,521,398 1,521,398
Expenses
46,799 46,563 (236) Personnel 464,029 466,101 2,072 450,760 560,813 557,441
1,835 662 (1,173) O/S Personnel 13,327 6,655 (6,672) 55,052 7,981 17,655
5,147 4,587 (560) O/S services 46,447 45,797 (650) 537,835 55,132 53,670
54,368 55,054 686 Funder
Provider payments
541,656 550,542 8,886 87,249 660,644 651,294
9,220 8,901 (319) Clinical Sup. 91,496 88,017 (3,479) 58,024 106,408 110,156
4,490 5,682 1,192 Infrastructure 53,468 56,286 2,818 450,760 67,589 66,219
121,859 121,449 (410) Operating Exp 1,210,423 1,213,398 2,975 1,188,920 1,458,567 1,456,435
5,314 4,936 378 Surplus after
operating Exp.
55,662 52,479 3,183 51,417 62,831 64,963
2,721 2,730 9 Depn. 27,079 27,298 219 27,220 32,757 32,293
1,025 1,097 72 Interest 10,386 10,970 584 10,569 13,164 12,572
1,608 1,178 (430) Capital Chg. 15,168 11,852 (3,316) 12,146 14,208 17,396
- - Gain on Sale - - - -
(40) (69) 29 Net Surplus 3,029 2,359 670 1,482 2,702 2,702
Better than 5%
Worse than 5%
32

Counties Manukau District Health Board Agenda 15 June 2016
Revenue
Month YTD Full Yr.
Act Bud Var. $000 Act Bud Var. Bud
70,107 69,211 896 Provider 701,815 694,135 7,680 832,606
119,042 119,106 (64) Funder 1,185,709 1,191,060 (5,351) 1,431,972
(63,141) (63,036) (105) Elimination (632,461) (630,363) (2,098) (756,435) 1,165 1,104 61 Governance 11,022 11,045 (23) 13,255
127,173 126,385 788 Total 1,266,085 1,265,877 208 1,521,398 Provider: Favourable for the month of April. The main drivers for the current month’s variance are: • Government Revenue; MoH revenue compensation for capital cost increase (offset by capital cost); ACC
arrears initiative; CTA revenue delay in invoicing; funded gastro procedures. • Patient/Consumer Sourced; Tahitian Burns, Non-resident unfavourable billings (offset by bad debts);
Patient co-payments. • Other Income; Interest received; Donation revenue, training course fees. • Funder Payments (internal transfers) for contracts outside base funding. i.e.: 20k days and localities.
Staff Costs (including Outsourced)
Month
YTD Full Yr.
Act Bud Var. $000 Act Bud Var. Bud 47,714 46,461 (1,253) Provider 469,308 465,116 (4,192) 559,626
920 764 (156) Governance 8,048 7,640 (408) 9,168 48,634 47,225 (1,409) Total 477,356 472,756 (4,600) 568,794
14,776 14,911 135 Medical 146,151 148,504 2,353 179,090
717 371 (346) Outsourced 7,125 3,710 (3,415) 4,452
15,493 15,282 (211) Total 153,276 152,214 (1,062) 183,542
17,283 17,342 59 Nursing 173,307 172,380 (927) 207,204
490 46 (444) Outsourced 2,693 458 (2,235) 550
17,773 17,388 (385) Total 176,000 172,838 (3,162) 207,754
6,558 6,733 175 Allied Health 65,549 68,063 2,514 81,684
8 32 24 Outsourced 282 316 34 380
6,566 6,765 199 Total 65,831 68,379 2,548 82,064
2,212 1,913 (299) Support Personnel 21,774 19,996 (1,778) 24,086
34 27 (7) Outsourced 357 270 (87) 324
2,246 1,940 (306) Total 22,131 20,266 (1,865) 24,410
5,970 5,664 (306) Management Admin 57,248 57,158 (90) 68,749
586 186 (400) Outsourced 2,870 1,901 (969) 2,275
33

Counties Manukau District Health Board Agenda 15 June 2016
6,556 5,850 (706) Total 60,118 59,059 (1,059) 71,024
46,799 46,563 (236) Internal 464,029 466,101 2,072 560,813
1,835 662 (1,173) Outsourced 13,327 6,655 (6,672) 7,981
48,634 47,225 (1,409) Total 477,356 472,756 (4,600) 568,794
Personnel costs are unfavourable for the month reflecting a leave revaluation provision as well as higher clinical demand in cleaning and orderly services (discharge lounge, ICU, SAU), offset by vacancies mainly in the Medical, Nursing and Allied Health Group’s . A level of vacancies exist across the organisation in all personnel categories (including Allied Health) and are partially covered by bureau, overtime and casual staff (see outsourced costs above). The favourable effect of the April school holidays (and Anzac Day) is expected to flow through in May (due to an early payroll cut-off in April). Note that the Personnel cost variance above includes $129k (24FTE) of costs incurred in delivering additional unbudgeted Provider revenue. Outsourcing to cover key vacancies (e.g. Mental Health) and to meet MoH targets (e.g. gastro, renal, MRI). Higher outsourced nursing costs reflect the need for patient watches due to clinical risk – mainly in the Surgical wards. A one-off historic catch-up on invoicing during the month has also contributed to the unfavourable cost of outsourced nursing.
Outsourced Services
Month YTD Full Yr.
Act Bud Var. $000 Act Bud Var. Bud
2,684 2,916 232 Corporate & Funder Services 27,897 29,165 1,268 28,296
2,463 1,671 (792) Clinical Service 18,550 16,632 (1,918) 18,864 5,147 4,587 (560) Total 46,447 45,797 (650) 55,267
Clinical Services to MoH targets (e.g. gastro, renal, MRI); partly offset by hA YTD cost benefit and savings in other expenses.
34

Counties Manukau District Health Board Agenda 15 June 2016
Independent Service Provider (Demand driven expenditure)
Month Major Categories YTD Full Yr.
Act Bud Var. $000 Act Bud Var. Bud
Personal Health
20,995 20,991 (4) IDF Personal Health 207,020 209,910 2,890 251,892
8,446 8,547 101 Pharmaceuticals 85,917 85,470 (447) 102,564
7,274 7,100 (174) Primary Practice
Services – Capitated
73,887 71,000 (2,887) 85,200
629 579 (50) Child and Youth 5,200 5,790 590 6,948
525 470 (55) Adolescent Dental Benefit 4,770 4,700 (70) 5,640
881 739 (142) Chronic Disease
Management and Education
7,385 7,390 5 8,868
480 363 (117) Palliative Care 4,797 3,630 (1,167) 4,356
260 258 (2) General Medical Subsidy 2,582 2,580 (2) 3,096
949 1,129 180 Other 5,952 11,287 5,335 13,537
40,439 40,176 (263) Total Personal Health 397,510 401,757 4,247 482,101
35

Counties Manukau District Health Board Agenda 15 June 2016
Mental Health
1,281 1,281 - IDF Mental Health 12,808 12,810 2 15,372
852 777 (75) Community
Residential Beds & Services
8,451 7,770 (681) 9,324
688 720 32 Other Home
Based Residential Support
6,979 7,200 221 8,640
339 322 (17) Alcohol & Other Drugs 3,401 3,220 (181) 3,864
271 273 2 Crisis Respite 2,749 2,730 (19) 3,276 351 358 7 Child & Youth 3,512 3,580 68 4,296
178 165 (13) Kaupapa Maori Community 1,754 1,650 (104) 1,980
163 170 7 Community Service 1,633 1,700 67 2,040
639 1,437 798 Other 7,645 14,370 6,725 17,244
4,762 5,503 741 Total Mental Health 48,932 55,030 6,098 66,036
Disability Support Services
4,499 4,130 (369) Residential Care: Hospitals 44,185 41,305 (2,880) 49,567
1,403 1,809 406 Residential Care: Rest Homes 17,843 18,090 247 21,708
1,731 1,665 (66) Home Support 16,316 16,650 334 19,980 1,294 1,573 279 Other 15,182 15,730 548 18,876
8,927 9,177 250 Total Disability Support Services 93,526 91,775 (1,751) 110,131
For the fourth month in a row we have seen an increased spending for new beds and new facilities. Pressure for aged population beds in the district is growing and we have seen an increase investment by the NGO sector in supplying those beds. The increased costs of home support have been offset by increased revenue for this service.
201 159 (42) tal Public Health 1,311 1,590 279 1,908
39 39 - tal Maori Health 377 390 13 468
54,368 55,054 686 Funder 541,656 550,542 8,886 660,644
36

Counties Manukau District Health Board Agenda 15 June 2016
Clinical Supplies Month YTD Full Yr.
Act Bud Var. $000 Act Bud Var. Bud
3,718 3,595 (123) Treatment Disposables 36,448 35,456 (992) 42,825
742 698 (44) Diagnostic Supplies &
Other Clinical Supplies
8,094 6,980 (1,114) 8,403
1,248 1,167 (81) Instruments & Equipment 11,805 11,500 (305) 13,910
290 306 16 Patient Appliances 3,134 2,993 (141) 3,629
1,412 1,454 42 Implants & Prostheses 14,211 14,073 (138) 17,156
1,512 1,357 (155) Pharmaceuticals 14,481 13,770 (711) 16,588
298 324 26 Other Clinical Supplies 3,323 3,245 (78) 3,897
9,220 8,901 (319) Total 91,496 88,017 (3,479) 106,408 • Clinical Supplies: unfavourable for the month.
Clinical Support. Drug overspend was driven by infection and nutrition; Blood costs include a high cost haematology patient and patients that required transfusion activations; other including overspend in testing kits. Surgical. Overspend driven by high complexity acute work, particularly knee prosthesis. Medicine. Renal fluids use down 8.9% for the month, as well as a one-off credit received for renal fluid pricing. Note that the Clinical Supplies cost variance above includes costs incurred in delivering additional unbudgeted revenue
Non-Clinical / Infrastructure (excluding Interest and Capital Charge) Month YTD Full Yr.
Act Bud Var. $000 Act Bud Var. Bud 4,153 5,419 1,266 Provider 50,443 53,641 3,198 62,749
337 263 (74) Governance 3,025 2,645 (380) 265 4,490 5,682 1,192 Total 53,468 56,286 2,818 63,014
Explained by one-off provision releases during the month.
37

Counties Manukau District Health Board Agenda 15 June 2016
Interest and Capital Charge
Month YTD Full Yr. Act Bud Var. $000 Act Bud Var. Bud 240 142 98 Interest - Received 2,985 1,420 1,565 1,699
1,025 1,097 72 Interest Paid - Debt 10,386 10,970 584 14,712
785 955 170 Net Interest Paid 7,401 9,550 2,149 13,013 1,608 1,178 (430) Capital Charge 15,168 11,852 (3,316) 14,136
Interest cost: Interest received; significantly improved cash position. Capital Charge: unfavourable variance reflects the actual cost of capital charged by MoH (increase
in the revaluation of land) against budget matched against additional revenue. Timing of top up payments expected but not confirmed until April.
Ratios Provider Arm (only) Costs to Revenue (%) last six months
Apr 16
Mar 16
Feb 16
Jan 16
Dec 15
Nov 15
Oct 15
Medical 21.01 21.96 19.94 20.62 21.18 20.58 21.13 Nursing 24.59 25.49 24.67 25.05 25.09 23.70 24.97 Allied 9.35 9.87 9.29 8.95 9.43 8.95 9.31 Support 3.16 3.25 2.75 3.38 3.21 2.96 3.12 Management 7.33 7.42 7.17 6.92 7.33 6.96 6.91 Personnel 65.44 67.99 63.81 64.92 66.24 63.16 65.44 Outsourced Pers. 2.58 1.89 1.73 1.79 1.90 2.24 1.93 Total Personnel 68.02 69.88 65.54 66.71 68.14 65.39 67.37 Outsourced Clinical Services 3.51 2.42 2.77 2.44 2.40 2.94 3.25
Outsourced Corp (hA) 3.59 3.68 3.75 3.73 3.37 3.97 3.82
Clinical Supplies 14.42 15.38 13.62 13.97 13.38 14.18 14.60 Infrastructure 12.28 13.53 13.71 13.41 14.49 14.04 13.22 Total 101.82 104.90 99.39 100.26 101.77 100.52 102.26
38

Counties Manukau District Health Board Agenda 15 June 2016
Provider cost as a percentage of revenue over the last four years and year to date 2016 2015 2014 2013 2012 Medical 20.8 20.9 20.7 21.2 20.5 Nursing 24.6 24.8 25.1 25.5 24.7 Allied Health 9.3 9.3 9.7 9.7 9.5 Support 3.1 3.0 2.9 2.7 2.7 Man/Admin 7.1 6.9 6.8 7.2 7.8 Personnel 65.0 65.0 65.2 66.3 65.2 Outsourced Personnel 2.1 2.0 1.8 1.8 1.7 Total Personnel 67.0 67.0 67.0 68.1 66.9 Outsourced Clinical Supplies 2.6 2.5 2.7 2.9 2.8 Outsourced Corporate 3.7 3.7 3.7 3.4 3.3 Clinical supplies 14.3 14.4 14.0 14.4 14.7 Infrastructure 13.4 13.2 13.0 12.4 13.2 Total 101.1 100.8 100.4 101.2 100.9 Depn 3.9 3.6 3.8 3.1 2.8 Interest 1.5 1.5 1.1 1.5 1.3 Capital Charge 2.2 1.8 1.7 1.7 1.7
39

Counties Manukau District Health Board Agenda 15 June 2016
Balance Sheet
Actual Budget Variance Opening
1st July 15 YTD
Movement Current Assets Petty Cash 10 10 - 10 - Bank 54,815 30,722 24,093 55,246 (431) Trust 897 896 1 886 11 Prepayments 476 920 (444) 945 (469) Debtors 50,432 50,074 358 45,074 5,358 Inventory 2,159 1,320 839 1,320 839
Assets Held for Sale - 12,503 (12,503) 12,503 (12,503)
Total current Assets 108,789 96,445 12,344 115,984 (7,195) Fixed Assets Land 155,005 144,683 10,322 144,683 10,322 Buildings & Plant 662,572 662,798 (226) 625,018 37,554 Investment Property 1,449 1,449 - 1,449 - Information Technology 5,759 5,432 327 5,332 427 Information Software 5,215 5,518 (303) 5,008 207 Motor Vehicles 4,319 4,501 (182) 4,291 28 Total Cost 834,319 824,381 9,938 785,781 48,538 Accum. Depreciation (208,545) (182,983) (25,562) (155,685) (52,860) Net Cost 625,774 641,398 (15,624) 630,096 (4,322) Work In-progress 19,815 5,234 14,581 5,234 14,581 Total Fixed Assets 645,589 646,632 (1,043) 635,330 10,259 Investments (hA IT / HBL) 36,538 38,990 (2,452) 29,390 7,148 Total Assets 790,916 782,067 8,849 780,704 10,212 Current Liabilities Creditors 86,220 91,615 (5,395) 92,005 (5,785) Income in Advance 10,323 - 10,323 1,920 8,403 GST and PAYE 18,907 12,942 5,965 12,929 5,978
Loans (short term less than one year) - - - -
Payroll Accrual & Clearing 33,797 38,138 (4,341) 36,861 (3,064) Employee Provisions 86,598 85,235 1,363 85,225 1,373 Total Current Liabilities 235,845 227,930 7,915 228,940 6,905 Working Capital (127,056) (131,485) 4,429 (112,956) (14,100) Net Funds Employed $555,071 $554,137 $934 $551,764 $3,307 Non-Current Liabilities Term Loans 292,500 292,500 - 292,500 -
Employee Provisions (non-current) 20,403 20,283 120 20,283 120
Trust and Special Funds 888 896 (8) 882 6
Insurance Liability- Non Current 1,489 1,337 152 1,337 152
Total Non-Current Liabilities 315,280 315,016 264 315,002 278 Crown Equity
40

Counties Manukau District Health Board Agenda 15 June 2016
Crown Equity 124,078 124,078 - 124,078 - Revaluation Reserve 173,729 173,729 - 173,729 - Retained Earnings (58,016) (58,686) 670 (61,045) 3,029 Total Crown Equity 239,791 239,121 670 236,762 3,029 Net Funds Employed $555,071 $554,137 $934 $551,764 $3,307 Note: Assets for sale have now been transferred back to Fixed Assets as the assets have been taken off the market. Commentary:
Net borrowings: Long and short term debt less bank balance better than budget $24.1m but in line with last year.
Debtors: On budget, $5.3m higher than June 15, due to payments outstanding with the Crown (see table below).
MOH Debtors $000
Total Current 30 day +
Invoiced 4,546 2,918 1,628
Accrued 345
Total 4,891
Last month 5,361
Accounts payable: $1.9m lower than budget and $4.8m lower than June 2015. Net Fixed Assets: Are $1.0m lower than budget (timing of capital spends see cash flow). Investments in Associates: New Zealand Health Partners $ 5.8m Note: we will need to continue to ensure that these investments have underlying value through the future success of NZHP. healthAlliance $30.7m for ICT capital investment. The first payment of $3.0m was made in March, with two more payment in April $1.5m and June scheduled. Payroll Accrual & Clearing: due to timing of payroll cut offs.
There are no other significant issues regarding the Balance Sheet.
41

Counties Manukau District Health Board Agenda 15 June 2016
Cash flow Month YTD Actual Budget Variance Actual Budget Variance Cash flows from operating activities: Crown Revenue 122,431 123,408 (977) 1,234,018 1,227,806 6,212 Other 3,345 2,835 510 32,826 29,731 3,095 Interest rec. 240 142 98 2,985 1,420 1,565 Expenses
Suppliers 75,144 74,541 (603) 753,089 743,296 (9,793)
Employees 44,036 46,563 2,527 465,600 472,091 6,491 Interest paid 1,025 1,226 201 10,386 12,260 1,874 Capital charge - - - 9,193 7,644 (1,549) Net cash from Operations 5,811 4,055 1,756 31,561 23,666 7,895
Cash flows from Investing Fixed Assets (4,855) (2,320) (2,535) (24,839) (38,600) 13,761 Sale of Asset Investments (hA & HBL) (1,513) (1,048) (465) (7,148) (9,587) 2,439
Restricted & Trust Funds 1 (1) 2 6 1 5
Net cash from Investing (6,367) (3,369) (2,998) (31,981) (48,186) 16,205
Debt - - - - - - Other non-current liability - - - - - -
Net cash from Financing - - - - - -
Net increase / (decrease) (556) 686 (1,242) (420) (24,520) 24,100
Opening cash 56,278 30,942 25,336 56,142 56,148 (6) Closing cash 55,722 31,628 24,094 55,722 31,628 24,094 Summary Month YTD Actual Budget Variance Actual Budget Variance Opening cash 56,278 30,942 25,336 56,142 56,148 (6) Operating 5,811 4,055 1,756 31,561 23,666 7,895 Investing (6,367) (3,369) (2,998) (31,981) (48,186) 16,205 Financing - - - - - - Closing cash 55,722 31,628 24,094 55,722 31,628 24,094 Commentary: Fixed Asset spending continues to be timing against the budgeted spend for Mental Health building (total $53.6m ytd spending 5.1m) and the laboratories (total 13.3m ytd spending 6.0m) move to the Harley Gray building. This reflects optimistic timelines in utilising the balance of the Harley Gray external funding i.e. timing difference only. Payment for $6.1m C class shares in healthAlliance will be paid in three amounts with the first paid in March $3.0m, and the balance paid in April $1.5m and June $1.6m.
42
Counties Manukau District Health Board Agenda 15 June 2016
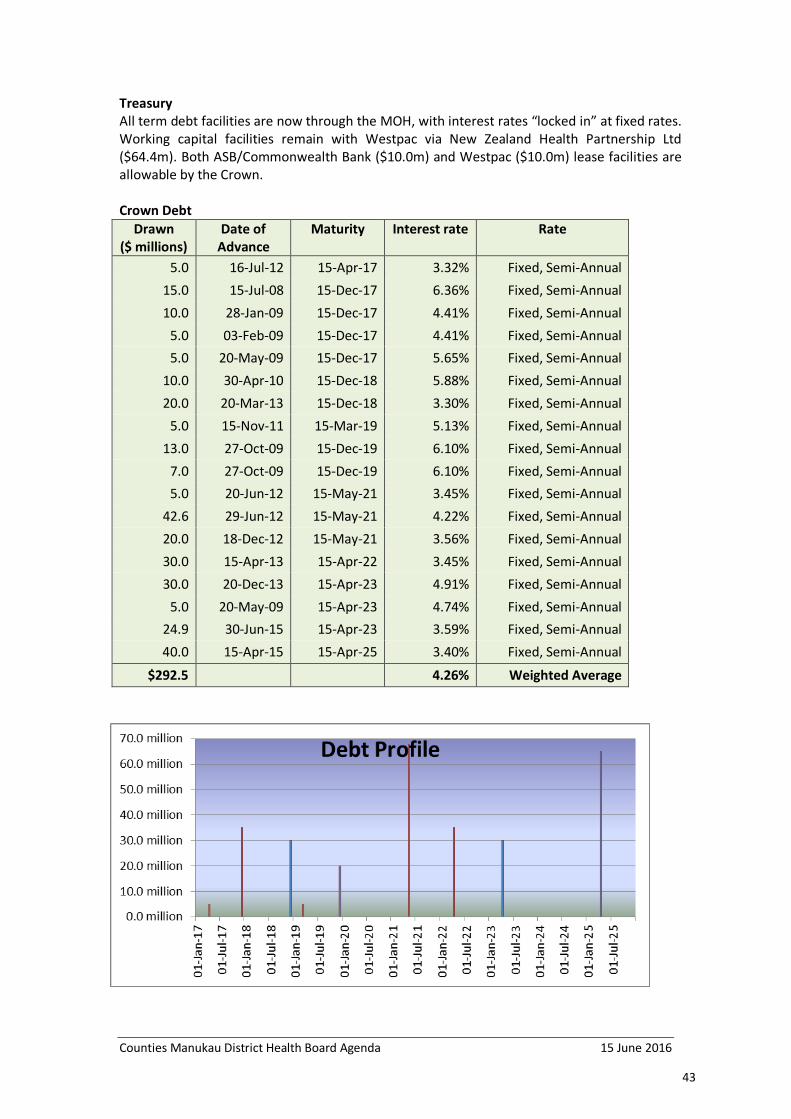
Treasury All term debt facilities are now through the MOH, with interest rates “locked in” at fixed rates. Working capital facilities remain with Westpac via New Zealand Health Partnership Ltd ($64.4m). Both ASB/Commonwealth Bank ($10.0m) and Westpac ($10.0m) lease facilities are allowable by the Crown. Crown Debt
Drawn ($ millions)
Date of Advance
Maturity Interest rate Rate
5.0 16-Jul-12 15-Apr-17 3.32% Fixed, Semi-Annual 15.0 15-Jul-08 15-Dec-17 6.36% Fixed, Semi-Annual 10.0 28-Jan-09 15-Dec-17 4.41% Fixed, Semi-Annual
5.0 03-Feb-09 15-Dec-17 4.41% Fixed, Semi-Annual 5.0 20-May-09 15-Dec-17 5.65% Fixed, Semi-Annual
10.0 30-Apr-10 15-Dec-18 5.88% Fixed, Semi-Annual 20.0 20-Mar-13 15-Dec-18 3.30% Fixed, Semi-Annual
5.0 15-Nov-11 15-Mar-19 5.13% Fixed, Semi-Annual 13.0 27-Oct-09 15-Dec-19 6.10% Fixed, Semi-Annual
7.0 27-Oct-09 15-Dec-19 6.10% Fixed, Semi-Annual 5.0 20-Jun-12 15-May-21 3.45% Fixed, Semi-Annual
42.6 29-Jun-12 15-May-21 4.22% Fixed, Semi-Annual 20.0 18-Dec-12 15-May-21 3.56% Fixed, Semi-Annual 30.0 15-Apr-13 15-Apr-22 3.45% Fixed, Semi-Annual 30.0 20-Dec-13 15-Apr-23 4.91% Fixed, Semi-Annual
5.0 20-May-09 15-Apr-23 4.74% Fixed, Semi-Annual 24.9 30-Jun-15 15-Apr-23 3.59% Fixed, Semi-Annual
40.0 15-Apr-15 15-Apr-25 3.40% Fixed, Semi-Annual
$292.5 4.26% Weighted Average
43
Counties Manukau District Health Board Agenda 15 June 2016
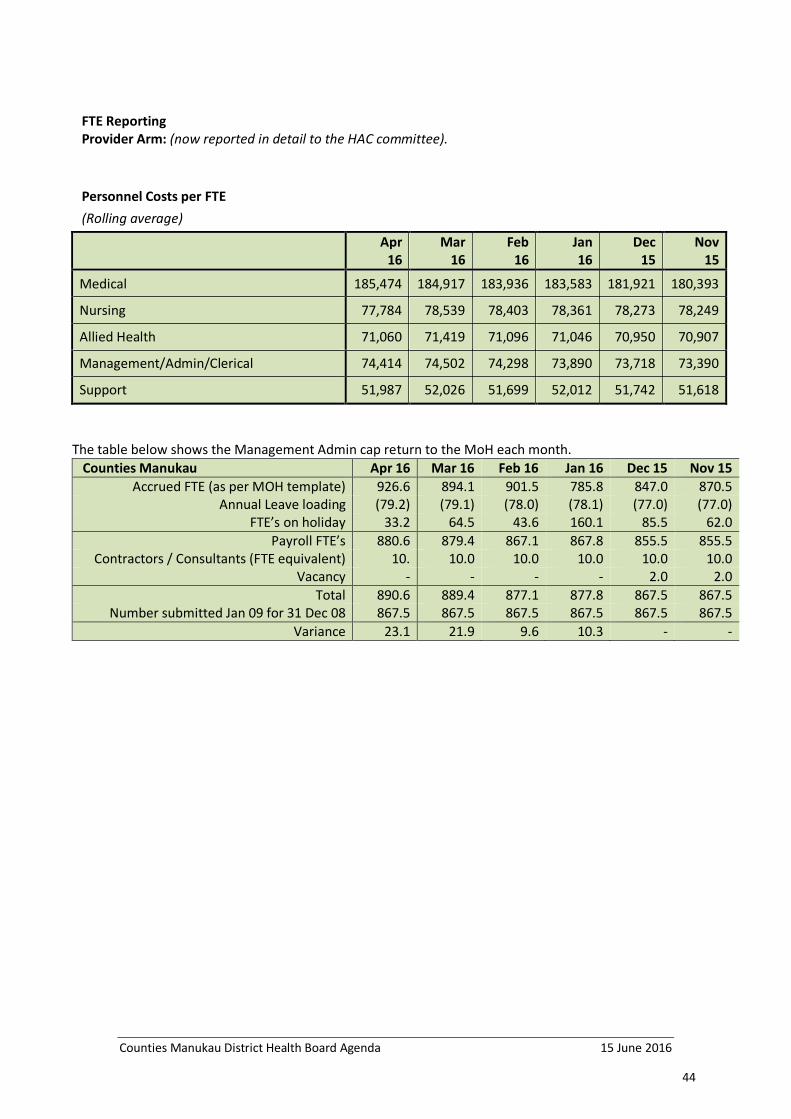
FTE Reporting Provider Arm: (now reported in detail to the HAC committee). Personnel Costs per FTE (Rolling average)
Apr 16
Mar 16
Feb 16
Jan 16
Dec 15
Nov 15
Medical 185,474 184,917 183,936 183,583 181,921 180,393
Nursing 77,784 78,539 78,403 78,361 78,273 78,249
Allied Health 71,060 71,419 71,096 71,046 70,950 70,907
Management/Admin/Clerical 74,414 74,502 74,298 73,890 73,718 73,390
Support 51,987 52,026 51,699 52,012 51,742 51,618
The table below shows the Management Admin cap return to the MoH each month. Counties Manukau Apr 16 Mar 16 Feb 16 Jan 16 Dec 15 Nov 15
Accrued FTE (as per MOH template) 926.6 894.1 901.5 785.8 847.0 870.5 Annual Leave loading (79.2) (79.1) (78.0) (78.1) (77.0) (77.0)
FTE’s on holiday 33.2 64.5 43.6 160.1 85.5 62.0 Payroll FTE’s 880.6 879.4 867.1 867.8 855.5 855.5
Contractors / Consultants (FTE equivalent) 10. 10.0 10.0 10.0 10.0 10.0 Vacancy - - - - 2.0 2.0
Total 890.6 889.4 877.1 877.8 867.5 867.5 Number submitted Jan 09 for 31 Dec 08 867.5 867.5 867.5 867.5 867.5 867.5
Variance 23.1 21.9 9.6 10.3 - -
44

Counties Manukau District Health Board Agenda 15 June 2016
6.0 Ko Awatea
Purpose of report: Information and strategic alignment. Please feedback requests for more detail.
Key Ko Awatea led or supported Collaboratives, Programmes & Campaigns
Healthy Services
Enhanced Primary Care Collaborative; Technology Enabling Change Programme; Enhanced Recovery After Surgery Collaborative; Faster Cancer Treatment Project; Hand Hygiene Project; Safety in Practice Collaborative; Enhanced Primary Care Collaborative; Community Health System Integration; Care Compass Programme; Early Learning Collaborative; Now We’re Talking Collaborative; National Improvement Network.
Healthy People, Whaanau & Families
Diabetes Care Collaborative, At Risk Individuals Programme, Mental Health First Aid Programme.
Healthy Communities Manaaki Hauora; Handle the Jandal; Health Equity Collaborative; Social Sector Collaboration.
Update
Key Performance Indicators • Core business support for CMH maintained and constantly improved. • Capability Building: Clinical, Academic and Community leaders are supported to grow; educational
offerings aligned with competencies developed. • Successful events delivered: cross-sector focus and drive for sustainability e.g. APAC, TEDx. • Equity and safety collaboratives are delivered. • Spread the use of e learning platform. • National improvement network to be established. measures ( • KA2 built to address high demand for centre space, driving sustainability, and increase cross-sector and
community involvement.
Building Capability. We continue to support CMH in achieving its strategic goals. The launch of the People Strategy and some key appointments helps focus priorities going forward. Key work is underway supporting the CHISI programme as well as the organisation’s Change Management initiative.
Health Intelligence. The increase in general or ad hoc requests continues, comprising queries on patient flow, efficiency or clinical best practice. They represent nearly half of all requests made to the HI&I Analyst team; the other half relates to research, on-going projects, data investigations and maintaining the automated reporting system
Engagement. Following a merger of the APAC and Ko Awatea websites in Jan 16 there has been significant increase in web engagement. Popular pages on the Ko Awatea websites are consistently APAC Forum, About KA and Programmes. Marketing & Communications continues to execute its programme to lift engagement across all channels.
Over this period, related metrics of Pages Viewed and Time Spent on the site all increased steadily.
This represents around half of all requests to the Health Intelligence & Informatics analyst team.
‘ADHOC’ REQUESTS FOR INFORMATION
UNIQUE VISITORS TO KO AWATEA/APAC WEBSITE
45

Counties Manukau District Health Board Agenda 15 June 2016
7.0 Compliance
7.1 No compliance issues to report on this month. The Health & Safety update is included below. 7.1.1 Health & Safety
The health and safety risk for community health workers continues to be addressed within a multi-disciplinary team engagement approach. It aims to embed improvement and mitigation strategies within the wider CMH Community Health Service Integration Project and includes input from the CM Health Risk Manager. Moving and Handling remains an ongoing risk. A proposal outlining options for consideration has been submitted to the Executive Leadership Team. As an accredited employer against the ACC Partnership Program, the organisation was due to pay ACC $2,580,214 in levies for the period 1 April 2016 to 31 March 2017. The ACCPP scheme is not only self-funding but creates a significant return to the DHB based on Health and Safety and Injury Management performance. As such the payment to ACC is $216,152 with a balance of $1,848,019 to fund work injury claims and claim management costs. This is to be considered in the context of injury treatment costs which have increased. CM Health is on track to meet the obligations of the new Health and Safety at Work Act 2015 (HSWA) with a number of documents being reviewed and made available to Board members at their request, with the aim of providing additional assurance. The Wellness Strategy continues to be developed and scoped. Early indications from analyses of trends indicate that non work related stress appears to be a factor in staff accessing subsidized counselling and forms an important focus in identifying intervention options. The formal component of the annual Flu Program has been completed with a 60% uptake. Peer vaccinators will continue to provide vaccinations until the vaccine is recalled.
7.1.2 Board & Board Committee Papers The project to improve advice to the Board and Board Committees is now into an implementation phase. An external review of a sample of papers identified areas that required improvement, such as the content being more relevant to the audience including their role, the style and length of papers. The following actions have therefore been undertaken: 1. An ELT learning lab on the roles of governance and expectations
on the executive led by Janine Smith, The Boardroom Practice has been completed. The external review findings were also covered in the learning lab.
2. A guideline has been developed to ensure that advice to the Board and Board Committees is more explicit on requirements.
46

Counties Manukau District Health Board Agenda 15 June 2016
In addition, some guidance has been incorporated into templates (to provide clarity and a link to the guideline) for Board and Board Committee papers (see Diligent Resource Centre). Executives are responsible for their advice to the Board and Board Committees. The key change in the process is that ELT will approve actual Board papers rather than the Board being provided with the same paper that was submitted to ELT. Deadlines and process will be strictly adhered to.
3. A practical workshop has been held for ELT, with a further workshop for second/third tier managers and other authors on the roles of the Board and Board Committees and how improvements to advice can be made. Engagement is planned with key teams and communication will take place across the organisation on expectations, guidelines and templates, timelines, roles of the Board and Board Committees.
4. Further samples of papers will be reviewed after six and twelve months, to gauge whether these changes have been effective and have subsequently led to an improvement in papers being submitted to Board and Board Committees.
I would expect to see an improvement in the clarity of papers being provided, and anticipate that they should better suit the Board and Board Committees’ needs. These changes will come into effect from the July Board and Board Committee meetings.
47

Counties Manukau District Health Board 15 June 2016
Counties Manukau District Health Board Occupational Health and Safety – Q3 Report
Recommendation It is recommended that the Board receive the Health and Safety quarterly report for the period ending 31 March 2016. Prepared and submitted by: Bev Stone, Manager Occupational Health & Safety Service Executive Summary This paper reports on quarterly health and safety activity for the period ending 31 March 2016. Quarterly Report Highlights Health and Safety Performance Overview LAG INDICATORS
LEAD INDICATORS
Lost Time Injuries:
Audits: Lost Time Injury Frequency Rate 12.88
Percentage Completed (Average) 93%
Lost Time Injury Severity Rate 621.24
Number of Hazards Identified 0 Lost Time Incidents 31
Training:
Number of Injury Claims 75
Number of H&S Reps Trained* 0 Cost of Injury Claims $52,150
Number of Managers Trained 14
Incidents:
Welcome Day Attendees 0 Total Number of Incidents 303
Health Monitoring:
Number of Serious Harms 5
Pre-Employment Health Screening 279 The above table provides a high level overview of Counties Manukau Health (CM Health) Health and Safety performance for this quarterly reporting period. Commentary is included in further detail in this report. *Please refer to the Training section further in this further report for full details on the H&S Representative training for the quarter
48

Counties Manukau District Health Board 15 June 2016
Quarterly Performance Serious Harm Notifications These injuries fulfill the criteria defined in the H&S Legislation and require external notification to WorkSafe NZ:
Division Location Injury Details
Injured Person Classification
Hazard/Process involved Date
MACS Laboratory Fractured hand
Walking down corridor when she fell
Employee Slip/Trip/Fall 5 Feb 2016
SACS MSC Module 3 Dislocated shoulder
Missed a step going down stairs
Employee Slip/Trip/Fall 16 Feb 2016
Facilities Non-Clinical Support
Disc protrusion
Lifting heavy laundry bags
Employee Manual Handling
16 Feb 2016
Corporate Finance Fractured elbow
Stumbled and fell when exiting office
Employee Slip/Trip/Fall 9 Mar 2016
SACS Orthopedics Fractured humerus
Fell as exiting lift
Employee Slip/Trip/Fall 17 Mar 2016
• CM Health has received formal response from WorkSafe indicating no further action or
investigation is required for the fractured humerus incident. • CM Health is awaiting response from WorkSafe on the remaining incidents. • All incidents have been investigated to identify hazards and risks. Mitigation activities have been
followed up.
Audits (As per the 2015/2016 Health and Safety Action Plan)
Internal Audits • The audit cycle is continuing on a bi-monthly schedule. During this reporting period, one cycle
was completed in February 2016. • The completion rates across CM Health for these audit cycles average 93%. • The next internal Inspections will be undertaken in April and June 2016.
49

Counties Manukau District Health Board 15 June 2016
• The audits identified one existing moderate risk (reparation of patient beside lights), which was
first identified in October 2015. This has been escalated to Facilities for repair. • Trends indicate marked improvement over the previous 12 months regarding the
implementation of mitigation plans in a timelier manner. This may be the result of greater management involvement in the audits/inspections, which results in addressing minor issues negating the need for escalation.
Executive Audits • An executive audit has been scheduled for April, and the reports will be provided in the next
quarter report.
External Audits • No external Health and Safety audits were undertaken for this reporting period. Injuries and Impact
Incident Notifications • The information presented is for the quarter January – March 2016. • All incidents are initially reviewed by the H&S team and where necessary referred for
operational intervention based on the severity of the incident, with OHS support as required. • BBFE incidents have increased across all Divisions. • Assaults and Patient/Manual Handling were the main cause of incidents across MACS in this
period. For this reporting period, 11 incidents relating to workplace stress, primarily due to workload and staff numbers were reported. This was managed with support from HR.
• Incidents and notifications in SACS have remained consistent with last quarter. • Mental Health incident notifications continued to reflect a high number of Assaults with other
incident types remaining consistent.
Incident Notifications - count of incidents with incident date occurring Jan – March 2016. Lost Time Injuries (LTI’s) - count of workplace injuries with injury date occurring Jan – March 16. * Not all Divisions are shown here so the total may be higher than the consolidated divisional data. Data is accurate as at time of reporting and may change month on month for some measures
50

Counties Manukau District Health Board 15 June 2016
CM Health Lost Time Injury Frequency Rate (LTIFR) and Lost Time Injury Severity Rate (LTISR)
Severity Rates for the quarter has decreased slightly while the Frequency Rate increased minimally, indicating that the number of injuries were similar to the previous quarter, but required less time off from work.
LTIFR LTISR
Oct – Dec 15 9.73 679.12 Jan – Mar 16 12.88 621.24
LTIFR (Lost Time Injury Frequency Rate) = (# of Lost Time Injuries / Hours Worked) x 1,000,000. LTISR (Lost Time Injury Severity Rate) = (# of Lost Hours / Hours Worked) x 1,000,000.
Explanation: • Finance: The increased frequency and severity rates were the result of a Slip/Trip/Fall incident
which resulted in a fractured elbow and time off work • Human Resources: A manual handling incident resulted in some time off work and the
increased frequency and severity rates. • As these injuries occurred in smaller teams with lower man-hours than a larger Division, the
overall impact on the teams is higher.
Number of Lost Time Injuries per Division
51

Counties Manukau District Health Board 15 June 2016
Injury Impact – Claims Overview
• A total of 100 ACC claims were received, with 25 being declined following investigation. • Trends indicate effective management of claims lodged vs. claims accepted. Injuries resulting
in ACC Claims are predominantly caused by musculoskeletal injuries.
* This includes Medical and Social Compensation costs and Weekly Compensation cost estimates for days lost which are based on average salaries across divisions, as provided by Well NZ (Third Party Administrator).
• The total claims cost for the period is $52,150 and the Weekly Compensation Costs equates to $23,070*.
• This indicates a decrease in the costs compared to the previous quarter.
* Please note: March 2016 costs will increase once consolidated by the end of April.
52

Counties Manukau District Health Board 15 June 2016
Injury Trends
• There was a minor increase in the number of incidents reflected in the OHS critical risk profile
from the previous reporting period. • All incidents have been investigated. Health and Safety Management Framework Improvement
The Health and Safety Management Framework is underpinned by the Health and Safety Action Plan 2015.2016. The action plan is up to date and work continues to be aligned to progress work against this plan. The Health and Safety Action Plan 2015/2016 is attached in Appendix A. The plan continues to have an ongoing focus on the following priority areas: Hazard and Risk Management • A guideline has been drafted providing a tool to manage hazards and risk registers (a register is
a compliance requirement) • A training package has been developed and will be delivered, with the aim of providing
awareness and understanding for the operational management of hazards and risks and the maintenance of a Risk Register
• The development of work area hazard/risk registers remains an ongoing focus • Community Health Worker registers are a current priority focus which is due to recent
feedback and increasing incidents in the Community Health working environment • The development of systems and processes to track and consolidate risk registers has been
commenced • Planning has commenced for the annual Flu Vaccination Program scheduled to begin on the 4th
April 2016 • A draft Wellness strategy has been submitted for comment and feedback with operational
activities in place to gauge employee feedback
Incident Management and Injury Prevention • The revised CM Health Incident Management Procedure has now been confirmed by the
Serious Sentinel Events Committee and has been published and provides a consolidated approach to both patient and employee incident procedures
• The Occupational Health and Safety “Incident Investigation Guide” has been published
53

Counties Manukau District Health Board 15 June 2016
• A detailed analysis of Incidents has been completed and has provided a deeper understanding of incident trends for the past three years. This information will form the basis of Risk and Incident Management activities in the future, including alignment with the organisational risk framework
Contractor Management • Liaison has continued with healthAlliance, CM Health Legal and Facilities to begin sharing an
understanding of processes and to identify cross-overs and obvious gaps. CM Health Project Manager will present a draft Procurement Process document to the Northern Region Procurement and Supply Chain Forum on 1 April. A regional approach to this issue will be advocated and if agreement is reached CFO endorsement will be sought for regional consistency to be achieved
• The ACC Partnership Program self-assessment continued to review legislative requirements for health and safety components of contractor management
• The development of “A Health and Safety Guideline to the Management of Contractors” is continuing
Hazardous Substance Management • The Hazardous Substance Management Advisor commenced work and will be working from
within the Facilities team. • Activities reported from feedback received from the incumbent:
• A systematic review of recently approved and proposed regulatory changes and an assessment of previous audits is anticipated to be completed in March.
• Development of a hazardous substance management framework outline is to coincide with this review
Training • During this quarter, no formal training was provided to H&S representatives due to the delay
in the new Worker Participation Guidelines under the new Act. • H&S Representative training modules are now being reviewed and updated to reflect the
minor changes required. • Health and Safety at Work Act (HSWA) update sessions for Managers commenced in March.
Sessions for Managers and H&S Representatives will continue into the next quarter.
H&S Representatives Number Total Number of H&S Representatives 224
Total Number of Trained H&S Reps 144 H&S Representative Training Sessions Attendees
Representative Training (Update session) 0 0 Total Number of Reps Trained in this Quarter 0 0 H&S Other Training Sessions Attendees Manager H&S Training 2 14 Nurse Orientation (Part of Onboarding) 3 37
• The orientation programme for experienced nurses has commenced for 2016 with 24 nurses
attending during this quarter. • The 2016 H&S training programme communication was sent to the organisation. • eLearning H&S Orientation has been finalised and is now pending L&D delivery dates. • Development of incident investigation training for managers has commenced.
54

Counties Manukau District Health Board 15 June 2016
Employee (Worker) Participation
• Commenced review of organisational employee meetings with the aim of providing guidance
and recommendation that Health and Safety is included as an agenda item, where appropriate. This approach will ensure a business-as-usual approach as a value-add activity rather than a compliance requirement which will reinforcement a silo outcome.
• The development of tools and templates for structured Health and Safety Committee activity has continued
Alignment of H&S IT Systems with CM Health Business improvement requirements
• Work will continue indefinitely as an improvement activity to develop relevant systems and processes to support the Health and Safety Framework and relevant communications.
External, Legislative and Industry Updates
• WorkSafe have advised that the majority of the first phase of regulations to support the new
Health and Safety at Work Act 2015 (HSWA) have been now been finalised and will come into force on 4 April 2016, along with the Act
• The regulations supported with information and guidance from WorkSafe New Zealand are intended to support businesses (particularly small businesses) to understand what they need to do to comply with the general duties of the Act. The regulations relate to matters such as:
• Asbestos • Engagement, worker participation and representation • General risk and workplace management • Major Hazard Facilities
• WorkSafe’s next steps include: • Finalizing regulations specifying infringement offences, fees and exemptions • Further regulations will be developed over the next two years
• CM Health is prepared for the legislative changes with the robust Health and Safety Plan currently in place.
• Meredith Connell have provided this assurance and also provided an update on due diligence and leadership to the Executive Leadership Team and Board
Next Steps • The Board will continue to be updated quarterly on progress against the Health and Safety
Action Plan 2015/2016 • This report will be presented to the Finance and Risk Meeting in Q4
55

Counties Manukau District Health Board 15 June 2016
Appendix A: Health and Safety Action Plan 2015/2016 Health and Safety Action Plan 2015/2016
H&S System 2015 2016
Q3 Q4 Q1 Q2 Q3 Q4
Leadership and Practice Responsibility, Commitment & Legal Obligations
Develop annual (15/16) Health and Safety Plan in alignment with priority health and safety core objectives
Guideline development for health and safety leadership, planning and due diligence
Annual review of Health & Safety Policy (update and issue accordingly) Assist in embedding of organisational H&S objectives
Develop annual (16/17) Health and Safety Plan in alignment with priority health and safety core objectives Establish H&S leadership and performance measurement targets
Engage with stakeholders on inclusion of H&S in recruitment processes.
Bi-annual review & update of EPG
H&S Information, Document Management & Communications
Implementation of online Pre-employment Health Screening Develop Health and Safety Recognition Programme collateral and communicate accordingly
Development of a Health and Safety Communications Strategy
Communicate legislative changes to organisation as appropriate Review and update HSMS manual
Review and update OHS intranet pages
Prepare communications and information for bi-annual ACC Partnership Programme Audit 2016
Prepare and disseminate communications and information for National Safety Week
Prevention as a Culture Hazard/Risk Management
Progress formalised hazard risk assessment system: 2nd pilot trial of Hazard Risk Register tool/template
Amalgamate pilot feedback into the tool/template and develop Hazard Risk Register guidelines
Hazard Risk Register training Support workplace area Hazard Risk Registers development (ongoing process)
Support workplace area Hazard Risk Registers development (ongoing process) Review of orgnasitonal health and safety critical risk profile
Engage with HR regarding workplace Bullying & harassment Investigate fatigue as an organisational risk
Emergency Preparedness & Response
Consult stakeholders on comprehensive emergency drills
Check ER plans/schemes for currency Objective review dates
Engage with Emergency Response (ER) stakeholders to obtain ER information for incorporation into the HSMS manual
Incorporate ER detail into the HSMS manual
Pre-ACC Partnership Programme audit checks of organisational ER
Engage with organisational ER stakeholders for participation in the 2016 ACC Partnership Programme audit
Contractor H&S Management
Investigate current state of health and safety as part of the contractor management process Commence review of clinical access agreements for tertiary providers
Commence ACC-based self-assessment to identify gaps in the health and safety contractor management area Finalise input of H&S as part of clinical access agreements for tertiary providers
Gather health and safety contractor management support documentation
Develop health and safety contractor management support documentation in consultation with stakeholders
Embed health and safety contractor management support documentation into consultation with stakeholders
56

Counties Manukau District Health Board 15 June 2016
Prevention as a Culture (Continued) Safe Design, Procurement & Disposal of Assets
Review health and safety as part of the procurement process
Investigate opportunity to embed health and safety into procurement processes and consult with stakeholders
Work with stakeholders to ensure health and safety is embedded into procurement processes
Hazardous Substances, Waste Management, Minimisation & Sustainability
Organisational HSNO certification due
Approved Handler certification due
Organisational HSNO certification due
Wellbeing and Medical Management
Currently being scoped and developed
Initiate Flu Programme Plan Flu Programme
H&S Training & Competency
Progression of organisational Manual Handling project Investigate feasibility of a National DHB HS Symposium
Finalisation of eLearning general health and safety orientation course (implementation TBC in alignment with organisational requirements) Manual Handling Project (ongoing) Review health and safety training programme and update for 2017
Develop health and safety capability building (training) material Review & update HS Rep training
Develop health and safety capability building (training) material (ongoing) Facilitate health and safety capability building training Identify preferred training provider network
Develop health and safety capability building (training) material (ongoing) Facilitate health and safety capability building training
Investigate development of Job Task Cards in collaboration with Recruitment Consult with the Building Capability team on Skills and training matrices
Incident Management
Health and safety system and structure development Commence development of incident investigation guideline Identify key CMH documents to embed health and safety data
Health and safety system and structure development (ongoing) Development of incident investigation guideline Embed health and safety data into identified key CMH documents
Health and safety system and structure development (ongoing) Conduct half yearly incident data analysis
Health and safety system and structure development (ongoing) Build capability in Incident Management
Investigate status of linkages between incident investigation findings and hazard & risk management Conduct half yearly incident data analysis and update organisational risk register and generic hazard/risk register if required
Check that improvement opportunities are assimilated into the hazard & risk management system
57

Counties Manukau District Health Board 15 June 2016
Employee Consultation & Involvement
Develop Health and Safety Recognition Programme
Develop JCC reporting template
H&S Recognition Programme implementation
Investigate opportunity for regular Health and Safety "drop-in" forum
Health and safety committee tool and template development
Finalise Health and safety committee tool and template (subject to stakeholder involvement)
2016 H&S Recognition Programme commencement
H&S Recognition Programme
National Safety Week (TBC)
Audit and Performance Measurement
ACC 'Injury Management and Rehabilitation' partnership programme audit preparation
Undertake ACC 'H&S' self-assessment
ACC 'Injury Management and Rehabilitation' partnership programme 2015 audit is completed
Review assessment (audit) tools
Undertake audits as per the health and safety Audit Programme
Commence preparation for the full ACC Partnership Programme Audit 2016
Undertake audits as per the health and safety Audit Programme (ongoing)
Preparation for the full ACC Partnership Programme Audit 2016 (ongoing)
Undertake audits as per the health and safety Audit Programme (ongoing)
Completion of full ACC Partnership Programme Audit 2016
Worker Empowerment and Engagement
Audit and Performance Measurement
58

Counties Manukau District Health Board Agenda 15 June 2016
Counties Manukau Health Board Meeting Resolution to Exclude the Public
Resolution:
That in accordance with the provisions of Schedule 3, Clause 32 and Sections 6, 7 and 9 of the NZ Public Health and Disability Act 2000:
The public now be excluded from the meeting for consideration of the following items, for the reasons and grounds set out below:
General Subject of items to be considered
Reason for passing this resolution in relation to each item
Ground(s) under Clause 32 for passing this resolution
1. Minutes of 4 May 2016 That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9(3)(g)(i))of the Official Information Act 1982. [NZPH&D Act 2000 Schedule 3, S32(a)]
Confirmation of Minutes For reasons given in the previous meeting.
2. Action Items That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9(3)(g)(i))of the Official Information Act 1982. [NZPH&D Act 2000 Schedule 3, S32(a)]
For reasons given in the previous meeting.
3. Maternity Review Panel Update
That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9(3)(g)(i))of the Official Information Act 1982. [NZPH&D Act 2000 Schedule 3, S32(a)]
Commercial Activities The disclosure of information would not be in the public interest because of the greater need to enable the Board to carry out, without prejudice or disadvantage, commercial activities. [Official Information Act 1982 S9(2)(i)]
4. System Level Measures
That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9(3)(g)(i))of the Official Information Act 1982. [NZPH&D Act 2000 Schedule 3, S32(a)]
Commercial Activities The disclosure of information would not be in the public interest because of the greater need to enable the Board to carry out, without prejudice or disadvantage, commercial activities. [Official Information Act 1982 S9(2)(i)]
5. Draft Long Term Investment Plan
That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section
Commercial Activities The disclosure of information would not be in the public interest because of the greater need to enable the Board to carry out, without prejudice or disadvantage, commercial activities.
59

Counties Manukau District Health Board Agenda 15 June 2016
9(3)(g)(i))of the Official Information Act 1982. [NZPH&D Act 2000 Schedule 3, S32(a)]
[Official Information Act 1982 S9(2)(i)]
6. Future Land Use for Manukau Site
That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9(3)(g)(i))of the Official Information Act 1982. [NZPH&D Act 2000 Schedule 3, S32(a)]
Commercial Activities The disclosure of information would not be in the public interest because of the greater need to enable the Board to carry out, without prejudice or disadvantage, commercial activities. [Official Information Act 1982 S9(2)(i)]
7. Botany Letter of Intent That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9(3)(g)(i))of the Official Information Act 1982. [NZPH&D Act 2000 Schedule 3, S32(a)]
Commercial Activities The disclosure of information would not be in the public interest because of the greater need to enable the Board to carry out, without prejudice or disadvantage, commercial activities. [Official Information Act 1982 S9(2)(i)]
8. Healthy Together 2020 – Technology Update
That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9(3)(g)(i))of the Official Information Act 1982. [NZPH&D Act 2000 Schedule 3, S32(a)]
Commercial Activities The disclosure of information would not be in the public interest because of the greater need to enable the Board to carry out, without prejudice or disadvantage, commercial activities. [Official Information Act 1982 S9(2)(i)]
9. Health Together 2020 – Technology – Clinical Portal Upgrade Regional Initiative
That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9(3)(g)(i))of the Official Information Act 1982. [NZPH&D Act 2000 Schedule 3, S32(a)]
Commercial Activities The disclosure of information would not be in the public interest because of the greater need to enable the Board to carry out, without prejudice or disadvantage, commercial activities. [Official Information Act 1982 S9(2)(i)]
10. Extension of Blood Culture Supply Agreement
That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9(3)(g)(i))of the Official Information Act 1982. [NZPH&D Act 2000 Schedule 3, S32(a)]
Commercial Activities The disclosure of information would not be in the public interest because of the greater need to enable the Board to carry out, without prejudice or disadvantage, commercial activities. [Official Information Act 1982 S9(2)(i)]
11. IS Projects Update That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which
Commercial Activities The disclosure of information would not be in the public interest because of the greater need to enable the Board to
60

Counties Manukau District Health Board Agenda 15 June 2016
good reason for withholding would exist, under section 6, 7 or 9 (except section 9(3)(g)(i))of the Official Information Act 1982. [NZPH&D Act 2000 Schedule 3, S32(a)]
carry out, without prejudice or disadvantage, commercial activities. [Official Information Act 1982 S9(2)(i)]
12. Second Draft Pacific Health Plan 2016/17
That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9(3)(g)(i))of the Official Information Act 1982. [NZPH&D Act 2000 Schedule 3, S32(a)]
Commercial Activities The disclosure of information would not be in the public interest because of the greater need to enable the Board to carry out, without prejudice or disadvantage, commercial activities. [Official Information Act 1982 S9(2)(i)]
13. Second Draft Asian Health Plan 2016/17
That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9(3)(g)(i))of the Official Information Act 1982. [NZPH&D Act 2000 Schedule 3, S32(a)]
Commercial Activities The disclosure of information would not be in the public interest because of the greater need to enable the Board to carry out, without prejudice or disadvantage, commercial activities. [Official Information Act 1982 S9(2)(i)]
14. Workforce Development – Tindall Foundation
That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9(3)(g)(i))of the Official Information Act 1982. [NZPH&D Act 2000 Schedule 3, S32(a)]
Commercial Activities The disclosure of information would not be in the public interest because of the greater need to enable the Board to carry out, without prejudice or disadvantage, commercial activities. [Official Information Act 1982 S9(2)(i)]
15. Confirmation of NRA Directors
That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9(3)(g)(i))of the Official Information Act 1982. [NZPH&D Act 2000 Schedule 3, S32(a)]
Commercial Activities The disclosure of information would not be in the public interest because of the greater need to enable the Board to carry out, without prejudice or disadvantage, commercial activities. [Official Information Act 1982 S9(2)(i)]
16. IHI Special General Meeting That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9(3)(g)(i))of the Official Information Act 1982. [NZPH&D Act 2000 Schedule 3, S32(a)]
Commercial Activities The disclosure of information would not be in the public interest because of the greater need to enable the Board to carry out, without prejudice or disadvantage, commercial activities. [Official Information Act 1982 S9(2)(i)]
61

Counties Manukau District Health Board Agenda 15 June 2016
17. Updated Board & Board Committee Terms of Reference
That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9(3)(g)(i))of the Official Information Act 1982. [NZPH&D Act 2000 Schedule 3, S32(a)]
Commercial Activities The disclosure of information would not be in the public interest because of the greater need to enable the Board to carry out, without prejudice or disadvantage, commercial activities. [Official Information Act 1982 S9(2)(i)]
62