covid19 and the pediatric heart: myocarditis, mis-c
TRANSCRIPT

COVID19 and the Pediatric Heart: Myocarditis, MIS-c, Return to Play and
Post-Immunization Myocarditis
Lauren Sterrett, PA-C
Physician Assistant in Division of Pediatric Cardiology
November 4, 2021

Disclosure
2
▪ I have no relevant financial relationships with the manufacturer(s) of any commercial product(s) and/or
provider(s) of commercial services discussed
Objectives
3
▪ Discuss COVID-19’s acute effect on the cardiovascular system
▪ Review the cardiovascular complications of COVID-related peri-myocarditis
▪ Review the cardiovascular involvement in Multisystem Inflammatory Syndrome in Children (MIS-C)
▪ Review guidelines for returning to play
▪ Review the acute cardiovascular course with post-COVID immunization myocarditis

Mechanisms of Myocardial Injury
4
▪ Severe hypoxia/demand imbalance
▪ Right heart strain
▪ Systemic inflammation/cytokine storm
▪ Stress cardiomyopathy
▪ Coronary artery disease/pre-existing heart disease
▪ Myocarditis

Potential Cardiac Effects of COVID-19
5A Review of the Cardiac and Cardiovascular Effects of COVID-19 in Adults and Children, (1)

Pediatric Cardiac Effects of COVID-19
6
▪ There is limited published data on the incidence of myocardial injury in hospitalized pediatric patients with
acute COVID-19
▪ Pericarditis: Pericarditis as a primarily clinical manifestation of COVID-19 in adolescents (2)
▪ In an initial study of COVID-19 infection in 48 North American children admitted to pediatric ICUs (1)
▪ 83% had serious comorbidities;
▪ 73% presented with respiratory symptoms,
▪ 38% needed invasive ventilation, and
▪ 23% had failure of at least 2 organ systems.

7
Pediatric Myocardial Injury Associated with Acute COVID-19

8
▪ There is little data about the overall occurrence of arrhythmia in the context of acute infection
▪ Single center retrospective chart review included 36 patients with symptoms of COVID, PCR+ and who were
placed on telemetry (8)
Pediatric EKG Changes with Acute COVID-19

9
▪ 28 patients had at least one 12-lead EKG (8)
▪ 10 (35%) had ‘significant findings’
⎻ Low-voltage QRS (N=5)
⎻ ST-segment changes (N=1)
⎻ LV hypertrophy (N=1)
⎻ RV hypertrophy (N=1)
⎻ Left axis deviation (N=1)
⎻ Right axis deviation (N=1)
Pediatric QTc Changes with Acute COVID-19 and Treatment

10
www.crediblemeds.org

11
▪ Presumably, this is an at-risk population, especially those with the most severe forms
▪ Low cardiopulmonary reserve
▪ Chronic hypoxia/cyanosis
▪ Physiology dependent on low pulmonary artery pressures (single ventricle physiology)
▪ Risk for arrhythmia
▪ Underlying genetic syndromes (e.g. Down's syndrome, Digeorge, Heterotaxy, etc)
▪ Associated comorbidities (lung disease, liver impairment, kidney disease, neurological sequalae, impaired
immunity)
COVID-19 and Congenital Heart Disease

Riley Experience – Acute COVID Hospitalization
12
N=155
Age (years, avg) 8.04
Previously Healthy 67 (43%)
Needed ICU 38 (24%)
Clinically significant
arrhythmia1 (0.6%)
No Cardiac Testing 79 (51%)
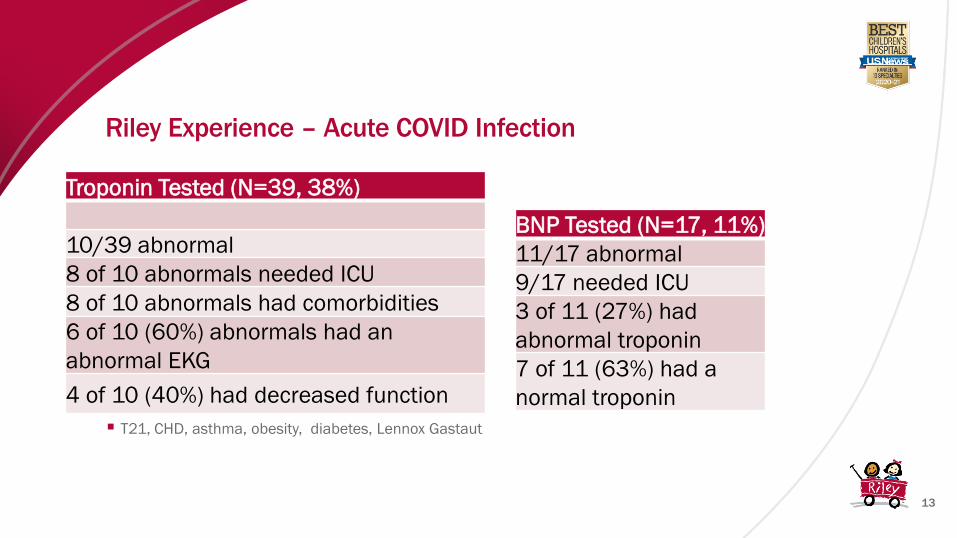
Riley Experience – Acute COVID Infection
13
▪ T21, CHD, asthma, obesity, diabetes, Lennox Gastaut
BNP Tested (N=17, 11%)
11/17 abnormal
9/17 needed ICU
3 of 11 (27%) had
abnormal troponin
7 of 11 (63%) had a
normal troponin
Troponin Tested (N=39, 38%)
10/39 abnormal
8 of 10 abnormals needed ICU
8 of 10 abnormals had comorbidities
6 of 10 (60%) abnormals had an
abnormal EKG
4 of 10 (40%) had decreased function

Riley Experience – Acute COVID Infection
14
EKGs Performed (N=60)
20/60 (33%) normal
22/60 (37%) ST/T wave changes
14/60 (23%) Sinus tachycardia
5/60 (8%) Ventricular hypertrophy
2/60 (3%) Low QRS
3/60 (5%) PVCs
3/60 (5%) Prolonged QT
1/60 (2%) Junctional escape
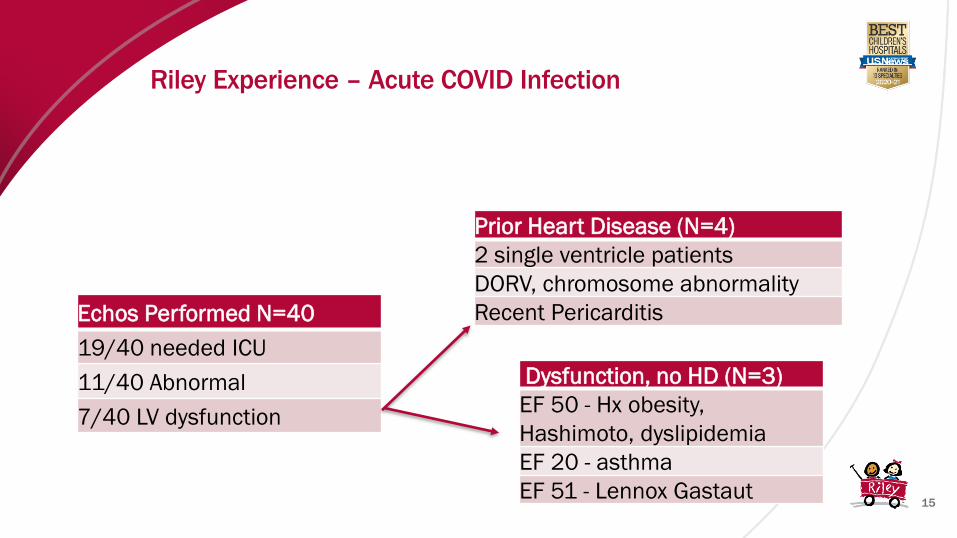
Riley Experience – Acute COVID Infection
15
Echos Performed N=40
19/40 needed ICU
11/40 Abnormal
7/40 LV dysfunction
Prior Heart Disease (N=4)
2 single ventricle patients
DORV, chromosome abnormality
Recent Pericarditis
Dysfunction, no HD (N=3)
EF 50 - Hx obesity,
Hashimoto, dyslipidemia
EF 20 - asthma
EF 51 - Lennox Gastaut

Cardiac Complications in Acute COVID Infection
16
▪ There are cases of myocarditis, pericarditis, arrhythmia and cardiac dysfunction in
Pediatrics with acute COVID19, but they are uncommon in otherwise healthy children
▪ There is some overlap between COVID19 cardiac complications and MIS-C
▪ Predominant cardiac involvement related to COVID19 infections are exertional symptoms
post-COVID or MIS-C

Multisystem Inflammatory Syndrome in Children (MIS-C)
18

19
▪ An individual aged <21 years presenting with fever*, laboratory evidence of inflammation**, and evidence
of clinically severe illness requiring hospitalization, with multisystem (>2) organ involvement (cardiac, renal,
respiratory, hematologic, gastrointestinal, dermatologic or neurological); AND
▪ No alternative plausible diagnoses; AND
▪ Positive for current or recent SARS-CoV-2 infection by RT-PCR, serology, or antigen test; or exposure to a
suspected or confirmed COVID-19 case within the 4 weeks prior to the onset of symptoms.
MIS-C CDC Case Definition
20
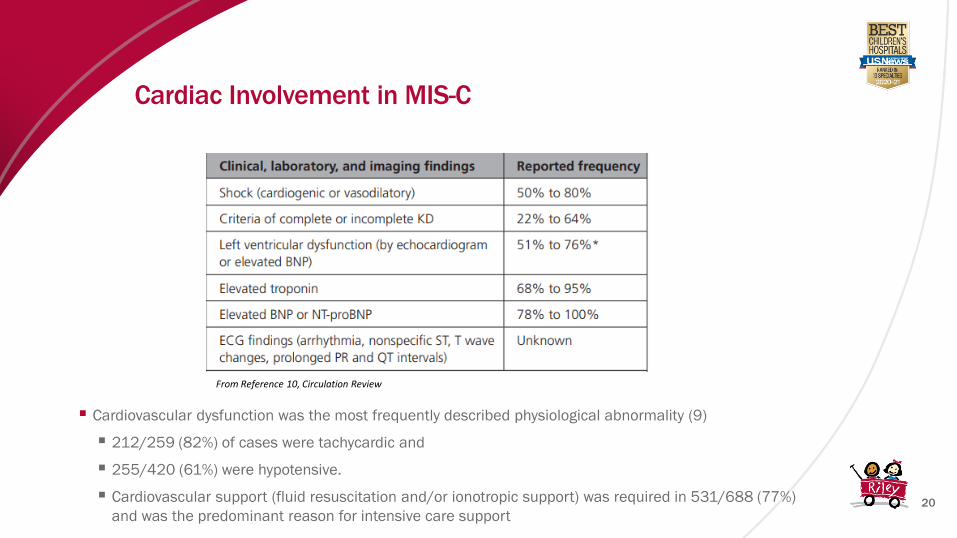
▪ Cardiovascular dysfunction was the most frequently described physiological abnormality (9)
▪ 212/259 (82%) of cases were tachycardic and
▪ 255/420 (61%) were hypotensive.
▪ Cardiovascular support (fluid resuscitation and/or ionotropic support) was required in 531/688 (77%)
and was the predominant reason for intensive care support
Cardiac Involvement in MIS-C
From Reference 10, Circulation Review
21
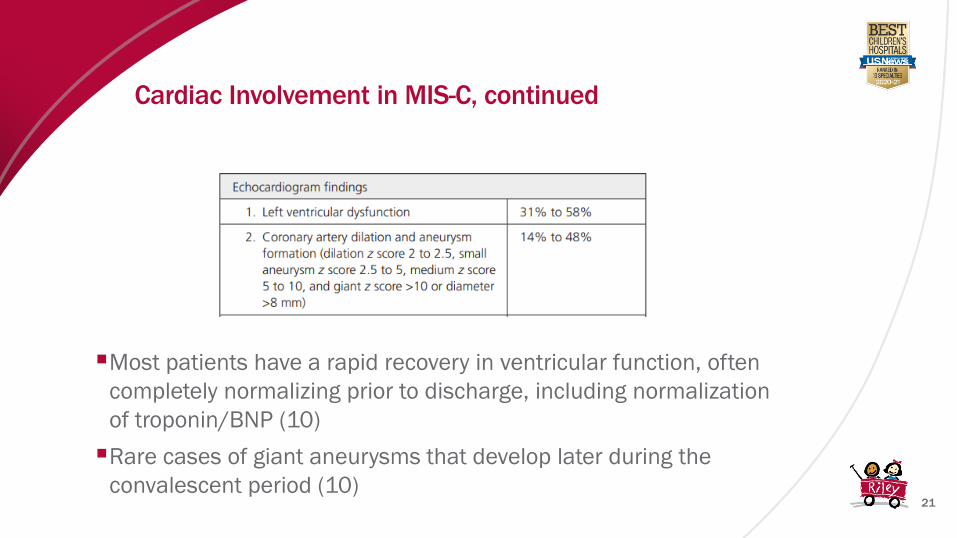
▪Most patients have a rapid recovery in ventricular function, often
completely normalizing prior to discharge, including normalization
of troponin/BNP (10)
▪Rare cases of giant aneurysms that develop later during the
convalescent period (10)
Cardiac Involvement in MIS-C, continued

22
▪Treatment protocols are derived from experience with KD, septic shock,
and myocardial injury treatment (10)
▪ IVIG, steroids, immunomodulatory agents
▪ Fluid resuscitation in small boluses, inotropes, mechanical ventilation, ECMO
▪ Antiplatelet therapy, especially for those with coronary involvement or thrombus
▪ Therapeutic anticoagulation should be strongly considered in all patients with severe ventricular
dysfunction or giant aneurysms (Z score >10, absolute measurement > 8 mm)
Cardiac Involvement in MIS-C, continued
23
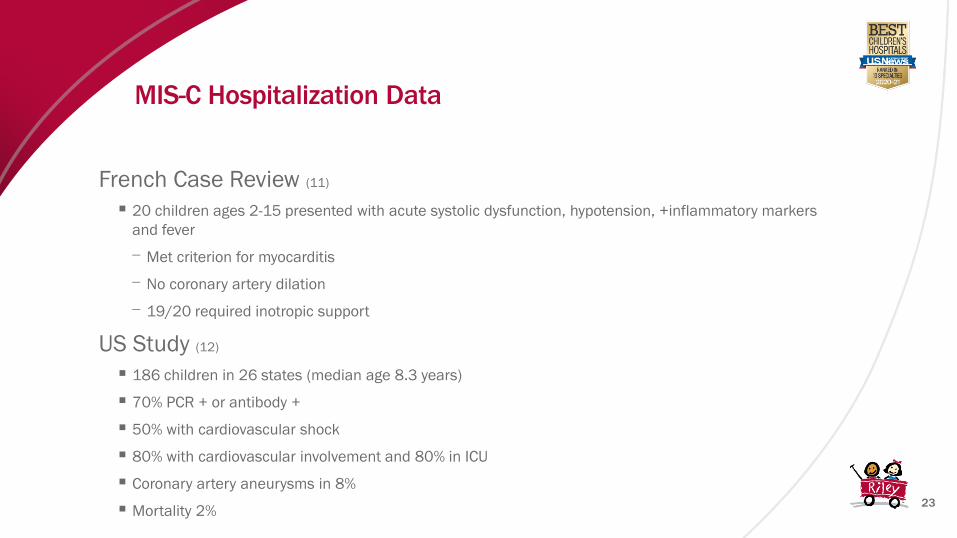
French Case Review (11)
▪ 20 children ages 2-15 presented with acute systolic dysfunction, hypotension, +inflammatory markers
and fever
⎻ Met criterion for myocarditis
⎻ No coronary artery dilation
⎻ 19/20 required inotropic support
US Study (12)
▪ 186 children in 26 states (median age 8.3 years)
▪ 70% PCR + or antibody +
▪ 50% with cardiovascular shock
▪ 80% with cardiovascular involvement and 80% in ICU
▪ Coronary artery aneurysms in 8%
▪ Mortality 2%
MIS-C Hospitalization Data

Riley MIS-C Outpatient Experience
25
▪Outpatient
▪Multidisciplinary MIS-C clinic with Cardiology, Infectious Disease, and Rheumatology.
Occurs twice monthly
▪Follow up scheduled in the first 1-3 weeks post discharge then 4 weeks after with
echo, EKG and labs
▪ Long term follow up and additional testing depend on age, athletic status, and
severity of cardiovascular involvement
⎻ Young, not a competitive athlete, and with normal/normalized testing: follow up at
6 months and 1 year
⎻ Older, competitive athlete, history of cardiac involvement/dysfunction: follow up at
3 month post discharge for additional testing prior to sports clearance (eg. Exercise
stress test, MRI, Holter)

26
▪ N=50
▪ Ages 9 months to 17 years
▪ 66% with cardiovascular involvement (52% with vasoactive support)
▪ 2 week follow-up:
▪ 47% with exertional fatigue
▪ 1 with mild LV systolic dysfunction
▪ Diastolic dysfunction in 11%
▪ 4% with aneurysms, 2% with coronary dilation, 21% lack of tapering
▪ 8 week follow-up:
▪ 12% with exertional fatigue
▪ Diastolic dysfunction in 9%
▪ Coronary abnormalities 12% total
▪ 6 month follow-up:
▪ Diastolic dysfunction in 4% (1 patient) with normal CMRI at 8 weeks
▪ 94% with normalization of cardiac abnormalities
Six Month Post-MIS-C Follow-up (24)

Return to Play
27

28

30
▪Largest prospective multicenter observational cohort study assessed the
prevalence, clinical characteristics, and outcomes of cardiac involvement in
collegiate athletes in the U.S. (13)
▪19,378 athletes were tested, 3,018 tested positive and underwent cardiac
evaluation
▪2820 received at least one of the following tests: EKG, troponin, or
echocardiogram/MRI
SARS-CoV2 Cardiac Involvement in Young Athletes
31
▪ Athletes had asymptomatic infection (33%) (13)
▪ Mild symptoms (29%) were defined as cough, fatigue, gastrointestinal symptoms (nausea, vomiting, and/or
diarrhea), headache, anosmia, ageusia, rhinorrhea, sore throat, or nasopharyngeal congestion
▪ Moderate symptoms (23%) were defined as the presence of COVID toes/fingers, chills, fever, or myalgias.
▪ Cardiopulmonary symptoms (13%) were defined as chest pain, shortness of breath, palpitations, or exercise
intolerance.
▪ Outcomes included adverse cardiovascular events (new clinically significant arrhythmias, clinical heart
failure, or sudden cardiac arrest or death) or hospitalizations related to SARS-CoV-2.
SARS-CoV2 Cardiac Involvement in Young Athletes

32
▪ 21/2820 athletes met criteria for definite (N=11), probable (N=4), or possible (N=6) COVID cardiac involvement (13)
▪ 6 were identified as part of the 198 who underwent primary screening MRI
⎻ 3 of the 6 athletes were asymptomatic or had mild symptoms with normal triad testing
⎻ 2 small pericardial effusion on MRI, 2 abnormal T1 imaging
▪ 15 (71%) were identified by either abnormal triad screening or greater than moderate symptoms
▪ Cardiopulmonary symptoms (OR 3.1) and ANY abnormal triad test (OR 37.4) were predictive of cardiac involvement
▪ No adverse cardiac events were reported in any athletes with definite, probable, or possible cardiac involvement
▪ ***Late gadolinium enhancement on MRA/MRI noted also in some healthy athletes
SARS-CoV2 Cardiac Involvement in Young Athletes

34
Also...No
current
exertional CV
symptoms
▪ Mild: Loss of
taste/smell,
headache, mild
fatigue, URI, mild GI
symptoms
▪ CV symptoms: dyspnea,
exercise intolerance,
chest tightness,
dizziness, syncope,
palpitations

35
Normal Abnormal
Restrict exercise until cardiology referral and clearance
▪ Moderate: Fever,
chills, myalgias,
lethargy, dyspnea,
chest tightness

36
Cards Referral

37

38

Post-Vaccination Myocarditis
39
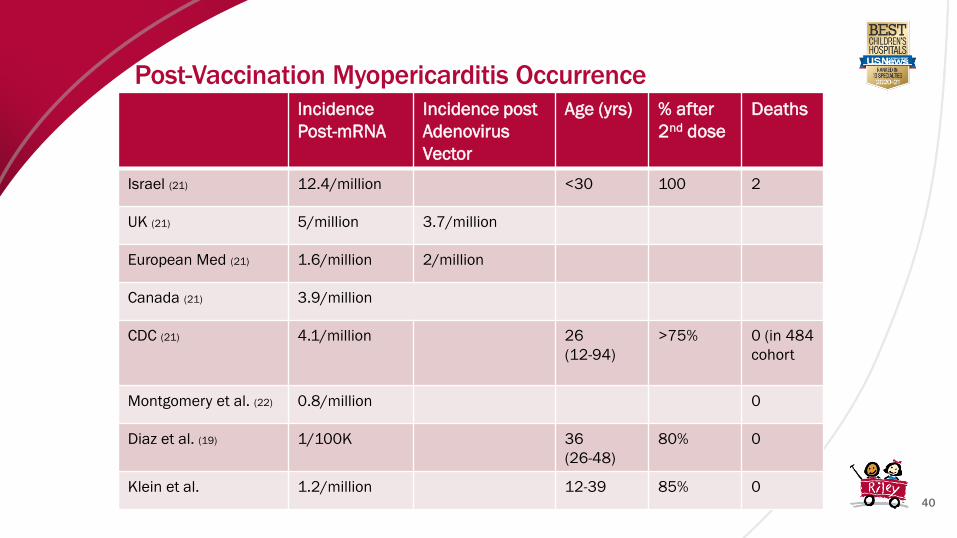
Post-Vaccination Myopericarditis Occurrence
40
Incidence
Post-mRNA
Incidence post
Adenovirus
Vector
Age (yrs) % after
2nd dose
Deaths
Israel (21) 12.4/million <30 100 2
UK (21) 5/million 3.7/million
European Med (21) 1.6/million 2/million
Canada (21) 3.9/million
CDC (21) 4.1/million 26
(12-94)
>75% 0 (in 484
cohort
Montgomery et al. (22) 0.8/million 0
Diaz et al. (19) 1/100K 36
(26-48)
80% 0
Klein et al. 1.2/million 12-39 85% 0

Post-Vaccination MyopericarditisCharacteristics
41
From Diez et al. (19)

American Academy of Pediatrics Insights
42

43
• Acute COVID
• Although less common than in adults, cardiovascular injury does occur in pediatric patients
with acute COVID infection and can also present as primary cardiac involvement
• Cardiac involvement is more common in pediatric patients with comorbidities
• Arrhythmia seems uncommon, although telemetry monitoring is reasonable in critically ill
children
• MIS-C
• Cardiac involvement is VERY common, but usually transient
• Short and mid-term prognosis appears favorable
• Initiation of heart failure or arrythmia medication is rare
Take Away Points
44
• Return-to-Sports
• Cardiac involvement after COVID infection is rare, with vigilance for myocarditis or MIS-C is
necessary
• Risk stratification based on severity of illness and presence of cardiovascular symptoms is
a reasonable way to guide the need for cardiac testing,
• Cardiac findings on MRI have been described in asymptomatic patients with normal
baseline testing
• Post-Vaccination Myocarditis
• Occurs in 1-2% of vaccinated persons, predominately in <30 year olds
• Presents with chest pain
• Majority of biomarkers, symptoms, EKG/echo changes self-resolve within days
Take Away Points

References
46
1. A Review of the Cardiac and Cardiovascular Effects of COVID-19 in Adults and Children, 8/2/2021, Bibhuti B. Das, MD; Tex Heart Inst J (2021) 48 (3): e207395.
2. Dimopoulou, Dimitra MD, PhD*; Spyridis, Nikolaos MD, PhD*; Dasoula, Foteini MD*; Krepis, Panagiotis MD*; Eleftheriou, Eirini MD*; Liaska, Marianthi MD*; Servos, Giorgos MD†;
Maritsi, Despoina MD, PhD*; Tsolia, Maria MD, PhD. The Pediatric Infectious Disease Journal: May 2021 - Volume 40 - Issue 5 - p e197-e199)
3. COVID-19 Cardiac involvement in a 38 day old infant. Barba et al.
4. Pericarditis as the Main Clinical Manifestation of COVID-19 in Adolescents. Dimopoulou et al.
5. Fulminant COVID-19-related myocarditis in an infant. Kesici et al.
6. Fatal Eosinophilic Myocarditis in a Healthy 17-Year-Old Male with Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2c). Craver et al.
7. New onset severe right ventricular failure associated with COVID-19 in a young infant without previous heart disease. Rodriguez-Gonzalez et al.
8. Incidence of arrhythmias and electrocardiograhic abnormalities in symptomatic pediatric patients with PCR-positive SARS-CoV-2 infection, including drug-induced changes in the
corrected QT interval. Samuel et al.
9. Review of Cardiac Involvement in Multisystem Inflammatory Syndrome in Children. Alsaied et al. Circulation. 2021.
10. Multi-system inflammatory syndrome in children & adolescents (MIS-C): A systematic review of clinical features and presentation, Pediatric Respiratory Rev. 6/2021.
11. Grimaud, M., Starck, J., Levy, M. et al. Acute myocarditis and multisystem inflammatory emerging disease following SARS-CoV-2 infection in critically ill children. Ann. Intensive
Care 10, 69 (2020).
12. Feldstein LR et al.; Overcoming COVID-19 Investigators; CDC COVID-19 Response Team. Multisystem Inflammatory Syndrome in U.S. Children and Adolescents. N Engl J Med. 2020 Jul
23;383(4):334-346. doi: 10.1056/NEJMoa2021680. Epub 2020 Jun 29. PMID: 32598831; PMCID: PMC7346765.
13. SARS-CoV-2 Cardiac Involvement in Young Competitive Athletes, Moulson N et al, April 2021
14. Kim JH, Levine BD, Phelan D, et al. Coronavirus Disease 2019 and the Athletic Heart: Emerging Perspectives on Pathology, Risks, and Return to Play. JAMA Cardiol. 2021;6(2):219–227.
doi:10.1001/jamacardio.2020.5890
15. Elliott N, Martin R, Heron N, Elliott J, Grimstead D, Biswas A. Infographic. Graduated return to play guidance following COVID-19 infection. Br J Sports Med. 2020 Oct;54(19):1174-1175.
doi: 10.1136/bjsports-2020-102637. Epub 2020 Jun 22. PMID: 32571796; PMCID: PMC7371566.
16. Unusual Presentation of Acute Perimyocarditis Following SARS-COV-2 mRNA-1237 Moderna Vaccination, Khogali F et al.
17. Acute Myocarditis Following mRNA-1273 SARS-CoV-2 Vaccination, Williams C et al.
18. Myocarditis and Pe4ricarditis after vaccination for COVID-19, Hudson et al, July 2021
19. Myocarditis and Pericarditis After Vaccination for COVID-19, Diaz G et al, August 2021
20. Perimyocarditis in Adolescents After Pfizer-BioNTech COVID-19 Vaccine, Tamo et al
21. Pepe et al, 2021, Myocarditis, Pericarditis and Cardiomyopathy after COVID-19 Vaccination
22. Montgomery J, Ryan M, Engler R, et al. Myocarditis Following Immunization With mRNA COVID-19 Vaccines in Members of the US Military. JAMA Cardiol. 2021;6(10):1202–1206.
doi:10.1001/jamacardio.2021.2833
23. Klein et al, 2021, Myocarditis Analyses in the Vaccine Safety Datalink: Rapid Cycle Analyses and “Head-to-Head” Product Comparisons
24. Capone et al., Six Month Follow-up of Patients With Multi-System Inflammatory Syndrome in Children. Pediatrics Oct 2021, 148 (4) e2021050973; DOI: 10.1542/peds.2021-050973