coxibs and heart disease: what we have learned and … sota 7-06 to 8-08/coxibs and heart disease -...
TRANSCRIPT

doi:10.1016/j.jacc.2006.10.003 2007;49;1-14; originally published online Dec 12, 2006; J. Am. Coll. Cardiol.
Ignatius Gerardo E. Zarraga, and Ernst R. Schwarz Know
Coxibs and Heart Disease: What We Have Learned and What Else We Need to
This information is current as of August 9, 2008
http://content.onlinejacc.org/cgi/content/full/49/1/1located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by on August 9, 2008 content.onlinejacc.orgDownloaded from

T(pfs(fpte2is
cteNaetwerwn
FoDC
a
Journal of the American College of Cardiology Vol. 49, No. 1, 2007© 2007 by the American College of Cardiology Foundation ISSN 0735-1097/07/$32.00P
STATE-OF-THE-ART PAPER
Coxibs and Heart DiseaseWhat We Have Learned and What Else We Need to Know
Ignatius Gerardo E. Zarraga, MD,* Ernst R. Schwarz, MD, PHD, FACC*†
Galveston, Texas; and Los Angeles, California
Since their approval in 1998, the popularity of selective cyclooxygenase-2 (COX2) inhibitors has swung from adomination of drug sales to serious disputes about their cardiovascular safety. Despite the numerous studies onCOX2 inhibitors that have emerged, drawing conclusions about their cardiovascular safety has been complicatedby conflicting results, underpowered clinical trials, and the lack of a placebo group and use of post hoc analysesin many trials. Nonetheless, certain conclusions can be made with reasonable accuracy. This review addressesthe controversy in 3 segments. It begins with a discussion of the several mechanisms proposed to explain how selec-tive COX2 inhibition impacts the cardiovascular system. This is followed by a recount of the several clinical studiesthat delved into the cardiovascular outcomes associated with COX2 inhibitors. Finally, answers to key questions areprovided to assist the clinician in devising a systematic approach to the risk-benefit analysis of COX2 inhibitors in ac-tual practice. (J Am Coll Cardiol 2007;49:1–14) © 2007 by the American College of Cardiology Foundation
ublished by Elsevier Inc. doi:10.1016/j.jacc.2006.10.003
ttiiccFcpcU
dwCa(vcsadcaVpesd
r
he transformation of arachidonic acid to prostaglandin H2PGH2) is a step that commits arachidonic acid down theath of prostaglandin-thromboxane synthesis. This trans-ormation is catalyzed by cytosolic prostaglandin G/Hynthase, more commonly known as cyclooxygenaseCOX). Prostaglandin H2 is an unstable intermediate and isurther converted to one of many prostanoids, such asrostacyclin (PGI2) and thromboxane A2 (TXA2), byissue-specific isomerases. As early as 1987, evidencemerged showing that the COX enzyme probably existed in
isoforms (1). Today it is well established that thesesoforms, COX1 and COX2, exist and are encoded byeparate genes on different chromosomes.
Cyclooxygenase inhibition formed the basis for the suc-ess of non-steroidal anti-inflammatory drugs (NSAIDs) inreating a variety of pain syndromes. The drawback, how-ver, was that every year, 2% to 4% of patients takingSAIDs suffered from symptomatic gastrointestinal ulcers
nd their complications (2). As the science behind the COXnzyme progressed, it became apparent that COX2 inhibi-ion mediated the anti-inflammatory effects of NSAIDs,hereas COX1 inhibition was responsible for the adverse
ffects on the gastrointestinal tract. It therefore becameeasonable to assume that inhibiting COX2 selectivelyould result in the same anti-inflammatory benefits thatonselective NSAIDs provided but with fewer gastrointes-
rom the *Division of Cardiology, Department of Internal Medicine, The Universityf Texas Medical Branch, Galveston, Texas; and the †Division of Cardiology,epartment of Internal Medicine, Cedars-Sinai Medical Center and University ofalifornia Los Angeles, Los Angeles, California.
dManuscript received June 27, 2006; revised manuscript received July 31, 2006,
ccepted August 8, 2006.
content.onlinejaDownloaded from
inal side effects. This rekindled the interest of pharmaceu-ical industries in manufacturing new analgesic and anti-nflammatory medications known as selective COX2nhibitors or coxibs. In 1995, the first generation of coxibs,elecoxib (by Monsanto) and rofecoxib (by Merck), enteredlinical trials. In 1998, celecoxib was approved by the U.S.ood and Drug Administration (FDA), followed by rofe-oxib in 1999. These drugs soon dominated therescription-drug market for NSAIDs. By October 2000,elecoxib and rofecoxib had sales exceeding $3 billion in the.S. (3).At the time that COX2 inhibitors were approved, ran-
omized trials aimed at proving their gastrointestinal safetyere still ongoing. It was not until 2000 that 2 large studies,LASS (Celecoxib Long-Term Arthritis Safety Study) (2)
nd VIGOR (Vioxx Gastrointestinal Outcomes Research)4), showed their superior gastrointestinal profile over con-entional NSAIDs. Both studies, however, were not free ofontroversy. For the CLASS trial, the gastrointestinaluperiority of celecoxib in its 6-month data became disput-ble when this superiority failed to manifest in its 12-monthata (5). On the other hand, the VIGOR study raisedoncerns about the cardiovascular safety of rofecoxib. Tomplify this concern, near the time of completion of theIGOR study, preliminary evidence supporting the biologiclausibility of COX2-induced adverse cardiovascular eventsmerged. From hereon, the use of coxibs became plagued byafety concerns on the basis of both mechanistic and clinicalata.As a result of the evolving understanding of the potential
isks of selective COX2 inhibition, in 1999, Merck intro-
uced a standard operating procedure to evaluate andby on August 9, 2008 cc.org

dsmpAsIicwTba
tcfva(vicdovagc(air
if
mCttwo
Mto
CtCebepeoabssaaaCmap(ctttdtg(kbtscvt
ctad
2 Zarraga and Schwarz JACC Vol. 49, No. 1, 2007Coxibs and Heart Disease January 2/9, 2007:1–14
adjudicate cardiovascular eventsin all ongoing and future rofe-coxib clinical trials (6). In 2002,the FDA also issued a new warn-ing in the package insert of rofe-coxib, stating that “. . . cautionshould be exercised when Vioxxis used in patients with a medicalhistory of ischemic heart dis-ease.” This decision of the FDAto opt for a mere label change andnot a more practice-changing in-tervention, such as compellingmanufacturers to initiate trials oncardiovascular safety, has beenhighly criticized (7). As a matterof fact, for a good number ofyears after the VIGOR trialstirred controversy, no random-ized controlled trial was initiatedto address the cardiovascular tox-icity of coxibs as a primary endpoint. Instead, more trials were
esigned to show the efficacy of coxibs for other indications,uch as the prevention of recurrent colonic polyps, manage-ent of postoperative pain, and slowing down of the
rogression of Alzheimer’s dementia. One such trial was thePPROVe (Adenomatous Polyp Prevention on Vioxx)
tudy (8), which now stands among landmark clinical trials.t was prematurely terminated after investigators found anncreased cardiovascular risk among patients taking rofe-oxib, and served as the basis for the immediate worldwideithdrawal of rofecoxib by Merck on September 30, 2004.housands of lawsuits against Merck followed this event,ecause by this time an estimated 80 million people hadlready taken the drug (9).
Not too long thereafter, the results of 2 more randomizedrials of coxibs were published and showed unfavorableardiovascular outcomes as well. One was a celecoxib trialor colonic adenoma prevention (10), and the other was aaldecoxib/parecoxib trial for the management of postoper-tive pain after coronary artery bypass grafting (CABG)11). In addition to being linked with a heightened cardio-ascular risk, valdecoxib and parecoxib had previously beenmplicated in life-threatening hypersensitivity reactions, in-luding anaphylaxis, angioedema, Stevens-Johnson syn-rome, and toxic epidermal necrolysis (12). Consequently,n April 7, 2005, the FDA requested that Pfizer removealdecoxib from the market. Furthermore, the FDA issued
cautionary note against the coxibs, and NSAIDs ineneral: “. . . an increased risk of serious adverse [cardiovas-ular] events appears to be a class effect of NSAIDsexcluding aspirin). The FDA has requested that the pack-ge insert for all NSAIDs, including Celebrex, be revised tonclude a boxed warning to highlight the potential increased
Abbreviationsand Acronyms
CABG � coronary arterybypass grafting
CAD � coronary arterydisease
CHF � congestive heartfailure
COX � cyclooxygenase
FDA � Food and DrugAdministration
HR � hazard ratio
MI � myocardial infarction
NSAID � non-steroidal anti-inflammatory drug
OA � osteoarthritis
PG � prostaglandin
PPI � proton pumpinhibitor
RA � rheumatoid arthritis
TX � thromboxane
isk of [cardiovascular] events and . . . to include a contra- ucontent.onlinejaDownloaded from
ndication for use in patients immediately postoperativerom CABG” (13).
In the following discussion, we highlight the severalechanisms that have emerged to explain how selectiveOX2 inhibition impacts the cardiovascular system. We
hen review the landmark clinical studies that delved intohe cardiovascular outcomes associated with coxibs. Finally,e present a systematic approach to the risk-benefit analysisf coxibs in actual clinical practice.
echanisms Underlyinghe Cardiovascular Effectsf Selective COX2 Inhibitors
yclooxygenase-1 is expressed constitutively in most cellypes and is the only functioning COX in mature platelets.yclooxygenase-2, on the other hand, is an isoform with an
xpression that is induced by inflammatory stimuli such asacterial endotoxin and cytokines. Induction of COX2xpression has also been demonstrated in atheromatouslaques (14,15) and neoplasms (16). This led to the hypoth-sis that COX2 inhibition might be useful in the treatmentr prevention of atherosclerosis and various cancers. In fact,few reports have suggested that COX2 inhibition might
e cardioprotective. For example, Dinchuk et al. (17) havehown that COX2-knockout mice developed cardiac fibro-is. Two histologic studies, performed by Baker et al. (14)nd Schonbeck et al. (15), showed the presence of COX2 intherosclerotic lesions of native and transplanted coronaryrteries, but not in normal coronary arteries. Furthermore,OX2 expression was localized to macrophages/foam cells,edial smooth muscle cells, and endothelial cells within the
therosclerotic plaque, all of which are established keylayers in atherogenesis. A similar study by Cipollone et al.18) on carotid plaques showed a significantly higher con-entration of COX2 in plaques associated with a recentransient ischemic attack or stroke compared with asymp-omatic plaques. Cyclooxygenase 2 expression also appearso be induced by many of the same stimuli implicated in theevelopment of atherosclerosis, including free radicals (19),umor necrosis factor, interleukin-1 (20), platelet-derivedrowth factor (21), and increased arterial wall shear stress22). Finally, because inflammation of the endothelium isnown to diminish its capacity to produce nitric oxide, it haseen suggested that COX2 inhibition can improve endo-helial function in this setting. This was shown by 2 small,hort-term studies (�2 weeks in duration) in which cele-oxib led to significant improvements in flow-mediatedasodilation compared with placebo in patients with hyper-ension or coronary artery disease (CAD) (23,24).
In reality, predicting the effect of COX2 inhibition on theardiovascular system has not been straightforward. Al-hough COX2 can be viewed as a “bad” player in thetherosclerotic process based on most of the aforementionedata, it can also be regarded as a “good” player if its
p-regulation is thought of as a compensatory mechanismby on August 9, 2008 cc.org

tbbsptp(iT(siAbb
ohtpPAesassrsebthCwCcACamo
RC
TiaVmc7ai
ctegsedmtwttuihtFwapn
astaptfretPdkrTraouraRDprg
(astwt
3JACC Vol. 49, No. 1, 2007 Zarraga and SchwarzJanuary 2/9, 2007:1–14 Coxibs and Heart Disease
o help maintain vascular health. In addition, in 1998, itecame apparent that the 2 COX isoforms affected thealance of vasoactive prostanoids differently. Several studiesuggested that TXA2, a vasoconstrictor and promoter oflatelet aggregation, was largely COX1-derived, whereashe synthesis of the vasodilator and potent inhibitor oflatelet aggregation, PGI2, was linked to COX2 induction25,26). Specifically, the up-regulation of COX2 (e.g., bynterleukin-1�) shifted arachidonic acid metabolism fromXA2 synthesis to the preferential production of PGI2
27). Furthermore, although nonselective COX inhibitors,uch as aspirin and ibuprofen, suppressed TXA2 productionn platelets, selective COX2 inhibitors did not (25,26).ltogether, a clear suggestion was made that COX2 inhi-ition could tip the vascular homeostasis into a prothrom-otic state.More investigations have since led to the unraveling of
ther mechanisms behind coxib-induced cardiovasculararm. For example, it has been suggested in animal modelshat COX2 mediates the cardioprotective effects of the latehase of ischemic preconditioning and that PGE2 andGI2 are the likely effectors of such protection (28,29).ccordingly, COX2 inhibition can block the protective
ffect of late-phase preconditioning against myocardialtunning and infarction. In another study of mice models oftherosclerosis, antagonism of the TXA2 receptor washown to retard atherogenesis, but the combination ofelective COX2 inhibition and TXA2-receptor antagonismesulted in atherosclerotic lesions that lacked fibrotic caps,uggesting a destabilizing effect on these plaques (30). Wut al. (31) also showed that when angiogenesis was inducedy vascular endothelial growth factor, cell proliferation andhe formation of vascular structures were increased inuman umbilical vein endothelial cells that overexpressedOX2, whereas cell proliferation was significantly reducedhen the endothelial cells were pretreated with a selectiveOX2 inhibitor. These findings suggest that COX2 may be
ardioprotective, in part because of its role in angiogenesis.s will be discussed in later sections of this review, someOX2 inhibitors have been associated with hypertension
nd oxidative modification of lipids, providing yet anotherechanism by which these drugs might produce adverse
utcomes.
isk of Ischemicardiovascular Events With Rofecoxib
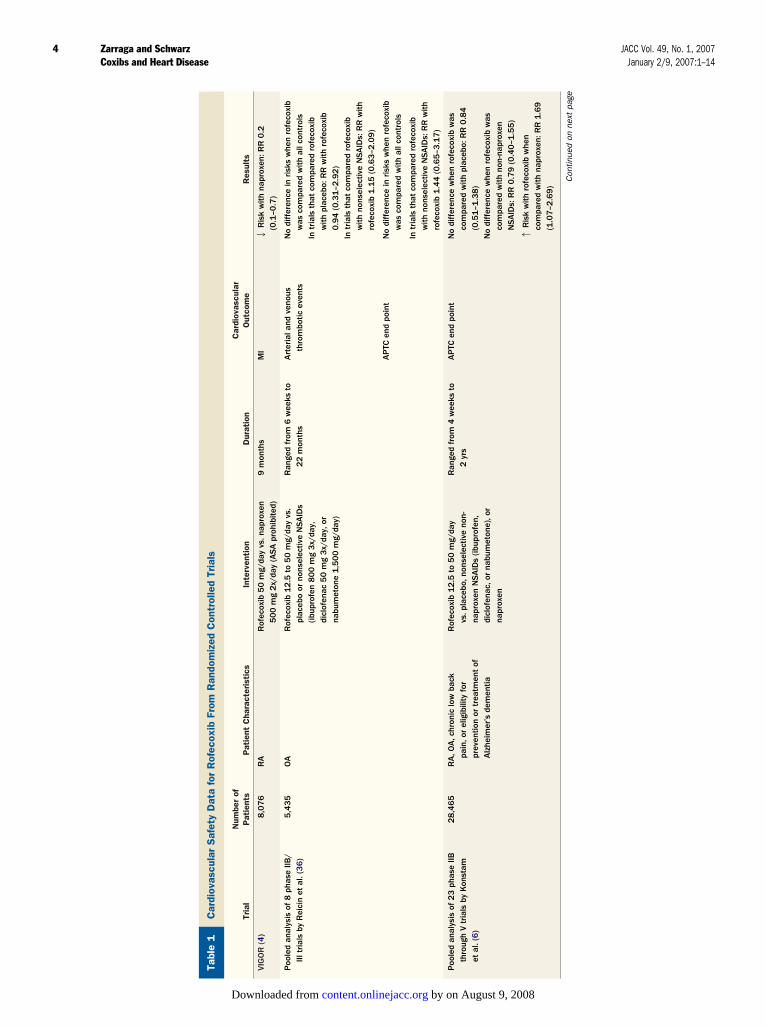
he first major postmarketing multicenter trials on COX2nhibitors were the CLASS and VIGOR trials (Tables 1nd 2) (2,4). Although safety concerns were raised by theIGOR trial, neither of these trials convinced the entireedical community of the increased cardiovascular risk of
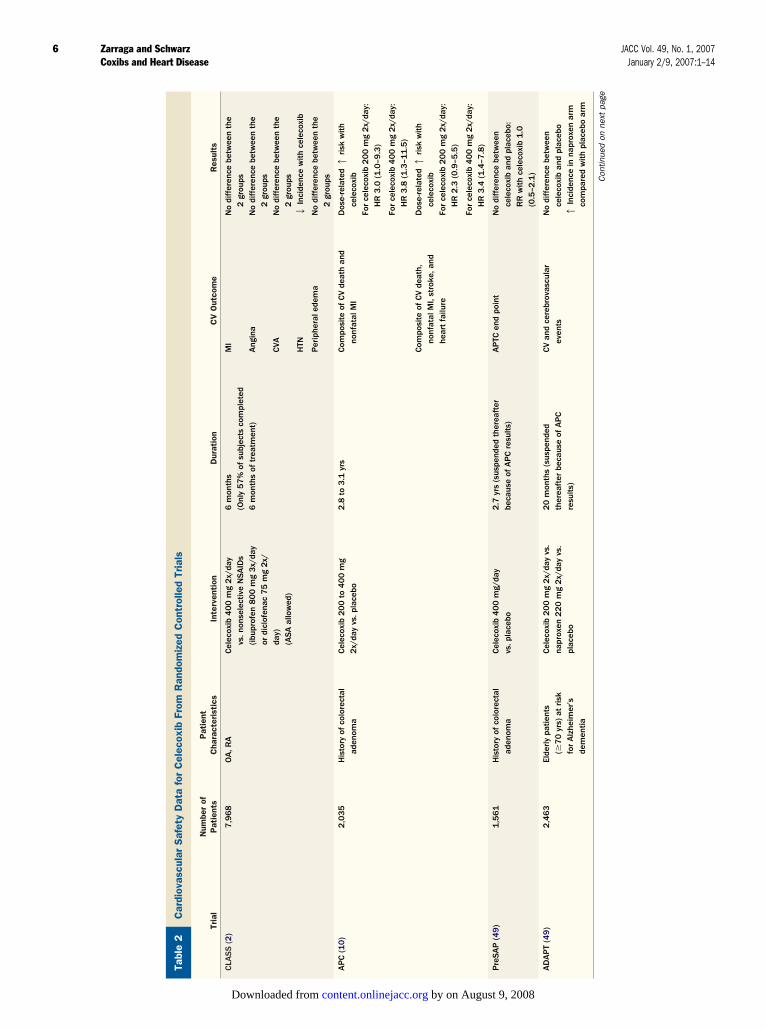
oxib use. The CLASS trial was a double-blind trial of,968 patients with osteoarthritis (OA) or rheumatoidrthritis (RA) who were randomized to high-dose celecoxib,
buprofen, or diclofenac. Patients were allowed to take gcontent.onlinejaDownloaded from
ardioprotective doses of aspirin. At the end of 6 months,here was no difference in the incidence of cardiovascularvents between the celecoxib and nonselective NSAIDroups, irrespective of aspirin use. The VIGOR study was aimilar trial that randomized 8,076 patients with RA toither 50 mg rofecoxib daily or 500 mg naproxen twiceaily. As in the CLASS trial, the coxib dose was over theaximum recommended dose for long-term administra-
ion, and was in keeping with the objective of the study,hich was to rigorously assess the gastrointestinal safety of
he drug even at supratherapeutic doses. Unlike the CLASSrial, patients in the VIGOR trial were prohibited fromsing aspirin. During a median follow-up of 9 months, thencidence of myocardial infarction (MI) was several-foldigher in the rofecoxib group: 4-fold higher as reported byhe VIGOR study group; 5-fold higher as reported in theDA files (32). Because the study lacked a placebo arm, itas unclear how much of the increased risk of MI was
ttributable to a harmful effect of high-dose rofecoxib, arotective effect of naproxen, chance (because of the smallumber of events), or a combination of these factors.When this unexpected outcome from rofecoxib unfolded
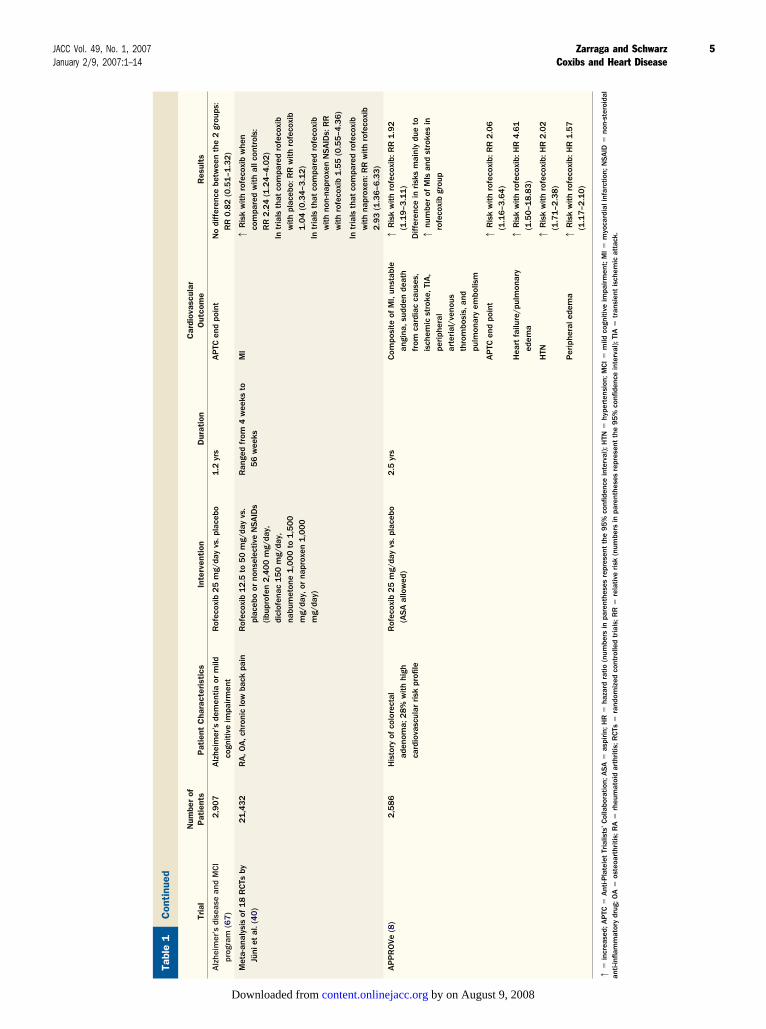
nd mechanisms to explain its biologic plausibility emerged,everal observational studies were published to help confirmhe finding, but the results were conflicting (33–35). Poolednalyses of previous randomized trials likewise did notrovide a clear answer to the issue. Three pooled analyses ofrials before and after the marketing of rofecoxib, publishedrom 2001 to 2003, supported the cardiovascular safety ofofecoxib (Table 1). These included the studies by Konstamt al. (6) and Reicin et al. (36), which found similar rates ofhrombotic events and similar rates of the APTC (Anti-latelet Trialists’ Collaboration) end point (combined inci-ence of death from cardiovascular, hemorrhagic, or un-nown cause; nonfatal MI; and nonfatal stroke) withofecoxib, placebo, and comparator non-naproxen NSAIDs.he data evaluated by Konstam et al. (6) included the
esults of the VIGOR trial and indicated that naproxen wasn outlier NSAID in that it was associated with a lower riskf cardiovascular events compared with rofecoxib. In anpdated review, Weir et al. (37) reiterated in 2003 thatofecoxib was safe from a cardiovascular standpoint. Inddition to the pooled analyses of Konstam et al. (6) andeicin et al. (36), they included data from the Alzheimer’sisease and Mild Cognitive Impairment program, a com-
osite of placebo-controlled trials that again showed similarates of cardiovascular events in the rofecoxib and placeboroups.
In contrast to the above data, in 2001, Mukherjee et al.38) published a review highlighting the cardiovascular riskssociated with coxibs. In their analysis of the VIGORtudy, the relative risk of an adjudicated cardiovascularhrombotic event with rofecoxib compared with naproxenas 2.38 (95% confidence interval [CI] 1.39 to 4.00). They
hen looked into the rate of similar events in a placebo
roup, which they derived from a meta-analysis of 4 aspirinby on August 9, 2008 cc.org
rdio
vasc
ular
Saf
ety
Dat
afo
rR
ofec
oxib
From
Ran
dom
ized
Con
trol
led
Tria
ls
able
1C
ardi
ovas
cula
rS
afet
yD
ata
for
Rof
ecox
ibFr
omR
ando
miz
edC
ontr
olle
dTr
ials
Tria
lN
umbe
rof
Pat
ient
sP
atie
ntC
hara
cter
isti
csIn
terv
enti
onD
urat
ion
Car
diov
ascu
lar
Out
com
eR
esul
ts
IGO
R(4
)8
,07
6R
AR
ofec
oxib
50
mg/
day
vs.n
apro
xen
50
0m
g2
x/da
y(A
SA
proh
ibite
d)9
mon
ths
MI
2R
isk
with
napr
oxen
:RR
0.2
(0.1
–0.7
)
oole
dan
alys
isof
8ph
ase
IIB/
IIItr
ials
byR
eici
net
al.(
36
)5
,43
5O
AR
ofec
oxib
12
.5to
50
mg/
day
vs.
plac
ebo
orno
nsel
ectiv
eN
SA
IDs
(ibup
rofe
n8
00
mg
3x/
day,
dicl
ofen
ac5
0m
g3
x/da
y,or
nabu
met
one
1,5
00
mg/
day)
Ran
ged
from
6w
eeks
to2
2m
onth
sA
rter
iala
ndve
nous
thro
mbo
ticev
ents
No
diff
eren
cein
risk
sw
hen
rofe
coxi
bw
asco
mpa
red
with
allc
ontr
ols
Intr
ials
that
com
pare
dro
feco
xib
with
plac
ebo:
RR
with
rofe
coxi
b0
.94
(0.3
1–2
.92
)In
tria
lsth
atco
mpa
red
rofe
coxi
bw
ithno
nsel
ectiv
eN
SA
IDs:
RR
with
rofe
coxi
b1
.15
(0.6
3–2
.09
)
AP
TCen
dpo
int
No
diff
eren
cein
risk
sw
hen
rofe
coxi
bw
asco
mpa
red
with
allc
ontr
ols
Intr
ials
that
com
pare
dro
feco
xib
with
nons
elec
tive
NSA
IDs:
RR
with
rofe
coxi
b1
.44
(0.6
5–3
.17
)
oole
dan
alys
isof
23
phas
eIIB
thro
ugh
Vtr
ials
byK
onst
amet
al.(
6)
28
,46
5R
A,O
A,c
hron
iclo
wba
ckpa
in,o
rel
igib
ility
for
prev
entio
nor
trea
tmen
tof
Alz
heim
er’s
dem
entia
Rof
ecox
ib1
2.5
to5
0m
g/da
yvs
.pla
cebo
,non
sele
ctiv
eno
n-na
prox
enN
SA
IDs
(ibup
rofe
n,di
clof
enac
,or
nabu
met
one)
,or
napr
oxen
Ran
ged
from
4w
eeks
to2
yrs
AP
TCen
dpo
int
No
diff
eren
cew
hen
rofe
coxi
bw
asco
mpa
red
with
plac
ebo:
RR
0.8
4(0
.51
–1.3
8)
No
diff
eren
cew
hen
rofe
coxi
bw
asco
mpa
red
with
non-
napr
oxen
NSA
IDs:
RR
0.7
9(0
.40
–1.5
5)
1R
isk
with
rofe
coxi
bw
hen
com
pare
dw
ithna
prox
en:R
R1
.69
(1.0
7–2
.69
)
Con
tinue
don
next
page
4 Zarraga and Schwarz JACC Vol. 49, No. 1, 2007Coxibs and Heart Disease January 2/9, 2007:1–14
Ca T V P P
by on August 9, 2008 content.onlinejacc.orgDownloaded from
ntin
ued
able
1C
onti
nued
Tria
lN
umbe
rof
Pat
ient
sP
atie
ntC
hara
cter
isti
csIn
terv
enti
onD
urat
ion
Car
diov
ascu
lar
Out
com
eR
esul
ts
lzhe
imer
’sdi
seas
ean
dM
CI
prog
ram
(67
)2
,90
7A
lzhe
imer
’sde
men
tiaor
mild
cogn
itive
impa
irm
ent
Rof
ecox
ib2
5m
g/da
yvs
.pla
cebo
1.2
yrs
AP
TCen
dpo
int
No
diff
eren
cebe
twee
nth
e2
grou
ps:
RR
0.8
2(0
.51
–1.3
2)
eta-
anal
ysis
of1
8R
CTs
byJü
niet
al.(
40
)2
1,4
32
RA
,OA
,chr
onic
low
back
pain
Rof
ecox
ib1
2.5
to5
0m
g/da
yvs
.pl
aceb
oor
nons
elec
tive
NSA
IDs
(ibup
rofe
n2
,40
0m
g/da
y,di
clof
enac
15
0m
g/da
y,na
bum
eton
e1
,00
0to
1,5
00
mg/
day,
orna
prox
en1
,00
0m
g/da
y)
Ran
ged
from
4w
eeks
to5
6w
eeks
MI
1R
isk
with
rofe
coxi
bw
hen
com
pare
dw
ithal
lcon
trol
s:R
R2
.24
(1.2
4–4
.02
)In
tria
lsth
atco
mpa
red
rofe
coxi
bw
ithpl
aceb
o:R
Rw
ithro
feco
xib
1.0
4(0
.34
–3.1
2)
Intr
ials
that
com
pare
dro
feco
xib
with
non-
napr
oxen
NSA
IDs:
RR
with
rofe
coxi
b1
.55
(0.5
5–4
.36
)
Intr
ials
that
com
pare
dro
feco
xib
with
napr
oxen
:RR
with
rofe
coxi
b2
.93
(1.3
6–6
.33
)
PP
RO
Ve(8
)2
,58
6H
isto
ryof
colo
rect
alad
enom
a;2
8%
with
high
card
iova
scul
arrisk
profi
le
Rof
ecox
ib2
5m
g/da
yvs
.pla
cebo
(ASA
allo
wed
)2
.5yr
sCom
posi
teof
MI,
unst
able
angi
na,s
udde
nde
ath
from
card
iac
caus
es,
isch
emic
stro
ke,T
IA,
periph
eral
arte
rial
/ven
ous
thro
mbo
sis,
and
pulm
onar
yem
bolis
m
1R
isk
with
rofe
coxi
b:R
R1
.92
(1.1
9–3
.11
)D
iffer
ence
inrisk
sm
ainl
ydu
eto
1nu
mbe
rof
MIs
and
stro
kes
inro
feco
xib
grou
p
AP
TCen
dpo
int
1R
isk
with
rofe
coxi
b:R
R2
.06
(1.1
6–3
.64
)
Hea
rtfa
ilure
/pul
mon
ary
edem
a1
Ris
kw
ithro
feco
xib:
HR
4.6
1(1
.50
–18
.83
)
HTN
1R
isk
with
rofe
coxi
b:H
R2
.02
(1.7
1–2
.38
)
Per
iphe
rale
dem
a1
Ris
kw
ithro
feco
xib:
HR
1.5
7(1
.17
–2.1
0)
incr
ease
d;A
PTC
�A
nti-P
late
let
Tria
lists
’Col
labo
ratio
n;A
SA
�as
pirin;
HR
�ha
zard
ratio
(num
bers
inpa
rent
hese
sre
pres
ent
the
95
%co
nfide
nce
inte
rval
);H
TN�
hype
rten
sion
;MCI�
mild
cogn
itive
impa
irm
ent;
MI�
myo
card
iali
nfar
ctio
n;N
SA
ID�
non-
ster
oida
l-in
flam
mat
ory
drug
;OA
�os
teoa
rthr
itis;
RA
�rh
eum
atoi
dar
thritis
;RCTs
�ra
ndom
ized
cont
rolle
dtr
ials
;RR
�re
lativ
erisk
(num
bers
inpa
rent
hese
sre
pres
ent
the
95
%co
nfide
nce
inte
rval
);TI
A�
tran
sien
tis
chem
icat
tack
.
5JACC Vol. 49, No. 1, 2007 Zarraga and SchwarzJanuary 2/9, 2007:1–14 Coxibs and Heart Disease
Co T A M A
1�
anti
by on August 9, 2008 content.onlinejacc.orgDownloaded from
Car
diov
ascu
lar
Saf
ety
Dat
afo
rC
elec
oxib
From
Ran
dom
ized
Con
trol
led
Tria
ls
able
2C
ardi
ovas
cula
rS
afet
yD
ata
for
Cel
ecox
ibFr
omR
ando
miz
edC
ontr
olle
dTr
ials
Tria
lN
umbe
rof
Pat
ient
sP
atie
ntC
hara
cter
isti
csIn
terv
enti
onD
urat
ion
CV
Out
com
eR
esul
ts
LASS
(2)
7,9
68
OA
,RA
Cel
ecox
ib4
00
mg
2x/
day
vs.n
onse
lect
ive
NSA
IDs
(ibup
rofe
n8
00
mg
3x/
day
ordi
clof
enac
75
mg
2x/
day)
(ASA
allo
wed
)
6m
onth
s(O
nly
57
%of
subj
ects
com
plet
ed6
mon
ths
oftr
eatm
ent)
MI
Ang
ina
CVA
HTN
No
diff
eren
cebe
twee
nth
e2
grou
psN
odi
ffer
ence
betw
een
the
2gr
oups
No
diff
eren
cebe
twee
nth
e2
grou
ps2
Inci
denc
ew
ithce
leco
xib
Per
iphe
rale
dem
aN
odi
ffer
ence
betw
een
the
2gr
oups
PC
(10
)2
,03
5H
isto
ryof
colo
rect
alad
enom
aCel
ecox
ib2
00
to4
00
mg
2x/
day
vs.p
lace
bo2
.8to
3.1
yrs
Com
posi
teof
CV
deat
han
dno
nfat
alM
ID
ose-
rela
ted1
risk
with
cele
coxi
bFo
rce
leco
xib
20
0m
g2
x/da
y:H
R3
.0(1
.0–9
.3)
For
cele
coxi
b4
00
mg
2x/
day:
HR
3.8
(1.3
–11
.5)
Com
posi
teof
CV
deat
h,no
nfat
alM
I,st
roke
,and
hear
tfa
ilure
Dos
e-re
late
d1
risk
with
cele
coxi
bFo
rce
leco
xib
20
0m
g2
x/da
y:H
R2
.3(0
.9–5
.5)
For
cele
coxi
b4
00
mg
2x/
day:
HR
3.4
(1.4
–7.8
)
reSA
P(4
9)
1,5
61
His
tory
ofco
lore
ctal
aden
oma
Cel
ecox
ib4
00
mg/
day
vs.p
lace
bo2
.7yr
s(s
uspe
nded
ther
eaft
erbe
caus
eof
AP
Cre
sults
)A
PTC
end
poin
tN
odi
ffer
ence
betw
een
cele
coxi
ban
dpl
aceb
o:R
Rw
ithce
leco
xib
1.0
(0.5
–2.1
)
DA
PT
(49
)2
,46
3El
derly
patie
nts
(�7
0yr
s)at
risk
for
Alz
heim
er’s
dem
entia
Cel
ecox
ib2
00
mg
2x/
day
vs.
napr
oxen
22
0m
g2
x/da
yvs
.pl
aceb
o
20
mon
ths
(sus
pend
edth
erea
fter
beca
use
ofA
PC
resu
lts)
CV
and
cere
brov
ascu
lar
even
tsN
odi
ffer
ence
betw
een
cele
coxi
ban
dpl
aceb
o1
Inci
denc
ein
napr
oxen
arm
com
pare
dw
ithpl
aceb
oar
m
Con
tinue
don
next
page
6 Zarraga and Schwarz JACC Vol. 49, No. 1, 2007Coxibs and Heart Disease January 2/9, 2007:1–14
T C A P A
by on August 9, 2008 content.onlinejacc.orgDownloaded from
pgr(tc(wc
twciAt(iserNtoIoeIiiTtcocwntr
dchthrpiwpsmtmm
Con
tinu
ed
able
2C
onti
nued
Tria
lN
umbe
rof
Pat
ient
sP
atie
ntC
hara
cter
isti
csIn
terv
enti
onD
urat
ion
CV
Out
com
eR
esul
ts
lzhe
imer
’sD
isea
seStu
dyIQ
5-9
7-0
2-0
01
(49
)4
25
Alz
heim
er’s
dem
entia
Cel
ecox
ib2
00
mg
2x/
day
vs.p
lace
bo1
yrCV
thro
mbo
ticev
ents
(com
posi
teof
MI,
stro
ke,
and
periph
eral
vasc
ular
thro
mbo
sis)
Inci
denc
e:2
.1%
with
plac
ebo
3.8
%w
ithce
leco
xib
MI
Inci
denc
e:0
%w
ithpl
aceb
o1
.4%
with
cele
coxi
b
UCCES
S-1
(49
)1
3,1
94
OA
,RA
Cel
ecox
ib1
00
or2
00
mg
2x/
day
vs.n
apro
xen
50
0m
g2
x/da
yvs
.dic
lofe
nac
50
mg
2x/
day
12
wee
ksCom
posi
teof
MI,
isch
emic
CVA
,and
periph
eral
vasc
ular
thro
mbo
sis
MI
No
diff
eren
ceam
ong
the
thre
egr
oups
:inc
iden
ce0
.3%
inea
chgr
oup
Inci
denc
e:�
0.1
%w
ithno
nsel
ectiv
eN
SA
IDs,
0.1
%w
ithce
leco
xib
20
0m
g2
x/da
y,an
d0
.2%
with
cele
coxi
b1
00
mg
2x/
day
decr
ease
d;CV
�ca
rdio
vasc
ular
;CVA
�ce
rebr
ovas
cula
rac
cide
nt;o
ther
abbr
evia
tions
asin
Tabl
e1
.
7JACC Vol. 49, No. 1, 2007 Zarraga and SchwarzJanuary 2/9, 2007:1–14 Coxibs and Heart Disease
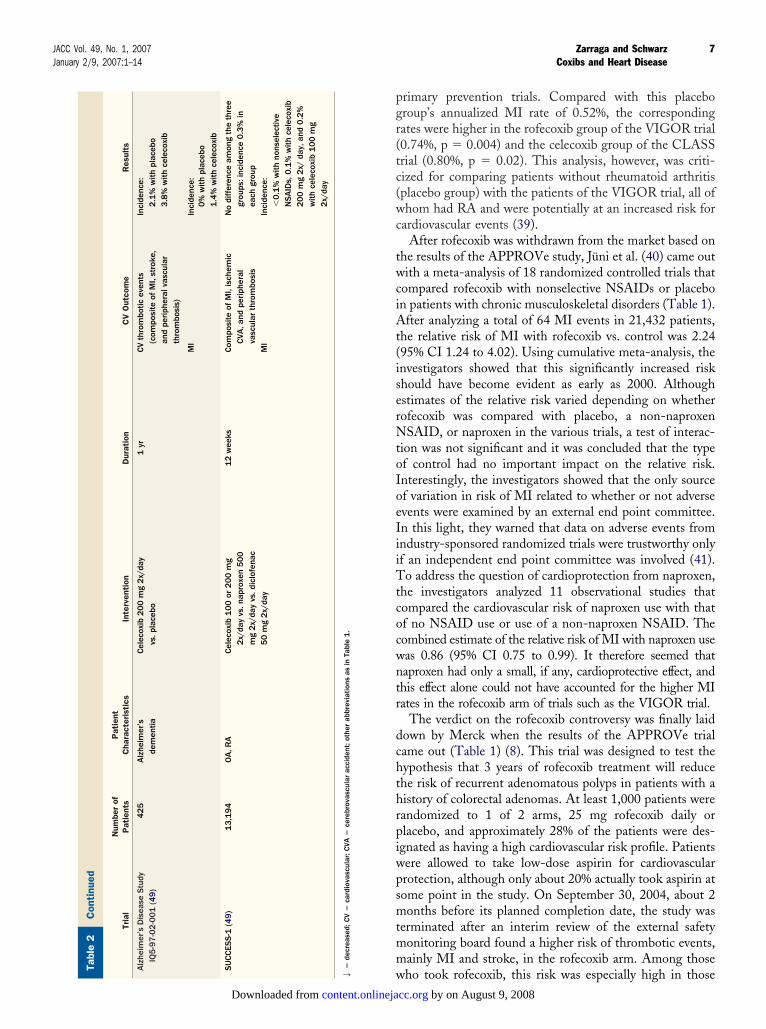
rimary prevention trials. Compared with this placeboroup’s annualized MI rate of 0.52%, the correspondingates were higher in the rofecoxib group of the VIGOR trial0.74%, p � 0.004) and the celecoxib group of the CLASSrial (0.80%, p � 0.02). This analysis, however, was criti-ized for comparing patients without rheumatoid arthritisplacebo group) with the patients of the VIGOR trial, all ofhom had RA and were potentially at an increased risk for
ardiovascular events (39).After rofecoxib was withdrawn from the market based on
he results of the APPROVe study, Jüni et al. (40) came outith a meta-analysis of 18 randomized controlled trials that
ompared rofecoxib with nonselective NSAIDs or placebon patients with chronic musculoskeletal disorders (Table 1).fter analyzing a total of 64 MI events in 21,432 patients,
he relative risk of MI with rofecoxib vs. control was 2.2495% CI 1.24 to 4.02). Using cumulative meta-analysis, thenvestigators showed that this significantly increased riskhould have become evident as early as 2000. Althoughstimates of the relative risk varied depending on whetherofecoxib was compared with placebo, a non-naproxenSAID, or naproxen in the various trials, a test of interac-
ion was not significant and it was concluded that the typef control had no important impact on the relative risk.nterestingly, the investigators showed that the only sourcef variation in risk of MI related to whether or not adversevents were examined by an external end point committee.n this light, they warned that data on adverse events fromndustry-sponsored randomized trials were trustworthy onlyf an independent end point committee was involved (41).o address the question of cardioprotection from naproxen,
he investigators analyzed 11 observational studies thatompared the cardiovascular risk of naproxen use with thatf no NSAID use or use of a non-naproxen NSAID. Theombined estimate of the relative risk of MI with naproxen useas 0.86 (95% CI 0.75 to 0.99). It therefore seemed thataproxen had only a small, if any, cardioprotective effect, andhis effect alone could not have accounted for the higher MIates in the rofecoxib arm of trials such as the VIGOR trial.
The verdict on the rofecoxib controversy was finally laidown by Merck when the results of the APPROVe trialame out (Table 1) (8). This trial was designed to test theypothesis that 3 years of rofecoxib treatment will reducehe risk of recurrent adenomatous polyps in patients with aistory of colorectal adenomas. At least 1,000 patients wereandomized to 1 of 2 arms, 25 mg rofecoxib daily orlacebo, and approximately 28% of the patients were des-gnated as having a high cardiovascular risk profile. Patientsere allowed to take low-dose aspirin for cardiovascularrotection, although only about 20% actually took aspirin atome point in the study. On September 30, 2004, about 2onths before its planned completion date, the study was
erminated after an interim review of the external safetyonitoring board found a higher risk of thrombotic events,ainly MI and stroke, in the rofecoxib arm. Among those
who took rofecoxib, this risk was especially high in thoseT A S
2�
by on August 9, 2008 content.onlinejacc.orgDownloaded from
wvsomctdbbfMt
ofdbotodrhteiomwc
RE
WccineCi
hoomi(rltoId
eIouw1fta13FrNvceim
swP(c4weh
S
A
8 Zarraga and Schwarz JACC Vol. 49, No. 1, 2007Coxibs and Heart Disease January 2/9, 2007:1–14
ho had a history of symptomatic atherosclerotic cardio-ascular disease or diabetes. Although the original articleuggested that the excess risk surfaced only after 18 monthsf rofecoxib use, a correction to this claim was recentlyade; a re-analysis of the data did not suggest that a shorter
ourse (�18 months) of rofecoxib was safe (42). Althoughhe APPROVe trial was a relatively small trial that was notesigned primarily to investigate cardiovascular outcomes, itrought forward a new dimension to the rofecoxib analysisy using placebo as the control and having a treatment andollow-up duration well beyond 24 months. Thereafter
erck could have accepted a black box warning, but it choseo pull the drug out of the world market immediately.
On May 11, 2006, Merck released their data on anff-drug extension of the APPROVe trial in which theyollowed up the over 2,500 patients for another year afteriscontinuation of the study drug (43). There continued toe more cardiovascular thrombotic events in those previ-usly randomized to rofecoxib (28 events vs. 16 events inhose previously randomized to placebo), with a relative riskf 1.64 (95% CI 0.89 to 3.04). When the off-drug extensionata were combined with the 3-year on-drug data, theelative risk over 4 years was 1.74 (95% CI 1.19 to 2.55),inting that the increased cardiovascular risk in those whoook rofecoxib was slow to abate—in fact, more slowly thanxpected if the only mechanism invoked was a coxib-nduced prothrombotic state. An in-depth analysis of theff-drug extension data is currently under way. In theeantime, continued follow-up of this cohort of patientsill be valuable in understanding the long-term risks asso-
iated with rofecoxib.
isk of Ischemic Cardiovascularvents With the Other Coxibs
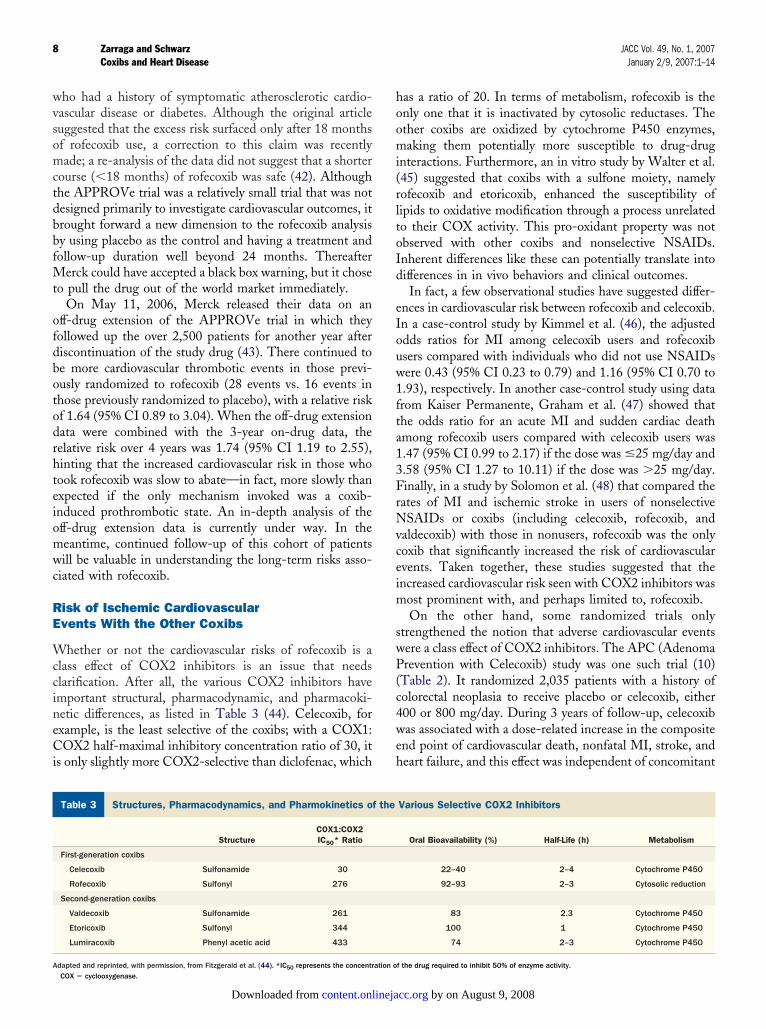
hether or not the cardiovascular risks of rofecoxib is alass effect of COX2 inhibitors is an issue that needslarification. After all, the various COX2 inhibitors havemportant structural, pharmacodynamic, and pharmacoki-etic differences, as listed in Table 3 (44). Celecoxib, forxample, is the least selective of the coxibs; with a COX1:OX2 half-maximal inhibitory concentration ratio of 30, it
s only slightly more COX2-selective than diclofenac, which
tructures, Pharmacodynamics, and Pharmokinetics of the Various
Table 3 Structures, Pharmacodynamics, and Pharmokinetics o
StructureCOX1:COX2IC50* Ratio
First-generation coxibs
Celecoxib Sulfonamide 30
Rofecoxib Sulfonyl 276
Second-generation coxibs
Valdecoxib Sulfonamide 261
Etoricoxib Sulfonyl 344
Lumiracoxib Phenyl acetic acid 433
dapted and reprinted, with permission, from Fitzgerald et al. (44). *IC50 represents the concentration oCOX � cyclooxygenase.
content.onlinejaDownloaded from
as a ratio of 20. In terms of metabolism, rofecoxib is thenly one that it is inactivated by cytosolic reductases. Thether coxibs are oxidized by cytochrome P450 enzymes,aking them potentially more susceptible to drug-drug
nteractions. Furthermore, an in vitro study by Walter et al.45) suggested that coxibs with a sulfone moiety, namelyofecoxib and etoricoxib, enhanced the susceptibility ofipids to oxidative modification through a process unrelatedo their COX activity. This pro-oxidant property was notbserved with other coxibs and nonselective NSAIDs.nherent differences like these can potentially translate intoifferences in in vivo behaviors and clinical outcomes.In fact, a few observational studies have suggested differ-
nces in cardiovascular risk between rofecoxib and celecoxib.n a case-control study by Kimmel et al. (46), the adjusteddds ratios for MI among celecoxib users and rofecoxibsers compared with individuals who did not use NSAIDsere 0.43 (95% CI 0.23 to 0.79) and 1.16 (95% CI 0.70 to.93), respectively. In another case-control study using datarom Kaiser Permanente, Graham et al. (47) showed thathe odds ratio for an acute MI and sudden cardiac deathmong rofecoxib users compared with celecoxib users was.47 (95% CI 0.99 to 2.17) if the dose was �25 mg/day and.58 (95% CI 1.27 to 10.11) if the dose was �25 mg/day.inally, in a study by Solomon et al. (48) that compared the
ates of MI and ischemic stroke in users of nonselectiveSAIDs or coxibs (including celecoxib, rofecoxib, and
aldecoxib) with those in nonusers, rofecoxib was the onlyoxib that significantly increased the risk of cardiovascularvents. Taken together, these studies suggested that thencreased cardiovascular risk seen with COX2 inhibitors was
ost prominent with, and perhaps limited to, rofecoxib.On the other hand, some randomized trials only
trengthened the notion that adverse cardiovascular eventsere a class effect of COX2 inhibitors. The APC (Adenomarevention with Celecoxib) study was one such trial (10)
Table 2). It randomized 2,035 patients with a history ofolorectal neoplasia to receive placebo or celecoxib, either00 or 800 mg/day. During 3 years of follow-up, celecoxibas associated with a dose-related increase in the composite
nd point of cardiovascular death, nonfatal MI, stroke, andeart failure, and this effect was independent of concomitant
ctive COX2 Inhibitors
Various Selective COX2 Inhibitors
Oral Bioavailability (%) Half-Life (h) Metabolism
22–40 2–4 Cytochrome P450
92–93 2–3 Cytosolic reduction
83 2.3 Cytochrome P450
100 1 Cytochrome P450
74 2–3 Cytochrome P450
Sele
f the
f the drug required to inhibit 50% of enzyme activity.
by on August 9, 2008 cc.org
ufiCptAtSSwccbAodrcwtfbs
spsTofbloca
pt
tscpecddldswdafleipwsShalitNbho
C
C per os1
9JACC Vol. 49, No. 1, 2007 Zarraga and SchwarzJanuary 2/9, 2007:1–14 Coxibs and Heart Disease
se of aspirin or lipid-lowering medication. Notably, thesendings contrasted with those of other studies, includingLASS (celecoxib vs. ibuprofen or diclofenac) and 3 un-ublished studies, namely PreSAP (Prevention of Colorec-al Sporadic Adenomatous Polyps; celecoxib vs. placebo),DAPT (Alzheimer’s Disease Anti-inflammatory Preven-
ion Trial; celecoxib vs. naproxen or placebo), andUCCESS-1 (the first Successive Celecoxib Efficacy andafety Study; celecoxib vs. naproxen or diclofenac), all ofhich did not show any statistical difference in the risk of
ardiovascular thrombotic events between celecoxib and aomparator nonselective NSAID and/or placebo (49) (Ta-le 2). It should be emphasized, however, that like thePPROVe study, the strength of the APC trial lay in its usef a placebo as control and its treatment and follow-upuration of over 24 months. In a recent meta-analysis ofandomized trials of celecoxib, Caldwell et al. (50) con-luded that celecoxib significantly increased the risk of MIhen compared with placebo (odds ratio 2.26, 95% CI 1.0
o 5.1) or when compared with placebo, diclofenac, ibupro-en, and paracetamol (odds ratio 1.88, 95% CI 1.15 to 3.08),ut did not significantly increase the risk of other outcomesuch as cardiovascular death and stroke.
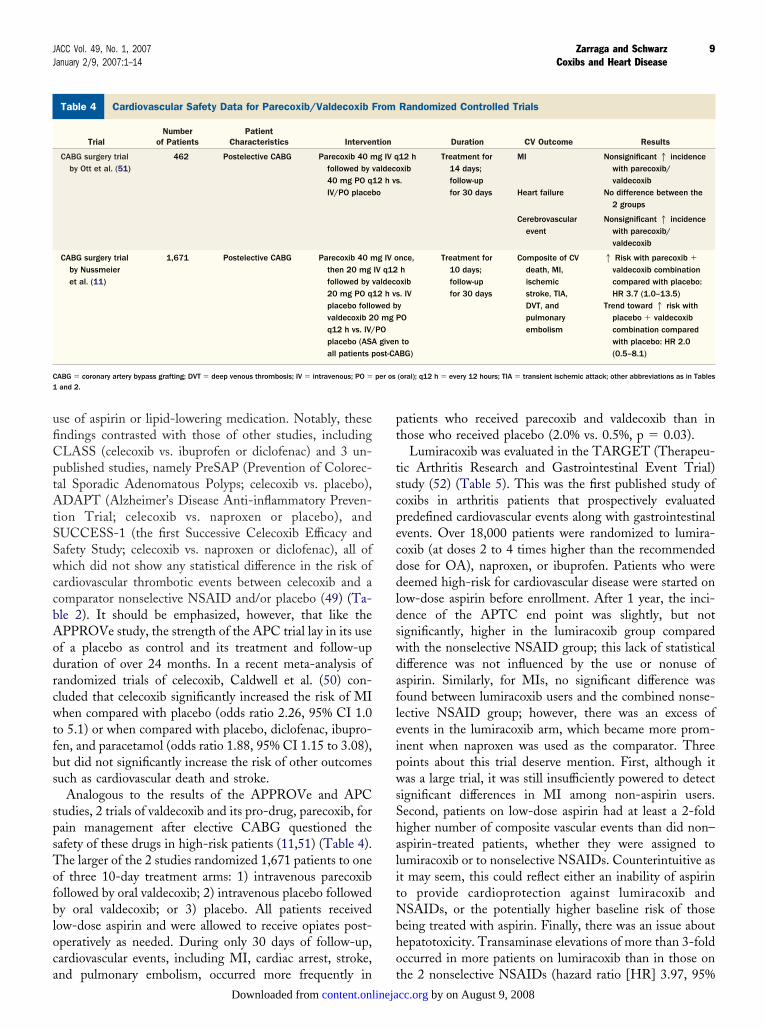
Analogous to the results of the APPROVe and APCtudies, 2 trials of valdecoxib and its pro-drug, parecoxib, forain management after elective CABG questioned theafety of these drugs in high-risk patients (11,51) (Table 4).he larger of the 2 studies randomized 1,671 patients to onef three 10-day treatment arms: 1) intravenous parecoxibollowed by oral valdecoxib; 2) intravenous placebo followedy oral valdecoxib; or 3) placebo. All patients receivedow-dose aspirin and were allowed to receive opiates post-peratively as needed. During only 30 days of follow-up,ardiovascular events, including MI, cardiac arrest, stroke,
ardiovascular Safety Data for Parecoxib/Valdecoxib From Random
Table 4 Cardiovascular Safety Data for Parecoxib/Valdecoxib F
TrialNumber
of PatientsPatient
Characteristics Interven
CABG surgery trialby Ott et al. (51)
462 Postelective CABG Parecoxib 40 mfollowed by v40 mg PO q1IV/PO placeb
CABG surgery trialby Nussmeieret al. (11)
1,671 Postelective CABG Parecoxib 40 mthen 20 mgfollowed by v20 mg PO q1placebo follovaldecoxib 2q12 h vs. IV/placebo (ASAall patients p
ABG � coronary artery bypass grafting; DVT � deep venous thrombosis; IV � intravenous; PO �
and 2.
nd pulmonary embolism, occurred more frequently in tcontent.onlinejaDownloaded from
atients who received parecoxib and valdecoxib than inhose who received placebo (2.0% vs. 0.5%, p � 0.03).
Lumiracoxib was evaluated in the TARGET (Therapeu-ic Arthritis Research and Gastrointestinal Event Trial)tudy (52) (Table 5). This was the first published study ofoxibs in arthritis patients that prospectively evaluatedredefined cardiovascular events along with gastrointestinalvents. Over 18,000 patients were randomized to lumira-oxib (at doses 2 to 4 times higher than the recommendedose for OA), naproxen, or ibuprofen. Patients who wereeemed high-risk for cardiovascular disease were started on
ow-dose aspirin before enrollment. After 1 year, the inci-ence of the APTC end point was slightly, but notignificantly, higher in the lumiracoxib group comparedith the nonselective NSAID group; this lack of statisticalifference was not influenced by the use or nonuse ofspirin. Similarly, for MIs, no significant difference wasound between lumiracoxib users and the combined nonse-ective NSAID group; however, there was an excess ofvents in the lumiracoxib arm, which became more prom-nent when naproxen was used as the comparator. Threeoints about this trial deserve mention. First, although itas a large trial, it was still insufficiently powered to detect
ignificant differences in MI among non-aspirin users.econd, patients on low-dose aspirin had at least a 2-foldigher number of composite vascular events than did non–spirin-treated patients, whether they were assigned toumiracoxib or to nonselective NSAIDs. Counterintuitive ast may seem, this could reflect either an inability of aspirino provide cardioprotection against lumiracoxib andSAIDs, or the potentially higher baseline risk of those
eing treated with aspirin. Finally, there was an issue aboutepatotoxicity. Transaminase elevations of more than 3-foldccurred in more patients on lumiracoxib than in those on
Controlled Trials
Randomized Controlled Trials
Duration CV Outcome Results
12 hxib.
Treatment for14 days;follow-upfor 30 days
MI
Heart failure
Nonsignificant1 incidencewith parecoxib/valdecoxib
No difference between the2 groups
Cerebrovascularevent
Nonsignificant1 incidencewith parecoxib/valdecoxib
nce,hxib. IVyO
toBG)
Treatment for10 days;follow-upfor 30 days
Composite of CVdeath, MI,ischemicstroke, TIA,DVT, andpulmonaryembolism
1 Risk with parecoxib �
valdecoxib combinationcompared with placebo:HR 3.7 (1.0–13.5)
Trend toward1 risk withplacebo � valdecoxibcombination comparedwith placebo: HR 2.0(0.5–8.1)
(oral); q12 h � every 12 hours; TIA � transient ischemic attack; other abbreviations as in Tables
ized
rom
tion
g IV qaldeco2 h vso
g IV oIV q12aldeco2 h vswed b0 mg PPOgiven
ost-CA
he 2 nonselective NSAIDs (hazard ratio [HR] 3.97, 95% by on August 9, 2008 cc.org

Cpcaaaba
ciu
ht(
C
B r abbre
10 Zarraga and Schwarz JACC Vol. 49, No. 1, 2007Coxibs and Heart Disease January 2/9, 2007:1–14
I 2.96 to 5.32). Whether or not this was a dose-dependenthenomenon related to supratherapeutic doses of lumira-oxib remains unanswered. Nonetheless, on the basis of thebove findings, it is difficult to justify the use of lumiracoxibt this time (53). For patients not taking aspirin, thebsolute reduction of 0.72% in ulcer complications is offsety an excess of 2.0% of liver function test abnormalities and
ardiovascular Safety Data for Etoricoxib and Lumiracoxib From Ra
Table 5 Cardiovascular Safety Data for Etoricoxib and Lumiraco
TrialNumber
of PatientsPatient
Characteristics Intervention
Pooled analysisof etoricoxibphase IIB/IIItrials (54)
�6,700 RA, OA, chronic lowback pain
Etoricoxib vs. placebo
Etoricoxib vs. non-naproxen NSAID
Etoricoxib vs. naprox
EDGE (54) 7,111 OA Etoricoxib 90 mg/davs. diclofenac150 mg/day
EDGE II (54) �4,090 RA Etoricoxib 90 mg/davs. diclofenac150 mg/day
MEDAL (54) �23,450 RA, OA EtoricoxibOA: 60 mg/dayRA: 90 mg/day
vs. diclofenac150 mg/day
TARGET (52) 18,325 OA Lumiracoxib 400 mg/day vs. naproxen 50mg 2x/day vs.ibuprofen 800 mg3x/day(ASA allowed)
P � blood pressure; OR � odds ratio (numbers in parentheses represent the 95% interval); othe
n excess of 0.17% of MI if naproxen is used as the acontent.onlinejaDownloaded from
omparator NSAID. For patients taking low-dose aspirin, its even harder to justify lumiracoxib because the benefit oflcer complication reduction is lost.Etoricoxib and lumiracoxib are the 2 newest coxibs that
ave yet to be examined for approval by the FDA. Clinicalrials of etoricoxib are ongoing and include EDGE IIEtoricoxib vs. Diclofenac Sodium Gastrointestinal Toler-
ized Controlled Trials
rom Randomized Controlled Trials
Duration CV Outcome Results
3 months Thrombotic CV events RR with etoricoxib 1.11(0.32–3.81)
36 months Thrombotic CV events RR with etoricoxib 0.83(0.26–2.64)
30 months Thrombotic CV events Trend toward1 risk withetoricoxib: RR 1.70(0.9–3.18)
Mean of 9 months(maximum of 16months)
Thrombotic CV events No difference between thetwo groups: RR 1.01(0.65–1.58)
APTC end point No difference between thetwo groups: RR 0.99(0.58–1.67)
Mean of 19 months(maximum of 34months)
Thrombotic CV events(predefined)
Trials are ongoing
Mean of 20 months(maximum of 40months)
1 yr APTC end point(predefined)
No difference among thethree groups
Lumiracoxib vs. nonselectiveNSAIDs: HR 1.14(0.78–1.66)
Lumiracoxib vs. naproxen:HR 1.46 (0.89–2.37)
Lumiracoxib vs. ibuprofen:HR 0.76 (0.41–1.40)
MI Trend toward1 risk withlumiracoxib comparedwith naproxen
Lumiracoxib vs. nonselectiveNSAIDs: HR 1.31(0.70–2.45)
Lumiracoxib vs. naproxen:HR 1.77 (0.82–3.84)
Lumiracoxib vs. ibuprofen:HR 0.66 (0.21–2.09)
Heart failure Less frequent in lumiracoxibgroup than nonselectiveNSAID group: OR 0.71(0.39–1.3)
Systolic and diastolicBP elevation
Less degree of elevationwith lumiracoxibcompared withnonselective NSAIDs
viations as in Tables 1 and 2.
ndom
xib F
en
y
y
0
bility and Effectiveness Trial in Rheumatoid Arthritis by on August 9, 2008 cc.org

PMtRctaml
OC
AiCttcsaoncptCcNwteac
aeamppHlciHrh15nshw�c
shpCptcwv�
C
Dafapphtnidlcowam(
hctt
ArtenasScedcsrlcsA
11JACC Vol. 49, No. 1, 2007 Zarraga and SchwarzJanuary 2/9, 2007:1–14 Coxibs and Heart Disease
atients), which included 4,000 patients with RA, andEDAL (Multinational Etoricoxib and Diclofenac Arthri-
is Long-term Study), which included 23,500 patients withA and OA. The data from these 2 studies will be
ombined with those from the recently completed EDGErial, another trial of etoricoxib involving 7,111 patients, andn analysis of predefined cardiovascular outcomes will beade. Together, the data from these trials will form the
argest NSAID analysis ever designed (54) (Table 5).
ther Potential Adverseardiovascular Effects of Coxibs
lthough nonselective NSAIDs have been associated with anncreased risk of congestive heart failure (CHF) or worseningHF (55,56), it is less clear whether COX2 inhibitors share
he same risk. At least 2 observational studies have suggestedhat this risk is associated with rofecoxib but less so withelecoxib (57,58). One of them was a population-based cohorttudy that compared the rates of hospitalization for CHFmong NSAID-naive elderly individuals who were startedn rofecoxib (n � 14,583), celecoxib (n � 18,908), andonselective NSAIDs (n � 5,391), and a randomly selectedontrol group of non-NSAID users (n � 100,000). Com-ared with control patients and after adjustment for poten-ial confounders, the relative risk (RR) of admission forHF was significantly higher in those who received rofe-
oxib (RR 1.8, 95% CI 1.5 to 2.2) and nonselectiveSAIDs (RR 1.4, 95% CI 1.0 to 1.9), but not in thoseho received celecoxib (RR 1.0, 95% CI 0.8 to 1.3). In
he APPROVe study, CHF and pulmonary edema occurredarlier (about 5 months after starting the study drug) and athigher rate in patients who took rofecoxib than in the
ontrol group (HR 4.61, 95% CI 1.50 to 18.83) (8).Non-steroid anti-inflammatory drugs have also been
ssociated with blood pressure elevation and lower extremitydema (59). Coxibs may share these risks, although oncegain, the greatest risk seems to be with rofecoxib. In aeta-analysis of 19 randomized trials involving 45,461
atients, the weighted mean difference in systolic bloodressure was �3.85/�1.06 mm Hg and �2.83/�1.34 mmg when coxibs were compared with placebo and nonse-
ective NSAIDs, respectively (60). Among the differentoxibs that were compared with placebo, the largest increasen systolic blood pressure was with rofecoxib (�5.66 mm
g vs. �2.60 mm Hg with celecoxib). Rofecoxib alsoesulted in a statistically significant increase in the risk ofypertension compared with placebo (RR 2.63, 95% CI.42 to 4.85), whereas celecoxib (RR 0.81, 95% CI 0.13 to.21) and etoricoxib (RR 1.23, 95% CI 0.44 to 3.44) didot. Data from the CLASS and APPROVe trials suggestedimilar findings. In the CLASS trial, the incidence ofypertension was lower in the celecoxib group comparedith the nonselective NSAID group (1.7% vs. 2.3%, p
0.05), whereas the incidence of peripheral edema was
omparable between the 2 groups (2). The APPROVe tcontent.onlinejaDownloaded from
tudy, on the other hand, suggested an increased risk ofypertension and peripheral edema with rofecoxib com-ared with nonselective NSAIDs (8). Like celecoxib in theLASS trial, lumiracoxib was not implicated in bloodressure elevation in the TARGET trial; in fact, nonselec-ive NSAIDs were associated with significantly higher meanhanges in systolic and diastolic blood pressure comparedith lumiracoxib (systolic blood pressure: �2.1 mm Hgs. �0.4 mm Hg, p � 0.0001; diastolic blood pressure:0.5 mm Hg vs. �0.1 mm Hg, p � 0.0001) (52).
onclusions
rawing conclusions from the numerous studies on coxibsnd their cardiovascular risk obviously has not been straight-orward. Although it is understandable why clinical trials onrthritis patients would use nonselective NSAIDs as com-arators, the lack of a placebo arm complicates the inter-retation of the results, especially because NSAIDs mayave cardiovascular effects themselves. In addition, most ofhe data we have on coxibs were derived from post hoc andon-prespecified analyses of randomized trials. We are still
n need of randomized controlled trials that are purposelyesigned and adequately powered to examine the cardiovascu-
ar effects of these drugs. One such trial has been planned forelecoxib, PRECISION (Prospective Randomized Evaluationf Celecoxib Integrated Safety vs. Ibuprofen or Naproxen),hich hopes to assess the relative safety of these drugs in
bout 21,000 patients with OA or RA and known CAD orultiple risk factors for CAD over a duration of 2 years
61).Amidst the multitude of studies on coxibs, one thing we
ave learned is what specific questions to ask. Although theurrent data have their limitations, fortunately it is possibleo draw a fair number of conclusions to answer some ofhese questions.
First, are all coxibs the same? We do not believe so.lthough there are good data from randomized trials of
ofecoxib, valdecoxib/parecoxib, and celecoxib to suggesthat each of these drugs can result in adverse cardiovascularvents (as though to suggest a class effect), there are likewiseumerous studies that indicate different degrees of riskssociated with different coxibs. The latter has been under-cored by studies such as CLASS, PreSAP, ADAPT, andUCCESS-1, which have shown no increased risk withelecoxib, and observational studies that have shown differ-nces in risks between rofecoxib and celecoxib. That theseifferences are related to the COX2 selectivity of the drug orertain moieties within its chemical structure has beenuggested but cannot fully account for the findings of theandomized trials. For example, of the various coxibs,umiracoxib is the most COX2 selective, followed by rofe-oxib and then celecoxib. The associated cardiovascular riskseen in the TARGET (lumiracoxib), VIGOR andPPROVe (rofecoxib), and CLASS and APC (celecoxib)
rials, however, did not line up in quite the same order. by on August 9, 2008 cc.org

Uhwittsctod
pWiCtsmbTd
cvosAhdtrosntnfitnC
mbcvwtdtvttcp
ia
ppdNtbtcecemafnipwStCtrtstaemwfsnatopvpPs
RDBE
R
12 Zarraga and Schwarz JACC Vol. 49, No. 1, 2007Coxibs and Heart Disease January 2/9, 2007:1–14
nfortunately, there are no clinical trials that have madeead-to-head comparisons of the various coxibs on whiche can substantiate this idea of a differential risk. It is also
mportant to point out that as much as we have scrutinizedhe different coxibs, similar emphasis should be placed onhe impact of different doses on outcomes. The APC trialhowed quite clearly that the adverse events associated withelecoxib were dose-dependent. In this light, concerns abouthe safety of lumiracoxib in the TARGET trial, and mostther coxibs for that matter, may be attenuated if loweroses are used.Second, how should the cardiovascular risk profile of a
atient affect our decision to use or not use a coxib?hen the absolute risk increase in cardiovascular events
s expected to be high with coxib use, as in a patient withAD or multiple risk factors for CAD, it is but prudent
o avoid a coxib. For the young, low-risk individual, thecenario is less clear. The absolute risk increase in eventsay be lower, but the relative risk increase can potentially
e greater and still reach magnitudes of unacceptability.his is a specific issue that needs clarification by well-esigned studies.Third, is it beneficial to add aspirin when prescribing a
oxib to a patient with an intermediate or high cardio-ascular risk profile? Although the intuitive answer is yes,nce again, the clinical trials do not provide us with atraightforward answer. The post hoc analysis of thePC data showed that patients who took aspirin did notave lower rates of cardiovascular events than those whoid not take aspirin. Similarly, in the APPROVe trial,he increased cardiovascular risk experienced by theofecoxib group did not seem to be influenced by baseliner subsequent use of aspirin. Findings such as theseuggest that the adverse outcomes from coxib use mightot be solely a consequence of COX2 inhibition (or ahromboxane-prostacyclin imbalance), and other mecha-isms might be at play. What is perhaps clearer is thending that when aspirin is taken together with a coxib,he gastrointestinal safety advantage of the coxib over aonselective NSAID is lost. This was seen at least in theLASS and TARGET trials.Finally, is there still a place for coxibs in our scheme ofanaging patients with pain syndromes? Are there safer
ut equally efficacious alternatives? We believe thatoxibs will continue to be clinically useful, although in aery select group of patients. These are the individualsho continue to require nonsteroidal anti-inflammatory
reatment despite optimization of other modalities (e.g.,isease-modifying drugs for RA and analgesics, physicalherapy, and physical aids for OA), have a low cardio-ascular risk profile, and have a relatively high gastroin-estinal bleeding risk. Although the vast majority of trialshat compared nonselective NSAIDs with coxibs for painontrol did not show superiority of the latter, in clinical
ractice, the response to pain management varies fromcontent.onlinejaDownloaded from
ndividual to individual, and it is not uncommon to havepatient who reports better pain relief with a coxib.Currently, the impetus for avoiding coxibs is the
otential to cause cardiovascular harm. Three importantoints arise from this statement. First, we actually lackefinitive data about where the various nonselectiveSAIDs, the presumed alternatives to coxibs, stand in
erms of cardiovascular safety. This is because there haseen no long-term placebo-controlled trial of conven-ional NSAIDs designed to evaluate cardiovascular out-omes. The vast majority of observational studies, how-ver, have not shown any significant cardiovascularonsequence from nonselective NSAID use, with thexception of naproxen, which has been implicated to beildly cardioprotective by a few studies. A recent meta-
nalysis of placebo-controlled randomized trials alsoailed to show any significant cardiovascular effect ofonselective NSAIDs, including nabumetone, ibuprofen,
ndomethacin, diclofenac, and even naproxen, exceptossibly in trials of Alzheimer’s disease, in which thereas a nonsignificant trend toward increased events (62).econd, certain NSAIDs, such as ibuprofen, can blunthe antiplatelet effect of aspirin, presumably by binding toOX1 and blocking the channel that aspirin must
raverse to bind COX1 (63). In view of this, it has beenecommended that if aspirin and an NSAID are to beaken on a regular basis, the soluble form of aspirinhould be ingested 2 hours before the NSAID (64). Thisype of interaction becomes essentially irrelevant whenspirin is combined with a coxib because COX2 is notxpressed in mature platelets. Finally, if a decision isade to avoid a coxib, the combination of an NSAIDith a proton pump inhibitor (PPI) may be just as safe
or the upper gastrointestinal tract (65), but perhaps noto for the lower gastrointestinal tract, in which a PPI isot expected to provide any protection (67). A cleardvantage of using a nonselective NSAID/PPI combina-ion is its lower cost compared with a coxib, especially ifver-the-counter equivalents (e.g., naproxen or ibuprofenlus omeprazole) are used. In patients with high cardio-ascular risk who need to be on aspirin, more complexolypharmacy-type combinations such as coxib/aspirin/PI and nonselective NSAID/aspirin/PPI have beenuggested but have not been compared directly (66).
eprint requests and correspondence: Dr. Ernst R. Schwarz,ivision of Cardiology, Cedars Sinai Medical Center, 8700everly Boulevard, Suite 6215, Los Angeles, California 90048.-mail: [email protected].
EFERENCES
1. Tanaka Y, Ward SL, Smith WL. Immunochemical and kineticevidence for two different prostaglandin H-prostaglandin E isomerasesin sheep vesicular gland microsomes. J Biol Chem 1987;262:1374–81.
2. Silverstein FE, Faich G, Goldstein JL, et al. Gastrointestinal toxicitywith celecoxib vs nonsteroidal anti-inflammatory drugs for osteoar-
by on August 9, 2008 cc.org

1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
13JACC Vol. 49, No. 1, 2007 Zarraga and SchwarzJanuary 2/9, 2007:1–14 Coxibs and Heart Disease
thritis and rheumatoid arthritis: the CLASS study: a randomizedcontrolled trial. Celecoxib Long-term Arthritis Safety Study. JAMA2000;284:1247–55.
3. IMS Health. IMS Health reports Cox-2 drug sales in U.S. surge 137%in six month period. Westport, CT: IMS Health Inc., 2000. Availableat: http://ww0.ne.imshealth.com/public/structure/dispcontent/1,2779,1341-1341-81004,00.html. Accessed February 8, 2006.
4. Bombardier C, Laine L, Reicin A, et al., VIGOR Study Group.Comparison of upper gastrointestinal toxicity of rofecoxib andnaproxen in patients with rheumatoid arthritis. N Engl J Med2000;343:1520 – 8.
5. Drazen JM. COX-2 inhibitors—a lesson in unexpected problems.N Engl J Med 2005;352:1131–2.
6. Konstam MA, Weir MR, Reicin A, et al. Cardiovascular thromboticevents in controlled, clinical trials of rofecoxib. Circulation 2001;104:2280–8.
7. Maxwell SR, Webb DJ. COX-2 selective inhibitors—important les-sons learned. Lancet 2005;365:449–51.
8. Bresalier RS, Sandler RS, Quan H, et al., Adenomatous PolypPrevention on Vioxx (APPROVe) Trial Investigators. Cardiovascularevents associated with rofecoxib in a colorectal adenoma chemopre-vention trial. N Engl J Med 2005;352:1092–102.
9. Topol EJ. Failing the public health: rofecoxib, Merck, and the FDA.N Engl J Med 2004;351:1707–9.
0. Solomon SD, McMurray JJ, Pfeffer MA, et al., Adenoma Preventionwith Celecoxib (APC) Study Investigators. Cardiovascular risk asso-ciated with celecoxib in a clinical trial for colorectal adenoma preven-tion. N Engl J Med 2005;352:1071–80.
1. Nussmeier NA, Whelton AA, Brown MT, et al. Complications of theCOX-2 inhibitors parecoxib and valdecoxib after cardiac surgery.N Engl J Med 2005;352:1081–91.
2. U.S. Food and Drug Administration Talk Paper. Bextra label updatedwith boxed warning concerning severe skin reactions and warningregarding cardiovascular risk. Available at: http://www.fda.gov/bbs/topics/ANSWERS/2004/ANS01331.html. Accessed June 26, 2006.
3. U.S. Food and Drug Administration Alert for Practitioners. Celecoxib(Marketed as Celebrex). Available at: http://www.fda.gov/cder/drug/infopage/celebrex/celebrex-hcp.htm. Accessed June 26, 2006.
4. Baker CS, Hall RJ, Evans TJ, et al. Cyclooxygenase-2 is widelyexpressed in atherosclerotic lesions affecting native and transplantedhuman coronary arteries and colocalizes with inducible nitric oxidesynthase and nitrotyrosine particularly in macrophages. ArteriosclerThromb Vasc Biol 1999;19:646–55.
5. Schonbeck U, Sukhova GK, Graber P, Coulter S, Libby P. Aug-mented expression of cyclooxygenase-2 in human atheroscleroticlesions. Am J Pathol 1999;155:1281–91.
6. Dannenberg AJ, Subbaramaiah K. Targeting cyclooxygenase-2 inhuman neoplasia: rationale and promise. Cancer Cell 2003;4:431–6.
7. Dinchuk JE, Car BD, Focht RJ, et al. Renal abnormalities and analtered inflammatory response in mice lacking cyclooxygenase II.Nature 1995;378:406–9.
8. Cipollone F, Prontera C, Pini B, et al. Overexpression of functionallycoupled cyclooxygenase-2 and prostaglandin E synthase in symptom-atic atherosclerotic plaques as a basis of prostaglandin E(2)-dependentplaque instability. Circulation 2001;104:921–7.
9. Adderley SR, Fitzgerald DJ. Oxidative damage of cardiomyocytes islimited by extracellular regulated kinases 1/2-mediated induction ofcyclooxygenase-2. J Biol Chem 1999;274:5038–46.
0. Jones DA, Carlton DP, McIntyre TM, Zimmerman GA, PrescottSM. Molecular cloning of human prostaglandin endoperoxide syn-thase type II and demonstration of expression in response to cytokines.J Biol Chem 1993;268:9049–54.
1. Xie W, Herschman HR. Transcriptional regulation of prostaglandinsynthase 2 gene expression by platelet-derived growth factor andserum. J Biol Chem 1996;271:31742–8.
2. Topper JN, Cai J, Falb D, Gimbrone MA Jr. Identification of vascularendothelial genes differentially responsive to fluid mechanical stimuli:cyclooxygenase-2, manganese superoxide dismutase, and endothelialcell nitric oxide synthase are selectively up-regulated by steady laminarshear stress. Proc Natl Acad Sci U S A 1996;93:10417–22.
3. Chenevard R, Hurlimann D, Bechir M, et al. Selective COX-2inhibition improves endothelial function in coronary artery disease.
Circulation 2003;107:405–9.content.onlinejaDownloaded from
4. Widlansky ME, Price DT, Gokce N, et al. Short- and long-termCOX-2 inhibition reverses endothelial dysfunction in patients withhypertension. Hypertension 2003;42:310–5.
5. Cullen L, Kelly L, Connor SO, Fitzgerald DJ. Selective cyclo-oxygenase-2 inhibition by nimesulide in man. J Pharmacol Exp Ther1998;287:578–82.
6. McAdam BF, Catella-Lawson F, Mardini IA, Kapoor S, Lawson JA,FitzGerald GA. Systemic biosynthesis of prostacyclin by cyclo-oxygenase (COX)-2: the human pharmacology of a selective inhibitorof COX-2. Proc Natl Acad Sci U S A 1999;96:272–7.
7. Caughey GE, Cleland LG, Penglis PS, Gamble JR, James MJ. Rolesof cyclooxygenase (COX)-1 and COX-2 in prostanoid production byhuman endothelial cells: selective up-regulation of prostacyclin syn-thesis by COX-2. J Immunol 2001;167:2831–8.
8. Shinmura K, Tang XL, Wang Y, et al. Cyclooxygenase-2 mediates thecardioprotective effects of the late phase of ischemic preconditioning inconscious rabbits. Proc Natl Acad Sci U S A 2000;97:10197–202.
9. Birnbaum Y, Ye Y, Rosanio S, et al. Prostaglandins mediate thecardioprotective effects of atorvastatin against ischemia-reperfusioninjury. Cardiovasc Res 2005;65:345–55.
0. Egan KM, Wang M, Fries S, et al. Cyclooxygenases, thromboxane,and atherosclerosis: plaque destabilization by cyclooxygenase-2 inhi-bition combined with thromboxane receptor antagonism (erratum inCirculation 2005;111:2412). Circulation 2005;111:334–42.
1. Wu G, Luo J, Rana JS, Laham R, Sellke FW, Li J. Involvement ofCOX-2 in VEGF-induced angiogenesis via P38 and JNK pathways invascular endothelial cells. Cardiovasc Res 2006;69:512–9.
2. Targum SL. Food and Drug Administration: cardiovascular safetyreview rofecoxib, 2001. Available at: http://www.fda.gov/ohrms/dockets/ac/01/briefing/3677b2_06_cardio.pdf. Accessed June 26,2006.
3. Mamdani M, Rochon P, Juurlink DN, et al. Effect of selectivecyclooxygenase 2 inhibitors and naproxen on short-term risk of acutemyocardial infarction in the elderly. Arch Intern Med 2003;163:481–6.
4. Ray WA, Stein CM, Daugherty JR, Hall K, Arbogast PG, GriffinMR. COX-2 selective non-steroidal anti-inflammatory drugs and riskof serious coronary heart disease. Lancet 2002;360:1071–3.
5. Solomon DH, Schneeweiss S, Glynn RJ, et al. Relationship betweenselective cyclooxygenase-2 inhibitors and acute myocardial infarctionin older adults. Circulation 2004;109:2068–73.
6. Reicin AS, Shapiro D, Sperling RS, Barr E, Yu Q. Comparison ofcardiovascular thrombotic events in patients with osteoarthritis treatedwith rofecoxib versus nonselective nonsteroidal anti-inflammatorydrugs (ibuprofen, diclofenac, and nabumetone). Am J Cardiol 2002;89:204–9.
7. Weir MR, Sperling RS, Reicin A, Gertz BJ. Selective COX-2inhibition and cardiovascular effects: a review of the rofecoxib devel-opment program. Am Heart J 2003;146:591–604.
8. Mukherjee D, Nissen SE, Topol EJ. Risk of cardiovascular eventsassociated with selective COX-2 inhibitors. JAMA 2001;286:954–9.
9. Lipani J. Cox-2 inhibitors and cardiovascular risk: the data are inconclu-sive, and these drugs are needed. Cleve Clin J Med 2001;68:961–2.
0. Jüni P, Nartey L, Reichenbach S, Sterchi R, Dieppe PA, Egger M.Risk of cardiovascular events and rofecoxib: cumulative meta-analysis.Lancet 2004;364:2021–9.
1. Jüni P, Reichenback S, Dieppe PA, Egger M. Discontinuation ofVioxx: authors’ reply. Lancet 2005;365:28.
2. Bresalier RS, Sandler RS, Quan H, et al., APPROVe Trial Investi-gators. Cardiovascular events associated with rofecoxib in a colorectaladenoma chemoprevention trial (erratum in N Engl J Med 2006;355:221). N Engl J Med 2005;352:1092–102.
3. Merck. APPROVe Extension Statistical Package. Available at:http://www.merck.com/newsroom/vioxx_withdrawal/pdf/APPROVe_Extension_Statistical_Package.pdf. Accessed June 26, 2006.
4. FitzGerald GA. COX-2 and beyond: approaches to prostaglandininhibition in human disease. Nat Rev Drug Discov 2003;2:879–90.
5. Walter MF, Jacob RF, Day CA, Dahlborg R, Weng Y, Mason RP.Sulfone COX-2 inhibitors increase susceptibility of human LDL andplasma to oxidative modification: comparison to sulfonamide COX-2inhibitors and NSAIDs. Atherosclerosis 2004;177:235–43.
6. Kimmel SE, Berlin JA, Reilly M, et al. Patients exposed to rofecoxib
and celecoxib have different odds of nonfatal myocardial infarction.Ann Intern Med 2005;142:157–64.by on August 9, 2008 cc.org

4
4
4
5
5
5
5
5
5
5
5
5
5
6
6
6
6
6
6
6
6
14 Zarraga and Schwarz JACC Vol. 49, No. 1, 2007Coxibs and Heart Disease January 2/9, 2007:1–14
7. Graham DJ, Campen D, Hui R, et al. Risk of acute myocardialinfarction and sudden cardiac death in patients treated withcyclooxygenase 2 selective and non-selective non-steroidal anti-inflammatory drugs: nested case-control study. Lancet 2005;365:475–81.
8. Solomon DH, Avorn J, Sturmer T, Glynn RJ, Mogun H, SchneeweissS. Cardiovascular outcomes in new users of coxibs and nonsteroidalantiinflammatory drugs: high-risk subgroups and time course of risk.Arthritis Rheum 2006;54:1378–89.
9. Advisory Committee Briefing Document: Celecoxib and ValdecoxibCardiovascular Safety. Available at: http://www.fda.gov/ohrms/dockets/ac/05/briefing/2005-4090B1_03_Pfizer-Celebrex-Bextra.pdf.Accessed June 26, 2006.
0. Caldwell B, Aldington S, Weatherall M, Shirtcliffe P, Beasley R. Riskof cardiovascular events and celecoxib: a systematic review and meta-analysis. J R Soc Med 2006;99:132–40.
1. Ott E, Nussmeier NA, Duke PC, et al., Multicenter Study ofPerioperative Ischemia (McSPI) Research Group; Ischemia Researchand Education Foundation (IREF) Investigators. Efficacy and safety ofthe cyclooxygenase 2 inhibitors parecoxib and valdecoxib in patientsundergoing coronary artery bypass surgery. J Thorac Cardiovasc Surg2003;125:1481–92.
2. Farkouh ME, Kirshner H, Harrington RA, et al., TARGET StudyGroup. Comparison of lumiracoxib with naproxen and ibuprofen inthe Therapeutic Arthritis Research and Gastrointestinal Event Trial(TARGET), cardiovascular outcomes: randomised controlled trial.Lancet 2004;364:675–84.
3. Topol EJ, Falk GW. A coxib a day won’t keep the doctor away. Lancet2004;364:639–40.
4. Etoricoxib: FDA ACM Background Document. Available at:http://www.fda.gov/ohrms/dockets/ac/05/briefing/2005-4090B2_01_Merck-Etoricoxib.pdf. Accessed June 26, 2006.
5. Page J, Henry D. Consumption of NSAIDs and the development ofcongestive heart failure in elderly patients: an underrecognized publichealth problem. Arch Intern Med 2000;160:777–84.
6. Feenstra J, Heerdink ER, Grobbee DE, Stricker BH. Association ofnonsteroidal anti-inflammatory drugs with first occurrence of heartfailure and with relapsing heart failure: the Rotterdam Study. Arch
Intern Med 2002;162:265–70.content.onlinejaDownloaded from
7. Mamdani M, Juurlink DN, Lee DS, et al. Cyclooxygenase-2 inhibitorsversus non-selective non-steroidal anti-inflammatory drugs and con-gestive heart failure outcomes in elderly patients: a population-basedcohort study. Lancet 2004;363:1751–6.
8. Hudson M, Richard H, Pilote L. Differences in outcomes of patientswith congestive heart failure prescribed celecoxib, rofecoxib, or non-steroidal anti-inflammatory drugs: population based study. BMJ 2005;330:1370.
9. Johnson AG, Nguyen TV, Day RO. Do nonsteroidal anti-inflammatory drugs affect blood pressure? A meta-analysis. Ann InternMed 1994;121:289–300.
0. Aw TJ, Haas SJ, Liew D, Krum H. Meta-analysis of cyclooxygenase-2inhibitors and their effects on blood pressure. Arch Intern Med2005;165:490–6.
1. Sullivan MG. Pain relievers’ long-term CV risks under scrutiny.Internal Medicine News 2006;39:19.
2. Salpeter SR, Gregor P, Ormiston TM, et al. Meta-analysis: cardio-vascular events associated with nonsteroidal anti-inflammatory drugs.Am J Med 2006;119:552–9.
3. Catella-Lawson F, Reilly MP, Kapoor SC, et al. Cyclooxygenaseinhibitors and the antiplatelet effects of aspirin. N Engl J Med2001;345:1809–17.
4. Konstantinopoulos PA, Lehmann DF. The cardiovascular toxicity ofselective and nonselective cyclooxygenase inhibitors: comparisons,contrasts, and aspirin confounding. J Clin Pharmacol 2005;45:742–50.
5. Chan FK, Hung LC, Suen BY, et al. Celecoxib versus diclofenac andomeprazole in reducing the risk of recurrent ulcer bleeding in patientswith arthritis. N Engl J Med 2002;347:2104–10.
6. Goldstein JL, Eisen GM, Lewis B, Gralnek IM, Zlotnick S, Fort JG.Video capsule endoscopy to prospectively assess small bowel injurywith celecoxib, naproxen plus omeprazole, and placebo. Clin Gastro-enterol Hepatol 2005;3:133–41.
7. Reicin A, DiBattiste P, Mukhopadhyay S, et al. CardiovascularSafety Profile of Rofecoxib in Elderly Patients with Alzheimer’sDisease or Cognitive Impairment: An Updated Pooled Analysis.Presented at: EULAR 2003: European League Against Rheuma-tism Annual European Congress of Rheumatology: Lisbon, Portu-
gal, 2003.by on August 9, 2008 cc.org
doi:10.1016/j.jacc.2006.10.003 2007;49;1-14; originally published online Dec 12, 2006; J. Am. Coll. Cardiol.
Ignatius Gerardo E. Zarraga, and Ernst R. Schwarz Know
Coxibs and Heart Disease: What We Have Learned and What Else We Need to
This information is current as of August 9, 2008
& ServicesUpdated Information
http://content.onlinejacc.org/cgi/content/full/49/1/1including high-resolution figures, can be found at:
References
http://content.onlinejacc.org/cgi/content/full/49/1/1#BIBLfree at: This article cites 54 articles, 35 of which you can access for
Citations
eshttp://content.onlinejacc.org/cgi/content/full/49/1/1#otherarticlThis article has been cited by 1 HighWire-hosted articles:
Rights & Permissions
http://content.onlinejacc.org/misc/permissions.dtltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://content.onlinejacc.org/misc/reprints.dtl
Information about ordering reprints can be found online:
by on August 9, 2008 content.onlinejacc.orgDownloaded from