cqi projects summaryii - ungerboeck separate cqi projects improving response to suicide ideation 6...
TRANSCRIPT
10/2/2014
1
CQI Projectsand
Productivity Studies
MDCH Child and Adolescent Health CentersQuEST: Quality & Evaluation Support Team
Sherry Rose, RN, MSN, PNPLisa Rutherford, MA
October 16, 2014
Inspired by a Focus on Males
Disparities in health risk: males and females
3 separate CQI projects
◦ Improving response to suicide ideation
◦ 6 health centers volunteered for HPV immunization with: 2 focusing on improving parental, community acceptance 4 focusing on increasing HPV immunization rates among
males
◦ Increase the proportion of male clients (in process)
Project Kick-Off
Data we have Data we need (and how to get it)
Current process/activities
“Plus/Minus Contributors”
Next Steps

10/2/2014
2
Project Organization
Determine what the data is telling us
Develop AIM
Develop PDSA (Plan, Do, Study, Act)
Determine resources, support needed
Courtesy of Colorado DPHE
Improving Response: Suicide Risk/Ideation
Reviewed current process ◦ Just by talking it out, revealed holes
We aim to strengthen follow-up with access to services and referrals for clients with depression a/o suicide risk
By working on the process we expect to have a clearer referral system and to increase access to needed mental health interventions
Originally thought that the project would focus on males
◦ Review of RAAPS data for disparities found girls were greater risk for depression and suicide ideation
10/2/2014
3
Courtesy of Colorado DPHE
Wexford AWC: PDSA
Ensure RAAPS completed on each client w/ follow-up as appropriate
Review/revise follow-up policy/procedures
◦ Follow-up on referrals w/in 5 to 7 days
Developed a Process Map to guide work…
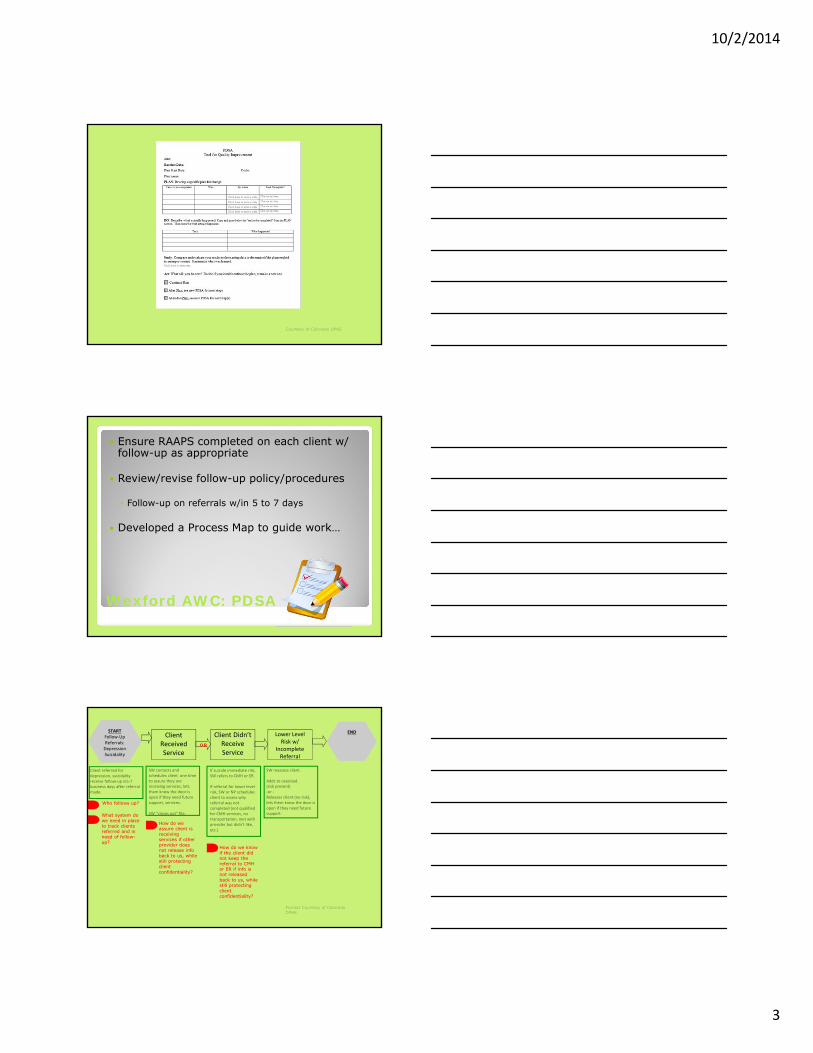
STARTFollow‐Up Referrals: DepressionSuicidality
Client Didn’t Receive Service
END
OR
Client referred for depression, suicidality receive follow‐up in5‐7 business days after referral made.
How do we know if the client did not keep the referral to CMH or ER if info is not released back to us, while still protecting client confidentiality?
Who follows up?
How do we assure client is receiving services if other provider does not release info back to us, while still protecting client confidentiality?
What system do we need in place to track clients referred and in need of follow-up?
Client Received Service
SW contacts and schedules client one time to assure they are receiving services, lets them know the door is open if they need future support, services.
SW “closes out” file.
If suicide immediate risk, SW refers to CMH or ER.
If referral for lower level risk, SW or NP schedules client to assess why referral was not completed (not qualified for CMH services, no transportation, met with provider but didn’t like, etc.)
SW reassess client .
Adds to caseload. (risk present)‐or ‐Releases client (no risk), lets them know the door is open if they need future support.
Lower Level Risk w/
Incomplete Referral
Format Courtesy of Colorado DPHE

10/2/2014
4
Outcomes
RAAPS completed on each client ◦ MH provider began administering
Process map informed revisions to policies/procedures
Follow-up on referrals w/in 5 to 7 days Some need more support than others Explanation needs to be offered as to why clients are referred out, at the time of referral
Grand Traverse: PDSA/Phase 1
Reflecting on the take-home message from the annual meeting
Getting more guys involved in the CAC and health center events to:◦ Promote awareness of the center◦ Determine perceptions of the health center
◦ How to make the health center more guy-friendly
◦ Find out what information they wanted to learn and how they wanted to learn it
◦ How to frame messages that would reach guys
Grand Traverse: PDSA/Phase 1
SAC planned, hosted Wellness Day Vendors & reps from tech programs & colleges
◦ PT/Sports Med: physical activity, wt. training◦ Male yoga instructor◦ “Dent and Scratch” – take care of equipment Sprains Physical symptoms: self-care, when to see a “doctor”
◦ Male counselor from health centers provided outreach, played up services for males

10/2/2014
5
What They Learned
Survey results reinforced parent involvement
◦ They like to go to parents for health information◦◦ They prefer to receive health information face-to-
face vs. electronically/through social media
The top three topics when thinking of health:◦ Injury◦ Nutrition◦ Death
Coming Attraction…
Students from the Career Tech Center’s media and automotive classes combining forces to make an infomercial encouraging guys to “take care of the equipment” via a contest
Plans to show at the State Theatre prior to movies
Grand Traverse: PDSA/Phase 2
Selection of male-friendly materials and décor
Determine outlets to get health center info out and the right messages
Sharpen clinical strategies to improve clinical interactions with males, comfort level

10/2/2014
6
Grand Traverse: PDSA/Phase 2
Identify clinical questions/clinical strategies to improve health outcomes for males
◦ Are we screening males for STI’s as appropriate?
◦ Are we getting completed RAAPS for males?
◦ Are we providing education in a way that makes males feel comfortable?
◦ Are we referring males for services at the appropriate level?
◦ Are education programs hitting home with males?
Improving HPV Immunization Rates among Males
HPV vaccine coverage among US adolescents is low compared to other recommended vaccines
Lower among males than females
What can CAHC’s do to improve HPV immunization rates among males?
Health Delivery, Inc.: PDSA
QuEST evaluation on attitudes, intention around HPV immunization
Incorporate HPV education into Safer Choices for 9th/10th graders
Incorporate HPV education into TETO, Real Talk Youth Symposium
TAC and CAC meet in fishbowl format for discussion on perceptions, barriers, and opportunities
Clinical Process: clean rosters, keep updated

10/2/2014
7
Not having provider recommendation
Recommendation from a health care provider is one of the most important factors in a parent’s decision to consent to the vaccine for their children!
Your Recommendation Matters!
0%10%20%30%40%50%60%70%80%
Received HPVImm:
HAD ProviderRecommendation
Did Not ReceiveHPV Imm:
DID NOT HAVEProvider
Recommendation
74%
52%
72%
26% GirlsBoys
In Practice…
When offering vaccine, providers tend to:
◦ Provide little information
◦ Highlight as optional
◦ Use a risk-based approach to offering
◦ Preferred to vaccinate girls more than boys
◦ Preferred to vaccinate older vs. younger adolescents
Holman et. al, 2013
10/2/2014
8
R.E.A.D.Y.
Recommend – using ACIP guidelines and the same as you would any other vaccine
Explain- protection offered, benefits, safety, efficacy
Answer/Assure-any questions on concerns e.g., cost, help with birds and bees talk (if mentioned)
Discuss-concerns and questions
Your whole team needs to have the same message and be willing to share it
QuEST
Provider support materials◦ Articles◦ CDC Tip Sheets, Posters, Brochures, Videos
Developed or assisted with survey questions Developed pre/post to use at events
Referred to regional MCIR coordinator for TA on features e.g., reminder and recall
Trouble-shooting, mid-point checks
Wexford AWC: PDSA
Write policy for f/up including time frame, methods
Learn to use MCIR reminder/recall features
Meet w/ YAC for ideas about promoting immunization/effective social media use
Contact rep re: magnet reminders
10/2/2014
9
What They Learned
◦ Texting better than a letter◦ Remind students and parents
Care Coordinator focused on follow-up can help but…
◦ A few parents did not want to complete the series although it had been initiated
◦ Some declined all immunizations
Gwinn AHC: PDSA
All health center staff have a united front when it comes to talking about immunizations
Revamp clinical process for reminders, scheduling
◦ Use EHR features to recall for appointments, reschedule missed appointments
◦ Send home (mail, w/ client)
◦ Call parent to follow-up on receipt, lack of
Gwinn AHC: PDSA
School provides info on 7th graders so GAHC can target mail
◦ Letters on HPV/immunization◦ Health center brochure◦ VIS sheet
Classroom distribution of materials in 6th and 7th grades
◦ Consent Form, VIS targeting clients on roster◦ Follow-up calls over summer to boost
10/2/2014
10
What They Learned
Community likes to see kids take charge and wants to support them
Success stems in part from increased parent outreach◦ When parents learn about HPV immunization, the anxiety dissipates (for parent & client)
Frequency of visits = more opportunities ◦ When a client receives immunizations at the health center, it encourages them to continue
HDNW-MI: PDSA
Assess, adjust HPV educational materials
Meet w/ CAC, YAC for promotional ideas Meet w/ peer educators
Incorporate HPV education elsewhere Press release: local survivor story
Survey local docs: really not supportive?

10/2/2014
11
What They Learned
Reframe with a strong cancer prevention message
Urban myths
Local docs DO support HPV immunization
◦ Who at the doc’s office isn’t supporting it?◦ What are other parent concerns?
New Slogans are Created…
Spread the word, not the germ…
Productivity Studies
Ten health centers completed productivity studies in 2014
Most all completed productivity studies in two different quarters for verification and comparison

10/2/2014
12
What Did We Learn?
Number of unduplicated users and visits related to the number of days/hours the center is open and the number of clinical hours provided
If a center diverts clinical staff away from clinical duties and closes its doors ~ difficult time reaching the number of unduplicated users and staying busy with visits
What Did We Learn?
Kids have to know the health center is open and they have to be able to build a relationship with the staff or they will not use the health center
Productivity will suffer, and so will revenue
What Did We Learn?
In general, centers in schools with <860 students see a higher proportion of the student population (>60%) as opposed to those in larger schools
◦ They also generally see around 500 users even when the school enrollment is not much more than 500
Visibility, a greater presence, relationship building
10/2/2014
13
What Did We Learn?
Health education may be more important than general community meetings in terms of return on investment of time
Centers with a high number of community meetings (not including CAC meetings) did not have a higher number of users/visits
What Did We Learn?
Correlation between providing health education in the school and number of unduplicated users?
Trend: centers with health education (+/-20 hours per quarter): ◦ Greater proportion of students enrolled ◦ Higher number of unduplicated users
What Did We Learn?
Health education may be of particular importance to school-linked centers and to school-based centers where populations may be transient or where there is diversity in the racial/ethnic population
May allow for familiarity with health center staff and services◦ Build trust◦ Increase comfort level in accessing services

10/2/2014
14
What Did We Learn?
Number of visits may be another way to look at productivity but consider acuity◦ May see a lot of users for “quicker & easier” visits such as immunizations but…
Providing more intensive services e.g., physical exams, asthma management, etc. takes longer◦ Impacts overall number of visits but also may increase reimbursement
What Did We Learn?
Staff size does not appear to be related to productivity
There is little time spent on Medicaid outreach events despite amount of uninsured population at some centers
FY15 CQI Projects
Increasing HPV Immunizations
Addressing Identified Disparities
10/2/2014
15
Feedback and Support
Feedback and Support
Posters