creating healthy environments: supporting the mental ... · hell…can't talk to nobody…i...
TRANSCRIPT

w w w . n c 4 y c . o r g
N a t i o n a l C e n t e r f o r Y o u t h i n C u s t o d y
Creating Healthy Environments: Supporting the Mental Health of Youth in Confinement Facilities
March 13, 2013
2:00-3:30 p.m. ET

w w w . n c 4 y c . o r g
Today’s Moderator:
Joyce Burrell is the Juvenile Justice Program Leader and Principal Investigator at the American Institutes for Research, and the Project Director for the OJJDP State Training and Technical Assistance Center. Joyce also serves as a content expert on the TA Partnership funded through the Comprehensive Community Mental Health Services to Children and Their Families, awarded by the Center on Mental Health Services at SAMHSA. Joyce has over twenty years of experience in juvenile justice, having run the juvenile justice systems for the state of New York, Washington, D.C., and Philadelphia, PA. She is a past president of the Council of Juvenile Correctional Administrators and sits on numerous boards and committees dedicated to improving outcomes for neglected, delinquent, and at-risk children. She is also a member of the NC4YC Working Group. Joyce has been recognized for her work, including as a recipient of the Albert Elias Award for Excellent Leadership in Juvenile Justice and the Golden Eagle Award from the National Juvenile Services Project for excellence in the field of juvenile justice. Joyce has a M.S. from the University of the District of Columbia, and a B.S. from D.C. Teacher's College.
Joyce Burrell

w w w . n c 4 y c . o r g
Facing the Need for Treatment in Juvenile Justice Facilities
• Screening and assessment made convincing
arguments to the field
• Investigation findings of unsafe conditions and insufficient mental health services
• Early reports and research predicted growth in mental health issues in facilities
• Budgets threatened by treatment costs

w w w . n c 4 y c . o r g
4
High Needs Youth in an Age of Reform
• Lower Numbers
• Shorter Lengths of Stay
• Staggering Costs
• Legal Interventions
• Higher Needs Youth Left Behind
– Complex
– Costly
– Risky for youth, staff, jurisdictions

w w w . n c 4 y c . o r g
5
Eating the Elephant in Times of Reform
Progress Over the Years
• Jurisdictions accept complex needs of youth
• Grappling for resources when population drops
• Mutual Aid helps, but…
• Lawsuits continue, but do not provide permanent resources

w w w . n c 4 y c . o r g
Presenter:
Located in Kalamazoo, Michigan, the Kalamazoo County Juvenile Home Schools—Intensive Learning Center provides education for court-involved youth who reside in the community. The center is a highly structured, behavior based program that provides instruction in the core academic subjects as well as specialized personal and social growth oriented courses.
*Readings from the FreeWrite Jail Arts and Literacy Program and “Growing Up Locked Down: Youth in Solitary Confinement in Jails and Prisons across the United States”, a report by Human Rights Watch and the American Civil Liberties Union
Youth from the Kalamazoo County Juvenile Home Schools-
Intensive Learning Center
Ivoriana
Demarcus
Tyrell

w w w . n c 4 y c . o r g
7
Readings Depicting the Pain
“Years of Tears” by Isaac C. – FreeWrite Jail Arts and Literacy Program Over the years I've cried many tears The days and the months combined And through the tears I could not see I thought I would not see forever The years of tears of which I have cried Are the results of my dreams which have died.
“The loneliness made me depressed and the depression caused me to be angry, leading to a desire to displace the agony by hurting others. I felt an inner pain not of this world. I allowed the pain that was inflicted upon me from my isolation placement build up while in isolation. And at the first opportunity of release, whether I was being released from isolation or receiving a cell-mate, I erupted like a volcano, directing violent forces at anyone in my path.” - From “Growing up Locked Down”

w w w . n c 4 y c . o r g
8
Readings Depicting the Pain “The cell was hell. Hell…Can't talk to nobody…I counted the bricks. There was a bed, a desk, a toilet, a sink, and a window. It was small because all the stuff was there…you can see outside - buses, birds, fields, people in the yard. You could see freedom, but you can't get out. It makes your time hell…The first thing I thought was, damn, I'm going to be here for 60 days…I felt like shit. Damn! No contact with anyone for 60 days?”
- From “Growing Up Locked Down”
“The only thing left to do is go crazy – just sit and talk to the walls . . . I catch myself talking to the walls every now and again. It’s starting to become a habit because I have nothing else to do. I can't read a book. I work out and try to make the best of it. But there is no best. Sometimes I go crazy and can't even control my anger any more . . . I can't even get out of solitary confinement early if I do better, so it is frustrating and I just lose it. Screaming, throwing stuff around . . . I feel like I am alone, like no one cares about me – sometimes I feel like, why am I even living?” - From “Growing Up Locked Down”
“I felt like I was going mad. Nothing but a wall to stare at. This was my tenth wall to stare at in my detention. I started to see pictures in the little bumps in the walls. Eventually, I said the hell with it and started acting insane. I made little characters with my hands and acted out video games I used to play on the outside – Dragon Ball Z, Sonic, Zelda – stuff like that. The staff would stare at me – looking at me like I'm crazy. I started talking to myself and answering myself. Talking gibberish. I even made my own language.”
- From “Growing Up Locked Down”
“Empty” by Joseph – FreeWrite Jail Arts and Literacy Program
How does it feel to be empty inside? What do you feel when you see a demon cry? The mirror shows me pain when I smile. I laugh to release pain, to get peace of mind Hope is hard to gain. It doesn't matter about guns or a knife It matters about the cries and screams inside at night. Hurt and frustration never leaves. When I cry it all out, that's what makes me empty inside.

w w w . n c 4 y c . o r g
Presenter:
Rodney Erwin, M.D., is a child and adolescent psychiatrist with Kaiser Permanente in Northern California. Dr. Erwin is a member of the NC4YC Working Group and is currently working with the OJJDP/DOJ OPDAT to train judges and prosecutors in Morocco on adolescent brain development and juvenile justice issues.
Dr. Erwin has worked as a psychiatric consultant to residential treatment centers for youth with severe emotional disorders, usually related to trauma and neglect. He also served as the psychiatrist in a juvenile detention facility and county jail, working with a severely at-risk population. He has served as a mental health care and medical care monitor for juvenile justice facilities in California and Georgia.
Dr. Erwin received his M.D. from the University of Texas Southwestern Medical Center in Dallas. He completed his internship in Pediatrics at the Combined Residency Program in Boston before completing residency and child and adolescent psychiatry fellowship at the University of California-San Francisco.
Dr. Rodney Erwin

w w w . n c 4 y c . o r g
10
Youth with Mental Health Diagnoses
• Disproportionately represented in juvenile justice facilities
• Reflect higher needs and risks
• Require even greater collaboration of all involved stakeholders
w w w . n c 4 y c . o r g
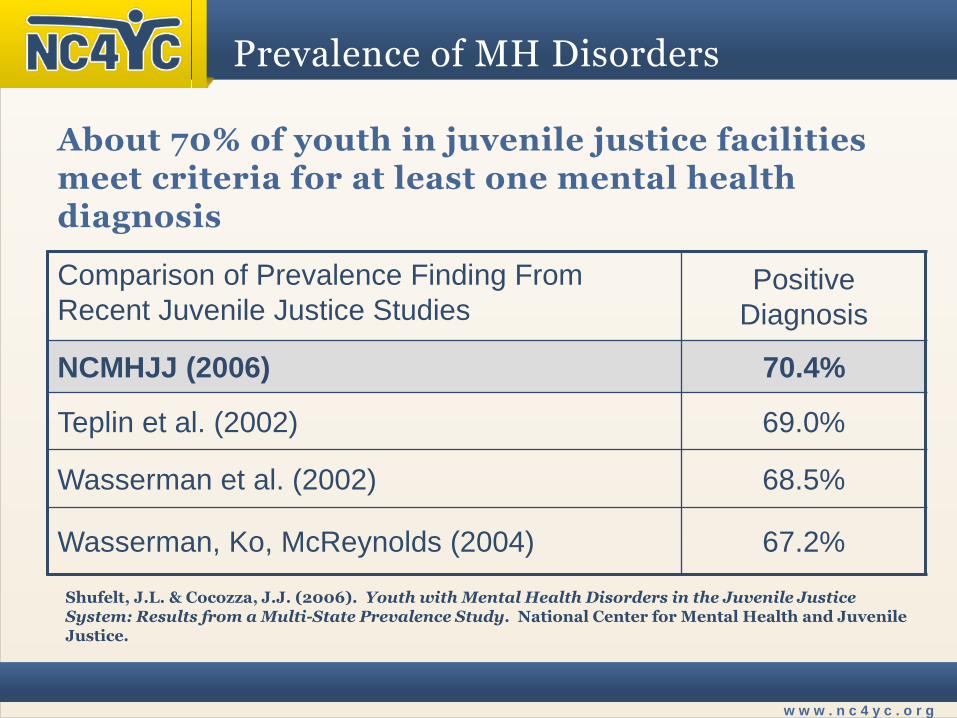
About 70% of youth in juvenile justice facilities meet criteria for at least one mental health diagnosis
Comparison of Prevalence Finding From
Recent Juvenile Justice Studies Positive
Diagnosis
NCMHJJ (2006) 70.4%
Teplin et al. (2002) 69.0%
Wasserman et al. (2002) 68.5%
Wasserman, Ko, McReynolds (2004) 67.2%
Shufelt, J.L. & Cocozza, J.J. (2006). Youth with Mental Health Disorders in the Juvenile Justice System: Results from a Multi-State Prevalence Study. National Center for Mental Health and Juvenile Justice.
Prevalence of MH Disorders
w w w . n c 4 y c . o r g
12
Comorbidities and Severity
• Comorbidities – 79% of youth with mental health disorder met criteria for 2
or more diagnoses, with over 60% with 3 or more disorders – Over 90% of youth with Conduct Disorders also
experienced at least one other mental disorder
• Link with Substance Abuse
– 60.8% of youth with a mental disorder also had a substance use disorder
• Severity
– About 27% of justice-involved youth have disorders that are serious enough to require immediate and significant treatment
Shufelt, J.L. & Cocozza, J.J. (2006). Youth with Mental Health Disorders in the Juvenile Justice System: Results from a Multi-State Prevalence Study. National Center for Mental Health and Juvenile Justice.

w w w . n c 4 y c . o r g
13
Mental Health for Girls
Justice-Involved Girls at Higher Risk for MH Disorders than Boys
66.8%
26.4%
14.3%
44.9% 43.2%
81%
56%
29.2%
51.3% 55.1%
0
10
20
30
40
50
60
70
80
90
AnyDisorder
AnxietyDisorder
MoodDisorder
DisruptiveDisorder
SubstanceAbuse
Disorder
Males
Females
Shufelt, J.L. & Cocozza, J.J. (2006). Youth with Mental Health Disorders in the Juvenile Justice System: Results from a Multi-State Prevalence Study. National Center for Mental Health and Juvenile Justice.
w w w . n c 4 y c . o r g
14
Issues of Treatment
• Is it the role of juvenile justice facilities to provide mental health treatment?
• What are potential advantages and disadvantages of delegating this task to facilities?
• Does providing mental health treatment reduce future delinquency and recidivism?

w w w . n c 4 y c . o r g
15
Relationships Between Mental Health and Delinquency
• Youth with affective disorders
– increased irritability, anger, and hostility
• Youth with anxiety disorders
– less aggressive than their peers, except youth with PTSD, who may respond to threats aggressively and unexpectedly
• Youth with PTSD and Conduct Disorders
– more impulsive and aggressive than youth with Conduct Disorders alone
• Youth with ADHD
– more impulsive and tend to be more emotionally reactive

w w w . n c 4 y c . o r g
16
Relationships Between Mental Health and Delinquency
• Substance use disorders in youth
– increased risk of violence, risky sexual behaviors, poor judgment and impulse control, and continued contact with the juvenile justice system
• Substance use disorders + depression + anxiety
– increased odds of serious and violent offenses as adults
– more predictive than substance use alone

w w w . n c 4 y c . o r g
17
Relationships Between Mental Health and Delinquency
Youth may display signs & symptoms of their MH disorders that lead to behaviors that are:
- Misinterpreted - More challenging to manage
These signs & symptoms include: - Anger - Irritability - Cognitive deficits - Impulsivity - Paranoia - Heightened emotional and physical reactivity to
environmental stimuli - Flight-or-fight syndrome

w w w . n c 4 y c . o r g
18
Interventions
OJJDP Survey of Youth in Residential Placement (2010)
Use of Force
– More than 33% reported staff used unnecessary force with residents
Physical and Chemical Restraints
– 28% reported staff used some method of restraint on them
– 7% reported staff’s use of pepper spray on them
– 4% reported being placed in a restraint chair
Isolation
– 35% reported being place in isolation (55% for longer than 24 hours)

w w w . n c 4 y c . o r g
19
Interventions
• Most successful interventions for most youth with MH disorders
– community-based
– address the youth’s needs in the context of his/her community and social life
• Examples include Functional Family Therapy and Multi-Systemic Therapy

w w w . n c 4 y c . o r g
20
What Can Facilities Do?
Screen Youth for MH Issues
• Every youth upon intake
• Standardized, evidence-based, well-validated, brief, relevant, youth-oriented screening tools essential
– Example of MAYSI-2
• Identification of imminent risk and current mental health needs of youth

w w w . n c 4 y c . o r g
21
What Can Facilities Do?
Assess & Plan for Treatment
• Assessment is further evaluation identified through screening process
• More extensive psychosocial evaluation
• More detailed diagnostic information that may be used in creating individualized treatment plans for youth
– Example of DISC-IV

w w w . n c 4 y c . o r g
22
What Can Facilities Do?
• Create Positive & Therapeutic Environments
• Implement Evidence-Based Treatments
– Drug and Alcohol Treatment
– Cognitive-Behavioral Therapy (CBT), including Trauma-Focused CBT
– Medication Management
– Principles of Functional Family Therapy & Multi-Systemic Therapy
w w w . n c 4 y c . o r g
Presenter:
Ines Nieves is the Associate Commissioner for Youth Programs and Services for the New York State Office of Children and Family Services (OCFS). She is responsible for the operation and supervision of several bureaus including Education, Health Services, Youth in Transition, Behavioral Health Services, Ministerial Services, Special Priorities and the agency Chief Psychiatrist. At OCFS, Ines has helped move the juvenile justice system towards becoming a more therapeutic, trauma informed, and integrated system of care. She has led teams in developing new restraint policies and techniques, the New York State trauma-responsive model of care, implementation of the Sanctuary Model and Dialectical Behavioral Therapy, and strategies to address “culture change” in residential settings. Ines has over thirty years of experience in juvenile justice. She has been a partner in several consulting businesses, has provided training for juvenile correctional programs nationally, and has received national recognition for her work with female offenders and gender specific programming. Ines received her Master of Science Degree from Springfield College in Massachusetts.
Ines Nieves

w w w . n c 4 y c . o r g
Presenter:
Dr. Tomassone is the Chief of Treatment Services for the New York State Office of Children and Family Services Division of Juvenile Justice and Opportunities for Youth (DJJOY). In addition to individual facility clinical oversight, he is responsible for developing mental health policy and programming for the Bureau of Behavioral Health within the Division. He is the principal author of The NY Model, a trauma-responsive program which revises and reconceptualizes the delivery of services to juvenile justice involved youth throughout New York State. Dr. Tomassone is responsible for the implementation and oversight of mental health programming in several DJJOY residential facilities. He has over twenty five years of experience working with children, adolescents, and families, including as a direct care clinician, and has helped developed various DJJOY programs, including the psycho educational curriculum, Adelanté, which addresses abuse issues in young women. Dr. Tomassone received his Ph.D. in Clinical Psychology from the University of Rochester, and trained at the Child and Adolescent Psychiatry Clinic at Strong Memorial Hospital in Rochester NY. He is a licensed psychologist in New York State.
Dr. Joseph Tomassone
w w w . n c 4 y c . o r g
25
New York State: New Directions
• NYS Transformation of the Juvenile Justice System
– New York State System Changes 2004
– Increasing Youth Special Needs (from 2010 Internal Screening)
• Mental Health – approx. 70%
• Substance Abuse – approx. 80%
• Special Education – approx. 30%
– External Pressures to Change
– 2007 – Political Changes
• Juvenile Justice Reform Agenda

w w w . n c 4 y c . o r g
26
Juvenile Justice Reform Agenda
• Juvenile Justice Reform Agenda – Restraints
• Re-examine the use of physical interventions
– State Fiscal Crisis
• Rethinking services to youth
• Juvenile justice service systems were shrinking
– NYS closures
– Recognition of Trauma
• Prevalence of trauma in JJ populations
– Full PTSD diagnosis - estimates to 50%+ (Wolpaw, et al., 2004)
– Trauma single incident - estimates to 90%+ (Abram, et al., 2004)

w w w . n c 4 y c . o r g
27
Trends: Trauma
• Impacts of trauma on staff and system trauma
– Staff histories of trauma
• Personal histories
• Professional experiences
– System Traumas
• Politicization of JJ youth care
• Media scrutiny and criticism
• Downsizing of JJ and juvenile MH systems
• System instability and unpredictability
– Job (in)security, career and family impacts
w w w . n c 4 y c . o r g
28
Results for NYS JJ System
– High levels of stress in the system for both youth and staff
– Poor youth compliance and engagement in residential programming
– Low staff morale, high rates of workman’s comp and unscheduled absences and call-in’s
– High levels of use of physical force with youth
– High levels of staff and youth injuries

w w w . n c 4 y c . o r g
29
Goals and Challenges for NYS
General Goal: Provide residential care services and supports to an increasingly smaller but increasingly complex and challenged population of youth.
Specific Goals:
– Create and maintain emotional and physical safety for both youth and staff
– Reduce the use of unnecessary and potentially harmful physical interventions
– Address previous, and reduce both current and future impacts of trauma on both youth and staff

w w w . n c 4 y c . o r g
30
Goals and Challenges for NYS
Specific Goals (cont.):
– Meet the therapeutic and MH needs of an increasingly complex and multi-challenge population of youth in care
– Change our organizational culture
• From focus on custody, to focus on treatment
• From focus on safety via authority, to focus on safety via relationships
• From focus on youth as individuals to focus on youth as members of a family system, a community, and in their own unique context
w w w . n c 4 y c . o r g
31
The NY Model: T.R.E.A.T.
• Trauma Responsive Engagement And Treatment
– a.k.a. “The NY Model”
– Uses a trauma informed environment as the critical foundation for creating and maintaining safety.
– Youth generated goals are identified and linked to the supports, services and skills needed to achieve them. Youth are thus engaged in their own individual pursuits.
– Relies on a community of support people who are engaged to assist youth and family in acquiring the skills needed to achieve their goals.

w w w . n c 4 y c . o r g
32
Strategies to Enhance Treatment Capacity (1 of 4)
• Create an infrastructure of licensed MH professionals who provide assessment and guide youth treatment planning.
– Hired licensed SWs, Psychologists, & Psychiatrists
– Full time, part time, contract, partnered with NYS OMH and community providers
– Promoted or hired MH supervisors (coaches)
– Created hybrid positions: Admin/MH
– Enhanced line staff and case management lines

w w w . n c 4 y c . o r g
33
Strategies to Enhance Treatment Capacity (2 of 4)
• De-mystify the provision of MH services to youth so that line staff are integral to treatment.
– Line staff know the youth best
• Input to youth program is critical
• Understanding of youth (including MH) enables them to do their job effectively
• Equal importance within youth’s Support Team
– Line staff “own” the facility environments
• Responsible for physical environments
• Responsible for emotional environment
• Responsibility + Authority = Ownership/Pride

w w w . n c 4 y c . o r g
34
Strategies to Enhance Treatment Capacity (3 of 4)
• Create “community” among those in facility and within the youth’s community to support youth.
– Everyone who interacts with youth regularly is part of their Support Team
– Youth Support Team also includes youth, their family, and members of the community (staff and others) who support and care for the youth
– The youth and family set the goals
– The TEAM takes responsibility for solving problems and supporting the youth to achieve their goals

w w w . n c 4 y c . o r g
35
Strategies to Enhance Treatment Capacity (4 of 4)
• Design individual plans and programming with youth generated goals as focus to maximize motivation and reduce power struggles.
– Youth and family goals are the center of youth programming
– Youth work harder at goals that have meaning for them
– Setbacks or problem behaviors then become an issue of helping the youth get back on “their” track
– Helps to avoid power struggles or youth opposition to “facility” rules or “our goals” for youth

w w w . n c 4 y c . o r g
36
T.R.E.A.T. – Foundational Elements
• Create and Maintain Safety
• Enhance Skills and Promote Effective Goal-Directed Behaviors
• Facilitate Engagement
Safety
Engagement Skills

w w w . n c 4 y c . o r g
37
T.R.E.A.T. – Program Components
• Synthesis of Ecological and Treatment Programming
The Sanctuary Model ®, Sandra Bloom, M.D. • Trauma informed environment • Organizational change • Promising practice
Dialectical Behavior Therapy (DBT), Marsha Linehan, Ph.D. • Cognitive Behavioral base • Strengths and skills focused • Goal: emotional self-regulation leading to behavioral self-regulation • Validated for JJ populations • Empirically validated treatment
The Missouri Model (Missouri Youth Services Institute - MYSI) • Formation of Youth and Staff Community • Formation of Teams and Effective Teamwork • Engagement of youth and staff • Solidify trauma informed and skills/strengths focused environment

w w w . n c 4 y c . o r g
38
T.R.E.A.T. - SAFETY
• Trauma-informed environment
– Increase staff and youth knowledge & understanding of trauma and its impacts and outcomes
• Non-judgmental approach with accountability
– Does not blame youth, but does not absolve responsibility for problem behavior either.
– Behavior has outcomes—positive or negative
– “You did not create all of your problems,
but you MUST be involved in solving them”.
– People are “stuck”, not “broken”.
Safety
Engagement
Skills

w w w . n c 4 y c . o r g
39
T.R.E.A.T. - SKILLS
• Enhance Skills and Promote Effective Goal-Directed Behaviors
– Strengths-based systems – crucial
– Cognitive-Behavioral based system
– Daily skill/behavior reinforcement program
– Line staff provide the vast majority of the interventions
– Line staff “own” units Safety
Engagement
Skills

w w w . n c 4 y c . o r g
40
T.R.E.A.T. - ENGAGEMENT
• Facilitate Engagement (& Empowerment)
– Focus on group process (i.e., team, family)
– Focus on relationships (youth-staff, staff-staff, admin-staff)
– Youth and family set their own goals
– Staff and others support the youth in achieving goals.
• Staff are aligned with youth goals
– ALL staff are agents of change for youth.
We should take them where THEY want to go,
Not where WE think they should go.
Safety
Engagement
Skills

w w w . n c 4 y c . o r g
41
Maintenance of the NY Model
Maintenance of a Trauma Responsive
Model
Focus on Outcomes
Training Training Training
Coaching
Supervision and
Accountability
Changing the
Culture
Tracking of Data &
Creating a Data Base
Quality Assurance
System

w w w . n c 4 y c . o r g
42
The NY Model: T.R.E.A.T.
• T.R.E.A.T. creates a trauma-responsive program which uses relationships between youth and staff, in the context of an entire community of supportive people and systems, to promote the use of skillful and effective behaviors to assist youth in reaching self-identified goals.
• The creation of a safe environment is supported and maintained by trained staff and the motivated and engaged behavior of youth who are striving for achievements and goals that are meaningful to them.
• The concepts, principles and strategies of the T.R.E.A.T. model apply equally to ALL members of our organizational community.

w w w . n c 4 y c . o r g
Questions & Answers
Moderator:
Ms. Joyce Burrell
Ms. Ines Nieves
Dr. Rodney Erwin Dr. Joseph Tomassone

w w w . n c 4 y c . o r g
NC4YC
Upcoming Webinars:
Solitary Confinement of Youth
April 3, 2013, 2 p.m. – 4 p.m.
Family Engagement
May 8, 2013, 2 p.m. – 3:30 p.m.
Sustaining the Quality: Internal/External Monitoring of Conditions Issues
May 22, 2013, 2 p.m. – 3:30 p.m.
Please complete the webinar evaluation at the conclusion of the webinar. Thank you!

w w w . n c 4 y c . o r g
This project is supported by Cooperative Agreement 2010-JF-FX-K005 awarded by the Office of Juvenile Justice and Delinquency Prevention (OJJDP), Office of Justice Programs, U.S. Department of Justice. Points of view or opinions expressed in this document do not necessarily represent the official position or policies of these agencies.