cross sectional anatomy ventricular septal defects: a€¦ · brheartj1988;59:339-51 thecross...
TRANSCRIPT
Br Heart J 1988;59:339-51
The cross sectional anatomy of ventricular septaldefects: a reappraisal
E J BAKER,* M P LEUNG,t R H ANDERSON, D R FISCHER, J R ZUBERBUHLER
From the Division of Cardiology, Children's Hospital, Pittsburgh, Pennsylvania, USA
SUMMARY The cross sectional echocardiographic description of holes in the ventricular septumhas been unsatisfactory, .chiefly because there are so many classifications of this defect. Theaccurate description of the anatomy of individual defects, from cross sectional images, is moreimportant than. attempts to fit them into a preconceived classification. One hundred specimens ofhearts with a ventricular septal defect were reviewed to identify those features that are of value inthe interpretation of cross sectional images. Three groups of defect were identified: those whichabutted the central fibrous body, those with a margin partly formed by an area offibrous continuitybetween the leaflets. of the aortic and pulmonary valves, and those with entirely muscular margins.Each group had features that were readily discernible in cross section. Other features of the defectsseen in the-cross sectional images identified defects that opened between the two ventricular inlets,defects that opened between the two subarterial outlets, and those that extended solely into thetrabecular septum. The criteria for describing the, anatomy of defects were established in heartswith normal connections, but they were found to be equally applicable in hearts with discordantatrioventricular connection, discordant ventriculoarterial connection, common arterial trunk, anddouble outlet.from the morphologically right ventricle. Cross sectional imaging, by echocardio-graphy and potentially by other techniques, provided a uniquely detailed and precise descriptionof the morphology of ventricular septal.defects.
he- understanding of the morphology of holesbetween t-he ventricles has been complicated by theplethora of existing and proposed schemes of clas-sification. Several cross sectional echocardiographicstudies of the anatomy of ventricular septal defectshave been published."' In each, the authors inter-preted the echocardiographic images by reference toan established classification. Despite these reports, orperhaps because ofthem, uncertainties remain aboutthe- interpretation of cross sectional images of ven-tricular septa-l ddects. We have, therefore, restudiedthe morbid anatomy of ventricular septal defects toidentify those morphological features that are impor-tant in the interpretation of cross sectional images.
Requuests for reprints to Dr E J Baker, Department of PaediatricCardiology, Guy7s Hospital, London SEI 9RT.
*Prescnt address: Department of Paediatric Cardiology,, Guy's Hospital,London SEI 9RT.tPresent address: Grantham Hospital, University of Hong Kong.
Acceptedfor publication.21 September 1987
Patients and method
We examined a representative series -of specimenswith a ventricular septal defect from the heartmuseum of the Children's Hospital of Pittsburgh.Hearts with an atrioventricular septal defect, pul-monary or aortic atresia, or a univentricular atrioven-tricular connection were excluded. The margins ofeach defect were carefully inspected to identify thefeatures that were amenable to cross sectional imag-ing. Where necessary, hearts were sectioned tosimulate echocardiographic planes and to clarify thecross sectional appearances. After the anatomicalstudy, cross sectional echocardiograms from patientswith ventricular septal defects studied at the Chil-dren's Hospital, Pittsburgh were selected to illustratesome of the important morphological features.
Results
In all, 100 hearts were examined (table). Fifty twohad a ventricular septal defect in the setting of usual(concordant) chamber connections. In addition, we
339
group.bmj.com on October 22, 2017 - Published by http://heart.bmj.com/Downloaded from
340
Table A list of hearts examined with the category ofventricular septal defect
Connection No
Normal connections:Perimembranous 42Muscular 8Doubly committed and juxta-arterial 2
Complete transposition:Perimembranous 4Muscular 9Doubly committed and juxta-arterial 1
Congenitally corrected transposition:Perimembranous 2Doubly committed and juxta-arterial 1Both doubly committed and perimembranous 1
Double outlet of the right ventricle:Perimembranous 14Muscular 1Doubly committed and juxta-arterial 4
Common arterial trunkPerimembranous 8Muscular right ventricular margin 3
examined 18 hearts with ventricular septal defect anda discordant ventriculoarterial connection-14 ofthese had a concordant atrioventricular connectionand four a discordant atrioventricular connection. Acommon arterial trunk was present in 11 hearts, all
Baker, Leung, Anderson, Fischer, Zuberbuhlerwith a concordant atrioventricular connection. Afinal group of 19 hearts was studied with doubleoutlet from themorphologically right ventricle, againin the setting of a concordant atrioventricular con-nection. Some of the hearts in this series have beendescribed in previous studies.'
HEARTS WITH CONCORDANTATRIOVENTRICULAR AND VENTRICULOARTERIALCONNECTIONS
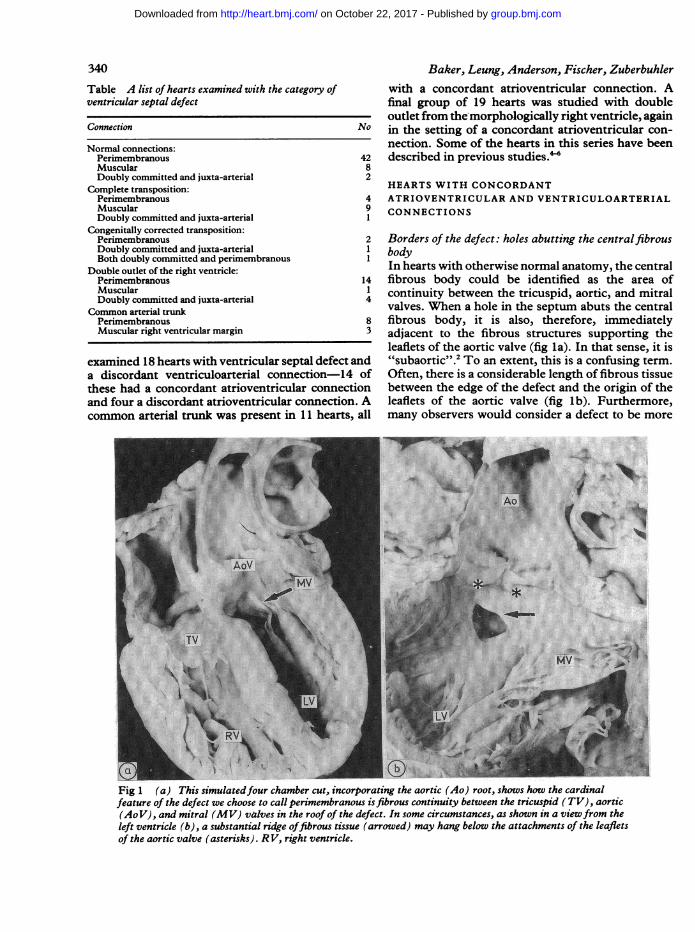
Borders of the defect: holes abutting the centralfibrousbodyIn hearts with otherwise normal anatomy, the centralfibrous body could be identified as the area ofcontinuity between the tricuspid, aortic, and mitralvalves. When a hole in the septum abuts the centralfibrous body, it is also, therefore, immediatelyadjacent to the fibrous structures supporting theleaflets of the aortic valve (fig la). In that sense, it is"subaortic".2 To an extent, this is a confusing term.Often, there is a considerable length of fibrous tissuebetween the edge of the defect and the origin of theleaflets of the aortic valve (fig lb). Furthermore,many observers would consider a defect to be more
...._....~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~...
Fig 1 (a) This simulatedfour chamber cut, incorporating the aortic (Ao) root, shows how the cardinalfeature of the defect we choose to call perimembranous isfibrous continuity between the tricuspid (TV), aortic(AoV), and mitral (MV) valves in the roof of the defect. In some circumstances, as shown in a viewfrom theleft ventricle (b), a substantial ridge offibrous tissue (arrowed) may hang below the attachments of the leafletsof the aortic valve (asterisks). R V, right ventricle.
group.bmj.com on October 22, 2017 - Published by http://heart.bmj.com/Downloaded from
Cross sectional anatomy of ventricular septal defectsobviously "subaortic" when there is overriding ofthevalve orifice as, for example, in the tetralogy ofFallot.There is, none the less, a need to describe specificallythose defects bordered superiorly by the fibroustissue supporting the aortic root. A major componentof this tissue is the atrioventricular membranousseptum and the defects are disposed around thisfibrous partition. For this reason, and despite thereservations expressed by others, we continue todescribe this group of defects as perimembranous.7Perimembranous defects were the most common
in this series. The openings ofsome ofthem extendedinto the inlet, outlet, or trabecular zones of theventricles. Small defects could be judged morpho-logically to be opening into the right ventricular inletor outlet by virtue of their relation to the medialpapillary muscle. Defects above the papillary musclehave been termed "outlet", and those beneath it"inlet", while trabecular extension is indicated byinsertion ofthe papillary muscles at the apical marginof the defect.7 This morphological distinction wasdifficult to make in the hearts in which the medialpapillary muscle was multiple or ill defined. Further-more, this relation seemed unlikely to be identified bycross sectional imaging. Thus for imaging purposes
PT..... . : s b... S .. n No. . ...... ; ...... .. . . - . -.... .. ... ........... .. ....... ....* ... .. i .*:. :: ::::
....... * .:w.:1E
..S §. d: e .... :: '* : _C:::. .:: .. e. !_ _: . .. :::: ::?q ! .':} .:
.-S'.
.t'
... :. .::..:: :: .:: .-3:
:: ,.'.::SS::.. :. :SiE:'{
:i.}^w£ _
RY r
341we considered it inappropriate to use the terms"inlet", "outlet", and "trabecular" for the descrip-tion of small perimembranous defects. Largeperimembranous defects extending posteriorly toopen into the right ventricular inlet formed a welldefined group, as did those large defec-ts that exten-ded anteriorly to open into the subpulmonary rightventricular outflow tract. In contrast, large perimem-branous "trabecular" defects did not form a distinctgroup. Indeed, they had no morphological featuresthat distinguished them from perimembranousdefects extending to open into both the outlet andinlet ofthe right ventricle. This group was, therefore,described as "confluent".
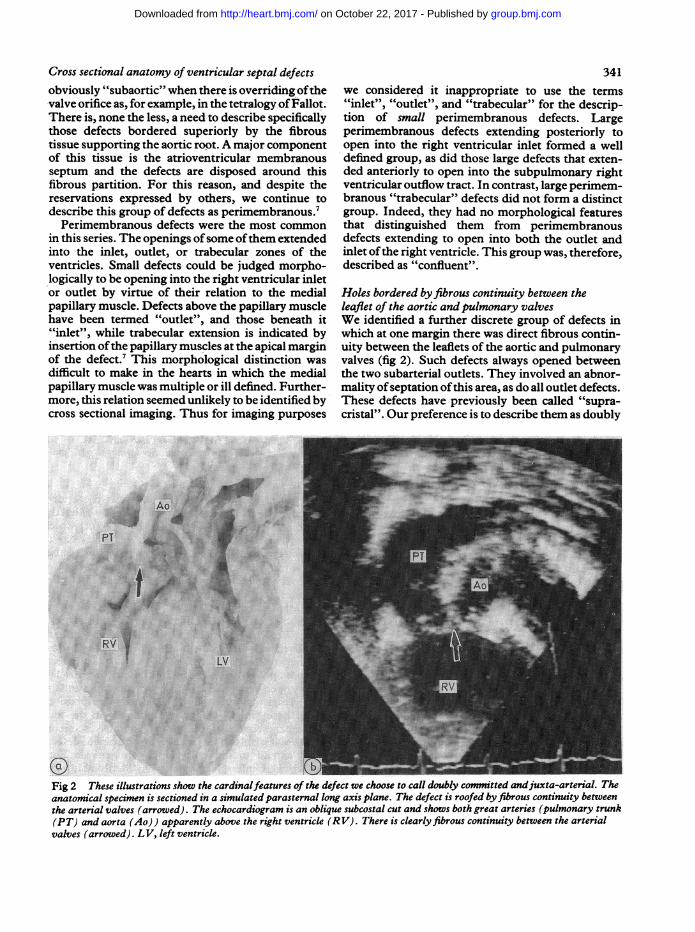
Holes bordered byfibrous continuity between theleaflet of the aortic and pulmonary valvesWe identified a further discrete group of defects inwhich at one margin there was direct fibrous contin-uity between the leaflets of the aortic and pulmonaryvalves (fig 2). Such defects always opened betweenthe two subarterial outlets. They involved an abnor-mality ofseptation ofthis area, as do all outlet defects.These defects have previously been called "supra-cristal". Our preference is to describe them as doubly
Fig 2 These illustrations show the cardinalfeatures of the defect we choose to call doubly committed andjuxta-arterial. Theanatomical specimen is sectioned in a simulated parasternal long axis plane. The defect is roofed byfibrous continuity betweenthe arterial valves (arrowed). The echocardiogram is an oblique subcostal cut and shows both great arteries (pulmonary trunk(PT) and aorta (Ao)) apparently above the right ventricle (RV). There is clearlyfibrous continuity between the arterialvalves (arrowed). LV, left ventricle.
:
group.bmj.com on October 22, 2017 - Published by http://heart.bmj.com/Downloaded from
Baker, Leung, Anderson, Fischer, Zuberbuhler
LV
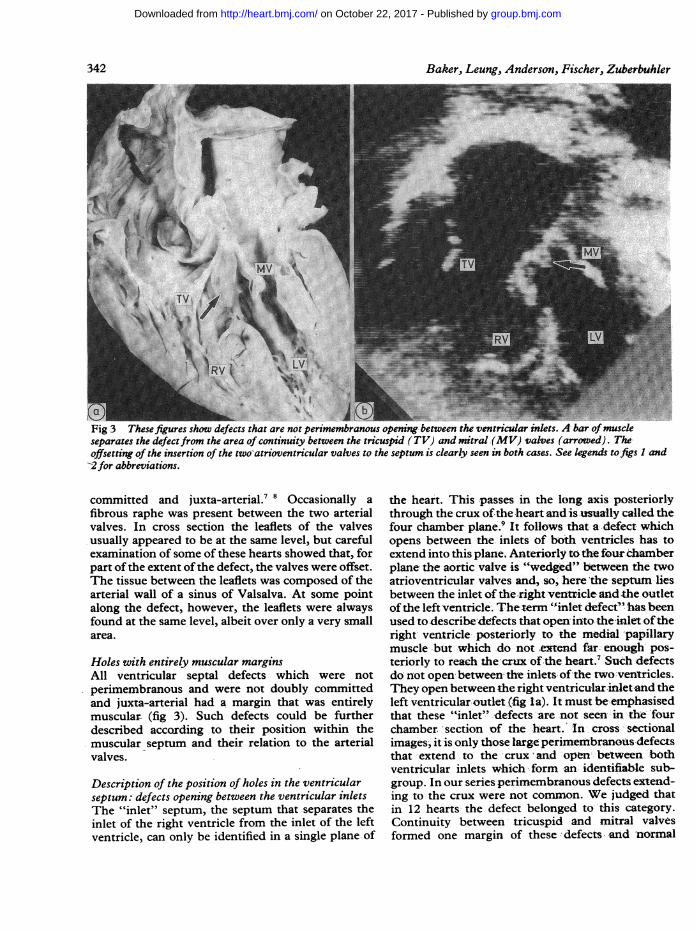
Fig 3 These figures show defects that are not perimembranous opening-between the ventricular inlets. A bar of muscleseparates the defectfrom the area of continuity between the tricuspid (TV) and mitral (MV) valves (arrowed). Theoffsetting of the insertion of the two-atrioventricular valves to the septum is clearly seen in both cases. See legends tofigs I and2for abbreviations.
committed and juxta-arterial.7 8 Occasionally afibrous raphe was present between the two arterialvalves. In cross section the leaflets of the valvesusually appeared to be at the same level, but carefulexamination of some of these hearts showed that, forpart of the extent ofthe defect, the valves were offset.The tissue between the leaflets was composed of thearterial wall of a sinus of Valsalva. At some pointalong the defect, however, the leaflets were alwaysfound at the same level, albeit over only a very smallarea.
Holes with entirely muscular marginsAll ventricular septal defects which were notperimembranous and were not doubly committedand juxta-arterial had a margin that was entirelymuscular (fig 3). Such defects could be furtherdescribed according to their position within themuscular septum and their relation to the arterialvalves.
Description of the position of holes in the ventricularseptum: defects opening between the ventricular inletsThe "inlet" septum, the septum that separates theinlet of the right ventricle from the inlet of the leftventricle, can only be identified in a single plane of
the heart. This -passes in the long axis posteriorl-ythrough the crux of the heart and is usually called thefour chamber plane.9 It follows that a defect whichopens between the inlets of boih ventricles has toextend into this plane. Anteriorly to the fourchamberplane- the aortic valve is "wedged" between the twoatrioventricular valves and, so, here 'the septumn liesbetween the inlet of the right ventricleandthe outletof the left ventricle. Thetenn "inlet defect" has beenused to describe-defects that open into the -inlet oftheright ventricle posteriorly to the medial papillarymuscle but-which do not extend far. enough pos-teriorly to reach the cr-ux of the heart.7 Such-defectsdo not open' between the inlets of-the two ventricles.They open between the right ventricular inlet.nd theleft ventricular outlet (fig Ia). It must be emphasisedthat these "inlet".-defects -are not seen in the 'fourchamber section of the heart. In cross sectionalimages, it is only those large perimembranous defectsthat extend to the crux and open between bothventricular inlets which form an identifiable sub-group. In our series perimembranous defects extend-ing to the crux were not common. We judged thatin 12 hearts the defect belonged to this category.Continuity between tricuspid and mitral valvesformed one margin of these defects -and normal
342
group.bmj.com on October 22, 2017 - Published by http://heart.bmj.com/Downloaded from
Cross sectional anatomy of ventricular septal defects
RV rW
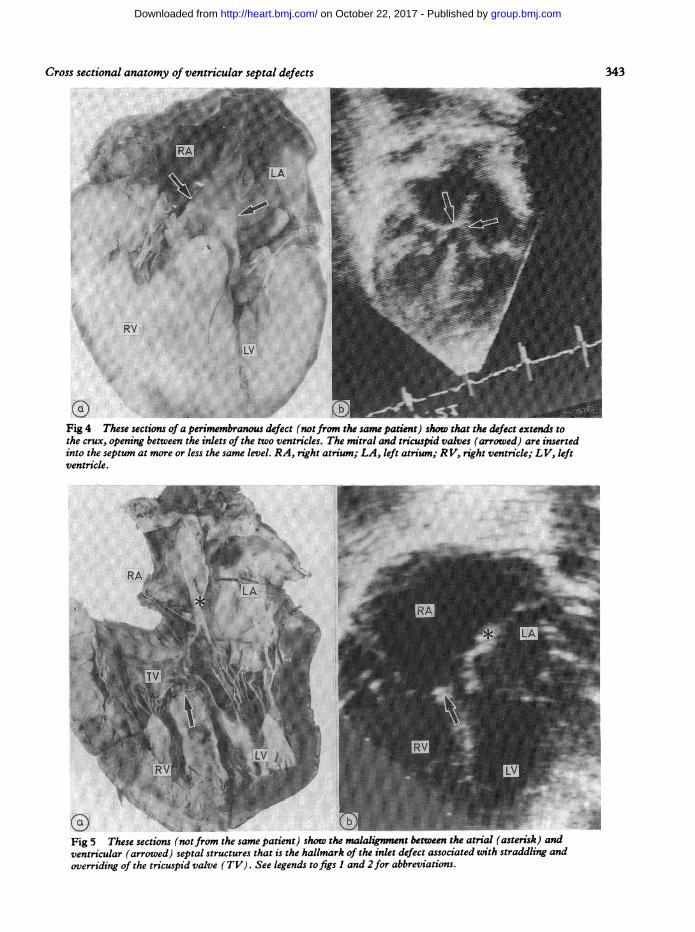
Fig 4 These sections of a perimembranous defect (notfrom the same patient) show that the defect extends tothe crux, opening between the inlets of the two ventricles. The mitral and tricuspid valves (arrowed) are insertedinto the septum at more or less the same level. RA, right atrium; LA, left atrium; RV, right ventricle; LV, leftventricle.
Fig 5 These sections (notfrom the same patient) show the malalignment between the atrial (asterisk) andventricular (arrowed) septal structures that is the hallmark of the inlet defect associated with straddling andoverriding of the tricuspid valve (TV). See legends to figs I and 2for abbreviations.
343
group.bmj.com on October 22, 2017 - Published by http://heart.bmj.com/Downloaded from
344
offsetting of the two atrioventricular valves wasabsent (fig 4). In one heart in this group, the tricuspidvalve overrode and straddled the defect so that theinferoseptal commissure was attached to a papillarymuscle within the left ventricle. This was associatedwith considerable malalignment between the atrialseptum and the posterior component of the muscularventricular septum (fig 5). None of these heartsshowed the morphological stigmata of atrio-ventricular septal defects ("endocardial cushiondefects") and none had trileaflet left atrioventricularvalves. They are appropriately described asperimembranous defects opening between the inletsof both ventricles-they should not be called"atrioventricular canal defects".Muscular defects opening between the ventricular
inlets also extended into the four chamber plane.They were, in contrast, separated from the atrio-ventricular valves by a muscle bundle and the normaloffsetting of insertion of the valves into the septumwas preserved (fig 3). In one heart with a muscularinlet defect, the defect straddled the tricuspid valve.
Holes between the subarterial outletsThe relation between the aortic and pulmonaryvalves in normal hearts is such that a true "outletseptum", a septum separating the outflows of the left
Baker, Leung, Anderson, Fischer, Zuberbuhler
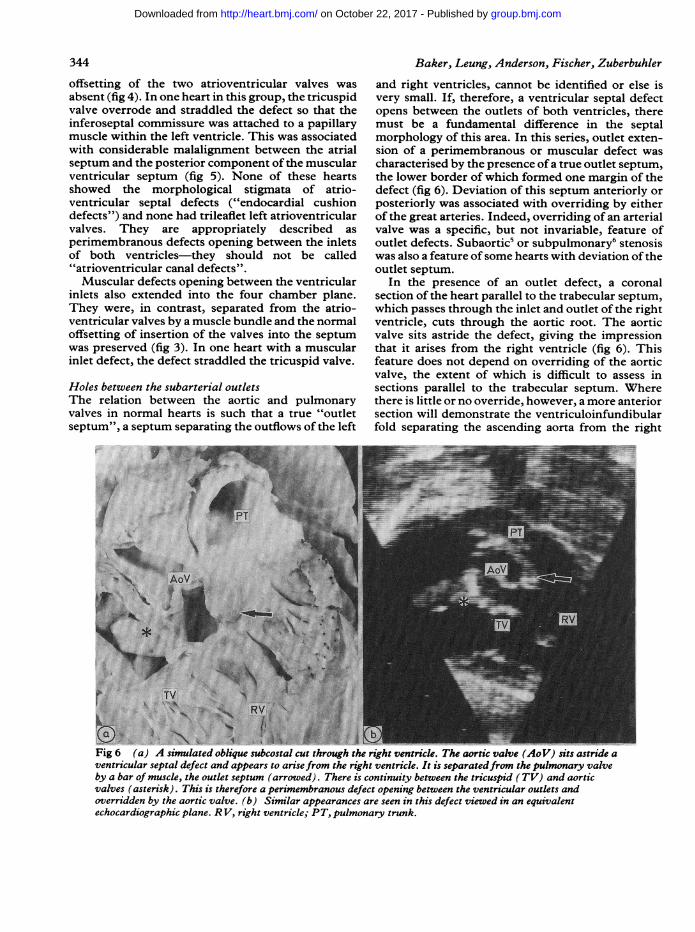
and right ventricles, cannot be identified or else isvery small. If, therefore, a ventricular septal defectopens between the outlets of both ventricles, theremust be a fundamental difference in the septalmorphology of this area. In this series, outlet exten-sion of a perimembranous or muscular defect wascharacterised by the presence ofa true outlet septum,the lower border of which formed one margin of thedefect (fig 6). Deviation of this septum anteriorly orposteriorly was associated with overriding by eitherof the great arteries. Indeed, overriding of an arterialvalve was a specific, but not invariable, feature ofoutlet defects. Subaortic' or subpulmonary6 stenosiswas also a feature ofsome hearts with deviation of theoutlet septum.
In the presence of an outlet defect, a coronalsection of the heart parallel to the trabecular septum,which passes through the inlet and outlet of the rightventricle, cuts through the aortic root. The aorticvalve sits astride the defect, giving the impressionthat it arises from the right ventricle (fig 6). Thisfeature does not depend on overriding of the aorticvalve, the extent of which is difficult to assess insections parallel to the trabecular septum. Wherethere is little or no override, however, a more anteriorsection will demonstrate the ventriculoinfundibularfold separating the ascending aorta from the right
'td:mgr
...:.4
AO 4
TVj K D v ;9 RV 'LJ. N, N .xr ,Xi.. . g8. _
Fig 6 (a) A simulated oblique subcostal cut through the right ventricle. The aortic valve (AoV) sits astride aventricular septal defect and appears to arisefrom the right ventricle. It is separatedfrom the pulmonary valveby a bar of muscle, the outlet septum (arrowed). There is continuity between the tricuspid (TV) and aorticvalves (asterisk). This is therefore a perimembranous defect opening between the ventricular outlets andoverridden by the aortic valve. (b) Similar appearances are seen in this defect viewed in an equivalentechocardiographic plane. RV, right ventricle; PT, pulmonary trunk.
..c
:i 16...:.. "I
.ft ;.:.:..;..-,----:
group.bmj.com on October 22, 2017 - Published by http://heart.bmj.com/Downloaded from
Cross sectional anatomy of ventricular septal defects
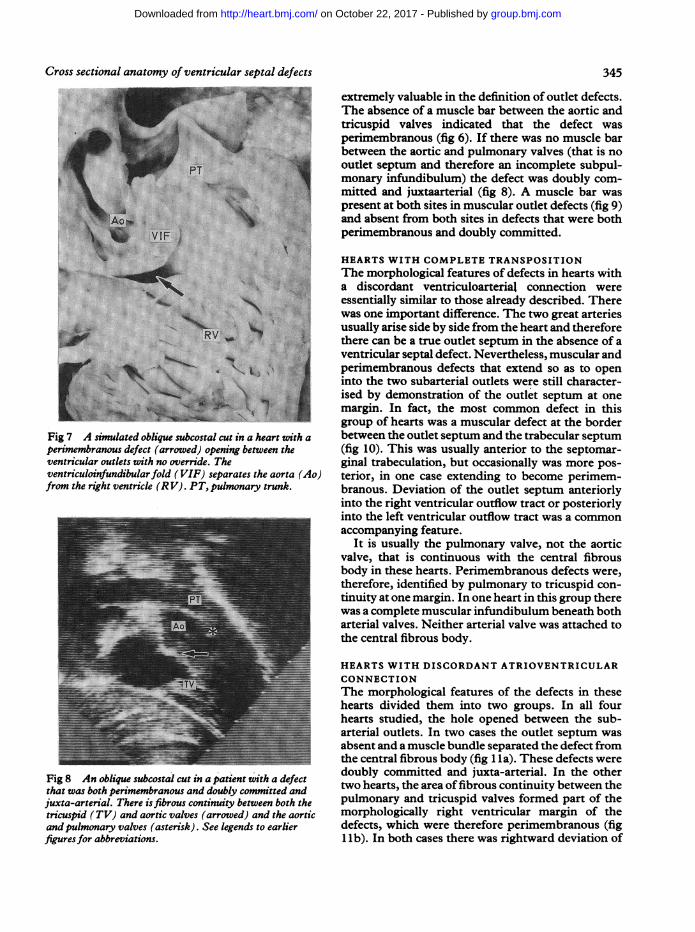
Fig 7 A simnulated oblique subcostal cut in a heart with a
perimembranous defect (arrowed) opening between theventricular outlets with no override. Theventriculoinfundibular fold (VIF) separates the aorta (Ao)from the right ventricle (RV). PT, pulmonary trunk.
Fig 8 An oblique subcostal cut in a patient with a defectthat was both perimembranous and doubly committed andjuxta-arterial. There isfibrous continuity between both thetricuspid (TV) and aortic valves (arrowed) and the aorticand pulmonary valves (asterisk). See legends to earlierfigures for abbreviations.
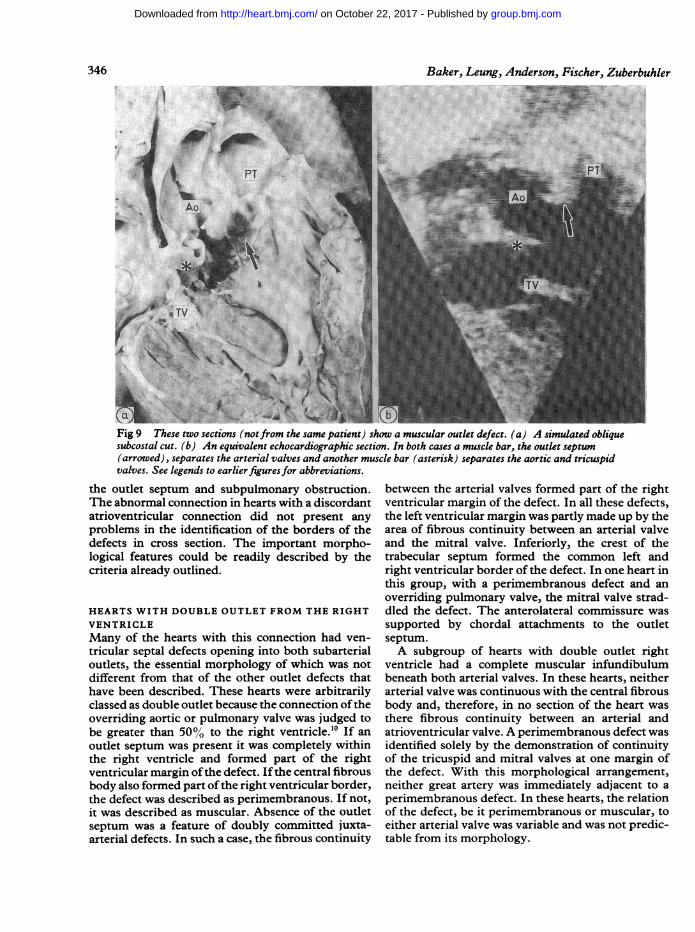
extremely valuable in the definition of outlet defects.The absence of a muscle bar between the aortic andtricuspid valves indicated that the defect wasperimembranous (fig 6). If there was no muscle barbetween the aortic and pulmonary valves (that is nooutlet septum and therefore an incomplete subpul-monary infundibulum) the defect was doubly com-mitted and juxtaarterial (fig 8). A muscle bar waspresent at both sites in muscular outlet defects (fig 9)and absent from both sites in defects that were bothperimembranous and doubly committed.
HEARTS WITH COMPLETE TRANSPOSITIONThe morphological features of defects in hearts witha discordant ventriculoarterial connection wereessentially similar to those already described. Therewas one important difference. The two great arteriesusually arise side by side from the heart and thereforethere can be a true outlet septum in the absence of aventricular septal defect. Nevertheless, muscular andperimembranous defects that extend so as to openinto the two subarterial outlets were still character-ised by demonstration of the outlet septum at onemargin. In fact, the most common defect in thisgroup of hearts was a muscular defect at the borderbetween the outlet septum and the trabecular septum(fig 10). This was usually anterior to the septomar-ginal trabeculation, but occasionally was more pos-terior, in one case extending to become perimem-branous. Deviation of the outlet septum anteriorlyinto the right ventricular outflow tract or posteriorlyinto the left ventricular outflow tract was a commonaccompanying feature.
It is usually the pulmonary valve, not the aorticvalve, that is continuous with the central fibrousbody in these hearts. Perimembranous defects were,therefore, identified by pulmonary to tricuspid con-tinuity at one margin. In one heart in this group therewas a complete muscular infundibulum beneath botharterial valves. Neither arterial valve was attached tothe central fibrous body.
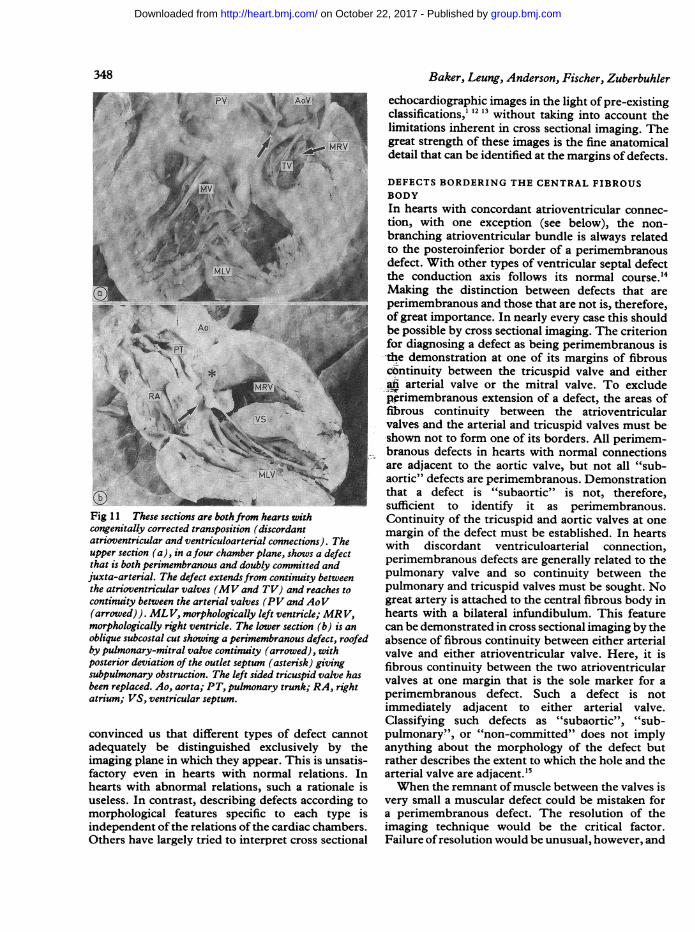
HEARTS WITH DISCORDANT ATRIOVENTRICULARCONNECTIONThe morphological features of the defects in thesehearts divided them into two groups. In all fourhearts studied, the hole opened between the sub-arterial outlets. In two cases the outlet septum wasabsent and a muscle bundle separated the defect fromthe central fibrous body (fig 1 la). These defects weredoubly committed and juxta-arterial. In the othertwo hearts, the area offibrous continuity between thepulmonary and tricuspid valves formed part of themorphologically right ventricular margin of thedefects, which were therefore perimembranous (fig1 Ib). In both cases there was rightward deviation of
345
group.bmj.com on October 22, 2017 - Published by http://heart.bmj.com/Downloaded from
~~~~~~~~~~~~~Baker,Leung, Anderson, Fischer, Zuberbuhler
Fig 9 These two sections (notfrom the same patient) show a muscular outlet defect. (a) A simulated obliquesubcostal cut. (b) An equivalent echocardiographic section. In both cases a muscle bar, the outlet septum(arrowed), separates the arterial valves and another muscle bar (asterisk) separates the aortic and tricuspidvalves. See legends to earlierfigures for abbreviations.
the outlet septum and subpulmonary obstruction.The abnormal connection in hearts with a discordantatrioventricular connection did not present anyproblems in the identification of the borders of thedefects in cross section. The important morpho-logical features could be readily described by thecriteria already outlined.
HEARTS WITH DOUBLE OUTLET FROM THE RIGHTVENTRICLEMany of the hearts with this connection had ven-tricular septal defects opening into both subarterialoutlets, the essential morphology of which was notdifferent from that of the other outlet defects thathave been described. These hearts were arbitrarilyclassed as double outlet because the connection oftheoverriding aortic or pulmonary valve was judged tobe greater than 50% to the right ventricle.10 If anoutlet septum was present it was completely withinthe right ventricle and formed part of the rightventricular margin ofthe defect. Ifthe central fibrousbody also formed part ofthe right ventricular border,the defect was described as perimembranous. If not,it was described as muscular. Absence of the outletseptum was a feature of doubly committed juxta-arterial defects. In such a case, the fibrous continuity
between the arterial valves formed part of the rightventricular margin of the defect. In all these defects,the left ventricular margin was partly made up by thearea of fibrous continuity between an arterial valveand the mitral valve. Inferiorly, the crest of thetrabecular septum formed the common left andright ventricular border of the defect. In one heart inthis group, with a perimembranous defect and anoverriding pulmonary valve, the mitral valve strad-dled the defect. The anterolateral commissure wassupported by chordal attachments to the outletseptum.A subgroup of hearts with double outlet right
ventricle had a complete muscular infundibulumbeneath both arterial valves. In these hearts, neitherarterial valve was continuous with the central fibrousbody and, therefore, in no section of the heart wasthere fibrous continuity between an arterial andatrioventricular valve. A perimembranous defect wasidentified solely by the demonstration of continuityof the tricuspid and mitral valves at one margin ofthe defect. With this morphological arrangement,neither great artery was immediately adjacent to aperimembranous defect. In these hearts, the relationof the defect, be it perimembranous or muscular, toeither arterial valve was variable and was not predic-table from its morphology.
346
Y'
biE.-a:i .:.,
I1
group.bmj.com on October 22, 2017 - Published by http://heart.bmj.com/Downloaded from
Cross sectional anatomy of ventricular septal defects_8 1:: :20::; Y : . . .-w-1|: .. .s *
*: :: ': f:.:. .:.::
siE j * A: ..
.R.: _@w H_t*,=; E j ) x Y s.
o'*i! ts'sCiA } } }.
'!V / 2: ,. .e.'S.X°:w: : .of. X^
:: _.|, _:.
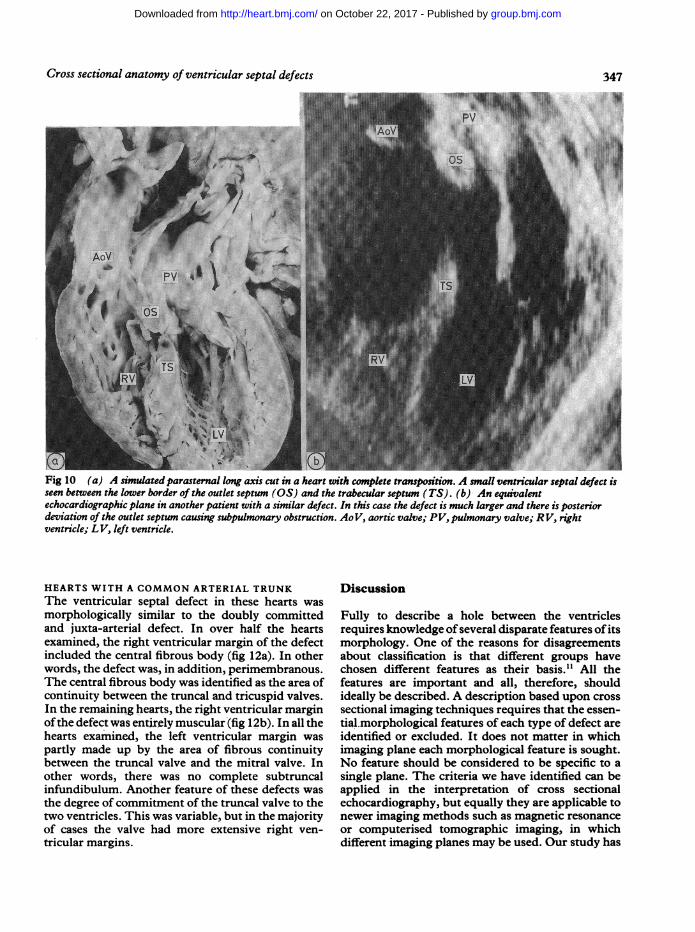
PV. 4.* \ .. .. ffi ffi... s_..... ___Fig 10 (a) A simulatedparasternal long axis cut in a heart with complete transposition. A small ventricular septal defect isseen between the lower border of the outlet septum (OS) and the trabecular septum (TS). (b) An equivalentechocardiographic plane in another patient with a similar defect. In this case the defect is much larger and there is posteriordeviation of the outlet septum causing subpulmonary obstruction. AoV, aortic valve; PV, pulmonary valve; RV, rightventricle; LV, left ventricle.
HEARTS WITH A COMMON ARTERIAL TRUNKThe ventricular septal defect in these hearts was
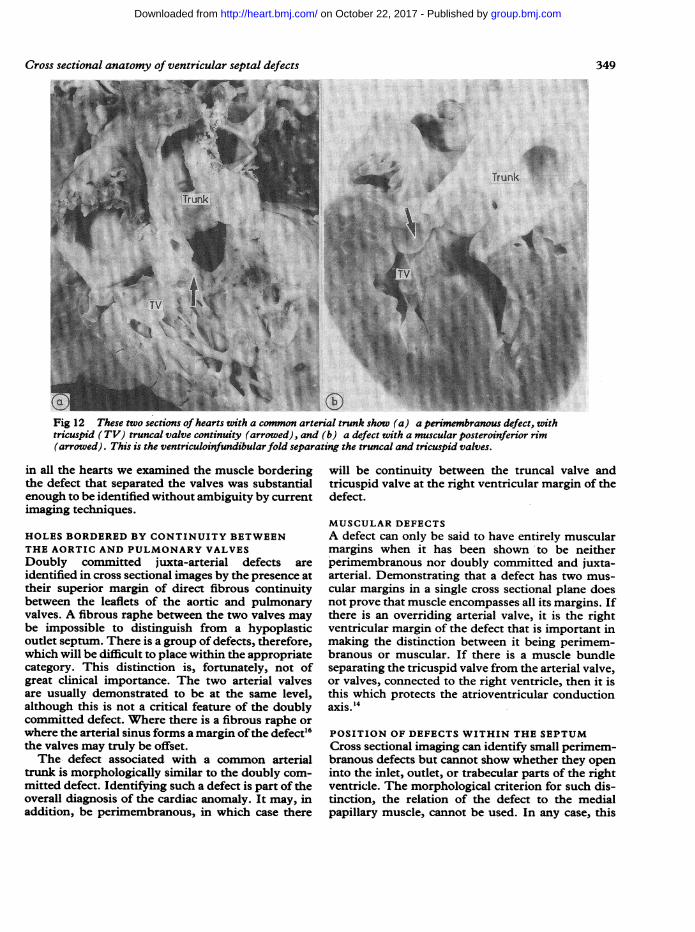
morphologically similar to the doubly committedand juxta-arterial defect. In over half the heartsexamined, the right ventricular margin of the defectincluded the central fibrous body (fig 12a). In otherwords, the defect was, in addition, perimembranous.The central fibrous body was identified as the area ofcontinuity between the truncal and tricuspid valves.In the remaining hearts, the right ventricular marginofthe defect was entirely muscular (fig 12b). In all thehearts examined, the left ventricular margin waspartly made up by the area of fibrous continuitybetween the truncal valve and the mitral valve. Inother words, there was no complete subtruncalinfundibulum. Another feature of these defects was
the degree of commitment of the truncal valve to thetwo ventricles. This was variable, but in the majorityof cases the valve had more extensive right ven-tricular margins.
Discussion
Fully to describe a hole between the ventriclesrequires knowledge ofseveral disparate features of itsmorphology. One of the reasons for disagreementsabout classification is that different groups havechosen different features as their basis.1' All thefeatures are important and all, therefore, shouldideally be described. A description based upon crosssectional imaging techniques requires that the essen-tial.morphological features of each type of defect areidentified or excluded. It does not matter in whichimaging plane each morphological feature is sought.No feature should be considered to be specific to asingle plane. The criteria we have identified can beapplied in the interpretation of cross sectionalechocardiography, but equally they are applicable tonewer imaging methods such as magnetic resonanceor computerised tomographic imaging, in whichdifferent imaging planes may be used. Our study has
347
group.bmj.com on October 22, 2017 - Published by http://heart.bmj.com/Downloaded from
348
' MLLV
Fig 11 These sections are bothfrom hearts withcongenitally corrected transposition (discordantatrioventricular and ventriculoarterial connections). Theupper section (a), in afour chamber plane, shows a defectthat is both perimembranous and doubly committed andjuxta-arterial. The defect extendsfrom continuity betweenthe atrioventricular valves (MV and TV) and reaches tocontinuity between the arterial valves (PV and AoV(arrowed)). ML V, morphologically left ventricle; MRV,morphologically right ventricle. The lower section (b) is anoblique subcostal cut showing a perimembranous defect, roofedby pulmonary-mitral valve continuity (arrowed), withposterior deviation of the outlet septum (asterisk) givingsubpulmonary obstruction. The left sided tricuspid valve hasbeen replaced. Ao, aorta; PT, pulmonary trunk; RA, rightatrium; VS, ventricular septum.
convinced us that different types of defect cannotadequately be distinguished exclusively by theimaging plane in which they appear. This is unsatis-factory even in hearts with normal relations. Inhearts with abnormal relations, such a rationale isuseless. In contrast, describing defects according tomorphological features specific to each type isindependent of the relations ofthe cardiac chambers.Others have largely tried to interpret cross sectional
Baker, Leung, Anderson, Fischer, Zuberbuhler
echocardiographic images in the light of pre-existingclassifications,''213 without taking into account thelimitations inherent in cross sectional imaging. Thegreat strength of these images is the fine anatomicaldetail that can be identified at the margins of defects.
DEFECTS BORDERING THE CENTRAL FIBROUSBODYIn hearts with concordant atrioventricular connec-tion, with one exception (see below), the non-branching atrioventricular bundle is always relatedto the posteroinferior border of a perimembranousdefect. With other types of ventricular septal defectthe conduction axis follows its normal course.'4Making the distinction between defects that areperimembranous and those that are not is, therefore,of great importance. In nearly every case this shouldbe possible by cross sectional imaging. The criterionfor diagnosing a defect as being perimembranous isthe demonstration at one of its margins of fibrouscontinuity between the tricuspid valve and eitherati arterial valve or the mitral valve. To excludepprimembranous extension of a defect, the areas offibrous continuity between the atrioventricularvalves and the arterial and tricuspid valves must beshown not to form one of its borders. All perimem-branous defects in hearts with normal connectionsare adjacent to the aortic valve, but not all "sub-aortic" defects are perimembranous. Demonstrationthat a defect is "subaortic" is not, therefore,sufficient to identify it as perimembranous.Continuity of the tricuspid and aortic valves at onemargin of the defect must be established. In heartswith discordant ventriculoarterial connection,perimembranous defects are generally related to thepulmonary valve and so continuity between thepulmonary and tricuspid valves must be sought. Nogreat artery is attached to the central fibrous body inhearts with a bilateral infundibulum. This featurecan be demonstrated in cross sectional imaging by theabsence of fibrous continuity between either arterialvalve and either atrioventricular valve. Here, it isfibrous continuity between the two atrioventricularvalves at one margin that is the sole marker for aperimembranous defect. Such a defect is notimmediately adjacent to either arterial valve.Classifying such defects as "subaortic", "sub-pulmonary", or "non-committed" does not implyanything about the morphology of the defect butrather describes the extent to which the hole and thearterial valve are adjacent.'5When the remnant ofmuscle between the valves is
very small a muscular defect could be mistaken fora perimembranous defect. The resolution of theimaging technique would be the critical factor.Failure ofresolution would be unusual, however, and
group.bmj.com on October 22, 2017 - Published by http://heart.bmj.com/Downloaded from
Cross sectional anatomy of ventricular septal defects
Fig 12 These two sections of hearts with a common arterial trunk show (a) a perimembranous defect, withtricuspid (TV) truncal valve continuity (arrowed), and (b) a defect with a muscular posteroinferzor rim(arrowed). This is the ventriculoinfundibular fold separating the truncal and tricuspid valves.
in all the hearts we examined the muscle borderingthe defect that separated the valves was substantialenough to be identified without ambiguity by currentimaging techniques.
HOLES BORDERED BY CONTINUITY BETWEENTHE AORTIC AND PULMONARY VALVESDoubly committed juxta-arterial defects areidentified in cross sectional images by the presence attheir superior margin of direct fibrous continuitybetween the leaflets of the aortic and pulmonaryvalves. A fibrous raphe between the two valves maybe impossible to distinguish from a hypoplasticoutlet septum. There is a group of defects, therefore,which will be difficult to place within the appropriatecategory. This distinction is, fortunately, not ofgreat clinical importance. The two arterial valvesare usually demonstrated to be at the same level,although this is not a critical feature of the doublycommitted defect. Where there is a fibrous raphe orwhere the arterial sinus forms a margin ofthe defect"6the valves may truly be offset.The defect associated with a common arterial
trunk is morphologically similar to the doubly com-mitted defect. Identifying such a defect is part of theoverall diagnosis of the cardiac anomaly. It may, inaddition, be perimembranous, in which case there
will be continuity between the truncal valve andtricuspid valve at the right ventricular margin of thedefect.
MUSCULAR DEFECTSA defect can only be said to have entirely muscularmargins when it has been shown to be neitherperimembranous nor doubly committed and juxta-arterial. Demonstrating that a defect has two mus-cular margins in a single cross sectional plane doesnot prove that muscle encompasses all its margins. Ifthere is an overriding arterial valve, it is the rightventricular margin of the defect that is important inmaking the distinction between it being perimem-branous or muscular. If there is a muscle bundleseparating the tricuspid valve from the arterial valve,or valves, connected to the right ventricle, then it isthis which protects the atrioventricular conductionaxis."
POSITION OF DEFECTS WITHIN THE SEPTUMCross sectional imaging can identify small perimem-branous defects but cannot show whether they openinto the inlet, outlet, or trabecular parts of the rightventricle. The morphological criterion for such dis-tinction, the relation of the defect to the medialpapillary muscle, cannot be used. In any case, this
349
group.bmj.com on October 22, 2017 - Published by http://heart.bmj.com/Downloaded from
350
differentiation is of little value. None the less,attachments of the leaflets of the tricuspid valvearound the defect indicate extension into thetrabecular or inlets zones. This is not a feature ofdefects that extend to open solely between the sub-arterial outles& The term "perimembranous inletdefect" is best reserved for those large defects thatextend to the crux of the heart and open between theinlets ofboth ventricles. These defects, roofed by themitral and tricuspid valves in fibrous continuity, canreadily be displayed by cross sectional imaging (fig7).
Extension ofperimembranous or muscular defectsinto the outlets can be demonstrated by the iden-tification, at one margin, ofan outlet septum, definedas a bar of muscle separating the space beneath thetwo arterial valves. As we have seen, demonstratingthat the defect is adjacent to the aortic valve does not,in itself, indicate outlet extension. This is a featureof all perimembranous defects. In hearts withdiscordant ventriculoarterial connection, defects are
commonly found at the lower border of the outletseptum. Distinguishing these from defects moreapically placed in the trabecular septum requires an
arbitrary judgement because there is no marker forthe level of the junction of the outlet and trabecularseptum.
Morphologically, perimembranous defects thatextend into both the inlet and outlet parts ofthe rightventricle can be termed "confluent". Cross sectionalimaging permits the identification of a very largedefect that extends both to the crux and into thesubarterial outlets. But a confluent defect that doesnot extend to the crux cannot be distinguished from a
perimembranous outlet defect.Muscular defects that do not open into the outlets
may be identified as opening between the ventricularinlets if they are seen in the septum immediatelybeneath both atrioventricular valves and are
separated from them by a bar of muscle. Othermuscular defects can be described as trabecular.These defects can be further characterised by thedistance they are from the apex in long axis sections.They can be multiple and have a tortuous course andhence, if small, may be difficult to detect in cross
sectional images. 217
OVERRIDING OF THE GREAT ARTERIES
There is a fundamental anomaly in septation inhearts with defects opening into both ventricularoutlets. Overriding of a great artery is an importantfeature of some of these defects. The anomaly inthese hearts should not be thought of as a simple holein the ventricular septum. The leaflets ofthe overrid-ing arterial valve form the roof of a conical space, thefloor of which is the crest of the trabecular septum.
Baker, Leung, Anderson, Fischer, Zuberbuhler
This space has both right and left ventricular mar-gins. The right ventricular margin corresponds to thedefect in similar hearts without an overriding arterialvalve. The left ventricular margin is commonlycalled the "defect" in hearts with double outlet oftheright ventricle.10 In these hearts, -tbe ventricularseptal defect should be considered as a three dimen-sional structure. All borders of the defect need to bedescribed." Only cross sectional imaging permitsthis.
Overriding of either great arterial valve is arelatively common feature of all defects openingbetween both ventricular outlets, be they perimem-branous, muscular, or doubly committed and juxta-arterial. When present, it is a marker for outletextension of a defect. The morphology of thesedefects is excellently demonstrated in coronal sec-tions through the right ventricle,'8 but in suchsections the extent ofthe override cannot be assessed.This is best done using long axis sections ofthe heart.Override of both great arteries can occur in thepresence of a doubly committed defect.'9
RELATION OF DEFECTS TO ARTERIAL VALVESThe terms "subaortic" and "subpulmonary" havebeen used to describe different aspects of the spatialrelations between defects and the arterial valves. Ifthis relation is described precisely, rather than clas-sifying it in this way, ambiguity can be avoided.Hence, one type of "subaortic" defect can be des-cribed as a perimembranous defect immediatelyadjacent to the aortic valve,2 while another "sub-aortic" defect could be described as opening betweenthe subarterial outlets with overriding of the aorticvalve.'5 In the context of double outlet from the rightventricle with bilateral infundibulum, the relationbetween the defect and the arterial valves cannot bepredicted from the morphology of the defect. Theclassifications of "subaortic" and "subpulmonary"can be used to describe, in this context, a judgementby the observer about the feasibility of surgicallyconnecting the defect to either arterial valve.'0 A fulldescription of the relation of the defect to the arterialvalves, however, is likely to be of more value than anarbitrary classification.
STRADDLING AND OVERRIDING OF THEATRIOVENTRICULAR VALVESStraddling and overriding of the mitral valve is also afeature of some outlet defects. Usually it is seenwhere there is a discordant ventriculoarterial connec-tion or, as in this series, double outlet right ventriclewith an overriding pulmonary valve, the so-calledTaussig-Bing heart." 2" Straddling and overriding ofthe tricuspid valve is a feature of a particularperimembranous inlet defect. It is associated with
group.bmj.com on October 22, 2017 - Published by http://heart.bmj.com/Downloaded from
Cross sectional anatomy of ventricular septal defects 351
considerable malalignment of the atrial septumrelative to the muscular ventricular septum, which nolonger extends to the crux. Identification of thisdefect is straightforward because of the septalmalalignment. These defects are the only exceptionto the rule that, in hearts with concordant atrioven-tricular connection, the conduction axis is alwaysposterioinferior to perimembranous defects.'Recognition of this anatomy is essential.CONCLUSIONThere is no need for a further classification ofventricular septal defects on morphological criteriaand we have not attempted to produce one. Authorsof the various existing classifications have chosen toemphasise different morphological features of thedefects they studied, and they have, therefore,arrived at seemingly contradictory conclusions. Wehave not made a judgement that any one aspect ofthe morphology of ventricular septal defects isfundamental to their description. Ideally, all themorphological features need to be identified anddescribed. We believe that, using the criteria we havedescribed, it is possible virtually to achieve this aim.If, in this way, the morphology of a defect iscompletely described, its place in any of the diverseschemes of classification should be readily apparent.An additional problem is that some of the terms thathave been used to describe the morphologicalfeatures of ventricular septal defects are ambiguous,having been used by different workers to describedifferent features. To be ofvalue descriptions need tobe precise and so we have used terminology whichdescribes the morphology of defects exactly and havediscarded ambiguous terms. The great strength ofcross sectional imaging is that it defines mor-phological detail at the margins of defects exception-ally well and, so, it is without equal in the clinicalstudy of ventricular septal defects.This work was performed when RHA was on asabbatical from the Cardiothoracic Institute,Brompton Hospital, London SW3 6HP. It wassupported by a grant from the Patrick Dick MemorialFund.
References1 Sutherland GR, Godman MJ, Smallhorn JF, Guiterras
P, Anderson RI-, Hunter S. Ventricular septaldefects. Two dimensional echocardiographic andmorphological correlations. Br Heart J 1982;47:316-28.
2 Capelli H, Andrade JL, Somerville J. Classification ofthe site of ventricular septal defect by 2-dimensionalechocardiography. Am J Cardiol 1983;51:1474-80.
3 Piot JD, Lucet P, Losay J, et al. Diagnosis andlocalisation of ventricular septal defects by twodimensional echocardiography. Arch Mal Coeur1981;74:1001-9.
4 Anderson RH, Lenox CC, Zuberbuhler JR.Mechanisms of closure of perimembranousventricular septal defects. Am J Cardiol 1983;52:341-5.
5 Anderson RH, Lenox CC, Zuberbuhler JR.Morphology of ventricular septal defect associatedwith coarctation ofthe aorta. Br Heart J 1983;50: 176-81.
6 Anderson RH, Allwork SP, Ho SY, Lenox CC,Zuberbuhler JR. Surgical anatomy of the tetralogy ofFallot. J Thorac Cardiovasc Surg 1981;81:887-96.
7 Soto B, Becker AE, Moulaert AJ, Lie JT, AndersonRH. Classification of ventricular septal defects. BrHeart J 1980;43:332-43.
8 Capelli H, Somerville J. Atypical Fallot's tetralogy withdoubly committed sub-arterial defect. Diagnosticvalue of 2-dimensional echocardiography. Am JCardiol 1983;51:282-5.
9 Silverman NH, Hunter S, Anderson RH, Ho SY,Sutherland GR, Davies MJ. Anatomical basis ofcrosssectional echocardiography. Br Heart J 1983;50:421-31.
10 Macartney FJ, Rigby ML, Anderson RH, Stark J,Silverman NH. Double outlet right ventricle. Crosssectional echocardiographic findings, theiranatomical explanation, and surgical relevance. BrHeart J 1984;52:164-77.
11 Anderson RH, Becker AE, Tynan M. Description ofventricular septal defects-or how long is a piece ofstring? Int J Cardiol 1986;13:267-78.
12 Bierman FZ, Fellows K, Williams RG. Prospectiveidentification of ventricular septal defects in infancyusing subxiphoid two-dimensional echocardio-graphy. Circulation 1980;62:807-17.
13 Hagler DJ, Edwards WD, Seward JB, Tajik AJ. Stan-dardized nomenclature of the ventricular septum andventricular septal defects, with applications for two-dimensional echocardiography. Mayo Clin Proc1985;60:741-52.
14 Milo S, Ho SY, Wilkinson JL, Anderson RH. Surgicalanatomy and atrioventricular conduction tissues ofhearts with isolated ventricular septal defects. JThorac Cardiovasc Surg 1980;79:244-55.
15 Lev M, Bharati S, Memg CCL, Liberthson RR, PaulMH, Idriss F. A concept of double outlet rightventricle. J Thorac Cardiovasc Surg 1972;64:271-81.
16 Ando M, Takao A. Pathological anatomy of ventricularseptal defect associated with aortic valve prolapse andregurgitation. Heart and Vessels 1986;2:117-26.
17 Cheatham JP, Latson LA, Gutgesell HP. Ventricularseptal defect in infancy: detection with two-dimen-sional echocardiography. Am J Cardiol 1981;47:85-9.
18 Magherini A, Margiotta C, Simonetti L, et al. Cross-sectional echocardiography with pulsed and contin-uous wave Doppler in management of ventricularseptal defects. Int J Cardiol 1987;15:317-28.
19 Ueda M, Becker AE. Double outlet right ventricle: anunusual variant with overriding ofboth great arteries,absent outlet septum and mitral-to-aortic-to-pul-monary continuity. Int J Cardiol 1986;12:155-60.
20 Milo S, Ho SY, Macartney FJ, et al. Straddling andoverriding atrioventricular valves; morphology andclassification. Am J Cardiol 1979;44:1122-34.
group.bmj.com on October 22, 2017 - Published by http://heart.bmj.com/Downloaded from
reappraisal.ventricular septal defects: a The cross sectional anatomy of
R ZuberbuhlerE J Baker, M P Leung, R H Anderson, D R Fischer and J
doi: 10.1136/hrt.59.3.3391988 59: 339-351 Br Heart J
http://heart.bmj.com/content/59/3/339Updated information and services can be found at:
These include:
serviceEmail alerting
online article. article. Sign up in the box at the top right corner of the Receive free email alerts when new articles cite this
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on October 22, 2017 - Published by http://heart.bmj.com/Downloaded from