crucible - cyclomedica · this crucible concentrates on revisiting the recommended procedure for...
TRANSCRIPT

providing contra-argument for the oft quoted statement that ‘CT gives more information’.The purpose of this article is to outline Cyclomedica’s recommended proto-col, as defined in the Technegas User Manual, for generating and delivering Technegas; consistently, reproducibly and optimally.
INITIAL STEPS
Follow the usual steps in preparing the Technegas generator (TG) or Techne-gasPlus generator (TP) to generate Technegas:1) Argon bottle ‘On’.2) Regulator ‘Open’ to the recom-mended Argon flow rate.3) Turn Main Power switch on. Green light indicates that the power is on. Once power is on leave on the rest of the day. This keeps the battery at optimal charge.4) Turn off power at night and week-ends.5) Regulator off Regulator
6) Turn off Argon Bottle.When inserting the carbon crucible ALWAYS wet with 95% ethanol.The reason for this is that when Tech-netium is simmered TG at 70 degrees Celsius in a dry crucible, air bubbles can form which blows Technetium out of the crucible and lowers the yield of Technegas.
95% ethnaol is also needed so that no impurities which could potentially be breathed by patient are introduced.
The Alcohol is NOT used to sterilise the carbon crucible.So, wet the carbon crucible, discard the alcohol leaving a moist crucible to inject the Technetium into and imme-diately insert the crucible between the contacts with the forceps provided.
Seat the crucible by rocking back-wards and forwards in the contacts until a squeaking sound is heard. This ensures good electrical contact and a good Technegas yield.
Remember to follow the prompts of the TG and change the contacts every 50 burns. Failure to do so will result in continued - page 2/
n travelling around Australasia over the past few years it has be-come apparent that there seem to be as many variations for how
Technegas is generated and delivered to patients as there are sites that use it. We therefore thought it opportune that Cyclomedica revisits the ‘recom-mended’ Technegas generation and delivery protocol as this method has proven optimal over many years. This ‘recommended’ protocol is fully de-fined in the Technegas User Manual.First of all, Cyclomedica recommends that V/Q SPECT imaging should be performed in all cases of suspected Pulmonary Embolism (PE).
There are many reasons for this:1) V/Q SPECT allows a binary response in all but a very few instances. Re-ferring physicians want a yes or no answer to their question not a proba-bilistic ‘non-response’.2) Sensitivity and Negative Predictive Value, are higher than CT and Specific-ity, Accuracy are AT LEAST the equiva-lent of CT and vastly superior to Planar3) V/Q SPECT with Technegas allows other respiratory co-morbidities to be identified (C.O.P.D., pneumonia, left heart failure, tumour, asthma, etc.)
CRUCIBLETHE
VOL 6 / NO. 3 - AUGUST 2013CYCLOMEDICA NUCLEAR MEDICINE
IN THIS ISSUE
Recommended Technegas Delivery Protocol 1-4
Comment 4
Spectlung / Reporting / Tech Tips Reference Material 5
Technegas Generator - FDG / Posijet 6
Recommended Technegas Delivery Protocol
I
Procedures

/2 poor contact with the carbon crucible, poor Technegas yield and in some instances an error message: ‘failure to reach burn temperature’.
You should now be ready to load the crucible with Technetium-99m. If you notice that the crucible has dried before you get the chance to administer the Technetium, repeat the process: wet, seat, Technetium.
GENERATION OF TECHNEGAS
Using a 1 ml syringe inject the activity into the crucible by resting the needle in the crucible well and filling to level. Once withdrawn the activity level should be concave. (If too much ac-tivity is injected i.e. convex shape, the Argon flow used during the simmer will blow activity out of the crucible thereby diminishing Technegas yield.
Within a few breaths, two to three in most instances, enough Technegas
should be administered to the patient to achieve the recommended count rate of 2,500 cps in the lung required to perform the Ventilation study. This equates to approximately 1mCi of Technetium activity in the lung.
It is important that high specific activ-ity Technetium is used (approximately 5 GBq/ml or 140 mCi/ml). The aim is to burn about 750 MBq or 20 mCi in the carbon crucible which has a volume of only 0.14ml. (Note that the recom-mended loading for the crucible is be-tweeen 400 and 900 MBq.) Following the prompts on the screen, Push Start to initiate the Burn cycle.
If the specific activity is too low, multi-ple simmers must be performed. This is achieved by:1) Loading the crucible with activity available.2) Simmering for 3 minutes.3) Interrupting the 6 minute cycle by ‘double push’ on the CANCEL button.4) Topping up the crucible with more activity.5) Starting the simmer cycle once more.
6) Repeating until such time as 750 MBq (20mCi) has been loaded onto the crucible. 7) Follow the prompts on the screen to initiate the burn cycle.
When the Technegas is ready to be administered to the patient, Turn off the Power and unplug (as prompted), Turn off Regulator and disconnect the Argon hose from the back of the machine.
Under normal circumstances when the crucible is loaded with sufficient activity, the simmer process should take only six minutes. After the burn cycle the Technegas is ready to be delivered to the patient.
During this 6 minute simmer cycle, time the patient can be instructed on the appropriate breathing technique:
1) Open the PAS in front of the patient.2) Discuss the best option of mouth piece or mask to ensure that the pa-tient does not breathe into the room.3) Nose clip on.4) Practice with the patient.5) Deep breath.6) Hold (count one, two, three).7) Exhale.8) Repeat 2 or 3 times.
CALIBRATING THE COUNT RATE
It is recommended that Technegas NOT be administered to the patient in the camera room. Despite the best efforts of technologists and patient cooperation, some Technegas may escape into the atmosphere and be drawn into the gamma camera heads.
The following is recommended:1) In the supine position, administer Technegas for 2 or 3 breaths in a room other than the scanning room.continued - page 3/
‘failure to reach burn temperature’.
/3(measure the activity over the chest toensure that about 30 MBq reached the lungs.)2) Take the patient to the gamma camera.3) Elevate the bottom head of a dou-ble headed gamma camera as close to the patient’s back as possible.4) Measure the count rate. Remem-ber we are looking for approximately 2000- 2,500 cps (in the inhaling room preferably).5) If the count rate is too low, take the patient back to the Technegas generator and administer 2 to 3 more breaths.6) Continue until the recommended count rate is achieved .7) Next. Measure the count rate emanating from the patient’s lungs using a gamma probe/ survey meter or similar to calibrate the reading from the Gamma camera.8) Mark this number on the probe.9) In future use the figure on the probe to estimate the count rate ex-pected on the gamma camera.10) This saves time and potential con-tamination of the scanning room.11) Insert an i.v. cannula in prepara-tion for the administration of Tc-MAA to prevent any patient movement.
DELIVERING THE TECHNEGAS
For best results, be ready to adminis-ter the Technegas immediately after generation.
Always remember that once the Technegas has been generated there is only 10 minutes available to deliver to the patient and the sooner after its generation, the more activity there is available in the 6 litre chamber.Once in the patient, the Ventilation scan may be performed when the gamma camera is available. Tech-netium has a half-life of 6 hours and Technegas remains adhered to the alveoli of the lung thereby giving the department flexibility in the timing of when the study can be performed. Following is the recommended proce-dure for delivering Technegas to the patient:
1) Turn off the power to the Techne-gas generator.2) Regulator off.3) Disconnect the gas hose from the back of the generator.4) Take the Technegas generator to
the patient (now operating on the battery).5) Once the PAS is connected to the patient and the Technegas generator push the Start button (as prompted) to release the Technegas.6) In the prone position, instruct the patient to exhale.7) Upon commencement of the next breath, hold down the delivery knob AND KEEP IT DOWN.8) EVERY INHALATION WILL DELIVER TECHNEGAS (while the delivery knob is down). If the technologist tries to synchronise every inspiration with a push down of the delivery knob and gets it wrong, ONLY AIR WILL BE DELIVERED. 9) Instruct the patient to take 2 to 3 breaths.
10) Ensure count rate is approximate-ly 2,500 cps as described previously.11) Remove hand from the delivery knob BUT instruct the patient to take 2 to 3 more breaths. This clears the tubing and traps all radioactivity in the filter inside the PAS.12) Dispose of the PAS in the ap-proved manner.13) NEVER REUSE. After the Tech-negas delivery procedure, the PAS is radioactive and the filter may also be contaminated by unrecognised respi-ratory infections carried by the patient (hazardous and radioactive).
NEXT STEPS
The patient is now ready for the Venti-
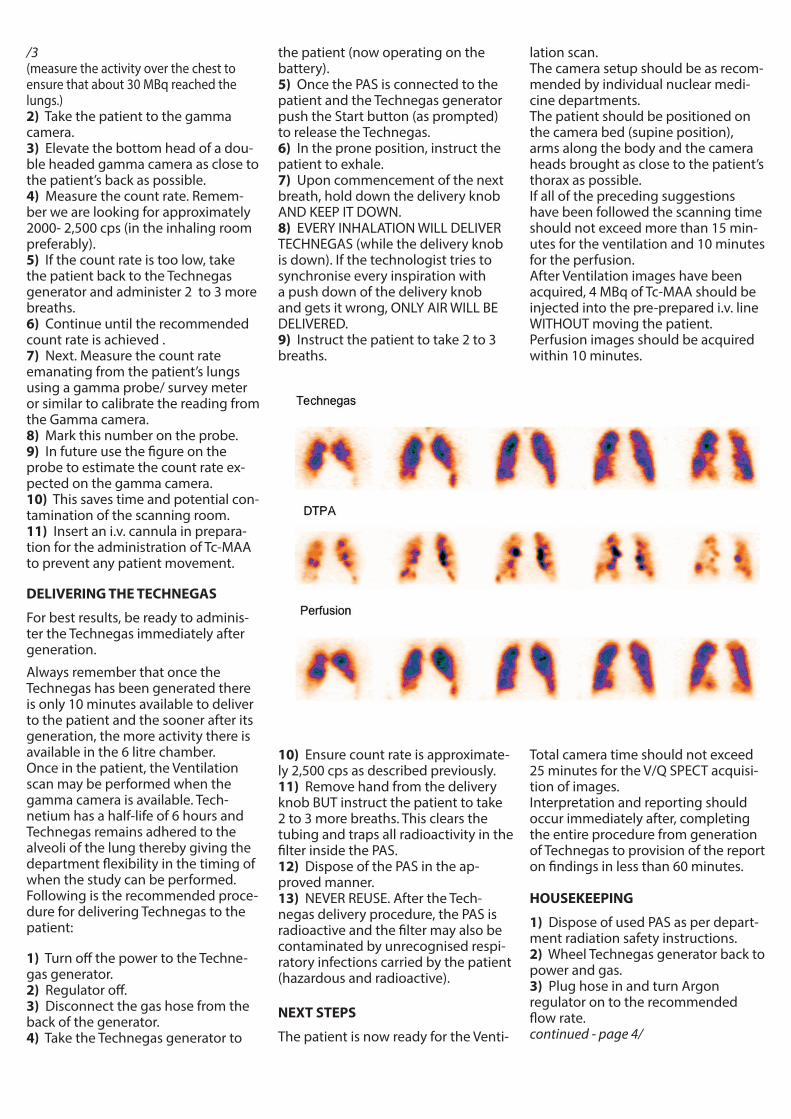
lation scan.The camera setup should be as recom-mended by individual nuclear medi-cine departments.The patient should be positioned on the camera bed (supine position), arms along the body and the camera heads brought as close to the patient’s thorax as possible.If all of the preceding suggestions have been followed the scanning time should not exceed more than 15 min-utes for the ventilation and 10 minutes for the perfusion.After Ventilation images have been acquired, 4 MBq of Tc-MAA should be injected into the pre-prepared i.v. line WITHOUT moving the patient.Perfusion images should be acquired within 10 minutes.
Total camera time should not exceed 25 minutes for the V/Q SPECT acquisi-tion of images.Interpretation and reporting should occur immediately after, completing the entire procedure from generation of Technegas to provision of the report on findings in less than 60 minutes.
HOUSEKEEPING
1) Dispose of used PAS as per depart-ment radiation safety instructions.2) Wheel Technegas generator back to power and gas.3) Plug hose in and turn Argon regulator on to the recommended flow rate.continued - page 4/
This Crucible concentrates on revisiting the recommended procedure for generating and delivering Technegas. These recommendations have withstood the test of time and been demonstrated to result in optimal Technegas yields and the most patient friendly delivery method. We at Cyclomedica understand that, over time, variations in the protocols people employ may evolve but we highly recommend that you adhere to these suggestions as strictly as possible to min-imize the potential for failures and suboptimal results to creep into your practice.
The method suggested is a step by step approach designed to guide experienced and novice alike and to ensure consistency and repro-ducibility. No suggestions are given for optimal camera set-up as each department seems to have a defined protocol of its own.
I have been under-whelmed by the response to reproduce clinical images and reporting of interesting respiratory disease cases for our lung atlas. There must be many cases of unusual or rare Technegas findings in people’s data files which could be used to enhance aware-ness of the variety of lung diseases observed by clinicians. If you pos-sess these cases how about tasking a technologist to put the informa-tion together and submitting it to us? We’ll pay them $150.00 for their trouble if we decide to feature it in subsequent Crucibles.
I must also reiterate previous comment regarding ‘ancient’ Technegas generators. Trade them in while they are still functioning and receive a trade-in for a TechnegasPlus generator. Parts for the old machines are difficult and expensive to source and much of the electronics are obsolete. We have plenty of new TechnegasPlus Generators in stock and can readily replace your old generator with a brand new one.
As you are aware we have a division called Cyclopet at Macquarie University Hospital which supplies FDG. Please consider acquiring some of your FDG from Cyclopet. We have plenty of excess capacity and are very flexible on delivery times. Supporting us with the FDG will allow us to more readily bring other desirable fluorinated com-pounds to you. We also market the Lemer-Pax mobile FDG injecting system. Discuss a package deal with us.
I hope you enjoy reading this edition and welcome feedback.
COMMENT
CharlesCharles ButtigiegAsia-Pacific Marketing & Sales MgrCyclomedica
/44) Plug in and Turn power on.5) Machine will go into a cleaning cycle, 3 minutes or 6 minutes depend-ing on local requirements.6) The cleaning cycle will be displayed on the screen.7) Leave the Technegas generator onduring the day.8) Before the first use next day re-move broken crucible and store for decay accordingly.
SUMMARY
There are several critical elements involved in this process:
1) Technologists must standardise the manner in which Technegas is produced in order to generate the best images for physicians toreport.
2) Appropriate interpretive soft-ware must be available if images are to be reconstructed optimally.
3) Physicians need to develop the skills required to take advantage and make full use of the tools available to them.
We at Cyclomedica can assist with the first of these elements. Devel-oping expertise and confidence with elements 2 and 3 will lead to improved reporting accuracy in Pulmonary Embolism and safer patient outcomes as well as an expansion of the respiratory conditions Technegas, when used in SPECT mode, is capable of identifying.
Medical Information and Adverse Reaction ReportingCyclomedica provide distributor and customer support with medical information queries on the products.Customers are advised to initially contact their local distributor, or they may contact Cyclomedica Austra-lia direct using the contact details below.If you wish to report an adverse reaction to the product this can be done using the same contacts details. Telephone +61 (0)2 9541 0411Facsimile +61 (0)2 9543 0960 orEmail: [email protected]
Have you visited -
www.spectlung.com
The information source for all aspects of lung imaging including Case Study examples of PE detection, Literature, Imaging Issues, Diagnostic Options, GP Info and Links to other sites.
TECH TIPSKeeping your TechnegasPlus Generator running smoothly.
1) Customers should periodically check the condition of the wheels on the Technegas trolleys. In some instances lint and dirt has been seen to accumulate in this area and if not addressed could potentially result in damage to the wheel mechanism. Could you please inform the Service Department if you note any discrepancies in this area?
2) Argon Gas Bottles. It has been observed that some departments do not have adequate restraint on the Argon Gas cylinders. It is highly recommended that an approved mounting bracket be used to secure the bottle. Argon in the cylinder is under extremely high pressure. Should the bottle topple and the regulator break, the outcome could be lethal for anyone standing in front of the projectile that follows. BOC have approved mounting brackets. 3) Alcohol for wetting the crucible. Cyclomedica specify 95% ethanol or better to wet the carbon crucible. The use of 95% ethanol is to ‘wet’ the crucible in order to receive the Sodium Pertechnetate, IT IS NOT TO STERILISE. Without wetting, Technegas yields may be reduced by air bubbles forming in a dry crucible. High purity ethanol is required to ensure that no impurities are burned and ultimately breathed by the patient.
Richard F Gotch Global Service Manager. Cyclomedica Australia P/L. Mobile +61 (0) 418 203 629
IMAGING PULMONARY EMBOLISM WITH SPECT
Normal V/Q SPECT study using Technegas.• Studies are viewed co-registered in all planes in 3D to provide high contrast resolution.• SPECT allows visualisation of segments previously not identifi ed on planar imaging, for example medial basal segment of right lung.• Improves detection and characterisation of defects.Q* indicates a perfusion scan with Technegas from the ventilation scan present.• Perfusion only (Q) is obtained by subtracting ventilation from perfusion (Q*-V) allowing for decay and diff erence in acquisition times per projection.
Example of PE positive V/Q SPECT Scan• A small subsegmental perfusion mismatch identifi ed in the medial segment of the right middle lobe.• Subtraction of ventilation counts from perfusion data to show true perfusion counts only, improves visualisation of defects.• V:Q ratio parametric image demonstrates areas of high ventilation to perfusion (>1.0) (4).
• Helps quantify degree of mismatch in PE.
Fusion V/Q SPECT with CTPA • SPECT imaging allows the V:Q scan to be combined with anatomical imaging such as CTPA (3).
• In the example, V/Q SPECT identifi ed a large single segmental perfusion mismatch which was not initially seen on CTPA.• Fusion of functional and anatomical imaging improved the confi dence of the treating clinician and confi rmed the presence of PE.• The combination of both V/Q SPECT and CTPA unequivocally demonstrated PE.
Sample V/Q SPECT Acquisition Protocol: Ventilation SPECT parameters: Perfusion SPECT parameters: Collimator LEHR Collimator LEHR Matrix 128 x 128 Matrix 128 x 128 Acquisition Orbit 360o Acquisition Orbit 360o Np 120 images Np 120 images Radial sampling 3 degree steps Radial sampling 3 degree steps Zoom 1.0 Zoom 1.0 Orbit Type Non-Circular Orbit Type Non-Circular Continuous or Step and Shoot Continuous or Step and Shoot Time per Projection 15-20 seconds Time per Projection 12-15 seconds Radiopharmaceutical 99mTc-Technegas Radiopharmaceutical 99mTc-MAA Peaks 140keV Peaks 140keV Energy Window 20% Energy Window 20% Administered Dose 40–50MBq Administered Dose 160–220MBq
Dose Estimates from Lung Imaging
1. ICRP. ICRP Publication 53: Radiation Dose to Patients from Radiopharmaceuticals; 1988.2. ARSAC. Notes for Guidance on the Clinical Administration of Radiopharmaceuticals and Use of Sealed Radioactive Sources - March 2006, UK3. Hurwitz LM, Reiman RE, Yoshizumi TT, et al. Radiation dose with contemporary cardiothoracic multidetector CT protocols with an anthropomorphic female phantom: Implications for cancer induction. Radiol 2007; 245:742-750. 4. Milne EN. Female breast radiation exposure. Am J Roentgen 2006; 186:E245. ImPACT CT Dose Calculator (http://www.impactscan.org/ctdosimetry.htm) In. London: NHS(UK); 2006
References:1. IRCP Publication 53: Radiation Dose to Patients from Radiopharmaceuticals; 19882. Bailey DL, Schembri GP, Harris BE, Bailey EA, et al. Generation of planar images from lung ventilation/perfusion SPECT. Ann Nuc Med 2008: 22:437-4453. Harris B, Bailey DL, Roach PJ, et al. A clinical comparison between traditional planar V/Q images and planar images generated from SPECT V/Q scintigraphy. Nucl Med Commun 2008;29:323-30.4. Harris B, Bailey D, Roach P, Bailey E, King G. Fusion imaging of computed tomographic pulmonary angiography and SPECT ventilation/perfusion scintigraphy: initial experience and potential benefi t. Eur J Nucl Med Mol Imaging 2007;34:135-42.5. Harris B, Bailey D, Miles S, et al. Objective analysis of tomographic ventilation-perfusion scintigraphy in pulmonary embolism. Am J Respir Crit Care Med 2007;175:1173-80.6. Bajc M, Neilly JB, Miniati M, et al. EANM Guidelines for ventilation/perfusion scintigraphy. Part 1: Pulmonary imaging with ventilation/perfusion single photon emission tomography. Eur J Nucl Med Mol Imaging (2009) 36:1356-13707. Bajc M, Neilly JB, Miniati M, et al. EANM Guidelines for ventilation/perfusion scintigraphy. Part 2: Algorithms and clinical considerations for diagnosis of pulmonary embolism with V/PSPECT and MDCT. Eur J Nucl Med Mol Imaging (2009) 36:1528-1538
Planar Images from SPECT data The reprojection planar method developed by Bailey et al(2) using a simple dual energy window acquisi-tion is based on reprojection of the reconstructed SPECT images using the entire SPECT dataset to produce planar images at any viewing angle; An additional scatter energy window (108keV with 25% window) is acquired simultaneously with the emission window during SPECT acquisition to create a synthetic attenuation (μ) map; This μ-map is used to generate an AC transverse reconstructed SPECT dataset; The SPECT volume is then forward projected to generate planar images in multiple projections, including ‘single-lung’ medial and lateral images by removing interference from the contra-lateral lung. The reprojected planar images utilise counts from the entire SPECT dataset, typically 8-12 x 106 counts per planar image
SPECT Reconstruction Guidelines It is recommended to use OSEM (Ordered Subset Expectation Maximization) for SPECT reconstruction. Generally 4-8 subsets and 2-4 iterations will produce good images within a reasonable processing time. This can vary between camera systems and software packages Filtering based on the total counts per image. As a guide, a Butterworth or low-pass fi lter using a cut-off (Nyquist frequency) of 0.7 to 1.0 cycles/cm and an order of 6 to 10 will produce good quality images.
V
Q*
V
V:Q
Q*
Q
Cyclomedica gratefully acknowledges the assistance of the team from the Department of Nuclear Medicine at Royal North Shore Public Hospital - Sydney for their kind permission to reproduce the data within this poster.
The fi gure above shows planar images reprojected from the reconstructed SPECT V/Q lung scans at the conventional viewing angles. To do so, the SPECT data need to be reprojected through an attenuation ( )map. This can be obtained from a CT scan on a SPECT/CT combined system, or, alternatively, a ‘synthetic’ attenuation map can be produced from the lung scan’s photopeak and scatter windows. The steps in producing the syn-thetic map are shown in the fi gure on the right with (A) and (B) showing the reconstructed scatter and photopeak windows respectively, and then the steps in processing and combining these, replacing the reconstructed values with assumed values for lung and soft tissue (bone is ignored). This approach has been shown to be suitable for the formation of the planar images and can be easily implemented on any gamma camera.
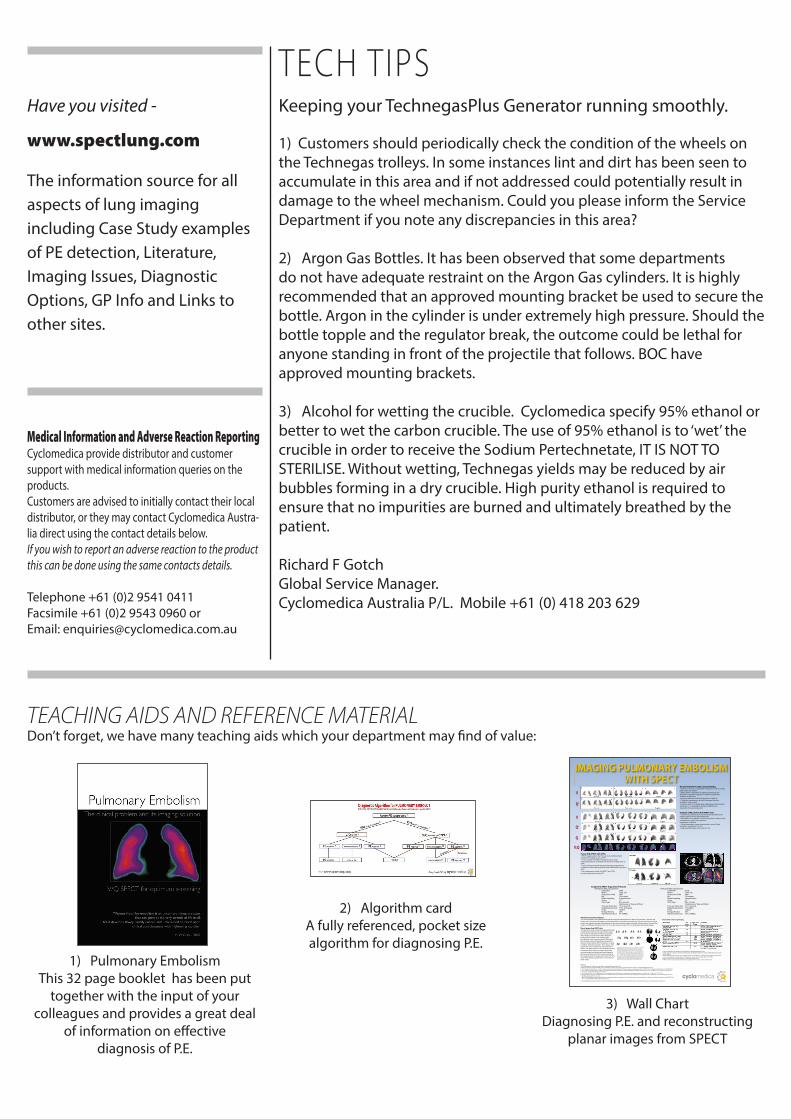
TEACHING AIDS AND REFERENCE MATERIALDon’t forget, we have many teaching aids which your department may find of value:
1) Pulmonary Embolism This 32 page booklet has been put
together with the input of your colleagues and provides a great deal
of information on effective diagnosis of P.E.
2) Algorithm cardA fully referenced, pocket size algorithm for diagnosing P.E.
3) Wall ChartDiagnosing P.E. and reconstructing
planar images from SPECT

NUCLEAR MEDICINE
TechnegasPLUS FDG + PosijetTotal control - the power, convenience and precision of bulk dose operations
Load one bulk FDG dose - Minimal exposure to patient or operator
Completely manoeuvrable - move to the patient
Internal power - no need for power points
Draws up patient dose for injection - exact dosage
Connects to patient records - Completely current files
Patient dosage printout - Stays with patient for confirmation
Step by step touch screen - Added safety in operation
Manual injection -Added asssurance of cannula placement
If you have a PET facility or contemplating one, call to discuss your FDG supply and mobile injector options.
Cyclopet FDG - No compromise
Best agent for V/Q SPECT
• Provendiagnosticaccuracy-especiallyin presence of COPD• Almost4millionstudiesperformed in 53 countries• Noexclusioncriteria;neonatestofrail-aged• 1-3breathsforfulldose• Noninvasive• LowradiationburdencomparedwithCTPA*
* About 1/7th of breast tissue exposure
NUCLEAR MEDICINE
CURRENTLY AUSTRALIA ONLY
Contact your nearest office -ASIA / PACIFIC / STH AFRICA - Cyclomedica Australia - [email protected] Ph: + 61 2 9541 0411 Fx: + 61 2 9543 0960 Contact - Charles Buttigieg Ph: + 61 2 9541 0411 M: +61 (0)418 285 048 E: [email protected] / MIDDLE EAST / NTH AFRICA - Contact Mr Bjorn Altmann - [email protected] Ph: +49 (0) 5341 550802 Fx: +49 (0) 5341 55803CANADA - Cyclomedica Canada - [email protected] Ph: +1 905 319 9610 Fx: +1 905 319 0497Contact - Lynn McLauchlin Ph: +1905 690 0345 Fx: +1905 690 0553LATIN AMERICA- Cyclomedica Latin America - [email protected] Ph: + 54 11 4585 9172 Fx: + 54 11 4586 0251 Contact - Martin Lema Ph: + 54 911 5174 1639GERMANY - Cyclomedica Germany - [email protected] Ph: +49 (0) 5341 550802 Fx: + 49 (0) 5341 55803 Contact - Bjorn Altmann