ct diagnosis of acute mesenteric
TRANSCRIPT
8/14/2019 CT Diagnosis of Acute Mesenteric
http://slidepdf.com/reader/full/ct-diagnosis-of-acute-mesenteric 1/9
408 AJR:192, February 2009
tion, and hypoperfusion associated with non-occlusive vascular disease, and the CT nd-ings vary widely depending on the cause andunderlying pathophysiology [1–5, 9]. CTndings of acute mesenteric ischemia shouldbe characterized on the basis of the cause. Inaddition, the severity of bowel ischemia (i.e.,supercial mucosal or transmural bowel wallnecrosis), the location (i.e., small or largebowel), and the presence and degree of hem-orrhage or subsequent superinfections mayaffect the CT appearance. In this article, cur-rent imaging techniques and CT ndings ofmesenteric ischemia resulting from variouscauses are reviewed with their underlyingpathophysiology.
CT ExaminationPreparation
Oral and rectal administration of contrastmaterial is recommended for accurate CTand assessment of acute bowel ischemia [1].A variety of contrast materials providingpositive, neutral, or negative contrast are
available. Whether contrast material is indi-cated should be carefully considered for pa-tients with bowel obstruction; materials con-taining barium are contraindicated in patientswith bowel leak or perforation. However, inthe acute state, particularly in patients withlife-threatening conditions, indication oftrans oral contrast may not be possible or maynot be signicant because of an adynamicileus preventing contrast material from mov-ing through the intestine.
CT Diagnosis of Acute MesentericIschemia from Various Causes
Akira Furukawa1 Shuzo KanasakiNaoaki KonoMakoto WakamiyaToyohiko TanakaMasashi TakahashiKiyoshi Murata
Furukawa A, Kanasaki S, Kono N, et al.
1All authors: Department of Radiology, Shiga University
of Medical Science, Seta Tsukinowa-cho, Otsu, Shiga520-2192 , Japan. Address correspondence toA. Furukawa ([email protected]).
G a s t r o i n t e s t i n a l I m a g i n g • Re v i e w
CMEThis article is available for CME credit.See www.arrs.org for more information.
AJR 2009; 192:408–416
0361–803X/09/1922–408
© American Roentgen Ray Society
Acute mesenteric ischemia is alife-threatening condition, with areported mortality rate of50–90% [1–3], that requires early
diagnosis and treatment. Angiography hasbeen the reference standard imaging exami-nation; however, the role of CT in this settinghas expanded with the advent of helical CTscanners [3–9]. In particular, MDCT tech-nology has dramatically improved the perfor-mance of CT by allowing rapid volumetricdata acquisition to provide increased longitu-dinal spatial resolution over a large anatomicvolume. From the volume data, retrospectivethin or thick sections; sagittal, coronal, orcurved multiplanar reformatted images; andCT angiograms with 2D or 3D visualizationcan be obtained. The rapid scanning capabil-ity of this technique coupled with IV boluscontrast injection substantially optimizesscan timing to allow both the arterial and ve-nous phases to be imaged. These advantagesare helpful in identifying the site, level, andcause of bowel ischemia by showing abnor-
malities in the bowel wall, mesentery, andmesenteric vessels. With these developments,the ability of CT for diagnosing mesentericischemia has recently been reported to havea sensitivity of approximately 90% [3, 10,11]. It can also provide alternative diagnosesfor patients in whom mesenteric ischemia issuspected.
Acute mesenteric ischemia can be causedby various conditions such as arterial occlu-sion, venous occlusion, strangulating obstruc-
Keywords: acute mesenteric ischemia, CT, emergencyradiology, mesenteric arterial occlusion, mesentericvenous occlusion, nonocclusive mesenteric ischemia,strangulating bowel obstruction
DOI:10.2214/AJR.08.1138
Received April 29, 2008 ; accepted after revisionJuly 22, 2008.
OBJECTIVE. Acute mesenteric ischemia can be caused by various conditions such asarterial occlusion, venous occlusion, strangulating obstruction, and hypoperfusion associatedwith nonocclusive vascular disease, and the CT ndings vary widely depending on the causeand underlying pathophysiology. The aim of this article is to review the CT appearances ofacute mesenteric ischemia in various conditions.
CONCLUSION. Recognition of characteristic CT appearances and the variations as-
sociated with each cause may help in the accurate interpretation of CT in the diagnosis ofmesenteric ischemia.
Furukawa et al.CT Diagnosis of Acute Mesenteric Ischemia
Gastrointestinal ImagingReview

8/14/2019 CT Diagnosis of Acute Mesenteric
http://slidepdf.com/reader/full/ct-diagnosis-of-acute-mesenteric 2/9
AJR:192, February 2009 409
CT Diagnosis of Acute Mesenteric Ischemia
Luminal contrast material may be useful inrelatively stable patients, and neutral contrastmaterial should be used for the correct assess-ment of bowel enhancement after IV contrastadministration [3, 10, 12]. The use of neutralcontrast material is also benecial in the for-mation of multiplanar images and in CT an-giography because neutral contrast materialdoes not interfere with image quality [3].
Positive contrast mater ial may be advanta-geous in assessing patients with ischemiccolitis by showing thickened bowel wall andrevealing the presence of bowel obstructionor in evaluating patients with a contraindica-tion for IV contrast administration. Whencontrast material is applied, oral administra-tion of 600–750 mL of luminal contrast ma-terial 30–120 minutes before scanning andrectal administration of 400–800 mL of lu-minal contrast material are used [1, 10].
CT TechniqueCT images are obtained from the dome of
the liver to the level of the perineum to coverthe entire course of the intestine. WithMDCT scanners, a collimation of 0.5–2.5mm and a detector pitch of 1.0–2.0 are used.Images with a 5- to 7-mm section thicknessare usually constructed for image interpreta-tion; however, thinner sections of contiguous1–2 mm should also be constructed for mul-tiplanar image reformations and CT angiog-raphy. Sagittal images are helpful in assess-ing the origin of the mesenteric arteries and
their variations [10].Acquisition of both unenhanced and con-
trast-enhanced CT scans is always necessary.
The role of unenhanced CT is to identify vas-cular calcication, hyperattenuating intravas-cular clotting, and intramural hemorrhage;the role of contrast-enhanced CT is to identi-fy thrombi in the mesenteric arteries andveins, abnormal enhancement of the bowelwall, and the presence of embolism or infarc-tion of other organs [1]. For contrast-en-hanced CT, 100–150 mL of iodinated contrastmaterial is administered at a rate of 2–5 mL/s,and scanning starts with delay times of 30and 60 seconds for dual acquisition and 40–60 seconds for single acquisition [1, 10, 13].
CT Findings in Acute Bowel IschemiaAcute bowel ischemia provides various
morphologic and attenuation abnormalitieson CT images in the bowel wall, mesentericvessels, and mesentery. The lumen of thebowel may dilate when lled with air or uid.These variations depend on the pathogenesisof bowel ischemia as well as the acuteness,duration, site, and extent of the ischemic at-tack and the state of the collateral circula-tion. Superimposed bowel wall infection andthe presence of perforation may also affectthe CT appearances of acute bowel ischemia.In lm interpretation, radiologists should as-sess the bowel wall, its thickness and attenu-ation; luminal dilatation; mesenteric vessels;mesentery; and other organs [1, 14, 15].
Bowel Wall Bowel wall thickness— Normal bowel
ranges from 3 to 5 mm thick depending onthe degree of bowel distention [1, 14–16].Bowel wall thickening is not a specic but is
the most frequently observed CT nding inmesenteric ischemia and is caused by muraledema, hemorrhage, or superinfection ofthe ischemic bowel wall [1, 10, 17] (Fig. 1).The degree of thickening is usually less than1.5 cm, typically 8–9 mm [10], and is oftenobserved in mesenteric venous occlusion,strangulation, ischemic colitis, and mesen-teric arterial occlusion after reperfusion [1,4–6, 10].
In exclusively arterial occlusive mesen-teric ischemia or infarction, however, thebowel wall becomes thinner rather thanthicker because there is no arterial ow andneither mural edema nor hemorrhage occurs.Thinning of the bowel wall or “paper-thinwall” is caused by volume loss of tissue andvessels in the bowel wall and by loss of intes-tinal muscular tone [1, 4–6, 8, 10] (Fig. 2).Bowel wall thickening is not a consistent CTnding in mesenteric ischemia, and the de-gree of thickening does not correlate withseverity [1].
Bowel wall attenuation— Bowel wall at-tenuation should always be assessed on bothunenhanced and contrast-enhanced CT im-ages to avoid misinterpretation of high den-sity of the bowel wall as normal positiveenhancement on contrast-enhanced CT incases of intramural hemorrhage. On unen-hanced CT images, low attenuation of thebowel wall indicates bowel wall edema,which typically occurs in mesenteric arterialocclusion after reperfusion, mesenteric ve-
nous occlusion, strangulation, and ischemiccolitis [1, 14–16, 18]. High at tenuation of thewall is caused by intramural hemorrhage
Fig. 1—Contrast-enhanced CT image of abdomen in 40-year-old woman withsuperior mesenteric vein and portal vein thrombosis. Wall thickening of ascendingand transverse colon ( arrowheads ) is shown. Engorgement of mesenteric veins isalso visible.
Fig. 2—Contrast-enhanced CT image of abdomen in 78-year-old man withembolism of superior mesenteric artery. Bowel loops are distended with air and their wall is “paper-thin.”
8/14/2019 CT Diagnosis of Acute Mesenteric
http://slidepdf.com/reader/full/ct-diagnosis-of-acute-mesenteric 3/9
410 AJR:192 , February 200 9
Furukawa et al.
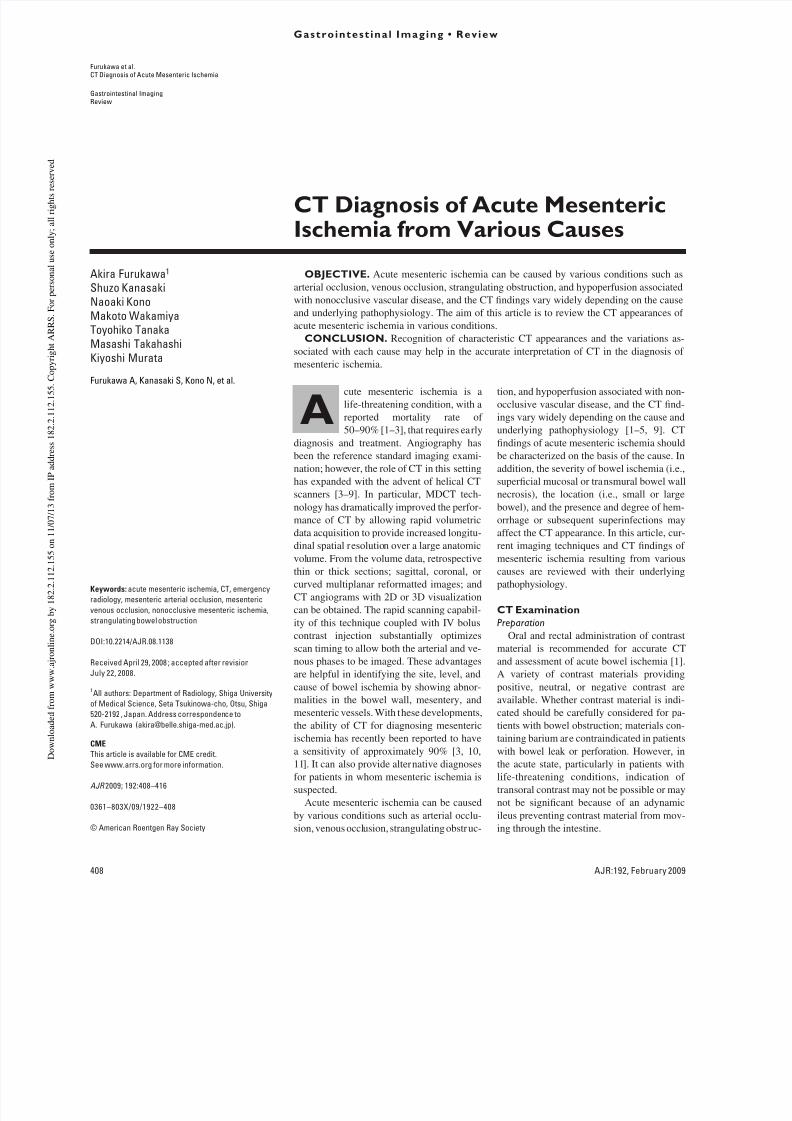
and hemorrhagic infarction [1, 14–16, 18](Fig. 3).
On contrast-enhanced CT, a highly spe-cic but not sensitive nding for acute mes-enteric ischemia is absent or diminished con-trast enhancement of the bowel wall [1, 6,19]. A halo or target appearance is also in-dicative of mesenteric ischemia, representinghyperemia and hyperperfusion associatedwith surrounding mural edema, and can beseen in arterial occlusion after reperfusion,
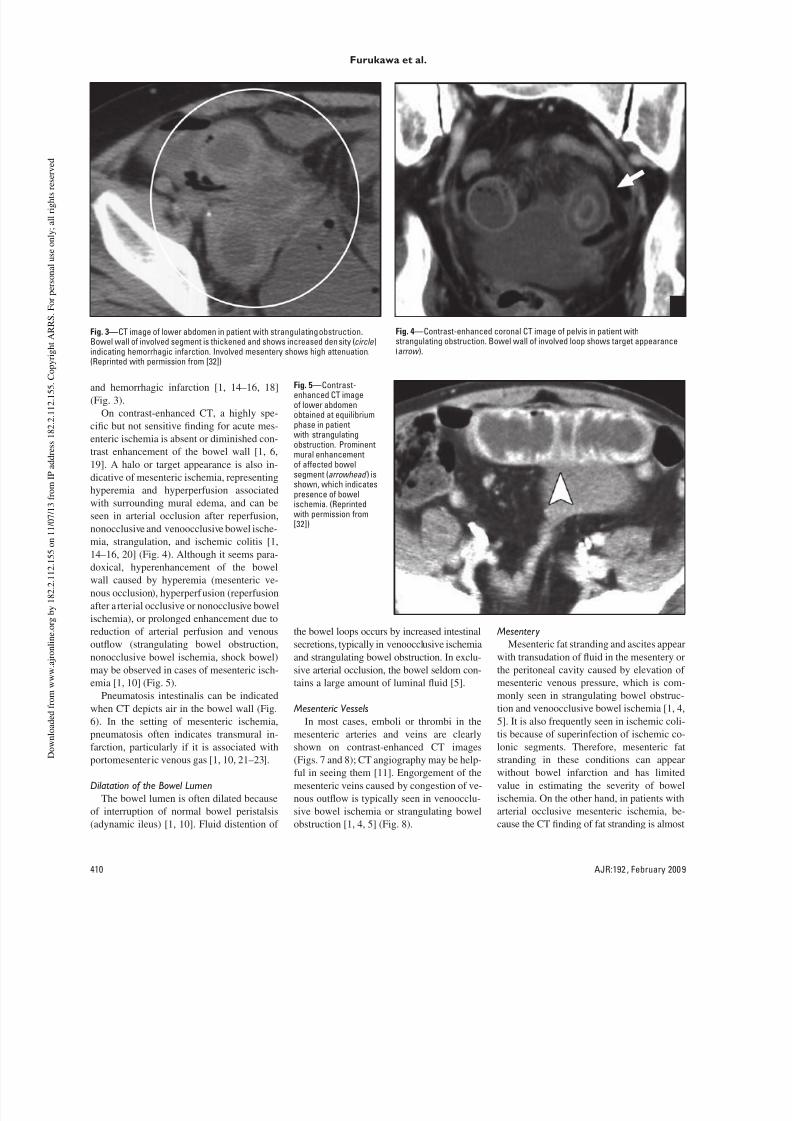
nonocclusive and venoocclusive bowel ische-mia, strangulation, and ischemic colitis [1,14–16, 20] (Fig. 4). Although it seems para-doxical, hyperenhancement of the bowelwall caused by hyperemia (mesenteric ve-nous occlusion), hyperperfusion (reperfusionafter a rterial occlusive or nonocclusive bowelischemia), or prolonged enhancement due toreduction of arterial perfusion and venousoutow (strangulating bowel obstruction,nonocclusive bowel ischemia, shock bowel)may be observed in cases of mesenteric isch-emia [1, 10] (Fig. 5).
Pneumatosis intestinalis can be indicatedwhen CT depicts air in the bowel wall (Fig.6). In the setting of mesenteric ischemia,pneumatosis often indicates transmural in-farction, particularly if it is associated withportomesenteric venous gas [1, 10, 21–23].
Dilatation of the Bowel LumenThe bowel lumen is often dilated because
of interruption of normal bowel peristalsis(adynamic ileus) [1, 10]. Fluid distention of
the bowel loops occurs by increased intestinalsecretions, typically in venoocclusive ischemiaand strangulating bowel obstruction. In exclu-sive arterial occlusion, the bowel seldom con-tains a large amount of luminal uid [5].
Mesenteric VesselsIn most cases, emboli or thrombi in the
mesenteric arteries and veins are clearlyshown on contrast-enhanced CT images(Figs. 7 and 8); CT angiography may be help-ful in seeing them [11]. Engorgement of themesenteric veins caused by congestion of ve-nous outow is typically seen in venoocclu-sive bowel ischemia or strangulating bowelobstruction [1, 4, 5] (Fig. 8).
Mesentery Mesenteric fat stranding and ascites appear
with transudation of uid in the mesentery orthe peritoneal cavity caused by elevation ofmesenteric venous pressure, which is com-monly seen in strangulating bowel obstruc-tion and venoocclusive bowel ischemia [1, 4,5]. It is also frequently seen in ischemic coli-tis because of superinfection of ischemic co-lonic segments. Therefore, mesenteric fatstranding in these conditions can appearwithout bowel infarction and has limitedvalue in estimating the severity of bowelischemia. On the other hand, in patients witharterial occlusive mesenteric ischemia, be-cause the CT nding of fat stranding is almost
Fig. 3—CT image of lower abdomen in patient with strangulating obstruction.Bowel wall of involved segment is thickened and shows increased density ( circle )
indicating hemorrhagic infarction. Involved mesentery shows high attenuation.(Reprinted with permission from [32])
Fig. 4—Contrast-enhanced coronal CT image of pelvis in patient withstrangulating obstruction. Bowel wall of involved loop shows target appearance
(arrow ).
Fig. 5—Contrast-enhanced CT imageof lower abdomenobtained at equilibriumphase in patientwith strangulatingobstruction. Prominentmural enhancementof affected bowelsegment ( arrowhead ) isshown, which indicatespresence of bowelischemia. (Reprintedwith permission from
[32])

8/14/2019 CT Diagnosis of Acute Mesenteric
http://slidepdf.com/reader/full/ct-diagnosis-of-acute-mesenteric 4/9
AJR:192 , February 200 9 411
CT Diagnosis of Acute Mesenteric Ischemia
exclusively present with transmural infarc-tion, this nding can be helpful in estimatingthe severity of bowel ischemia [1, 4, 5].
Bowel Ischemia and Infarction inVarious Conditions
Bowel ischemia and infarction can becaused by various conditions such as mesen-teric arterial occlusion, mesenteric venousocclusion, strangulating bowel obstruction,
and hypoperfusion associated with nonoc-clusive vascular disease. The clinical fea-tures and typical CT appearances of eachcondition are summarized in Table 1.
Acute Mesenteric Arterial OcclusionAcute mesenteric arterial occlusion is typ-
ically caused by a thromboembolism associ-ated with cardiovascular problems followedby arterial thrombosis, which accounts for
60–75% (arterial embolism, 40–50%; arte-rial thrombosis, 20–30%) of all acute bowelischemia cases [1–3, 24–26]. Most emboliwedge at branching points around or dista l tothe middle colic artery, whereas thrombosistypically occurs at or near the origin of themesenteric arteries [3]. Although the severi-ty may vary, bowel ischemia is typically fol-lowed by infarction, perforation, and perito-nitis unless reperfusion occurs.
On contrast-enhanced CT images, emboliand thrombi can be seen as defects in the su-perior mesenteric artery and its branches [2,10] (Figs. 7 and 9). The diameter of the supe-rior mesenteric artery is often larger than thatof the superior mesenteric vein. The th icknessof the bowel wall of the involved segments isthe same as or thinner than that of the healthysegments unless reperfusion occurs [1, 4, 9].The lumen of the bowel may be lled with
uid, gas, or both; however, the bowel sel-dom contains a large amount of uid. Con-trast enhancement of the involved bowel isabsent or diminished [1–5, 9, 10] (Fig. 9).Pneumatosis can typically be observed incases with transmural infarct ion with or with-out associated portomesenteric venous gas.In cases with reperfusion or rich collaterals,the involved bowel segments may thicken andshow the halo or target pattern of contrast en-hancement [1, 4, 9] (Fig. 10). Coexisting em-bolism of other organs may also be observedon contrast-enhanced CT, which supports thediagnosis of mesenteric ischemia (Fig. 11).
The diagnosis of acute mesenteric arterialocclusion is usually made based on a combi-nation of the CT ndings described earlier.The diagnostic performance of CT for mes-enteric ischemia conned to mesenteric arte-rial occlusion has not been ascertained, toour knowledge; however, the diagnostic per-formance of CT for primary mesenteric is-chemia, including arterial and venous occlu-sive and nonocclusive mesenteric ischemia,has been reported as 64–96% in sensitivityand 92–100% in specicity [6, 11]. In thecase of each CT nding, a lack of focal bow-el wall enhancement and the presence ofpneumatosis intestinalis are relatively sensi-
tive (sensitivity, 42%) and highly specic(specicity, 97–100%) [11]. Findings of de-fects or occlusion of the mesenteric arteriesor veins and gas in the mesenteric or portalveins or in the mesenteric arteries are lesssensitive (12–15%) but are highly specic(94–100%) [11]. Findings of bowel wallthickening and mesenteric stranding are rel-atively high in sensitivity (85–88%) but areless specic (61–72%) [11].
A
Fig. 6—56-year-oldman with mesenteric
infarction.A–C, Contrast-enhancedCT images of upper(A), mid (B), and lower(C) abdomen showgas in portal venousbranches ( A), gas inmesenteric veins ( circle ,B), and gas in bowel wall(arrowheads , C).
B
C

8/14/2019 CT Diagnosis of Acute Mesenteric
http://slidepdf.com/reader/full/ct-diagnosis-of-acute-mesenteric 5/9
412 AJR:192 , February 200 9
Furukawa et al.
Venous Occlusion
Thrombosis of the mesenteric vein can beprimary or secondary to portal hypertensionor infection or can be associated with varioushypercoagulopathy states [1, 2, 20, 27]. Mes-enteric venous obstruction does not typicallylead to severe bowel ischemia; however,thrombosis of the mesenteric vein, particu-larly at a distal level, may cause bowel in-farction and accounts for 5–10% of acutebowel ischemia. Impairment of venous drain-age causes elevation of the hydrostatic pres-sure, which leads to extravascular leakage of
plasma, RBCs, or both into the bowel wall,
mesentery, and peritoneal cavity. The bowelloops are typically prominently dilated [1, 3,26]. Impairment of venous drainage mayalso compromise the arterial blood ow andcause bowel ischemia and infarction.
On contrast-enhanced CT, thrombus inthe mesenteric and portal veins is usuallyvisible, and mesenteric venous obstructioncan be conrmed by CT in more than 90% ofcases [28–30] (Fig. 12). Engorgement of themesenteric veins is also observed. Fat strand-ing in the mesentery and ascites are common
ndings. The bowel wall is prominently
thickened with absent or diminished en-hancement, hyperenhancement, or a halo ortarget pattern of contrast enhancement [1–5,7, 28]. Absent or diminished contrast en-hancement of the bowel wall usually indi-cates transmural infarction, particularlywhen it is associated with pneumatosis andportomesenteric venous gas [28–30]. On thecontrary, the degree of bowel wall thicken-ing, mesenteric fat stranding, or ascites doesnot correlate with the severity of ischemicbowel damage [28].
TABLE 1: Clinical Features and Typical CT Findings of Mesenteric Ischemia in Various Conditions
Characteristic Arterial Occlusion Venous Occlusion Strangulation Nonocclusion
Incidence 60–70% of PMI 5–10% of PMI 10% of SBO 20% of PMI
Presentation Acute Subacute Acute Acute or subacute
Risk factors Arrhythmia, myocardialinfarction, valve disease,atherosclerosis a, prolongedhypotension a
Portal hypertension, venoushypercoagulopathy,right-sided heart failure
Previous abdominal surgery,internal and external hernia,intestinal malrotation
Hypovolemia, hypotension,low cardiac output, digoxin,α -adrenergic agonists
Bowel wall Thinning, no change, or thickening with reperfusion
Thickening Thickening No change or thickening withreperfusion
Attenuation of bowel wallon unenhanced CT
Not characteristic Low with edema; high withhemorrhage
Low with edema; high withhemorrhage
Not characteristic
Enhancement of bowel wallon contrast-enhanced CT
Diminished, absent, targetappearance or high withreperfusion
Diminished, absent, targetappearance, or increased
Diminished, absent, targetappearance, or increased
Diminished, absent,heterogeneous indistribution
Bowel dilatation Not apparent Moderate to prominent Prominent (lled with uid) Not apparent
Mesen ter ic vessels Defect or defects in ar ter ies ,arterial occlusion, SMA >SMV in diameter
Defect or defects in veins,venous engorgement
No defect, venous engorgement No defect, arterialconstriction
Mesentery Not hazy until mesentericinfarction occurs
Hazy wi th ascites Hazy with asci tes, “whirl sign”[44], or “spoke wheel sign” [45]
Not hazy until mesentericinfarction occurs
Note—P MI = primary mesenteric ischemia (i.e., arterial or venous occlusive or nonocclusive bowel ischemia), SBO = small-bowel obstruction, SMA = superiormesenteric artery, SMV = superior mesenteric vein.
aA risk factor for thrombosis.
Fig. 7—Contrast-enhanced CT image in patient with embolism of superiormesenteric artery shows defect ( arrowhead ) in superior mesenteric artery.
Fig. 8—Contrast-enhanced CT image in 40-year-old man (same patient as Fig. 2)with superior mesenteric vein thrombosis shows defect in superior mesentericvein (arrowhead ). Distal branches of vein are engorged.

8/14/2019 CT Diagnosis of Acute Mesenteric
http://slidepdf.com/reader/full/ct-diagnosis-of-acute-mesenteric 6/9
AJR:192, February 2009 413
CT Diagnosis of Acute Mesenteric Ischemia
A B
Fig. 9—71-year-old woman with superior mesenteric artery embolism.A, Contrast-enhanced CT image obtained cephalad to B shows defect in superior mesenteric artery ( arrowhead ).B, Contrast-enhanced CT image shows that mural enhancement is absent at most intestinal loops.
Fig. 10—Contrast-enhanced CT image in 83-year-old woman with superiormesenteric artery embolism after reperfusion. Mural thickening of intestine(circle ) is visible, showing target appearance.
Fig. 11—Contrast-enhanced CT image in 74-year-old man with superiormesenteric artery embolism shows defect ( arrowhead ) in superior mesentericartery. In addition, contrast enhancement of right kidney ( arrow ) is absent, whichindicates embolism of right renal artery.
A B
Fig. 12—46-year-old man with superior mesenteric vein thrombosis.A, Contrast-enhanced CT image obtained cephalad to B shows thrombi in superior mesenteric vein ( arrowhead ) and splenic vein ( arrow ).B, Contrast-enhanced CT image shows engorgement of mesenteric veins ( arrowhead ) and mural thickening of intestine. Ascites is present.

8/14/2019 CT Diagnosis of Acute Mesenteric
http://slidepdf.com/reader/full/ct-diagnosis-of-acute-mesenteric 7/9
414 AJR:192, February 2009
Furukawa et al.
Strangulating Obstruction: Closed-LoopBowel Obstruction
Strangulating obstruction is a mechanicalbowel obstruction associated with bowelischemia that is seen in approximately 10%of patients with small-bowel obstruction [31,32]. Strangulating obstruction is almost ex-
clusively associated with a closed-loop ob-
struction (Figs. 13 and 14), which is causedmost often by an adhesive band and occa-sionally by an internal or external hernia. Aclosed-loop obstruction tends to involve themesentery and mesenteric vessels and isprone to produce a volvulus. Typically, stran-gulation in a closed-loop bowel obstruction
is caused initially by impairment of venous
outow followed by arterial ischemia be-cause the arterial pressure is higher than thevenous pressure. Congestion or hemorrhagein the bowel wall and mesentery occurs, andthe affected bowel loops are distended andlled with uid.
On CT, a closed-loop obstruction is identi-
ed by a unique conguration of C - or U -
Fig. 13—Illustration of closed-loop obstruction. Closed-loop obstruction is uniqueform of mechanical bowel obstruction in which two points of intestine along itscourse are obstructed at single site. Arrowhead shows site of obstruction. C =closed loop, P = proximal loop, D = distal loop.
Fig. 14—Example of closed-loop obstruction. Axial MR image in 52-year-oldwoman shows site of obstruction ( arrowhead ), closed loop (C), proximal loop (P),and distal loop (D).
Fig. 15—Contrast-enhanced CT image shows closed-loop obstruction at rightlower abdomen. Distended loops are seen lled with uid and mesentery isconverging toward site of obstruction ( circle ). Bowel wall is slightly thickened anddensity of mesentery is increased. (Reprinted with permission from [31])
Fig. 16—Contrast-enhanced coronal CT image shows closed-loop obstructionat lower abdomen. Distended loops are seen around their mesentery. Contrastenhancement is absent at bowel loops on righ t-hand side ( arrowheads ) andattached mesentery shows increased density, which indicates mesentericischemia.

8/14/2019 CT Diagnosis of Acute Mesenteric
http://slidepdf.com/reader/full/ct-diagnosis-of-acute-mesenteric 8/9
AJR:192 , February 200 9 415
CT Diagnosis of Acute Mesenteric Ischemia
shaped distended loops with the mesentericvessels converging toward the site of obstruc-tion (Figs. 14–16). The obstructed site of theclosed loops can be located by following thecourse of the distended bowel loops [31–35].The affected bowel is lled almost exclusive-ly with only uid and no gas. The affectedmesentery typically shows a fan shape. Incases with strangulation, the bowel wall isthickened and shows absent or diminishedenhancement, hyperenhancement, or a haloor target pattern of enhancement on contrast-
enhanced CT examination. The affectedmesentery shows inltration and strandingassociated with engorged mesenteric veins.Ascites is also observed [31–35].
CT performance in diagnosing strangula-tion is reported as 83–100% in sensitivity,61–93% in specicity, 72–88% in positivepredictive value, and 93–100% in negativepredictive value [36–39], although a relative-ly low sensitivity of 51.9% has been reportedrecently [40]. The diagnosis of strangulationis based on the characteristic ndings de-scribed earlier or their combination. Amongthose ndings, absent or diminished bowelwall enhancement and inltration of the af-fected mesentery are highly specic. The“small-bowel feces sign” is also reported as auseful nding indicating the presence ofstrangulation [40].
Hypoperfusion Associated with NonocclusiveVascular Disease
Bowel ischemia and infarction can occurwith a reduction of mesenteric blood supply
Fig. 17—Contrast-enhanced CT image ( A) of pelvis in 69-year-old man with nonocclusive mesenteric ischemia. Contrast enhancement is prominently diminished orabsent at distal ileal loops ( arrowheads ). Bowel wall thickening is not present. Af ter reperfusion, bowel loops show prominent wall thickening with appearance of targetsign (B).
without vascular occlusion, which is callednonocclusive mesenteric ischemia or infarc-tion. This type of bowel ischemia accountsfor 20–30% of all acute mesenteric ischemiaor infarction cases, with mortality rates from30% to 93% [3, 41, 42]. A reduction of themesenteric blood supply is the result of mes-enteric arterial vasoconstriction on reex tohypotension or administration or abuse ofdigitalis, ergotamine, vasopressin or othervasoconstrictive agents, amphetamine, andcocaine [3, 7, 41, 42]. Ischemic injury may
range from reversible supercial damage lo-calized to the watershed areas to a more se-vere form that extends to the entire bowel.Hypoperfusion results in increased vascularpermeability that leads to extravascular leak-age of plasma, RBCs, or both into the bowelwall, mesentery, and peritoneal cavity.
Shock bowel is a var iation of nonocclusivemesenteric ischemia caused by hypotensiveshock induced by blunt abdominal trauma [3,43]. Ischemic colitis and obstructive colitisare considered similar disease entities [1, 4,5]. On CT, the bowel wall of the involvedsegments may be normal or thickened (Fig.17). The pattern of enhancement is variableas absent or diminished enhancement, in-creased enhancement, or halo or target typeof enhancement [1, 4, 5]. Fat stranding of themesentery and ascites are visible. Amongvarious conditions of mesenteric ischemia,nonocclusive mesenteric ischemia is the mostdifcult condition to diagnose on CT, andangiography is often required for correct andcondent diagnosis [42].
ConclusionAn accurate and early diagnosis is essential
for the appropriate and successful treatmentof patients with acute mesenteric ischemia toimprove their prognoses. With the advancesin CT technology, CT has realized a high di-agnostic performance and become an essen-tial diagnostic tool in this clinical setting. Fora correct diagnosis, a technically appropriateCT examination and proper interpretation ofimages are mandatory. Because acute mesen-teric ischemia can be caused by various condi-
tions, the CT ndings vary widely, dependingon the cause and underlying patho physiologyand the presence of associated complica-tions. Recognition of the characteristic CTappearances and variations of each causemay help in the accurate interpretation of CTin the diagnosis of mesenteric ischemia.
AcknowledgmentsWe thank Tsutomu Sakamoto, Katsumi
Hayakawa, and Masato Fujita for their in-struction and assistance with the manuscript.
References 1. Wiesner W, Khurana B, Ji H, Ros PR. CT of acute
bowel ischemia. Radiology 2003; 226:635–650
2. Oldenburg WA, Lau LL, Rondenburg TL, Ed-
monds HJ, Burger CD. Acute mesenteric isch-
emia. Arch Intern Med 2004; 164:1054–1062
3. Segatto E, Morte lé KJ, Ji H, Wiesner W, Ros PR.
Acute small bowel ischemia: CT imaging ndings.
Semin Ultrasound CT MR 2003; 24:364–376
4. Chou CK, Mark CW, Tzeng WS, Chang JM. CT
of small bowel ischemia. Abdom Imaging 2004;
A B

8/14/2019 CT Diagnosis of Acute Mesenteric
http://slidepdf.com/reader/full/ct-diagnosis-of-acute-mesenteric 9/9
416 AJR:192 , February 200 9
Furukawa et al.
29:18–22
5. Chou CK. CT manifestations of bowel ischemia.
AJR 2002; 178:87–91
6. Taourel PG, Deneuville M, Pradel JA, Régent D,
Bruel JM. Acute mesenteric ischemia: diagnosis
with contrast-enhanced CT. Radiology 1996; 199:
632–636
7. Rha SE, Ha HK, Le SH, et al. CT and MR imag-ing ndings of bowel ischemia from various pri-
mary causes. RadioGraph ics 2000; 20:29–42
8. Hoton KM, Fishman EK. Multi-detector row CT
of mesenteric ischemia: can it be done? Radio-
Graphics 2001; 21:1463–1473
9. Levy AD. Mesenteric ischemia. Radiol Clin North
Am 2007; 45:593–599
10. Horton KM, Fishman EK. Multidetecto r CT an-
giography in the diagnosis of mesenteric ischemia.
Radiol Clin North Am 2007; 45:275–288
11. Kirkpa trick ID, Kroeker MA, Greenberg HM. Bi-
phasic CT with mesenteric CT angiography in the
evaluation of acute mesenteric ischemia: initial
experience. Radiology 2003; 229:91–98
12. Megibow IJ, Babb JS, Hecht EM, et al. Evaluation
of bowel distention and bowel wall appearance by
using neutral oral contrast agent for multi-detector
row CT. Radiology 2005; 238:87–95
13. Schindera ST, Nelson RC, DeLong DM, et al.
Multi-detector row CT of the small bowel: peak
enhancement temporal window—initial experi-
ence. Radiology 2007; 243:438–444
14. Macari M, Balthazar EJ. CT of bowel wall thick-
ening: signicance and pitfalls of interpretation.
AJR 20 01; 176:1105–1116
15. Macari M, Megibow AJ, Balthazar EJ. A pattern
approach to the abnormal small bowel: observa-tions at MDCT and CT enterography. AJR 2007;
188:1344–1355
16. Wittenberg J, Harising hani MG, Jhaveri K, Var-
ghese J, Mueller PR. Algorithmic approach to CT
diagnosis of the abnormal bowel wall. Radio-
Graphics 2002; 22:1093–1109
17. Lee R, Tung HK, Tung PH, Cheung SC, Ch an FL.
CT in acute mesenteric ischemia. Clin Radiol
2003; 58:279–287
18. Bertnicke BJ, Balfe DM. CT appea rance of intes-
tinal ischemia and intramural hemorrhage. Radiol
Clin North Am 1994; 32:845–860
19. Klein HM, Lensing R, Klosterhalfen B, Toens C,
Guenther RW. Diagnostic imaging of mesenteric
infarction. Radiology 1995; 197:79–82
20. Ha HK, Rha SE, Kim AY, Auh YH. CT and MR
diagnosis of intestinal ischemia. Semin Ultra-
sound CT MR 2000 ; 21:40–55
21. Wiesner W, Mortelé KJ, Glickman JN, Ji H, Ros
PR. Pneumatosis intestinalis and portomesenteric
venous gas in intestinal ischemia: correlation of
CT ndings with severity of ischemia and clinical
outcome. AJR 2001; 177:1319–1323
22. Kernagis LY, Levine MS, Jacobs JE. Pneumatosis
intestinalis in patients with ischemia: correlation
of CT ndings with viability of the bowel. AJR
2003; 180:733–736
23. Ho LM, Paulson EK, Thompson WM. Pneumato -
sis intestinalis in the adult: benign to life-threat-
ening causes. AJR 2007; 188:1604–1613
24. Bradbury AW, Er ittenden J, McBride K , Ruckley
CV. Mesenteric ischemia: a multidisciplinary ap-
proach. Br J Surg 1995; 82:1446–1459
25. Mansour MA. Management of acute mesenter ic
ischemia. Arch Surg 1999; 134:328–330
26. Stoney RJ, Cunningha m CG. Acute mesenteric
ischemia. Surgery 1993; 114:489–490
27. Grendel JH, Ockner RK. Mesenteric venous
thrombosis. Gastroenterology 1982; 82:358–372
28. Bradbury MS, Kavanagh PV, Bechtold RE, et a l.
Mesenteric venous thrombosis: diagnosis and
noninvasive imaging. RadioGraph ics 2002; 22:
527–541
29. Rh ee RY, Gloviczki P. Mesenteric venous throm-
bosis. Surg Clin North Am 1997; 77:327–338
30. Harward TR, Green D, Bergan JJ, Rizzo RJ, YaoJS. Mesenteric venous thrombosis. J Vasc Surg
1989; 9:328–333
31. Fu rukawa A, Yamasaki M, Furuichi K, et al. Heli-
cal CT in the diagnosis of small bowel obstruc-
tion. RadioGraphics 2001; 21:341–355
32. Furukawa A, Yamasaki M, Takahashi M, et al.
CT diagnosis of small bowel obstruction: scan-
ning technique, interpretation and role in the di-
agnosis. Semin Ultrasound CT MR 2003; 24:336–
352
33. Frager DH, Baer JW. Role of CT in evaluating pa -
tients with small-bowel obstruction. Semin Ultra-
sound CT MR 1995; 16:127–140
34. Balthazar E J. George W. Holmes Lecture: CT of
small-bowel obstruction. AJR 1994; 162:255–261
35. Balthazar EJ, Birnbaum BA, Megibow AJ, Gor-
don RB, Whelan CA, Hulnick DH. Closed-loop
and strangulating intestinal obstruction: CT signs.
Radiology 1992; 185:769–775
36. Zalcman M, Sy M, Donckier V, Closset J, Gan-
sbeke DV. Helical CT signs in the diagnosis of
intestinal ischemia small-bowel obstruction. AJR
2000; 175:1601–1607
37. Frager D, Baer JW, Medwid SW, Rothpearl A,
Bossart P. Detection of intestinal ischemia in pa-
tients with acute small-bowel obstruction due to
adhesions or hernia: efcacy of CT. AJR 1996;
166:67–71
38. Balthazar EJ, Liebeskind ME, Macari M. Intesti-
nal ischemia in patients in whom small bowel ob-
struction is suspected: evaluation of accuracy,
limitations, and clinical implications of CT in di-
agnosis. Radiology 1997; 205 :519–522
39. Ha HK, Kim JS, Lee MS, et al. Differentiation of
simple and strangulated small-bowel obstruc-
tions: usefulness of known CT criteria. Radiology
1997; 204:507–512
40. Sheedy SP, Earnest IVF, Fletcher JC, Fidler JL,
Hoskin TL. CT of small-bowel ischemia associ-
ated with obstruction in emergency department
patients: diagnostic performance evaluation. Ra-
diology 2006 ; 241:729–736
41. Clotz S, Vestring T, Rötker J, Schmidt C, Scheld
HH, Schmid C. Diagnosis and treatment of non-
occlusive mesenteric ischemia after open heart
surgery. Ann Thorac Surg 20 01; 72:1583–1586 42. Trompeter M, Brazda T, Remy CT, Vestring T,
Reimer P. Non-occlusive mesenteric ischemia:
etiology, diagnosis, and interventional therapy.
Eur Radiol 2002; 12:1179–1187
43. Kim AY, Ha HK. Evaluation of suspected mesen-
teric ischemia: efcacy of radiologic studies. Ra-
diol Clin North Am 2003; 41:327–342
44. Khurana B. T he whirl sign. Radiology 2003;
226:69–70
45. Rudloff U. The spoke wheel sign: bowel. Radiol-
ogy 2005; 237:1046–1047
F O R Y O U R I N F O R M A T I O N
This a rt icl e i s avai lable for CME credit . See www.ar rs.org for more info rmation.