ctu orientation manual title - macpeds.com€¦ · gastroenterology, allergy and immunology,...
TRANSCRIPT
CTU 1 and 2 Orientation Manual
For Residents and Clinical Clerks 2015-‐2016
Editor: Dr. Moyez Ladhani
Table of Contents Welcome Letter .................................................................................................................................. 3 Introduction to the Division of General Pediatrics ................................................................ 4 Clinical Issues: ................................................................................................................................................... 7 Calling in Sick ................................................................................................................................................. 10 Evaluations ...................................................................................................................................................... 10 Contacts ............................................................................................................................................................ 10
Allied Health: Contacts ................................................................................................................. 11 Division of General Pediatrics CTU 1, CTU 2, Expectations .............................................. 13 Division of General Pediatrics: CTU 1 and 2 Weekly Schedule ....................................... 16 CTU 1 & 2 Faculty Expectations ................................................................................................. 17 Orientation Checklist for Teams 1 and 2 ............................................................................... 20 Patient Care/Charting ................................................................................................................... 22 Role of the Clinical Clerk .............................................................................................................. 24 Role of the Family Practice Resident/BCT ............................................................................. 25 Role of the Junior Pediatric Resident ...................................................................................... 27 Role of the Junior Pediatric Resident ...................................................................................... 29 Roles and Responsibilities of the Senior Pediatrics Resident on CTU ......................... 31 Role of the General Pediatric Fellow ....................................................................................... 35 Some Practical Tips on Being a Senior Pediatric Resident at McMaster ..................... 36 SPR Role for Consults .................................................................................................................... 40 Junior Float Objectives ................................................................................................................. 44 McMaster Pediatrics CTU Weekend and Holiday Call Guidelines .................................. 47 Day Float Objectives ...................................................................................................................... 51
Welcome Letter Dear Residents Rotating on Pediatrics, Welcome to your pediatrics CTU (teams 1 and 2) rotation. I hope that you have a good learning experience with us. Don’t hesitate to contact the pediatric chief residents, at [email protected] if you have any questions or concerns. The CTU Director is Dr. Ladhani [email protected]. The CTU administrative support is Skye Levely [email protected]. With respect to your first day, at MUMC please show up for handover at 7:15am sharp in 3N26. Weekend handover is at 8:30am. Your attending will meet you for orientation, to discuss objectives and sign your learning contract on 3C as follows. The PERC clinic is a component of the Pediatrics rotation for Family Medicine residents. You will be sent a schedule of which week during your rotation you are to attend the PERC clinic. The clinic starts at 8:45am in the Peds ER - ask at the registration desk & they will direct you to the PERC office. Please come as soon as your morning teaching is finished. You will be asked to get an Encounter Card filled for each day you attend clinic. Please keep these Encounter Cards & give them to the Pediatric Attending who will be completing your final evaluation. If no clinic is scheduled for a given day or your clinics finish early, please head back to the ward to help with inpatient duties and consults. Call will be in a float model, information about this will be sent to you by our chief residents. You should have received the “Green Book” (the pediatric survival guide) from your department. If you have not received one please contact your department coordinator. If you have lost it or need to buy one, please see Skye Levely ext. 75639, who can sell you one for $10.00. This can also be found at: http://www.macpeds.com/resources_for_residents.html Objectives, expectations and resources for the rotation can be found at: http://www.macpeds.com/general_pediatrics.html The green book and resources provided above should be reviewed prior to the start of the rotation as they contain information about the day-to-day running of the wards. Sincerely, Moyez Ladhani
3
Introduction to the Division of General Pediatrics
The Division of General Pediatrics is the largest division within the Department of Pediatrics. The division consists of 20 pediatricians. The pediatricians provide consulting services at McMaster Children's Hospital and St. Joseph's Healthcare Hamilton. All pediatricians are affiliated with McMaster University.
General pediatricians work in four teams - teams 1, 2 and 3 at McMaster and team 4 at St. Joseph's Hospital. Team 1 and 2 have up to forty general pediatric ward patients. Team 3 covers twelve Level II neonatal patients and up to six chronic complex pediatric patients. As well, pediatricians on team 1, 2 and 3 provide consults to the Emergency Department, new born nursery, surgical teams, as well as consult requests from the regional hospitals and regional community physicians.
At St. Joseph's Healthcare, we are responsible for up to 18 Level II neonatal patients. In addition we attend deliveries, see consult requests from the newborn nursery and rarely from the emergency room.
The Division of General Pediatrics provides 24/7 on-call coverage at both hospitals. In addition to on-service and on-call work in these hospitals, our group has a commitment to the medical needs of the community. All the General Pediatricians provide follow up and consulting services to children within Hamilton and the surrounding regions. Care provided is based on the best available evidence in a family-centred environment.
CTU 1 and 2 is covered by a core group of pediatricians in addition to pediatricians from our community and St Joes stream. The attending paediatricians rotate through CTU every two weeks starting on Mondays.
The core group:
Dr. Kristen Hallett:
Dr. Hallett joined our Division in 2006. Dr. Hallett practised as a pharmacist prior to becoming a pediatrician. Following her training at McMaster, Dr. Hallett relocated to Owen Sound for seven years. There, she was recognized for detecting the first pediatric cases of E.coli 0157 in the Walkerton Water Crisis. She recently completed her Masters in Health Law at York University Osgoode Hall Law School. Dr. Hallett was the program director for the general pediatric fellowship since its inception in 2009 to 2011.
4
Dr. Andrea Hunter
Dr. Hunter completed both medical school and pediatric residency training at McMaster University. She joined our Division in 2008. Dr. Hunter is a recognized teacher, with significant involvement in medical education at both the undergraduate and postgraduate levels. Her clinical interests include pediatric refugee & immigrant health and global child health. She has recently completed a Diploma in Tropical Medicine and Hygiene in London, UK. Dr. Hunter has been involved in coordinating community-based pediatric refugee/immigrant health clinics in Hamilton since 2004. She is involved in ongoing pediatric education programs in Uganda and Guyana.
Dr. Moyez B. Ladhani
Dr.Ladhani is the Deputy Chief for the Division of General Pediatrics, as well as the Program Director for the Pediatric Residency Program. He also is the chair of the student advisor program for the undergraduate MD program. Dr. Ladhani has been involved in many program development activities and search committees. Currently he chairs numerous committees, his main focus being on medical education and CME activities. He organized and chaired the Practical Pediatrics conference from 2000 to 2011. He has won numerous teaching wards for his excellence in medical education.
5
Dr. Gita Wahi
Dr. Gita Wahi joined our division in 2010 after completing medical school at the University of Western Ontario, Pediatrics Residency at the University of British Columbia, and an Academic General Pediatrics fellowship at the Hospital for Sick Children in Toronto. Dr. Wahi has a clinical and academic interest in the determinants and prevention of childhood obesity. She recently completed a Masters degree in Health Research Methodology from McMaster University. Her educational interests are continuing medical education and she organizes the Divisions weekly rounds and since 2012 co-chairs the annual Practical Pediatrics conference.
Dr. Giuliana Federici
Dr. Federici is a Hamilton “lifer”, born at St Joseph’s Hospital and completing all of her post secondary education and medical training at McMaster University. Prior to pursuing medicine she was a pediatric nurse. She has worked within the Division of General Pediatrics in the city hospitals since 1991 and contributes to under grad and postgraduate education as well as managing a community-based practice. She has been an advisor for many pediatric residents and since 2003 has been Finance Lead for the Division of General Pediatrics. She is a member of the Finance Management Committee in the Department of Pediatrics.
6
Dr. Iman Shbash
Dr Shbash is an assistant clinical professor at McMaster University. She completed her medical school in Tripoli University, Tripoli, Libya. She did her pediatrics training at McMaster University followed by one-year academic pediatric fellowship. Dr. Shbash interest is in medical education and quality assurance.
Others that cover the service:
Dr. Lucy Giglia
Dr. Andrew Latchman
Dr. Kelly Fitzpatrick
Dr. Bojana Babic
Dr. Natalie Orovec
Dr. Kathy Gambarotto
Dr. Sandi Seigel
Clinical Issues:
a) Inpatients
The pediatric inpatient wards at McMaster Children’s Hospital include wards 3B, 3C and 3Y. General Pediatrics is typically the most-responsible physician (MRP) for most admitted pediatric medical patients. There are exceptions and these are evolving. Neurology is MRP for elective overnight video EEG patients and
7
patients initiating ketogenic diet. Endocrinology is MRP for newly diagnosed Type 1 Diabetes and DKA once acidosis is corrected. Cardiology may be MRP for specific cases.
Pediatric subspecialty services include general surgery, neurology, neurosurgery, gastroenterology, allergy and immunology, infectious disease, cardiology, endocrinology, hematology / oncology, genetics, metabolics and urology.
Subspecialists may only recommend treatments and interventions on general pediatric patients. A Most Responsible Team member must agree to and sign any subspecialty recommendation or order.
b) Rounds
Inpatients are admitted to Team 1 and Team 2. A Most Responsible Team member must round and write a progress note on each patient daily. A team member is responsible for keeping patient issues current on the patient list. Lab results may be accessed on the computers equipped via “Meditech” or through any computer using “Citrix”.
Residents and clerks must properly document in the chart. This includes daily notes, completing the details of the facesheet and timely completion of consultations and discharges. Physicians responsible for follow-up of more acute concerns should be contacted by phone, as dictated notes may not be available to the receiving physician in sufficient time.
If a discharge is anticipated over the weekend, the learners should ensure that the facesheet is completed and discharge dictated in advance as a courtesy to the on call person who may not be as familiar with the patient.
c) Call Handover occurs at 4:30. The call team consists of a senior resident, two junior resident and a clinical clerk. The senior resident will assign you patients to see as consults come in. All patients must be reviewed with the senior resident. If the senior resident is busy the cases will be reviewed with the attending. When the senior resident gets a consult they will “eyeball” the patient and write bridging orders. You should make an attempt to be with the senior during this time, as it is a good learning experience. Patient lists must be updated with new patients for the day team before morning handover. Post-call you are required to stay for teaching and are free to go home after the sessions end at 9 am.
d) Documentation/Admission Notes/Progress Notes/Orders
Please see the “green book” for guidelines on this topic.
8
e) Patient Lists
All team inpatients should be added to the daily Patient List. Ongoing or outstanding patient care issues should be added to the list AND relayed verbally during transfer of care, as required.
Information contained on these lists is confidential and therefore must be properly stored and carried. If the list is found off site or in non-confidential areas, you will not be permitted to carry a list.
f) Consultation Requests
General Pediatrics provides consultations to ER, PCCU (Pediatric Critical Care Unit), PACU (Post-Anesthetic Care Unit) and subspecialists as requested. Consultations are prioritized by illness severity. Consults after 1700h are handled by the on-call Senior Pediatric Resident (SPR) who will delegate learners to patients. Any pending consultations and/or admissions not completed at the time of handover must be handed over to the SPR.
Each consult must contain:
- Patient’s name (stamp or sticker) - Date and time (in 2400h clock) on each page - LEGIBLE printed name, signature, training level and pager # - Name of staff with whom case discussed
All resident consultations must be reviewed with a staff or fellow.
g) PACE: Pediatric Assessment of Critical Events
• PACE is the McMaster Children’s Hospital Medical Emergency Consultative Team whose goal is to detect patient’s clinical deterioration before leading to a Code Blue, cardiac arrest or unplanned PCCU admission
• PACE can be activated in several ways:
• Vital sign triggers
• Healthcare provider (HCP) concern about the patient’s status
• Patient or family concern if RN or other HCP cannot be located
• Team should consider PACE consultation for children who have worsening medical status who may require transfer to the ICU
• PACE team consists of the PCCU Resident (Peds 1000 pager), PACE MD, (generally one of the pediatric intensivists or PCCU Fellow); PCCU RN with additional training and pediatric RT.
9
• Activate PACE by calling paging (ext. 76443). Provide patient’s ward and room location. Paging will activate the team members.
• All non-emergent PACE therapies and recommendations should be discussed with the patient’s most responsible team. A member of the patient’s most responsible team (staff, resident, fellow) should be present during the PACE activation. If they are not, then the most responsible house staff should be paged immediately after the PACE team arrives.
Calling in Sick
Please contact your staff supervisor if you cannot come into work by paging them directly, email communication is not acceptable. Please inform the CTU Director of absences > 48 hours.
Evaluations
The staff are encouraged to give midway evaluations. If they have not please ask the staff for feedback midway through your rotation. You should arrange a time to meet your staff for a final face-to-face evaluation. It is preferred that during orientation you make set a time near the end of the rotation to meet to discuss the final evaluation. The staff will fill out an evaluation on One 45 every two weeks. For pediatric residents the staff will also do one Mini-MAS/week, it is your responsibility that these are completed. The staff will also do a hand-over cex every two weeks.
Contacts
Dr. Moyez Ladhani CTU 1 and 2 Director,
Ms. Skye Levely CTU Administrative Assistant, 3N11H [email protected]
Chief Residents [email protected]
10
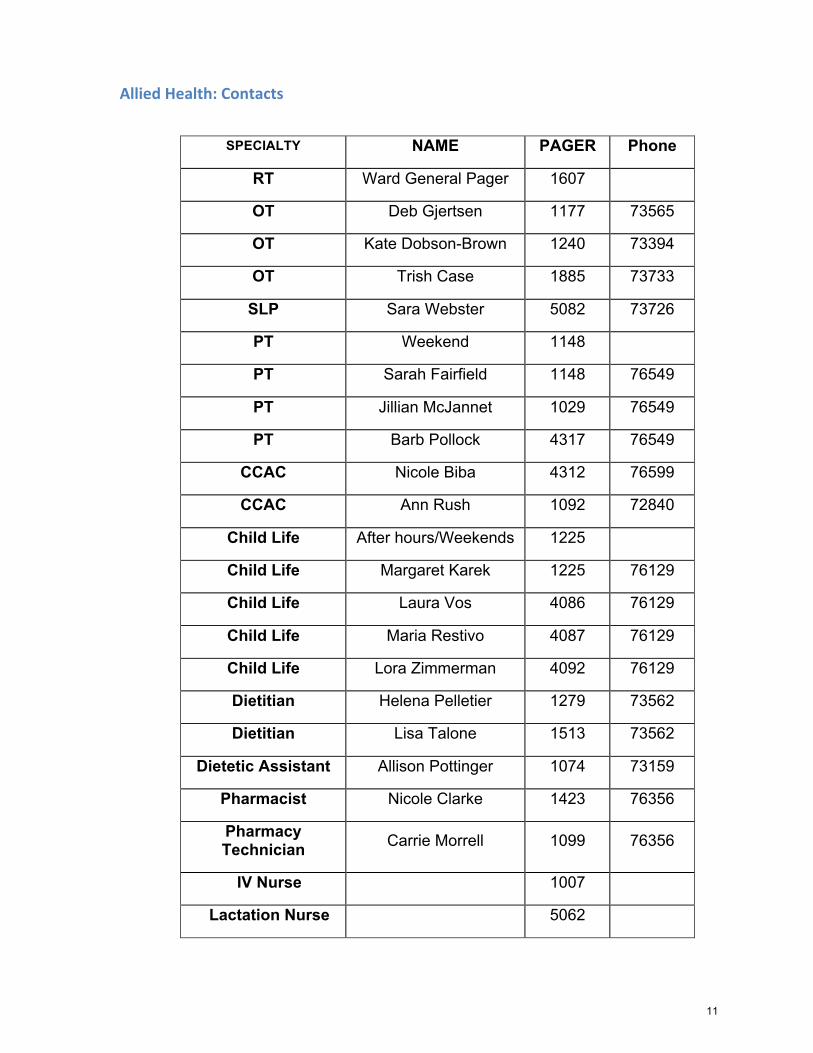
Allied Health: Contacts
SPECIALTY NAME PAGER Phone
RT Ward General Pager 1607
OT Deb Gjertsen 1177 73565
OT Kate Dobson-Brown 1240 73394
OT Trish Case 1885 73733
SLP Sara Webster 5082 73726
PT Weekend 1148
PT Sarah Fairfield 1148 76549
PT Jillian McJannet 1029 76549
PT Barb Pollock 4317 76549
CCAC Nicole Biba 4312 76599
CCAC Ann Rush 1092 72840
Child Life After hours/Weekends 1225
Child Life Margaret Karek 1225 76129
Child Life Laura Vos 4086 76129
Child Life Maria Restivo 4087 76129
Child Life Lora Zimmerman 4092 76129
Dietitian Helena Pelletier 1279 73562
Dietitian Lisa Talone 1513 73562
Dietetic Assistant Allison Pottinger 1074 73159
Pharmacist Nicole Clarke 1423 76356
Pharmacy Technician Carrie Morrell 1099 76356
IV Nurse 1007
Lactation Nurse 5062
11
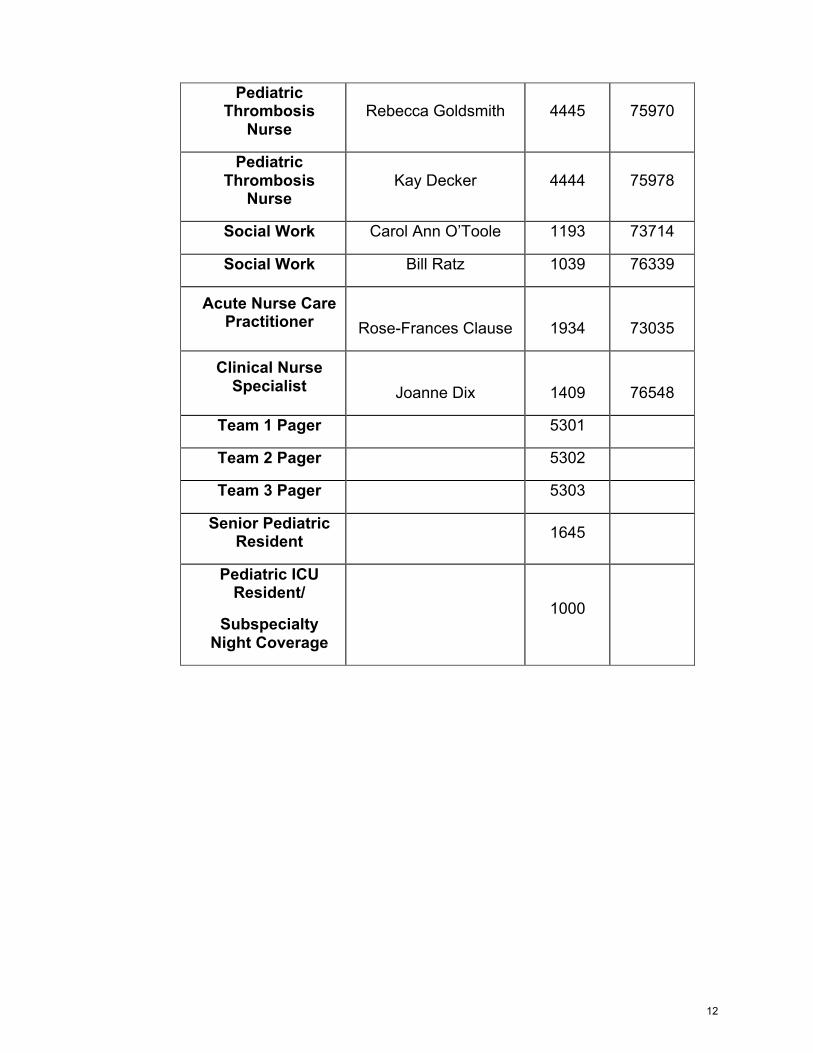
Pediatric Thrombosis
Nurse Rebecca Goldsmith 4445 75970
Pediatric Thrombosis
Nurse Kay Decker 4444 75978
Social Work Carol Ann O’Toole 1193 73714
Social Work Bill Ratz 1039 76339
Acute Nurse Care Practitioner
Rose-Frances Clause
1934
73035
Clinical Nurse Specialist
Joanne Dix
1409
76548
Team 1 Pager 5301
Team 2 Pager 5302
Team 3 Pager 5303
Senior Pediatric Resident 1645
Pediatric ICU Resident/
Subspecialty Night Coverage
1000
12

Division of General Pediatrics CTU 1, CTU 2, Expectations
Handover:
Handover is to take place from 0715-‐0745 hrs. It is therefore important to complete a succinct handover within the allotted 30 minutes. The senior residents will meet with the charge nurses from 3B/3C/3Yto review potential discharges at 9:15am.
Discharge Rounds:
Discharge rounds will be a brief meeting with the attending paediatrician, and Senior Pediatric Residents. Patients that can go home will be identified at this time and discharges for these patients should occur promptly. Discharge planning should always be occurring and the team should discuss patients that could potentially go home the night before. This would then be the time to ensure that if those patients are ready that the patients are discharged.
See Patients:
During this time the team will see their assigned patients. The chart and nursing notes should be reviewed to identify any issues that have arisen over night. The patient should be seen and examined. All lab work and radiological procedures that are pending should be reviewed. The house staff should then come up with a plan for the day and be ready to present that patient during ward rounds. It is not necessary that full notes be written at this time, as there will be time allotted for that later in the day.
Ward Rounds:
During ward rounds the attending paediatrician, with/without Senior Resident, and house staff will round on patients for their team. These are work rounds. All efforts should be made to go bedside to bedside to ensure that all patients are rounded on. Some spontaneous teaching during rounds and at the bedside can occur during this time, however there is allotted time for that later in the day.
Case Based Learning
There will be 10 modules that the learners should complete during their stay on the CTU over a one-‐month period. The senior resident will be responsible to assign the cases to be discussed. The team should read the articles provided and work on the objectives prior to the discussion with the senior and other learners. The attending is encouraged to play a supervisory role during the discussions.
13
Patient Care:
During this time residents will follow through with decisions made during ward rounds. They will finish charting on patients. This is also the time for them to get dictations done and to complete face sheets.
Teaching Sessions:
There are various teaching sessions throughout most days on the CTU. Please refer to the CTU teaching schedule for locations – this will be posted online as well as on the wards.
• Monday morning from 08:00-‐09:00 will be Division of General Paediatric Rounds.
• Mondays from 15:00 to 16:00 – there will be Specialty teaching session. It is the goal during this time to get various specialties to come in and teach around patients that are on the ward.
• Bedside case teaching. The individual teams will do these as time permits. • Tuesdays from 08:00 to 09:00 – Teaching for all learners, except third
Tuesday, which is for Pediatric residents only. • Wednesdays 4th Wednesday of the month will be Peds Cardiology
teaching – “Heart to Heart” which is from 08:00-‐09:00 • Wednesday is Academic Half Day for pediatric residents. • Thursdays from 08:00 to 09:00 – Pediatric Grand Rounds • Thursdays from 15:00 to 16:00: There will be radiology teaching once a
month and possibly other teaching session booked. • Friday 08:00-‐09:00, can be used for the Case Based Learning modules. • Nurses and other health care professionals are welcome to attend these
rounds.
Evaluations:
Time is left in the schedule for evaluations. This would be the time to give residents mid-‐way evaluations, as well as end of rotation evaluations.
Handover 1630 hrs:
Handover will occur to the on-‐call team. Refer to the handover document for further details.
14

Orientation:
At the beginning of each month the attending should meet with their team members to review the objectives, expectation and schedule of the rotation. The senior resident may have valuable input during this time.
Multi-‐Disciplinary Rounds:
Team 1 and 2 will occur on Tuesdays. Team 1 will be from 1300-‐1330; Team 2 will be from 1330-‐1400.
15
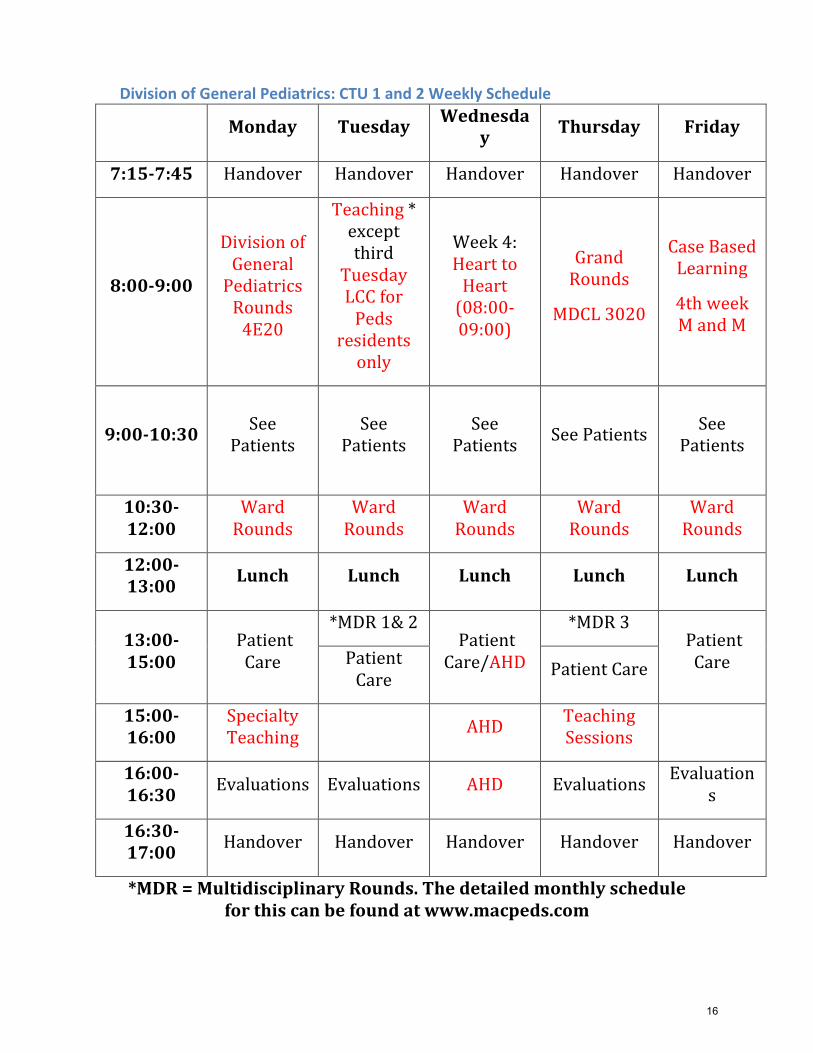
Division of General Pediatrics: CTU 1 and 2 Weekly Schedule
Monday Tuesday Wednesday Thursday Friday
7:15-‐7:45 Handover Handover Handover Handover Handover
8:00-‐9:00
Division of General Pediatrics Rounds 4E20
Teaching * except third
Tuesday LCC for Peds
residents only
Week 4: Heart to Heart (08:00-‐09:00)
Grand Rounds
MDCL 3020
Case Based Learning
4th week M and M
9:00-‐10:30 See Patients
See Patients
See Patients See Patients See
Patients
10:30-‐12:00
Ward Rounds
Ward Rounds
Ward Rounds
Ward Rounds
Ward Rounds
12:00-‐13:00 Lunch Lunch Lunch Lunch Lunch
13:00-‐15:00
Patient Care
*MDR 1& 2 Patient Care/AHD
*MDR 3 Patient Care Patient
Care Patient Care
15:00-‐16:00
Specialty Teaching AHD Teaching
Sessions
16:00-‐16:30 Evaluations Evaluations AHD Evaluations Evaluation
s
16:30-‐17:00 Handover Handover Handover Handover Handover
*MDR = Multidisciplinary Rounds. The detailed monthly schedule for this can be found at www.macpeds.com
16
CTU 1 & 2 Faculty Expectations
Staff Handover Weekdays: Staff for Team 1 and 2 will do handover before 8 am or after 9 pm by a previously agreed method.
Staff Handover Weekends: Staff to arrive at 0800 hrs. and handover will occur on 3C either in person or by phone.
Service Handover: Will occur on Monday morning in person after Division of General Pediatric Rounds.
Daily Schedule for Weekdays:
• Staff for Team 1 & Team 2 are expected to be present within the hospital from 0800-‐1700 hrs.
• At 0900 hrs. the staff and senior resident will meet to decide on discharges. • At 0915 hrs. the staff or senior resident will attend the huddle to discuss
discharges with the charge nurses • Admissions to the teams will occur as follows; from 0800 to 1700 hrs.
admissions on even days will go to Team 2 and on odd days will go to Team1. After 1700 hrs. admissions throughout the night would alternate between Team 1 and Team 2. It will be easiest to admit to the team of the admitting clerk or resident. The senior resident will need to balance the admissions to keep the numbers even on both teams.
Orientation:
• All learners will receive a welcome email from the General Pediatric Administrative staff one week prior to their rotation starting.
• Learners will be expected to arrive for handover at 0715 hrs. at the start of their rotation.
• The attending will meet the senior resident at 0900 hrs. to review objectives and sign the learning contract.
• The attending will meet the junior resident and other learners at 0930 hrs. to review objectives and sign the learning contract.
• Orientation will be a shared responsibility of the faculty and SPR. Use the orientation checklist as a guide.
This would also be an opportune time to discuss the residents’ vacations, half day, make arrangements for mini MAS, and set time to discuss the mid-‐rotation and end-‐rotation evaluations.
17
Evaluations:
• CTU staff are expected to do mid-‐rotation feedback with each learner informally after each week of service. If there are concerns with any of the residents’ performance, the evaluation must be in writing. An evaluation is available on WebEval or contact Dr. Ladhani/Shirley Ferguson, who can send you a form.
• After each 2-‐week block, the staff is to give formal feedback in writing to all learners and face-‐to-‐face feedback.
• A mini-‐MAS for every pediatric resident must occur once per week (it is the resident’s responsibility to plan ahead to ensure that this is completed).
• The Clerks need 1 mini-‐CEX during their ward rotation from the attending. • All mini-‐MASs should be an observed clinical encounter. • Each attending will do one handover mini-‐CEX during a 2-‐week block. • The handover mini CEX is an observation of the evening handover by the Senior
and Junior Residents. • There is a provider and recipient form. • http://www.macpeds.com/documents/HandoffEducationprovider.pdf • http://www.macpeds.com/documents/Handoffcexrecepient.pdf
Teaching:
• CBL cases have been developed for the CTU 1 and 2 rotation • These will comprise of a case, objectives and articles that will be available to all
learners ahead of time. • The faculty/SPR will facilitate when these cases will be discussed. • A minimum of 5 cases need to be worked through by all learners in a 2-‐week
period. • There will be teaching on Monday and Thursdays 1500-‐1600 hrs. • All residents will have morning teaching on Monday, Tuesday, Wednesday and
Thursday 0800-‐0900 hrs. • Friday morning 0800-‐0900 will be used for the case based teaching modules.
Rounding:
• It is highly recommended that rounds be conducted in a walk around fashion. • The Senior Resident is to act as a Junior Attending with appropriate supervision. • At minimum each patient should be seen by all learners at least once per week.
18
19
Orientation Checklist for Teams 1 and 2 (What to review with new learners)
q Welcome to Pediatrics! q Roles of Peds Sr., Residents, Clerks on ward – see outlined expectations on website q Review Goals and Objectives q Responsibilities: 3B, 3C, 3Y, ER q Team 1, Team 2 Attending, Sr. Resident, Peds Resident, Residents, Clerks q Review website and reading list with learners q Make a list of contact information (pagers) and post on all wards each week! q Discuss the issue of confidentiality, talking about patients in public areas, leaving
sheets lying around…
q Daily schedule: refer to green book/website q 07:15 Handover q 08:00 Teaching – Review Teaching schedule for topic and location q 09:00 “Pre Round” – see patients, check progress overnight, review labs, etc. q 10:30 Team rounds with Sr. Resident and/or Staff q 13:00-15:00 Patient care - Write notes, orders, arrange investigations, follow-up labs,
multidisciplinary rounds, etc. q 15:00-16:00 Teaching - see Teaching schedule for topic and location q 16:00pm Update Team Lists for evening handover, check labs etc. q 16:30pm Handover
q ER consult responsibilities q Senior will “Eye-ball” patient before allowing clerk/ resident to take history/examine
patient, clerk/resident should be present q Write full admission note, orders for labs/investigations q Dictate a full note for all consults q Write admission orders, and notify ward resident of any children admitted q Patient is still your responsibility while in ER – ensure orders have been carried out,
and reassess frequently… q Add patients to Team List
q Daily progress notes q Outline chronic + active issues q Full ‘summary note’ on Thursdays, anticipating weekend coverage q Arrange investigations as early as possible in morning, and follow results closely q Keep ‘Patient Problem List’ updated q Update Team List of patients with active issues, management plans
q Consult requests q Fill out green sheet for each consult, request, once approved by general peds
attending q You must notify physician directly for all subspecialty consultations (including
anaesthesia consults for sedated procedures) q Do not consult a service unless approved by you staff person
20
q Discharge procedures q Complete all discharges in the morning prior to rounds if possible. q Check with staff before discharging any pediatric patient q Write discharge orders, scripts, follow-up appointment arrangements q Fill out ‘face sheet’ with all possible diagnoses, etc, give a copy to parents q Dictate discharge summary, write ID# on facesheet
q On call q Responsibilities on-call (team 1,2,3 Subspec, PICU etc), review 5301, 5302, 5303 q Location of call rooms, greens, lounge q Call switches q Hand over patients before leaving post-call, expected to stay until teaching done in
morning when post-call,
q Other q Arrange investigations as early as possible in morning, and follow results closely q Computer passwords etc.-– Email Skye with Citrix username to get access to patient
lists q Brief orientation to Meditech, PACS, etc q Show them where Team Lists are on each computer Review www.macpeds.com,
and also let house staff know about the general pediatric articles on line.
q TOUR q Show each of the wards (3B, 3C, 3Y)
q White boards of patient lists q Charts q New forms: progress notes, orders, radiology reqs, etc etc q Discharged charts (in drawers behind desk clerk)
q ER q Call room area: lounge, call rooms, greens, q Other (if you have time)
q Radiology q PICU
q Please emphasize: q Put contact person beside each patient with pager number – each day! q Hand over all your patients before leaving for half-day, post call etc q Please arrive for handover on time and prepared with an updated patient list… finish
notes, dictations as necessary after handing over at 4:30pm q Dictate discharge summaries promptly – charts disappear in <48hrs! q Split up patients for optimal learning among the team members – assign a resident to
supervise clerk patients too.
q We are all here to learn and have fun!
21
Patient Care/Charting
Admissions
• Write full admission orders (include MRP on-call, transfer care to ‘Team 1/Team 2’ in a.m.)
• Ensure history & physical is documented on chart
Charting
• Admission note should include complete history & physical, assessment & plan
• Progress notes should be written daily on every patient • All complex patients admitted to the hospital and residing in
the hospital for over a week should have a summary of interval progress documented every Thursday by the resident or assigned learner. This should consist of a brief update of events of the week, significant physical findings, investigation results, and care provided during the preceding week. This will facilitate the provision of care over the weekend as well as help keep the numerous sub-specialists involved with each such patient updated. Further this weekly summary will be a great help in dictating the final discharge summary.
• Off-service notes (at the end of a month/rotation) are also helpful and expected.
• All patient care meetings such as those conducted with parents or multispecialty meetings should be documented in the chart by the learner assigned to the case, with a summary of the discussion.
Patient Referrals
• All referrals to sub-specialists will take place with the explicit consent and request of the attending rather than a direct referral from the resident to the sub-specialists. The referral request will specify the question for which subspecialty input is required. Parents need to be aware of the request for subspecialty consult, especially involving Mental Health / Adolescent Medicine. The urgency of the consult should be relayed to the sub-specialist being called. The MRP should be fully aware of the patient’s details, as should the Resident / Learner calling the sub-specialist.
22
Transferring patients
• When transferring patients, please verbally notify the resident on the new service (staff to staff handover should also take place independently).
• Transfer orders to general pediatrics, Level 2 Nursery are expected.
• Dictate transfer summary and write brief transfer summary in chart.
Discharging patients
• Dictate a discharge summary for every pediatric patient. This should include dates of admission/discharge, admission/discharge diagnosis, discharge medications, follow-up plans, brief history & physical, pertinent investigation results and summary of course in hospital. See templates for general peds, Level II nursery, NICU, etc.
• Complete face sheet prior to patient leaving hospital – this will be faxed to family physician’s office at the time of discharge. Face sheet completion prior to discharge is the responsibility of the learner. The face-sheet will be completed in detail, at the time of discharge. Information on this will include salient course in hospital, diagnosis at discharge, and follow up plan.
• Complete any prescriptions, CCAC requests, and other forms prior to discharge.
23
Role of the Clinical Clerk Responsibilities
• Primarily responsible for caring for their assigned patients on the ward. • Acts as primary contact person for their assigned patients. • Completes discharge summaries and arranges follow up for assigned patients. • Brings concerns/questions to the Junior/ Senior Pediatric Resident/Ward
Attending. • Sees patients in the ER with the Senior Pediatric Resident or Attending.
Daily Schedule
07:15 Handover
08:00 Teaching – Review Teaching schedule for topic and location
09:00 “Pre Round” – Examine patients, check progress overnight, review labs, etc.
10:30-12:00 Team rounds with Sr. Resident and/or Staff
12:00-13:00 Lunch
13:00-15:00 Patient care
• Wrap up discussion of new and outstanding issues with attending/SPR. • Write progress notes; arrange investigations and consults, follow-up labs,
multidisciplinary rounds, etc. • Complete daily progress notes and discharge summaries. • Resident-led teaching sessions and bedside teaching. • Discharges for the next day planned and arranged with specific criteria.
15:00-16:00 Teaching - see Teaching schedule for topic and location
16:00pm Update Team Lists for evening handover, check labs etc.
16:30pm Handover
Call and Post Call
• Will do call at McMaster • Will see consults from ER, in-‐patient services or transfers to Level 2 Nursery • Will update patient lists before morning handover. • Will attend morning handover and teaching post-‐call (will leave at
approximately 09:00 on post call days.) • Will hand their patients over to a team member (Clinical Clerk, Junior
resident or Senior Pediatric Resident) prior to going home post call. • Will cover the patients of fellow Clinical Clerks when they are post call.
Discharge Planning
• Each morning, the team will discharge patients ready for discharge early if discharge criteria are met.
• Discharge planning begins at the time of admission and is an ongoing process.
24
Role of the Family Practice Resident/BCT Responsibilities
• Primarily responsible for running the ward with other Residents and to learn ward management skills.
• Helps to delegate patients to and supervise Clinical Clerks. • Helps co-‐ordinate activities of the ward (test results, examining patients,
discharge planning etc) • Brings concerns/questions to the Senior Pediatric Resident/Ward Attending.
Daily Schedule
07:15 Handover
08:00 Teaching – Review Teaching schedule for topic and location
09:00 “Pre Round” – Examine patients, check progress overnight, review labs, etc.
10:30-12:00 Team rounds with Sr. Resident and/or Staff
12:00-13:00 Lunch
13:00-15:00 Patient care
• Wrap up discussion of new and outstanding issues with attending/SPR. • Write progress notes; arrange investigations and consults, follow-up labs,
multidisciplinary rounds, etc. • Complete daily progress notes and discharge summaries. • Resident-led teaching sessions and bedside teaching. • Discharges for the next day planned and arranged with specific criteria.
15:00-16:00 Teaching - see Teaching schedule for topic and location
16:00pm Update Team Lists for evening handover, check labs etc.
16:30pm Handover
Call and Post Call
• Will do call at McMaster in a float model, junior float will be scheduled in the master rotational schedule, residents will have an opportunity to review and request changes to the rotational schedule before it is finalized. After the schedule is locked in if the resident chooses to take a vacation, they must find a qualified replacement.
• Will see consults from ER, in-‐patient services or transfers to Level 2 Nursery • Will update patient lists before morning handover. • Will have encounter card completed by senior resident for every call. • Will attend morning handover and teaching post-‐call (will leave at approx.
09:00 on post call days.) • Will hand their patients over to a team member (Junior resident or Senior
Pediatric Resident) prior to going home post call.
25
• Will cover the patients of fellow residents when they are post call.
Vacation
• Residents may take 1 week of vacation (5 days) per 4-‐week rotation on the inpatient CTU.
• More than one Family Practice Resident/BCT on the same team may not take vacation at the same time.
• All requests need to be approved by the CTU administrator and chief residents on Medportal prior to staring the rotation.
Discharge Planning
• Each morning patients ready for discharge will be discharged early by the resident if discharge criteria are met.
• Discharge planning begins at the time of admission and is an ongoing process.
26
Role of the Junior Pediatric Resident Responsibilities
• Primarily responsible for running the ward with other Residents and to learn ward management skills.
• Delegates patients to BCT’s, Family Practice Residents and Clinical Clerks. • Co-‐ordinates activities of the ward (test results, examining patients,
discharge planning etc) • Brings concerns/questions to the Senior Pediatric Resident/Ward Attending.
Daily Schedule
07:15 Handover
08:00 Teaching – Review Teaching schedule for topic and location
09:00 “Pre Round” – Examine patients, check progress overnight, review labs, etc.
10:30-12:00 Team rounds with Sr. Resident and/or Staff
12:00-13:00 Lunch
13:00-15:00 Patient care
• Wrap up discussion of new and outstanding issues with attending/SPR. • Write progress notes; arrange investigations and consults, follow-up labs,
multidisciplinary rounds, etc. • Complete daily progress notes and discharge summaries. • Resident-led teaching sessions and bedside teaching. • Discharges for the next day planned and arranged with specific criteria.
15:00-16:00 Teaching - see Teaching schedule for topic and location
16:00pm Update Team Lists for evening handover, check labs etc.
16:30pm Handover
Call and Post Call
• Will do call at McMaster in a float model. Junior float will be scheduled in the master rotational schedule, residents will have an opportunity to review and request changes to the rotational schedule before it is finalized. After the schedule is locked in if the resident chooses to take a vacation, they must find a qualified replacement.
• Will see consults from ER, in-‐patient services or transfers to Level 2 Nursery • Will update patient lists before morning handover. • Will attend morning handover and teaching post-‐call (will leave at approx.
09:00 on post call days.) • Will hand their patients over to a team member (Junior resident or Senior
Pediatric Resident) prior to going home post call. • Will cover the patients of fellow residents when they are post call.
27
Vacation
• Residents may take 1 week of vacation (5 days) per 4-‐week rotation on the inpatient CTU.
• Senior Pediatric Resident and Junior Pediatric Resident may not take vacation at the same time
• All requests need to be approved by the CTU administrator and chief residents on Medportal prior to staring the rotation.
Discharge Planning
• Each morning patients ready for discharge will be discharged early by the resident if discharge criteria are met.
• Discharge planning begins at the time of admission and is an ongoing process.
28
Role of the Junior Pediatric Resident Responsibilities
• Primarily responsible for running the ward with other Residents and to learn ward management skills.
• Delegates patients to BCT’s, Family Practice Residents and Clinical Clerks. • Co-‐ordinates activities of the ward (test results, examining patients,
discharge planning etc) • Brings concerns/questions to the Senior Pediatric Resident/Ward Attending.
Daily Schedule
07:15 Handover
08:00 Teaching – Review Teaching schedule for topic and location
09:00 “Pre Round” – Examine patients, check progress overnight, review labs, etc.
10:30-12:00 Team rounds with Sr. Resident and/or Staff
12:00-13:00 Lunch
13:00-15:00 Patient care
• Wrap up discussion of new and outstanding issues with attending/SPR. • Write progress notes; arrange investigations and consults, follow-up labs,
multidisciplinary rounds, etc. • Complete daily progress notes and discharge summaries. • Resident-led teaching sessions and bedside teaching. • Discharges for the next day planned and arranged with specific criteria.
15:00-16:00 Teaching - see Teaching schedule for topic and location
16:00pm Update Team Lists for evening handover, check labs etc.
16:30pm Handover
Call and Post Call
• Will do call at McMaster in a float model. Junior float will be scheduled in the master rotational schedule, residents will have an opportunity to review and request changes to the rotational schedule before it is finalized. After the schedule is locked in if the resident chooses to take a vacation, they must find a qualified replacement.
• Will see consults from ER, in-‐patient services or transfers to Level 2 Nursery • Will update patient lists before morning handover. • Will attend morning handover and teaching post-‐call (will leave at approx.
09:00 on post call days.) • Will hand their patients over to a team member (Junior resident or Senior
Pediatric Resident) prior to going home post call. • Will cover the patients of fellow residents when they are post call.
29
Vacation
• Residents may take 1 week of vacation (5 days) per 4-‐week rotation on the inpatient CTU.
• Senior Pediatric Resident and Junior Pediatric Resident may not take vacation at the same time
• All requests need to be approved by the CTU administrator and chief residents on Medportal prior to staring the rotation.
Discharge Planning
• Each morning patients ready for discharge will be discharged early by the resident if discharge criteria are met.
• Discharge planning begins at the time of admission and is an ongoing process.
30
Roles and Responsibilities of the Senior Pediatrics Resident on CTU
CanMEDS Roles: Medical Expert, Scholar, Manager, Communicator, Collaborator, Advocate and Professional
Responsibilities
Will be assigned to ONE Team at the start of their rotation for the duration of their rotation, for which they are subsequently responsible for the following:
• Helps to co-‐ordinate prompt discharge of patients in the morning. • Assigns patients to the learners on the team. • Ensures all patients are seen and proper documentation done by
learners on all charts. • Ensures all labs and referrals have been followed up by learners on all
patients. • Junior Consultant role on morning rounds on assigned team, will do
walk around rounds on all patients with the team. • Reports to attending after rounds on all patients (this needs to be
decided on at the start of the rotation -‐ the attending is encouraged to be available and in the building, but does not necessarily need to be present on morning rounds; however some attendings may prefer to be physically present during rounds in which case they should play a supervisory role).
• Acts as first contact for Junior Residents and other learners. • Brings concerns/questions about the rotation and learners to the
ward Attending. • Provides teaching at the bedside and sit-‐down teaching to learners on
the team. • Ensures the team is present at all scheduled ward teaching sessions,
unless a team member is required to assess a consult/transfer in a timely manner.
• Ensures brief afternoon rounds are done to follow up on “to do “list and also to re-‐assess patients for possible discharge.
• Attends and lead the discussions at Multi-‐Disciplinary rounds. • From 10:00 am to 12:00pm, the attending will take calls from the ER
to allow the senior to conduct rounds. If the senior receives an ER call during that time, this should be directed to the attending.
• When there is a Day Float resident, works collaboratively with the resident. Please refer to Day Float guide.
• Responsible for referrals from the ER • From 08:00 to 16:30, patients will be admitted as follows: Odd
days: Team 1, Even Days: Team 2, corresponding SPR to carry pager.
31
• From 16:30 to 08:00, the admission should alter between teams, try and admit under the team of the junior learner. The SPR will manage the admissions to ensure the teams remain relatively balanced. Further balancing of numbers can also occur at handover.
• The order should be written as: Admit to Team___, under Dr. (on call pediatrician), transfer care to Dr. (attending pediatrician of the team admitted to) in morning.
Orientation
1. Introduce yourself and your role as Team Senior to the charge nurse, house-‐staff & team attendings and ensure their name, pager number and the team that they are responsible for is posted on White boards on 3B, 3Y & 3C.
2. Orient new residents when starting at MUMC, review the teaching and daily ward schedule, review team expectations (use the orientation checklist.)
3. Assign clinical clerks to their teams if not already done. 4. Review www.macpeds.com, and also let house staff know about the general
pediatric articles on line. 5. Ensure the pager system is reviewed with the team: 5301 and 5302 should
be carried by the CTU Junior. 6. Please emphasize that the Junior and off-‐service residents are also
responsible for: a. Supervising the clerks. b. Following up on any patients they admitted from the ER. c. Writing daily progress notes. d. Writing a weekly summary note every Thursday clearly outlining
treatment plans for each patient. e. Writing a detailed off-‐service note for all patients prior to completion
of the rotation. f. Dictating BOTH admission and discharge summaries. g. Ensuring the front page in the chart is filled out at discharge. h. Handing over patients to another resident or clerk when post-‐call or
leaving for half-‐day.
Morning Handover
1. Ensure on time attendance of all learners. 2. Ensure handover begins on time (7:15 am) with brief discussion of overnight
admissions and pertinent issues that arose overnight. 3. Meet with the charge nurses from 3B, 3Y and 3C after rounds at 9:15
(huddle) to discuss any possible discharges. 4. Ensure learners are at their teaching session on time at 8 am. 5. Ensure each team re-‐types their team list by an appropriate time with the
name of the responsible resident or clerk beside each patient. 6. Ensure the team communication tasks are completed.
32
7. Ensure 5301/5302 pager system is explained to the team. 8. Ensure complex and chronic patients are cared for by residents instead of
clerks, to improve continuity of care.
Education
1. Ensure learners attend all ward-‐teaching sessions on time. 2. Ensure teaching sessions have been assigned to the house staff for the case
based learning. 3. Please refer to the ward-‐teaching schedule for details. 4. Provide bedside and case based teaching to learners based on the cases on
teams. 5. Provide feedback to learners regularly on their progress. 6. Provide a list of radiology cases to the radiologist a few days in advance of
the scheduled radiology teaching sessions.
Call and Post Call
• SPR float will be scheduled in the master rotational schedule, residents will have an opportunity to review and request changes to the rotational schedule before it is finalized. After the schedule is locked in if the resident chooses to take a vacation, they must find a qualified replacement.
Vacation
• Residents may take 1 week of vacation (5 days) per 4-‐week rotation on the inpatient CTU.
• Junior & Senior pediatrics residents should avoid taking vacation leave at the same time if possible.
• If a Senior resident takes vacation/professional leave, it is the responsibility of the staff-‐attending for their team to assume the SPR CTU role during their absence, including running rounds, being available to house-‐staff for questions, following-‐up on investigations in the afternoon, ensuring documentation, etc.
• All requests need to be approved by Division of General Pediatrics Office prior to starting the rotation as per PARO.
Discharge Planning
• Each morning, patients ready for discharge will be discharged early by the Residents if discharge criteria are met
• Discharges for the next day will be decided upon the afternoon before and all arrangements made (e.g. follow up appointments and outpatient investigations).
• Patients should be re-‐assessed in the afternoon for possible discharge.
33
Administrative
The senior resident should ensure efficient workings of the teams. They should provide back up and support to the junior learners. They should demonstrate and teach time management to the junior learners. They should be at handover at 7:15 sharp to ensure these rounds are efficiently run. They need to attend and be prepared to run multi-‐disciplinary rounds weekly.
1645
If both residents are present on CTU, the senior resident on the admitting team will carry 1645 for the day. From 10am until noon, the ER staff will page the CTU staff on service directly for consults. If the ER pages 1645 during that time, the senior can make their staff aware, who can return the call to the ER.
If there is only 1 senior resident on CTU (Due to either vacation, sick day, or post call days) 1645 will be held as follows:
If the senior on CTU is on the accepting team, they will carry 1645 as above.
If the senior on CTU is not on the accepting team, the senior resident present will carry 1645 for the day. The staff on the team on intake will accept ER consults on their personal pager from 10am until noon and will triage consults as needed. If during rounds the senior gets pages from ER, they can let the staff on intake know, and they can call the ER back. The senior resident present will cover 1645 for the afternoon. The full consult will be given to a junior resident to see. The senior will review the completed consult with the accepting staff physician.
The senior resident who was absent will not need to repay the covering senior resident.
Please refer to Day Float guide, when there is a Day Float resident scheduled.
The Day Float resident will not be responsible to cover teams if the CTU senior takes vacation.
34

Role of the General Pediatric Fellow
General Pediatric Fellow is expected to function as a junior consultant. This position of supervision and leadership is learned and earned. Triaging, time-management and communication are essential skills to be developed over the course of the fellowship. The staff pediatrician expects and relies on the fellow to have accurate and current information on patients under their care.
The McMaster Pediatric Residency Program provides a gradual approach to supervision. Clinical Clerks and Junior Pediatric Residents review patients directly with the Senior Pediatric Resident. The Senior Pediatric Resident (SPR) is then expected to present a concise summary of the patient to the General Pediatric Fellow or Supervising Staff. Depending on patient volume and/or acuity, the fellow may be required to review patients directly with junior house staff and/or see the patient directly. The fellow must have an overview of all patient issues on the clinical teaching unit (CTU). The fellow is expected to assume and/or assist with the care of sicker children admitted to their team.
On nights and weekends with less available house staff, the fellow is expected to take on the additional responsibility of ensuring that more junior team members provide optimal patient care. Patient transfers between subspecialists, NICU or PCCU require staff/fellow to staff/fellow handover. Residents will handover to residents. Residents review and confirm the need for subspecialist consultation with the fellow and/or staff.
General Pediatric Fellow will be expected to directly examine patients. Fellow will need to write and/or sign progress notes at sufficient intervals to ensure oversight of care provided by others, to summarize pertinent patient issues, and to be able to evaluate resident notes and professionalism. These skills remain integral to professionalism and the practice of medicine.
Academically, General Pediatric Fellows are expected to attend and contribute to the ward teaching and education, including: Practice Parameter Rounds, Morbidity and Mortality Rounds, PICU (Mock Code) Rounds and ward teaching, when on service.
35
Some Practical Tips on Being a Senior Pediatric Resident at McMaster
This document is meant to provide practical information to help junior pediatric residents’ transition to the Senior pediatric resident role. Challenges special to the SPR role include supervising junior residents and clinical clerks and delegating duties appropriately. As a manager and collaborating with ER and PICU staff, the SPR facilitates getting patients where they need to go. Being a medical expert is an important role as an SPR, but specific patient management is not the focus of this discussion. Experience will afford you your own style as an SPR, but there are some guidelines that every SPR should abide by, for patient safety. No rules apply for every scenario, but some general trends arise that are described here.
Consults to ER
What information do I need to get from the referring emergency physician?
Get the patient’s name and location (locating your patient is often more difficult than you would imagine) as well as the name of the ER physician. Ask for vitals, general appearance, investigation and treatment done by the ER physician (e.g. back to back to back ventolins). You can also ask the emergency physician: “What are you most concerned about?” If the patient is unstable and you cannot go to the ER immediately, you can ask ER physician if they can watch the patient for 20 minutes and/or order some labs.
Should this consult really go to Peds? What if a consult seems inappropriate?
You should not refuse any consult, no matter how simplistic it seems. If you think a consult is inappropriate or can be seen on an outpatient basis, run the referral by your staff person. Some consults however require urgent management by another service (e.g. testis torsion) and needs to be redirected appropriately.
Note that we admit some complex patients under a different service (e.g. surgery) for whom pediatrics will be the primary care service (e.g. the “quarterback”). G tubes go to surgery; G-J tubes go to general pediatrics (interventional radiology is required).
If you are asked to see a patient without an official consult, please ask for an official consult. Every patient we see is on a consultation basis.
If you are ever unsure about any aspect of a consult (referral, assessment, management) then please ask your staff.
The SPR should redirect all outside calls (parent or physician), to the staff.
How do I deal with ER consults?
You must at least “eyeball” every patient. (Try and take a learner down when assessing the patient). This entails assessing general appearance, vitals and treatment to date. If there is any uncertainty regarding the patient’s stability, take whatever action is necessary immediately and ask for assistant ER doc or call PACE (call your on call staff to keep them in the loop and also for assistance. If the patient is clearly stable, write bridging orders (preferably with the learner present), delegate the consult to a clerk or resident and advise him or her of how long it should take (e.g. 1 hour is reasonable for most consults).
You may advise your learner on how to approach the history/ physical and what to look for on their assessment. It is helpful to ask a clerk or junior something like, “Have you seen many kids
36
with bronchiolitis?” to get an idea of how much direction they need before sending them into action. It also helps learners know that you are in touch with their learning needs. Triage patients appropriately, it is not a good learning experience to have the clinic clerk see the complex chronic patient.
Here is one of our Senior resident’s take on ER consults:
“Take the info from the consult, check the vitals and see the child for yourself. ALWAYS check vitals and then recheck HR and RR yourself. If the child is in any distress - you must stabilize them yourself (i.e. get the insulin, fluids and labs ordered in DKA, check neuro status and- if you’re happy- get someone to do the whole consult while you keep an eye on them intermittently). If the child is not clearly well (nor acutely sick), ask some pointed questions to determine the acuity of the situation.
Then decide who is most appropriate to see the consult (i.e. Peds Jr for more acute stuff and clerk for consults that can take an hour and it doesn't matter). Do all the consults you get. It's not our role to filter them (unless it’s a life threatening mistake i.e. bowel perforation and surgery hasn't been called, then consider calling surgery yourself and offer to do the consult anyway). If there are recurrent inappropriate consults from the same person, mention it to staff - it's their role to discuss staff-staff. It is our role to keep the patients safe. We shouldn't get mixed up in consult politics.
If a patient is crashing (or might), call PACE without delay. If they are stable, but have a bad story that makes you worry they might crash, call your senior/staff or ER doc for help. This is not the time to prove yourself or be a hero. What is best for the patient always comes first. While you wait for help, Stay calm and remember your A, B, C's, fluid boluses are good (unless they're obviously cardiac or fluid overloaded), think about STAT labs (CBC, cx, lytes, urea, Cr, glu, gas, lactate +/- more) and whether they need STAT meds (lorazepam, antibiotics, steroid, ventolin, epi). Remember that help is on the way and you are not alone.
Consider asking nursing to call PACE while you stabilize. Delegate tasks to others, so you can concentrate on decision-making.
When do I call a code (5555)?
If a patient is crashing (i.e. desaturating, apneic, symptomatic tachy/bradycardia, etc.) call a code (i.e. shout “call a code blue” or pick up the phone and dial 5555).
When do I consider paging PICU (1000)?
If you think a patient needs to go to the ICU, Call PACE.
An unofficial, non evidence based, SPR opinion of when a patient needs ICU:
- FiO2 greater than 40%
- two doses of lorazepam and still possible seizing
- more than 2 boluses of 20cc/kg crystalloid with no obvious improvement
Remember the other people in house: PICU resident (+/- fellow, staff), PACE, ER physician, anesthesia…
37
When I’m in the ER seeing patients, when do I call the staff?
• The on-call attending is expected to review all the patients seen from 1700-2300 hrs. in person, after each consult not clustered. You must contact the attending after each consult.
• All consults after 2300 hrs will be discussed in person in clusters of no more than three. The residents should call the attending after a cohort of three consults; the attending shall review the consults over the phone or in person.
• The attending will determine the detail of review depending on the level of training of the SPR.
• The SPR will be reminded that if at any time they have concerns they should not hesitate to call the on-call pediatrician.
What if the patient does not need to be admitted but needs outpatient follow up?
You can refer the patient to the PERC clinic or senior resident clinic as follow up. Alternatively, the pediatrician you are working with at that moment may arrange to see the patient either in their outpatient office or in the hospital if they’re on service.
What do I do in a trauma fan out (what is a trauma fan out)?
A “trauma fan out” is called by the ER physician in the case of trauma of sufficient severity to require the trauma team. The PICU resident, the trauma team leader (a staff, not necessarily PICU staff), the general surgery resident, and the anesthesia resident get paged. The SPR does not get paged for a trauma. Usually the role of trauma team leader (TTL) is assigned to the ER physician/ surgeon/ PCCU physician. The ER physician always assumes the role of TTL until the assigned TTL arrives on scene.
Teaching, Providing Feedback, and Debriefing Encounters with Juniors and Clerks
How should I provide positive feedback to clerks and juniors?
Try to give some specific positive feedback, such as, “It was great that you took a good social history because it will impact whether or not we can send this kid home,” or “I liked that you included a broad differential and I agree that this kid needs antibiotics.” Being a clerk or junior resident is psychologically tough and positive feedback is not only appreciated but is arguably essential.
How should I provide negative feedback to clerks and juniors?
Criticism is always difficult to bear so it should at least be constructive. Acknowledge that many situations are new for clerks and residents and it’s OK not to know everything. Try to fill in the gaps in the history, physical and encourage any attempts to formulate a differential and plan. Try to be specific in your criticism and provide some suggestions on how to improve. For example… ‘you take a long time to complete a consult. Before seeing the patient, spend 1-2 minutes considering what details would be pertinent on history/physical as this will save you time when assessing your patient’.
38
How do I approach teaching clerks/juniors/FM/BCT?
A useful teaching session can take place in 5 minutes and you don’t need to be an expert to execute one. It can be helpful to ask a clerk or junior a question like, “Do you know the risk factors for sepsis in a neonate?” especially when it relates to a case in front of you. If they already knew the answer, it helps their morale, and if they didn’t, it’s a digestible learning point. It’s also good for the senior to review, and you often learn something new, or identify gaps in your knowledge when the junior turns the tables on you…
How should I debrief encounters with clerks and juniors?
After finishing a case, it is useful for learners when the senior asks, “Did you have any questions about that case?” If the learner asks a question you don’t know the answer to (that’s OK) you might say something like, “I don’t know, I’ll have to look that up or ask the staff,” not a bad way demonstrate to clerks and juniors how you (as the senior) use cases to learn.
For emotionally draining cases (eg: non-accidental injuries), acknowledge the toll it might have on care providers. This will provide a safe forum.
Handover
What do I need to do during handover?
- Identify your team (juniors, clerks), write down their names and pager numbers.
- Get an updated patient list. Ask the juniors (and the outgoing senior), “Who is sick? Who needs to be seen?
- Have a fresh sheet of paper (or the back of the team lists) ready for the ER consults (that may be in various stages of waiting to be seen, being seen by a junior/clerk, or waiting for a bed).
- Get Heme/Onc handover from resident or staff on Heme/Onc (this may occur later- you can always call the staff on call for handover).
- Subspecialty handover (GI, endocrine, etc.): these services may or may not have inpatients, so the staff may give you handover. If you haven’t received handover on weekends, and the nurse calls you about a patient, you can tell the nurse to call the subspecialty staff or fellow.
What should I do before handing over in the morning?
- Briefly reassess the status of the sickest patients, especially new admissions who are still in the ER.
- Check the list to see if it has been updated and remind juniors and clerks to update the list.
- Be prepared and on time or early for handover to set the tone for juniors and clerks.
- Review what patients you are going to identify to the new SPR as the sickest and requiring attention, as well as any consults waiting to be seen.
39
SPR Role for Consults
CanMEDS: Manager, Scholar
The SPR will take call first call from the Emergency Department and also any internal consults. Outlined are guidelines for the SPR:
1. The residents are informed that if they do receive calls from anywhere else i.e. outside hospitals, outside physicians, outside consultants, healthcare workers, or parents, that those calls should not be accepted and should be directed to the on-‐call pediatrician or back to paging.
2. After receiving the call from the Emergency Department, it is the SPRs responsibility to go down to the ED in a timely manner as outlined in the attached flow chart. If the child is ill, the SPR should deal with the situation right away and should inform their attending that there is sick child in the ED and the steps being taken. The SPR should also be aware that the pediatric Emergency physicians could also be called upon to help in such a circumstance. Some tips when receiving calls from the ER:
a) The SPR is to return the page to ER physician within 5 minutes. When discussing the consult, the SPR should gather at least the following information:
a. Consult question/reason. (Reason could be “I think he needs admission.”)
b. Patient name, age, location, Short HPI, Stable or not, vitals, any significant PE or lab findings.
c. If the SPR is not given all this information, they are to ask the ER MD for this information, prior to starting the consult.
3. If the child is stable then it is the SPRs responsibility to ensure that the child is seen in a timely manner as outlined in the attached flow sheet. Please call the learner to come to the ER with you.
i. If the child needs admission, disposition plan and bridging orders should be written for the patient within 30 minutes. Bridging orders should include all anticipated monitoring and treatment required for the consulted patient over the next two hours. The full assessment can then be completed. This can start in the emergency room but should not delay the transfer
40
of the child to the ward. Assessments should then be completed on the ward.
ii. If the SPR feels the child does not need admission they should contact their staff right away, who will assist them in discharge planning and collaboration with the ER staff on this.
iii. In instances where urgent patient care prevents the SPR from being able to present to the ER in the timeline described above, the SPR should tell the ER physician that they will be able to come down within x minutes of time, but will be sending the JPR. If both the JPR and SPR are busy, inform the ER physician that one or both residents will be down as soon as possible. The attending physician should also be informed.
4. If at any time there is a backlog in the ED, in that many consultations are
building up, or the SPR is busy in another area, there should be no hesitation in contacting the attending pediatrician to ensure that our patients are receiving prompt and quality care in the ED.
5. If the SPR feels that a referral made from the ED is inappropriate, they should contact their attending physician and discuss this with them.
Eyeballing patients
Upon arrival in the ER, the SPR should:
1) Assess if the patient is stable or not (reviewing the patient’s vitals, brief history/examination).
2) Review the working differential diagnosis and treatment plan thus far. 3) Review bridging orders.
a. Remember that the bridging orders are brief orders, not full admission orders.
b. The SPR should also write “Admit-‐To” orders and any additional orders that are felt to be necessary. These should include an order that “SPR is to be paged when the patient arrives on the ward.”
If possible the above three steps should be done with the junior learner present.
4) Determine the proper location for the patient (Step down vs. ward). 5) Check-‐in with bedside nurse and review orders. 6) The patient should not be moved from the ER during this process.
NOTE: Please remember that the time the SPR arrives on the ER is logged. Once the SPR arrives in the ER, the SPR must identify themselves to the bedside nurse and/or the PEM. The patient is taken off the ER MD tracker, and as such they are no longer following the patient.
41
NOTE: If there is concern regarding the patient’s condition, please engage the ER physician. The patient is not to be moved from the ER while this discussion is going on. If necessary, please contact the appropriate consultant attending for assistance.
Reviewing Consults with the On Call Attending:
CanMEDS: Communication, Collaboration, Professional Manager and Medical Expert
• The SPR and On Call attending/fellow should collaborate at the start of the on call period to review how the team will function through the night.
• The SPR will be first call and will do a brief assessment of the referred patient.
• If the SPR feels a patient does not need an admission they will contact the on-‐call attending/fellow, who will then come in to see the patient and collaborate with the ED physician if they do not feel an admission is warranted.
• If the patient needs admission, the SPR will write brief admitting orders. At which point if there is a bed the patient will go up to the ward where the full assessment and orders will be done.
• The on-‐call attending/fellow is expected to review all the patients seen from 1700-‐2300 hrs. in person, after each consult not clustered. You must contact the attending/fellow after each consult.
• All consults after 2300 hrs will be discussed in clusters of no more than three. The residents should call the attending/fellow after a cohort of three consults; the attending/fellow shall review the consults with the resident over the phone or in person.
• The attending/fellow will determine the detail of review depending on the level of training of the SPR.
• The SPR will be reminded that if at any time they have concerns they should not hesitate to call the on-‐call pediatrician.
Admitting Team:
• From 08:00 to 16:30, patients will be admitted as follows: odd days: Team 1, Even Days: Team 2
• From 16:30 to 08:00, the admission should alter between teams, try and admit under the team of the junior learner. The SPR will manage the admissions to ensure the teams remain
42
relatively balanced. Further balancing of numbers can also occur at handover.
• The order should be written as: Admit to Team___, under Dr. (attending pediatrician of the team admitted to), Dr. (on call) to cover until 8 am.
Teaching:
• Please refer to tip on being a senior guide • The senior resident will be responsible to teach the Junior
resident the Mac at Night curriculum time permitting
Evaluations:
Every SPR call should be evaluated with an encounter card. They should also seek verbal feedback from their attending staff. The Junior Pediatric Resident at the end of their float block will also evaluate the senior resident. They will be responsible for evaluating the off service junior resident nightly by filling in an encounter card. They will be responsible for evaluating the Junior Pediatric resident at the end of the two-‐week float block. Senior residents should attempt to have an encounter observed and a Mini-‐MAS completed.
43
Junior Float Objectives
The Royal College of Physicians and Surgeons of Canada has outlined the expectations for pediatric trainees (http://rcpsc.medical.org/residency/certification objectives/pediat_e.pdf). This rotation will enable residents to integrate many of the specific objectives achieved in previous ward and subspecialty rotations. The junior-float resident will have a unique opportunity to build medical expert, communication, collaboration and management skills while providing efficient and quality care to patients.
General Objectives:
1. The objectives for the junior float block are listed in the competency based medical education (CBME) booklet.
At the beginning of the rotation, each resident must develop personal learning objectives for the two-week block. These should be recorded by the resident on their learning contract. This should be kept as part of their portfolio. Your program director can help you with the objectives. Some of the over-arching Royal College objectives of pediatric training can be specifically addressed during this rotation. Residents will be evaluated on their ability to:
- perform a complete and appropriate assessment of a patient - perform a focused, efficient, orderly physical examination, and record this information - accurately elicit and synthesize relevant information and perspectives of patients and
families, colleagues, and other professionals - convey relevant information and explanations accurately to patients and families,
colleagues and other professionals - participate effectively and appropriately in an interprofessional healthcare team - work effectively with other health professionals to prevent, negotiate, and resolve
interprofessional conflict - facilitate the learning of patients, families, students, residents, and other health
professionals, as appropriate. We hope that this rotation will be a relevant experience that consolidates previous learning and challenges residents to see their potential as consultant pediatricians.
JUNIOR FLOAT ROTATION GUIDELINES
General Responsibilities:
I. Pager: Carry the junior pager between 16:30 to 07:15 a. The JPR on call will carry the following pagers overnight:
• Pager 5301 (Team 1) OR Pager 5302 (Team 2) as pre-‐determined on the call schedule
• Pager 5303 (Team 3 – Level 2 nursery and complex care team)
• Pager 5304 (Heme-‐Onc) **If 2 JPRs are on call at night, then pager 5303 will be assigned to one
resident and 5304 to the other (it is the JPR’s responsibility to receive handover from the appropriate team). Off-‐service residents will NOT carry 5303 or 5304
44
II. Be available to the senior resident for consults. III. Be available to “eye ball“ consults with the senior resident. IV. Be able to complete a history & physical, admission/transfer note & dictation. V. Review all consults with the senior residents in a timely manner if the senior resident is
busy should review with the faculty on call. VI. Be responsible for calls form the wards and respond to them in a timely manner. If
concerned about a patient, inform the senior resident or faculty on call promptly. VII. Provide support to the off service resident and clinical clerks if required.
VIII. For issues on the hematology/oncology (H/O) ward, the H/O faculty or fellows are available for support and the resident should not hesitate to contact them if there are any concerns. If you need to contact the HO staff or fellow:
1. Page the staff on-call through Hospital Locating (x76443)
2. If no response after 15 minutes, then page the staff on-call again via locating
3. If no response after 5 minutes, then call the staff on-call via home or cell number (locating has access to these numbers). All admissions must be reviewed with the H/O staff on call. The SPR is available for back up at any time.
Handover
1. Ensures adequate handover to the appropriate resident. 2. Updates the team lists in a timely manner such that the new admissions and consults are
available at handover. Education
7. The resident will get teaching informally by the senior resident. 8. The senior resident will also provide the Mac at Night curriculum throughout the float
block. 9. The junior resident should provide teaching to the off-service residents and clerks on call. 10. The junior resident will also provide the Mac at Night curriculum to the off-service
residents and clerks if the senior resident is unable to do so..
Call
The junior float resident will be on call 16:30-07:15 plus handover.
Vacation
Junior float will be scheduled in the master rotational schedule. Residents will have an opportunity to review and request changes to the rotational schedule before it is finalized. After the schedule is locked in it is the resident’s responsibility to find a qualified replacement if they choose to take vacation during their scheduled float.
45
EVALUATION AND FEEDBACK
Regular feedback for Junior Float resident should be sought from the senior who has dealt directly with that resident during the rotation.
- The junior resident should be encouraged to ask for feedback (history, physical, assessment, differential, plan and management) regarding specific patients at the time of handover to the team.
- The senior must complete an encounter card evaluation for the two weeks. - The junior resident will also be required to complete an encounter card evaluation for the
senior resident. - The junior resident should seek out opportunities to complete Mini-MAS evaluations.
46
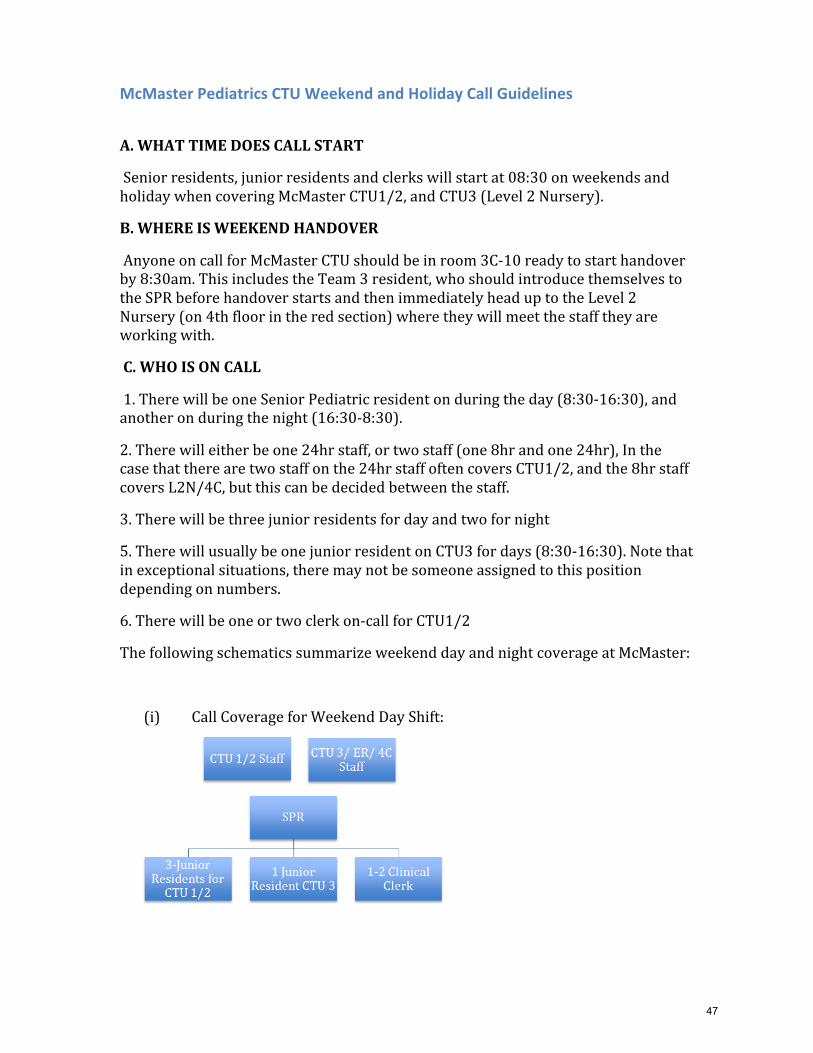
McMaster Pediatrics CTU Weekend and Holiday Call Guidelines
A. WHAT TIME DOES CALL START
Senior residents, junior residents and clerks will start at 08:30 on weekends and holiday when covering McMaster CTU1/2, and CTU3 (Level 2 Nursery).
B. WHERE IS WEEKEND HANDOVER
Anyone on call for McMaster CTU should be in room 3C-‐10 ready to start handover by 8:30am. This includes the Team 3 resident, who should introduce themselves to the SPR before handover starts and then immediately head up to the Level 2 Nursery (on 4th floor in the red section) where they will meet the staff they are working with.
C. WHO IS ON CALL
1. There will be one Senior Pediatric resident on during the day (8:30-‐16:30), and another on during the night (16:30-‐8:30).
2. There will either be one 24hr staff, or two staff (one 8hr and one 24hr), In the case that there are two staff on the 24hr staff often covers CTU1/2, and the 8hr staff covers L2N/4C, but this can be decided between the staff.
3. There will be three junior residents for day and two for night
5. There will usually be one junior resident on CTU3 for days (8:30-‐16:30). Note that in exceptional situations, there may not be someone assigned to this position depending on numbers.
6. There will be one or two clerk on-‐call for CTU1/2
The following schematics summarize weekend day and night coverage at McMaster:
(i) Call Coverage for Weekend Day Shift:
47
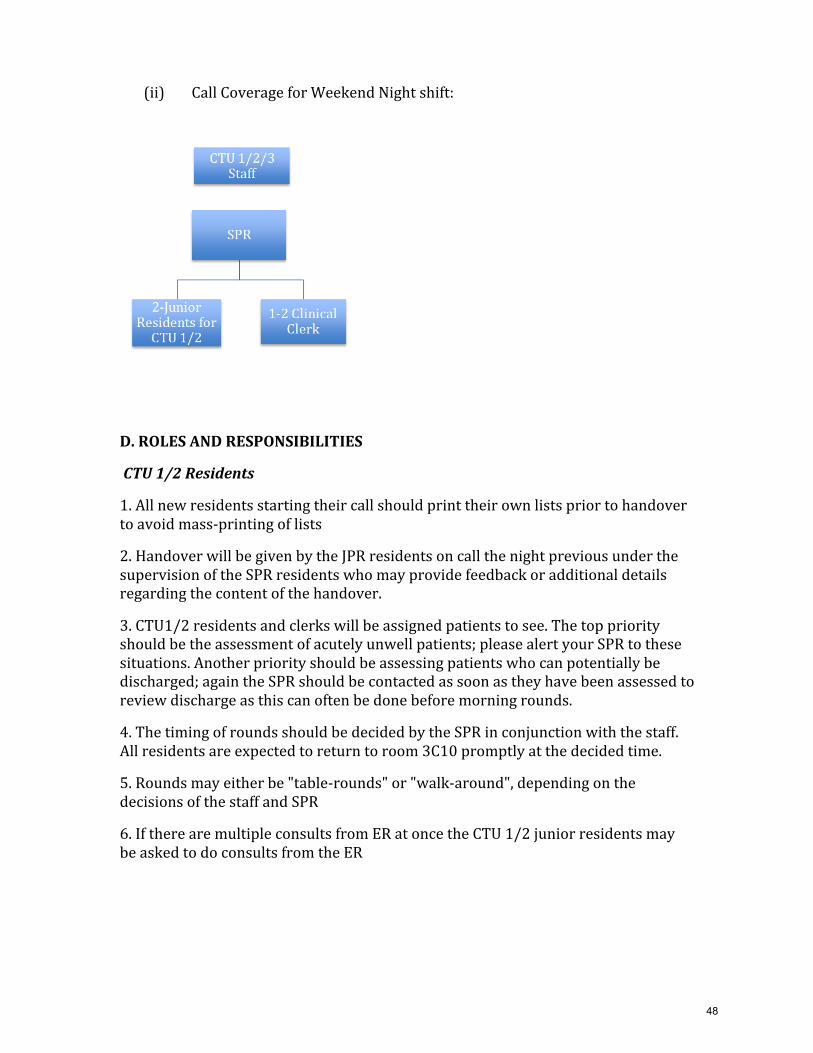
(ii) Call Coverage for Weekend Night shift:
D. ROLES AND RESPONSIBILITIES
CTU 1/2 Residents
1. All new residents starting their call should print their own lists prior to handover to avoid mass-‐printing of lists
2. Handover will be given by the JPR residents on call the night previous under the supervision of the SPR residents who may provide feedback or additional details regarding the content of the handover.
3. CTU1/2 residents and clerks will be assigned patients to see. The top priority should be the assessment of acutely unwell patients; please alert your SPR to these situations. Another priority should be assessing patients who can potentially be discharged; again the SPR should be contacted as soon as they have been assessed to review discharge as this can often be done before morning rounds.
4. The timing of rounds should be decided by the SPR in conjunction with the staff. All residents are expected to return to room 3C10 promptly at the decided time.
5. Rounds may either be "table-‐rounds" or "walk-‐around", depending on the decisions of the staff and SPR
6. If there are multiple consults from ER at once the CTU 1/2 junior residents may be asked to do consults from the ER
48
CTU 3 Resident
1. Discuss with staff in L2N how to approach assessing and rounding on patients in the L2N.
2. Round on any Team 3 (complex care patients on the ward)
2. See any 4C consults and follow ups.
3. Will be the first junior resident in line to see any new consults from the ER. In the case that L2N/ 4C is busy, resulting in the team 3 resident being busy/unavailable, the staff and SPR should come to an agreement about which junior resident is in the best position to attend to the ER consultation.
4. If there is not an8 hour staff available, the CTU 1 and 2 residents may be called upon to help with CTU 3.
E. CONSULTS FROM MCMASTER EMERGENCY DEPARTMENT
Consults will go to pager 1645 the senior resident.
In the case that there is only one staff on-‐call:
The staff and SPR should decide which of them should go assess the patient and write bridging orders. The team 3 resident should be given first priority to see the consult, followed by the CTU1/2 residents or clerks. Once the junior is finished with the consult, one of the staff or SPR will review the consult. When the team is finished rounding the SPR will assess all new consults in the ER and then assign a junior resident to do the full consult. The SPR should also review this consult with the junior, and then review with the staff. The junior resident chosen will depend on the service load of the various CTU teams.
In the case that there are two staff on-‐call:
1. The SPR should assess and write bridging orders for the patient. A junior resident should then review the case directly with the SPR who will discuss with the staff. The Junior resident chosen will depend on the service load of the services.
2. In the case that the SPR feels they are still very busy caring for acutely unwell patients even after rounds are over they should discuss their situation with their staff, and whether or not it is a reasonable situation to ask the 8-‐hour staff to help with ER consults.
49
F. EVENING HANDOVER
1. All of the team lists should be updated with the day’s events prior to evening handover.
2. The residents covering the night shift should print their own up-‐to-‐date list.
3. The team 3 resident should handover the list to the resident carrying the Team 3 pager that night
4. All of the residents and clerks on CTU1/2 should be in 3C-‐10 to handover at 16:30. In the event that they are delayed for any reason it is expected that this should be communicated.
5. Each team list must be handed over in an orderly fashion. All patients must be reviewed for the benefit of the SPR starting their night shift
50
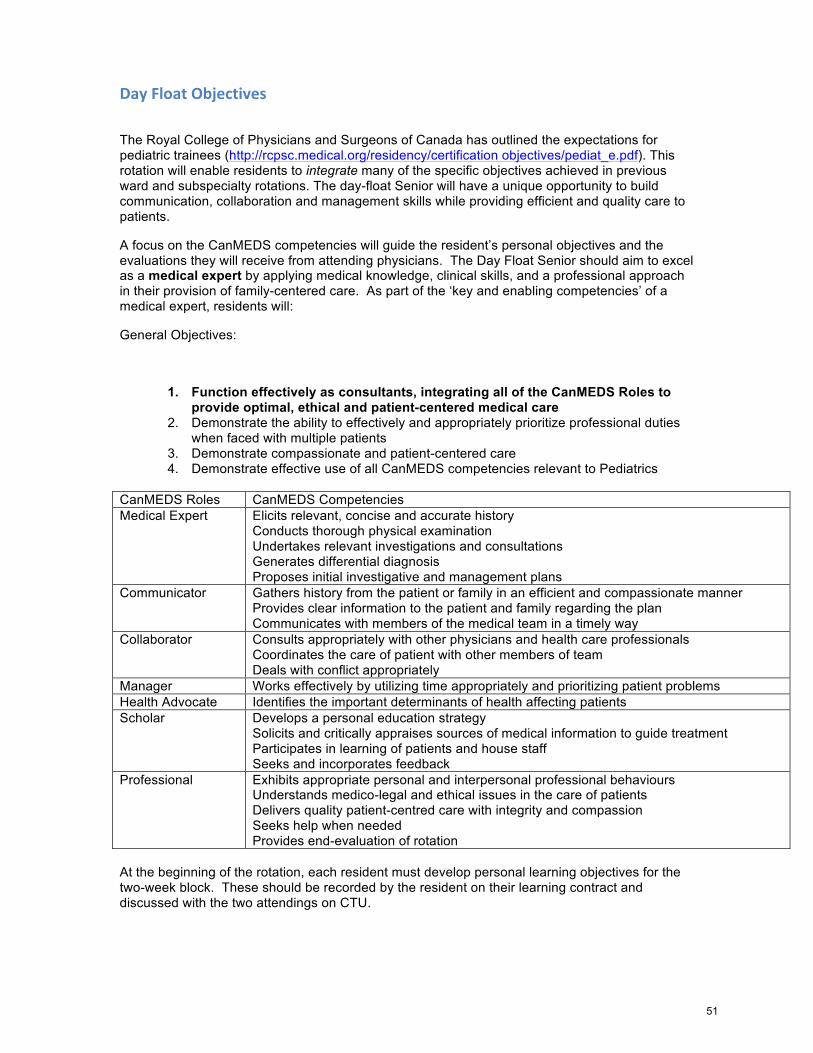
Day Float Objectives
The Royal College of Physicians and Surgeons of Canada has outlined the expectations for pediatric trainees (http://rcpsc.medical.org/residency/certification objectives/pediat_e.pdf). This rotation will enable residents to integrate many of the specific objectives achieved in previous ward and subspecialty rotations. The day-float Senior will have a unique opportunity to build communication, collaboration and management skills while providing efficient and quality care to patients.
A focus on the CanMEDS competencies will guide the resident’s personal objectives and the evaluations they will receive from attending physicians. The Day Float Senior should aim to excel as a medical expert by applying medical knowledge, clinical skills, and a professional approach in their provision of family-centered care. As part of the ‘key and enabling competencies’ of a medical expert, residents will:
General Objectives:
1. Function effectively as consultants, integrating all of the CanMEDS Roles to provide optimal, ethical and patient-centered medical care
2. Demonstrate the ability to effectively and appropriately prioritize professional duties when faced with multiple patients
3. Demonstrate compassionate and patient-centered care 4. Demonstrate effective use of all CanMEDS competencies relevant to Pediatrics
CanMEDS Roles CanMEDS Competencies Medical Expert Elicits relevant, concise and accurate history
Conducts thorough physical examination Undertakes relevant investigations and consultations Generates differential diagnosis Proposes initial investigative and management plans
Communicator Gathers history from the patient or family in an efficient and compassionate manner Provides clear information to the patient and family regarding the plan Communicates with members of the medical team in a timely way
Collaborator Consults appropriately with other physicians and health care professionals Coordinates the care of patient with other members of team Deals with conflict appropriately
Manager Works effectively by utilizing time appropriately and prioritizing patient problems Health Advocate Identifies the important determinants of health affecting patients Scholar Develops a personal education strategy
Solicits and critically appraises sources of medical information to guide treatment Participates in learning of patients and house staff Seeks and incorporates feedback
Professional Exhibits appropriate personal and interpersonal professional behaviours Understands medico-legal and ethical issues in the care of patients Delivers quality patient-centred care with integrity and compassion Seeks help when needed Provides end-evaluation of rotation
At the beginning of the rotation, each resident must develop personal learning objectives for the two-week block. These should be recorded by the resident on their learning contract and discussed with the two attendings on CTU.
51
Some of the over-arching Royal College objectives of pediatric training can be specifically addressed during this rotation. Residents will be evaluated on their ability to:
- perform a complete and appropriate assessment of a patient - perform a focused, efficient, orderly physical examination, and record this information - accurately elicit and synthesize relevant information and perspectives of patients and
families, colleagues, and other professionals - convey relevant information and explanations accurately to patients and families,
colleagues and other professionals - participate effectively and appropriately in an interprofessional healthcare team - work effectively with other health professionals to prevent, negotiate, and resolve
interprofessional conflict - facilitate the learning of patients, families, students, residents, and other health
professionals, as appropriate. We hope that this rotation will be a relevant experience that consolidates previous learning and challenges residents to see their potential as consultant pediatricians.
DAY FLOAT ROTATION GUIDELINES
General Responsibilities:
II. Carry pager (#1645) between 9:15 to 17:15 III. Be available to all residents and clinical clerks to answer questions and provide
assistance. IV. During the hours of approximately 09:15-1230h, try to manage all ER/4C/L2N/PICU
transfers or consults independently (i.e. history & physical, admission/transfer note & dictation, review with staff) to allow the CTU teams to finish inpatient rounds. However, house-staff may be asked/required to see these consults/transfers during these hours if there are either a) several consults that need to be seen in a timely manner or b) the house staff-to-inpatient ratio allows for house staff to be excused without compromising inpatient rounds.
V. After CTU rounds are complete, the resident will: a. Triage ER consults first to the admitting team house-staff, then as the next option
to the non-admitting team house-staff. b. The residents will triage ward consults and transfers first to the admitting team
house-staff, then as the next option to the non-admitting team house staff. c. The resident will triage L2N transfers and 4C consults to Team 3 house-staff.
VI. The day float resident will review all cases with the house-staff in a timely manner. VII. The day float resident will review the cases with the appropriate attending +/- the
appropriate team’s senior resident if available. VIII. The day float resident will call the appropriate attending if multiple patients have been
referred to ensure optimum patient care and flow. Please see outline of priorities in the “role” section below to help guide how to triage multiple consults are referred at the same time.
IX. The day float resident will collaborate with the admitting team senior when patients are admitted to the CTU. If not busy the day float resident should continue to manage that patient until evening handover. Patients admitted by the day float resident that have not been transferred to the ward will remain the responsibility of the day float resident.
X. The resident may assist with the care of the patients admitted overnight to “no bed” in the ER upon collaboration with the appropriate CTU senior.
XI. When not busy, the day float will collaborate with the team senior to assist with discharges or procedures.
52
Handover
1. Ensures adequate handover to the appropriate CTU senior resident of all patients admitted to teams through the day.
2. Updates the team lists in a timely manner such that the new admissions and consults are available at handover.
Education
1. Should attend all ward teaching if not busy in the ER. 2. Should attend AHD on Wednesday afternoon, as this is a protected teaching time for the
day float resident. The resident is expected to return to the ward after AHD for handover and completion of the shift.
3. Provides bedside and case based teaching to learners. If there is a teaching resident available, the day float resident will collaborate with the teaching resident.
Call
The day float resident will be on call 09:15-17:15.
Vacation
Day float will be scheduled in the master rotational schedule, residents will have an opportunity to review and request changes to the rotational schedule before it is finalized. After the schedule is locked in if the resident chooses to take a vacation, they must find a qualified replacement.
Administrative
The day float senior resident should ensure efficient workings of the consult service. They should provide back up and support to the junior learners. They should demonstrate and teach time management to the junior learners. They need to provide support and back up to the CTU seniors when not busy.
ROLE The Day Float Senior role is challenging in that multiple demands must be managed at one time, as residents facilitate patient flow throughout the hospital. Guidelines have been developed to assist residents in determining the order in which tasks should be completed. In order of priority, the Admitting Senior will attend to the following:
1. Consultations and admissions of patients from the ED 2. Direct admissions from outlying hospitals. 3. Transfer from PCCU. 4. 4C consults 5. Level 2 admissions
Other roles might include:
6. Inpatient Pediatric Consults 7. Help with procedures when the CTU senior is busy
- This should be in a supervisory role as much as possible, to ensure junior learners have the opportunity to do procedures.
53
8. Bedside teaching around cases and observation of learners - If teams are not busy, medical students or junior learners should be assigned to
the consult and the day-float Senior can supervise and review the case 9. Help with discharges 10. Help with subspecialty admissions.
The Day Float Senior role does NOT involve the following:
- Assuming care for inpatients on the teams. If the CTU senior is away, the Day Float resident does not assume the role of CTU senior.
COMMUNICATION
The Day Float Senior will be expected to hand over each patient admitted or transferred to the appropriate ward Senior and/or staff immediately after the admission/transfer is complete.
- The Day Float Senior is to communicate with the staff member for each team at the beginning of the week to determine logistics and expectations of handover for each admitted/transferred patient.
- When time allows, all handover of admissions/transfers will be done in person with the Ward Senior/staff at the bedside to optimize senior learning opportunity. When it is busy, case presentation may be done over the phone with the senior and/or staff.
- The Day Float Senior will add the admitted/transferred patient to the respective ward team list ASAP unless communication with the ward team dictates otherwise. This is NOT to be done at the end of the day, as admitted patients need to be on the list for evening handover.
- After the Day Float Senior has handed over the patient to the team (i.e. Ward Senior or staff) and the patient is on the ward, the responsibility of that patient’s care transfers to the team.
On Wednesday afternoons (resident academic half-day), the Day Float Senior should communicate any pending admissions to the appropriate team staff. These admissions should be done in a timely fashion, as would be expected from an admitting or ward senior resident. These admissions are not meant to wait in the Emergency Department until the Night Float Senior is available to see the patients.
EVALUATION AND FEEDBACK
Regular feedback for Day Float Seniors should be sought from attending MDs who have dealt directly with that resident during the rotation.
- The senior should be encouraged to ask for feedback (history, physical, assessment, differential, plan and management) regarding specific patients at the time of handover to the team.
- At least 7 encounter cards must be completed during the two weeks and 2 Mini-MAS assessments
- ED and subspecialty staff should also provide feedback to the Admitting senior, and should communicate with the ward staff if they have any contributions to the final evaluation.
54
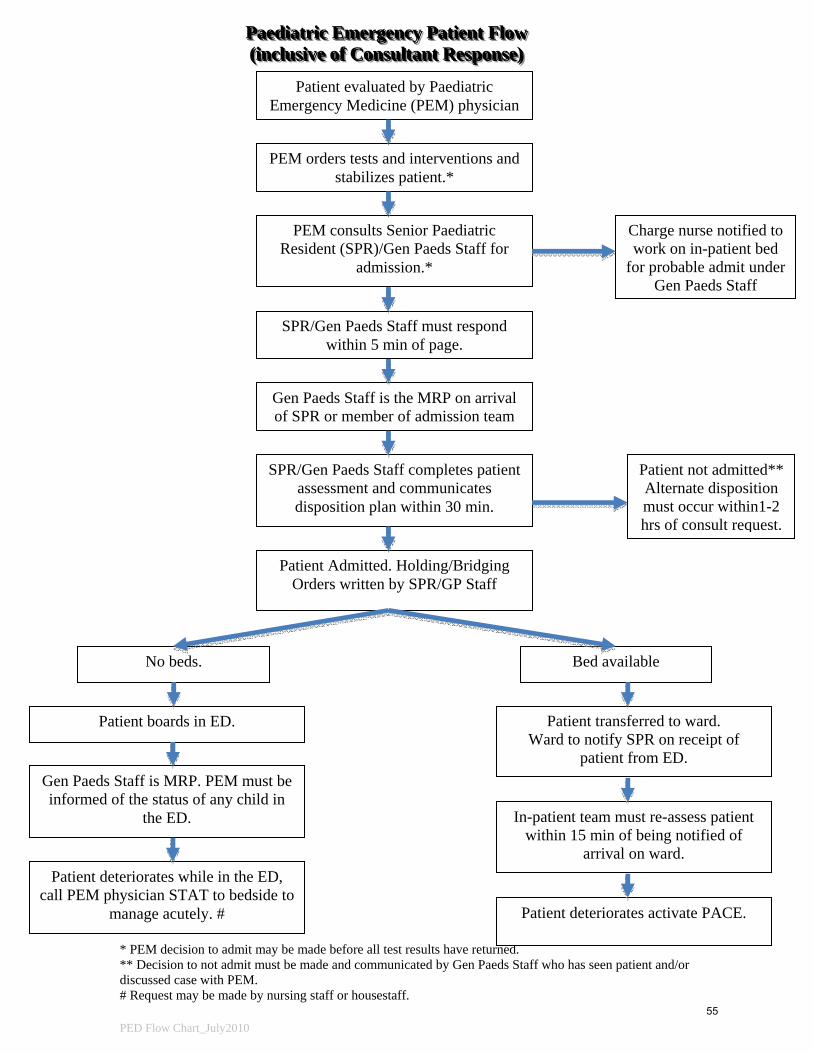
PPPaaaeeedddiiiaaatttrrriiiccc EEEmmmeeerrrgggeeennncccyyy PPPaaatttiiieeennnttt FFFlllooowww (((iiinnncccllluuusssiiivvveee ooofff CCCooonnnsssuuullltttaaannnttt RRReeessspppooonnnssseee)))
* PEM decision to admit may be made before all test results have returned. ** Decision to not admit must be made and communicated by Gen Paeds Staff who has seen patient and/or discussed case with PEM. # Request may be made by nursing staff or housestaff. PED Flow Chart_July2010
Patient evaluated by Paediatric Emergency Medicine (PEM) physician
PEM orders tests and interventions and stabilizes patient.*
PEM consults Senior Paediatric Resident (SPR)/Gen Paeds Staff for
admission.*
SPR/Gen Paeds Staff must respond within 5 min of page.
SPR/Gen Paeds Staff completes patient assessment and communicates disposition plan within 30 min.
Patient boards in ED.
Gen Paeds Staff is MRP. PEM must be informed of the status of any child in
the ED.
Gen Paeds Staff is the MRP on arrival of SPR or member of admission team
Patient deteriorates while in the ED, call PEM physician STAT to bedside to
manage acutely. #
Patient not admitted** Alternate disposition must occur within1-2 hrs of consult request.
Patient Admitted. Holding/Bridging Orders written by SPR/GP Staff
Charge nurse notified to work on in-patient bed
for probable admit under Gen Paeds Staff
No beds. Bed available
Patient transferred to ward. Ward to notify SPR on receipt of
patient from ED.
Patient deteriorates activate PACE.
In-patient team must re-assess patient within 15 min of being notified of
arrival on ward.
55