cultural and genetic diversity in america
TRANSCRIPT

byValentine J. Burroughs, MD
Chair, Health Policy CommitteeBoard of Trustees
National Medical Association
Randall W. Maxey, MD, PhDChairman, Board of TrusteesNational Medical Association
Lavera M. Crawley, MDAdvisory Board, Division of
Biomedical Education and ResearchNational Medical Association
Richard A. Levy, PhDVice President, Scientific AffairsNational Pharmaceutical Council
Cultural and Genetic Diversityin America:The Need for IndividualizedPharmaceutical Treatment

About the AuthorsValentine J. Burroughs, MD, is Chair of the Health Policy Committee for the National Medical
Association Board of Trustees. Dr. Burroughs is a practicing Board Certified endocrinologist andinternist in New York City. He is Medical Director of Health Care New York IPA, Associate MedicalDirector at Group Health Insurance of New York, and Associate Medical Director and Chairman ofMedicine at North General Hospital in Manhattan.
Randall W. Maxey, MD, PhD, is Chairman of the National Medical Association Board of Trusteesand past President of the Golden State Medical Association and the Charles R. Drew MedicalSociety. He has practiced nephrology in the Los Angeles area for over 24 years and holds staffappointments at various hospitals. He has conducted research in cardiovascular pharmacology andhypertension. Dr. Maxey has established several dialysis centers in California, the South Pacific andin Africa.
Lavera M. Crawley, MD, is a member of the Advisory Board for the National Medical AssociationDivision of Biomedical Research and Education. She also serves as the Executive Director for theInitiative to Improve Palliative Care for African Americans, as well as a researcher and Lecturer inMedicine at the Stanford University Center for Biomedical Ethics. Dr. Crawley’s publications focuson issues of cultural diversity in serious illnesses, and in race/ethnicity and trust in doctor-patientrelationships.
Richard A. Levy, PhD, is Vice President for Scientific Affairs at the National Pharmaceutical Council(NPC). Dr. Levy has spent over thirty years teaching, writing, and conducting research in universitiesand private industry. His current interests include tracking, analyzing, and communicating trendsaffecting pharmaceutical innovation; and developing information on management of medications byindividuals and organizations. Before coming to NPC, he taught and conducted research inneuropharmacology at the University of Illinois College of Medicine.
About the National Medical Association (www.nmanet.org)The National Medical Association (NMA) is the collective voice of African American physicians
and the leading force for parity and justice in medicine and the elimination of disparities in health.The National Medical Association is a 501(c)(3) national professional and scientific organizationrepresenting the interests of more than 25,000 physicians and their patients. Established in 1895,NMA is committed to 1) preventing the diseases, disabilities and adverse health conditions thatdisproportionately or differentially impact African American and underserved populations, 2) supporting efforts that improve the quality and availability of health care to poor and underservedpopulations, and 3) increasing the representation and contribution of African Americans in medicine.
About the National Pharmaceutical Council (www.npcnow.org)Since 1953, the National Pharmaceutical Council (NPC) has sponsored and conducted scientific,
evidence-based analyses of the appropriate use of pharmaceuticals and the clinical and economicvalue of pharmaceutical innovations. NPC provides educational resources to a variety of health carestakeholders, including patients, clinicians, payers and policy makers. More than 20 research-basedpharmaceutical companies are members of the NPC.
© November, 2002. National Pharmaceutical Council and National Medical Association

Executive Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2
Abstract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2
Recommendations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3
Toward Individualized Therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5
Purposes of This Report . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .7
Disparities in Health Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8
Disparities in Cultural Competency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .10
Disparities in Health Literacy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .10
Interplay of Environmental, Genetic, and Cultural Factors . . . . . . . . . . . . . . . . . . . . . . . . . . .12
Environmental Factors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .12
Genetic Factors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .13
Clinical relevance of genetic differences (polymorphisms) . . . . . . . . . . . . . . . . . . . . . .14
Racial differences in response to medication . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .16
Cultural Factors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .17
Trust and respect . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .17
Health beliefs and practices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .18
Family values . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .20
Effect of cultural factors on medication compliance . . . . . . . . . . . . . . . . . . . . . . . . . . .21
The Future of Individualized Therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .22
Conclusions and Recommendations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .23
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .25
1
TABLE OF CONTENTS

This report reviews the environmental, geneticand cultural factors that underlie variations indrug response among different populationgroups. Population groups that have beenconventionally defined along racial and ethniccategories comprise important subgroups whosespecial needs and drug responses traditionallyhave been undervalued or ignored. Given thegenetic and cultural variation among individuals
in these groups, drugmanagement policies in bothpublic and private paypharmaceutical programs mustbe flexible enough toaccommodate patients’ specificneeds.
The factors determiningpopulation variations in responseto medications are complex andinterdependent. Environmentalfactors (e.g., climate, smoking,alcohol consumption) may have aprofound effect on drugmetabolism. Biologic factors suchas genetic polymorphisms(naturally occurring variations inthe structures of genes, drug
metabolism enzymes, receptor proteins, andother proteins involved in drug response ordisease progression), age, and gender havesignificant influence and may require the use ofalternate drugs or dosages in patients ofdifferent racial and ethnic backgrounds. Geneticresearch in the past few decades has uncoveredsignificant differences among populations in the
metabolism, clinical effectiveness, and sideeffect profiles of therapeutically importantdrugs; however, most of the research applies toAfrican Americans, Asians, and Caucasians.Fewer studies have specifically targetedHispanics who, according to the 2000 U.S.Census, represent the second-largestethnocultural group.
Cultural or psychosocial factors have beendocumented to affect a patient’s adherence to,and therefore the effectiveness of, drug therapy.For example, trust and respect for patients andtheir health beliefs and practices, as well ascommunications issues, have been found toinfluence adherence to medication regimens.Patients’ beliefs about the nature of disease,acceptance of side effects, and preferencesregarding herbal or traditional therapies may beinfluenced by a range of socioculturalinfluences, including gender, socioeconomicclass, education, immigrant status, and religion,all of which must be taken into account.Additionally, communications barriers may leadto incorrect interpretations of diagnoses andinstructions regarding treatment. A frequentlyoverlooked and underemphasized barrier,especially in the elderly and in underrepresentedminorities, is inadequate health literacy. Thiscomprises their ability to understand and followthrough on health information matters. Ofgreater significance is the recognition of theconsiderable skills that these patients have inconcealing their poor health literacy. Takentogether, these variables dictate that in order tobe effective, therapy must be individualized.
2
EXECUTIVE SUMMARY
Genetic research inthe past few decadeshas uncoveredsignificant differencesamong racial andethnic groups in themetabolism, clinicaleffectiveness, andside effect profiles oftherapeuticallyimportant drugs.
It is now well documented that substantial disparities exist in the quality and quantity of medicalcare received by minority Americans, especially those of African, Asian, and Hispanic heritage.Pharmacogenetic research in the past few decades has uncovered significant differences amongpopulation groups in the metabolism, clinical effectiveness, and side effect profiles of many clinicallyimportant drugs. In addition, differences in how various populations view and respond to medicinesunderscores the need for an individualized approach to pharmaceutical therapy. Historically, thespecial needs and responses to pharmaceutical treatment of these groups have been undervaluedor ignored. All of these differences must be taken into account in the design of cost managementpolicies such as formulary management, therapeutic drug substitution, and step-care protocols.These programs should be broad and flexible enough to enable rational choices and individualizedtreatment for all patients, regardless of racial or ethnic origin.

3
Recommendations
Health care policy makers and providers shouldpay attention to the need to individualize drugtherapy for specific population groups. Thefollowing recommendations could benefit thequality of care for racial and ethnicsubpopulations and may also help to controlhealth care costs.
1. Health care institutions should implementcost containment practices that are broad andflexible enough to enable rational choices ofdrugs and formulations for all patients,regardless of race or ethnic origin.
2. Physicians should give individualizedtreatment to each patient and prescribe drugtherapy that takes into account racial orethnic origin and sociocultural influences.Physicians should also be alert to atypicaldrug responses or unexpected side effects(especially with cardiovascular or psychotropicagents) when they treat patients from diverseracial and ethnic backgrounds. Patients maynot be taking the medication properly due tomisunderstood instructions, ormisperceptions about Western medicine orthe severity of the disease. Dosageadjustments may be required in somepatients if supported by pharmacologicalevidence.
3. Pharmaceutical companies should continue toinclude significant numbers of patientsrepresenting varied racial and ethnic groups indrug metabolism studies and clinical trials.Most companies test and evaluate newpharmacological compounds on numerouspopulation subgroups. Inclusion of differentracial and ethnic populations in clinical trials islikely to reveal drug actions and side effectsspecific to these groups, and may also to leadto the discovery of therapies of specificadvantage to patients of varied racial andethnic backgrounds.
4. Hospitals, managed care groups, and otherproviders of health care services shouldendeavor to employ practitioners who areracially and ethnically representative of thepatient population being served. Providerorganizations should develop and institutespecific training in cultural competence for allpractitioners who have direct patientcontact–especially physicians, pharmacists,nurses, and physician assistants.
Toward Individualized Therapy
Race and ethnicity have been used as factors indetermining if an individualwill respond in theexpected way to a givendrug therapy. However,race is an imprecisesubstitute for geneticvariations that an individualmay or may not possess.Technological advances inthe wake of the HumanGenome Project willeventually enable us tomove beyond flawedconcepts of race and totailor drug therapyprecisely to each patient. Itis now possible to take a genetic “fingerprint”of an individual and precisely determine thepresence of polymorphisms in the genes knownto be involved in drug interaction. Instead of aperson’s racial category being a risk factor forthe possession of polymorphisms involved indrug response, a genotypic profile candetermine with certainty whether or not theindividual possesses these polymorphisms.
In the future, drug treatment will be individuallytailored rather than race-based. Geneticfingerprinting using DNA arrays is alreadypractical, but the knowledge base relatinggenomic variations to drug response and diseaseprogression has not been developed. Studies inwhich DNA fingerprints are correlated with datapresent in medical records about medical historyand drug response will have a profound impacton the ways in which new drugs are developedand used.
Racial and ethnicgroups compriseimportantsubpopulations whosespecial needs and drugresponses traditionallyhave been undervaluedor ignored.

However, treating individuals involves more thanawareness of genetic variations. Apart from thephysiological complexities associated withappropriate prescribing for different racial andethnic groups, practitioners face the addedchallenge of delivering effective pharmaceuticalcare to people within a psychosocial contextappropriate to their culture and level of healthliteracy. The great diversity in our patientpopulation demands a framework in which thepractitioner can approach all patients, regardlessof racial, ethnic, or sociocultural background, asegalitarian partners in care.
Although any discussion of socioculturalcompetence can list examples of ourdifferences, it is important to remember themany similarities exist among diverse peoples.All patients seeking care have recognized aneed for that care. All share feelings of need,fear, mistrust, lack of control, hope, anddisconnection from their normal world of health.When these feelings are acknowledged andrespected by a culturally competent practitioner,partnerships can be built in which any culturalhealth belief or treatment preference can bediscussed.
4

5
Individual genetic polymorphisms are naturallyoccurring variants in the structures of genes,drug metabolism enzymes, receptor proteins,and other proteins involved in drug response ordisease progression. These polymorphismschange gradually in prevalence acrosscontinents and do not separate populations intoclearly demarcated groups that correspond topopular ideas of race.
The most obvious manifestations of racialdifferences – skin color, cranial features, etc. – aresuperficial characteristics that have little relevanceto drug responses or to the progression ofcomplex diseases such as diabetes mellitus,coronary heart disease, etc.1,2 It should beemphasized that humans are one species.Although we have evolved as geographicallyseparated groups, our differences have not yieldedlarge variations in genetic composition. Thosegenetic differences that do exist reflect variationsfrom only a small number of genes. Therefore,“race” is an imprecise substitute measure ofgenetic differences among populations.
The idea of race is extremely complex. It refersto a grouping of humans into specific categoriesthat have no underlying biological underpinning.Yet, because the groupings are largely based onphysically visible features, race appears to bereal. This may explain why race as a flawedconcept is difficult to eradicate from usage – inboth scientific and general discourse. Forexample, skin pigmentation has been used as amarker for race (white, black, red, yellow). Butskin color alone is quite deceptive, as the samerange of colorations can be found amongpersons from different population groups. Forexample, those from certain Asian backgroundscan be as dark as those from Africa. And thosefrom African ancestries can be as light as thosewhose ancestry can be traced to Europe.3
Historically, the categorization of human beingsaccording to physical attributes linked togeography and later termed race can be tracedback to the eighteenth century.3,4,5 Not only werevarieties of humans described, but also ahierarchical ordering was ascribed to thesevarieties, where one group (those who couldlater be called “white”) was considered themost superior. Therefore, embedded in the ideaof race is this notion of the ascendancy of somegroups over others.
In the U.S., criteria used to identify “racialized”groups have not been based solely on biologicalmarkers, but also on the idea of ethnic orcultural indicators. For example, Hispanicscomprise a group of individuals who generallyshare a linguistic heritage but who representmultiple nationalities and racialized groupings,including white, black and indigenous Indians.
The terms ethnicity and culture have also beensubject to conceptual misunderstanding andthus require more precise and coherentdefinitions if they are to be useful. Together theyrefer to combinations of “socioeconomic,religious, and political qualities of humangroups, including language, diet, dress,customs, kinship systems, and historical orterritorial identity.”6
Like “race”, both ethnicity and culture are alsosubject to social constructions whoseborderlines arenot easilymapped.7,8 Theyreflect our ownprojections andare also subjectto individualfluidity. One caninhabit multiplecultural or ethnicidentities andmove betweenthem dependingon need orcircumstance.Thus, we mustresist any temptation to view these concepts ashaving material reality. The conditions and wayscertain individuals or groups can be assigned toa specific ethnic or cultural group must bespecified. For example, we should speak not ofHispanic culture but rather of cultural beliefsheld by certain populations of persons fromspecific areas, say Puerto Rico or El Salvador.
INTRODUCTION
In addition to the physiologicalcomplexities associated withappropriate prescribing for differentracial and ethnic groups,practitioners face the addedchallenge of delivering effectivepharmaceutical care to theseindividuals within a psychosocialcontext appropriate to their culture.

6
Research in the last 35 years has uncoveredvarying distributions of genetic polymorphismsin enzymes and receptors associated with drugmetabolism. These are reflected in differencesamong population groups in clinical responsesto drugs and in drug side effects. For example,black and white patients have been shown todiffer significantly in their responses to beta-blockers, angiotensin-converting enzyme (ACE)inhibitors, and diuretics used either alone or incombination for the treatment of high bloodpressure. Some populations of Chinese areconsiderably more sensitive than whites to theeffects of the beta-blocker propranolol on heartrate and blood pressure. African Americans andChinese Americans metabolize nicotine moreslowly than do whites, and genetic variationsassociated with slower nicotine metabolism aremore common in some Asian populations.9,10,11
As compared to some whites, certain Asiangroups are more likely to require lower dosagesof a variety of different drugs used to treatmental illness, including lithium,antidepressants, and antipsychotics.
Concepts of identity based on racial markers,ethnicity or culture may be useful whendiscussing trends among populations, but theycannot predict individual behavior. We cannotrely on a form of racial profiling – using visible orsocially constructed markers, such as skinpigmentation, eye-shape, language use, orhealth beliefs, to accurately identify thepresence or absence of polymorphisms in drug-metabolizing enzymes or drug receptors.2,12
The usefulness of these concepts lies in theirability to increase the clinician’s awareness ofdifferences and the threshold for consideringalternative treatment modalities, but not forlimiting options in diagnosis or treatment for anindividual patient. To do otherwise would be tostereotype in ways that could, in turn,contribute to the inequities reflected in healthdisparities. In addition to the physiologicalcomplexities associated with appropriateprescribing for different racial and ethnicgroups, practitioners face the added challengeof delivering effective pharmaceutical care tothese individuals within a psychosocial contextappropriate to their cultural beliefs andpractices. The great diversity in our patientpopulation demands a framework in which thepractitioner can approach all patients asegalitarian partners in care, regardless ofcultural background.
Although any discussion of socioculturalcompetence can list examples of ourdifferences, it is important to remember themany similarities among diverse peoples. Allpatients seeking care have recognized a needfor that care. All share feelings of need, fear,mistrust, lack of control, hope, anddisconnection from their normal worlds ofhealth. When these feelings are acknowledgedand respected by a culturally competentpractitioner, partnerships can be built in whichany cultural health belief or treatmentpreference can be discussed.

7
Terms Used in This Report:
• Ethnicity and Culture – Refer to combinations of socioeconomic, religious, and political qualitiesof human groups, including language, diet, dress, religions, customs, beliefs, worldviews,kinship systems, and historical or territorial identity.
• Extensive Metabolizer – An individual who metabolizes a drug at a normal rate of efficiency.
• Health Literacy – The ability of an individual to understand and follow through on healthinformation matters.
• Pharmacodynamic Properties – Effect of a drug on the body.
• Pharmacogenetics – The study of variations in a gene on drug response.
• Pharmacogenomics – The study of variations in multiple genes on drug response.
• Pharmacokinetic Properties – Absorption, distribution, metabolism, excretion of a drug.
• Polymorphisms – Naturally occurring variations in the structures of genes, drug metabolismenzymes, receptor proteins, and other proteins involved in drug response or diseaseprogression.
• Poor Metabolizer – An individual who does not metabolize a drug efficiently.
• Racial Group – A group of people who share socially constructed differences based on visiblecharacteristics or regional linkages.
Purposes of This Report
This report 1) reviews the interrelated causes ofvariability in response to medicines among racialand ethnic groups; 2) discusses examples ofdrugs to which racial and ethnic groups responddifferently; 3) discusses the implication forpharmaceutical cost containment practices; and4) makes recommendations for health careproviders and policy makers who areresponsible for clinical decisions affectingpatient care.

Disparities in the quality of medical careprovided to patients representing different racialand ethnic groups have been extensivelydocumented.13 The recent report of the Instituteof Medicine (IOM), "Unequal Treatment:Confronting Racial and Ethnic Disparities inHealthcare," illustrates in detail that racial andethnic disparities in health care do exist and areprevalent in both the treatment of medicalillness and in the delivery of health careservices to minorities in the U.S.14
Of greater significance is the finding that thesedisparities still exist even after adjustment fordifferences in socioeconomic status, insurancecoverage, income, age, co-morbid conditions,
expression of symptoms, and access-relatedfactors. These disparities are not confined to anyone aspect of health care, and can also befound in the delivery of pharmaceutical services.
Most studies have focused on AfricanAmericans, but other studies have shown thatHispanic and Asian Americans are similarlyaffected. Patients in these groups receive lessintensive medical treatment than the nation as awhole, including fewer vaccinations, less drugtherapy for pain, fewer antiretroviral drugs forHIV/AIDS, and fewer antidepressants.15,16,17,18,19,20
Low-income Hispanic children with asthma wereless likely than their white and African Americancounterparts to have taken inhaled beta-agonistor anti-inflammatory medications beforehospitalization.21
African American and Hispanic patients withsevere pain are less likely than white patients tobe able to obtain commonly prescribed painmedicines, because pharmacies inpredominantly non-white communities do notcarry adequate stocks of opiates.22 Other studieshave revealed undertreatment of Hispanics andAfrican Americans for pain from fractures,inadequate management of postoperative painin non-white patients, and a lower likelihood of
curative surgery for cancerin African Americans thanin whites of equivalentsocioeconomic status.20
Disparities in the quantityand quality of carereceived can stem from avariety of causes. Thereare often communicationobstacles between apatient and provider thatcan be due to language, adifference in culturalbackground, preconceivedstereotypes, or incorrectassumptions about whatthe patient does and doesnot understand abouttheir health. This can leadto noncompliance withprescribed treatments andineffective managementof disease.
8
DISPARITIES IN HEALTH CARE
Figure 1. Diversity of the U.S. Population
Source: Bureau of Census data for 2000.
White
HispanicBlack or African
American
Asian
American Indian andAlaska Native
Two or more races
Other
Native Hawaiian andOther Pacific Islander
The recent report of the Institute of Medicine(IOM), "Unequal Treatment: Confronting Racialand Ethnic Disparities in Healthcare," illustratesin detail that racial and ethnic disparities inhealth care do exist and are prevalent in boththe treatment of medical illness and in thedelivery of health care services to minorities inthe United States.

9
The demographic changes anticipated over thenext decade magnify the importance of thesedisparities. According to the 2000 census, racialand ethnic groups other than “white” make upalmost one third of the U.S. population (Figure1). African Americans and Hispanics represent agrowing percentage of the urban population inthe U.S. These groups constitute the new urbanmajority in cities such as Washington, Detroit,and Los Angeles.
A disproportionate fraction of these urbanAmericans depend on Medicare or Medicaid astheir sole health care payer. As drug coveragepolicies within these programs evolve, theymust account for the special needs of a growingpercentage of the patient groups they are
intended to serve. These groups may be furtherdisadvantaged if they do not have access toindividualized care with appropriatepharmaceuticals.
Common Cultural Themes and Health Beliefs of the Dominant Society in the U.S.
Although not universal, there are some common themes and health beliefs of the dominantsociety in this country. These broad concepts are only crude indicators and certainly do notcharacterize the thinking of all Americans. On the other hand, neither are they necessarily heldonly by the non-Hispanic white majority. The authority of the dominant society has beeninternalized by many groups. In addition to ethnic and cultural differences, generational andgender factors are also likely to be important determinants of health beliefs for Americans. Somecommon themes include:23
• A relative intolerance of pain. Unlike many other culturally held beliefs, where pain is seen aspart of life, the typical Western attitude toward pain is to relieve it as soon as possible.
• A high expectation that one’s disease can and will be cured or at least “managed.”
• The need to leave the doctor’s office with a prescription.
• The belief that medications should be powerful but free of risk, and that strong medicationsshould be available only by prescription.
• A belief in the magic of high technology and one’s entitlement to it.
• The belief that management of microbes is more important than bolstering resistance to them.
• The belief that the physical aspects of disease are separate from its emotional and spiritual dimensions.
• The belief that the body is a machine and that proper maintenance (diet, exercise) will prolongits useful life; and that technology enables replacement of defective or worn out parts.
• A belief in the sanctity of the doctor-patient relationship and the right to individualized treatment.
• A belief that mental diseases are not as important, or as “real” as somatic diseases.

Disparities in Cultural Competency
At the most basic level, care may becompromised due to cross-cultural language andother communication barriers. For instance,among adult Hispanics with asthma who spokeonly Spanish, there was a greater likelihood ofmissed follow-up appointments, non-adherenceto medications, and emergency room visitsamong those whose physician spoke only Englishcompared to those with bilingual physicians.24
Culturally shaped beliefs play a vital role indetermining whether an explanation of illness ortreatment makes sense. Indigenous systems ofhealth beliefs, practices and medicines exist inall societies and exert profound influence onpatients’ attitudes and behaviors.25,26 Sincecultural beliefs may greatly influence treatmentoutcomes, it is important to assess thelikelihood that a patient will act on these beliefs.
One strategy for improving cultural competenceamong health care providers is for health careproviders themselves to better reflect thediversity of those they serve. One in fourAmericans is non-white, Hispanic, or NativeAmerican, but fewer than 10 percent of those inthe health professions workforce represent theseminority groups.27 African American and Hispanicphysicians make up only 2.2 percent and 2.8percent of all practicing physicians in Americarespectively, a woefully inadequate number tocare for these groups, each of which exceeds 10 percent of the population. Health care providerorganizations that effectively close this gap willachieve a competitive advantage in serving theneeds of their ethnically diverse customers.
While ideally patients would be matched withproviders of similar backgrounds, realistically wemust find ways to train all health care providersto be sensitive to the sociocultural beliefs thatmay influence the effectiveness of anyprescribed treatment regimen. A mismatchbetween lay andprofessional perspectivesoften results in patients’dissatisfaction withtreatment.28,29,30
Disparities in Health Literacy
Health literacy refers to the set of skills neededto read, understand, and act on basic healthcare information. Over 90 million adults in theU.S. have low health literacy skills, with limitedability to read and understand the instructionscontained on prescriptions or medicine bottles,appointment slips, informed consentdocuments, insurance forms, and healtheducational materials.31
Members of socioculturally disadvantagedgroups, especially those for whom English is asecond language, are more likely than educatedor socioeconomically advantaged adults to havelimited literacy skills, thus impacting their abilityto understand and follow prescribed health careregimens.31,32 There is a relationship between lowliteracy and self-management skills, including theability to take medications properly. For example,asthma patients with lower literacy levels werefound to have a relatively poorer technique whenusing their metered-dose inhaler.33
In another case, many patients receiving acutecare at two urban hospitals were unable to readand understand basic medical instructions.34
Forty-two percent did not understand directionsfor taking medication on an empty stomach, andtwenty-six percent did not understand informationon scheduling their next appointment. Thirty-fivepercent of the English-speaking patients hadinadequate or marginal functional literacy, but forthe Spanish-speaking patients, the figure waseven higher (62 percent).
For some serious chronic diseases, such asdiabetes, low health literacy poses acompounded threat to overall health. Becauseself-management relies heavily on printedinstructions, literacy is a key factor. A study oflow-income African American patients with non-insulin-dependent diabetes found the functionalhealth literacy level was adequate in only 25 to
10
One in four Americans is non-white, Hispanic, orNative American, but fewer than 10 percent ofthose in the health professions workforcerepresent these minority groups.

11
47 percent of patients at diabetes clinics.35
Another study found that patients withinadequate health literacy were more likely tohave poor control of their blood sugar levels andto report eye problems (usually involving bloodvessels of the retina) which may progress toblindness.36
Furthermore, low-literacy patients did not readilyidentify themselves; 43 percent of those withlow health literacy denied having any difficulty inreading; 54 percent of those with low-literacysaid they did not usually ask anyone to helpthem read medical forms, and only 29 percentreported asking someone (usually relatives orneighbors) to help them read the writtenmaterials given to them. Such patients wereleast likely to ask their physician for help.35
Standard patient informational practices havebeen shown to be insufficient to overcome thebarriers posed by low health literacy.37 Often,health educational materials are written at aninappropriate reading level, especially for minoritygroups in which English may be a secondarylanguage. For example, in one study, althoughmany American Indian diabetic patients scored ata 5th grade reading level, the diabetes education
materials designed for them were written at a10th grade reading level.38 In another example,less than half of the cancer education materialsspecifically targeting African Americans reflectedthe cultural values of African Americans, and fewwere written at a reading grade level for thosewith low literacy skills.39
Although much effort has been devoted toimproving the quality of written information,improvement in oral and visual communicationto convey necessary medical information hasreceived inadequate attention.37 Health carepractitioners are therefore challenged tocommunicate clearly and concisely withpatients and to take a patient-focused approachto care. This also involves perceiving andsurmounting less visible barriers such aspatient confidence, shame, or fear. Practitionersmust be able to communicate effectively acrosscultural, socio-economic, educational, andgeographical differences.
Practitioners must be able to communicateeffectively across cultural, socio-economic,educational, and geographical differences.
The Language of Medicine
Due to the highly technical nature of the language of medicine, patients may not understandseemingly common medical terms. Compounding the problem is the skill of patients inconcealing their poor health literacy. They usually will not acknowledge their deficiency due tofeelings of shame, even though it interferes with their health.40
In a study of health vocabulary, only 13 percent of participants understood the meaning of the word“terminal,” only 18 percent understood “malignant,” and only 35 percent understood “orally.”41
In a study of Medicare patients, striking deficiencies were found in their understanding ofcritical areas of health care:42
• 48 percent did not understand written instructions to “take medicine every six hours.”• 68 percent could not interpret a blood sugar level.• 27 percent did not understand “take medicine on an empty stomach.”• 27 percent could not identify their next appointment.• 100 percent could not understand a statement of Medicaid rights written at a 10th grade
reading level.

12
INTERPLAY OF ENVIRONMENTAL, GENETIC, AND
CULTURAL FACTORS
The factors contributing to variability in drugresponse are complex and interrelated (Figure2). Differences in drug response among racialand ethnic groups are determined byenvironmental, genetic and cultural (in thiscontext, psychosocial) factors. These factorsmay operate independently or they may interactdynamically and synergistically.
Environmental Factors
Environmental factors – diet, climate, smoking,alcohol, drugs, pollutants, and environmentaltoxins – may cause wide variations inpharmacological response within an individualand even wider variations between groups ofindividuals.43 Several of these factors canoperate simultaneously in the same individual,thus affecting the processes of drug absorption,distribution, metabolism, excretion, andreceptor interaction in different ways and todifferent degrees.44
Differences in diet may significantly alter themetabolism rate or the amount of a drugpresent in the blood among different ethnicpopulations. Studies comparing the metabolismof a specific drug (antipyrine) between AsianIndians in rural villages and Indian immigrants inEngland demonstrated that, as immigrantsadopted the lifestyle and dietary habits of theBritish, their drug metabolism accelerated.
Similar findings have been observed amongSudanese and Western Africans.45
Additionally, smoking can be an important factorin determining response to pharmaceuticals.This is of particular note since cigarette smokingaccelerates the metabolism of manyprescription drugs commonly used to treatchronic diseases such as asthma and high bloodpressure, thereby making them less effective.However, some drugs used to treat theseconditions are not affected by smoking;prescribing can be individualized to use theseagents in smokers.46
Smoking-related disease and mortality isdisproportionately prevalent among AfricanAmericans. Up to 45 percent of urban-dwellingAfrican Americans reported that they weresmokers, compared with 25 percent for thegeneral population.47,48 The smoking patterns ofAfrican Americans are very different from thoseof whites.49 African Americans smoke fewercigarettes per day (15 vs. 25 for whites), prefermentholated and higher tar or nicotinecigarettes, and are more likely to smoke within10 minutes of awakening.49,50 African Americansalso metabolize nicotine more slowly and havehigher serum nicotine metabolite levels percigarette smoked than whites.9,10 They may alsodevelop dependence at lower levels of smoking,making it more difficult for them to quit.49,51,52 The
Figure 2. Factors Contributing to Variability in Drug Response
Adapted from Poolsup et al43

13
Human Migration:The Distribution of Genetic Polymorphisms
Anatomically modern humans evolved in Africa about 100,000 years ago.55 Some of these peoplemigrated from East Africa into Eurasia, and subpopulations spread east into southern Asia. Australiawas inhabited around 50,000 years ago (and subsequently remained completely isolated from the restof the world until the late 18th century). Modern humans first inhabited Western Europe about 40,000years ago. The northern latitudes were penetrated quite late. Following the habitation of Siberia 15,000to 35,000 years ago, humans spilled into Alaska and rapidly occupied the whole of the North andSouth American continents. The Pacific islands were colonized by peoples originating in South Chinabeginning about 5500 years ago and continuing into the historic period.56 Human populationscontinued to migrate throughout prehistoric and historic times, displacing, coexisting, or intermixingwith indigenous peoples. The result is that there are no distinct geographic boundaries betweengenetic variations; rather, there are gradations in the prevalence of polymorphisms acrossgeographical distance.
Two factors led to genetic differences among peoples and hence potentialdifferences in drug response. First, genetic mutations continued to arisespontaneously in populations that were geographically isolated from oneanother. These mutations were subject to environmental selection. Second,because these population movements were initiated by subgroups ofpeople, they tended to represent only a particular subset of the geneticpolymorphisms that were present in the entire human population. Thesmaller the migrant subgroup, the more genetically distinct it would be fromother subgroups – a phenomenon called the “founder effect” – leading todistinct patterns of polymorphisms in the descendent populations.
*Much of the material in this section is derived from: Burroughs VJ, Maxey RW, Levy RA.Racial and ethnic differences inresponse to medicines: Towards individualizd pharmaceutical treatment. Journal of the National Medical Association.2002;94(9)(suppl)1-26.
success rate for blacks who try to quit smokingis 34 percent lower than for whites.49 Sustainedrelease bupropion has been found to beparticularly effective as an adjunct to helpAfrican Americans quit smoking.53 The drugseems to alter nicotine metabolism in blacksmore than whites, in addition to its knowneffect as an antidepressant.
Genetic Factors*
Although age and gender affect drug response,the primary biological factor impacting theeffectiveness of properly followed treatments isgenetics. Studies of twins and blood relativeshave shown that genetic differences are themajor biological factors determining the normalvariation in drug effects, and are responsible formany differences in drug activity among healthysubjects studied under carefully controlledenvironmental conditions. More than 100
examples have been documented in whichinherited individual traits were implicated inatypical, exaggerated responses to drugs, noveldrug effects, or lack of effectiveness of drugs.54
The genetic makeup of an individual maychange the action of a drug in a number of waysas it moves through the body. Genetic factorsmay influence a drug’s action by altering itspharmacokinetic properties (absorption,distribution, metabolism, excretion) orpharmacodynamic properties (effect on thebody). Clinically, there may be an increase ordecrease in the intensity and duration of theexpected typical effect of the drug.
...genetic differences are the major biological factorsdetermining the normal variation in drug effects.

The study of genetically determined variations indrug response is called pharmacogenetics.Variations in drug response are caused by genepolymorphisms, which are naturally occurringvariations in the structures of genes, drugmetabolism enzymes, receptor proteins, andother proteins involved in drug response ordisease progression. Pharmacogeneticstraditionally meant the study of polymorphismsin individual genes. This field now has broadenedinto pharmacogenomics, which examines theeffects of multiple genes on drug response. Inpharmacogenomics, large arrays of genes arestudied in parallel, so that the entire spectrum ofgenes that determine the response to aparticular drug can be examined at one time.
Clinical relevance of genetic differences(polymorphisms)
Common polymorphisms in drug metabolismgenes have received the most attentionbecause they affect the metabolism of manyclinically important and commonly used drugs.Polymorphisms in these genes most oftenaffect drug metabolism by reducing it,sometimes by disrupting it, and occasionally byenhancing it. Individuals who do not metabolizea certain drug efficiently are called “poormetabolizers,” as opposed to normal or“extensive metabolizers.”
Poor metabolizers process drugs over a longerperiod of time, increasing not only the length oftime the body is exposed to a given drug, butalso the concentration of the drug in the
bloodstream, creating the equivalent of anoverdose. Poor metabolizers generally do notexperience increased effectiveness becausedosages are normally targeted to have optimumefficacy and higher dosages do not furtherincrease the effect. However, they often doexperience increased adverse events as if theyhad been given a dose that is too strong. Insum, poor metabolizers have a decreasedtherapeutic ratio (efficacy:toxicity) for thespecific drug.57
It is important to note whether a givenpolymorphism has clinical relevance in drugtherapy. Several factors determine the clinicalimportance of a genetic polymorphism:54
• First, polymorphisms only have clinicalimportance when they result in largedifferences between poor metabolizers andextensive metabolizers.
• Second, differences are relevant chiefly if the drug has a small therapeutic index, i.e.,the ratio of its therapeutic effect to itsadverse effects.
• Third, if physicians adjust drug dosage basedon the therapeutic effect (as is commonpractice with drugs to treat high bloodpressure), then differences between poor and extensive metabolizers are automaticallycorrected.
• Fourth, the clinical implications are broader for widely prescribed drugs such as beta-blockers and tricyclic antidepressants becausemore patients in more population subgroupsare affected.
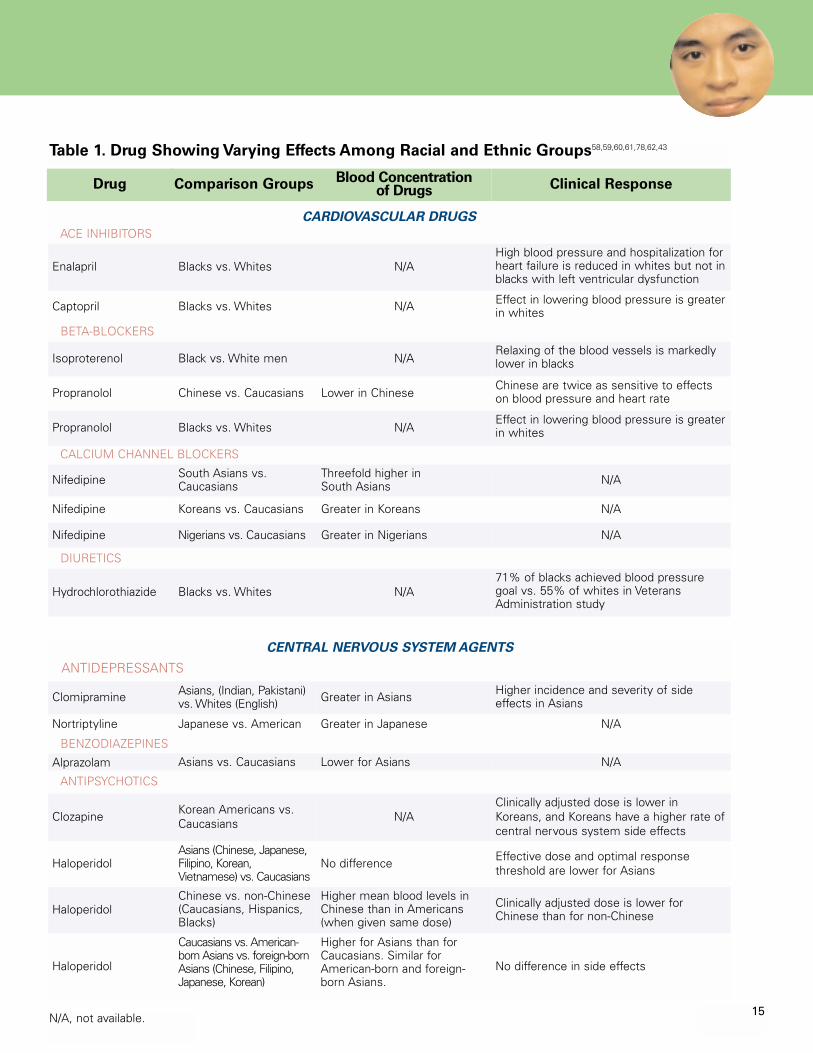
Most pharmacogenetic studies haveconcentrated on several groups of drugs andtheir activity in certain populations. These druggroups include cardiovascular agents and centralnervous system agents (Table 1). Cross-racialvariability in the action of drugs in thesecategories is clinically significant and resultsfrom differences in pharmacokinetic orpharmacodynamic factors, or in thepathophysiology of disease.
14
Factors Determining the Clinical Importance
of a Genetic Variation in Drug Metabolism54
1. There is a notable difference between extensivemetabolizers and poor metabolizers in how the drugaffects the body.
2. The drug has a narrow therapeutic index.
3. The dosage of the drug is not individually evaluatedon the basis of the therapeutic effect.
4. The drug is widely used by many physicians, not onlyby clinical specialists.
15
Drug Comparison Groups Blood Concentration of Drugs Clinical Response
Enalapril Blacks vs. Whites N/AHigh blood pressure and hospitalization forheart failure is reduced in whites but not inblacks with left ventricular dysfunction
Captopril Blacks vs. Whites N/A Effect in lowering blood pressure is greaterin whites
Isoproterenol Black vs. White men N/ARelaxing of the blood vessels is markedlylower in blacks
Propranolol Chinese vs. Caucasians Lower in ChineseChinese are twice as sensitive to effectson blood pressure and heart rate
Propranolol Blacks vs. Whites N/AEffect in lowering blood pressure is greaterin whites
Nifedipine South Asians vs.Caucasians
Threefold higher in South Asians N/A
Nifedipine Koreans vs. Caucasians Greater in Koreans N/A
Nifedipine Nigerians vs. Caucasians Greater in Nigerians N/A
Hydrochlorothiazide Blacks vs. Whites N/A71% of blacks achieved blood pressuregoal vs. 55% of whites in VeteransAdministration study
CARDIOVASCULAR DRUGS
ACE INHIBITORS
BETA-BLOCKERS
CALCIUM CHANNEL BLOCKERS
DIURETICS
Table 1. Drug Showing Varying Effects Among Racial and Ethnic Groups58,59,60,61,78,62,43
Clomipramine Asians, (Indian, Pakistani)vs. Whites (English) Greater in Asians Higher incidence and severity of side
effects in Asians
Nortriptyline Japanese vs. American Greater in Japanese N/A
Alprazolam Asians vs. Caucasians Lower for Asians N/A
Clozapine Korean Americans vs.Caucasians N/A
Clinically adjusted dose is lower inKoreans, and Koreans have a higher rate ofcentral nervous system side effects
HaloperidolAsians (Chinese, Japanese,Filipino, Korean,Vietnamese) vs. Caucasians
No difference Effective dose and optimal responsethreshold are lower for Asians
HaloperidolChinese vs. non-Chinese(Caucasians, Hispanics,Blacks)
Higher mean blood levels inChinese than in Americans(when given same dose)
Clinically adjusted dose is lower forChinese than for non-Chinese
Haloperidol
Caucasians vs. American-born Asians vs. foreign-bornAsians (Chinese, Filipino,Japanese, Korean)
Higher for Asians than forCaucasians. Similar forAmerican-born and foreign-born Asians.
No difference in side effects
CENTRAL NERVOUS SYSTEM AGENTS
ANTIDEPRESSANTS
ANTIPSYCHOTICS
N/A, not available.
BENZODIAZEPINES

16
Racial differences in response to medications
As shown in Table 1, drugs used to treatconditions affecting the cardiovascular systemand the central nervous system are frequentlysusceptible to the effects of geneticpolymorphisms. Within the black population, thecardiovascular effects are especially notable.
High blood pressure is disproportionatelyprevalent in the black population and isassociated with higher incidences ofcerebrovascular and kidney complications andenlargement of the heart. However, the overallrisk of coronary artery disease in the black malepopulation is lower than that in white males,particularly in Europe and the Caribbean, and toa lesser extent in the U.S.
There are general differences in the underlyingcauses of high blood pressure between theblack and white populations. For instance, blackpatients retain more salt and therefore have ahigher incidence of salt-sensitive high bloodpressure. These factors may underlie some ofthe observed differences in the effectiveness ofvarious high blood pressure drugs in blackpopulations. Ultimately, the choice of therapymust be tailored to the individual patient.
Although there is a long-standing discussionabout the best type of drug to use for treatinghigh blood pressure in black patients,63 AfricanAmericans respond to drugs from all classes.2,64
There is no specific class of high blood pressuredrugs that categorically should not be usedbased on race. Diuretics are frequently used tocounteract increased salt retention amongblacks. Although some studies find that beta-blockers, ACE inhibitors, and angiotensinreceptor blocking agents do not control bloodpressure in African Americans with the samedegree of effectiveness as in whites, targetedblood pressure levels can usually be achieved byadding a second agent such as a low-dosediuretic.65,66,67,68,69
The Veterans Administration CooperativeStudies showed that blacks may responddifferently to different beta-blockers. Forexample, the beta-blockers propranolol, nadolol,atenolol, and penbutolol were less effectiveamong blacks than whites, but this differentialeffect can be eliminated by the addition of adiuretic. ACE inhibitors can be as effective inblacks as calcium channel blockers or diuretics,and in some cases they may be more effectiveas a first-line treatment. However, becauselower doses of ACE inhibitors can be lesseffective in black patients, higher doses may berequired than are normally prescribed.70,71,72 Inpatients with high blood pressure complicatedby the presence of other medical conditionssuch as diabetes, ACE inhibitors are first-lineagents in black as well as white patients.73
However, ACE inhibitors appear to be lesseffective in black populations for the preventionand treatment of heart failure in some patients.
Within Asian groups, central nervous systemagents show similar susceptibility to geneticpolymorphisms. In one study, lower dosages ofantidepressants were found to be effective forAsians compared with Caucasians.45 Asiansliving in diverse areas of the world (Los Angeles,St. Louis, Hong Kong, and Beijing) have alsoshown consistently slower metabolism oftranquilizers, suggesting that genetic factors aremore important than environmental factors incontrolling the metabolism of these agents.45
Tricyclic antidepressants have a narrowtherapeutic index and therefore are among themost commonly affected central nervoussystem agents. Poor metabolizers and ultra-extensive metabolizers of these drugs may haveclinical problems when they are taken at usuallyprescribed doses. Poor metabolizers oftendevelop elevated blood concentrations, whichmay result in adverse effects. These side effectsare rarely life threatening, but they aresufficiently unpleasant to cause problems withpatient compliance. Ultra-extensivemetabolizers, on the other hand, may notrespond to recommended doses because drugconcentrations are too low to be effective.
Hispanic patients have been reported to requirelower doses of antidepressants and toexperience more side effects compared withwhite non-Hispanics. Likewise, for a given dose
Hispanic patients have been reported to requirelower doses of antidepressants and toexperience more side effects compared withCaucasians.

17
of an antidepressant, African Americansachieved higher blood levels and fastertherapeutic response, but also more side effectscompared with whites.74
Ethnic groups such as Ashkenazi Jews may alsorespond differently to antipsychotic agents,especially with regard to side effects. A drugused to treat schizophrenia was associated withthe development of a potentially life-threateningblood disorder in 20 percent of Jewish patients,although this adverse reaction develops in onlyabout one percent of chronic schizophrenicpatients in the general population.75 Genetictesting revealed that all of the affectedAshkenazi Jewish patients possessed a specificset of genes that is found in 83 percent ofpatients who developed the disease, but thatthese genes were found in only 8 percent ofschizophrenic patients who did not develop thereaction. This set of genes occurs in 10 to 12percent of the Jewish population in Israel andthe U.S., but is characteristically found in lessthan one percent of the total Caucasianpopulation of the U.S. The increasedsusceptibility of Ashkenazi Jews in this study tothe development of this blood disorder as aresult of drug therapy may be due to the morecommon presence of these genes among thisethnic group.76
Medicines used to treat pain, such as codeine,can be influenced by genetic polymorphisms.This may have important clinical implicationssince codeine is often a drug of first choice forthe treatment of chronic severe pain. Tenpercent of codeine is metabolized in the body tomorphine, from which it derives its painrelieving effect. Poor metabolizers of codeinetherefore receive no therapeutic effect from thedrug, even at higher doses.77 Five to 10 percentof white patients, vs. 1 percent of Asians, lackan enzyme that converts codeine to morphine.But even the 99 percent of Asians who doconvert codeine to morphine experience a
weaker effect than do whites, since they clearmorphine faster and metabolize more rapidlythat portion of codeine that is not converted tomorphine.78
Cultural Factors
Cultural or psychosocial factors, such as theattitudes and health beliefs held by variousgroups, may affect the effectiveness of, oradherence to, a particular drug therapy. However,all persons from different ethnic and culturalgroups share the universal need to be heard, tobe respected, and to be valued. There also aresome common cultural themes shared by all ofthe major ethnic groups. These themes can beorganized into issues of trust and respect, healthbeliefs and practices, and family values. Althoughclearly not confined to a particular population,some specific themes may be more characteristicof some cultural groups than others.79
Trust and respect
Sensitivity, understanding, and respect areessential to building trust. Trust is a vitaldeterminant of treatment adherence and,ultimately, may be more important totherapeutic outcome than any procedure ormedication. Trust is generated within thecontext of doctor-patient interactions, asillustrated below:
• Some cultural groups place great reliance oneye contact, body posture, and other non-verbal communications (facialexpressions, nods of the head, tone of voice).When there is a language barrier, such bodylanguage assumes even greater importance.
• Physical contact is important to some patientswho may feel slighted if the doctor does nottouch them. To others, some physical touchingmay represent a cultural taboo particularlywhen related to gender differences.
Medicines used to treat pain, such as codeine,can be influenced by genetic polymorphismsaffecting central nervous system agents.
Trust is a vital determinant oftreatment adherence and,ultimately, may be more importantto therapeutic outcome than anyprocedure or medication.

18
• Folk religion and healing rituals can be animportant influence in the culture of workingclass immigrants, and a negative response tothese rituals from the physician may beconstrued as a direct assault on their beliefs orreligion. For example, newly arrived Hispanicimmigrants in East Harlem often favor folkmedicine and midwives, the type of healthcare familiar to them in the rural areas of theirhomeland, because they believe that medicineprescribed by an American health careprovider is made of harmful chemicals and istherefore toxic. An example of this is an eight-year-old girl with AIDS who is prescribedseveral medications. “Although the purposeand side effects of each medication have beenexplained to her grandmother, she continuesto use herbal remedies for hergranddaughter’s affliction instead.”80
• Another study of the use of folk healing andhealers by Latinos from Columbia, theDominican Republic and Guatemala living inNew England found that “a major reason fornot using mainstream health care providersmore frequently was the perceived lack ofholistic care and the use of medicines that arenot natural.”81 Family nurse practitionersworking with Mexican-Americans report thatsome of their clients are skeptical of Westernmedicine and only seek it when self-treatmentand folk-healing have been unsuccessful.82
• For patients accustomed to a more formalrelationship with their providers, a casualappearance or attitude may be detrimental tothe development of respect and trust.
• Providers may exhibit discriminatory behaviorstoward minority patients by not involving them in health education or preventativemedicine programs, believing they lack the necessary skills or are otherwise unable to benefit. As a result, referrals to specialistssuch as nutritionists or diabetes educators are sometimes delayed until the disease is advanced.
• Some groups have an inherent distrust of theAmerican health care system. Newly arrivedLatinos in East Harlem viewed health careworkers as extensions of governmentagencies and feared deportation or othernegative consequences.80 For people of Africanheritage, there is a fear of being poisoned: theTuskegee Syphilis Study is often cited asvalidating perceptions of racism andmistreatment.
Health Beliefs and Practices
Although cultural beliefs should be accordedrespect, misinformation or lack of informationshould also be addressed. Problems may occurwhen patients do not tell their physician thatthey are taking herbal remedies or are seeing analternative medicine practitioner. For example,38 percent of Native American patients in anurban health center consulted with a NativeAmerican healer, and patients rated theirhealer's advice higher than their physician'sadvice 61 percent of the time.83 Only 15 percentof those seeing healers disclosed this to theirphysician. In another study, 83 percent of olderLatin patients who reported using an alternativetherapy in the previous month did not tell theirphysicians.84
Patients’ beliefs regarding the properties andeffects of medications are of central importancein determining compliance with treatmentregimens. The following are examples of thecomplex influence of health beliefs andpractices:
• Traditional healing is important among a varietyof population groups, and a dual system ofhealth care services often exists. In a study ofdiverse populations in a metropolitan area, folkmedicine remedies were used in addition to,rather than in place of, formal biomedicalhealth care.85 Although individuals fromdifferent populations often use traditionalpractitioners and treatments, mixed use ofthese health care alternatives appears to bethe most common pattern. Mostcomplementary and alternative medicinetherapies are used by U.S. adults inconjunction with conventional medicalservices. The overall use of these therapies

19
was higher for white non-Hispanic persons (31 percent) than for Hispanic (20 percent) andblack non-Hispanic persons (24 percent).86
• Attitudes toward diet, exercise, smoking,drinking, and body image are imbedded in allcultural beliefs and practices, and theseattitudes affect health and interactions withproviders in important ways.
• Among some culturally-based attitudes is thebelief that people should keep their illnessesto themselves. Persons holding such beliefsmay be likely to seek treatment at later stagesof the disease.
• The belief in fatalism exists among somepopulations, which can influence attitudestoward chronic disease. Even among youngchildren, an attitude of passive acceptance iscommon. A fatalistic attitude impedes a directconfrontation with the consequences ofunhealthy behaviors such as smoking.
• Among a group of older individuals inCalifornia, it was found that in contrast toAfrican Americans, Latinos did not holdmainstream Western views about health andthe management of illness.87 In fact, manyLatinos appeared not to understand themeaning of “chronic” relating to illness, ortheir role in managing their illness beyondtaking medication. They knew they must taketheir medication, but usually thedisappearance of symptoms as a result of themedication was taken to be a cure. Each newepisode was seen as a separate illnessunrelated to previous episodes, particularly inillnesses with multiple symptoms. In addition,
Mexican and Puerto Rican patients werefound to be concerned about the addictive andtoxic effects of medication, and thus reluctantto take medications indefinitely.88,89
• Immigrant minority groups may have accessto controlled substances and othermedications not generally available in the U.S.For example, antibiotic, neuroleptic, anti-emetic, and most other prescription drugs areeasily obtained over the counter in Brazilianpharmacies, and many pain-relievingmedicines are available without a prescription.Once in the U.S., it becomes difficult to obtainthese drugs and persons requiring them on aregular basis often request friends to bring asupply from Brazil.90 In Haiti, manymedications can be purchased without aprescription, so Haitians are often accustomedto keeping numerous topical and oralmedicines on hand to treat various symptoms.For example, an individual who suspects avenereal disease may buy penicillin injectionsand have someone administer them withoutconsulting a physician.90
Folk religion and healing rituals can be animportant influence in the culture ofworking class immigrants, and a negativeresponse to these rituals from thephysician may be construed as a directassault on their beliefs or religion.

20
Problems with Alternative Remedies
The use of alternative remedies and supplements is common. Among a multi-ethnic population,10.4 percent were regular users of alternative medicines; 7.4 percent regularly used non-prescribed vitamin supplements; and 5.3 percent used cod liver oil, primrose oil, or garlic
preparations. People of African origin were more likely to use alternative medicinesthan either whites or South Asians, who were the least common users.91
However the use of complementary and alternative medications can result in druginteractions, disease interactions, adverse reactions, or toxic effects:
• An evaluation of the use of alternative preparations in the El Paso, Texas regionidentified 599 instances of use of such remedies that could result in these effects,based on interviews with 547 survey participants.92
• A survey of Spanish-speaking Latino families visiting a pediatric clinic in Salt LakeCity found that 39 percent of parents from Mexico and 21 percent from othercountries reported using a nonsteroidal anti-inflammatory drug (metamizole)associated with a blood disorder side effect.93 The drug is available over-the-counterin Latin American countries and in markets serving immigrant communities in theU.S.
• Dozens of Chinese herbal remedies available in the U.S. contain the toxin aristolochicacid. The toxin was implicated in an outbreak of kidney trauma in Belgium, possiblycausing cancers in more than 30 people, and is suspected of the same in severalother countries.94 Another study found clinically relevant liver enzyme elevations inabout 1 of 100 patients treated with traditional Chinese drugs.95
Family Values
The strengths of the African American, Asian,Hispanic, and Native American family values,along with extended family, church andcommunity organizations, can be importantresources in supporting the patient and infacilitating adherence to medication and othertreatment regimens. Such networks can providesubstantial support in times of illness.
• Opinions of Asian family members and otherelders are accorded great respect in times ofillness. In Hispanic families, the mother orgrandmother (of the husband especially)usually makes the health care decisions. Inaddition, the needs of the children are alwaysparamount. Health care providers need to beaware of these relationships to optimizeadherence to treatment regimens.
• Family atmosphere may influence response tomedications. Non-Western patients withschizophrenia were found to have more social
support and better clinical outcomes than theirWestern counterparts. Patients whose familymembers expressed frequent criticism,hostility, and emotional over-involvementrelapsed more frequently and required higherdoses of medication.96,97
• Despite the wide use of a variety of non-Western treatments, the actual remedies maynot be perceived to be as critical to care asthe meaning of the cultural memories inherentin acts of caring. For example, within PuertoRican and African American groups, comfort,nurturance, and familiarity were found to be“intrinsic to the holistic nature of theremedies used and to be salient features ofthe memories of healing and curing.”98

21
Effect of cultural factors on medicationcompliance
Patients’ beliefs regarding the properties andeffects of medications are of central importancein determining compliance. For instance, somepatients from non-Western backgrounds areunfamiliar with the practice of taking long-termmedication for chronic illness and with thenotion of accepting unpleasant side effects asthe price for effective treatment. These reasonsmay account for why some patients stop takingtheir medication.99 Variations in attitudes towardmedicines tend to be driven by nationalcharacteristics, culture, and philosophy.100
Immigrants from countries with different non-Western medical cultures may therefore havedifferent expectations regarding the type of drugprescribed, tolerance of side effects, dosageform preference, or other aspects of drugtherapy. This clash between patient and providerexpectations may result in noncompliance withmedications.
In comparison to other societies, Americanmedicine tends to be very aggressive, leadingto a greater focus on the effectiveness oftreatment and a greater tolerance of sideeffects.100 Downward dosage adjustment byAsian patients is common and results from theperception that Western medicines are toostrong and that even relatively benign sideeffects are intolerable.
In Japan, in general, a medicine’s safety profile isstressed more than its effectiveness.101 This“pharmaceutical conservatism” mirrors theJapanese focus on slow and careful building ofpersonal relationships and consensus-basedbusiness decisions.102 This emphasis on safetyand a systematic approach may explain, in part,the general use of lower dosages compared withdosages used in the West, and the lowerincidence of side effects reported by Japanesecompared with American and Europeanpatients.102,103 In addition, patients in Japanfrequently are treated with multiple medicationsbecause Asian patients often believe that multipledrugs are more effective than monotherapy sincemultiple herbal ingredients are usually prescribedby traditional Asian doctors.104
European medicine reflects a middle-positionbetween the poles of American and Japanese
medical cultures. European practices differ interms of the patterns and types of drugsprescribed, the preference for different dosageforms (the French favor suppositories, LatinAmericans expect injections), and diagnoses insome countries that are not used in others(see100 for a detailed discussion).
There is also a general expectation among manycultures that medicines will provide quick relieffrom symptoms, and thus do not need to betaken long-term. In some developing countries,medications are customarily prescribed for onlya day or two.105 These beliefs may reflect theirexperiences with indigenous herbalpreparations, which generally cause fewer sideeffects, and with analgesics and antibiotics,which work rapidly.28 Hispanics and Asians oftenexpect rapid results and are cautious about theside effects of Western medicines.106,107 Thesebeliefs may interfere with the acceptance ofdrugs with a delayed onset of action (e.g.,antidepressants).
Lastly, poor health literacy may negativelyimpact patients’ ability to take medicationsproperly. Members of groups for whom Englishis a second language are more likely thansocioeconomically advantaged white adults tohave limited literacy skills, and there is arelationship between low literacy and self-management skills, including taking medicationsproperly.32,108
Downward dosage adjustment by Asianpatients is common and results from theperception that Western medicines are toostrong and that even relatively benign sideeffects are intolerable.
Some patients are unfamiliar with theWestern practice of taking long-termmedication for chronic illness and with thenotion of accepting unpleasant side effectsas the price for effective treatment.

22
THE FUTURE OF INDIVIDUALIZED THERAPY
Technological advances in the 1990s havechanged the nature of pharmacogeneticresearch and its future impact on medicine. Inthe early decades of its existence,pharmacogenetics focused on the enzymesresponsible for drug metabolism. Differences inthe genes encoding these enzymes wereinferred from differences in the structure andactivity of the enzymes themselves. Thefrequencies of polymorphisms in drugmetabolism enzymes were observed to varyamong different populations defined on thebasis of race. Thus, race is one factor (amongmany) that changes the probability that anindividual person will respond to a given drug.
Two features of the genomics revolution, withthe Human Genome Project as its centerpiece,have important consequences for therelationship between drug therapy and race.First, genetic variations are now determined bydirect analysis of genes themselves. Genesequencing (i.e., determination of a gene’snucleotide sequences) has become a rapid andautomated process. Second, the entirespectrum of genes that determine drug behaviorand sensitivity now can be studied genetically.That is, the effect of the entire genome on drugbehavior can be determined rather than theeffect of the individual gene – hence the changefrom pharmacogenetics to pharmacogenomics.In a sense, it is now possible to take a genetic“fingerprint” of an individual and preciselydetermine the presence of polymorphisms inthe genes known to be involved in druginteraction. Thus, instead of a person’s racebeing a marker for the possession ofpolymorphisms involved in drug response, agenotypic profile can determine with certaintywhether or not the individual possesses thesepolymorphisms.
In the future, drug treatment will be individuallytailored rather than based on race or othercategories such as sex or age. However, the fullimpact of these changes will take many years tounfold. Genetic fingerprinting using DNA arraysis already practical, but the knowledge baserelating genomic variations to drug responseand disease progression has not beendeveloped. Observational studies are under wayin which DNA fingerprints are being correlatedwith data present in medical records aboutmedical history and drug response, and it isexpected that the medical records of an entirecountry (Iceland) will be correlated withgenomic data. These developments will surelyhave a profound impact on the ways in whichnew drugs are developed and used.
Continuing research in pharmacogenomics islikely to reveal significant and far-ranginginformation regarding inter-individual and cross-racial differences in the actions of new andexisting drugs. These developments, along withthe increasing prevalence and influence ofpatients from a variety of races and ethnicitiesand the continued pressure to manage healthcare costs, will require programs having the dualobjectives of cost control and individualizedtherapy for a racially and ethnically diversepopulation of Americans. Balancing theseobjectives will challenge health policy makers inthe coming decades.
Continuing research inpharmacogenomics is likely toreveal significant and far-ranginginformation regarding inter-individual and cross-racialdifferences in the actions of newand existing drugs.
It is now possible to take a genetic“fingerprint” of an individual anddetermine precisely the presence ofpolymorphisms in the genes known to beinvolved in drug interaction.

23
As a result of advances in pharmacogeneticsresearch, as well as political and social changesaffecting racial and ethnic groups, moreconsideration is being given to the need forindividualized drug therapy. The availability of abroad range of medicines enables physicians totreat patients with precision and providesoptions when the first agent used is ineffective,not tolerated, or proper compliance is notachievable. Often, one drug cannot simply besubstituted for another of the same classbecause its clinical effects may vary amongracial and ethnic groups due to differences indrug metabolism. In order for health carepractitioners to engage in racially and ethnicallyappropriate prescribing, a wide range of optionsmust therefore remain available.
Policies that arbitrarily limit drug choices stand in opposition to an increasing body ofevidence indicating that drug therapy does themost good (and the least harm) when it istailored to the individual. Individualizedprescribing takes into account a number offactors, among them environmental, genetic,and cultural factors that may affect a drug’seffectiveness and compliance with prescribedtreatment regimens.
These factors are relevant to theimplementation of pharmaceutical costmanagement policies. Such policies mustconsider any possible discriminatory effects onracial and ethnic groups. Limiting access tooptimal medications may produce reduced orunexpected responses in subpopulations.Access to a variety of medications and dosingformulations, especially those enablingsimplified administration (e.g., once-daily orwithout regard to food) can facilitate complianceand may be particularly beneficial for patientswith low health literacy who may have troublefollowing complex instructions. Additionally,patients with low health literacy or languagebarriers may be ill-equipped to understand thelimitations of restrictive policies and the appealsprocesses necessary to obtain a moreappropriate drug. Restricting access tomedications that will provide optimal care cancontribute to existing disparities in health care.
The following recommendations offer practicalsuggestions that could not only benefit thequality of care provided by health care
institutions and physicians, but could also beuseful in controlling health care costs.
1. Health care institutions should implementpharmaceutical cost containment practicesthat are broad and flexible enough to enablerational choices of drugs and formulations forall patients, regardless of race or ethnic origin.
2. Pharmaceutical companies should continue toinclude significant numbers of patients fromvaried racial and ethnic backgrounds in drugmetabolism and clinical trials in cases wheregenetic polymorphism for that drug class isrelevant. The vast majority of drugmanufacturers test and evaluate newpharmacological compounds on populationsubgroups, including racial and ethnicsubgroups. This is likely to reveal drug actionsand side effects specific to these groups, andmay lead to the discovery of therapies ofspecific advantage to these populations. Itmay also reveal cultural barriers to use of thedrug among particular groups.
3. Hospitals, managed care groups, and otherproviders of health care services shouldendeavor to employ practitioners who areracially and ethnically representative of thepatient population being served. There is,however, a short supply of physicians frombackgrounds representing our most importantminority groups. Given this dearth ofproviders, we must seek to train the existinghealth care professionals to provideappropriate care to culturally diverse clients.Provider organizations should develop andinstitute specific training for all practitionerswho have direct patient contact – especiallyphysicians, pharmacists, nurses, andphysician assistants.
4. Health care providers should giveindividualized treatment to each patient. Forthe practicing physician, each patientrepresents a unique and dynamic interactionamong several determinants includingenvironmental, genetic, and cultural. Althoughit may be impossible for a physician toanticipate how a particular patient willrespond in every instance, it is imperative toindividualize therapy with respect to theappropriate choice of both drug and dose, andto make sure that the patient both
CONCLUSIONS AND RECOMMENDATIONS

24
understands and is able and willing to complywith the prescribed treatment.
5. Physicians should be alert to atypical drugresponses or unexpected side effects whenthey treat patients from varied racial andethnic backgrounds. Patients may not betaking the medication properly due tomisunderstood instructions, ormisperceptions of Western medicine or the severity of disease. Dosage adjustmentsmay need to be made for patients fromdifferent groups as supported bypharmacological evidence.
6. Providers should take special care tocommunicate clearly and concisely withpatients for whom there may be a linguisticcommunications barrier or a concern aboutthe patient’s level of health literacy. This also
involves perceiving and surmounting lessvisible barriers such as patient confidence,shame, or fear. Practitioners must be able tocommunicate effectively across cultural,socioeconomic, educational, and geographicaldifferences. Any written materials distributedshould be appropriate to the patient’s level ofhealth literacy and should reinforce spokendialogue.
7. Because advances in pharmacogenomics will improve the ability to individualizetreatment, all who are involved in patient care should actively monitor developments in this area to take advantage of newdiagnostic and therapeutic technologies as they become available.

25
1. Owens K, King MC. Genomic views of human history.Science. 1999;286(5439):451-453.
2. Schwartz RS. Racial profiling in medical research. N Engl J Med. 2001;344(18):1392-1393.
3. Gaines AD. "Race and Racism." In Encyclopedia ofBioethics. Warren T. Reich (Ed.). Second Edition. New York:Macmillan. Volume 4:2189-2201;1995.
4. Gamble V. Race and the New Genetics: A HistoricalPerspective. Paper presented at: The Implications ofGenetics for Health Professional Education; October 25-28, 1998; Santa Fe, New Mexico.
5. Bhopal R. Is research into ethnicity and health racist,unsound, or important science? British Med J.1997;314(7096):1751-1756.
6. Lee S, Mountain J, Koenig BA. The meanings of “race” inthe new genomics: implications for health disparitiesresearch. Yale J Health Policy Law Ethics. 2001;1:33-75.
7. Geertz C. Interpretation of Culture. New York: Basic Books.1972.
8. Anderson B. Imagined Communities: Reflections on theOrigin and Spread of Nationalism. Revised Edition ed.London and New York: Verso, 1991.
9. Caraballo RS, Giovino GA, Pechacek TF, et al. Racial andethnic differences in serum continine levels of adultcigarette smokers: Third National Health and NutritionExamination Survey, 1988-1991. JAMA. 1998;280:135-139.
10. Perez-Stable EJ, Herrera B, Jacob P, Benowitz NL.Nicotine metabolism and intake in black and whitesmokers. JAMA. 1998;280:152-156.
11. Benowitz NL, Perez-Stable EJ, Herrera B, Jacob P III.Slower metabolism and reduced intake of nicotine fromcigarette smoking in Chinese-Americans. J Natl CancerInst. 2002;94:108-115.
12. Wood AJ. Racial differences in the response to drugs--pointers to genetic differences. N Engl J Med. May 32001;344(18):1394-1396.
13. Fiscella K, Franks P, Gold MR, Clancy CM. Inequality inquality: addressing socioeconomic, racial, and ethnicdisparities in health care. JAMA. 2000;283(19):2579-2584.
14. Institute of Medicine Report. Unequal Treatment:Confronting Racial and Ethnic Disparities in Healthcare.Washington, DC: National Academy Press; 2002.
15. Bach PB, Cramer LD, Warren JL, Begg CB. Racialdifferences in the treatment of early-stage lung cancer. N Engl J Med. 1999;341:1198-1205.
16. Bernabei R, Gambassi G, Lapane K, et al. Managementof pain in elderly patients with cancer. JAMA.1998;279:1877-1882.
17. Moore RI, Stanton D, Gopalan R, Chaisson RE. Racialdifferences in the use of drug therapy for HIV disease inan urban community. N Engl J Med. 1994;330:763-768.
18. Shapiro MF, Morton SC, McCaffrey DF, et al. Variations inthe care of HIV infected adults in the United States:Results from the HIV Cost and Services Utilization Study.JAMA. 1999;281:2305-2375.
19. Schneider EC, Leape LL, Weissman JS, Piana RN,Gatsonis C, Epstein AM. Racial differences in cardiacrevascularization rates: does “overuse” explain higherrates among white patients? Ann Intern Med.2001;135(5):328-337.
20. Freeman HP, Payne R. Racial Injustice in health care. NEngl J Med. 2000;342(14):1045-1047.
21. Finkelstein JA, Brown RW, Schneider LC, et al. Quality ofcare for preschool children with asthma: the role of socialfactors and practice setting. Pediatrics. 1995;95:389-394.
22. Morrison RS, Wallenstein S, Natale DK, Senzel RS,Huang LL. “We Don’t Carry That”—Failure of pharmaciesin predominately nonwhite neighborhoods to stockopioid analgesics. N Engl J Med. 2000;342:1023-1026.
23. Levy R, Hawks J. Cultural Diversity in PharmaceuticalCare. Reston, VA: National Pharmaceutical Council; May1999.
24. Manson A. Language concordance as a determinant ofpatient compliance and emergency room use in patientswith asthma. Med Care. 1988;26:1119-1128.
25. Kleinman A, Eisenberg L, Good B. Culture, illness, and cure.Ann Intern Med. 1978; 88:251-258.
26. Landy D, editor. Culture, Disease, and Healing: Studies inMedical Anthropology. New York, MacMillan; 1977.
27. HRSA. Assuring Access to Essential Health Care. U.S.Department of Health and Human Services. 1998.
28. Smith M, Lin KM, Mendoza R. Non-biological IssuesAffecting Psychopharmacotherapy: CulturalConsiderations. In: Lin KM, Poland RE, Nakasaki, editors.Psychopharmacology and Psychobiology of Ethnicity.Washington, DC: American Psychiatric Press; 1992.
29. Young J, Garro LY. Variation in the choice of treatment in twoMexican communities. Soc Sci Med. 1982;16:1463-1466.
30. Borkan JM, Quirk M, Sullivan M. Finding meaning afterthe fall: injury narratives from elderly hip fracturepatients. Soc Sci Med. 1991;33:947-957.
31. Kirsch IS, Jungebut A, Jenkins L, Kolstad A. AdultLiteracy in America: A First Look at the Results of theNational Adult Literacy Survey. Washington, DC:Department of Education; 1993.
32. Reder S. The state of illiteracy in America: Estimates atthe local, state, and national levels. Washington, DC:National Institute for Literacy; 1998.
REFERENCES

26
33. Williams, MV, Baker, DW, Honig, EG, Lee TM, Nowlan A.Inadequate literacy is a barrier to asthma knowledge andself-care. Chest. 1998;114(4),1008–1015.
34. Williams MV, Parker RM, Baker DW, Parikh K, CoatesWC, Nurss JR. Inadequate functional health literacyamong patients at two public hospitals. JAMA.1995;2714(21):1677–1682.
35. Nurss JR, el-Kebbi IM, Galliana DL, Zeimer DC, MuseyVC, Lewis S, Liao Q, Philips LS. Diabetes in urban AfricanAmericans: Functional health literacy of municipalhospital outpatients with diabetes. Diabetes Educ.1995;23(5):563–568.
36. Schillinger D, Grumbach K, Piette J, et al. Association ofhealth literacy with diabetes outcomes. JAMA.2002;288:475-482.
37. Williams MV, Baker DW, Parker RM, Nurss JR.Relationship of functional health literacy to patients’knowledge of their chronic disease: A study of patientswith hypertension and diabetes. Arch Intern Med.1998;158(2):166–172.
38. Hosey GM, Freeman WL, Stracqualursi F, Gohdes D.Designing and evaluating diabetes education material forAmerican Indians. Diabetes Educ. 1990;16(5):407–414.
39. Guidry JJ, Fagan P, Walker V. Cultural sensitivity andreadability of breast and prostate printed cancer educationmaterials targeting African Americans. J Natl Med Assn.1998;90(3):165–169.
40. Williams MV. Recognizing and overcoming inadequatehealth literacy, a barrier to care. Cleve Clin J Med.2002;69(5):415-418.
41. Gibbs R, Gibbs P, Heinrich J. Patient understanding ofcommonly used medical vocabulary. J Fam Practice.1987;25:176-178.
42. Guzmararian JA, Baker DW, Williams MV, et al. Healthliteracy among Medicare enrollees in a managed careorganization. JAMA. 1999;281:545-551.
43. Poolsup N, Li Wan Po A, Knight TL. Pharmacogeneticsand psychopharmacotherapy. J Clin Pharm Ther.2000;25(3):197-220.
44. Vesell ES. The influence of host factors on drugresponse, I: ethnic background. Ration Drug Ther.1979;13(8):1-7.
45. Lin KM, Poland RE. Ethnicity, culture, andpsychopharmacology. In: Bloom FF, Kupfer DJ, editors.Psychopharmacology. The Fourth Generation of Progress.Nashville, TN: American College ofNeuropsychopharmacology; 2000.
46. Benowitz, NL. Substance Abuse: Dependence andTreatment. In: Melmon KL, Morelli HF, Hoffman BB,Nierenberg DW, editors. Clinical Pharmacology, BasicPrinciples in Therapeutics. New York: McGraw Hill; 1992.
47. Resnicow K, Futterman R, Weston RE, Royce J, Parms C,Freeman HP, Orlandi MA. Smoking prevalence in Harlem,New York. Am J Health Promot. 1996;10:343-346.
48. Ahluwalia JS, McNagny SE. Smoking prevalence anddesire to quit in inner city African American walk in clinicpatients. Clin Res.1993;41:752A.
49. Royce JM, Hymowitz N, Corbett K, Hartwell TD, OrlandiMA, for the COMMIT Research Group. Smokingcessation factors among African Americans and whites.Am J Public Health. 1993;83:220-226.
50. Kabat GC, Morabia A, Wynder EL. Comparison ofsmoking habits of blacks and whites in a case-controlstudy. Am J Public Health. 1991;81:1483-1486.
51. Giovino GA, Schooley MW, Zhu BP, et al. Surveillance forselected tobacco-use behaviors - United States, 1900-1994. Mor Mortal Wkly Rep CDC Surveill Summ.1994;43:1-43.
52. Fiore MC, Novotny TE, Pierce JP, Hatziandreu EJ, PatelKM, Davis RM. Trends in cigarette smoking in the U.S.;the changing influence of gender and race. JAMA.1989;261:49-55.
53. Ahluwalia JS, Harris KJ, Catley D, Okuyemi KS, MayoMS. Sustained-release bupropion for smoking cessationin African Americans. A randomized controlled trial.JAMA. 2002;288:468-474.
54. Meyer UA. Drugs in special patient groups: clinicalimportance of genetics in drug effects. In: Melmon KL,Morrelli HF, Hoffman BB, Nierenberg DW, editors.Melmon and Morrelli’s Clinical Pharmacology: BasicPrinciples in Therapeutics. New York, NY: McGraw-Hill,Inc; 1992.
55. Cavalli-Sforza LL. Genes, Peoples, and Languages. NewYork, NY: North Point Press; 2000.
56. Diamond J. Guns, Germs, and Steel. The Fates ofHuman Societies. New York, NY: W.W. Norton & Co;1999; 281:545-551.
57. Evans WE, Relling MV. Pharmacogenomics: translatingfunctional genomics into rational therapeutics. Science.1999;286(5439):487-491.
58. Wood AJ, Zhou HH. Ethnic differences in drugdisposition and responsiveness. Clin Pharmacokinet.1991;20(5):350-373.
59. Veterans Administration Cooperative Study Group onAntihypertensive Agents. Comparison of propranolol andhydrochlorothiazide for the initial treatment ofhypertension, II: results of long-term therapy. JAMA.1982;248:2004-2011.
60. Exner DV, Dries DL, Domanski MJ, Cohn JN. Lesserresponse to angiotensin-converting-enzyme inhibitortherapy in black as compared with white patients withleft ventricular dysfunction. N Engl J Med.2001;344:1351-357.

27
61. Lang CC, Stein CM, Brown RM, et al. Attenuation ofisoproterenol-mediated vasodilatation in blacks. N Engl JMed. 1995;333:155-160.
62. Veterans Administration Cooperative Study Group onAntihypertensive Agents. Comparison of propranolol andhydrochlorothiazide for the initial treatment ofhypertension, I: results of short-term titration withemphasis on racial differences in response. JAMA.1982;248:1996-2003.
63. Saunders E. Drug treatment considerations for thehypertensive black patient. J Fam Pract. 1988;26(6):659-664.
64. Flack JM, Mensah GA, Ferrario CM. Using angiotensinconverting enzyme inhibitors in African-Americanhypertensives: a new approach to treating hypertension andpreventing target-organ damage. Curr Med Res Opin.2000;16:66-79.
65. Flack JM, Saunders E, Gradman A, et al.Antihypertensive efficacy and safety of losartan aloneand in combination with hydrochlorothiazide in adultAfrican Americans with mild to moderate hypertension.Clin Ther. 2001; 23:1193-1208.
66. Prisant LM, Mensah GA. Use of beta-adrenergic receptorblockers in blacks. J Clin Pharmacol. 1996;36(10):867-873.
67. Richardson AD, Piepho RW. Effect of race onhypertension and antihypertensive therapy. Int J ClinPharmacol Ther. 2000;38:75-79.
68. Cushman WC, Reda DJ, Perry HM, Williams D, AbdellatifM, Materson BJ. The Department of Veterans AffairsCooperative Study Group on Antihypertensive Agents.Regional and racial differences in response toantihypertensive medication use in a randomizedcontrolled trial of men with hypertension in the UnitedStates. Arch Intern Med. 2000;160:825-831.
69. Saunders E, Weir MR, Kong W, et al. A comparison of theefficacy and safety of a beta-blocker, a calcium channelblocker, and a converting enzyme inhibitor in hypertensiveblacks. Arch Intern Med. 1990;150:1707-1713.
70. Racial differences in response to low-dose captopril areabolished by the addition of hydrochlorothiazide. Br J ClinPharmacol. 1982;14(suppl 2):97S-101S.
71. Chrysant SG, Brown RD, Kem DC, Brown JL.Antihypertensive and metabolic effects of a newconverting enzyme inhibitor, enalapril. Clin PharmacolTher. 1983;33(6):741-746.
72. Goodman C, Rosendorff C, Coull A. Comparison of theantihypertensive effect of enalapril and propranolol inblack South Africans. S Afr Med J. 1985;67(17):672-676.
73. Gibbs CR, Beevers DG, Lip GY. The management ofhypertensive disease in black patients. QJM.1999;92(4):187-192.
74. Strickland TL, Ranganath V, Lin KM, Poland RE, MendozaR, Smith MW. Psychopharmacologic considerations inthe treatment of black American populations.Psychopharmacol Bull. 1991;27(4):441-448.
75. Lieberman JA, Yunis J, Egea E, Canoso RT, Kane JM,Yunis EJ. HLA-B38, DR4, DQw3 and clozapine-inducedagranulocytosis in Jewish patients with schizophrenia.Arch Gen Psychiatry. 1990;47(10):945-948.
76. Turbay D, Lieberman J, Alper CA, et al. Tumor necrosisfactor constellation polymorphism and clozapine-inducedagranulocytosis in two different ethnic groups. Blood.1997;89(11):4167-4174.
77. Meyer UA, Zanger UM. Molecular mechanisms ofgenetic polymorphisms of drug metabolism. Annu RevPharmacol Toxicol. 1997;37:269-96.
78. Xie HG, Kim RB, Wood AJ, Stein CM. Molecular basis ofethnic differences in drug disposition and response.Annu Rev Pharmacol Toxicol. 2001;41:815-50.
79. Habits for Health. Health Care in a Diverse World.[audiotapes with JR Gavin III, JA Davidson, H Than, andWP Newman]. Somerville, NJ: Hoechst-RousselPharmaceuticals, 1992.
80. Canlas LG. Issues of health care mistrust in East Harlem.Mt Sinai J Med. 1999;9;66(4):257-258.
81. Zapata J, Shippee-Rice R. The use of folk healing andhealers by six Latinos living in New England: apreliminary study. J Transcult Nurs. 1999;4;10(2):136-142.
82. Gonzalez-Swafford MJ, Gutierrez MG. Ethno-medicalbeliefs and practices of Mexican-Americans. Nurse Pract.1983;11-12;8(10):29-30,32,34.
83. Marbella AM, Harris MC, Diehr S, Ignace G, Ignace G.Use of Native American healers among Native Americanpatients in an urban Native American health center. ArchFam Med. 1998;3-4;7(2):182-185.
84. Sleath B, Rubin RH, Campbell W, Gwyther L, Clark T.Ethnicity and physician-older patient communicationabout alternative therapies. J Altern Complement Med.2001;8;7(4):329-335.
85. Becerra RM, Iglehart AP. Folk medicine use: diversepopulations in a metropolitan area. Soc Work HealthCare. 1995;21(4):37-58.
86. Ni H, Simile C, Hardy AM. Utilization of complementaryand alternative medicine by United States adults: resultsfrom the 1999 national health interview survey. MedCare. 2002;4;40(4):353-358.
87. Becker G, Yewoubdar B, Newsom EM, Rodgers DV.Knowledge and care of chronic illness in three ethnicminority groups. Fam Med. 1998;30(3)173-179.
88. Martinez C. Mexican-Americans, In: Comas-Diaz L,Griffith EEH, editors. Clinical Guidelines in Cross-CulturalMental Health. New York: Wiley Series in General andClinical Psychiatry; 1988.

28
89. Ramos-McKay JM, Comas-Diaz L, Rivera LA: PuertoRicans. In: Comas-Diaz L, Griffith EEH, editors. ClinicalGuidelines in Cross-Cultural Mental Health. New York:Wiley Series in General and Clinical Psychiatry; 1988.
90. Purnell LD, Paulanka BJ, editors. Transcultural HealthCare. A Culturally Competent Approach. Philadelphia, PA:F.A. Davis; 1998.
91. Cappuccio FP, Duneclift SM, Atkinson RW, Cook DG. Useof alternative medicines in a multi-ethnic population. EthnDis. 2001;11(1):11-18.
92. Rivera JO, Ortiz M, Lawson ME, Verma KM. Evaluationof the use of complementary and alternative medicine inthe largest United States-Mexico border city.Pharmacotherapy. 2002;22(2):256-264.
93. Bonkowsky JL, Frazer JK, Buchi KF, Byington CL.Metamizole use by Latino immigrants: a common andpotentially harmful home remedy. Pediatrics.2002;109(6):e98.
94. Mishra, R. Some Chinese herb remedies called toxic.Available at http://www.mdadvice.com/news/2001/02/01/medic/2531-0231-pat_nytimes.html.Accessibility verified July 30, 2002.
95. Melchart D, Linde K, Hager S, et al. Monitoring of liverenzymes in patients treated with traditional Chinesedrugs. Complement Ther Med. 1999;7(4):208-216.
96. Jablensky A, Sartorius N, Ernberg G, et al.Schizophrenia: Manifestations, incidence, and course indifferent cultures. A World Health Organization ten-country study. Psychol Med Monogr Suppl. 1992;20:1-97.
97. Lin KM, Kleinman AM. Psychopathology and clinical courseof schizophrenia: a cross-cultural perspective. SchizophreniaBull. 1988;14:555-567.
98. Davis RE. Understanding ethnic women's experienceswith pharmacopoeia. Health Care Women Int.1997;18(5):425-437.
99. Kroll J, Linde P, Habenicht M, et al. Medicationcompliance, antidepressant blood levels, and sideeffects in Southeast Asian patients. J Clin Psychopharm.1990;10:279-283.
100. Payer L. Medicine and Culture: Varieties of Treatment inthe United States. New York: Penguin; 1988.
101. Murao N. Regulatory requirements and practices forclinical studies in Japan. Drug Info J. 1992; 26:333-339.
102. Henderson JT. Medical practice differences betweenEurope, the United States and Japan. In: Walker S,Lumley C, McAuslane N. The Relevance of EthnicFactors in the Clinical Evaluation of Medicines. London:Center for Medicines Research; 1994.
103. Homma M. Requirements for the assessment ofclinical safety regulatory perspectives. Proceedings ofthe First International Conference on Harmonization,1991, Brussels.
104. Binder RL, Kazamatsuri H, Nishimura T, McNiel DE.Tardive dyskinesia and neuroleptic-inducedParkinsonism in Japan. Amer J Psychiatry.1987;44:1494-1496.
105. Mull JD. Cross-cultural communication in thephysician’s office. Western J Med. 1993;159:609-613.
106. Lin KM, Shen WW. Pharmacotherapy for SoutheastAsian psychiatric patients. J Nerv Ment Dis.1991;179:346-350.
107. Westermeyer J. Psychiatric care of migrants: a clinicalguide. Gold JH, ed. Washington, DC: AmericanPsychiatric Press; 1989.
108. Kirsch IS, Jungeblut A, Jenkins L, Kolstad, A. Adultliteracy in America. Washington, DC: U.S. Departmentof Education; 1993.


For more information about NPC or foradditional resources, please contact:
The National Pharmaceutical Council1894 Preston White Drive
Reston, VA 20191-5433
Phone: 703-620-6390Fax: 703-476-0904www.npcnow.org
For more information about NMA or foradditional resources, please contact:
The National Medical Association1012 Tenth Street, N.W.
Washington, DC 20001-4492
Phone: 202-347-1895Fax: 202-842-3293www.NMAnet.org
1ETH0061102