culture psychology 2003 schmitz 383 406
TRANSCRIPT
http://cap.sagepub.com/Culture & Psychology
http://cap.sagepub.com/content/9/4/383The online version of this article can be found at:
DOI: 10.1177/1354067X0394004
2003 9: 383Culture PsychologyMark F. Schmitz, Prema Filippone and Elaine M. Edelman
1997−Social Representations of Attention Deficit/Hyperactivity Disorder, 1988
Published by:
http://www.sagepublications.com
can be found at:Culture & PsychologyAdditional services and information for
http://cap.sagepub.com/cgi/alertsEmail Alerts:
http://cap.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
http://cap.sagepub.com/content/9/4/383.refs.htmlCitations:
What is This?
- Dec 1, 2003Version of Record >>
at Alexandru Ioan Cuza on December 11, 2013cap.sagepub.comDownloaded from at Alexandru Ioan Cuza on December 11, 2013cap.sagepub.comDownloaded from

Abstract Considerable debate has arisen regarding many aspectsof attention deficit/hyperactivity disorder (ADHD), including the
existence, diagnosis and prevalence of the disorder, the use ofmedications in treating young children for the disorder, and the
long-term side-effects of the medications. A fundamental catalystin this debate involves the numerous and diverse social
representations of ADHD: the differing ways of perceiving whatADHD is, whom it affects, and the most appropriate treatments.This paper presents a discussion of social representations theory
and its previous applications to the study of mental illness,connecting this theory with research in media framing.
Quantitative and qualitative content analyses of print mediarepresentations of ADHD over a ten-year period are presented.
Using results from the media analysis, we examine differentprocesses through which these representations might influence
perceptions of individuals experiencing ADHD-relatedsymptoms, particularly as these perceptions relate to mental
health treatment decisions.
Key Words ADHD, content analysis, print media, socialrepresentations
Mark F. Schmitz, Prema Filippone and Elaine M.EdelmanRutgers, The State University of New Jersey, USA
Social Representations of AttentionDeficit/Hyperactivity Disorder,
1988–1997
Today approximately 3–5% of all children in the US have been diag-nosed with some form of attention deficit/hyperactivity disorder(ADHD). A large proportion of these children receive some form ofprescription stimulant medication as the primary treatment modality,although the exact proportion of medication use varies considerablyby age, race and geographic location (National Institutes of Health,1998). Considerable debate has arisen regarding many aspects ofADHD, including the existence, diagnosis and prevalence of thedisorder, the use of medications in treating young children for thedisorder, and the long-term side-effects of the medications (Anderson,1996; Angold, Erkanli, Egger, & Costello, 2000; Cantwell, 1996;
Culture & Psychology Copyright © 2003 SAGE Publications(London, Thousand Oaks, CA and New Delhi) www.sagepublications.com
Vol. 9(4): 383–406 [1354–067X(200312) 9:4; 383–406; 038823]
Article
CAP 9/4 03 Schmitz (ad/t) 15/1/04 2:06 pm Page 383
at Alexandru Ioan Cuza on December 11, 2013cap.sagepub.comDownloaded from

Goldman, Genel, Bezman, & Slanetz, 1998; Morrow, Morrow, &Haislip, 1998; Zito et al., 2000). The present study attempts to showthat a fundamental catalyst in this debate involves the diverse and con-flicting social representations of ADHD: the changing ways in per-ceiving the cause of ADHD, whom it affects, and the most appropriatetreatments.
Given the recent increase of children and adults receiving treatmentfor ADHD (National Institutes of Health, 1998), the social represen-tations of this illness are likely changing dramatically. Indeed, the per-ception of this disorder has evolved considerably over the past century.Beginning with the work of Still and Bradley, the hyperactive child wasviewed in mainly psychoanalytic terms (Bradley, 1937; Still, 1902).Later, Conrad (1976) described the use of the ADHD diagnosis andstimulant prescriptions as a form of social control. Technologicaladvances have resulted in ADHD research focusing on neurobiologyand brain-imaging techniques (Zametkin et al., 1990). The recentincrease in Ritalin production has been linked to the inclusion ofADHD as a learning disability under the 1990 Individuals with Dis-abilities Act (Diller, 1996). Thus, the social representations of ADHDcould be perceived as images involving parenting style, genetics,morality and self-control, social stress, deviance, disability and neuro-biology.
Background
Social Representations Theory and Mental IllnessSocial representations theory is a specific depiction of the processesmore broadly discussed within social constructionist perspectives(Wagner et al., 1999). Social representations refer to the stock ofcommon knowledge that people share as common-sense theories aboutthe social world (Flick, 1998). These cognitive maps act as referencepoints for the selection, categorization and organization of social infor-mation and experiences, and are critical to the process of forming andmaintaining a sense of self (Augoustinos & Walker, 1995). Socialrepresentations theory describes the development of particular socialrepresentations, identifying the ways in which different views of theworld arise from different social environments. Two key processes insocial representations theory are anchoring and objectification, whichentail the reorganization of some idea, object or phenomenon so thatsome parts are omitted and other parts are emphasized (Flick, 1998).
Anchoring, which occurs early in the construction of a socialrepresentation, involves a process of reducing unfamiliar ideas to
Culture & Psychology 9(4)
384
CAP 9/4 03 Schmitz (ad/t) 15/1/04 2:06 pm Page 384
at Alexandru Ioan Cuza on December 11, 2013cap.sagepub.comDownloaded from

ordinary categories and images. For a social group to come to anunderstanding of some novel or unfamiliar phenomenon, it is neces-sary for the members to identify characteristics about the phenomenonthat are familiar. The phenomenon becomes grounded, or anchored,within an already familiar set of terms and representations (Wagner etal., 1999). Through the anchoring process, the unfamiliar becomesembedded in the social classifications already available in everydaycommunications (Flick, 1998). Objectification, which occurs throughfurther discourse in the construction of the social representation, trans-lates abstract concepts into concrete images, weaving the perceivedessence of the phenomenon into the common knowledge of the socialgroup. The particulars of the objectification depend on political,historical and cultural conditions of the social group, through whichcertain social conditions of the group will favor different metaphorsand images that are used in objectification (Wagner et al., 1999).
Moscovici introduced the theory, based on Durkheim’s notion ofcollective representations (Durkheim, 1995), by examining the connec-tions between professional and lay understandings of psychoanalysis,particularly in describing the diffusion of psychoanalytic constructsinto popular belief and language (Moscovici, 1976). Other studies haveused social representations theory to describe the social constructionand representation of phenomena in mental health (de Rosa, 1987;Jodelet, 1991; Zani, 1995). The essential feature within these studies liesin the description and use of social representations to examine socialprocesses through which knowledge becomes distributed acrossdifferent social groups.
Jodelet’s study of the social representations of madness stands as oneof the prototypical studies using social representations theory (Jodelet,1991). Participant observation, intensive interviews and contentanalysis of documents were used to explore lay concepts of mentalillness, madness and the mentally ill. The central concept of the socialrepresentation of mental illness was a naïve theory of madness, domi-nated by a fear of contagion and concern for loss of distance from thementally ill. The participants in the study were members of a Frenchvillage where, for several generations, many villagers had lodgedmentally ill people from a nearby asylum in their own homes. Theimages of fear of contagion and concern for loss of distance explainedmany of the social practices Jodelet observed in the village, practicesthat ran counter to the long-term action of providing housing for thementally ill.
Another study of the social representations of mental illness foundthat the particular images varied significantly by age of the respondent
Schmitz et al. Social Representations of ADHD
385
CAP 9/4 03 Schmitz (ad/t) 15/1/04 2:06 pm Page 385
at Alexandru Ioan Cuza on December 11, 2013cap.sagepub.comDownloaded from

identifying the images (de Rosa, 1987). Young children were morelikely to connect the images of the madman and the deviant with thementally ill; adolescents tended to identify mental illness as a psycho-logical condition. These images were also present among adult respon-dents, as was the image of the mentally ill person as somethingmagical/fantastical (e.g. mythological figures, devils and monstrousfigures). This image of the fantastical was much less likely to beacknowledged verbally, but appeared in drawings by the respondents(both children and adults) when asked to ‘draw as a mad person’. Animportant point from de Rosa’s work is the polymorphous nature ofthe representations of mental illness held by any one individual. Thesedifferent models and images of mental illness typically co-exist withinan individual’s notions about mental illness.
A similar multiplicity of images about the mentally ill, while sharedby different groups of subjects, was found to vary according to the indi-vidual’s social position and experience with mental illness (Zani, 1995).However, respondents from different professional backgrounds andspecialties identified the same basic structure in the representation ofmental illness. Specifically, as compared with their positive perceptionsof a normal person, respondents presented persistently negativeconnotations of mental illness. Furthermore, the mentally ill personwas seen as extremely distant and different from the self; this distinct‘otherness’ was key for respondents in coming to understand and givemeaning to the presence of madness and mental illness (Zani, 1995).
Social Representations and Media FramingThe concepts of anchoring and objectification are similar to the conceptof framing in media analysis. Framing is a process through which acommunication source defines and constructs a public issue or con-troversy, and can have significant consequences for how people viewand understand an issue (Nelson, Clawson, & Oxley, 1997). Mediaframes can shape a person’s understanding by stressing specificfeatures or elements of the issue, thus reducing the complexity to a fewconstructs or aspects that receive particular emphasis in the story orarticle (Gamson, Croteau, Hoynes, & Sasson, 1992). Social represen-tations theory explicitly recognizes these dynamics, particularly in thespecification that representations form a part of culture as well as influ-ence individual cognitive processes (Farr, 1995). The media also servean important role in the construction of social representations, actingas intermediaries between research scientists and lay people (Farr,1993). Thus, a large body of research based on social representationstheory has used content analyses of various media (Farr, 1993, 1995;
Culture & Psychology 9(4)
386
CAP 9/4 03 Schmitz (ad/t) 15/1/04 2:06 pm Page 386
at Alexandru Ioan Cuza on December 11, 2013cap.sagepub.comDownloaded from

Kitzinger, 1995; Kruse, 1998; Moscovici, 1976; Potter & Wetherell, 1998;Sommer, 1998). Our examination of the social representations ofADHD, as presented in the United States, follows in this tradition byusing a content analysis of popular print media.
Methods
Print Media SampleTo obtain a sample of popular magazine and journal articles coveringADHD, the Readers’ Guide to Periodical Literature was searched for theyears 1969 to 1998 for all articles under the headings hyperactivity,hyperkinesis, attention deficit disorder, ADD and ADHD. The journalscovered in the Readers’ Guide include both popular (e.g. Time, Parent-ing and Seventeen) and more specialized titles (e.g. Psychology Today,Scientific American and Science News). A total of 198 articles were found(Figure 1).
Also presented in Figure 1 are the results from a search within theLibrary of Congress listing of books, using the same subject headingsand the same time frame as for the search in the Readers’ Guide toPeriodical Literature. The number of books published on ADHD showeda similar cyclical pattern as in the results from the Readers’ Guide, witha relatively steady interest during the mid-seventies and eighties,followed by a sharp increase in the nineties. This sharp increase in the1990s was also found in the number of professional journal articles
Schmitz et al. Social Representations of ADHD
387
Figure 1. ADHD articles and books listed in Readers’ Guide to Periodical Literature,Library of Congress and NIH National Library of Medicine ADHD bibliography
CAP 9/4 03 Schmitz (ad/t) 15/1/04 2:06 pm Page 387
at Alexandru Ioan Cuza on December 11, 2013cap.sagepub.comDownloaded from

published on ADHD, as identified in a bibliography developed by theNational Library of Medicine in preparation for a NIH consensus panelmeeting on ADHD in November 1998 (National Institutes of Health,1998).
The numbers of items found in each of these three sources showedvery strong correlations with each other and with the annual produc-tion quota of Ritalin (Table 1 and Figure 2), one of the most commonstimulant medications used for treating ADHD (Diller, 1996). The pro-fessional literature and book publications showed particularly strongcorrelations with Ritalin production (r = .81 and r = .88, respectively),and with each other (r = .76). These correlations show the strongrelationships between the patterns appearing in Figures 1 and 2, indi-cating an important shift in the societal awareness and perceptions ofADHD between the late 1980s and the late 1990s. This may be due to
Culture & Psychology 9(4)
388
Figure 2. US annual Ritalin production quote (Diller, 1996)
Table 1. Correlations among publication sources and yearly production quota of Ritalin
RG articles LOC books NIH articles
Number of Readers’ 1.00Guide articles
Number of Library of 1.46* 1.00Congress books
Number of NIH 1.63* 1.76* 1.00articles
Kilograms of Ritalin 1.40+ 1.88* 1.81*produced
* p < .05; + p < .10
CAP 9/4 03 Schmitz (ad/t) 15/1/04 2:06 pm Page 388
at Alexandru Ioan Cuza on December 11, 2013cap.sagepub.comDownloaded from

several societal trends. During this time period, the development ofmanaged behavioral care resulted in time and economic constraints onphysicians and therapists, bringing key changes in the client–clinicianrelationship and in the perceptions of suitability for different treatmentmodalities (Manderscheid, Henderson, Witkin, & Atay, 1999).Likewise, this time period coincides with the rise of the ‘ProzacCulture’ and the increased acceptance of the use of psychotropic medi-cations to improve mood and performance (Whitehouse, Juengst,Mehlman, & Murray, 1997). Finally, the inclusion of ADHD as alearning disability under the 1990 Individuals with Disabilities Actprovided a key legal tool for families of children with ADHD, helpingthem obtain special services from their school districts (Diller, 1996).
Content AnalysisTo examine in more detail the societal portrayal of ADHD, a contentanalysis (Riffe, Lacy, & Fico, 1998) was performed for a select portionof the articles listed in the Readers’ Guide to Periodical Literature.Focusing on the period that showed the most dramatic changes inRitalin production and print media attention to ADHD, 1988–1997,articles from popular print media were analyzed (Table 2). Two people(second and third authors) coded each article, identifying in each para-graph whether a particular code was present. After significant training,discussion of coding results and retraining, inter-rater reliabilitybetween the two coders was excellent (κ =.92). A third person (firstauthor) examined the resultant coding sheets and determined theparticular paragraph coding when the two coders disagreed. Four
Schmitz et al. Social Representations of ADHD
389
Table 2. Journals selected from the Readers’ Guide to Periodical Literature: number ofarticles and number of paragraphs used in content analysis
Journal Articles Paragraphs
Better Homes & Gardens 2 16Consumer Reports 1 17Good Housekeeping 2 51Ladies’ Home Journal 4 107Maclean’s 1 14Mademoiselle 1 8McCall’s 1 5Newsweek 5 61Parents 5 159People 1 13Redbook 3 75Seventeen 1 47Time 4 71US News & World Report 1 4
Total 32 648
CAP 9/4 03 Schmitz (ad/t) 15/1/04 2:06 pm Page 389
at Alexandru Ioan Cuza on December 11, 2013cap.sagepub.comDownloaded from

broad categories were used in the coding protocol: attribution source,cause of ADHD, treatment of ADHD and other ADHD-related issues.(The coding protocol is available from the first author upon request.)
Results
Attribution source was defined within the content analysis as a personor organization that gives information to news reporters; sources areexplicitly identified as such when reporters quote or paraphrase infor-mation from them in stories. An examination of the attribution sourcegives an indication of the particular voices most commonly presentedin the popular media. Five types of attribution sources were coded:medical, parent, child, teacher and other. As can be seen in Figure 3,the attribution source for citations within articles shifted in emphasisfrom 1988 to 1997, from a greater use of medical sources to ‘other’sources. The other category typically contained attributions to clinicalpsychologists or other types of therapists, as distinct from pediatriciansand psychiatrists. Parents were more consistently used as news sourcesthroughout the time period, with children and teachers being usedmuch less often.
A causal schema was coded, based on any mention of the funda-mental aspects or causes of ADHD. Six categories were used in thecontent analysis: biological, genetic, environment, diet, culture andunknown. The biological cause schema was identified given anymention of biological aspects of the origin of ADHD: for example,
Culture & Psychology 9(4)
390
Figure 3. Attribution source codes found in Readers’ Guide to Periodical Literature articles
CAP 9/4 03 Schmitz (ad/t) 15/1/04 2:06 pm Page 390
at Alexandru Ioan Cuza on December 11, 2013cap.sagepub.comDownloaded from

‘Some researchers see a link between the disorder and abnormalitiesin the brain.’ The genetic cause schema, coded as a distinct categoryfrom the biological cause schema, was identified given any mention ofgenetic aspects in the origin of ADHD. The environment cause schemawas identified given any mention of broad environmental aspects ofthe origin of ADHD: for example, ‘Many experts say environmentalfactors can aggravate an ingrained tendency and induce more of thebehavioral symptoms.’ The culture cause schema was identified givenany mention of specific cultural aspects in the origin of ADHD: forexample, ‘Our society is just making too many demands on these kids.’The unknown cause schema was identified given any mention ofuncertainty regarding what causes ADHD: for example, ‘We just don’treally know what the underlying cause of it is.’
Figure 4 shows that an emphasis on biological explanations forADHD was dominant in the early nineties, but declined through themid- and late nineties. A widely cited study that used brain-imagingtechnology to compare brain images of ADHD and non-ADHD adults(Zametkin et al., 1990) was the primary reason for the very largenumber of paragraphs citing a biological explanation for ADHD in1991. Genetics explanations for ADHD were more prominently pre-sented from 1990 through 1993 than in other years. Overall, causalexplanations for ADHD declined in number through the 1990s, regard-less of the specific type of explanation, although the unknown categoryappeared only in articles published prior to the Zametkin study.
Schmitz et al. Social Representations of ADHD
391
Figure 4. Proposed cause of ADHD codes found in Readers’ Guide to Periodical Literaturearticles
CAP 9/4 03 Schmitz (ad/t) 15/1/04 2:06 pm Page 391
at Alexandru Ioan Cuza on December 11, 2013cap.sagepub.comDownloaded from

This shift in emphasis of causal explanation, from uncertainty to bio-logical and genetic, can be seen in the way these issues were presentedin the articles. In 1988, articles emphasized that ‘there’s no knowncause or cure’ (US News and World Report, January 11, 1988, p. 61), ‘theactual origins are still unknown’ (Parents, December 1988, p. 215), and‘doctors disagree about what causes ADHD’ (Time, January 16, 1989,p. 65). But the Zametkin study served as a turning point in the causal-ity discussion, even though the study authors clearly expressed cautionin their conclusions, particularly noting their small and potentiallybiased sample of adults, and despite the fact that the study findingswere subsequently only partially replicated in adolescent samples(Cantwell, 1996). As noted in Time (November 26, 1990, p. 59),
. . . in more than 20 years of intense scientific scrutiny, no one was able tofind the key [to the cause of ADHD]. Until now. In a landmark study thatcould help put to rest decades of confusion and controversy . . . [scientistshave] traced ADHD for the first time to a specific metabolic abnormality inthe brain.
In Newsweek (December 3, 1990, p. 61), ‘research recently published inThe New England Journal of Medicine suggests that ADHD is related toa metabolic dysfunction in the brain’. In Mademoiselle (August 1991,p. 114), ‘[s]tudies show that people with ADD have lower metabolismin the parts of the brain that control attention and movement’. And inGood Housekeeping (July 1991, p. 175), ‘researchers at NIMH recentlyfound that the region of the brain associated with attention span andmotor control is less active in people with ADHD’.
The presentation of a biological basis for ADHD became refined inthe mid-1990s with the inclusion of reports of a genetic component forthe disorder. Thus in Time (April 19, 1993, p. 23) ‘[p]ay attentionparents, it is not your attitude but your genes that are to blame for theextreme restlessness and impulsiveness in your hyperactive child.’ Ayear later, Time (July 18, 1994, p. 46) reported, ‘The influence of genesis unmistakable.’ These issues essentially forced from the discussion allother possible explanations for the cause of ADHD. This transition wasso complete that, by 1996, ADHD was succinctly presented as ‘acomplex neurological impairment that takes the brakes off brains andderails concentration’ (Newsweek, March 18, 1996, p. 51). Similarly,‘Nick had problems paying attention, she [Nick’s psychiatrist] said,because the organizational center in his brain wasn’t doing his job’(Newsweek, March 18, 1996, p. 59). These images of ‘brakes off brains’,‘derails concentration’ and ‘organizational center in his brain’ serve anobjectification purpose, from the perspective of social representationstheory, by making the abstract concepts of a brain dysfunction more
Culture & Psychology 9(4)
392
CAP 9/4 03 Schmitz (ad/t) 15/1/04 2:06 pm Page 392
at Alexandru Ioan Cuza on December 11, 2013cap.sagepub.comDownloaded from
concrete and understandable as a social representation of ADHD. Thisobjectification process is particularly important in helping a childidentify and comprehend his or her experiences and sensationsrelevant to ADHD-related problems.
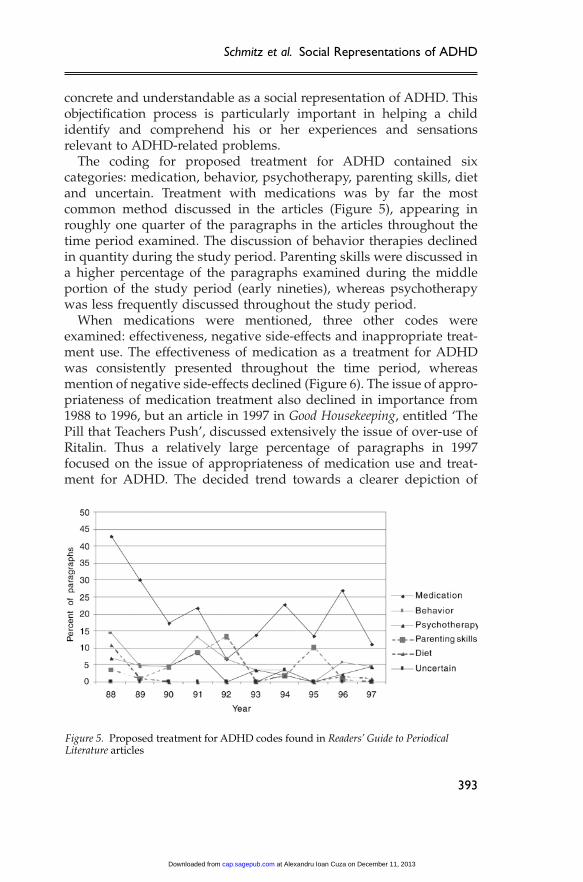
The coding for proposed treatment for ADHD contained sixcategories: medication, behavior, psychotherapy, parenting skills, dietand uncertain. Treatment with medications was by far the mostcommon method discussed in the articles (Figure 5), appearing inroughly one quarter of the paragraphs in the articles throughout thetime period examined. The discussion of behavior therapies declinedin quantity during the study period. Parenting skills were discussed ina higher percentage of the paragraphs examined during the middleportion of the study period (early nineties), whereas psychotherapywas less frequently discussed throughout the study period.
When medications were mentioned, three other codes wereexamined: effectiveness, negative side-effects and inappropriate treat-ment use. The effectiveness of medication as a treatment for ADHDwas consistently presented throughout the time period, whereasmention of negative side-effects declined (Figure 6). The issue of appro-priateness of medication treatment also declined in importance from1988 to 1996, but an article in 1997 in Good Housekeeping, entitled ‘ThePill that Teachers Push’, discussed extensively the issue of over-use ofRitalin. Thus a relatively large percentage of paragraphs in 1997focused on the issue of appropriateness of medication use and treat-ment for ADHD. The decided trend towards a clearer depiction of
Schmitz et al. Social Representations of ADHD
393
Figure 5. Proposed treatment for ADHD codes found in Readers’ Guide to PeriodicalLiterature articles
CAP 9/4 03 Schmitz (ad/t) 15/1/04 2:06 pm Page 393
at Alexandru Ioan Cuza on December 11, 2013cap.sagepub.comDownloaded from

ADHD as having biological and genetic sources, the primary and con-sistent emphasis on the effectiveness of medications for treatingADHD, and the declining emphasis on presentations of negative side-effects of medication treatments coincide with the dramatic rise in theproduction of Ritalin (Figure 2).
However, even with this focus on the biological basis for ADHD, thepresentation of the use of medications for the treatment of childrenremained ambivalent throughout the period. In subsequent paragraphs,the use of Ritalin can be presented as ‘one of the raving successes inpsychiatry . . . a pill that allows children and a growing number ofadults to focus their minds’, but also as a stimulant that ‘may be causingsome hidden havoc to their child’ and as a ‘ “quick fix” for childrenforced to live in an impatient culture’ (Newsweek, March 18, 1996, pp.51–52). Similarly, the admission that ‘[w]e really haven’t known whichtreatment to use for which child and how to combine treatments’ (Time,July 18, 1994, p. 49) shows the uncertainty regarding the appropriatechoice of treatment. This ambivalence in the popular print media con-tradicts the wide professional consensus for combined medication andbehavioral therapies as the appropriate treatment modality for mostpersons with ADHD (National Institutes of Health, 1998).
Several other issues related to ADHD were coded: disability,addiction, education, peer relations, race and gender. Among these,education appeared in a very large percentage of paragraphs in the lateeighties and early nineties (Figure 7), with a main emphasis onproblems that children with ADHD often experience in school. Peer
Culture & Psychology 9(4)
394
Figure 6. Medication treatment issues codes found in Readers’ Guide to PeriodicalLiterature articles
CAP 9/4 03 Schmitz (ad/t) 15/1/04 2:06 pm Page 394
at Alexandru Ioan Cuza on December 11, 2013cap.sagepub.comDownloaded from

relations showed up in a low but consistent percentage of paragraphs,as did gender-related issues. Concerns about addiction to ADHDmedications appeared primarily in the early nineties.
The most common persons presented as having ADHD were youngboys, either in pictures or in the article texts. Boys appeared 33 timesover the ten-year period, whereas girls appeared 19 times (although 10of those appearances were in a single article in 1992); adult femalesappeared 6 times, and adult males appeared 5 times. The presentationof adults with ADHD did not begin until 1993, corresponding to theincrease in adult ADHD diagnoses (Conrad & Potter, 2000).
Comparisons about race and socioeconomic class were never men-tioned in the magazine articles. An examination of the photographsand pictures presented in the articles indicated that middle-class,white boys were the typical subjects of discussion. Only whites wereshown, and generally the photographs showed pre-adolescent boys,except in articles devoted to specific populations such as adult malesor adolescent females. Similarly, ‘Dennis the Menace’ was used inseveral articles as a prototype of the child with ADHD, either in wordsor visually in cartoons. Other cartoon images used in the articlesshowed young white boys running circles around their cringingparents, always white and middle class (not obviously poor or rich).In trying to reduce the potential stigma in the disorder, some authorspresented historical figures as possible persons with ADHD.However, the images presented were always white males, such as
Schmitz et al. Social Representations of ADHD
395
Figure 7. Other issues related to ADHD codes found in Readers’ Guide to PeriodicalLiterature articles
CAP 9/4 03 Schmitz (ad/t) 15/1/04 2:06 pm Page 395
at Alexandru Ioan Cuza on December 11, 2013cap.sagepub.comDownloaded from
Benjamin Franklin, Albert Einstein, Winston Churchill and Bill Clinton(Time, July 18, 1994, p. 47).
Although relatively little research has explicitly examined racialdifferences in the development of ADHD (Samuel et al., 1997), this lackof any racial diversity in the images of persons with ADHD does notcorrespond to the empirical evidence that is available, which typicallyindicates higher percentages of African-American students than whitestudents receiving screening cutoff scores for ADHD (DuPaul et al.,1997; Nolan, Gadow, & Sprafkin, 2001). Importantly, these studies werebased on teacher ratings of ADHD symptom inventories based onDSM-IV criteria (American Psychiatric Association, 1994), and usedscale cutoff scores based on predominantly white norm samples(DuPaul, Power, Anastopoulos, & Reid, 1998). Even given this caveatregarding the basis for estimated racial prevalences of ADHD, the lackof any discussion of racial issues in the magazine articles, coupled with
Culture & Psychology 9(4)
396
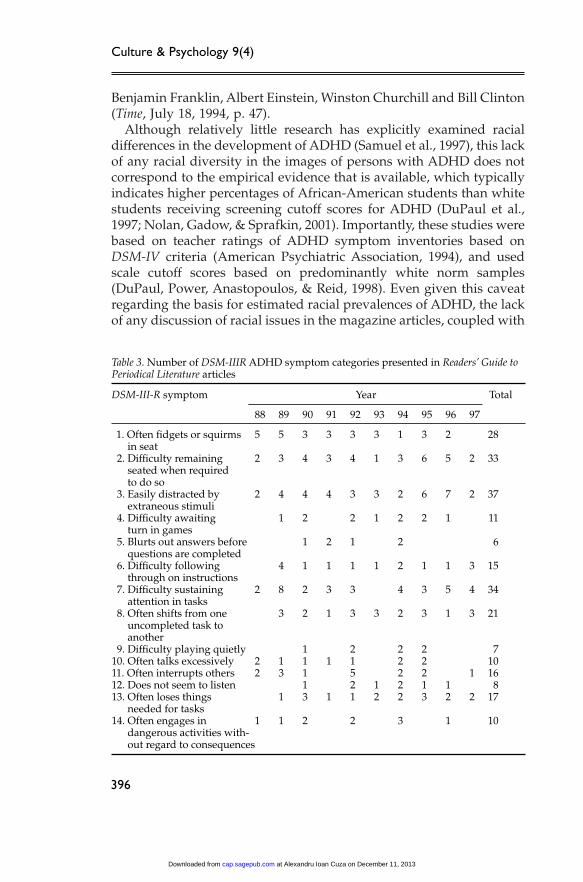
Table 3. Number of DSM-IIIR ADHD symptom categories presented in Readers’ Guide toPeriodical Literature articles
DSM-III-R symptom Year Total
88 89 90 91 92 93 94 95 96 97
11. Often fidgets or squirms 5 5 3 3 3 3 1 3 2 28in seat
12. Difficulty remaining 2 3 4 3 4 1 3 6 5 2 33seated when requiredto do so
13. Easily distracted by 2 4 4 4 3 3 2 6 7 2 37extraneous stimuli
14. Difficulty awaiting 1 2 2 1 2 2 1 11turn in games
15. Blurts out answers before 1 2 1 2 6questions are completed
16. Difficulty following 4 1 1 1 1 2 1 1 3 15through on instructions
17. Difficulty sustaining 2 8 2 3 3 4 3 5 4 34attention in tasks
18. Often shifts from one 3 2 1 3 3 2 3 1 3 21uncompleted task toanother
19. Difficulty playing quietly 1 2 2 2 710. Often talks excessively 2 1 1 1 1 2 2 1011. Often interrupts others 2 3 1 5 2 2 1 1612. Does not seem to listen 1 2 1 2 1 1 813. Often loses things 1 3 1 1 2 2 3 2 2 17
needed for tasks14. Often engages in 1 1 2 2 3 1 10
dangerous activities with-out regard to consequences
CAP 9/4 03 Schmitz (ad/t) 15/1/04 2:06 pm Page 396
at Alexandru Ioan Cuza on December 11, 2013cap.sagepub.comDownloaded from

the sole use of whites in all of the pictures presented in the article, givesa substantially inaccurate depiction of the typical person with ADHD.
The types of symptoms identified in the articles were coded accord-ing to DSM-III-R criteria for ADHD (American Psychiatric Association,1987). The numbers of symptoms found in the articles are presented inTable 3. Of the fourteen symptoms presented in DSM-III-R, only fourwere consistently presented throughout the ten-year period: oftenfidgets or squirms in seat; difficulty remaining seated when requiredto do so; easily distracted by extraneous stimuli; and difficulty sus-taining attention in tasks. These four symptoms were also the mostprominently presented ones, as seen in the total number of times eachwas identified, and form the core identifying characteristics of ADHD,as presented in these magazine articles. The majority of symptoms wasrelatively rarely presented, especially: difficulty awaiting turn; blurtsout answers; difficulty playing quietly; does not seem to listen; andengages in dangerous activities. In 1990, 1992 and 1994, all fourteensymptoms were presented in single articles.
The presentation of these four basic ADHD symptoms correspondsto the change in diagnostic criteria with DSM-IV in 1994 (AmericanPsychiatric Association, 1994). In DSM-IV, four more symptoms wereadded to the DSM-III-R criteria and three broad categories of ADHDwere proposed: inattention, hyperactivity/impulsivity and combined.The numbers of symptoms found in the magazine articles, coded intothe two main categories of inattention and hyperactivity/impulsivity,are presented in Table 4. On average, 13 inattention and 12 hyperac-tivity/impulsivity symptoms were presented each year in themagazine articles, with no discernible trend over time. This balance inthe presentation of broad ADHD symptom categories is somewhatcontrary to findings based on teacher-completed behavior ratingscales, which typically find the inattentive symptoms about twice asprevalent among schoolchildren as the hyperactivity/impulsivitysymptoms (Carlson, Tamm, & Gaub, 1997; DuPaul et al., 1998; Gaub &Carlson, 1997; Nolan et al., 2001).
A large number of ‘other symptoms’ could not be explicitly
Schmitz et al. Social Representations of ADHD
397
Table 4. Number of DSM-IV ADHD symptom categories presented in Readers’ Guide toPeriodical Literature articles
DSM-IV category Year Total
88 89 90 91 92 93 94 95 96 97
Inattention 4 20 13 10 13 10 14 17 17 14 132Hyperactivity/Impulsivity 12 14 15 9 20 5 17 17 9 3 121Other 14 24 13 15 5 14 6 21 22 16 150
CAP 9/4 03 Schmitz (ad/t) 15/1/04 2:06 pm Page 397
at Alexandru Ioan Cuza on December 11, 2013cap.sagepub.comDownloaded from

identified according to DSM-IV ADHD criteria (Table 4). Indeed, onaverage there were a larger number of other symptoms presented eachyear in the magazine articles, compared with the average number ofinattention and hyperactivity/impulsivity symptoms (15 versus 13and 12). This finding corresponds to the recent research showing strongevidence for comorbidity of ADHD with other children’s mental dis-orders, particularly anxiety disorders, oppositional defiant disorderand conduct disorder (Jensen, Martin, & Cantwell, 1997; Newcorn etal., 2001). An important issue is the ability to distinguish anxious ordefiant children from children with ADHD. For example, anxiouschildren may appear inattentive, and oppositional and disruptivechildren may appear hyperactive or impulsive, even though the under-lying disorder is not ADHD, or there may be no mental disorderpresent at all (Abikoff, Courtney, Pelham, & Koplewicz, 1993).
As presented in the magazine articles, a common reaction for indi-viduals upon receiving a diagnosis of ADHD is a sense of relief andunderstanding, particularly among adults. ‘It’s been such a weight offmy shoulders. I had 38 years of thinking I was a bad person. Now I’mrewriting the tapes of who I thought I was to who I really am’ (Time,July 18, 1994, p. 43). Even for children, the need to understand andincorporate these images into their self-concept is critical. Thus amother, in helping her son through this process of self-identity, canmake
. . . it my mission to give him words to better understand himself. One timeI told him he was like the New York City subway system, part of his brainon Express and part of it a Local. They get to the same place but the Localhas to make more stops. Nick’s life would be easier if his brain ran on thesame tracks. But I no longer believe it would be better. (Newsweek, March 18,1996, p. 59)
The incorporation of medication treatment into self-identity appearsin the reflections of an 18-year-old girl, Corinne, on her eight years oftaking Ritalin:
Corinne says that whenever she has a burst of energy, ‘people ask me if I’veforgotten my ‘Rit,’ as dad calls it. I can’t express myself or be overly energeticwithout somebody reminding me to take my Ritalin. It’s weird. This littlepill totally changes who I am—but not really. I’m chemically imbalanced,and Ritalin gives me the chemicals I need. (Seventeen, January 1995, p. 98)
Not only has Corinne come to understand herself as a person needingthe medication, and being transformed as a person by the medication,but she also gains feedback from significant others that corroboratesthese same perceptions of her self-identity. Likewise, the report from
Culture & Psychology 9(4)
398
CAP 9/4 03 Schmitz (ad/t) 15/1/04 2:06 pm Page 398
at Alexandru Ioan Cuza on December 11, 2013cap.sagepub.comDownloaded from

an adult male shows the effect on the sense of self that can arise fromthe start of medication treatment for ADHD: ‘Right after I started thetreatment I saw ‘Awakenings.’ I cried and cried because that was howI felt, like I had awakened’ (Newsweek, July 26, 1993, p. 49).
Many of these processes in social identity intimately involve socialcomparisons, particularly in the motivational aspects of strivingtowards reducing uncertainty and in the crystallization of distinct pro-totypes used in self-categorization and evaluation (Hogg, 2000). Interms of health and illness, social comparison processes provideimportant roles in the interpretation of symptoms, the realization ofbeing ill and the decision to seek professional care (Suls, Martin, & Lev-enthal, 1997; Tennen, McKee, & Affleck, 2000). Social representationsof selfhood, which differ considerably in different cultural contexts(Oyserman & Markus, 1998), form the foundation for these compari-son processes. Representations of the self become especially inter-twined with the representations of the illness, as the individualelaborates further the disease model (Leventhal, Hudson, & Robitaille,1997). This process is clearly indicated above in the personal responsesto the diagnosis and treatment of ADHD symptoms.
The processes of anchoring and objectification in social represen-tations theory contain certain characteristics resembling aspects ofsocial comparison theories that incorporate the concept of a prototype.In these versions of social comparison theory, the individual holds inher/his mind an image of the prototypical person in a particularcategory (e.g. the prototypical smoker). Two aspects of the prototypeimage are keys for individual behaviors. First, the more closely that anindividual perceives him/herself as resembling the prototype, themore similarly to the prototype the individual will behave. Second, themore positive the prototype image an individual perceives, the morelikely the individual will behave like the prototype. Thus a persondeciding about smoking cigarettes will be more likely to smoke a cig-arette the more positive the image of a prototypical smoker she hasand the more similar she perceives herself as compared with the pro-totypical smoker (Gibbons & Gerrard, 1997; Tennen et al., 2000).
The social representation of ADHD can act like a prototype, particu-larly in the dominant images of hyperactive children: ‘They are Dennisthe Menace come to life, half-pint hellions who drive parents andteachers to distraction with their disruptive antics’ (Time, January 16,1989, p. 65). A parent who sees his child as being similar to this pro-totypical ADHD child, and perceives fewer stigmas attached to thatimage, will be more likely to follow the treatment aspects associatedwith that image. Given the dominance of the medical model for
Schmitz et al. Social Representations of ADHD
399
CAP 9/4 03 Schmitz (ad/t) 15/1/04 2:06 pm Page 399
at Alexandru Ioan Cuza on December 11, 2013cap.sagepub.comDownloaded from
causation of ADHD and the corresponding emphasis on a medicationapproach in treatment, this would imply a greater likelihood of the useof Ritalin or similar medications. A parent who does not see her childas being similar to the prototypical ADHD child, or has a greater senseof stigma in the image, will be less likely to identify Ritalin as a suitabletreatment option.
Discussion
In this paper, we have identified some of the fundamental character-istics in the social representation of ADHD, following the unfolding ofthis representation over a ten-year period, 1988–1997. Key aspects ofthe representation include a biological and genetic understanding ofcause, an emphasis on symptoms of hyperactivity rather than inatten-tion, and a dominant image of young white boys being the most likelypersons to have ADHD. The construction of a causal aspect to theADHD social representation showed the two phases of this process. Inthis example, uncertainty about the causal aspects of ADHD becameanchored in a physical illness depiction through the scientific findingsusing brain-imaging technology (Zametkin et al., 1990). The colorfuland exciting brain imagery in this single study was presented exten-sively in the print media, and encouraged the use of medical languagein depicting the cause of ADHD-related behaviors. Objectification ofthe ADHD representation arose through further discourse in the printmedia in the following years, primarily through words like ‘brokenbrain’, ‘brakes off brains’ and ‘derailed concentration’. This languagemade the more abstract images from the brain-imaging technology intomore concrete and understandable terms for lay people.
Recent theoretical arguments have been raised postulating ADHD asimpairment in the behavioral inhibition system (Baird, Stevenson, &Williams, 2000; Barkley, 1997). In this perspective, self-control andbehavioral inhibition serve a critical foundation for task performance.As children mature, they develop the ability to engage in variousmental activities, called executive functions, which allow them to focuson tasks, remember goals and complete the required steps for attain-ing those goals. Four key executive functions have been identified: theoperation of working memory; the internalization of self-directedspeech; controlling emotions, motivation and state of arousal; and thecapacity for restructuring observed behaviors into new actions not pre-viously learned from experience (Barkley, 1997). ADHD can be seen asthe failure of one or all of these executive functions to operate properly,resulting in personal and/or social harms.
Culture & Psychology 9(4)
400
CAP 9/4 03 Schmitz (ad/t) 15/1/04 2:06 pm Page 400
at Alexandru Ioan Cuza on December 11, 2013cap.sagepub.comDownloaded from

Only if the essence of this theory about ADHD becomes part of thecommon language, that is, the social representation of ADHD, will thetheory help illuminate the popular understanding of ADHD. The roleof the media as intermediary between scientist and lay person is ofvital concern (Farr, 1993). This process will require scientific supportfor the hypotheses generated by the theory, development of diagnostictools that emphasize both specificity and sensitivity, and skillfulpresentation of the perspective in the popular media. In terms of socialrepresentations theory, this third issue will require appropriate use ofobjectifying images for making the abstract theoretical concepts,particularly in identifying the specific executive functions associatedwith ADHD, understandable and acceptable to lay people (Farr, 1993).This concrete imagery, a strength of the brain images so widely citedfrom Zametkin’s study (Zametkin et al., 1990), must be drawn uponwhen further elaborating any theoretical foundations about ADHD.
Also of great importance are the potential influences of the ADHDsocial representation on individual identity formation and mentalhealth decisions. The sharing of social representations in a socialgroup strongly influences social identity of group members (Carugati& Selleri, 1998; Oyserman & Markus, 1998; Wagner et al., 1999). Thewhite, middle-class, young boy characteristics in the social represen-tation necessarily reduce the likelihood of persons with other types ofcharacteristics identifying with the image. In particular, the completelack of any racial diversity in the social representation of ADHD limitsthe images available to minority individuals, thus reducing the likeli-hood of incorporating crucial aspects of the ADHD social represen-tation. This corresponds well to recent research showing very differentand distinct perspectives about ADHD expressed by African-American (Bussing, Schoenberg, & Perwien, 1998) and Cuban-American (Arcia & Fernandez, 1998) mothers of young children ascompared with white mothers of young children. Because of this dis-junction between the representations of the illness and self, indi-viduals may experience a reduction of self-esteem, perhaps acompounding of symptoms related to ADHD, and the resultingincreased difficulties in social relations (Farr, 1995; Klasen, 2000; Lev-enthal et al., 1997). As the individual parent or child tries to sortthrough these conflicting social representations, a particular concernfor mental health practitioners will be the potential difficulty the clientexperiences in ascertaining, and adhering to, the most appropriatetreatment modality (Krueger & Kendall, 2001). Likewise, differingsocial representations of ADHD, as held by clinician, parent and child,can easily lead to contradictory understandings about causal
Schmitz et al. Social Representations of ADHD
401
CAP 9/4 03 Schmitz (ad/t) 15/1/04 2:06 pm Page 401
at Alexandru Ioan Cuza on December 11, 2013cap.sagepub.comDownloaded from

foundations for the child behaviors and the suitability of differenttreatment options.
Finally, findings from this study have implications for socialrepresentations theory. At the macro level, the use and incorporationof the social representation of ADHD involve an constructive processin which social location, context and experience can lead to verydistinct interpretations of the images presented in the media(Danforth & Navarro, 2001; Farr, 1995; Flick, 1998; Gamson et al.,1992). At the micro level, the processes of identifying symptoms,labeling them as ADHD and deciding among various treatmentoptions fundamentally involve agency in the individual and reflex-ivity of the self within a broad social context (Augoustinos & Walker,1995). Social representations of ADHD form the foundation for thisagency and reflexivity, by presenting reference points for the selection,categorization and organization of the individual’s perceptions andexperiences. As identified by social representations theory, it isthrough the processes of anchoring and objectification in which anindividual compares her/his own mental maps of self and symptomsensations that the social representations of the disorder providemeaning-making structures for the individual (Duveen & Lloyd, 1990;Flick, 1998). The social groups to which the individual belongs guidethe processes of perceiving and comparing, primarily through thisculturally and socially embedded knowledge about appropriatebehavior and mental health, and which we identify here as the socialrepresentation of ADHD.
Acknowledgements
This research, completed while the second author was a Project L/EARNintern at the Institute or Health, Health Care Policy and Aging Research atRutgers University, was supported in part by a NIMH Mental HealthEducation Grant to Project L/EARN (MH 58908–05).
References
Abikoff, H.B., Courtney, M., Pelham, W.E., & Koplewicz, H.S. (1993). Teachers’ratings of disruptive behaviors: The influence of halo effects. Journal ofAbnormal Child Psychology, 21, 519–533.
American Psychiatric Association. (1987). Diagnostic and statistical manual ofmental disorders (3rd rev. ed.). Washington, DC: Author.
American Psychiatric Association. (1994). Diagnostic and statistical manual ofmental disorders (4th ed.). Washington, DC: Author.
Anderson, J.C. (1996). Is childhood hyperactivity the product of westernculture? The Lancet, 348, 73–74.
Culture & Psychology 9(4)
402
CAP 9/4 03 Schmitz (ad/t) 15/1/04 2:06 pm Page 402
at Alexandru Ioan Cuza on December 11, 2013cap.sagepub.comDownloaded from
Angold, A., Erkanli, A., Egger, H.L., & Costello, E.J. (2000). Stimulanttreatment for children: A community perspective. Journal of the AmericanAcademy of Child and Adolescent Psychiatry, 39, 975–984.
Arcia, E., & Fernandez, M.C. (1998). Cuban mothers’ schemas of ADHD:Development, characteristics, and help seeking behavior. Journal of Child andFamily Studies, 7(3), 333–352.
Augoustinos, M., & Walker, I. (1995). Social cognition. London: Sage.Baird, J., Stevenson, J.C., & Williams, D.C. (2000). The evolution of ADHD: A
disorder of communication? Quarterly Review of Biology, 75, 17–35.Barkley, R.A. (1997). ADHD and the nature of self-control. New York: Guilford.Bradley, C. (1937). The behavior of children receiving benzedrine. American
Journal of Psychiatry, 94, 577–585.Bussing, R., Schoenberg, N.E., & Perwien, A.R. (1998). Knowledge and
information about ADHD: Evidence of cultural differences among African-American and white parents. Social Science & Medicine, 46, 919–928.
Cantwell, D.P. (1996). Attention deficit disorder: A review of the past 10 years.Journal of the American Academy of Child and Adolescent Psychiatry, 35,978–987.
Carlson, C.L., Tamm, L., & Gaub, M. (1997). Gender differences in childrenwith ADHD, ODD, and co-occurring ADHD/ODD identified in a schoolpopulation. Journal of the American Academy of Child and AdolescentPsychiatry, 36, 1706–1714.
Carugati, F.F., & Selleri, P. (1998). Social representations and development:Experts’ and parents’ discourses about a puzzling issue. In U. Flick (Ed.), Thepsychology of the social (pp. 170–185). New York: Cambridge University Press.
Conrad, P. (1976). Identifying hyperactive children: The medicalization of deviantbehavior. Lexington, MA: Lexington Books.
Conrad, P., & Potter, D. (2000). From hyperactive children to ADHD adults:Observations on the expansion of medical categories. Social Problems, 47,559–582.
Danforth, S., & Navarro, V. (2001). Hyper talk: Sampling the socialconstruction of ADHD in everyday language. Anthropology and EducationQuarterly, 32, 167–190.
de Rosa, A.S. (1987). The social representations of mental illness in childrenand adults. In W. Doise & S. Moscovici (Eds.), Current issues in Europeansocial psychology (Vol. 2, pp. 47–138). Cambridge: Cambridge UniversityPress.
Diller, L.H. (1996). The run on ritalin: Attention deficit disorder and stimulanttreatment in the 1990s. Hastings Center Report, 26, 1–8.
DuPaul, G.J., Power, T.J., Anastopoulos, A.D., & Reid, R. (1998). ADHD RatingScale-IV. New York: Guilford.
DuPaul, G.J., Power, T.J., Anastopoulos, A.D., Reid, R., McGoey, K.E., & Ikeda,M.J. (1997). Teacher ratings of attention deficit hyperactivity disordersymptoms: Factor structure and normative data. Psychological Assessment, 9,436–444.
Durkheim, É. (1995). The elementary forms of religious life. New York: Free Press.Duveen, G., & Lloyd, B. (1990). Social representations and the development of
knowledge. Cambridge: Cambridge University Press.
Schmitz et al. Social Representations of ADHD
403
CAP 9/4 03 Schmitz (ad/t) 15/1/04 2:06 pm Page 403
at Alexandru Ioan Cuza on December 11, 2013cap.sagepub.comDownloaded from

Farr, R.M. (1993). Common sense, science and social representations. PublicUnderstanding of Science, 2, 189–204.
Farr, R.M. (1995). Representation of health, illness and handicap in the massmedia of communication: A theoretical overview. In I. Marková & R.M. Farr(Eds.), Representations of health, illness and handicap (pp. 3–30). New York:Routledge.
Flick, U. (1998). Everyday knowledge in social psychology. In U. Flick (Ed.),The psychology of the social (pp. 41–69). New York: Cambridge UniversityPress.
Gamson, W.A., Croteau, D., Hoynes, W., & Sasson, T. (1992). Media imagesand the social construction of reality. Annual Review of Sociology, 18, 373–393.
Gaub, M., & Carlson, C.L. (1997). Gender differences in ADHD: A meta-analysis and critical review. Journal of the American Academy of Child andAdolescent Psychiatry, 36, 1036–1045.
Gibbons, F.X., & Gerrard, M. (1997). Health images and their effects on healthbehavior. In B.P. Buunk & F.X. Gibbons (Eds.), Health, coping, and well-being:Perspectives from social comparison theory (pp. 63–94). Mahwah, NJ: Erlbaum.
Goldman, L.S., Genel, M., Bezman, R.J., & Slanetz, P.J. (1998). Diagnosis andtreatment of attention-deficit/hyperactivity disorder in children andadolescents. Journal of the American Medical Association, 279, 1100–1107.
Hogg, M.A. (2000). Social identity and social comparison. In J. Suls & L.Wheeler (Eds.), Handbook of social comparison: Theory and research (pp.401–421). New York: Kluwer Academic/Plenum.
Jensen, P.S., Martin, D., & Cantwell, D.P. (1997). Comorbidity in ADHD:Implications for research, practice and DSM-V. Journal of the AmericanAcademy of Child and Adolescent Psychiatry, 36, 1065–1079.
Jodelet, D. (1991). Madness and social representations. Berkeley: University ofCalifornia Press.
Kitzinger, J. (1995). The face of AIDS. In I. Marková & R. M. Farr (Eds.),Representations of health, illness and handicap (pp. 49–68). New York:Routledge.
Klasen, H. (2000). A name, what’s in a name? The medicalization ofhyperactivity, revisited. Harvard Review of Psychiatry, 7, 334–344.
Krueger, M., & Kendall, J. (2001). Descriptions of self: An exploratory study ofadolescents with ADHD. Journal of Child and Adolescent Psychiatric Nursing,14, 61–72.
Kruse, L. (1998). The social representation of ‘man’ in everyday speech. In U.Flick (Ed.), The psychology of the social (pp. 196–206). New York: CambridgeUniversity Press.
Leventhal, H., Hudson, S., & Robitaille, C. (1997). Social comparison andhealth: A process model. In B.P. Buunk & F.X. Gibbons (Eds.), Health, coping,and well-being: Perspectives from social comparison theory (pp. 411–432).Mahwah, NJ: Erlbaum.
Manderscheid, R.W., Henderson, M.J., Witkin, M.J., & Atay, J.E. (1999).Contemporary mental health systems and managed care. In A.V. Horwitz &T.L. Scheid (Eds.), A handbook for the study of mental health: Social contexts,theories, and systems (pp. 412–426). New York: Cambridge University Press.
Culture & Psychology 9(4)
404
CAP 9/4 03 Schmitz (ad/t) 15/1/04 2:06 pm Page 404
at Alexandru Ioan Cuza on December 11, 2013cap.sagepub.comDownloaded from

Morrow, R.C., Morrow, A.L., & Haislip, G. (1998). Methylphenidate in theUnited States, 1990 through 1995. American Journal of Public Health, 88, 1121.
Moscovici, S. (1976). La psychanalyse: Son image et son public. Paris: PressesUniversitaires de France.
National Institutes of Health. (1998). Diagnosis and treatment of attentiondeficit hyperactivity disorder. NIH Consensus Statement 1998 Nov. 16–18(2).
Nelson, T.E., Clawson, R.A., & Oxley, Z.M. (1997). Media framing of a civilliberties conflict and its effect on tolerance. American Political Science Review,91, 567–583.
Newcorn, J.H., Halperin, J.M., Jensen, P.S., Abikoff, H.B., Arnold, L.E.,Cantwell, D.P., et al. (2001). Symptom profiles in children with ADHD:Effects of comorbidity and gender. Journal of the American Academy of Childand Adolescent Psychiatry, 40, 137–146.
Nolan, E.E., Gadow, K.D., & Sprafkin, J. (2001). Teacher reports of DSM-IVADHD, ODD, and CD symptoms in schoolchildren. Journal of the AmericanAcademy of Child and Adolescent Psychiatry, 40, 241–249.
Oyserman, D., & Markus, H.R. (1998). Self as social representation. In U. Flick(Ed.), The psychology of the social (pp. 107–125). New York: CambridgeUniversity Press.
Potter, J., & Wetherell, M. (1998). Social representations, discourse analysis,and racism. In U. Flick (Ed.), The psychology of the social (pp. 138–155). NewYork: Cambridge University Press.
Riffe, D., Lacy, S., & Fico, F.G. (1998). Analyzing media messages: Usingquantitative content analysis in research. Mahwah, NJ: Erlbaum.
Samuel, V.J., Curtis, S., Thornell, A., George, P., Taylor, A., Brome, D.R., et al.(1997). The unexplored void of ADHD and African-American research: Areview of the literature. Journal of Attention Disorders, 1, 197–207.
Sommer, C.M. (1998). Social representations and media communications. In U.Flick (Ed.), The psychology of the social (pp. 186–195). New York: CambridgeUniversity Press.
Still, G.F. (1902). Some abnormal psychical conditions in children. The Lancet,1008–1012.
Suls, J., Martin, R., & Leventhal, H. (1997). Social comparison, lay referral, andthe decision to seek medical care. In B.P. Buunk & F.X. Gibbons (Eds.),Health, coping, and well-being: Perspectives from social comparison theory (pp.195–226). Mahwah, NJ: Erlbaum.
Tennen, H., McKee, T.E., & Affleck, G. (2000). Social comparison processes inhealth and illness. In J. Suls & L. Wheeler (Eds.), Handbook of socialcomparison: Theory and research (pp. 443–483). New York: KluwerAcademic/Plenum.
Wagner, W., Duveen, G., Farr, R.M., Jovchelovitch, S., Lorenzi-Cioldi, F.,Marková, I., et al. (1999). Theory and method of social representations.Asian Journal of Social Psychology, 2, 95–125.
Whitehouse, P.J., Juengst, E., Mehlman, M., & Murray, T.H. (1997). Enhancingcognition in the intellectually intact. Hastings Center Report, 27(3), 14–22.
Zametkin, A.J., Nordahl, T.E., Gross, M., King, A.C., Semple, W.E., Rumsey, J.M., et al. (1990). Cerebral glucose metabolism in adults with hyperactivityof childhood onset. New England Journal of Medicine, 323, 361–366.
Schmitz et al. Social Representations of ADHD
405
CAP 9/4 03 Schmitz (ad/t) 15/1/04 2:06 pm Page 405
at Alexandru Ioan Cuza on December 11, 2013cap.sagepub.comDownloaded from

Zani, B. (1995). The mentally ill person and the others: Social representationsand interactive strategies. In I. Marková & R.M. Farr (Eds.), Representationsof health, illness and handicap (pp. 145–162). New York: Routledge.
Zito, J.M., Safer, D.J., dos Reis, S., Gardner, J.F., Boles, M., & Lynch, F. (2000).Trends in the prescribing of psychotropic medications to preschoolers.Journal of the American Medical Association, 283, 1025–1030.
Biographies
MARK F. SCHMITZ (Ph.D., Sociology, Iowa State University) is an AssistantProfessor in the School of Social Work at Rutgers University. His researchexamines the roles of culture, acculturation and ethnicity on parentalperceptions of child behaviors and the social representations of mentaldisorders. ADDRESS: Dr. Mark F. Schmitz, School of Social Work, Rutgers,The State University of New Jersey, 536 George Street, New Brunswick, NJ08901-1167, USA. [email: [email protected])
PREMA FILIPONE (BA, Psychology, Rutgers University), in her honors thesis,‘Media’s Portrayal of Attention-Deficit/Hyperactivity Disorder and thePotential for False Information’, did the coding of much of the data analyzedin this paper.
ELAINE M. EDELMAN (MSW, New York University) is a clinical socialworker and team leader of the West Brighton Clinic, St. Vincent CatholicMedical Center, Staten Island, NY. She is also a doctoral student in the Schoolof Social Work at Rutgers University. Her research examines BorderlinePersonality Disorder and trauma issues. ADDRESS: Elaine M. Edelman, St.Vincent Catholic Medical Centers, West Brighton Clinic, 690 CastletonAvenue, Staten Island, NY 10310, USA. [email: [email protected]]
Culture & Psychology 9(4)
406
CAP 9/4 03 Schmitz (ad/t) 15/1/04 2:06 pm Page 406
at Alexandru Ioan Cuza on December 11, 2013cap.sagepub.comDownloaded from