current and future management of serious skin and skin-structure infections
TRANSCRIPT

Current and Future Management Skin-Structure Infections
of Serious Skin and
Robert Schwartz, MD, Leena R. Das-Young, PharmD, ~ort~yers, Florida, Carlos Ramirez-Rot-da, MD, San Juan, Puerto Rico, Elliot Frank, MD, Neptune, New Jersey
The purpose of this study was to compare in a randomized, open-label clinical study, the efficacy and safety of cefepime (1 g every 12 hours) with that of ceftazidime (1 g every 8 hours) in patients with serious skin and skin- structure infections. Of 298 patients enrolled in the study, 130 with serious skin and skin- structure infections were evaluable. Demographics and underlying medical conditions were comparable in both groups. The most common infections were cellulitis, abscesses, ulcers, and postoperative wound infections. The most common pathogens isolated were Staphylococcus aureus, group A streptococci, Enterobacteriaceae, and Pseudomonas aeruginosa. Duration of therapy in the 93 patients treated with cefepime was 3-18 days and in the 37 ceftazidime-treated patients was 4-16 days. Pathogen bacteriologic response rates were high: 92% ( 124 of 135) of pathogens were eradicated by cefepime and 95% (55 of 58) by ceftazidime. Clinical response rates were satisfactory in 88% (82 of 93) of cefepime-treated patients and in 89% (33 of 37) of ceftazidime-treated patients. Adverse events occurred with similar frequency in both groups. Events probably related to study drugs affected 3% (6 of 198) of patients treated with cefepime and 4% (4 of 100) of ceftazidime-treated patients. Cefepime, a new parenteral cephalosporin administered every 12 hours, is an extremely well tolerated and effective alternative to ceftazidime given every 8 hours for the treatment of serious skin and skin- structure infections. Am J Med. 1996;1OO(suppl 6A): 9os-95s.
From Associates in Infectious Diseases and Research, Fort Myers, Florida (R.S., L.R.D.Y.); Veterans Affairs Medical Center, San Juan, Puerto Rico (C.R.-R.); and Neptune, New Jersey 1E.F.).
Requests for reprints should be addressed to Robert Schwartz, MD, Associates in infectious Diseases and Research, 3677 Central Avenue, Suite D, Fort Myers, Florida 33901.
6A-90s 01996 by Excerpta Medica. Inc. All rights resewed.
S kin and skin-structure infections occur most fre- quently when trauma or a breach in the natural
skin barrier allows bacteria to invade subcutaneous tissues. These breaches are typically su,sceptible to surface contamination, and infections are commonly caused by Staphylococcus aureus or streptococci. Serious infections of the skin and skin structures may be caused by multiple gram-positive and gram- negative pathogens, such as S. aureus, Pseudo- monas aeruginosa , and Enterobacteriaceae.’ Treat- ment of a difficult mixed infection of the skin and skin structure may be complicated by multiple-drug resistance or by drugs that require frequent dosing, which may lead to missed doses. Desirable charac- teristics of an antimicrobial, therefore, include a long half-life, a high level of tissue penetration, and activ- ity against bot,h gram-negative (P. a.eruginosa) and gram-positive (S. aureus) organisms.’
Cefepime is a fourth-generation intravenous ceph- alosporin with an extended spectrum of activity against both gram-positive bacteria, such as staphy- lococci and streptococci, and many gram-negative bacteria, including Enterobacteriaceae and P. a,eru- ginosa .2 Cefepime, which is extremely stable against ,&lactamases, is active against bacteria that have be- come resistant to other cephalosporins, notably cef- triaxone, cefoperazone, cefotaxime, and ceftazi- dime.2z3
On the basis of these characteristics, cefepime ap- pears to be appropriate for the treatment of skin and skin-structure infections caused by a wide range of bacterial pathogens. The current study was con- ducted to compare the safety and efficacy of cefe- pime with that of ceftazidime for the treatment of serious skin and skin-structure infections.
PATIENTS AND METHODS This multicenter, randomized (2 : 1, cefepime : cefta-
zidime), open-label study compared the safety and efficacy of cefepime (1 g every 12 hours) with that of ceftazidime ( 1 g every 8 hours). Both study drugs were administered by 30-minute intravenous in- fusion.
Men and women with symptoms consistent with skin and skin-structure infections were eligible if they were 2 18 years of age, had a pathogen believed to be susceptible to cefepime and ceftazidime, and gave written informed consent. Patienls were ex-
0002-9343/96/$15.00 PII SOOO2-9343(96)00111-8
SYMPOSIUM ON ANTlMlCROBlAL THERAPY/SCHWARTZ ET Al
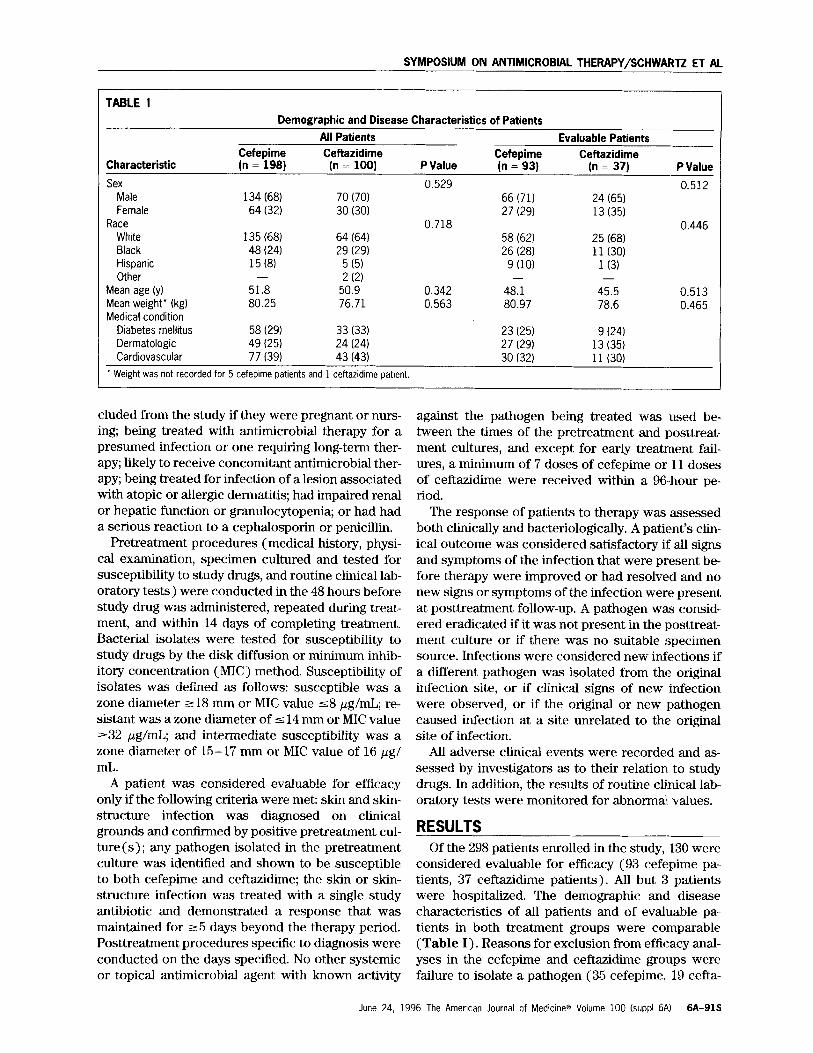
TABLE I Demographic and Disease Characteristics of Patients
All Patients Evaluable Patients Cefepime Ceftazidime Cefepime Ceftazidime
Characteristic (n = 198) (n = 100) P Value (n = 93) (n = 37) P Value
Sex 0.529 0.512 Male 134 (68) 70 (70) 66 (71) 24 (65) Female 64 (32) 30 (301 27 (29) 13 (35)
Race 0.718 0.446 White 135 (68) 64 (64) 58 (621 25 (68) Black 48 (24) 29 (29) 26 (281 11 (30) Hispanic 15 (8) 5 (5) 9 (10) 1 (3) Other - 2 (2) - -
Mean ty) age 51.8 50.9 0.342 48.1 45.5 0.513 Mean weight* (kg) 80.25 76.71 0.563 80.97 78.6 0.465 Medical condition
Diabetes mellitus 58 (29) 33 (33) 23 (25) 9 (24) Dermatologic 49 (25) 24 (24) 27 (29) 13 (35) Cardiovascular 77 (39) 43 (43) 30 (32) 11 (30)
* Weight was not recorded for 5 cefepime patients and 1 ceftazidime patient.
eluded from the study if they were pregnant or nms- ing; being treated with antimicrobial therapy for a presumed infection or one requiring long-term ther- apy; likely to receive concomitant antimicrobial ther- apy; being treated for infection of a lesion associated with atopic or allergic dermatitis; had impaired renal or hepatic function or granulocytopenia; or had had a serious reaction to a cephalosporin or penicillin.
Pretreatment procedures (medical history, physi- cal examination, specimen cultured and tested for susceptibility to study drugs, and routine clinical lab- oratory tests) were conducted in the 48 hours before study drug was administered, repeated during treat- ment, and within 14 days of completing treatment. Bacterial isolates were tested for susceptibility to study drugs by the disk diffusion or minimum inhib- itory concentration (MIC) method. Susceptibility of isolates was dellned as follows: susceptible was a zone diameter 218 mm or MIC value 58 pg/mL; re- sistant was a zone diameter of 5 14 mm or MIC value 232 pg/mL; and intermediate susceptibility was a zone diameter of 15-17 mm or MIC value of 16 pg/ mL.
A patient was considered evaluable for efficacy only if the following criteria were met: skin and skin- structure infection was diagnosed on clinical grounds and confirmed by positive pretreatment cul- ture(s); any pathogen isolated in the pretreatment culture was identified and shown to be susceptible to both cefepime and ceftazidime; the skin or skin- structure infection was treated with a single study antibiotic and demonstrated a response that was maintained for ~5 days beyond the therapy period. Posttreatment procedures specific to diagnosis were conducted on the days specified. No other systemic or topical antimicrobial agent with known activity
against the pathogen being treated was used be- tween the times of the pretreatment and posttreat- ment cultures, and except for early treatment fail- ures, a minimum of 7 doses of cefepime or 11 doses of ceftazidime were received within a 96..hour pe- riod.
The response of patients to therapy was assessed both clinically and bacteriologically. A patient’s clin- ical outcome was considered satisfactory if all signs and symptoms of the infection that were present be- fore therapy were improved or had resolved and no new signs or symptoms of the infection were present at posttreatment follow-up. A pathogen was consid- ered eradicated if it was not present in the posttreat- ment culture or if there was no suitable specimen source. Infections were considered new infections if a different pathogen was isolated from the original infection site, or if clinical signs of new infection were observed, or if the original or new pathogen caused infection at a site unrelated to the original site of infection.
All adverse clinical events were recorded and as- sessed by investigators as to their relation to study drugs. In addition, the results of routine clinical lab- oratory tests were monitored for abnormal values.
RESULTS Of the 298 patients enrolled in the study, 130 were
considered evaluable for efficacy (93 cefepime pa- tients, 37 ceftazidime patients). All but 3 patients were hospitalized. The demographic and disease characteristics of all patients and of evaluable pa- tients in both treatment groups were comparable (Table I). Reasons for exclusion from efficacy anal- yses in the cefepime and ceftazidime groups were failure to isolate a pathogen (35 cefepime, 19 cefta-
June 24, 1996 The Amencan Journal of Medicine8 Volume 100 Isuppl 6rSI 6A-91s
SYMPOSIUM ON ANTIMICROBIAL THERAPY/SCHWARTZ ET AL
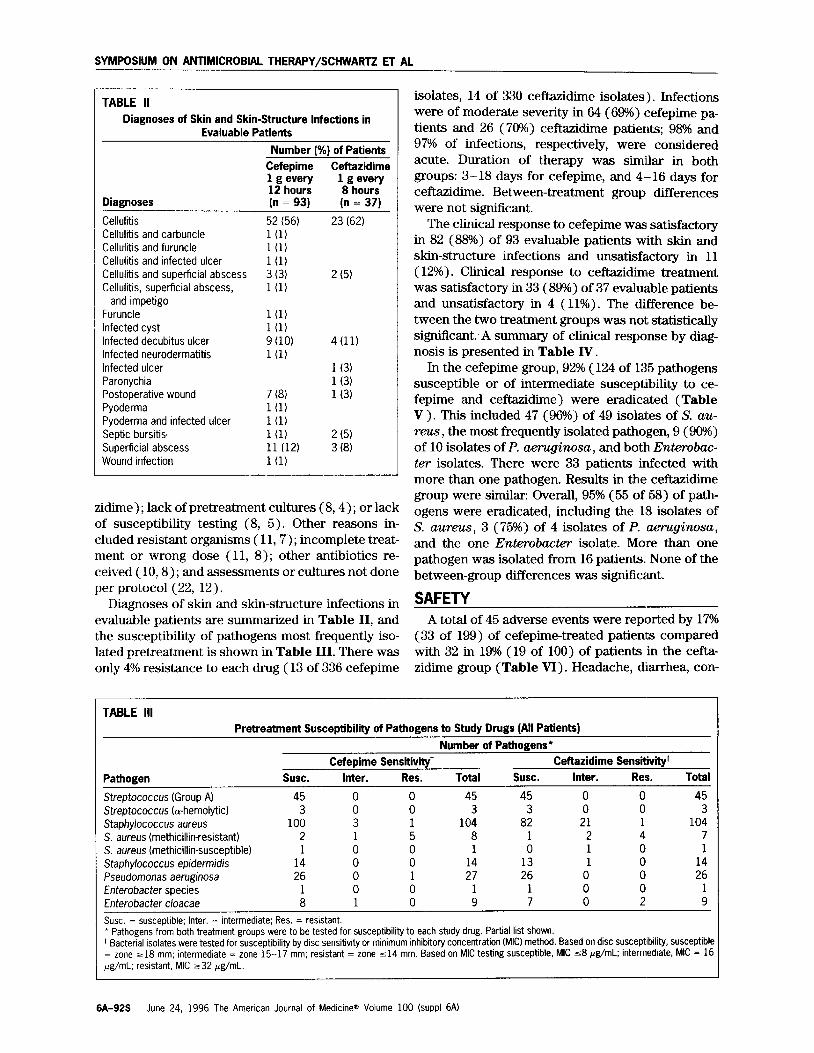
TABLE II
Diagnoses of Skin and Skin-Structure Infections in Evaluable Patients
Number (%) of Patients Cefepime Ceftazidime 1 g every 1 g every 12 hours 8 hours
Diagnoses (n = 93) (n = 37)
Cellulitis 52 (56) 23 (62) Cellulitis and carbuncle l(l) Cellulitis and furuncle l(l) Cellulitis and infected ulcer l(l) Cellulitis and superficial abscess 3 (3) 2 (5) Cellulitis, superficial abscess, l(1)
and impetigo Furuncle l(l) Infected cyst l(1) Infected decubitus ulcer 9 (10) 4(11) Infected neurodermatitis l(l) Infected ulcer 1 (3) Paronychia 1 (3) Postoperative wound 7 (8) 1 (3) Pyoderma l(l) Pyoderma and infected ulcer l(1) Septic bursitis, l(1) 2 (5) Superficial abscess 11 (12) 3 (8) Wound infection l(1)
isolates, 14 of 330 ceftazidime isolates). Infections were of moderate severity in 64 (69%) cefepime pa- tients and 26 (70%) ceftazidime patients; 98% and 97% of infections, respectively, were considered acute. Duration of therapy was similar in both groups: 3- 18 days for cefepime, and 4- 16 days for ceftazidime. Between-treatment group differences were not significant.
The clinical response to cefepime was satisfactory in 82 (88%) of 93 evaluable patients with skin and skin-structure infections and unsatisfactory in 11 (12%). Clinical response to ceftazidime treatment was satisfactory in 33 (89%) of 37 evaluable patients and unsatisfactory in 4 (11%). The difference be- tween the two treatment groups was not statistically significant. A summary of clinical response by diag- nosis is presented in Table IV.
zidime) ; lack of pretreatment cultures (8,4) ; or lack of susceptibility testing (8, 5). Other reasons in- cluded resistant organisms ( 11,7) ; incomplete treat- ment or wrong dose ( 11, 8) ; other antibiotics re- ceived ( 10,B) ; and assessments or cultures not done per protocol (22, 12).
Diagnoses of skin and skin-structure infections in evaluable patients are summarized in Table II, and the susceptibility of pathogens most frequently iso- lated pretreatment is shown in Table III. There was only 4% resistance to each drug (13 of 336 cefepime
In the cefepime group, 92% (124 of 135 pathogens susceptible or of intermediate susceptibility to ce- fepime and ceftazidime) were eradicated (Table V ) . This included 47 (96%) of 49 isolates of S. au- reus, the most frequently isolated pathogen, 9 (90%) of 10 isolates of P. aeruginosa, and both Enterobac- ter isolates. There were 33 patients infected with more than one pathogen. Results in the ceftazidime group were similar: Overall, 95% (55 of 58) of path- ogens were eradicated, including the 18 isolates of S. aureus, 3 (75%) of 4 isolates of P. aeruginosa, and the one Enterobacter isolate. More than one pathogen was isolated from 16 patients. None of the between-group differences was significant.
SAFETY A total of 45 adverse events were reported by 17%
(33 of 199) of cefepime-treated patients compared with 32 in 19% (19 of 100) of patients in the cefta- zidime group (Table VI). Headache, diarrhea, con-
TABLE Ill Pretreatment Susceptibility of Pathogens to Study Drugs (All Patients)
Number of Pathogens* Cefepime Sensitivity+ Ceftazidime Sensitivityt
Pathogen susc. Inter. Res. Total susc. Inter. Res. Total
Streptococcus (Group A) 45 0 0 45 45 0 0 45 Streptococcus (a-hemolytic) 3 0 0 3 3 0 0 3 Staphylococcus aureus 100 3 1 104 82 21 1 104 S. aureus (methicillin-resistant) 2 1 5 8 1 2 4 7 S. aureus (methicillin-susceptible) 1 0 0 1 0 1 1 Staphylococcus epidermidis 14 0 0 14 13 1
: 14
Pseudomonas aeruginosa 26 0 1 27 26 0 0 26 Enterobacter species 1 0 0 1 1 0 0 1 Enterobacter cloacae 8 1 0 9 7 0 2 9
Susc. = susceptible; Inter. = intermediate; Res. = resistant. * Pathogens from both treatment groups were to be tested for susceptibility to each study drug. Partial list shown. + Bacterial isolates were tested for susceptibility by disc sensitivity or minimum inhibitory concentration (MIC) method. Based on disc susceptibility, susceptible = zone -18 mm; intermediate = zone 15-17 mm; resistant = zone ~14 mm. Based on MIC testing susceptible, MIC ~8 &mL; intermediate, MIC = 16 &mL; resistant, MIC ~32 pg/mL.
6A-92s June 24, 1996 The American Journal of Medicine@ Volume 100 (suppl 6A)

TABLE IV Clinical Response
Number of Patients Cefepime Ceftazidime
Diagnoses Sat. Unsat. Total Sat. Unsat. Total
Single diagnosis/single pathogen
Cellulitis 34 1 35 11 0 11 Mixed cellulitis* 3 1 i 2 0 2 Superficial abscess 8 1 3 0 3 Furuncle 1 0 1 0 0 0 Postoperative wound i 0 4 0 0 0 Infected ulcer 0 0 1 0 1 Infected decubitus ulcer 2 0 2 1 0 Other’ 4 1 5 2 1 :
Multiple pathogens
Cellulitis 15 1 16 11 12 Other’ Total patients (%I ii: (88)
6 17 2 :
4 11 (12) 93 33 (89) 4 (11) 37
Sat. = Satisfactory; Unsat. = Unsatisfactory. * Included cellulitis and superficial abscess, cellulitis and infected ulcer, pyoderma and infected ulcer. + Included infected cyst, wound infection, paronychia, septic bursitis, infected neurodermatitis, and multiple cellulitis infection. * included cellulitis and infected ulcer, cellulitis and superficial abscess, pyoderma, pyoderma and infected ulcer, superficral abscess, postoperative wound, and infected decubitus ulcer.
TABLE V Bacteriologic Response by Pathogen
Number of Pathogens’ Cefepime Ceftazidime
Pathogen Erad. Pers. Total Erad. Pers. Total
Streptococcus (group A) 19 0 19 12 0 12 Streptococcus (a-hemolytic) 1 1 2 0 0 0 Streptococcus tp-hemolytic) 1 0 1 0 0 0 Streptococcus species 7 0 7 4 0 4 Staphylococcus aureus 47 2 49 18 0 18 Staphylococcus aureus fmethicillin-resistant) 0 1 1 0 0 0 Staphylococcus koagulase-negative) 1 0 1 0 0 0
Staphylococcus epidermidis 7 0 7 3 1 Staphylococcus species 2 0 2 0 0 : Pseudomonas aeruginosa 9 10 3 4 Pseudomonas species 1
:, 1 0
:, 0
Escherichia coli 6 1 7 0 1 Klebsiella pneumoniae 5 0 5
: 0 2
Serratia marcescens 1 0 1 2 0 2 Proteus mirabilis 8 3 11 4 1 5 Other Enterobacteriaceae’ 9 11 6 0 6 Total pathogens 1%) 124 (92)
1: (8, 135 55 (95) 3 (5) 58
Erad. = eradicated; Pers. = persisted. Reponse was classified as “eradicated” if all original pathogens in that infection type were eradicated, or “persisted” if one of the original pathogens remained. * Based on 93 cefepime patients and 37 ceftazidime patients. + Included ~3 each of Edwardsiella tarda, Citrobacter diversus, Klebsiella oxytoca, Enterobacter cloacae, Proteus vulgaris, Morganella morgqsnii, Proteus stuartii, Pasteurella multocida, Acinetobacter anitratus, and Aeromonas hydrophila.
stipation, and nausea were reported most commonly pruritis, 2; fever, 1; headache, 1; and nausea, 1) were by cefepime-treated patients, whereas nausea, diar- considered probably related to therapy, and 5 events rhea, cough, rash, and edema were most common in in 4 patients were considered probably related to ceftazidime-treated patients. Seven of these common ceftazidime (nausea, 2; headache, 1; diarrhea, 1; events in 6 patients treated with cefepime (rash, 2; pruritis, 1). None of these events related to therapy
June 24. 1996 The American Journal of Medicine8 Volume 100 kuppl 6A) 6A-93s

SYMPOSIUM ON ANTIMICROBIAL THERAPY/SCHWARTZ ET AL
was severe. In neither treatment group was diarrhea due to Clostridium d@i&e. No patients treated with cefepime, and one treated with ceftazidime dis- continued treatment because of an adverse event (rash). There were no significant differences be- tween the two groups.
Most abnormalities in clinical laboratory test re- sults during treatment with either study drug were not clinically relevant. One patient with cellulitis had elevated liver function tests that resulted in discon- tinuation of cefepime therapy. These liver function tests improved within 1 week of terminating therapy and returned to normal by posttreatment day 42.
Administration of study antibiotics was well tol- erated by 96% of patients receiving cefepime and 98% of those receiving ceftazidime. Infiltration at the site of infusion occurred in 2% of patients in each group. In no case was treatment discontinued because of local intolerance.
DISCUSSION The results of this trial demonstrate that cefepime
(1 g every 12 hours) is effective for the treatment of serious skin and skin-structure infections. The clin- ical response and bacteriologic eradication rates were high (88% and 92%, respectively) and were comparable with those observed with ceftazidime (1 g three times daily; 89% and 95%, respectively). These results are in agreement with those from an open trial of 22 patients in which the clinical re- sponse rate to cefepime was 91% and the bacterio- logic eradication rate was 81%.4 Several other stud- ies, using 1 g twice daily and 2 g twice daily also demonstrated efficacy and safety in the management of skin and skin-structure infections.5-s
Both cefepime and ceftazidime are broad-spec- trum antimicrobial agents that demonstrate in vi- tro activity against most pathogens likely to cause
skin and skin-structure infections (staphylococci, Enterobacteriaceae, and streptococci). In the present trial and that by Oster and coworkers, 4 in- fections primarily were due to S. aureus and strep- tococci. Of pathogens isolated before treatment, only 4Oh were resistant to cefepime. This low resis- tance pattern in a multicenter study suggests that skin and skin-structure infections will likely re- spond to cefepime treatment regardless of geo- graphic location. In this study, cefepime demon- strated excellent efficacy against S. aureus, P. aeruginosa, and Enterobacter species.
Because of their excellent safety profile (as well as efficacy), parenteral cephalosporins have an es- tablished role in the treatment of skin and skin-struc- ture infections in hospitalized patients as well as out- patients with complicated infections with more resistant pathogens. In this study, cefepime was well tolerated, with only 7 adverse events attributable to cefepime therapy; none required discontinuation. Most abnormal laboratory values were not clinically relevant and returned to normal after treatment was completed. The safety profile of cefepime was simi- lar to that of eeftazidime and consistent with those reported for other parenteraI cephalosporins. It is also noteworthy that many patients had underlying illnesses (40% cardiovascular disease, 29% diabetes mellitus), and that most received concomitant med- ications (94% received at least one and 26% at least four).
In conclusion, the results of this study demon- strated that the excellent clinical and bacteriologic efficacy of cefepime against skin and skin-struc- ture infections is comparable to that of ceftazi- dime. Cefepime was well-tolerated, and no patient discontinued treatment because of adverse events. Cefepime, administered every 12 hours, is an ef- fective, well-tolerated, and convenient, alternative
TABLE VI Summary of Most Frequently Reported Adverse Clinical Events by Relationship to
Study Drug *
Number (%) Patients Cefepime (n = 198) Ceftazidime (n = 100)
Event Prob. Not Unk. Total Prob. Not Unk. Total
Headache 1 2 7 10 (5) 1 0 0 l(1) Diarrhea 0 2 2 4 (2) 1 0 2 3 (3) Constipation 0 2 1 3(Z) 0 0 0 Nausea 1 1 1 3(Z) 2 2 2 6 (6) Cough 0 0 0 0 0 2 0 2 (2) Rash 2 0 : 2(l) 0 0 1 1 (1) Edema 0 0 0 0 0 2 2 (2)
Data are number 1%) of patients. Prob. = probably related to therapy; Not = not related; Unk. = unknown relationship. * Patients may have reported more than one adverse event.
6A-94s June 24, 1996 The American Journal of Medlcinee Volume 100 lsuppl 6A)

SYMPOSIUM ON ANTIMICROBIAL THERAPY/SCHWARTZ ET AL
to ceftazidime administered every 8 hours for the treatment of serious skin and skin-structure infec- tions.
ACKNOWLEDGMENTS The following investigators also enrolled patients in this trial: R. Bolivar-Bri.
cero, MD, Houston, TX; J. Daly, MD, Brighton, MA; S. Farkas, MD, Barberton,
Off; S. Forlenza, MD, East Meadow, NY; R. Gainer, MD, Morgantown, WV; M.
Gelfand, MD, Memphis, TN; S. Handwerger, MD, New York, NY; P. Jurgensen,
MD, Savannah, GA; C. Lerner, MD, San Antonio, TX; T. Madhaven, MD, Madison
Heights, MI; L. Parish, MD, PhIadefphra, PA: G. Plotkin, MD, WilkesBarre, PA;
R. Prance, PharMD, fowa City, IA; B. Sreger, MD, Orlando, FL; T. Sorg, MD,
Dayton, OH; B. Yangco, MD, Tampa, FL.
1. Swartz MN. Cellulibs and subcutaneous tissue infections. In: Mandell GL,
Douglas RG Jr, Bennett JE, eds. frincipfes and Practice of Infectious Diseases,
4th ed. New York: Churchill Livingstone, 1995:909-929.
2. Kessler RE, Bies M, Buck RE, et al. Comparison of a new cephalosporin,
BMY 28142, with other broad-spectrum @actam antrbiobcs. Antimicrob Agents
Chemother. 1985;27:207-216. 3. Fung-Tome J, Dougherty T, DeOrro F, SimrchJacobson V, and Kessler RE.
Activity of cefepime agarnst ceftazidime- and cefotaxime-resistant gramnega-
tive bacteria and its relationship to p-lactamase levels. Antimicrob Agents Chem
other. 1989;33:498-502. 4. Oster S, Edelstein H, Cassano K, McCabe R. Open trial of cefepime (BMY
28142) for infections in hospitalized patrents. Antimrcrob Agents Chemother.
1990;34:954-957. 5. Giamarellou H. Low-dosage cefepime as treatment for serious bacterial In-
fections. J Antimicrob Chemother. 1993;32(suppl B):123-132. 6. Jaurequi L, Matzke D. Scott M, Minns P, Hageage G. Cefepime as treatment
for osteomyelrtis and other bactenal rnfections. J Antimicrob Chemother.
1993;32fsuppl B):141-149. 7. Mouton Y, Chidiac C, Humbert G, et al. Anoncomparative, mulhcentre study
of cefepime in the treatment of serious bacterial infections. JAntirnrcrob Chem
other. 1993;32tsuppl B):133-140.
8. Hoepelman A, Kieft H, Aoun M, et al. International comparative study of
cefepime and ceftazidime in the treatment of serious bacterial infections. J
Antrmicrob Chemother. 1993;32(suppl B):175-186.
June 24, 1996 The American Journal of Medrcine” Volume 100 (SUPPI 64) 6A-95s