current and novel endoscopic therapies for luminal cancers
TRANSCRIPT

Current and Novel Endoscopic Therapies for Luminal Cancers
Kenneth K. Wang, MDDirector Advanced Endoscopy Group
Van Cleve Professor of Gastroenterology Research
Mayo Clinic, Rochester, MN

Aims• Describe what is meant by an early Barrett’s esophageal cancer
• Understand the risk of metastasis of early esophageal adenocarcinoma
• Understand the biology of early cancer lesions• Formulate a strategic approach to early esophageal cancers

Curative Esophagectomy in Barrett’s Esophagus
• 22 studies with 530 patients who underwent esophagectomy for Barrett’s esophagus with high grade dysplasia
• 0.94% mortality rate• 17 studies without any reported mortality• Total of 5 deaths reported from expert centers

Rationale for Endoscopic Approaches
Birkmeyer JD, et al. N Engl J Med. 2002;346:1128–1137.
2018
16
11
8
0
5
10
15
20
25
<2 2–4 5–7 8–19 >19
Number of Esophagectomies
Adjusted
Mortality Ra
tes (%)

The Therapeutic Balance
Risk of DeathBenefit to Patient

Early Cancer
Risk of Metastasis in Early Esophageal Adenocarcinoma
• T1a cancers– Above the muscularis mucosae– 61 studies published to date– 1350 patients– Overall risk of metastasis 1.9% (1.2‐2.7%)
Dunbar, Am J Gastroenterol 2012; 107:850–8

Metastatic T1a ACA: n=26• Most were M3 cancers
– M2 cancer described– No M1 cancers
• Lymphovascular invasion in 2• Poorly differentiated tumor in only one
cancer
Dunbar, Am J Gastroenterol 2012; 107:850–8
Do Early Cancers Possess Metastatic Potential ?
• 10 surgically resected early cancers T1a without metastatic spread
• All 10 expressed markers of epithelial mesenchymal transition (Slug, Snail, Twist) as well as CD133 marker of cancer stem cells
• These markers were uniform across the tumor
Tomizawa, Oncology Letters,2:1059‐1063. 2012

Early Cancer Survival
Rice, Ann Surg Oncol (2010) 17:1721–1724

Squamous Cell Cancersn=190
Gastrointest Endosc 2011;73:881‐9

Undifferentiated Cancers
• 153 pts with gastric undifferentiated cancer• 101 underwent ESD, 52 underwent surgery• Curative resection in 83%, en bloc resection in 99%
• Median follow‐up 40 months• 1 synchronous and 1 metachronous cancer (3%)
• 97% 5 year disease free survival
Okada, Endoscopy 2012; 44: 122–127

Factors in Decision Making
PatientPatient
Endoscopic ExpertiseEndoscopic Expertise
Surgical ExpertiseSurgical Expertise
LesionLesion
PersonalityPersonality

Early Cancer Approach
• EUS: +/‐• Biopsy before EMR• Nodule: 40% risk of cancer (Gastroenterology 2001;120:1630‐
9)
• EMR– Defines depth of invasion
• T1a: Superficial, above muscularis mucosa• T1b: Submucosal, increased risk of mets

Defining Lesions to be Removed
• Dye spraying– Surface enhancement dyes– Dyes with cellular absorption
• Narrow band imaging– Enhanced detection of borders of lesions– Sensitivity not sufficient
• Marking borders of lesions with cautery

Tumor
Submucosa
T1a Cancer

Do You Need EUS ?
• EUS is primarily used to determine unresectability
• If EUS shows submucosal invasion, most likely is invasive
• If EUS shows mucosal disease, submucosalinvasion present in 40% (Gastrointestinal Endoscopy, 2005. 62(1): p. 16‐23)
• Assessment of lymph node status

Case
• 78 year old white male under surveillance for Barrett’s esophagus for 3 years. Recently developed high grade dysplasia in a C3M5 Barrett’s segment– PMH: COPD, ASHD, Sleep Apnea
• Ablation with RFA performed • Complete elimination of all dysplasia and IM• Returns for surveillance at 18 months after complete response

Confocal Laser Microscopy Probe

Volumetric Laser Endomicroscopy

Removing the Mucosa
• Endoscopic Mucosal Resection: Snare
• Endoscopic SubmucosalDissection: Knife

Why Perform Endoscopic Mucosal Resection ?
• Actual histological diagnosis. Best endoscopic assessment of depth of invasion (Wang, Journal of Gastrointestinal Surgery 2010;14:946‐7)
• Improves histological diagnosis over biopsies (Nijhawan, Wang. Gastrointestinal Endoscopy 2000;52:328‐32)

Why Perform Endoscopic SubmucosalDissection
• En bloc resection of lesion – Decreased recurrence– Ability to assess margins with larger lesions (>1.5 cm) (Cao, Endoscopy 2009;41:751‐7)
– Increased bleeding and perforation

Human Esophagus
Muscularis mucosae
Submucosa
Muscularis propria
Mucosa
EMR/ESD Resection
Biopsy

Cap EMR

Mayo Experience
• 466 pts, 386 males and 80 females– Median age 70 (IQR 60‐76)– EUS prior to EMR– 807 EMR session
• 558 (69%) single EMR• 162 (20%) double EMR• 87 (11%) >2 EMR (16 maximum)

Complications
• Complications– 51 (6%) strictures (PDT)– 11 (1%) bleeding– No Perforations

Efficacy of EMR and Ablation for T1a Adenocarcinoma
0.00.10.20.30.40.50.60.70.80.91.0
Sur
vivi
ng
0 10 20 30 40 50 60 70 80 90 100 120 140accurint overall survival
• EMR + Ablation: 42 +2.5 mths• Follow‐up
• Endoscopic 43 mths• Surgery: 64 mths
• N=178• Surgery 46• Endoscopic 132
Gastroenterology 2009;137:815‐23.
Surgery
EMR + Ablation

EMR Treatment of Early Esophageal Cancer
• 100 consecutive early low risk cancers
• All treated with endoscopic resection
• 11% recurrence rate with 37 month follow‐up
Ell, Gastrointest Endosc 2007;65:3‐10

ESD
• Initial circumscribed incision: Needle Knife• Early submucosal dissection: Initiate with Hook knife
• Late submucosal dissection: After a “flap” is created, IT or ceramic tip knife

Submucosal Dissection

Endoscopic Submucosal Dissection

Outcomes ESD
• High rate of en bloc resection
• Low rate local recurrence
• Ease of performance– Gastric easiest– Esophagus moderate– Colon most difficult
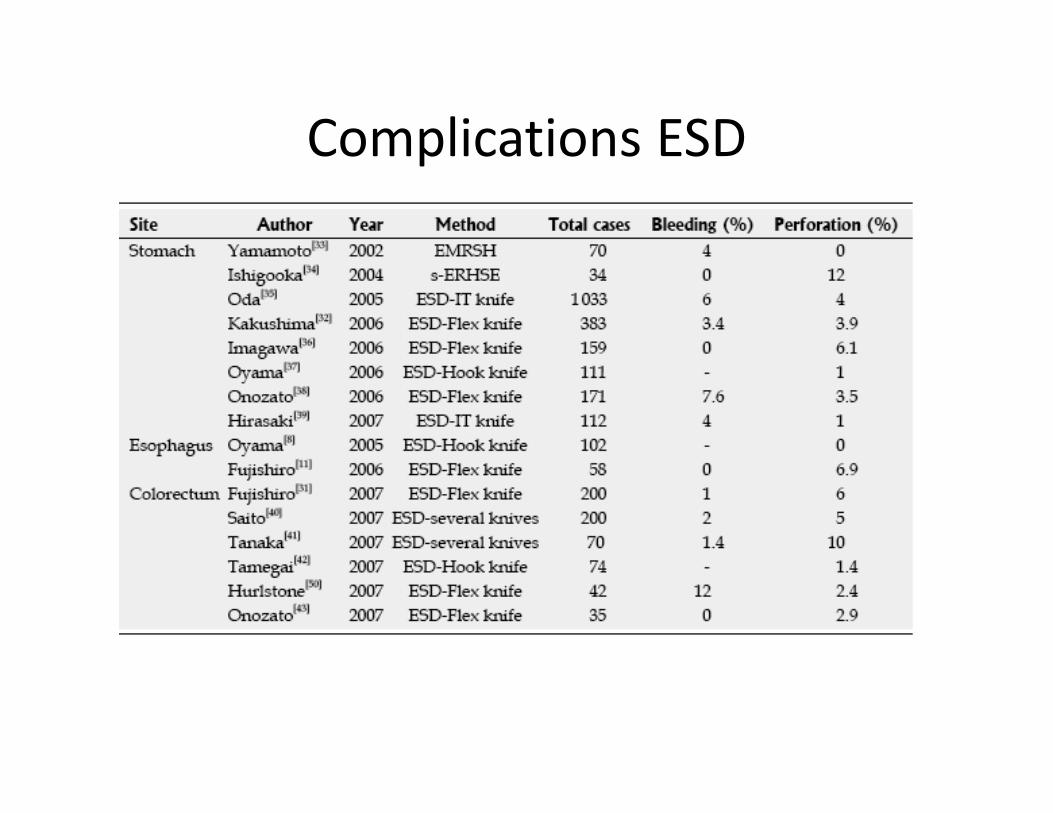
Complications ESD
World J Gastroenterol 2008 May 21; 14(19): 2962‐2967

Frozen Section EMR
• 30 EMR frozen• Kappa 0.8 for margins
• Kappa 0.93 for depth of invasion
Clinical Gastroenterology And Hepatology 2006;4:173–178

Overstich
• Endoscopic suturing device• Can create running suture to close a perforation

Mayo Experience Submucosal Cancer
• 1260 esophagectomies were performed during the selected study period.
• 120 patients had evidence of submucosal invasion.
• Slides of 70 patients were available for review
• The distribution of submucosal invasion was: sm1 in 24 (34%), sm2/3 in 46 (66%)
Clinical Gastroenterology & Hepatology 8(3): 248‐253, 2010

Submucosal Cancer
0.00.10.20.30.40.50.60.70.80.91.0
Sur
vivi
ng
0 10 20 30 40 50 60 70 80 90 100 110 120130 140overall survival,months( accurint-surg date)
SM1
SM2‐3
SM1 cancers had similar metastatic risk as SM2‐3

Mucosal Resection versus Endoscopic Mucosal Dissection
EMR ESD
Technique Easy Hard
Training Relatively short Long
Duration of Procedure Short, 10 minutes Long, 1.5 hours
Complications Manageable Serious
Effectiveness <15 mm lesions >15 mm lesions
Depth of resection Submucosa Submucosa
Best lesions type Flat, elevated, well differentiated
Flat, elevated, well differentiated

Controlled by two variables: – Primary: Length of tissue freeze
time – Secondary: Repetitions of freeze–
thaw cycles
4 x 10 seconds =
Lamina Propria to shallow
Submucosal injury
3 x 20 seconds =
Submucosal injury
0.5 mm
Am J Gastro 2006;101:S532. Cryo Spray Ablation (CSA) in the Esophagus: Optimization of Dosimetry.
Dosimetry

Cryotherapy Systems
CSA Medical, Inc. GI Supply, Inc.
Liquid nitrogen at -196°CLow-pressure systemElectrically warmed 7F catheterFoot pedal activation
Compressed CO2 at -78°C (Joule-Thompson effect)High-pressure system (8 L/min)Evacuation tubingFoot pedal activation

Results
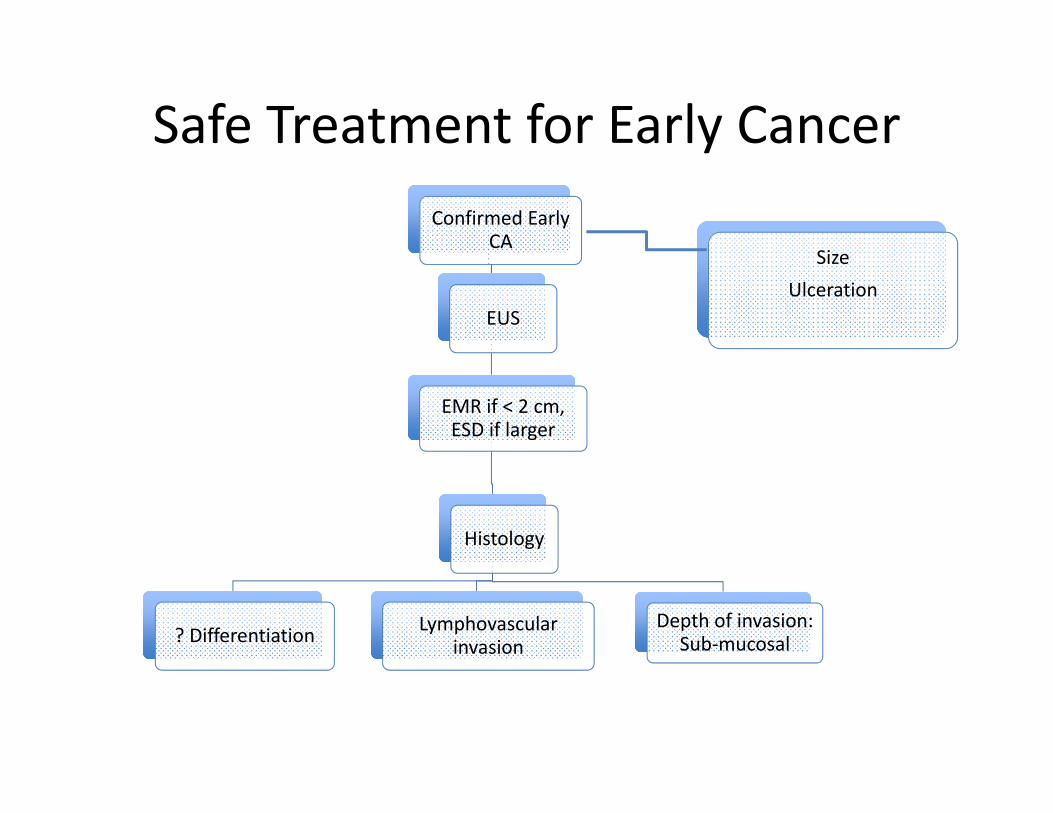
Safe Treatment for Early CancerConfirmed Early
CA
EUS
EMR if < 2 cm, ESD if larger
Histology
Lymphovascularinvasion
Depth of invasion: Sub‐mucosal? Differentiation
SizeUlceration

Summary
• Early cancer can be endoscopically treated– T1a lesion– No evidence of metastatic disease
• EMR/ESD for staging and treatment• Follow up mucosal ablation in high risk patients