current management of splenic trauma no financial disclosures
TRANSCRIPT
Current Management of Current Management of Splenic TraumaSplenic Trauma
No financial disclosures

Historical Milestones2nd-12th Cent. Seat of emotions; source of
laughter, mirth, anger, malice or bad temper, latent malevolence, melancholy, depression, black bile cleanse the blood
1549 First splenectomy for disease
1590 Partial splenectomy for trauma
1678 Total splenectomy for trauma

Historical Milestones, cont’d
1892 Splenectomy for blunt trauma
1900 Nonoperative Tx associated with mortality of 90-100%
Prevalence of “delayed rupture” (15-30%)
1895-1930 Splenorrhaphy, partial splenectomy

“Injuries of the spleen demand excision of the gland. No evil effects follow its removal, while the danger of hemorrhage is effectually stopped.”
Kocher, 1911

Historical Milestones, cont’d
1952 Increased infection in children after splenectomy
1969 Overwhelming Post Splenectomy Infection (OPSI)
1971 Nonoperative management of spleen (pediatric patients)
1990’s Nonop management in adults

Epidemiologic Facts Related to Epidemiologic Facts Related to Infections after SplenectomyInfections after Splenectomy
Pneumococcal pneumonia is a common community acquired pneumonia
Post splenectomy cases often poorly documented
Other risk factors for pneumonia/infection are often present
Not all infections after splenectomy are OPSI
Therefore ……Therefore ……
What is the risk of OPSI after splenectomy?
Best guess is < 1% in adults after trauma (0.02-0.2%)
More frequently rapidly fatal in adults (less meningitis)
Impact of immunization after splenectomy

Diagnostic Modalities Influence Diagnostic Modalities Influence Treatment of Blunt Splenic InjuriesTreatment of Blunt Splenic Injuries
Physical Exam Physical Exam (premodern era) (premodern era)
Physical Exam (modern Physical Exam (modern era)era)
DPLDPL
Computed tomographyComputed tomography
?Ultrasound/CT??Ultrasound/CT?
No specific treatmentNo specific treatment
SplenectomySplenectomy
SplenorrhaphySplenorrhaphy
Nonoperative Nonoperative managementmanagement
??????????
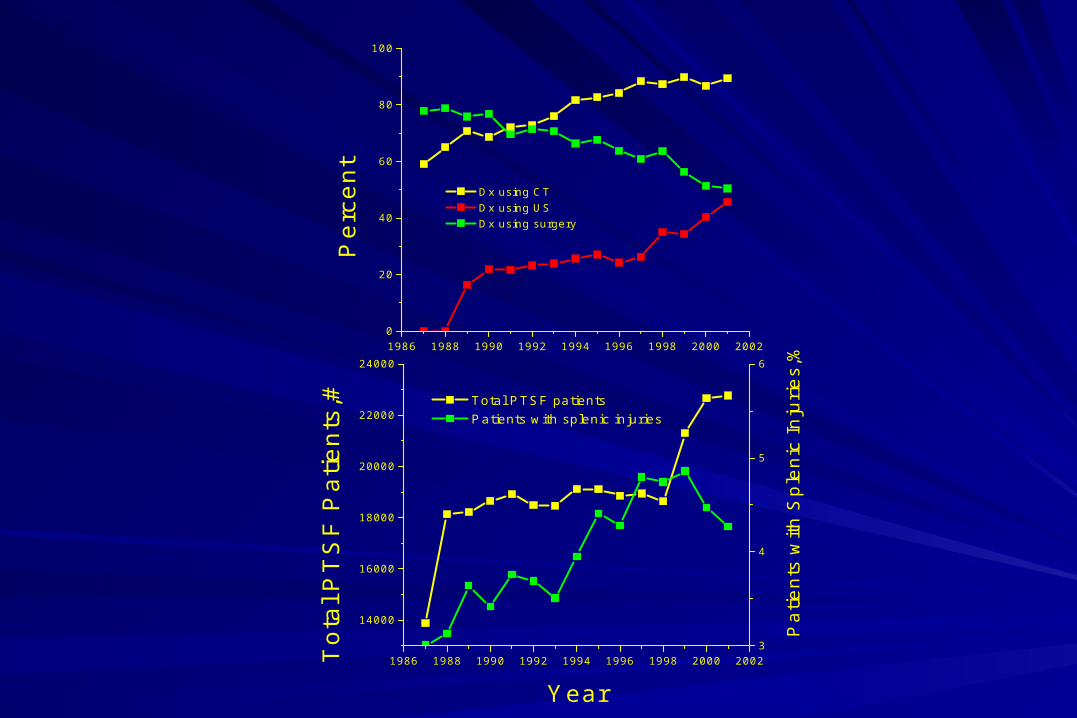
1986 1988 1990 1992 1994 1996 1998 2000 20020
20
40
60
80
100
Per
cent
Dx using CT Dx using US Dx using surgery
1986 1988 1990 1992 1994 1996 1998 2000 2002
14000
16000
18000
20000
22000
24000
Total PTSF patients Patients with splenic injuries
Year
Tot
al P
TS
F P
atie
nts,
#
3
4
5
6
Pat
ient
s w
ith S
plen
ic In
jurie
s,%

Magnitude of Splenic Injury is Magnitude of Splenic Injury is changing over timechanging over time
1986 1988 1990 1992 1994 1996 1998 2000 20020
100
200
300
400
500
600
700
800
900
1000
Nu
mb
er
of P
atie
nts
Year
All Injuries 865.04 865.03 865.02 865.01
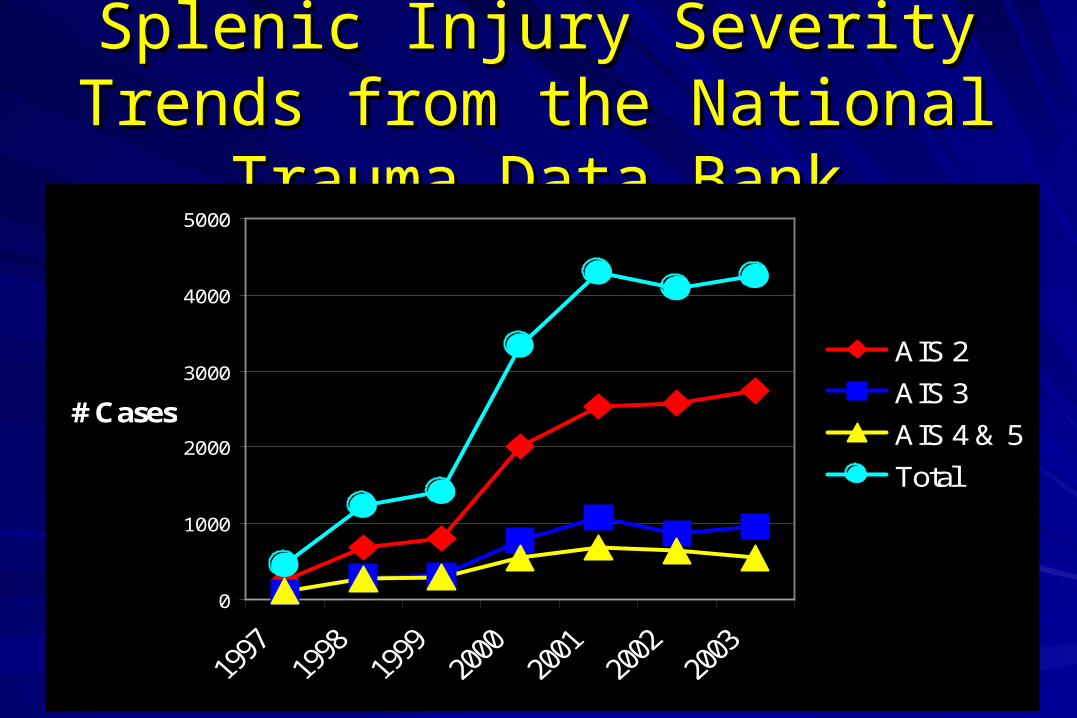
Splenic Injury Severity Trends from Splenic Injury Severity Trends from the National Trauma Data Bankthe National Trauma Data Bank
0
1000
2000
3000
4000
5000
# Cases
AIS 2
AIS 3
AIS 4 & 5
Total
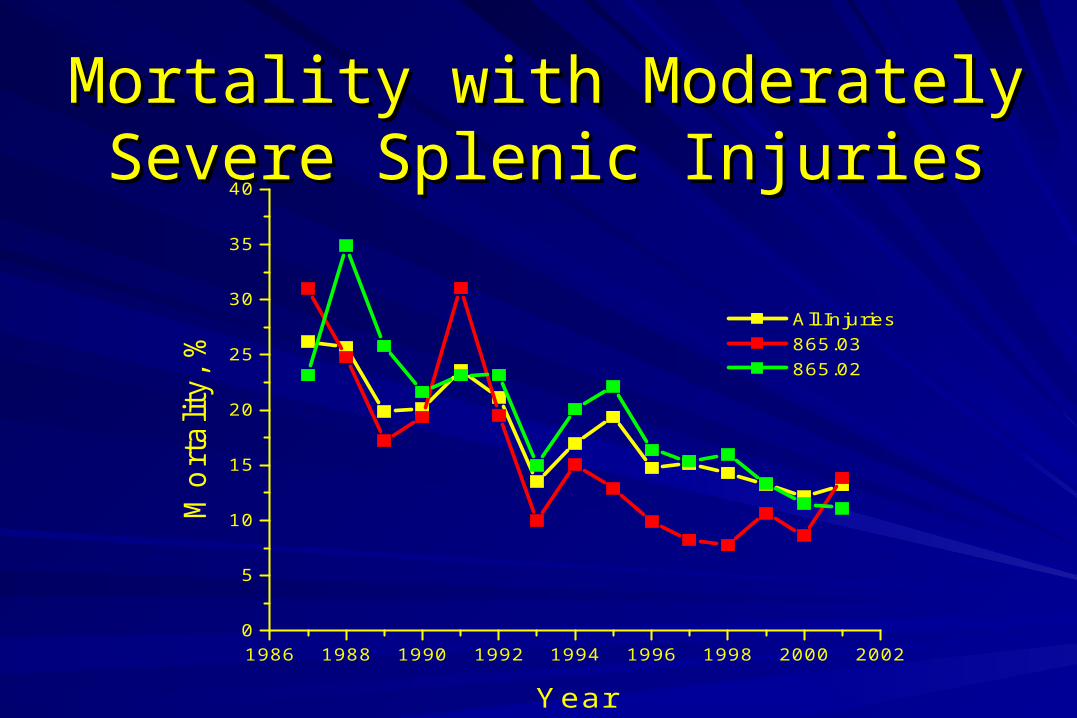
Mortality with Moderately Severe Mortality with Moderately Severe Splenic InjuriesSplenic Injuries
1986 1988 1990 1992 1994 1996 1998 2000 20020
5
10
15
20
25
30
35
40M
ort
alit
y, %
Year
All Injuries 865.03 865.02

1986 1988 1990 1992 1994 1996 1998 2000 20020
10
20
Year
Per
cent
40
50
60 MV
C, P
ercent
MVC
Other
Fall
Mechanism of Injury is changing over time
MCC, Assaults, Peds struck were unchanged
Nonoperative treatment is the most Nonoperative treatment is the most common form of management for common form of management for
blunt splenic injuries blunt splenic injuries
More frequent use of CT for diagnosis/triageMore frequent use of CT for diagnosis/triage
More low magnitude splenic injuriesMore low magnitude splenic injuries
Low velocity accidentsLow velocity accidents
Decreased overall number/severity of associated Decreased overall number/severity of associated injuriesinjuries
Delay in Tx
Missed Injuries
Risk of operation
OPSI
Nonoperative Management
Operative Management

Operative vs Nonoperative Tx
Is this splenic injury actively bleeding?(likely to bleed)?

Splenic Injury with extravasation of Splenic Injury with extravasation of contrastcontrast

Minor Blunt Splenic InjuryMinor Blunt Splenic Injury
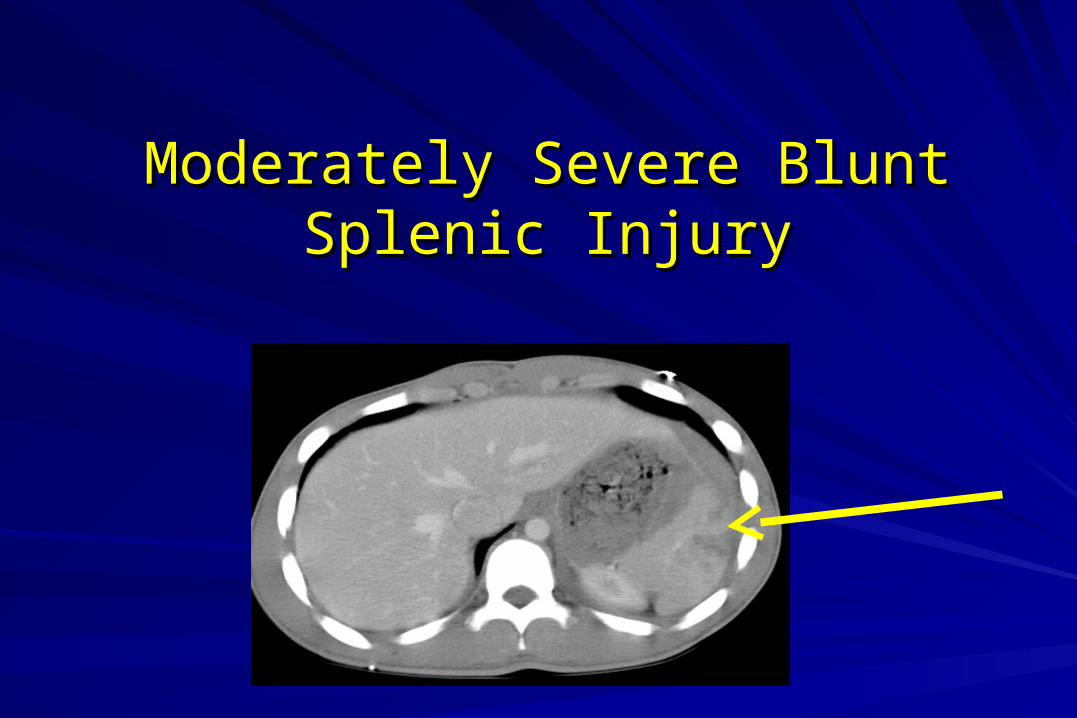
Moderately Severe Blunt Splenic Moderately Severe Blunt Splenic InjuryInjury

Grade of Splenic InjuryGrade of Splenic InjuryI Hematoma subcapsular, <10%
Laceration < 1cm deep
II Hematoma subcapsular, 10-50%
intraparenchymal, <5 cm
Laceration 1-3 cm deep
III Hematoma >50%, ruptured, >5cm
Laceration >3 cm, + trabecular vessels
IV Laceration segmental or hilar vessel with major devascularization
V Laceration shattered spleen, avulsion

Grade of Splenic Injury Grade of Splenic Injury correlates with success of NOMcorrelates with success of NOM
EAST, J Trauma 2000
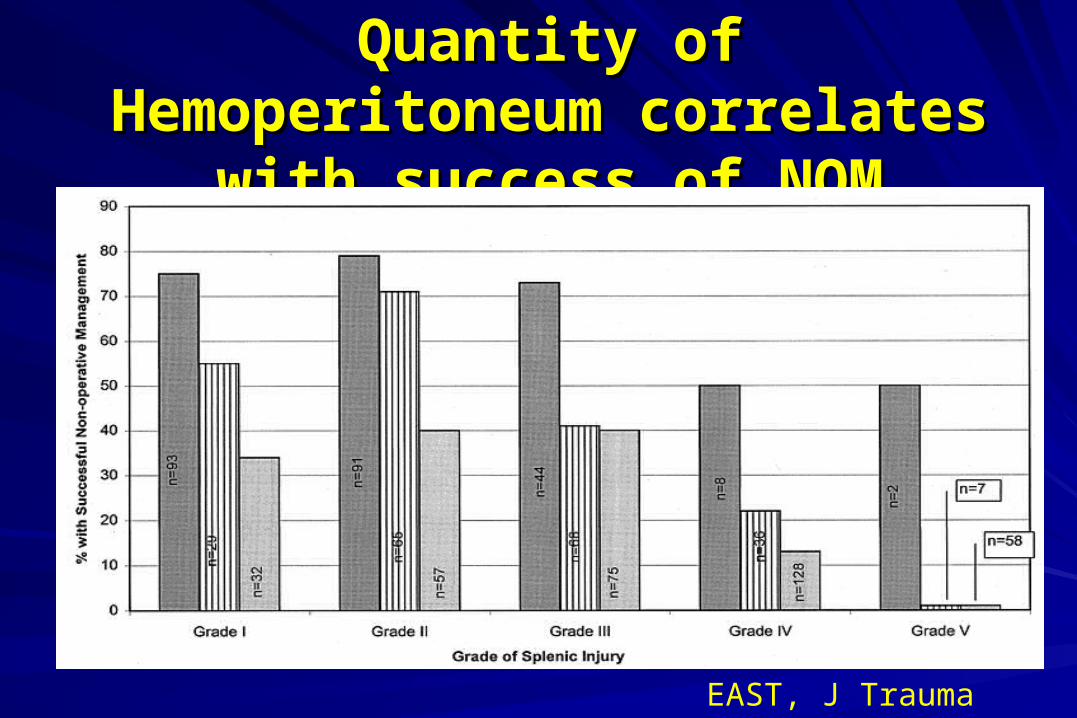
Quantity of Hemoperitoneum Quantity of Hemoperitoneum correlates with success of NOMcorrelates with success of NOM
EAST, J Trauma 2000
1 2 310
15
20
25
30
35
40
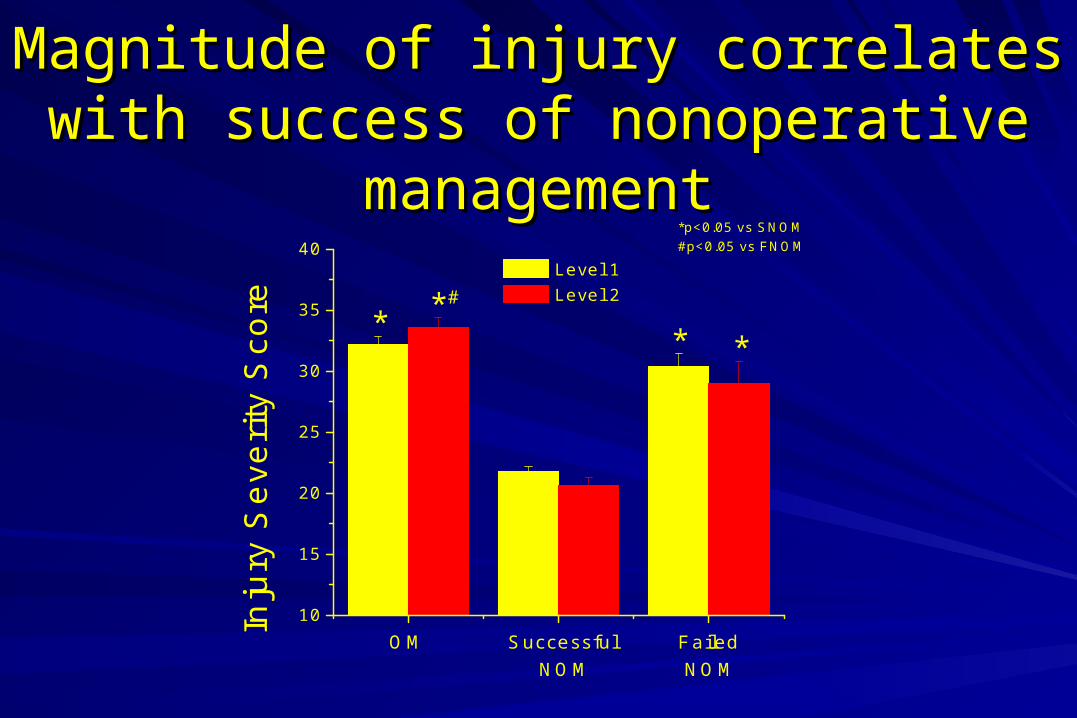
*p<0.05 vs SNOM#p<0.05 vs FNOM
#****
Failed NOM
Successful NOM
OM
Inju
ry S
ever
ity S
core
Level 1 Level 2
Magnitude of injury correlates with Magnitude of injury correlates with success of nonoperative managementsuccess of nonoperative management

1 2
0
20
40
60
80
@p=.054 vs Age#p<0.05 vs Age
*p<0.05 vs Successful
Unsuccessful Nonop
Successful Nonop
** @,
#
#29.212.3
8.33.6%
of Patients
Age<55 Age>55
Age impacts Nonoperative Management

Blunt splenic injury in adultsBlunt splenic injury in adults
Selection of adults for treatment of blunt splenic Selection of adults for treatment of blunt splenic injuryinjury
– hemodynamic stability statushemodynamic stability status
– severity of injury (ISS)severity of injury (ISS)
– grade of splenic injurygrade of splenic injury
– quantity of hemoperitoneumquantity of hemoperitoneum
– AgeAge
– ? Co-morbidities ?? Co-morbidities ?

0
50
100
150
200#
Pa
tien
ts
Op Success Nonop
Failed Nonop
37%
93.5% 6.5%
ULH Experience 1/2009-6/2010

0
2
4
6
8
10
12
14
Failed Nonop
Success Nonop
Op
Mo
rta
lity,
%15/136
11/216
2/15
EAST 25.9%Smith 23.2%
EAST 4.2%Smith 8.6%
EAST 16.5%Smith 8.2%

Kentucky Pediatric Experience

What should the surgeon do with What should the surgeon do with high grade splenic injuries?high grade splenic injuries?
Proportionately less common injuriesProportionately less common injuries
Some can be managed nonoperatively but which ones?Some can be managed nonoperatively but which ones?
Price associated with failure (morbidity, mortality) is realPrice associated with failure (morbidity, mortality) is real
Problem with using historical controlsProblem with using historical controls
Impact of patients taken directly to the operating roomImpact of patients taken directly to the operating room
Does angiography have an impact?Does angiography have an impact?

Splenic Artery EmbolizationSplenic Artery EmbolizationAngiography for diagnosis reported in 1957
Angiography for hemostasis reported in 1981
(gelfoam-2, coil-1, vasopressin-1)
Angiography as a triage tool reported in 1991
44 stable patients 1984-87
19 without extravasation on angio
17 with extravasation embolized
8 underwent laparotomy (no angio)

Splenic Artery Embolization, Splenic Artery Embolization, cont’dcont’d
Angiographic technique affects splenic vessel recanalization and splenic function
Proximal vs Distal
Coil vs gelfoam/clot
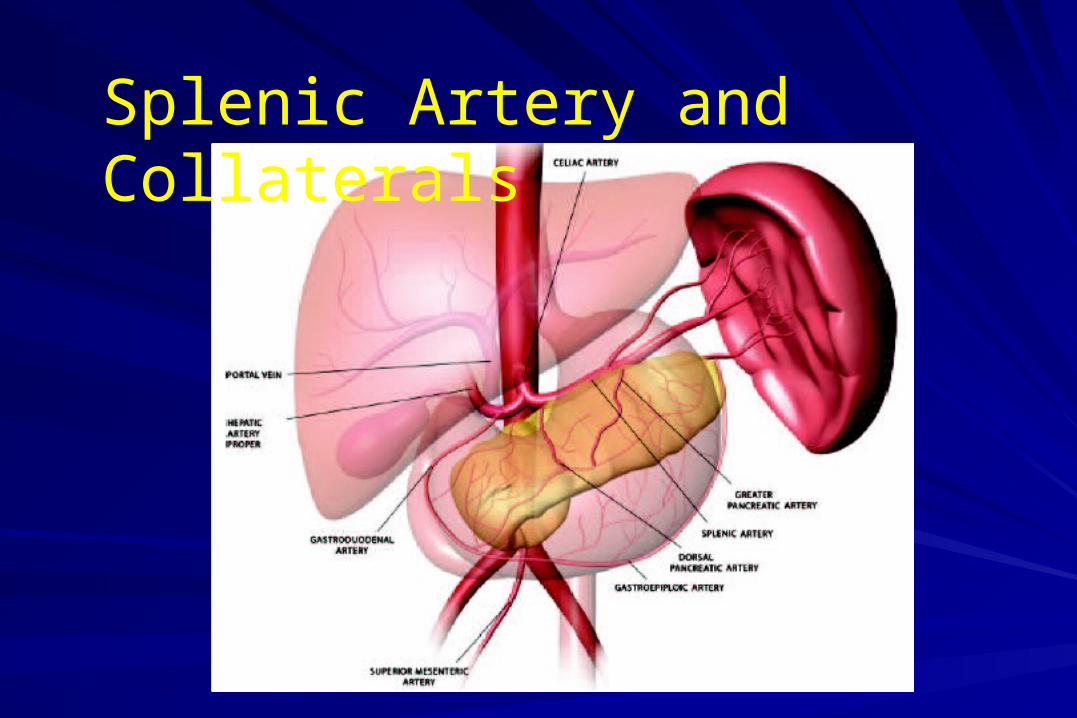
Splenic Artery and Collaterals

Does angiography/embolization Does angiography/embolization improve splenic salvage?improve splenic salvage?
Haan et al, J Trauma 2004Haan et al, J Trauma 2004
Multicenter study, n=155 w/ embolizatonMulticenter study, n=155 w/ embolizaton
Splenic salvage of 87% reportedSplenic salvage of 87% reported
Failure rate of 14%, infarction rate of 27%Failure rate of 14%, infarction rate of 27%
? how many patients had angio without ? how many patients had angio without embolization ?embolization ?
Compared to historical controlsCompared to historical controls
Does angiography/embolization Does angiography/embolization improve splenic salvage?improve splenic salvage?
Dent et al, J Trauma 2004Dent et al, J Trauma 2004Report 168 injuries, 13 patients undergoing Report 168 injuries, 13 patients undergoing
emboembo
Overall nonop success rate of 98%Overall nonop success rate of 98%
Did not stratify by injury gradeDid not stratify by injury grade
Compared to historical controlsCompared to historical controls
38% required repeat angio/embo38% required repeat angio/embo

Does angiography/embolization Does angiography/embolization improve splenic salvage?improve splenic salvage?
Haan et al, J Trauma 2005Haan et al, J Trauma 2005
Protocolized angio/embo (all patients after Protocolized angio/embo (all patients after CT then only grades 3-5 deemed CT then only grades 3-5 deemed stable) (? n=298 ?)stable) (? n=298 ?)
Nonop success rate of 83-87% for grade 3-5Nonop success rate of 83-87% for grade 3-5
Not clear how this compared to no angio ptsNot clear how this compared to no angio pts
Compared to historical controls (8 yr old data)Compared to historical controls (8 yr old data)
UPMC ExperienceUPMC Experience
570 patients with blunt splenic trauma from 2000-570 patients with blunt splenic trauma from 2000-20042004
221 patients - immediate operation (39%)221 patients - immediate operation (39%)
349 patients - attempted nonoperative Tx 349 patients - attempted nonoperative Tx
46 (13%) underwent angio & 28 embolization46 (13%) underwent angio & 28 embolization
Decision of trauma attending (no protocol)Decision of trauma attending (no protocol)

UPMC ExperienceUPMC Experience
2000 2001 2002 2003 20040
10
20
Per
cent
age
unde
rgoi
ng
angi
o
Year
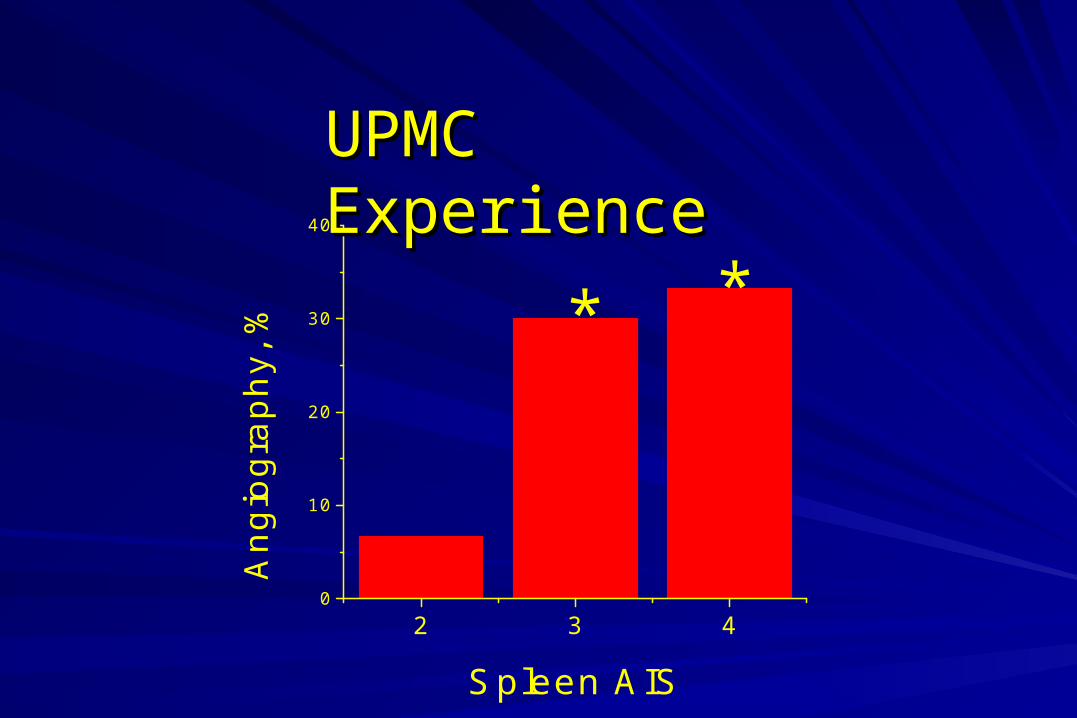
2 3 40
10
20
30
40
*A
ngio
grap
hy, %
Spleen AIS
*
UPMC ExperienceUPMC Experience

UPMC ExperienceUPMC Experience
2 3
0
20
40
60
80
100N
onop
Suc
cess
, %
Spleen AIS
Angio No Angio
2 3-5

Splenic Injury Presenting 3 Days Splenic Injury Presenting 3 Days after Fallafter Fall
Pseudoaneurysm

Delay in Tx
Missed Injuries
Risk of operation
OPSI
Nonoperative Management
Operative Management

Fry 1980
Wiseman 2006
Demetriades 2012
U of L09-10
U of LIsolated Spleen
Abd Abcess 11% 9% 6.2% 5% 0%
Wound Infection 16% 4% 8.2% 1.0% 0%
PancreatitisPanc Fistula
17% ----- ----- 1.0% 0%
Wound Dehis 5% ----- ----- 0% 0%
Hemorrhage ----- ----- ----- 1.0% 0%
Pneumonia 33% 30% 14.4% 23% 6%
Sepsis/Bacteremia 8% 19% 12.4% 3.0% 0%
UTI ----- 12% 2.1% 6.0% 6%
DVT/PE ----- ----- ----- 12% 0%
Complication Rates after Splenectomy
ConclusionsConclusions
More splenic injuries are being identifiedMore splenic injuries are being identifiedMore frequent use of CTMore frequent use of CTMore minor injuriesMore minor injuriesLow velocity mechanismsLow velocity mechanismsNumber of severe injuries unchangedNumber of severe injuries unchanged
Careful patient selection for nonoperative manage-Careful patient selection for nonoperative manage-ment is essential for severe injuriesment is essential for severe injuries
Morbidity and mortality are increased in Morbidity and mortality are increased in patients that patients that ultimately fail nonoperative Tx compared to patients who do ultimately fail nonoperative Tx compared to patients who do
not fail (?poor selection or failure-induced morbidity?)not fail (?poor selection or failure-induced morbidity?)

ConclusionsConclusions
Role of angiography remains to be definedRole of angiography remains to be definedtriage tool vs selective applicationtriage tool vs selective application
Splenectomy patients do suffer complicationsSplenectomy patients do suffer complicationsRate due to splenectomy itself is lowRate due to splenectomy itself is low
Role of associated injuriesRole of associated injuries
Patients still die of splenic injuriesPatients still die of splenic injuries
stop the hemorrhagestop the hemorrhage


Splenic Function, cont’dSplenic Function, cont’d
Immune Surveillance
White pulp (25% spleen volume)= lymphoid compartment
Bind Ag & differentiate into Ab-secreting cells
Initial site of IgM after bacterial challenge
Removal of opsonized particles

Embolization for Splenic Artery Embolization for Splenic Artery PseudoaneurysmsPseudoaneurysms

Natural History of Splenic Artery Pseudoaneurysm ?
Day of Injury

Natural History of Splenic Artery Pseudoaneurysm ?
Post Injury Day 4

Splenic Artery Embolization, cont’dSplenic Artery Embolization, cont’d
Does embolization impair or preserve splenic function ??
Does embolization increase splenic salvage ??
Does angiography/embolization improve overall outcome ??