current outcomes of prematurity. implications for optimal care of preterm neonates howard w....
TRANSCRIPT

Current Outcomes of Prematurity.Implications for optimal care of
preterm neonates
Howard W. Kilbride, MD
Division Director, Neonatology
Vice Chair of Perinatal Services, Department of Pediatrics
Professor of Pediatrics, University of Missouri-Kansas City School of Medicine

Objectives
• Overview of epidemiology of preterm deliveries
• Brief review of complications of preterm birth• Describe neurodevelopmental outcomes,
including unique issues for extremely preterm • Review factors related to
neurodevelopmental impairment• Discuss implications for neonatal care
You are counseling parents expecting a preterm delivery. What is the lowest gestational age at which you would
recommend comfort care?
A. <22 weeks
B. 22 wks
C. 23 wks
D. 24 wks
E. 25 wks
F. 26 wks
<22 weeks
22 wks
23 wks
24 wks
25 wks
26 wks
0% 0% 0%0%0%0%

Your answer to Question #1 is based on:
A. Likely high mortalityB. Risk for severe
neurodevelopmental impairment
C. Low likelihood of normal neurodevelopmental outcome
D. Other
Likely high
morta
lity
Risk fo
r severe neuro
dev...
Low lik
elihood of n
orma...
Other
0% 0%0%0%
Among ELBW survivors, cognitive outcomes are influenced equally by
gestational age and socioeconomic status.
A. True
B. False
True
False
0%0%
I am familiar with the online Premie Outcome Predictor.
A. Yes, but don’t use it
B. Yes, and I use it to assist parent counseling
C. Never heard of it
Yes, but d
on’t use
it
Yes, and I u
se it
to assi
st ...
Never heard
of it
0% 0%0%

Percentage of Preterm Births, US, 1990-2008Ref: Norwitz et al Rev Ob Gyn, 2011

Epidemiology of Preterm Births
< 32 wks
32 wks
33 wks
34 wks
35 wks
36 wks
37.1%
16%
5.1%
7777.7%
13%
21.2%
Davidoff, et al, Semin Perinatol 2006

National Center for Health Statistics, 2006-2013Prepared by March of Dimes Perinatal Data Center, 2015

Neurodevelopmental Consequences of Preterm Birth
• Cerebral Palsy
• Cognitive disabilities
• Sensorineural impairments: hearing/vision
• Epilepsy
• Behavioral/emotional concerns
• Executive functioning

Cerebral Palsy
• CP worldwide 2.11/1000 live births
BW 1000-1499 g 59.8/1000
> 2500 g 1.37/1000
GA < 28 wk 111.8/1000
> 36 wk 1.35/1000
Preterm birth accounts for 42-47% of Cerebral Palsy
REF: Chang, BMJ, 2015

Effect of Preterm Birthon Cognition
Bhutta AT, et al. JAMA. 2002;288:728-737

RISK FACTORS FOR SPECIAL EDUCATION
Odds Ratio
Male Gender 1.95
Parent Education <12 yr 1.63
BW <2500 g 1.48
Infants <2500 g represented 13% of non-orthopedically handicapped special education population
Ref: Andrews, et al. Am J Prev Med 1995;11:55
Impact of preterm births on prevalence of neurocognitive impairments
• 27% of cognitive delay
• 23% of hearing loss
• 37% of visual impairments
Estimated Cost: ~ 17 billion dollars annually (Institute of Medicine 2007)
Ref: Change, BMJ 2015
Behavioral Effects of Prematurity
• Infants: less adaptable, less persistent, more withdrawn.
• Increased risk of ADHD• Emotional/Anxiety Disorders
– Variable reports• Conduct Problems
– Related to neurologic risk– Additional environmental effects
• Lower Level of Social Competence

Effect of Preterm Birth on Occurrence of ADHD
Bhutta AT, et al. JAMA. 2002; 288:728-737

Late Preterms: Need for Intensive Care
• 17,000 NICU admissions annually > 33 wk GA
• Intensive care by GA34 weeks 50%35 weeks 15%36 weeks 8%
• Paradox– late preterm excluded from RCT of preterm
therapies (eg, surfactant, antenatal steroids)– included in term RCTs (HFOV, NO)
Ref: Angus et al. AmJRCCM, 2001

Late Preterm Issues• Acute clinical problems
- increased respiratory morbidity
- nutrition/feeding
- glucose stability
- thermal stability
- hyperbilirubinemia• Follow-up concerns
- apnea/SIDS
- ED visits/rehospitalizations
- neurodevelopmental outcome

Late PretermPotential for Neurodevelopmental Injury
• Brain weight at 34 weeks is 65% of term• Approximately 50% of fetal cortical volume
increase occurs 34 to 40 weeks• Cerebellar volume increases 25% in last 6
weeks• Developing brain tissue susceptible to
hypoxic-ischemic injury (less antioxidants) Adams-Chapman, Clin Perinatol 2006
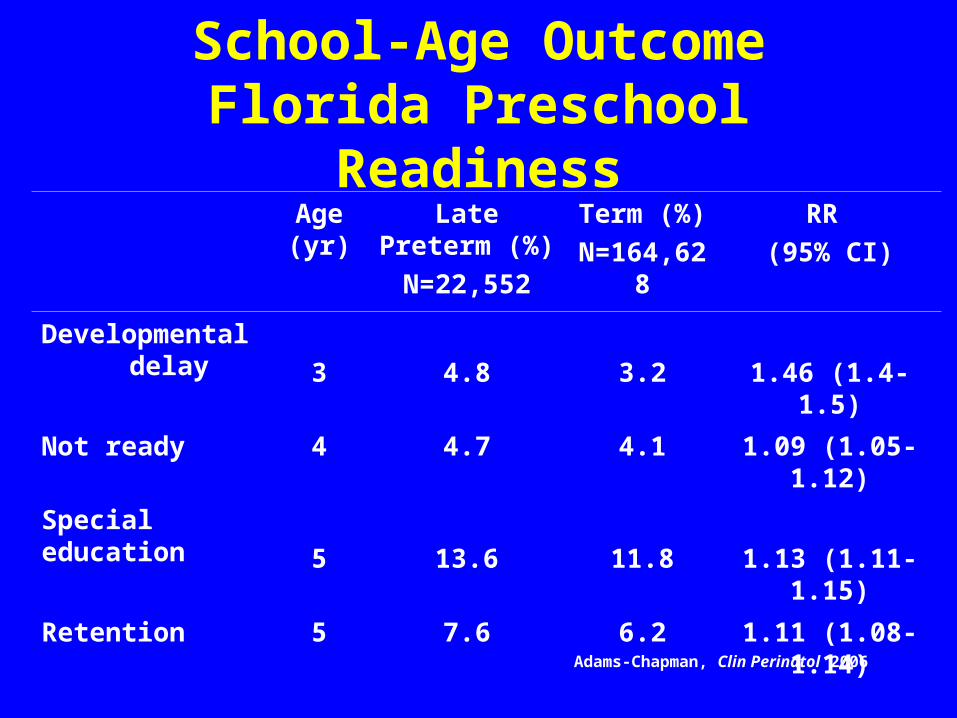
School-Age OutcomeFlorida Preschool Readiness
Age (yr)
Late Preterm (%)
N=22,552
Term (%)
N=164,628
RR
(95% CI)
Developmental delay 3 4.8 3.2 1.46 (1.4-1.5)
Not ready 4 4.7 4.1 1.09 (1.05-1.12)
Special education
5 13.6 11.8 1.13 (1.11-1.15)
Retention 5 7.6 6.2 1.11 (1.08-1.14)
Adams-Chapman, Clin Perinatol 2006
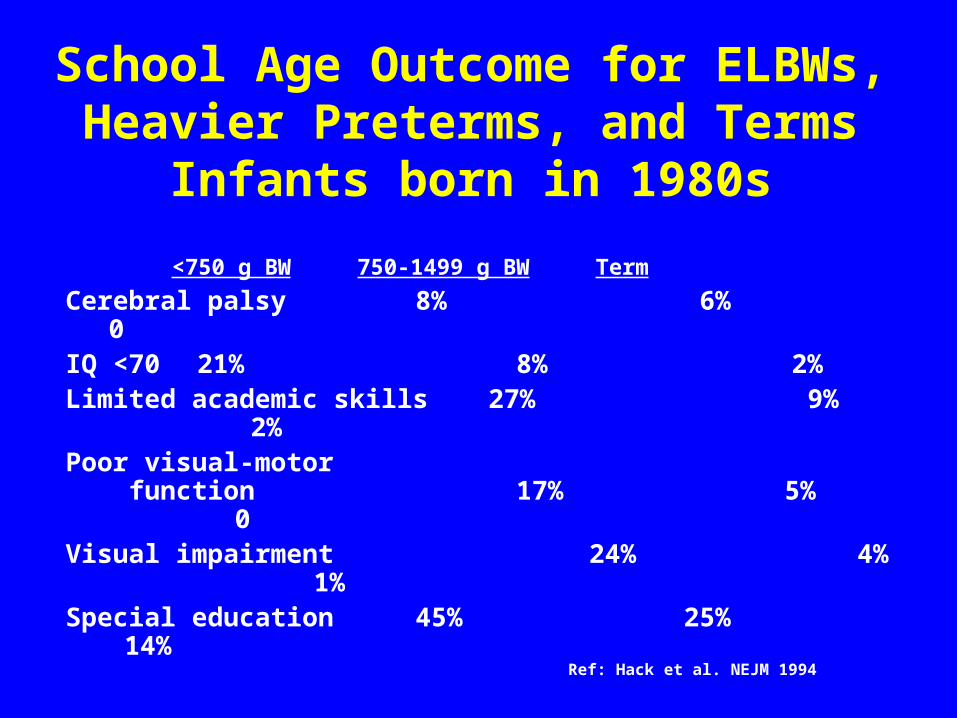
School Age Outcome for ELBWs, Heavier Preterms, and Terms
Infants born in 1980s
<750 g BW 750-1499 g BW Term
Cerebral palsy 8% 6% 0IQ <70 21% 8% 2%Limited academic skills 27% 9% 2%Poor visual-motor function 17% 5% 0Visual impairment 24% 4% 1%Special education 45% 25% 14%
Ref: Hack et al. NEJM 1994

Adverse Neuro Outcomes by GA Ref: Petrini et al, J Pediat 2009

EPIPAGE-2France population based 2011
22-34 wks GA23-26 wks 27-31 wks 32-34 wks
Severe IVH 12.9 % 3.7% 0.6%
Cystic PVL 2.4% 1.5% 0.5%
BPD 25.6 % 4.6 % 0
ROP 6.0% 0.3% 0
NEC 5.1% 3.5% 0.9%
Ref: Ancel et al, JAMA Ped 2015, 169, 230
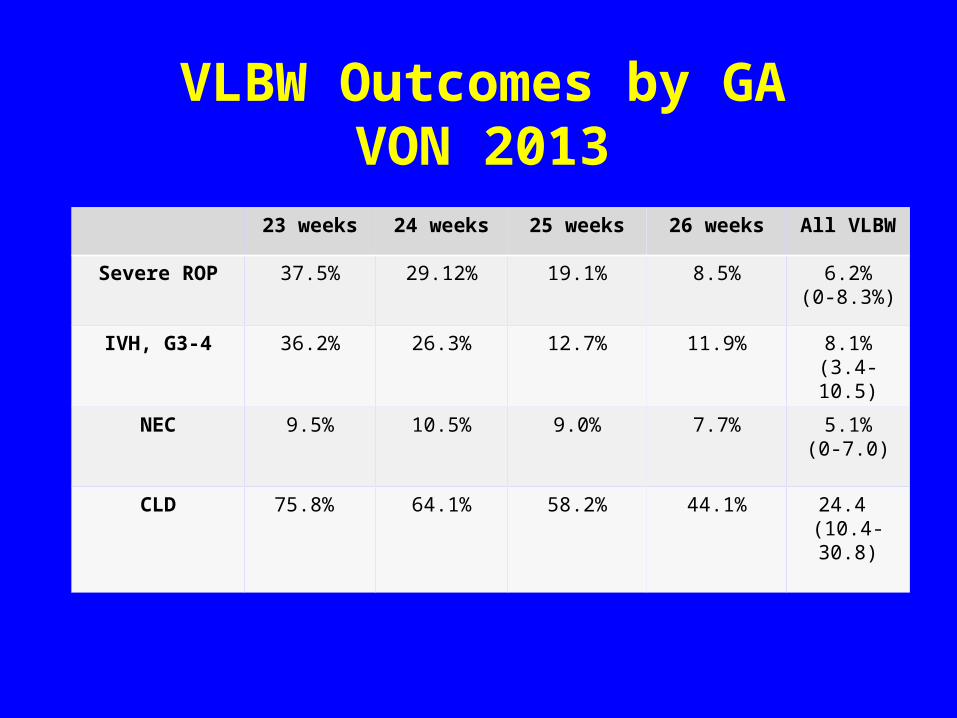
VLBW Outcomes by GAVON 2013
23 weeks 24 weeks 25 weeks 26 weeks All VLBW
Severe ROP 37.5% 29.12% 19.1% 8.5% 6.2%(0-8.3%)
IVH, G3-4 36.2% 26.3% 12.7% 11.9% 8.1%(3.4-10.5)
NEC 9.5% 10.5% 9.0% 7.7% 5.1%(0-7.0)
CLD 75.8% 64.1% 58.2% 44.1% 24.4 (10.4-30.8)

Vermont Oxford Network 2013Mortality-All VLBW Infants
by GA Week
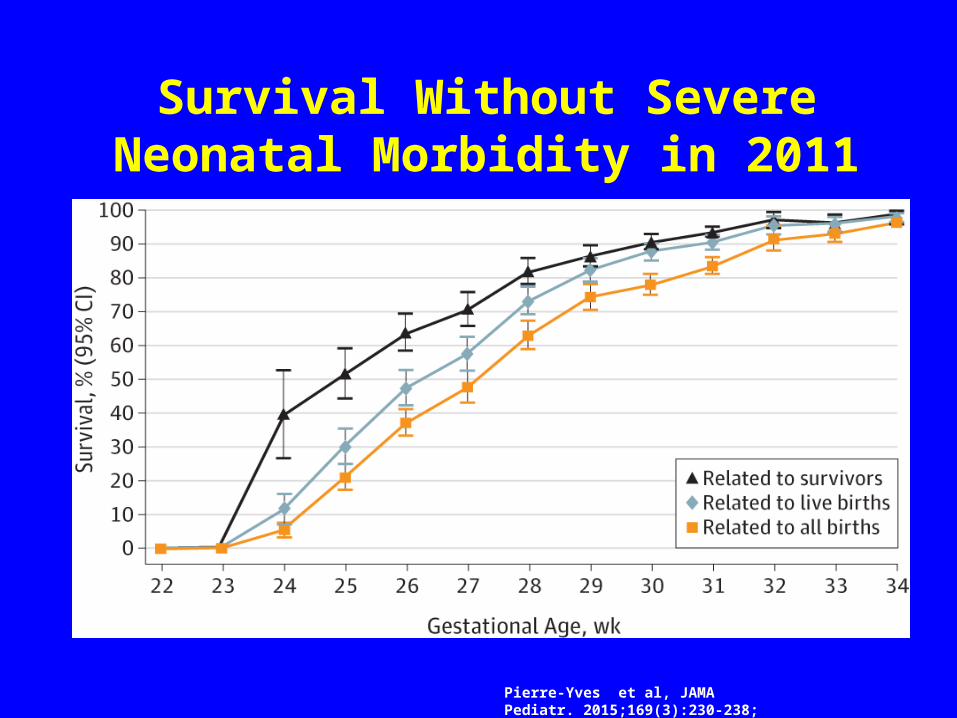
Survival Without Severe Neonatal Morbidity in 2011
Pierre-Yves et al, JAMA Pediatr. 2015;169(3):230-238;
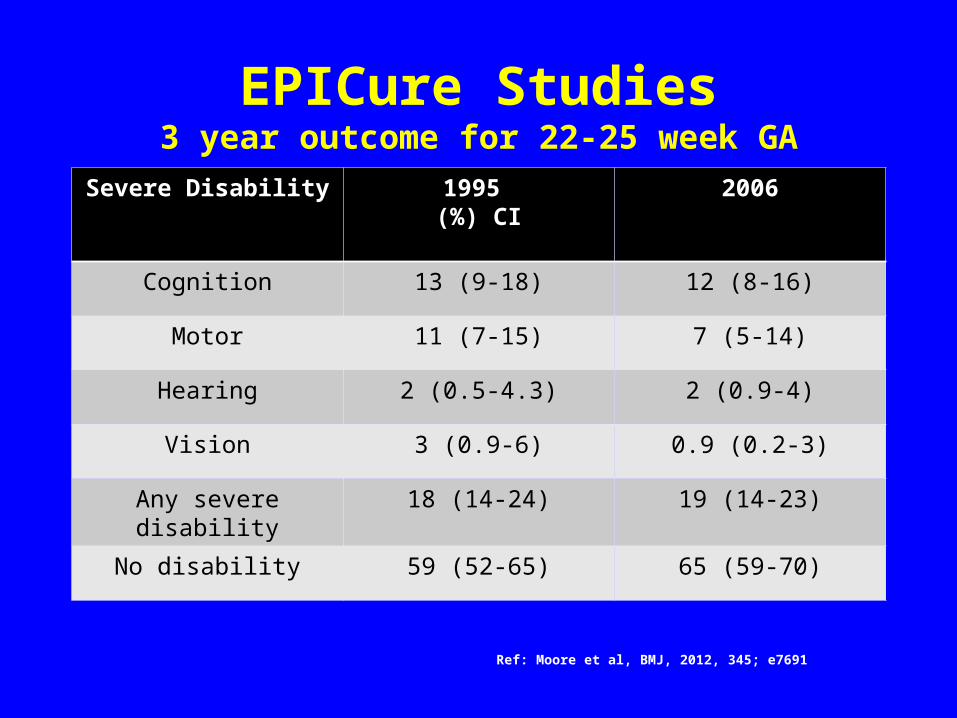
EPICure Studies3 year outcome for 22-25 week GA
Severe Disability 1995 (%) CI
2006
Cognition 13 (9-18) 12 (8-16)
Motor 11 (7-15) 7 (5-14)
Hearing 2 (0.5-4.3) 2 (0.9-4)
Vision 3 (0.9-6) 0.9 (0.2-3)
Any severe disability 18 (14-24) 19 (14-23)
No disability 59 (52-65) 65 (59-70)
Ref: Moore et al, BMJ, 2012, 345; e7691

Learning challenges in ELBWs even with normal cognitive scores
Factors associated with increased risk of neurodevelopmental impairments
• Inflammatory exposure: chorioamnionitis, sepsis, NEC
• In-utero/postnatal growth restriction, poor head growth
• Brain injury (IVH, PVL, encephalomalacia)• BPD• ROP• Low SES

Factors associated with improved neurodevelopmental outcomes for
preterms
• Greater gestational maturity
• Antenatal steroids
• Improved protein nutrition and growth/breast milk
• Developmental NICU care
• Neuroprotection: ? Magnesium, caffeine, Epogen

Antenatal Steroids26-34 wks GARef: Roberts, Cochrane review, 2006
Mortality 0.69 (0.58-0.8)
Moderate/Severe RDS 0.55 (0.43-0.71)
IVH 0.54 (0.43-0.69)
NEC 0.46 (0.29-0.74)
Systemic infection 0.56-(0.38-0.85)
Retrospective Review: also beneficial 23-25 weeksCarlo et al, JAMA, 2001
Developmental Care
• Individualized neurobehavioral assessments
• Individualized program to promote stability and self-regulation– positioning– minimize interruptions– lighting changes– noise avoidance– hammock, bunting– parental involvement

Journal of Perinatology, 2012

Evidenced Based Approach to Improving Outcomes of Preterms
• Delay Preterm Birth – Progesterone supplement
• Hx PTL: RR 0.66 (0.54-0.81) Meis et al, NEJM, 2007• Cervical shortening: RR 0.56 (0.36-0.88) Fouseca et al, NEJM
2007
• Antenatal Steroids
• Nutrition (protein, early enteral fdg with breast milk)
• Conservative ventilation, judicious oxygen use
• Developmental NICU Care

Support Trial: Comparing 02 Saturation Targets
Lower O2(85-89%)
Higher O2(91-95%)
P value
Death Before 18-22 months
22.1 % 18.2 % 0.046
NDI 9.5% 10.5 % 0.49
Death or NDI 30.2 % 27.5 % 0.21
Bilateral blindness
1.0 % 1.2% 0.86
ROP (original study)
8.6% 17.9% <0.001
Ref: Vaucher, NEJM 2012

NICHD Preemie Outcome predictor
http://www.nichd.nih.gov/about/org/cdbpm/pp/prog_epbo/epbo_case.cfm
Gestational Age (Best Obstetric Estimate in Completed Weeks):
Birth Weight (401 Grams to 1,000 Grams): gramsSex: Female MaleSingleton Birth: Yes NoAntenatal Corticosteroids (Within Seven Days Before
Delivery): Yes No
http://www2.aap.org/sections/perinatal/

Letter to Ed. NEJM 2004;351:836-837
"A girl with a birth weight of 280 g, now 14 years old"

Perception of Quality of Life
0
0.2
0.4
0.6
0.8
1
Jaime Chris Pat Sandy
MD/RN
Parents
Utility
Score
Hypothetical Outcomes; mean utility scores 95% CIRef: Saigal, et al. JAMA 1999

Parental Rating of Quality of Life for ELBWs
Ref: Saigal et al, Pediatr 2000

You are counseling parents expecting a preterm delivery. What is the lowest gestational age at which you would
recommend comfort care?
A. <22 weeks
B. 22 wks
C. 23 wks
D. 24 wks
E. 25 wks
F. 26 wks
<22 weeks
22 wks
23 wks
24 wks
25 wks
26 wks
0% 0% 0%0%0%0%
