cutaneous mast cell counts–what constitutes a ‘normal’ number?
TRANSCRIPT
J Cutan Pathol 2010: 37: 919–921 Copyright © 2009 John Wiley & Sons A/S
John Wiley & Sons. Printed in Singapore
Letter to the Editor
Cutaneous mast cell counts–Whatconstitutes a ‘normal’ number?To the Editor,
Mastocytosis is a condition involving an exces-sive mast cell burden on the body. The WorldHealth Organization (WHO) classification schemerecognizes three major categories: (a) cutaneous mas-tocytosis (CM), (b) systemic mastocytosis (SM) and(c) localized extracutaneous mast cell neoplasms.1
Cutaneous mastocytosis usually occurs in children,typically as pruritic macules and papules, with mastcells restricted to the skin. In SM, mast cells infiltratethe skin as well as other organs such as the liver, gas-trointestinal tract (GI) tract, bone marrow and spleen.
Despite the frequency with which cutaneous biop-sies are performed in diagnosing mastocytosis, thehistological criteria for confirmation remain poorlydefined.2,3 Without a reference range for mast cellnumbers in normal skin, demonstrating an ‘increased’count of these cells is impossible. Attempts toascertain this reference range in human skin havebeen previously undertaken.4– 10 However, with theemployment of various methodologies and anatomicsites of biopsy, the resulting data have been widelyvaried.3 For example, while most dermatopatholo-gists determine mast cell prevalence by counting thenumber of cells appreciated in a single high powerfield (MC/hpf), many previous studies reported theirfindings in counts per mm2 (MC/mm2).
Additionally, methods for identifying mast cellshave evolved over time. Previously, mast cell gran-ules have been stained using toluidine blue, Giemsa,chloroacetate esterase and alcian blue reagents.11
Immunoperoxidase staining for tryptase, microph-thalmia transcription factor and CD 117 can nowbe used to elucidate these cells more specifically.Antibodies to tryptase appear particularly useful inidentifying mast cells, as tryptase is expressed in allphases of mast cell development.12,13
We sought to perform a preliminary studycomparing the efficacy of toluidine blue and tryptasestains for detecting mast cells in otherwise normalskin as well as determining an ‘average’ number
of cells to better define an expected baselinecount when evaluating tissue for increased mastcell burden. The study material consisted of tissueobtained from 19 truncal excisions in otherwisehealthy adults undergoing surgery for the removalof a previously biopsied neoplasm. Patients with ahistory of conditions involving mast cell activationand/or proliferation (i.e. urticaria, mastocytosis, drugreactions, etc.) were excluded. Tissues demonstratingfibroplasia, repair reaction, inflammation, mucin andresidual tumor were disqualified from consideration.Tissue sections were stained for toluidine blue instandard fashion. Tryptase staining was performedusing monoclonal mouse antihuman antibody cloneAA1 (DakoCytomation, Carpinteria, California)diluted at 1:200 without tissue pretreatment. Anindirect biotin streptavidin system (iVIEW DAB,Ventana Medical Systems, Tucson, Arizona) usingan automated immunohistochemistry stainer wasemployed to detect antibody deposition. Five highpower fields [400×] each in the papillary and reticulardermis were selected, and the number of visible mastcells were manually counted for each stain. Fieldscontaining adnexal epithelium and/or nerve tissuewere excluded from analysis.
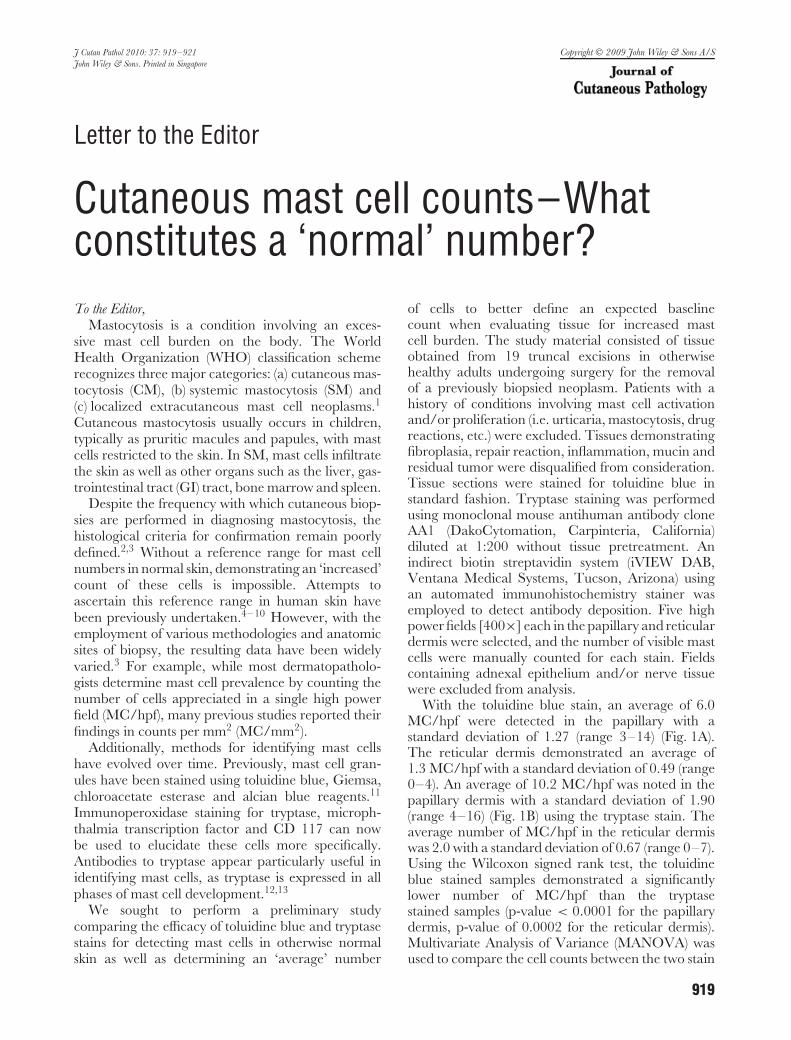
With the toluidine blue stain, an average of 6.0MC/hpf were detected in the papillary with astandard deviation of 1.27 (range 3–14) (Fig. 1A).The reticular dermis demonstrated an average of1.3 MC/hpf with a standard deviation of 0.49 (range0–4). An average of 10.2 MC/hpf was noted in thepapillary dermis with a standard deviation of 1.90(range 4–16) (Fig. 1B) using the tryptase stain. Theaverage number of MC/hpf in the reticular dermiswas 2.0 with a standard deviation of 0.67 (range 0–7).Using the Wilcoxon signed rank test, the toluidineblue stained samples demonstrated a significantlylower number of MC/hpf than the tryptasestained samples (p-value < 0.0001 for the papillarydermis, p-value of 0.0002 for the reticular dermis).Multivariate Analysis of Variance (MANOVA) wasused to compare the cell counts between the two stain
919

Letter to the Editor
(A)
(B)
Fig. 1. Representative histologic features of the tissue staining. Notethe enhanced number of visible mast cells in tissue sections stainedwith tryptase (A) compared to toluidine blue (B). (A–tryptase X 200,B–toluidine blue X 200).
types for the papillary and reticular dermis together.The p-value of Hotelling’s t-square test was < 0.0001.
Our study confirms the findings of previous authorsthat mast cell identification is significantly enhancedusing a tryptase stain vs. a toluidine blue stain.12,13
It is more sensitive and specific than toluidine blue,and in our experience is easier to visually identify.Tryptase is an endopeptidase present as α-tryptase,β-tryptase and δ-tryptase isoforms within mast cellgranules while the γ-tryptase isoform is membranebound. Variability in proportion of these isoformsexists based on mast cell location.11
A second aspect of our investigation involvedestablishing an expected average number of mastcells in normal truncal skin. We found an averageof 10.2 MC/hpf in the papillary dermis usingtryptase immunohistochemical staining. Rosen et al.7
reported similar results of 8.2 MC/hpf in the papillarydermis of truncal skin using Giemsa and Leder stains,but other studies have garnered different resultsusing MC/mm2. Janssens and co-workers5 utilized
a tryptase stain and found 79 MC/mm2 in truncaltissue, akin to the 77 MC/mm2 found in breast tissueby Kiszewski et al.3, with Giemsa staining. Otherinvestigators have detected 38 MC/mm2 in forearmskin and 47 MC/mm2 in arm skin using toluidineblue and methyelene blue stains respectively.7,9
It is important to consider mast cell distributionwhen interpreting these data. Greater numbers ofmast cells reportedly exist in distal extremity skin com-pared with the trunk and proximal extremities.5,14
However, as cutaneous lesions of mastocytosis typi-cally appear on the trunk and proximal extremities2,reference values for these areas may be useful fordiagnosing this condition.
Our study suffers from a lack of heterogeneitywith regard to the patient population evaluated. Allof the specimens investigated were from Caucasianpatients with an average age of 53 years and 14(74%) were male. Minimal research exists exploringthe possibility that mast cell counts in ‘normal skin’vary based on age, sex, ethnic origin and cumulativeultraviolet (UV) light exposure. Additionally, someof them conflicting leaving the question largelyunanswered. It has been suggested that there is anincrease in mast cells with age, perhaps secondaryto increased UV exposure.15,16 Other investigators,however, have found no effect of sun exposure17
or age14 on cutaneous mast cell numbers. Clearly,additional research is warranted before baseline mastcell counts can be delineated.
In conclusion, our results provide further supportfor the position that tryptase staining is superior tothat of toluidine blue for demonstrating mast cells inthe skin. Moreover, using a tryptase stain, an averageof 10–12 mast cells per high power field (400×) canbe expected in the papillary dermis in biopsies fromotherwise normal truncal skin from Caucasian adults.A comparison of mast cell counts using tryptase,microphthalmia transcription factor and CD 117immunohistochemical staining is being undertaken.
Megan O’Neill1
Lacey M. Thomas1
Alan S. Boyd1,2
1Department of Medicine (Dermatology), VanderbiltUniversity, Nashville, Tennessee and
2Department of Pathology, Vanderbilt University,Nashville, Tennessee
e-mail: [email protected]
References1. Horny HP, Sotlar K, Valent P. Mastocystosis: state of the art.
Pathobiology 2007; 74: 121.
920

Letter to the Editor
2. Wolff K, Komar M, Petzelbauer P. Clinical and histopatholog-ical aspects of cutaneous mastocytosis. Leuk Res 2001; 25:519.
3. Kiszewski A, Alvarez-Mendoza A, Rios-Barrera VA, et al. Mas-tocytosis in children: clinicopathological study based on 35 cases.Histopathology 2007; 22: 535.
4. Rosen LB, Frank B. Mast cells in sun-exposed and non-sun-exposed skin: an autopsy study. Am J Dermatopathol 1987; 9:208.
5. Janssens AS, Heide R, den Hollander JC, et al. Mast celldistribution in normal adult skin. J Clin Pathol 2005; 58:285.
6. Wilkinson B, Jones A, Kossard S. Mast cell quantitation byimage analysis in adult mastocytosis and inflammatory skindisorders. J Cutan Pathol 1992; 19: 366.
7. Eady RAJ, Cowen T, Marshall TF, et al. Mast cell populationdensity, blood vessel density and histamine content in normalhuman skin. Br J Dermatol 1979; 100: 623.
8. Kasper C, Freeman R, Tharp M. Diagnosis of mastocytosissubsets using a morphometric point counting technique. ArchDermatol 1987; 123: 1017.
9. Garriga MM, Friedman MM, Metcalfe DD. A survey of thenumber and distribution of mast cells in the skin of patients withmast cell disorders. J Allergy Clin Immunol 1988; 82: 425.
10. Sweet W, Smoller B. Perivascular mast cells in urticariapigmentosa. J Cutan Pathol 1996; 23: 247.
11. Metcalfe D. Mast cells and mastocytosis. Blood 2008; 112: 946.12. Walls AF, Jones DB, Williams JH, Church MK, Holgate ST.
Immunohistochemical identification of mast cells informaldehyde-fixed tissue using monoclonal antibodies specificfor tryptase. J Pathol 1990; 162: 326.
13. Horny HP, Sillaber C, Menke D, et al. Diagnostic value ofimmunostaining for tryptase in patients with mastocytosis. AmJ Surg Pathol 1998; 22: 1132.
14. Weber A, Knop AW, Maurer M. Pattern analysis of humancutaneous mast cell populations by total body surface mapping.Br J Dermatol 2003; 148: 224.
15. Grimbaldeston MA, Simpson A, Finlay-Jones JJ, Hart PH. Theeffect of ultraviolet radiation exposure on the prevalence of mastcells in human skin. Br J Dermatol 2003; 148: 300.
16. Grimbaldeston MA, Skov L, Finlay-Jones JJ, Hart PH.Increased dermal mast cell prevalence and susceptibility todevelopment of basal cell carcinoma in humans. Methods 2002;28: 90.
17. Valent P, Akin C, Escribano L, et al. Standards and standard-ization in mastocytosis: Consensus statements on diagnostics,treatment recommendations and response criteria. Eur J ClinInvest 2007; 37: 435.
921