cy 2016 medicare outpatient hospital final rule
TRANSCRIPT

CY 2016 MEDICARE OUTPATIENT HOSPITAL FINAL RULE
CRHF ECONOMICS & HEALTH POLICY DECEMBER 1, 2015

DISCLAIMER This presentation is intended only for educational use. Any duplication is prohibited without
written consent of the authors. This information does not replace seeking coding advice from the payer and/or your coding staff. The ultimate responsibility for correct coding lies with the provider of services. Please contact your local payer for their interpretation of the appropriate codes to use for specific procedures.
Medtronic makes no guarantee that the use of this information will prevent differences of opinion or disputes with Medicare or other third party payers as to the correct form of billing or the amount that will be paid to providers of service.
CPT copyright 2015 American Medical Association. All rights reserved. CPT is a registered trademark of the American Medical Association. Applicable FARS/DFARS Restrictions Apply to Government Use. Fee schedules, relative value units, conversion factors and/or related components are not assigned by the AMA, are not part of CPT, and the AMA is not recommending their use. The AMA does not directly or indirectly practice medicine or dispense medical services. The AMA assumes no liability for the data contained or not contained herein.
Note: CPT® code descriptions may be abbreviated and not listed in their entirety in all cases in this presentation. For full descriptions, please refer to your 2016 CPT code book.
CRHF ECONOMICS & HEALTH POLICY 2
CONTINUING EDUCATION UNITS
CRHF ECONOMICS & HEALTH POLICY 3
This program has prior approval of the American Academy of Professional Coders (AAPC) for one continuing education hour. Granting of this prior approval in no way constitutes endorsement by AAPC of the program content or the program sponsor.
The AAPC requires attendees to participate in the entire Web-EX presentation in order to qualify for the CEU certificate.
This program has prior approval of the American Health Information Management Association (AHIMA) for one continuing education unit. Granting of this prior approval in no way constitutes endorsement by AHIMA of the program content or the program sponsor.
Registered attendees that qualify will receive an email that includes the CEU certificate within a couple of weeks.

4 CRHF ECONOMICS & HEALTH POLICY
ABBREVIATION GLOSSARY
PVI: Pulmonary Vein Isolation
VT: Ventricular Tachycardia
SVT: Supraventricular Tachycardia
AV: Atrioventricular
SC: Singe Chamber
DC: Dual Chamber
PM: Pacemaker
ICD: Implantable Cardioverter Defibrillator
EP: Electrophysiologic
Gen: Generator
PBDs: Provider-Based Departments
NPI: National Provider Identifier
Sources: 2016 CPT code book; CY 2016 Hospital OPPS final rule; CY 2016 MPFS final rule

5 CRHF ECONOMICS & HEALTH POLICY
AGENDA
Coding and APC/C-APC Assignment
Other CY 2016 OPPS Updates
Medicare Coverage Policies
Provider-Based Designation
Device Monitoring
Appendix
Q&A

6 CRHF ECONOMICS & HEALTH POLICY
Coding and APC/C-APC Assignment
CMS renumbering of APCs resulted in new APC numbers
for all of the CRHF related procedure/services

7 CRHF ECONOMICS & HEALTH POLICY
Category III Code2
Description2
0387T Transcatheter insertion or replacement of permanent leadless pacemaker, ventricular
(CMS assigned to C-APC 5193: $14,612)3
0388T Transcatheter removal of permanent leadless pacemaker, ventricular (CMS assigned to C-APC 5182: $2,247)3
0389T Programming device evaluation (in person) with iterative adjustment of the implantable device to test the function of the device and select optimal permanent programmed values with analysis, review and report, leadless pacemaker system
(CMS assigned to APC 5141: $33.62)3
0390T Peri-procedural device evaluation (in person) and programming of device system parameters before or after a surgery, procedure or test with analysis, review and report, leadless pacemaker system
0391T Interrogation device evaluation (in person) with analysis, review and report, includes connection, recording and disconnection per patient encounter, leadless pacemaker system
(CMS assigned to APC 5141: $33.62)3
1 AMA 2016 CPT code book; 2 HCPCS: Healthcare Common Procedure Coding System; 3 Medicare CY 2016 OPPS final rule, Addendum B
CPT®1 / HCPCS2 CODES FOR CY 2016

8 CRHF ECONOMICS & HEALTH POLICY
APC / C-APC ASSIGNMENT FOR CRHF RELATED PROCEDURE/SERVICES FOR CY 2016
CPT Code Brief CPT Code Description
CY 2016 APC/
C-APC Assignment/ National Payment1
CY 2015 APC/ C-APC Assignment/ National Payment1
Electrophysiologic Procedures
93603, 93615, 93616, 93618, 93642
Right ventricular recording Esophageal recording Esophageal recording w/pacing Induction of arrhythmia EP evaluation, not at implant
5211 $845
0084 $873
93600, 93602, 93610, 93612, 93619-20, 93624, 93650
Bundle of His recording Intra-atrial recording Intra-atrial pacing Intraventricular pacing Comprehensive EP evaluations EP follow up study AV node ablation
5212 $4,698
0085 $4,635
93653, 93654, 93656
Catheter ablation of SVT Catheter ablation of VT Catheter ablation by PVI
5213 $15,561
0086 $14,362
1 https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/HospitalOutpatientPPS/index.html

9 CRHF ECONOMICS & HEALTH POLICY
APC / C-APC ASSIGNMENT FOR CRHF RELATED PROCEDURE/SERVICES FOR CY 2016
CPT Code Brief CPT Code Description
CY 2016 APC/
C-APC Assignment National Payment1
CY 2015 APC/ C-APC Assignment National Payment1
Pacemaker and Similar Procedures
33218, 33220, 33233, 33234, 33235, 33241, 33244
Repair single transvenous lead Repair 2 transvenous leads Remove pacemaker generator Remove PM lead from SC system Remove PM lead from DC system Remove ICD generator Remove ICD lead(s) transvenously
5221 $2,490
0105 $2,347 0105 $2,347 0090 $6,545 0105 $2,347 0105 $2,347 0105 $2,347 0105 $2,347
33210 33211 33212 33216 33217 33227 33282
Insert temporary SC electrode Insert temporary DC electrodes Insert PM generator only, attach to lead Insert single transvenous lead Insert 2 transvenous leads Remove PM generator with replacement of PM gen. single lead system Insert cardiac event recorder
5222 $6,697
0090 $6,545
1 https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/HospitalOutpatientPPS/index.html

10 CRHF ECONOMICS & HEALTH POLICY
APC / C-APC ASSIGNMENT FOR CRHF RELATED PROCEDURE/SERVICES FOR CY 2016
CPT Code Brief CPT Code Description
CY 2016 APC/
C-APC Assignment National Payment1
CY 2015 APC/ C-APC Assignment National Payment1
Pacemaker and Similar Procedures continued
33206, 33207, 33208, 33213, 33214, 33224, 33228
Insert SC PM generator & lead in atria Insert SC PM generator & lead in ventricle Insert DC PM generator & 2 leads Insert PM generator only, attach to leads Upgrade SC PM to DC pacemaker Insert LV lead & attach to existing gen. Remove PM generator with replacement of PM gen. dual lead system
5223 $9,273
0089 $9,493
33221, 33229
Insert PM generator only, attach to leads Remove PM generator with replacement of PM gen, multiple lead system
5224 $16,914
0655 $16,407
1 https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/HospitalOutpatientPPS/index.html

11 CRHF ECONOMICS & HEALTH POLICY
APC / C-APC ASSIGNMENT FOR CRHF RELATED PROCEDURE/SERVICES FOR CY 2016
CPT Code Brief CPT Code Description
CY 2016 APC/
C-APC Assignment National Payment1
CY 2015 APC/ C-APC Assignment National Payment1
ICD and Similar Procedures
33230, 33240, 33262, 33263
Insert ICD generator only, attach to leads Insert ICD generator only, attach to lead Remove ICD generator with replacement of ICD generator, single lead system Remove ICD generator with replacement of ICD generator, dual lead system
5231 $21,930
0107 $22,107
33231, 33249, 33264, 33270
Insert ICD generator only, attach to leads Insert ICD system with transvenous lead(s), SC or DC Remove ICD generator with replacement of ICD generator, multiple lead system Insert subcutaneous implantable defibrillator system with subcutanous lead
5232 $30,940
0108 $30,818
1 https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/HospitalOutpatientPPS/index.html

12 CRHF ECONOMICS & HEALTH POLICY
APC / C-APC ASSIGNMENT FOR CRHF RELATED PROCEDURE/SERVICES FOR CY 2016
CPT Code Brief CPT Code Description
CY 2016 APC/
C-APC Assignment National Payment1
CY 2015 APC/ C-APC Assignment National Payment1
Electronic Analysis of Devices
93291 ILR device interrogation evaluation (in person)
5732 $30.51
0450 $29.24
93260 93261, 93279-85, 93288-89, 93290 93293, 93296, 93299
Subcutaneous device programming evaluation (in person) Subcutaneous device interrogation (in person) PM, ICD and ILR device programming evaluation (in person) PM, ICD device interrogation (in person) Interrogation device evaluation, physiologic data elements (in person) Transtelephonic monitoring Remote monitoring PM, ICD Remote monitoring ILR, Implantable Cardiovascular Monitor (ICM)
5741 $33.62
0690 $35.15
1 https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/HospitalOutpatientPPS/index.html

13 CRHF ECONOMICS & HEALTH POLICY
CY 2016 OPPS MEDICARE PAYMENT COMPARISONS
Medicare CY 2016 OPPS final rule National Payments from Addendums
$8,230
$8,790
$9,493 $9,273
$7,500
$8,000
$8,500
$9,000
$9,500
$10,000
2013 2014 2015 2016
Single Chamber (RV) pacemaker system initial insertion
Single Chamber (RV)pacemaker systeminitial insertion
$10,187
$10,588
$9,493 $9,273
$8,500
$9,000
$9,500
$10,000
$10,500
$11,000
2013 2014 2015 2016
Dual Chamber pacemaker system initial insertion
Dual Chamberpacemaker systeminitial insertion

14 CRHF ECONOMICS & HEALTH POLICY
$15,280
$15,882
$16,407
$16,914
$14,000
$14,500
$15,000
$15,500
$16,000
$16,500
$17,000
$17,500
2013 2014 2015 2016
CRT-P initial insertion
CRT-P initial insertion
$30,680
$32,145
$30,818
$30,490
$29,500
$30,000
$30,500
$31,000
$31,500
$32,000
$32,500
2013 2014 2015 2016
CRT-D and ICD initial insertion
CRT-D and ICD initialinsertion
Medicare CY 2016 OPPS final rule National Payments from Addendums
CY 2016 OPPS MEDICARE PAYMENT COMPARISONS

15 CRHF ECONOMICS & HEALTH POLICY
Other CY 2016 OPPS Updates

16 CRHF ECONOMICS & HEALTH POLICY
TABLE 42 DEVICE INTENSIVE PROCEDURES APC payment adjustment for all replacement devices furnished in conjunction with a
procedure assigned to a device-intensive APC when the hospital receives a credit for the replaced device that is >50% of the replacement device cost. Only procedures that require an implantable device assigned to a “device-intensive” APC (Table 42) requires an applicable device code (HCPCS C-code).
CY 2016: Pages 70421-70424 of the Federal Register dated November 13, 2015.
CY 2016 APC CY 2016 APC Title
1565 New Technology - Level 28 ($5,000-$5,500)
1599 New Technology – Level 48 ($90,000-$100,000)
5125 Level 5 Musculoskeletal Procedures
5166 Level 6 ENT Procedures
5192 Level 2 Endovascular Procedures
5193 Level 3 Endovascular Procedures
5222 Level 2 Pacemaker and Similar Procedures (33210-33212, 33216-33217, 33227, 33271, 33282)
5223 Level 3 Pacemaker and Similar Procedures (33206-33208, 33213-33214, 33224, 33228)

17 CRHF ECONOMICS & HEALTH POLICY
TABLE 42: DEVICE INTENSIVE PROCEDURES
CY 2016 APC CY 2016 APC Title
5224 Level 4 Pacemaker and Similar Procedures (33221, 33229)
5231 Level 1 ICD and Similar Procedures (33230, 33240, 33262-33263)
5232 Level 2 ICD and Similar Procedures (33231, 33249, 33264, 33270)
5377 Level 7 Urology and Related Services
5462 Level 2 Neurostimulator and Related Procedures
5463 Level 3 Neurostimulator and Related Procedures
5464 Level 4 Neurostimulator and Related Procedures
5471 Implantation of Drug Infusion Device
5493 Level 3 Intraocular Procedures
5494 Level 4 Intraocular Procedures
CY 2016: Pages 70421-70424 of the Federal Register dated November 13, 2015.

18 CRHF ECONOMICS & HEALTH POLICY
PAYMENT REDUCTIONS FOR SPECIFIC MODIFIERS
An appropriate modifier should be reported on the hospital claim form when a
procedure is discontinued, partially reduced or cancelled. These modifiers and a brief description are:
-52: Partial reduction, cancellation, or discontinuation of services for which anesthesia is not planned -73: Procedure requiring anesthesia was terminated due to extenuating circumstances or circumstances that threatened the well being of the patient -74: Procedure requiring anesthesia was terminated after the induction of anesthesia or after the procedure was started
For claims that include an implantable device and Modifier -73, DOS on or after January 1, 2016 , and assigned to a Device Intensive APC (Table 42) , the reimbursement will be reduced by 100% of the device offset amount.
Page 70423-70425 of the Federal Register dated November 13, 2015.

19 CRHF ECONOMICS & HEALTH POLICY
CY 2016 OPPS DEVICE OFFSET TABLE FOR CRHF SERVICES
APC APC TITLE
CY 2016
APC RATE PERCENT
DOLLAR
AMOUNT
5211
Level 1 Electrophysiologic Procedures $845.04 1.00% $8.45
5212
Level 2 Electrophysiologic Procedures $4,697.97 32.93% $1,547.04
5213
Level 3 Electrophysiologic Procedures $15,561.11 38.60% $6,006.59
5221
Level1 Pacemaker and Similar Procedures $2,489.69 25.28% $629.39
5222
Level 2 Pacemaker and Similar Procedures $6,696.85 70.36% $4,711.90
5223
Level 3 Pacemaker and Similar Procedures $9,273.40 66.44% $6,161.25
5224
Level 4 Pacemaker and Similar Procedures $16,914.40 69.70% $11,789.34
5231 Level 1 ICD and Similar Procedures $21,930.03 77.37% $16,967.26
5232 Level 2 ICD and Similar Procedures $30,489.78 79.32% $24,184.49
https://www.cms.gov/apps/ama/license.asp?file=/Medicare/Medicare-Fee-for-Service-Payment/HospitalOutpatientPPS/Downloads/
2016-OPPS-APC-Offset-File.zip

20 CRHF ECONOMICS & HEALTH POLICY
OBSERVATION SERVICES CY 2015 Observation Services Payment Regulations: Extended Assessment and
Management (EAM) Composite APC 8009
Single payment for non-surgical encounters that include at least 8 hours of
observation (HCPCS G0378) as well as a high-level visit procedure. The
observation service cannot be provided on the same day of surgery or post
operatively.1
CY 2015 Medicare National Payment is $1,235.2
CY 2016 Observation Service Payment Regulations: A new Comprehensive Observation C-APC 8011
The claim includes at least 8 hours of observation (HCPCS G0378) as well as a visit code (99281-99285, 99291, G0379-G0384). Eligibility for the Observation service payment is based on the claim not including a procedure assigned a Status Indicator “T” or a “J1.” See Appendix for a partial list of Status Indicators.3
Surgical procedures are excluded from C-APC 8011. The hospital can expect to receive the applicable Surgical C-APC instead of Observation C-APC 8011.
CY 2016 Medicare National Payment is $2,274 and is assigned a “J2” Status Indicator.3 See Appendix for all “J2” codes/descriptions.
1 CY 2015: Page 66812 of the Federal Register dated November 10, 2014.The link is in the Appendix. 2 Medicare National Payment rates are from Addendum A for CY 2015 and CY 2016. 3 CY 2016: Pages 70333-70336 of the Federal Register dated November 13, 2015.

21 CRHF ECONOMICS & HEALTH POLICY
OBSERVATION SERVICES – HYPOTHETICAL EXAMPLE #1
Hospital submitted the claim to Medicare with the following services:
G0378 – 24 hours of Observation - Meets Criteria for OBS C-APC
99283 – ED Level 3 (SI – J2) - Meets Criteria for OBS C-APC
93005 – EKG
Various Laboratory Tests
The hospital can anticipate reimbursement based on C-APC 8011 ($2,274).
Status Indicator (SI) assignment and Medicare National Payment rates are from Addendum B.
Patient with chest pain arrives at ED
ED Physician orders tests,
receives/reviews results and orders
Cardiology consult.
Cardiologist orders Observation stay to determine if patient
needs inpatient admission.
Patient remains in OBS for 24 hours,
results are reviewed and patient is
discharged to home.

22 CRHF ECONOMICS & HEALTH POLICY
OBSERVATION SERVICES – HYPOTHETICAL EXAMPLE #2
Hospital submitted the claim to Medicare with the following services:
G0378 – More than 8 hours of Observation - Meets Criteria for OBS C-APC
99283 – ED Level 3 (SI J2) - Meets Criteria for OBS C-APC
93005 – EKG
70551 – MRI of brain
Various Laboratory Tests
33282 – ILR (Reveal/ LINQ implant) (SI – J1) – Claim with “J1” is ineligible for APC 8011.
The hospital can anticipate receiving ILR implant C-APC payment ($6,697).
Patient with syncopal event arrives at ED
ED Physician orders Lab tests , EKG and MRI of
brain, receives/reviews results and patient history, and orders
Cardiology and Neurology consults.
Neuro assessment negative. Cardiologist
orders Observation stay to further determine etiology and need for inpatient admission.
Patient remains in OBS for > 8 hrs.; Cardiologist confirms prerequisites
of coverage are met and orders ILR implant
Patient receives implant and is discharged to
home.
Status Indicator (SI) assignment and Medicare National Payment rates are from Addendum B.

23 CRHF ECONOMICS & HEALTH POLICY
THE NOTICE ACT
Related to concerns regarding to the increased use of Observation and the 2 Midnight Rule, a new Federal Law HR 876, passed by Congress and signed by the President in August 2015, requires patient disclosure of Observation cases.
The NOTICE Act, or Notice of Observation Treatment and Implication for Care Eligibility Act, would require hospitals nationwide to inform Medicare patients when they are receiving care under observation status.
The notification must be in writing with a verbal explanation of the implications of outpatient status to patient eligibility for subsequent services, such as SNF coverage.
Hospitals have 12 months to comply with the Act’s requirements.
Notice Act: http://www.gpo.gov/fdsys/pkg/BILLS-114hr876enr/pdf/BILLS-114hr876enr.pdf

24 CRHF ECONOMICS & HEALTH POLICY
TWO-MIDNIGHT RULE EXCEPTIONS
Original Implementation Date: October 1, 2013 (FY 2014)1
An inpatient admission is generally appropriate for Medicare Part A if the physician or other qualified professional admits the patient as an Inpatient based upon the expectation that the patient will need hospital care that crosses at least two midnights.
When assessing the duration of necessary care, the physician or other qualified professional may include outpatient hospital care received prior to inpatient admission.
If the patient is expected to need less than 2 midnights of care, these services should generally be billed as outpatient services.
2016 Exceptions to the Two-Midnight rule2, 3:
Case-by-Case basis by the physician responsible for the care of the Medicare beneficiary, subject to medical review.
Quality Improvement Organizations (QIOs) contractors assumed medical responsibility for the hospital stays associated with the Two-Midnight rule on October 1, 2015 and will conduct reviews for short stays, taking over that responsibility from the Medicare Administrative Contractors (MACs).
1 FY 2014: Pages 50938-50954 of the Federal Register dated August 19, 2013.The link is in the Appendix. 2 CY 2016: Page 70305 and 70602 of the Federal Register dated November 13, 2015. 3 The link for the CMS Fact Sheet dated October 30, 2015 is in the Appendix.

25 CRHF ECONOMICS & HEALTH POLICY
Medicare Coverage Policies
26 CRHF ECONOMICS & HEALTH POLICY
MEDICARE NCD FOR PACEMAKER IMPLANTS
August13,2013: Revised NCD in effect for DOS on or after 8/13/2013
NCD 20.8.3
July 7, 2014: Implementation – Claims Processing Rules ; Rescinded and Delayed
July 6, 2015: Implementation – Claims Processing rules
Change Request CR 9078; MLN Matters® MM9078
Transmittal 3384 dated October 25, 2015 – Claims Processing rules and CR 9078, MLN Matters MM9078 article revised on October 26, 2015:
Due to claims processing issues brought to the attention of CMS, MACs will implement this
NCD at the local level, until CMS is able to revise the claims processing instruction and edits.
See Appendix for links to NCD 20.8.3, Transmittal 3382 and MM9078

27 CRHF ECONOMICS & HEALTH POLICY
CARDIAC PACEMAKER EVALUATION SERVICES NCD §20.8.1 AND 20.8.1.1 OF CMS PUB. 100-03
The decision as to how often any patient's pacemaker should be monitored is the responsibility of the patient's physician who is best able to take into account the condition and circumstances of the individual patient.
Transtelephonic monitoring (TTM) Guidelines I and II are for both single and dual chamber pacemakers. The TTM guidelines are in this NCD.
Pacemaker clinic* service frequency guidelines for routine monitoring are:
Single chamber: Twice in the first 6 months following implant, then once every 12 months
Dual chamber: Twice in the first 6 months following implant, then once every 6 months
Increased frequency of monitoring must be supported by documented medical necessity.
* Please note that “Pacemaker clinic” also includes “Physician practice” and “Hospital device monitoring departments” Rev. 182, 05-22-15 is available at: http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/ncd103c1_Part1.pdf

28 CRHF ECONOMICS & HEALTH POLICY
Provider-Based Designation

29 CRHF ECONOMICS & HEALTH POLICY
PLACE OF SERVICE FOR PROVIDER-BASED PHYSICIANS A Practice designated as office-based reports POS 11 Office.
Provider-Based: Off-Campus or On-Campus claim submission1:
New POS 19: Off-Campus Outpatient Hospital A portion of an off-campus hospital provider based department that provides diagnostic, therapeutic (both surgical and nonsurgical), and rehabilitation services to sick or injured persons who do not require hospitalization or institutionalization.
POS 22 (description change only): On-Campus Outpatient Hospital A portion of a hospital’s main campus that provides diagnostic, therapeutic (both surgical and nonsurgical), and rehabilitation services to sick or injured persons who do not require hospitalization or institutionalization.
For existing Off-Campus Provider-Based practices (as of November 2, 2015), the hospital portion of the facility claim is paid separately (under OPPS) and the physician portion (professional claim) is reimbursed based on the Medicare Physician Fee Schedule (MPFS).
1 Pub 100-04 Medicare Claims Processing, Transmittal 3315 dated August 6, 2015 and effective on January 1, 2016 is available at: https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/Downloads/R3315CP.pdf Provider Based CMS Transmittal A-03-030 dated 4.18.2003: https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/downloads/a03030.pdf CMS Transmittal 143 dated 4.29.2011 https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/downloads/R143BP.pdf

30 CRHF ECONOMICS & HEALTH POLICY
THE PO MODIFIER
PO Modifier definition: Services, procedures and/or surgeries furnished at off-campus, provider-based outpatient departments.1
Reporting the PO modifier2:
Voluntary in CY 2015; mandatory January 1, 2016
Required to be reported with every code for OP hospital services provided at
an off-campus Provider-Based Department (PBD).
Not reported for services provided in:
• Remote locations of a hospital (hospital campus other than the main hospital
campus; facility or an organization that is either created by, or acquired by, a hospital that is a main provider for the purpose of furnishing Inpatient hospital services under the
name, ownership, and financial and administrative control of the main provider),
• Satellite facilities of a hospital (provides inpatient services in a building also used
by another hospital, or in one or more entire buildings located on the same campus as buildings used by another hospital, or in one or more entire buildings located on the same
campus as buildings used by another hospital),
• Emergency department
1 CY 2015: Pages 66913-66914 of the Federal Register (Vol. 79, No. 217) dated November 10, 2014. The link is included in the Addendix. 2 P0 modifier information: https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/Downloads/MM9097.pdf

31 CRHF ECONOMICS & HEALTH POLICY
PHYSICIAN OWNED PRACTICE AND PROVIDER-BASED PHYSICIAN PRACTICE EXAMPLES
CPT®
code CPT Brief Description CY 2016
Medicare National Payment
Physician owned practice and Place of Service 11 “Office”
93283 Dual lead ICD in person programming $82.401 Global
Provider-Based Physician practice and Place of Service 22 “On-Campus Outpatient Hospital – so Modifier PO is not applicable”
93283-26 Dual lead ICD in person programming $58.401 PC
93283 Dual lead ICD in person programming (Technical Component)
$33.622 TC
Hospital Outpatient APC*
Total Provider-Based Payment $92.02
PC: Professional Component TC: Technical Component Global: PC plus TC * APC: Ambulatory Payment Classification 1 Physician payment rate: http://www.cms.gov/apps/physician-fee-schedule/overview.aspx 2 Hospital payment rate: http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/HospitalOutpatientPPS/index.html
32 CRHF ECONOMICS & HEALTH POLICY
DEVICE MONITORING

33 CRHF ECONOMICS & HEALTH POLICY
OUTPATIENT HOSPITAL NATIONAL PAYMENT AMOUNTS CARDIAC DEVICE MONITORING
CPT® code Assigned Outpatient APC
January-December 2016
Medicare National Payment1
Pacemakers
93279-93281, 93288, 93293, 93296
5741 $33.62
ICDs
93282-93284, 93289, 93296 5741 $33.62
Implantable Cardiovascular Monitor (ICM)
93290, 93299 5741 $33.62
Implantable Loop Recorder (ILR)
93285, 93299 5741 $33.62
93291 5732 $30.51
1 Calendar Year 2016 Hospital APC payments are available at: http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/HospitalOutpatientPPS/index.html See Addendix for CPT code descriptions.

34 CRHF ECONOMICS & HEALTH POLICY
DEVICE MONITORING DIAGNOSIS CODES ICD-9 VERSUS ICD-10
Routine Device Monitoring
2016 ICD -10-CM and GEMs: https://www.cms.gov/Medicare/Coding/ICD10/2016-ICD-10-CM-and-GEMs.html
ICD-9-CM Diagnosis Code ICD-10-CM Diagnosis Code
Pacemaker
V45.01 Z95.0
Cardiac pacemaker in situ Presence of cardiac pacemaker
Implantable Defibrillator
V45.02 Z95.810
Automatic implantable cardiac defibrillator in situ
Presence of automatic (implantable) cardiac defibrillator
Other Cardiac Devices (ILR)
V45.09 Z95.818
Other specified cardiac device in situ
Presence of other cardiac implants and grafts

35 CRHF ECONOMICS & HEALTH POLICY
DEVICE MONITORING DIAGNOSIS CODES ICD-9 VERSUS ICD-10 Device Monitoring for Patients with a Complaint or a Symptom
ICD-9-CM Diagnosis Code ICD-10-CM Diagnosis Code
Pacemaker
V53.31 Z45.010
Fitting and adjustment of cardiac pacemaker Encounter for checking and testing of cardiac pacemaker pulse generator [battery]
Z45.018
Encounter for adjustment and management of other part of cardiac pacemaker
Implantable Defibrillator
V53.32 Z45.02
Fitting and adjustment of automatic implantable cardiac defibrillator
Encounter for adjustment and management of automatic implantable cardiac defibrillator
Implantable Loop Recorder (ILR)
V53.39 Z45.09
Fitting and adjustment of other cardiac device Encounter for adjustment and management of other cardiac device
2016 ICD -10-CM and GEMs: https://www.cms.gov/Medicare/Coding/ICD10/2016-ICD-10-CM-and-GEMs.html
36 CRHF ECONOMICS & HEALTH POLICY
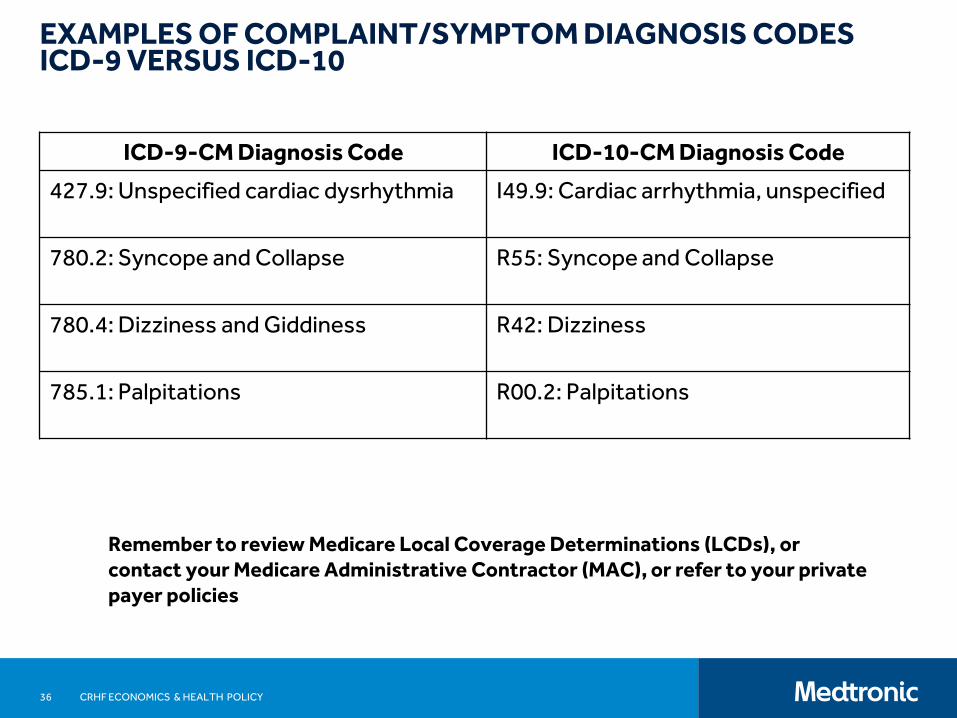
EXAMPLES OF COMPLAINT/SYMPTOM DIAGNOSIS CODES ICD-9 VERSUS ICD-10
Remember to review Medicare Local Coverage Determinations (LCDs), or contact your Medicare Administrative Contractor (MAC), or refer to your private payer policies
ICD-9-CM Diagnosis Code ICD-10-CM Diagnosis Code
427.9: Unspecified cardiac dysrhythmia
I49.9: Cardiac arrhythmia, unspecified
780.2: Syncope and Collapse
R55: Syncope and Collapse
780.4: Dizziness and Giddiness
R42: Dizziness
785.1: Palpitations
R00.2: Palpitations
37
CARDIAC RHYTHM AND HEART FAILURE (CRHF) INFORMATION CARDIAC RHYTHM AND HEART FAILURE (CRHF)
INFORMATION
To ensure you receive advance notification of webcast
events, it is very easy to register at
www.Medtronic.com/CRDMreimbursement:
Join our E-mail List Subscribe to receive news and updates.
CRHF
Economics and
Health Policy
Visit our website:
www.Medtronic.com/CRDMreimbursement
Email us:
Call our Coding Hotline:
1 (866) 877-4102
CRHF ECONOMICS & HEALTH POLICY

DOWNLOAD OUR ICD-10 DIAGNOSIS CROSSWALK
www.medtronic.com/crdmreimbursement
38 CRHF ECONOMICS & HEALTH POLICY
39 CRHF ECONOMICS & HEALTH POLICY
APPENDIX

40 CRHF ECONOMICS & HEALTH POLICY
SELECT STATUS INDICATORS: ADDENDUM D-1 Status Indicator / Item/Code/Service
OPPS Payment Status
C: Inpatient Procedures Not paid under OPPS. Admit patient. Bill as inpatient.
J1: Hospital Part B services paid through a comprehensive APC
Paid under OPPS; all covered Part B services on the claim are packaged with the primary "J1" service for the claim, except services with OPPS SI=F,G, H, L and U; ambulance services; diagnostic and screening mammography; all preventive services; and certain Part B inpatient services.
J2: Hospital Part B Services That May Be Paid Through a Comprehensive APC
Paid under OPPS; Addendum B displays APC assignments when services are separately payable.
(1) Comprehensive APC payment based on OPPS comprehensive-specific payment criteria. Payment for all covered Part B services on the claim is packaged into a single payment for specific combinations of services, except services with OPPS SI=F,G, H, L and U; ambulance services; diagnostic and screening mammography; all preventive services; and certain Part B inpatient services.
(2) Packaged APC payment if billed on the same claim as a HCPCS code assigned status indicator “J1.”
(3) In other circumstances, payment is made through a separate APC payment or packaged into payment for other services.
N: Items and Services Packaged into APC Rates
Paid under OPPS; payment is packaged into payment for other services. Therefore, there is no separate APC payment.

41 CRHF ECONOMICS & HEALTH POLICY
SELECT STATUS INDICATORS: ADDENDUM D-1
Status Indicator / Item/Code/Service
OPPS Payment Status
Q1: STV-Packaged Codes
Paid under OPPS; Addendum B displays APC assignments when services are separately payable.
(1) Packaged APC payment if billed on the same date of service as a HCPCS code assigned status indicator “S,” “T,” or “V.”
(2) In other circumstances, payment is made through a separate APC payment.
Q2: T – Packaged Codes Paid under OPPS; Addendum B displays APC assignments when services are separately payable.
(1) Packaged APC payment if billed on the same date of service as a HCPCS code assigned status indicator “T.”
(2) In other circumstances, payment is made through a separate APC payment.
Q4: Conditionally packaged laboratory tests
Paid under OPPS or CLFS.
(1) Packaged APC payment if billed on the same claim as a HCPCS code assigned published status indicator “J1,” “J2,” “S,” “T,” “V,” “Q1,” “Q2,” or “Q3.”
(2) In other circumstances, laboratory tests should have an SI=A and payment is made under the CLFS.

42 CRHF ECONOMICS & HEALTH POLICY
OBSERVATION C-APC 8011 - STATUS INDICATOR “J2”
Codes with Status Indicator “J2” from Addendum B and Descriptions from 2016 CPT code book
CPT® Code Brief Description
99281
Emergency department visit for the evaluation and management of a patient, which requires these 3 key components: A problem focused history; A problem focused examination; and Straightforward medical decision making. Usually, the presenting problem(s) are self limited or minor
99282
Emergency department visit for the evaluation and management of a patient, which requires these 3 key components: An expanded problem focused history; An expanded problem focused examination; and Medical decision making of low complexity. Usually, the presenting problem(s) are of low to moderate severity.
99283
Emergency department visit for the evaluation and management of a patient, which requires these 3 key components: An expanded problem focused history; An expanded problem focused examination; and Medical decision making of moderate complexity. Usually, the presenting problem(s) are of moderate severity.
99284
Emergency department visit for the evaluation and management of a patient, which requires these 3 key components: A detailed history; A detailed examination; and Medical decision making of moderate complexity. Usually, the presenting problem(s) are of high severity, and require urgent evaluation by the physician or other qualified health care professionals but do not pose an immediate significant threat to life or physiologic function.
99285
Emergency department visit for the evaluation and management of a patient, which requires these 3 key components within the constraints imposed by the urgency of the patient's clinical condition and/or mental status: A comprehensive history; A comprehensive examination; and Medical decision making of high complexity. Usually, the presenting problem(s) are of high severity and pose an immediate significant threat to life or physiologic function.

43 CRHF ECONOMICS & HEALTH POLICY
OBSERVATION C-APC 8011 - STATUS INDICATOR “J2”..CONTINUED
CPT® Code Brief Description
99291 Critical care, evaluation and management of the critically ill or critically injured patient; first 30-74 minutes
G0380
Level 1 hospital emergency department visit provided in a type B emergency department; (the ED must meet at least one of the following requirements: (1) it is licensed by the state in which it is located under applicable state law as an emergency room or emergency department; (2) it is held out to the public as a place that provides care for emergency medical conditions on an urgent basis without requiring a previously scheduled appointment; or (3) during the calendar year immediately preceding the calendar year in which a determination under 42 CFR 489.24 is being made, based on a representative sample of patient visits that occurred during that calendar year, it provides at least one-third of all of its outpatient visits for the treatment of emergency medical conditions on an urgent basis without requiring a previously scheduled appointment)
G0381
Level 2 hospital emergency department visit provided in a type B emergency department; (the ED must meet at least one of the following requirements: (1) it is licensed by the state in which it is located under applicable state law as an emergency room or emergency department; (2) it is held out to the public as a place that provides care for emergency medical conditions on an urgent basis without requiring a previously scheduled appointment; or (3) during the calendar year immediately preceding the calendar year in which a determination under 42 CFR 489.24 is being made, based on a representative sample of patient visits that occurred during that calendar year, it provides at least one-third of all of its outpatient visits for the treatment of emergency medical conditions on an urgent basis without requiring a previously scheduled appointment)
Codes with Status Indicator “J2” from Addendum B and Descriptions from 2016 CPT code book

44 CRHF ECONOMICS & HEALTH POLICY
CPT® Code Description
G0382
Level 3 hospital emergency department visit provided in a type B emergency department; (the ED must meet at least one of the following requirements: (1) it is licensed by the state in which it is located under applicable state law as an emergency room or emergency department; (2) it is held out to the public or other means) as a place that provides care for emergency medical conditions on an urgent basis without requiring a previously scheduled appointment; or (3) during the calendar year immediately preceding the calendar year in which a determination under 42 CFR 489.24 is being made, based on a representative sample of patient visits that occurred during that calendar year, it provides at least one-third of all of its outpatient visits for the treatment of emergency medical conditions on an urgent basis without requiring a previously scheduled appointment)
G0383
Level 4 hospital emergency department visit provided in a type B emergency department; (the ED must meet at least one of the following requirements: (1) it is licensed by the state in which it is located under applicable state law as an emergency room or emergency department; (2) it is held out to the public as a place that provides care for emergency medical conditions on an urgent basis without requiring a previously scheduled appointment; or (3) during the calendar year immediately preceding the calendar year in which a determination under 42 CFR 489.24 is being made, based on a representative sample of patient visits that occurred during that calendar year, it provides at least one-third of all of its outpatient visits for the treatment of emergency medical conditions on an urgent basis without requiring a previously scheduled appointment)
Codes with Status Indicator “J2” from Addendum B and Descriptions from 2016 CPT code book
OBSERVATION C-APC 8011 - STATUS INDICATOR “J2”..CONTINUED

45 CRHF ECONOMICS & HEALTH POLICY
CPT® Code
Description
G0384
Level 5 hospital emergency department visit provided in a type B emergency department; (the ED must meet at least one of the following requirements: (1) it is licensed by the state in which it is located under applicable state law as an emergency room or emergency department; (2) it is held out to the public as a place that provides care for emergency medical conditions on an urgent basis without requiring a previously scheduled appointment; or (3) during the calendar year immediately preceding the calendar year in which a determination under 42 CFR 489.24 is being made, based on a representative sample of patient visits that occurred during that calendar year, it provides at least one-third of all of its outpatient visits for the treatment of emergency medical conditions on an urgent basis without requiring a previously scheduled appointment)
G0379
Direct admission of patient for hospital observation care
G0463
Hospital outpatient clinic visit for assessment and management of a patient
Codes with Status Indicator “J2” from Addendum B and Descriptions from 2016 CPT code book
OBSERVATION C-APC 8011 - STATUS INDICATOR “J2”..CONTINUED

46 CRHF ECONOMICS & HEALTH POLICY
DEVICE MONITORING
2016 CPT code book
CPT® Code
Description
93279
Programming device evaluation (in person) with iterative adjustment of the implantable device to test the function of the device and select optimal permanent programmed values with analysis, review and report by a physician or other qualified health care professional; single lead pacemaker system
93280 dual lead pacemaker system
93281 multiple lead pacemaker system
93282
Programming device evaluation (in person) with iterative adjustment of the implantable device to test the function of the device and select optimal permanent programmed values with analysis, review and report by a physician or other qualified health care professional; single lead transvenous implantable defibrillator system
93283 dual lead transvenous implantable defibrillator system
93284 multiple lead transvenous implantable defibrillator system

47 CRHF ECONOMICS & HEALTH POLICY
DEVICE MONITORING..CONTINUED
CPT® Code
Description
93285
Programming device evaluation (in person) with iterative adjustment of the implantable device to test the function of the device and select optimal permanent programmed values with analysis, review and report by a physician or other qualified health care professional; implantable loop recorder system
93288 Interrogation device evaluation (in person) with analysis, review and report by a physician or other qualified health care professional, includes connection, recording and disconnection per patient encounter; single, dual, or multiple lead pacemaker system
93289 single, dual, or multiple lead transvenous implantable defibrillator system, including analysis of heart rhythm derived data elements
93290 implantable cardiovascular monitor system, including analysis of 1 or more recorded physiologic cardiovascular data elements from all internal and external sensors
93291 implantable loop recorder system, including heart rhythm derived data analysis
93293 Transtelephonic rhythm strip pacemaker evaluation(s) single, dual, or multiple lead pacemaker system, includes recording with and without magnet application with analysis, review and report(s) by a physician or other qualified health care professional, up to 90 days
2016 CPT code book

48 CRHF ECONOMICS & HEALTH POLICY
CPT® Code
Description
93296 Interrogation device evaluation(s) (remote), up to 90 days; single, dual, or multiple lead pacemaker system or implantable defibrillator system, remote data acquisition(s), receipt of transmissions and technician review, technical support and distribution of results
93299 Interrogation device evaluation(s), (remote) up to 30 days; implantable cardiovascular monitor system or implantable loop recorder system, remote data acquisition(s), receipt of transmissions and technician review, technical support and distribution of results
2016 CPT code book
DEVICE MONITORING..CONTINUED
49 CRHF ECONOMICS & HEALTH POLICY
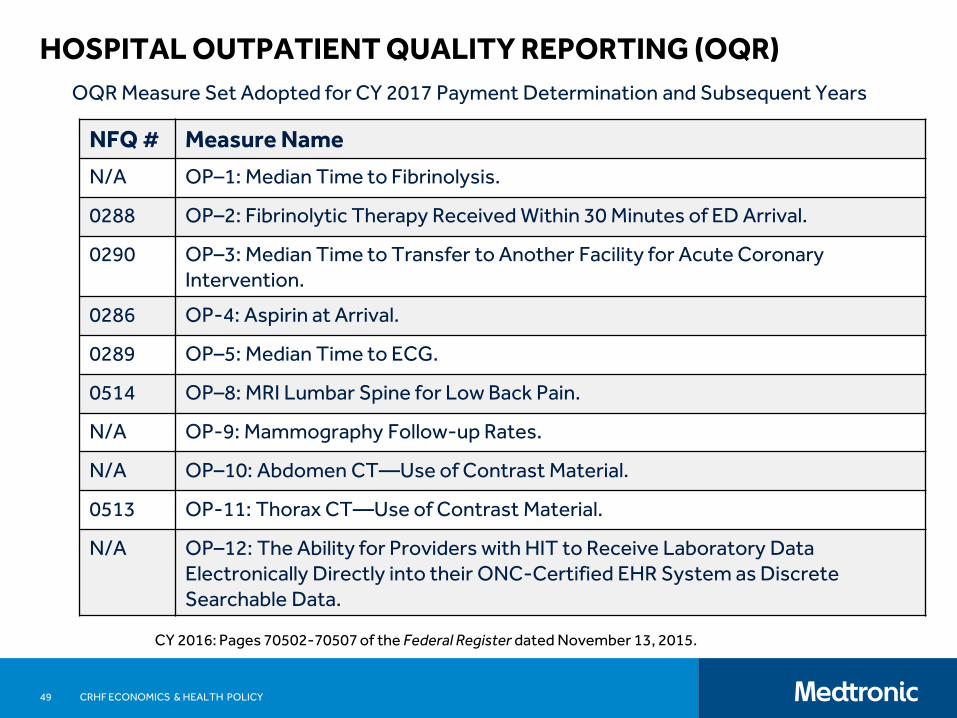
HOSPITAL OUTPATIENT QUALITY REPORTING (OQR)
CY 2016: Pages 70502-70507 of the Federal Register dated November 13, 2015.
NFQ # Measure Name
N/A OP–1: Median Time to Fibrinolysis.
0288 OP–2: Fibrinolytic Therapy Received Within 30 Minutes of ED Arrival.
0290 OP–3: Median Time to Transfer to Another Facility for Acute Coronary Intervention.
0286 OP-4: Aspirin at Arrival.
0289 OP–5: Median Time to ECG.
0514 OP–8: MRI Lumbar Spine for Low Back Pain.
N/A OP-9: Mammography Follow-up Rates.
N/A OP–10: Abdomen CT—Use of Contrast Material.
0513 OP-11: Thorax CT—Use of Contrast Material.
N/A OP–12: The Ability for Providers with HIT to Receive Laboratory Data Electronically Directly into their ONC-Certified EHR System as Discrete Searchable Data.
OQR Measure Set Adopted for CY 2017 Payment Determination and Subsequent Years

50 CRHF ECONOMICS & HEALTH POLICY
HOSPITAL OUTPATIENT QUALITY REPORTING (OQR)
CY 2016: Pages 70502-70507 of the Federal Register dated November 13, 2015. OP-15 Use of Brain Computed Tomography (CT) in the Emergency Department for Atraumatic Headache was removed.
NFQ # Measure Name
0669 OP–13: Cardiac Imaging for Preoperative Risk Assessment for Non-Cardiac Low-Risk Surgery.
N/A OP–14: Simultaneous Use of Brain Computed Tomography (CT) and Sinus Computed Tomography (CT).
N/A OP-17: Tracking Clinical Results between Visits.
0496 OP–18: Median Time from ED Arrival to ED Departure for Discharged ED Patients.
N/A OP-20: Door to Diagnostic Evaluation by a Qualified Medical Professional.
0662 OP–21: Median Time to Pain Management for Long Bone Fracture.
N/A OP-22: ED- Left Without Being Seen.
0661 OP–23: Head CT or MRI Scan Results for Acute Ischemic Stroke or Hemorrhagic Stroke who Received Head CT or MRI Scan Interpretation Within 45 minutes of ED Arrival.
OQR Measure Set Adopted for CY 2017 Payment Determination

51 CRHF ECONOMICS & HEALTH POLICY
HOSPITAL OUTPATIENT QUALITY REPORTING (OQR)
CY 2016: Pages 70502-70505 of the Federal Register dated November 13, 2015.
NFQ # Measure Name
N/A OP–25: Safe Surgery Checklist Use.
N/A OP–26: Hospital Outpatient Volume on Selected Outpatient Surgical Procedures. (Additional information is available at: www.qualitynet.org)
0431 OP-27: Influenza Vaccination Coverage among Healthcare Personnel.
0658 OP–29: Endoscopy/Polyp Surveillance: Appropriate Follow-up Interval for Normal Colonoscopy in Average Risk Patients.
0659 OP–30: Endoscopy/Polyp Surveillance: Colonoscopy Interval for Patients with a History of Adenomatous Polyps—Avoidance of Inappropriate Use.
1536 OP–31: Cataracts—Improvement in Patient’s Visual Function within 90 Days Following Cataract Surgery. (This measure is voluntary during CY 2015)
OQR Measure Set Adopted for CY 2017 Payment Determination and Subsequent Years

52 CRHF ECONOMICS & HEALTH POLICY
CONDITIONALLY PACKAGED DIAGNOSTIC LAB SERVICES
When Diagnostic Laboratory services are reported on an Outpatient hospital claim that includes a procedure/service assigned a Status Indicator of “J1,” “J2,” “Q1,” “Q2,” or “Q3’’ and also “S,” “T,” or “V”, the Q4 Conditionally Packaged Laboratory Test will be applicable.
Modifier L1 became effective in 2014 , the first year that Lab test were conditionally packaged, and should be reported with the Laboratory test when reporting an Unrelated Laboratory test procedure code(s).
CY 2016 Laboratory services are eligible for separate reimbursement if: (1) it is the only
service(s) provided to a hospital Outpatient and there is a payment rate included in the CLFS (Clinical Laboratory Fee Schedule) or (2) ordered for a different diagnosis than another outpatient hospital service by a practitioner different than the practitioner who ordered the other outpatient hospital service.
When only Laboratory services are reported and this test is included in the CLFS, the new Conditional Packaging Status Indicator “Q4: Conditionally Packaged Laboratory Test” is converted to Status Indicator “A” (Not Paid under OPPS) and reimbursed based on the amount included in the CLFS . The L1 modifier is not applicable for these services.
CY 2016: Pages 70304, 70348-70350, 70366 of the Federal Register dated November 13, 2015.

53 CRHF ECONOMICS & HEALTH POLICY
CHANGES IN OPPS DEVICE PASS-THROUGH PROCESS OPPS Device Pass-Through Payments: Enable initial access to new technology
Currently: CMS accepts and reviews applications on a quarterly basis through a subregulatory process.
In CY 2016:
The Quarterly subregulatory review process will include a description of application(s) received and rational for approving the application(s) in the next applicable Proposed OPPS rule. Applications that are not approved will also be included in the applicable Proposed OPPS rule unless the application is withdrawn.
Evaluate device pass-through applications through annual rule making.
Application must be submitted:
Within 3 years of FDA approval/clearance or the date of market availability if there is a documented, verifiable delay of product availability after receiving FDA approval/clearance.
CY 2016: Pages 70305, 70416-70420 of the Federal Register dated November 13, 2015. The link for the CMS Fact Sheet dated October 30, 2015 is in the Appendix.

54 CRHF ECONOMICS & HEALTH POLICY
APPENDIX: REFERENCES
OPPS CY 2016 Federal Register dated November 13, 2015 is available at:
http://www.gpo.gov/fdsys/pkg/FR-2015-11-13/pdf/2015-27943.pdf
Data files released with the CY 2016 final rule are available at:
https://www.cms.gov/Medicare/
Medicare-Fee-for-Service-Payment/HospitalOutpatientPPS/
Hospital-Outpatient-Regulations-and-Notices.html
Click on Regulation No. CMS-1633-FC and Regulation No. CMS-1607-FC
The “2016 Final Rule Addenda” zip file includes: Addendum A (APC payment), Addendum
B (HCPCS listing and APC assignment), Addendum C (APC assignment and then
every HCPCS assigned to that APC), Addendum D-1 (Status Indicators),
Addendum J (Complexity Adjusted APC details) and other files.
CMS Fact Sheets dated October 30, 2015: Fact Sheet Two-Midnight Rule: https://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2015-Fact-sheets-items/2015-10-30-4.html Fact Sheet CMS Finalizes Hospital Outpatient and Ambulatory Surgical Center Policy and Payment Changes, Including Changes to the Two-Midnight Rule and Quality Reporting for 2016: https://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2015-Fact-sheets-items/2015-10-30-3.html

55 CRHF ECONOMICS & HEALTH POLICY
APPENDIX: REFERENCES
Pacemaker CMS regulation links
NCD:
https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/Downloads/R186NCD.pdf
Claims Processing Transmittal No. 3384:
https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/Downloads/R3384CP.pdf
MM9078:
https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/Downloads/MM9078.pdf
FY 2014 final rule publication in the Federal Register dated August 19, 2013:
http://www.gpo.gov/fdsys/pkg/FR-2013-08-19/pdf/2013-18956.pdf
CY 2015 final rule publication in the Federal Register dated November 10, 2014:
http://www.gpo.gov/fdsys/pkg/FR-2014-11-10/pdf/2014-26146.pdf