cyberknife - introducing a new treatment approach to...
TRANSCRIPT

CyberKnife - Introducing a New Treatment Approach to Ireland
Gillian Moore. CyberKnife CoordinatorRadiotherapy and CyberKnife Centre.Hermitage Medical Clinic. Dublin

Overview:
• Introduction to the Cyberknife At HMC
• What can be treated and what have we treated??
• System Overview
• How it works?
• Tracking Systems --- Real time tracking

Hermitage Clinic CyberKnife

Hermitage Clinic CK Team DAY 1

What is CYBERKNIFE????
• The CyberKnife Radiosurgery System is the worlds first and only intelligent robotic radiosurgery system designed to treat tumours, cancerous and non-cancerous, anywhere in the body.
• It can track, detect and correct for tumour movement and patient movement throughout the treatment with sub millimeter accuracy.

What is CYBERKNIFE????• It delivers high dose pencil beams of radiation with pin-point
accuracy.
• Because the CyberKnife can deliver radiation beams from virtually any direction (non co-planar) the radiation beams can be focused more precisely on the tumour minimizing damage to the surrounding healthy tissue and any nearby critical structures.
• Each Radiotherapy treatment is delivered using as
many as 200 beams, as the dose is
painted onto the target.

CyberKnife® Robotic Radiosurgery: Beam Geometry
Non-Isocentric Beam DeliveryNon-Coplanar Beam Delivery
• ~100 unique positions (nodes) from which beams can be directed
• Multiple, non-isocentric beams from each node are used (although isocentric targeting is also possible)

Gantry Based Linac Treatment CyberKnife® Treatment
Restricted to clock-wise/counter-clockwise movement
Unrestricted non-coplanar treatment delivery
CyberKnife® Robotic Radiosurgery System

What is CYBERKNIFE????
• It is completely non-invasive. It provides a pain-free, non-surgical option for patients who have inoperable brain tumours or surgically complex tumours, or who may be looking for an alternative to surgery or may be unsuitable for surgery
• 1-5 fractions• No Anaesthetic• No infection risk.• Completely Pain Free • Out Patient Procedure• Little or No recovery time• Improved QOL for patients.• 1-5 days CK Vs 6-8 weeks RT

What can be Treated:
• Acoustic Neuroma
• Anaplastic Astrocytoma
• Arteriovenous Malformation (AVM)
• Craniopharyngioma
• DNET
• Ependymoma
• Epidural Haematoma
• Gangliocytoma
• GBM
• Germinoma
• Glioma
• Glomus Jugulare Tumour
• Hamangioblastoma
• Meningioma
• Neurocytoma
• NF2
• Oligodendroglioma
• PNET
• Pituitary Adenoma
• Schwannoma
• Trigeminal Neuralgia
• Osteosarcoma
• Nasopharyngeal
• Squamous cell Ca
• Non Small and Small Cell Lung
• Pancreatic
• Hepatocellular
• Prostate
• Renal Ca
• Colon
• Ovarian
• Uterine
• Solitary Mets anywhere
• The list is quite extenive. => Only Limiting factors are the size and the patient Status

What are we treating at HMC with CK?

At HMC we started off with Intracranial:
Intracranial = Meningiomas, Acoustic Neuromas, TGN, AVMs, Brain Metastases and Pituitary Tumours.
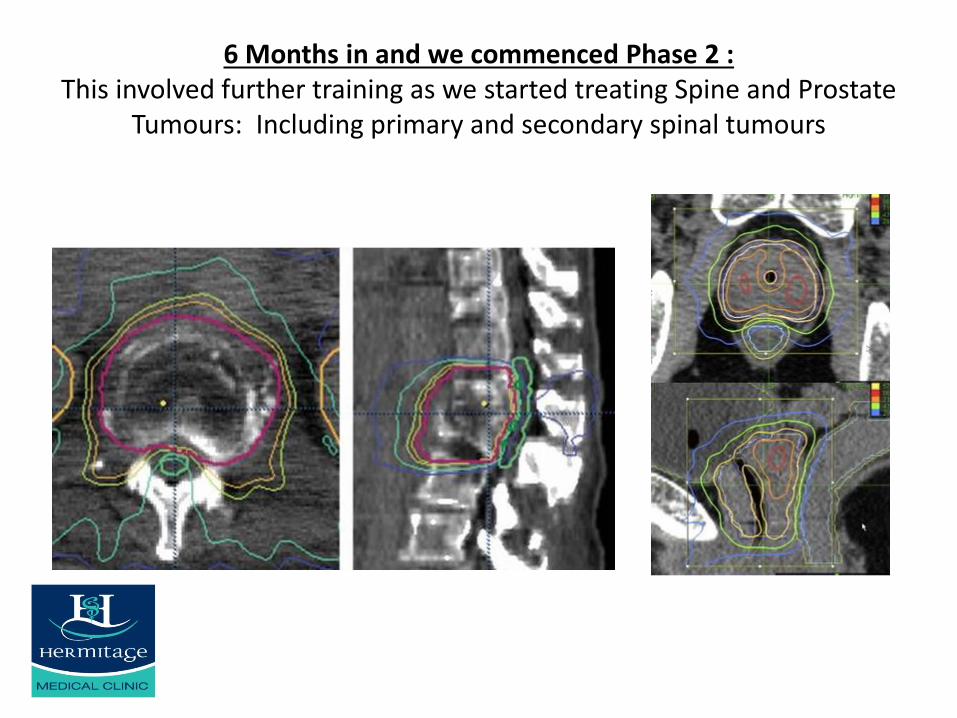
6 Months in and we commenced Phase 2 :This involved further training as we started treating Spine and Prostate
Tumours: Including primary and secondary spinal tumours
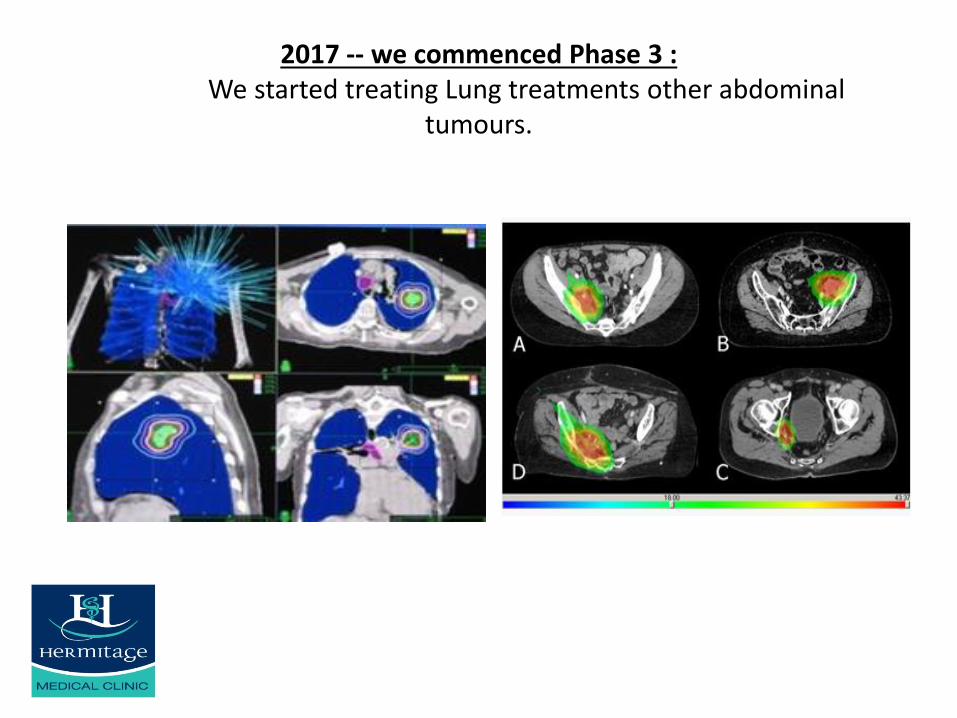
2017 -- we commenced Phase 3 : We started treating Lung treatments other abdominal
tumours.

Numbers to Date: 455 patients treated to date
0
2
4
6
8
10
12
14
16
18
No
v-1
3
Feb
-14
May
-14
Au
g-1
4
No
v-1
4
Feb
-15
May
-15
Au
g-1
5
No
v-1
5
Feb
-16
May
-16
Au
g-1
6
No
v-1
6
Feb
-17
May
-17
Pt Numbers
Pt Numbers

Numbers to Date: 455 CK Patients Treated to date
0
5
10
15
20
25
30
35
40
45
Pt Numbers every Quarter since Nov 13
Pt Numbers every Quartersince Nov 13

Numbers by Dx:
%
Acoustic Neuroma
Trigeminal Neuralgia
Meningioma
AVM
Brain Mets
Pituitary
Other
Spine
Prostate
lung
Acoustic Neuromas
TGN
Where did it come from???

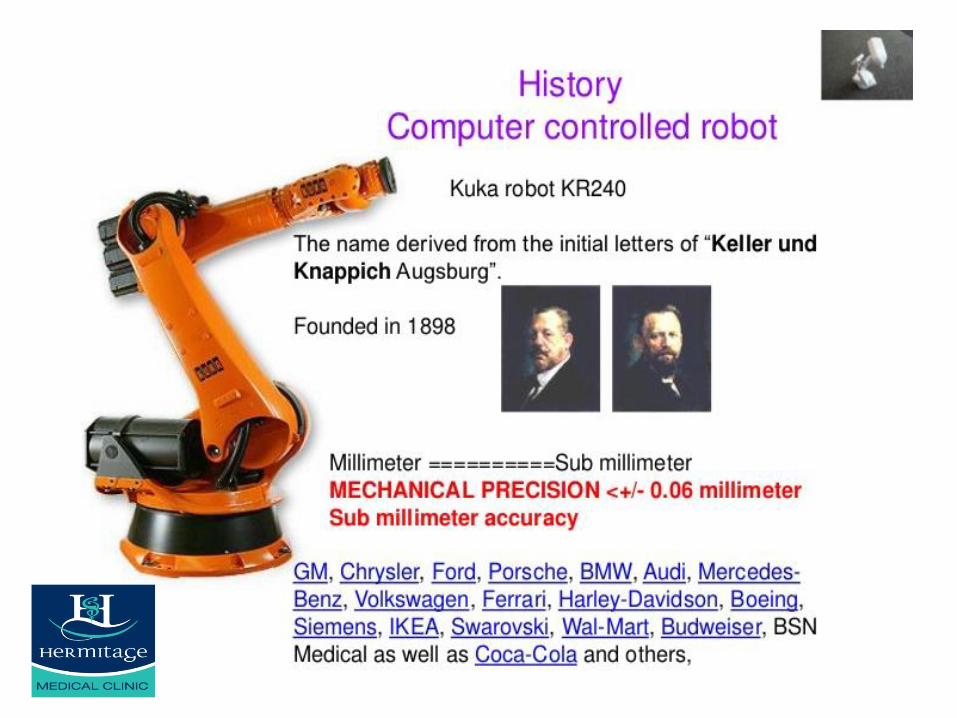
History ...
▪ Cyberknife was invented over a period of 10 years by John Adler at Stanford
University -- professor of Neurosurgery and Radiation Oncology.
▪ It was approved by the FDA in 2001 for a wide range of body sites.
▪ By December 2010 more than 100,000 patients treated worldwide with CK.
▪ There are more than 150 Hospitals and Medical Centers worldwide with
Cyberknife treatment units Installed.
▪ More than 200 peer review papers have been published providing evidence of
its efficacy.

How does it work????
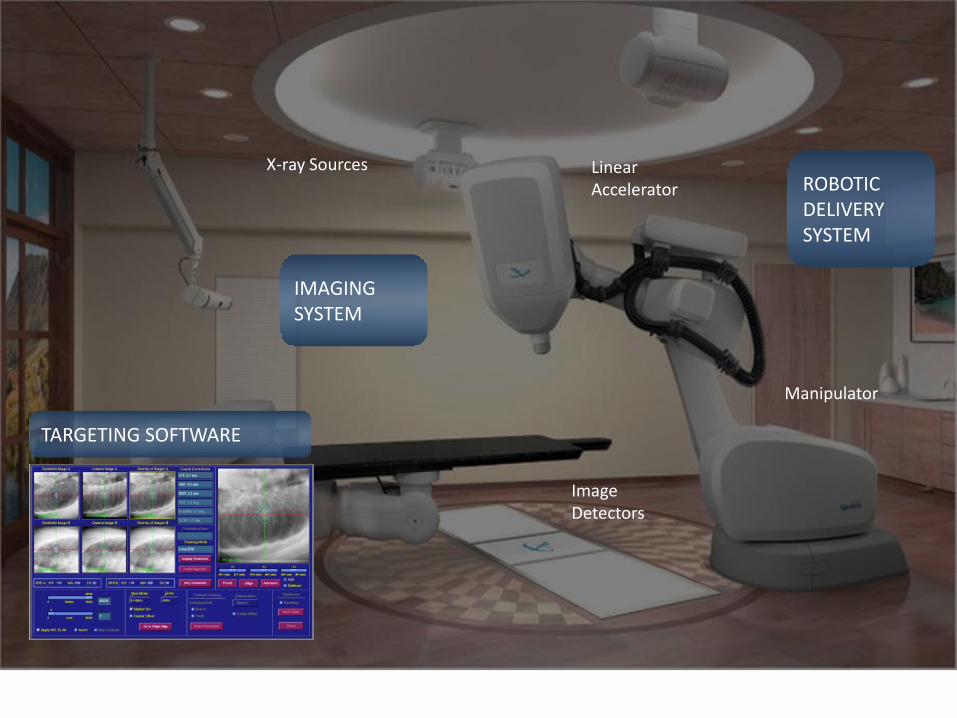
Linear Accelerator
Manipulator
ImageDetectors
X-ray Sources
IMAGINGSYSTEM
ROBOTICDELIVERYSYSTEM
TARGETING SOFTWARE

Methods of Beam shaping:
There are 12 secondary collimators to define the size ofthe beam.
Ranging in size from 5mm to 60 mm.

Iris Variable Aperture Collimator:
• Moves like the iris of your eye to collimate the beam.
• Tungsten segments rapidly move in and out to define beam shape / geometry.
• This reduces treatment times as no need to change the collimators during the treatment.

Referral pathway for Cyberknife treatment
Completion of data form
Diagnostic scans
Presentation at cyberknife
MDT
suitable
Not suitable feedback to referral
Consultation with Radiation oncologist
and coordinator
Immobilisation and primary/secondary
scans
Treatment planning and delivery

Treatment Delivery

Tumour tracking
Ability to track tumour/structure to ensure accurate treatment delivery
‘Real-time’ imaging: Linac-based- imaging means taking scan (1-2 minutes), reviewing (1-2 minutes), correcting (1-2 minutes) possibility target position has changed in this time.
Cyberknife- real time, corrects immediately after imaging and continuously throughout treatment.

Tracking systems:
– Imaging software that tracks anatomy to ensure beam is always directed at target.
– Allowing the robot to Automatically correct.

CyberKnife Tracking Methods
6D Skull Tracking
Xsight Lung Tracking System
Fiducial Tracking
SpineTracking
All methods are frameless and automated
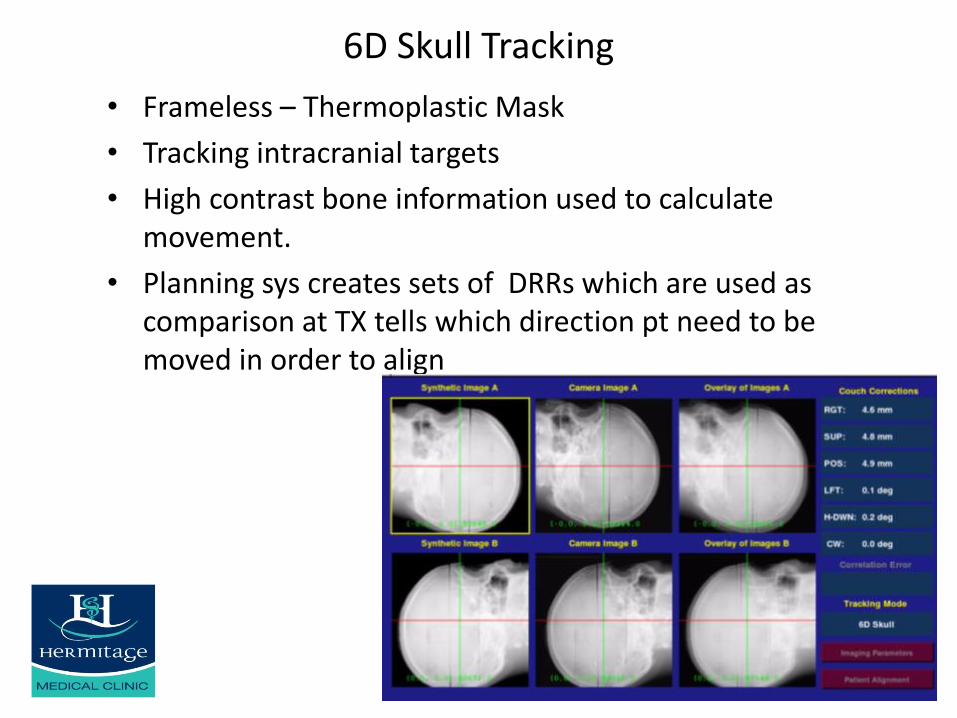
6D Skull Tracking
• Frameless – Thermoplastic Mask
• Tracking intracranial targets
• High contrast bone information used to calculate movement.
• Planning sys creates sets of DRRs which are used as comparison at TX tells which direction pt need to be moved in order to align

Tracking Method
Occasionally bony anatomy isn't sufficient to track tumour
This requires placement of gold fiducials within or near the target, these are placed as an outpatient procedure, similar to a needle biopsy
Imaging software then capture the position of these markers to guide treatment and correct for potential movement
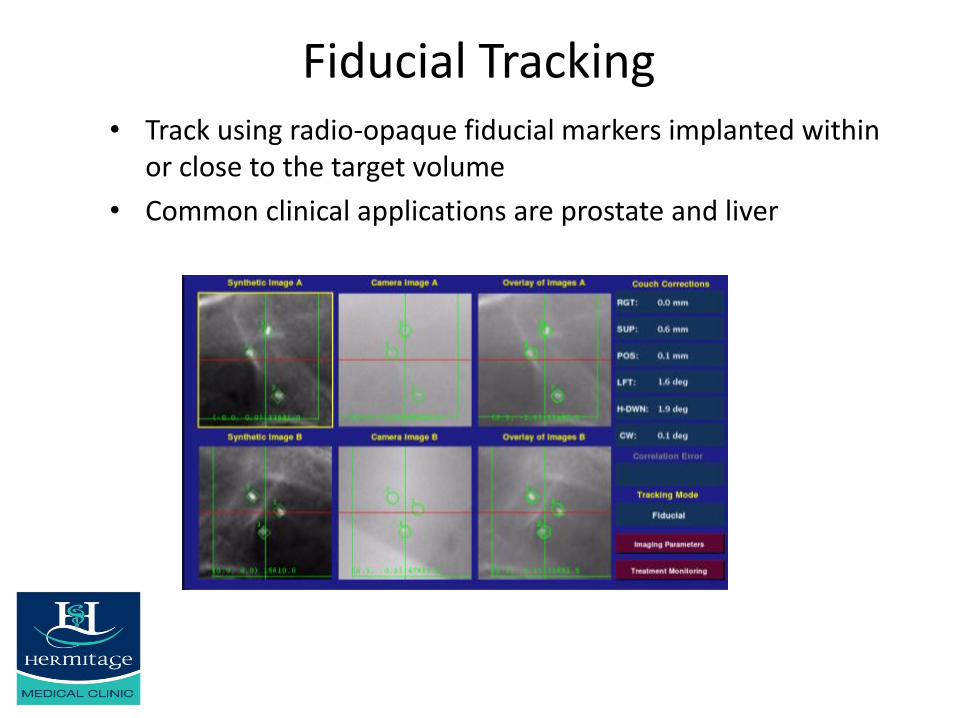
Fiducial Tracking• Track using radio-opaque fiducial markers implanted within
or close to the target volume
• Common clinical applications are prostate and liver

Fiducial Markers• Most fiducial markers are gold seeds, 0.8 – 1.2 mm diameter, 3-6 mm
long.
• We require a minimum of 3 markers to calculate rotations as well as translations, and placement of 5 markers is recommended as some may migrate before tx and are unsuitable for use.
• It is Important that fiducials are implanted a minimum, of 14 days before CT and MRI
• Marker placement is commonly made percutaneously under image guidance.

Xsight® Spine Tracking System
• Track targets in or near skeletal structures of the Spine without the need to implant fiducials
• Uses an algorithm similar to Skull tracking to compare bone densities.

Xsight® Lung Tracking System
• Introduced in 2006 by Accuray.
• Requires visibility of tumor in both orthogonal views.
• Using different algorithm the system will lock onto the tumour.
Reference: D. Fu et al. “Xsight Lung Tracking System: A Fiducial-Less Method for Respiratory Motion Tracking.” Robotic Radiosurgery: Treating Tumors that Move with Respiration. Edited by H.C. Urschel, Jr. Springer-Verlag (2007).

Synchrony® Respiratory Tracking System

Synchrony
• Continuously tracks, detects and automatically corrects for patient and tumor movement•Machine moves as patient breathes, no need to breath hold•Use LEDs on pts chest to build a breathing pattern on the synchrony system and then teach the robot to breath like the patient.
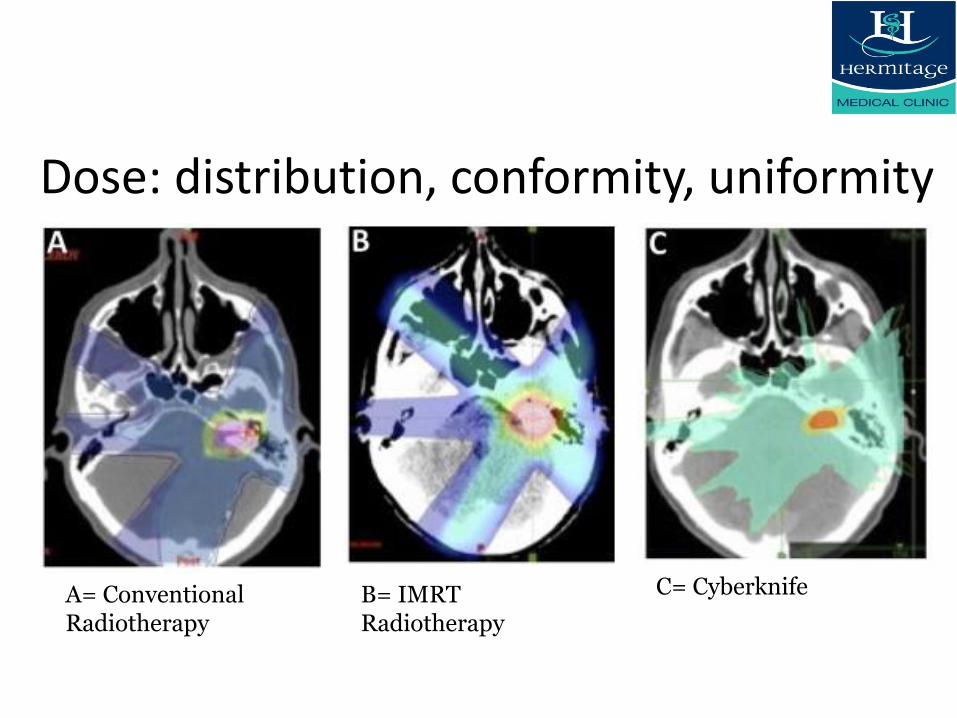
Dose: distribution, conformity, uniformity
A= Conventional Radiotherapy
B= IMRT Radiotherapy
C= Cyberknife

Summary:
• Cyberknife is the latest in the armoury against Cancer.
• It is completely non-invasive & provides a pain-free, non-surgical option for patients
• 1-5 fractions
• No Anaesthetic / Infection risk
• Completely Pain Free
• Out Patient Procedure with little or No recovery time
• Improved QOL for patients
• 1-5 days CK Vs 6-8 weeks RT
• Extremely accurate with excellent conformity

CyberKnife® Robotic Radiosurgery System

Thank You.

• http://www.accuray.com/sites/default/files/demos/vsi/index.html