d isoders of secondary hemostasis disorders of plasma clotting factors
TRANSCRIPT

DISODERS OF SECONDARY HEMOSTASISDisorders of plasma clotting factors

DISORDERS OF SECONDARY HEMOSTASIS Disorders of the proteins of fibrin formation Disorders of proteins associated with
fibrinolysis Symptoms of secondary hemostatic disorders
Delayed bleeding Deep muscular bleeding Spontaneous joint bleeding Symptoms common to primary and secondary
hemostatic disorders Ecchymoses GI bleeding Hematuria Hypermenorrhea Gingival bleeding Increased bleeding after tooth extraction Intracranial bleeding Epistaxis
Hereditary vs acquired Quantitative vs qualitative deficiencies
Laboratory screening tests (PT, APTT) Does not differentiate quantitative vs qualitative disorders
Qualitative abnormal proteins will Prolong clotting test Be recognized by immunologically-based procedures
Activity assays Essential when screening for deficiencies
DISORDERS OF PROTEINS OF FIBRIN FORMATION
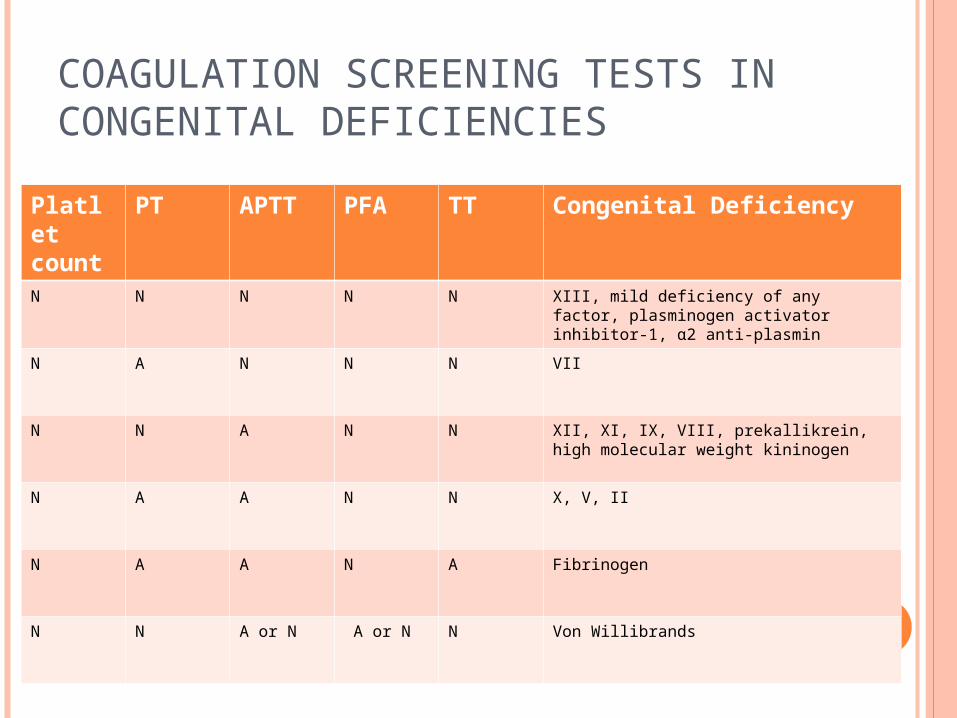
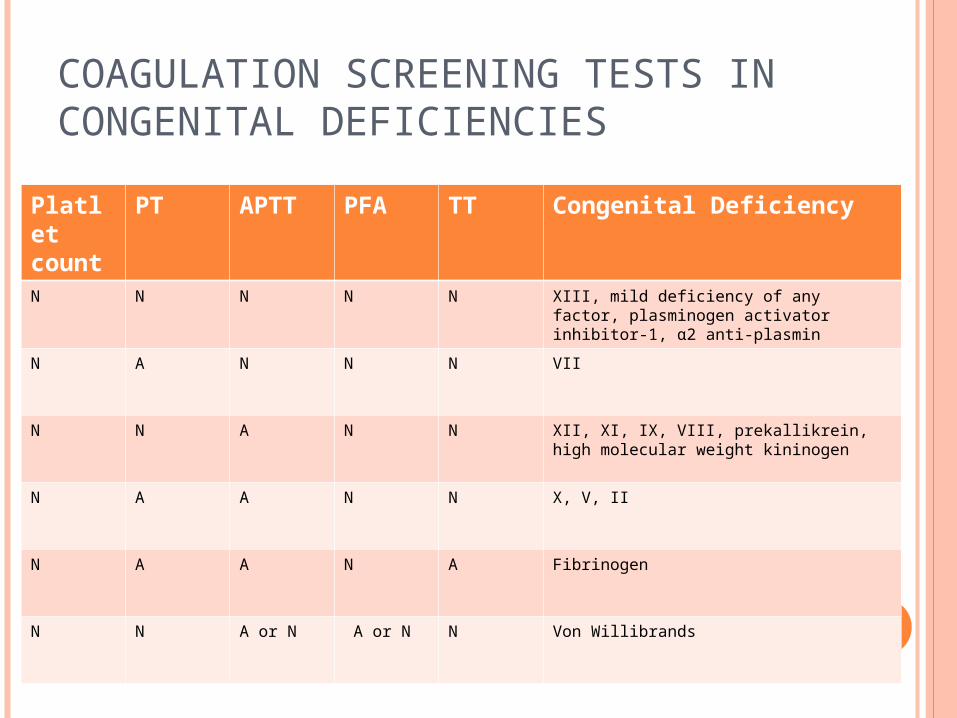
COAGULATION SCREENING TESTS IN CONGENITAL DEFICIENCIES
Platlet count
PT APTT PFA TT Congenital Deficiency
N N N N N XIII, mild deficiency of any factor, plasminogen activator inhibitor-1, α2 anti-plasmin
N A N N N VII
N N A N N XII, XI, IX, VIII, prekallikrein, high molecular weight kininogen
N A A N N X, V, II
N A A N A Fibrinogen
N N A or N A or N N Von Willibrands
Inherited hemorrhagic disorder Genetically and clinically heterogeneous Caused by a deficiency/dysfunction of VWF Most common hereditary bleeding disorder
VWF Multimeric blood protein Performs two major roles in hemostasis
Mediates adhesion of platelets to sites of vascular injury Is a carrier protein for F-VIII
Inherited defects in VWF may Interfere with biosynthetic processing or disrupt specific
ligand binding sites Cause bleeding by impairing either platelet adhesion or
blood clotting
VON WILLEBRAND DISEASE

Three major categories of VWD Type 1 VWD – partial quantitative deficiency of VWF Type 2 VWD – qualitative deficiency of VWF
Divided into 4 variants Type 2A – ↓ platelet-dependent function
Absence of high-molecular weight VWF multimers Type 2B – ↑ affinity for platlet GPIb Type 2M – ↓ platelet-dependent function
Not caused by the absence of HMW multimers Type 2N – Markedly ↓ affinity for F-VIII
Type 3 VWD – total deficiency of VWF Types 1 and 2 – autosomal dominant inheritance Type 3 – autosomal recessive inheritance
Diagnosis Specific tests
Quantify VWF and F-VIII activity
VWD
Hemorrhagic tendency is highly variable Depends on the type and severity of disease Patients with Type 1 and 2 disease
May have mild bleeding symptoms Characterized by hemorrhage from delicate mucocutaneous
tissues Epistaxis, easy bruising, GI bleeding, menorrhagia Hematoma and hemarthroses, characteristic of hemophilia A, are
not prominent Patients with severe type 3 VWD
Severe hemorrhagic tendency Spontaneous hemorrhage
Mucous membranes, GI tract Can be frequent and may be life threatening
Low F-VIII level Deep hematomas Joint hemorrhages – similar to hemophilia
VWD – CLINICAL MANIFESTATIONS
Goal Correct both bleeding time and coagulation
abnormalities Raise both F-VIII and VWF to normal levels
Desmopressin acetate (DDAVP) stimulates release of vWF from endothelial cells – won’t work for type 3
Intermediate purity factor VIII which contains intact vWF
VWD – THERAPY

Hemophilia A Factor VIII Deficiency
Antihemophilic Factor X-linked recessive disorder Most common type of hemophilia
Hemophilia B Factor IX Deficiency
Christmas Factor (from family of first patients diagnosed with the disorder)
X-linked recessive disorder Hemophilia C
Factor XI Deficiency Autosomal recessive disorder seen primarily in the
Ashkenazi Jewish population Symptoms range from mild to severe
HEMOPHILIAS
COAGULATION SCREENING TESTS IN CONGENITAL DEFICIENCIES
Platlet count
PT APTT PFA TT Congenital Deficiency
N N N N N XIII, mild deficiency of any factor, plasminogen activator inhibitor-1, α2 anti-plasmin
N A N N N VII
N N A N N XII, XI, IX, VIII, prekallikrein, high molecular weight kininogen
N A A N N X, V, II
N A A N A Fibrinogen
N N A or N A or N N Von Willibrands

Insufficient generation of thrombin by F-IXa/VIIIa complex through the intrinsic pathway of
coagulation cascade Bleeding severity complicated by excessive fibrinolysis
Clinical severity corresponds with level of factor activity
Severe hemophilia Factor coagulant activity <1% of normal Frequent spontaneous bleeding into joints and soft
tissues Prolonged bleeding with trauma or surgery
HEMOPHILIA
Moderate hemophilia Factor coagulant activity 1-5% of normal Occasional spontaneous bleeding Excessive bleeding with surgery or trauma
Mild hemophilia Factor coagulant activity >5% of normal Usually no spontaneous bleeding Excessive bleeding with surgery or trauma
HEMOPHILIA

Readily diagnosed In severe disease and patients with prior family history
Diagnosis based on Unusual bleeding symptoms early in life Age of first bleeding varies with severity of disease Family history Physical exam Laboratory evaluation
HEMOPHILIA – CLINICAL PRESENTATION
Replacement of clotting factor to achieve hemostasis Annual cost for patient with severe hemophilia
$20,000-100,000 Various products available
Plasma-derived low, intermediate and high purity products Plasma-derived ultrapure products Ultrapure recombinant products
Replacement products – benefits vs risks Blood-born pathogens
Hepatitis A, B, C, G; HIV, Parvovirus B-19 Thrombotic complications with some F-IX concentrations Development of alloantibody inhibitors
Neutralize coagulant effects of replacement therapy
HEMOPHILIA – TREATMENT
More common than hereditary disorders Usually involve defects of multiple hemostatic factors Bleeding often simultaneously from >1 site May occur in response to another disease process Can be produced by a variety of mechanisms
ACQUIRED DISORDERS
Normal balance of hemostasis is altered Results in the uncontrolled inappropriate formation and
lysis of fibrin within the blood vessels Activation of coagulation occurs systemically
Rather than locally at site of injury Fibrin is deposited diffusely within capillaries, arterioles
and venules Clotting proteins, inhibitors and platelets are
consumed faster than they are synthesized Acquired deficiency of multiple hemostatic components Fibrinolysis follows fibrin formation Patient generally bleeds spontaneously at the same time
that disseminated clotting is occurring
DISSEMINATED INTRAVASCULAR COAGULATION

CLINICAL CONDITIONS ASSOCIATED WITH DIC

Fibrin strands within small vessels result in Traumatic destruction of RBC
Microangiopathic hemolytic anemia Formation of schistocytes
Fibrin deposition in and obstruction of microvasculature Tissue anoxia/microinfarcts Renal failure, liver failure, respiratory failure, shock
and death
DIC - PATHOPHYSIOLOGY
DIC
HELLP syndrome High blood pressure Elevated liver enzymes Low platlets Occurs in pregnancy and is life-threatening If the CBC of a woman in labor shows
schistocytes and low platlets alert the physician immediately – the baby must be delivered immediately to save the mom!
Laboratory diagnosis is difficult Available tests are nonspecific No single test can establish the definitive diagnosis of
DIC PT, APTT, TT prolonged Fibrin degradation products are (+) Platelet count ↓; platelet function tests abnormal Schistocytes, thrombocytopenia on peripheral blood
smear
DIC – LABORATORY DIAGNOSIS

Eliminate underlying cause, if possible Acute DIC is often self-limited
Will disappear when fibrin is lysed Replacement therapy
Platelets, RBC, Cryoprecipitate or fresh frozen plasma
DIC – THERAPY
Precursor proteins synthesized by hepatocytes Not γ-carboxylated Ca++-binding sites are nonfunctional Induced functional deficiencies of all vitamin-K
dependent proteins Causes of vitamin K deficiency in adults
Malabsorptive syndromes Biliary tract obstruction Prolonged broad-spectrum antibiotics
Most often seen in newborns Hemorrhagic disease of the newborn
Due to newborn hepatic immaturity
VITAMIN K DEFICIENCY

Circulating anticoagulants Usually IgG or IgM immunoglobulins Inhibitors of single factors
Patients with inherited factor deficiencies After treatment with replacement concentrates
Associated with other conditions Diseases, drugs
Occasionally seen in otherwise healthy individuals Interfere with or neutralize clotting factor activity Prolonged screening test not corrected by 1:1 mixture with
normal plasma
ACQUIRED PATHOLOGIC INHIBITORS