d prabhakaran dm, frcp, fnascorigin.searo.who.int/entity/noncommunicable_diseases/events/ncd... ·...
TRANSCRIPT

D Prabhakaran DM, FRCP, FNAScVice President and Professor Epidemiology , Public Health Foundation of India
Executive Director, Centre for Chronic Disease Control, New Delhi
Chair, Department of Epidemiology, London School of Hygiene and Tropical Medicine, London, UK
Adjunct Professor, Emory University, Atlanta, GA, USA
Innovative Service Delivery Experiences from India

Innovations ?
Disruptive innovation : An innovation that creates a new
market by applying a different set of values, which ultimately
(and unexpectedly) overtakes an existing market.
Not necessarily new or path breaking

What are the innovations at the level of Health
Systems in Chronic Disease management and
control
• Health system strengthening through task shifting and task
sharing; team based care
• Use of affordable technologies
• Enhancing Human Resource Capacity
• Structured behavior change communication using frontline health
care workers
• Traditional approaches
• Integration of chronic care
• Setting based interventions
• Individual level
• Improving compliance/ FDC

• Health system strengthening through task
sharing using frontline health workers/nurses
and using inexpensive technology
– An example of disruptive innovation
Study/Program Location Features
mPower ( HT+
DM)
Himachal
Pradesh
frontline health workers/nurses and
mobile phone/tablet at CHCs
UDAY ( HT+ DM) Haryana/AP Comprehensive intervention package at
Community and Health system
SIMCARD (HT) Haryana/Tibet frontline health workers/nurses at
PHCs and Community
mWellcare (
Integration of
Chronic Care)
Haryana/TN frontline health workers at PHCs +m
Health

Why task
shifting/task
sharing
• High patient load
• Emphasis on curative
care over prevention
• Positive experience
of task shifting from
HIV and other
diseases
mHealth technologies
• Consumers : improved
convenience, more active
engagement in self-care, and
greater personalization.
• Clinicians: demands on time and
refocus on the art of medicine.
• Potential to change every aspect
of the health care environment;
delivering better outcomes and
substantially lowering costs
Need: Real-world clinical trial evidence to provide a roadmap for
implementation
Steinbuhl, Muse, Topol, JAMA, Oct 2013

From asking a research question to
scaling up: an example
Can we demonstrate the efficacy of frontline health
workers enabled with IT or smart phones in reducing
outcomes for patients with hypertension and diabetes ?

Receiver Operator Curve for comparing the
DSS and independent experts on drug management.
mhealth in HT: Development of EHR
and DSSFeb- September 2011
•Development
•Beta testing
•Validation
Methods
•Qualitative research
•End User testing
•Real vs virtual
comparison
•Comparison against
experts
Anchala R, Di Angelantonio E, Prabhakaran D, Franco OH (2013)
Development and Validation of a Clinical and Computerised Decision
Support System for Management of Hypertension (DSS-HTN) at a
Primary Health Care (PHC) Setting. PLoS ONE 8(11): e79638.

Mean blood pressure in randomised groups by month and
differences vs. baseline
Unpublished data – not for quoting
CBS: Chart based support; DSS: Decision Support System
*Covariates included: age, gender, height, waist, body mass index, alcohol intake, pickle and papad (salty food)
intake, portions of vegetable/fruit consumed per day and baseline differences in blood pressure
mhealth in HT: cRCT among physicians ( 16 PHCs ; AP)

Can these results be extended to
Community Health Workers?

CHWs and Hypertension Management in
India : Economic Modeling
– 3 day training program 3 day training program 3 day training program 3 day training program
– $700,000 hospital cost savings / million population annually$700,000 hospital cost savings / million population annually$700,000 hospital cost savings / million population annually$700,000 hospital cost savings / million population annually
– 700 CVD deaths / million averted700 CVD deaths / million averted700 CVD deaths / million averted700 CVD deaths / million averted
– 750 hospitalizations for stroke / MI averted 750 hospitalizations for stroke / MI averted 750 hospitalizations for stroke / MI averted 750 hospitalizations for stroke / MI averted
– If annual salary of CHW drops below $3500 ( 200000 Rs) If annual salary of CHW drops below $3500 ( 200000 Rs) If annual salary of CHW drops below $3500 ( 200000 Rs) If annual salary of CHW drops below $3500 ( 200000 Rs) then the program is cost saving.then the program is cost saving.then the program is cost saving.then the program is cost saving.
Gaziano, Prabhakaran et al. for ICHEALTH
Objective
• To design a feasible and
sustainable evidence-
based, decision support-
enabled, health care
delivery model for the
management of
hypertension and diabetes
at the primary health care
facilities of Himachal
Pradesh
Funded by Medtronic foundationUnpublished data: Please do not quote

Smartphone DSS

Screen-shot
Unpublished data: Please do not quote

#WCC2014
Screening of eligible patients at 5 CHCs (12
Months: March 2013- Feb 2014)
Unpublished data: Please do not quote
82,698 clinic attendees
17,590 eligible (>30 years)
5,968 HT or DM
New HT or DM (50.4%)

#WCC2014
Changes in BP and FBS at 3 and 6 months Follow up
Unpublished data: Do
not Quote

Innovations in Health Promotion :
Can we use frontline health workers?
• Diet and lifestyle InterventionS for
Hypertension Risk reduction
through Anganwadi Workers and
Accredited Social Health Activists
Acknowledgement: ICMR
‘Tell Me and I Will Forget; Show Me and I May
Remember; Involve Me and I Will Understand.’
Confucius, 551 - 479 BC

DISHA: ICMR Multicentric Study for BP
Management in Underserved Rural PopulationsCluster Randomised Controlled Trial
HP (2), Pondicherry, MP, Maharashtra, Rajasthan, AP, Orissa and Assam
Prabhakaran et al. DISHA Manual. 2012
Intervention Cluster: INTENSE intervention through IEC tools at the individual, household and community level. for control of hypertension and diabetes. The GOAL will be promotion of balanced diet, reduction of salt consumption, tobacco and alcohol consumption, and increasing physical activity. 18 months intervention by multiple methods including household visitsControl Cluster: USUAL intervention through IEC tools.


Secondary Prevention ( prevention of
second heart attack/stroke or death)
• Low hanging fruit for improving outcomes
• Ability to prevent almost 20% deaths and
hospitalization in the first year after heart attack
• Large scope for improvement (Only 10% get adequate
secondary prevention in LIC)
• Several approaches
– Role of Polypill ( CAD/Stroke/CHF); diabetes; hypertension)
– Quality improvement programs ( hospital/community)
– Traditional approaches
– Creation of Virtual clinics
– Universal Health coverage

Insights from Land of Registries:
Sweden
Study of registries concluded that•By investing $70 million yearly in disease registries, data analysis resources and information infrastructure
•Sweden could reduce its annual growth in healthcare spending from an estimated 4.7% to 4.1%
•Estimated cumulative return in reduced direct healthcare costs over 10 years: $7 billion
Policy outcome: Government prioritised expansion of
registries with increased financial commitment: $10 to $45 million/year by 2013
Larsson S et al., Health Affairs 2012;31:220-27.

Registries Improve Care by Catalyzing Healthcare
Providers: Hospitals’ Adherence to Swedish
National AMI Guidelines
Larsson S et al., Health Affairs 2012;31:220-27.

Eur Heart J 2013; 34:121-9.
Kerala ACS Registry

23
Wide variability in outcomes across hospitals

ACS Quality Improvement in Kerala
(ACS QUIK)
• We are leveraging the collaborative strength of the Kerala ACS
Registry network to develop a quality improvement program
for ACS patients in Kerala
– First of its kind in India
To develop, implement, and evaluate the impact of a quality
improvement toolkit on 30-day major adverse cardiovascular
event rates following ACS through a cluster-randomized,
stepped wedge clinical trial.
Specific Aim #1

Expectation
• ACS QUIK aims to improve in-hospital quality of care in Kerala
– Pre-hospital care
– Post-hospital care
– Other disease states (heart failure, stroke, e.g.)
– Other Indian states
• New information on how ACS affects health related quality of life and individual-/household-level costs
• ACS QUIK has the potential to contribute to the larger shift of evaluating the effect of cardiovascular quality improvement interventions using a stronger study design.
26
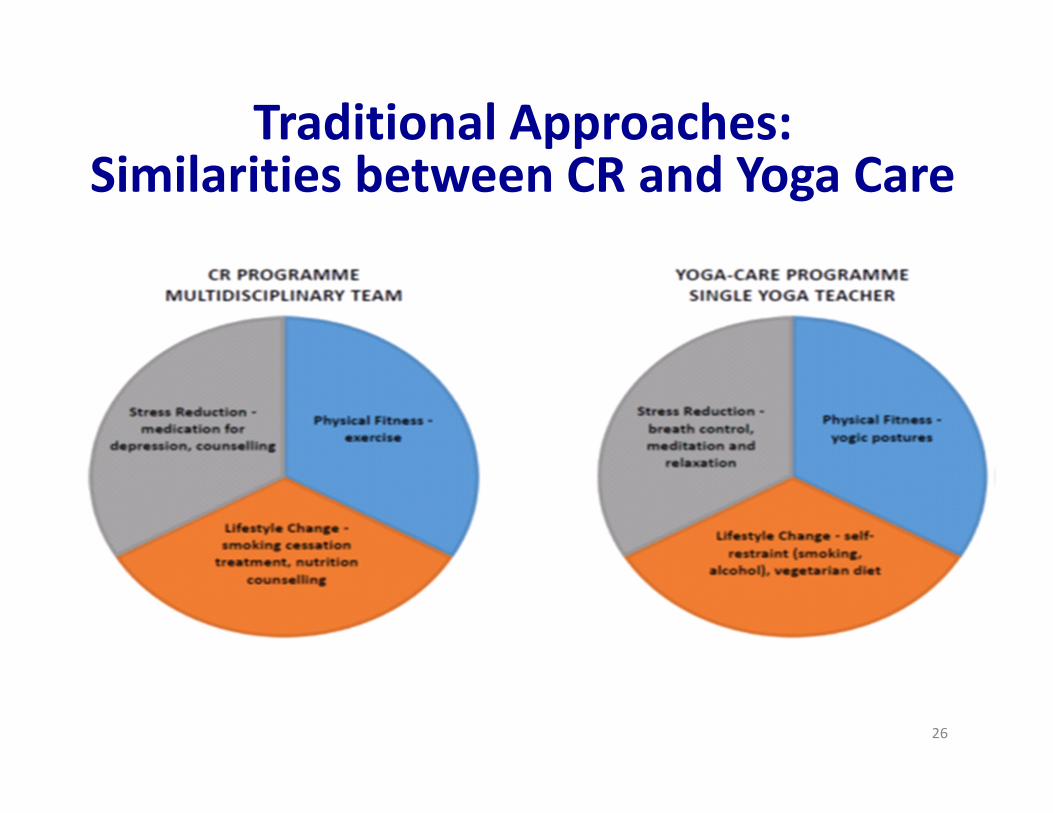
Traditional Approaches:Similarities between CR and Yoga Care

Using traditional approaches
• YogaCare Trial
• A clinical trial of yoga-based cardiac rehabilitation
programme on cardiovascular health in India
• Mechanistic study in UK
• 4000 patients from 16 hospitals in India
• Outcomes: Composite of death, MI & Stroke
? Yoga Care for Stroke/difficult to treat diabetes
? Yoga in palliative care of cancer patients
? Yoga in prevention of injuries particularly elderly

Increasing and improving Human
Resource capacity

Re education of Primary care
physicians
• On job Certificate courses
• Distance learning
• Innovative learning tools through case studies
and IT tools
• Creating networks for peer education
• 500000 primary care physicians in India: how
do we reach them?

Certificate Course in Evidence Based Diabetes
Management (CCEBDM)
•Objective: To develop core skills and competencies in primary care
physicians for the practice of evidence based diabetes
management and establish networks between primary care
physicians and existing specialized diabetes care centers in India.
• Key Features: 12 modular course, once a month contact session
on designated Sunday, executive on-job training, 1:10-12 class
ratio, latest and updated course curriculum taught by selected
regional Faculty.

SYNOPSIS OF CCEBDM CYCLE – I, II, III
Cycle I launched on 8th Aug, 2010
• 18 States, 57 Cities,
• 100 Centers
• 15 National Expert,
• 128 Regional Faculty, 61 Observers
• 1208 Participants
Cycle II launched on 11th Dec, 2011
• 19 States, 65 Cities,
• 119 Centers
• 15 National Expert,
• 149 Regional Faculty, 84 Observers
• 1568 Participants
Cycle III launched on 24th Feb, 2013
• 19 States, 73 Cities,
• 134 Centers
• 15 National Expert,
• 164 Regional Faculty
• 2306 Participants
Others
Advanced Certificate Course in Prevention and
Management of Diabetes & Cardiovascular Risk
Certificate Course in Hypertenison and Thyroid disorders
Certificate Course in GDM (~ 2500)

GIS Urban: Private Physicians
Private General
Physicians- 31

GIS Urban: RMPs
RMPs: 100
High SES
area
Multi Sectoral
Dialogue

Why and where do we need multi sectoral
action in improving healthcare
• Improve Surveillance system
– Use of tablets/phone for real time data gathering
– Using GIS for community hotspots of chronic diseases
• Improve diagnostics ( POCs for a range of diseases
with blue tooth and other technologies)
• Improve drugs: Polypill
• Improve drug availability and distribution ( e drug
facilities)
• Improve access: Virtual Polyclinic
• Integrating care within chronic Diseases and between
CD and other Diseases

“If you want something you have never had,
You must be willing to do something you have
never done”
Thomas Jefferson
A small group of thoughtful people could change the world.
Indeed, it's the only thing that ever has.
Margaret Mead
(Cultural anthropologist)