dear participant: helen hayes hospital offers three ...§ provide resistance for strengthening...
TRANSCRIPT
Dear Participant:
Helen Hayes Hospital offers three separate aquatic programs for people in the community.
The first program is the Helen Hayes Hospital Recreation Therapy Aquatic Exercise Program
(AEP). Prospective applicants must complete the Aquatics Questionnaire (attached). The
Aquatics Director will recommend a program of gentle exercises if needed. Participants will
exercise independently under lifeguard supervision. On request, the participant can bring an aide
to assist him/her in the water at no additional cost. However, the aide is there to assist the
participant and will not be able to do his or her own exercises. Due to our water temperature
of (92°-94°F), aerobic exercise programs are inappropriate and will not be permitted.
The second program is the Arthritis Foundation Aquatic Program (AFAP). Prospective
applicants must submit the Aquatics Questionnaire. Applicants will join a group and perform
gentle exercises developed by the Arthritis Foundation under the direction of a Certified Arthritis
Foundation Aquatic Leader/Instructor. Participants can bring an aide to assist with this program
as well, at no additional cost. However, as above, the aide is there to assist the participant and
will not be able to do his or her own exercises.
The third program is Ai Chi. Ai Chi is a simple water exercise and relaxation program performed
using a combination of deep breathing and slow, broad movements of arms, legs, and torso in
flowing continual patterns to promote relaxation and improve flexibility, balance and pain.
Under the guidance of a therapist, the Ai Chi postures or movements are practiced dynamically,
repeating the movement in rhythm with the breath.
The Helen Hayes Hospital Therapeutic Pool is a 25 x 60 foot warm water (92°-94°) pool
providing a flat floor divided into depth areas of 2 feet 9 inches, 4 feet and 5 feet. Platforms are
provided in the 5’ section bringing the floor bottom to 41/2 feet. The pool features two Arjo
hydraulic lifts with chairs and stretchers that detach from their undercarriages. These lifts slowly
swing out over the water and gently ease patients into the pool. Ambulatory patients are able to
access the pool from stairways fitted with handrails.
Howard A. Zucker, M.D., J.D.Acting Commissioner of Health
Aquatic Programs:
Participants experience body movement and control in ways that are not possible “on land”.
Warm water immersion, exercise and swimming can:
Χ Support body weight and lessen the effects of gravity
Χ Provide buoyancy and reduce weight-bearing stress on joints
Χ Promote deep breathing and cardiovascular endurance
Χ Increase circulation and promote healing
Χ Encourage relaxation
Χ Foster leisure/recreational skill development and socialization
Χ Promote perceptual-motor development and coordination
Χ Enhance self-concept and body image
Χ Provide resistance for strengthening exercises
Hospital policy requires that all individuals involved in our programs complete an Aquatic
Questionnaire.
If you have any further questions regarding the Helen Hayes Hospital therapeutic pool programs,
please do not hesitate to contact me at (845) 786-4457 or Eileen Andreassi, Director of
Recreational Therapy at (845) 786-4113. If neither of us is available at our extensions, please
leave a message.
Sincerely,
Alyssa A. Chagares, CTRS
Aquatics Director
Dear Community Participant:
Thank you for expressing interest in joining the Aquatics Program at Helen Hayes Hospital.
This program offers an Aquatic Exercise Program (AEP) and an Arthritis Foundation Aquatic
Program (AFAP).
The Aquatic Exercise Program (AEP) (independent exercise) is offered:
Mon., Wed. and Fri.: (9:00 am-10:00 am)(10:15am-11:15 am)(11:00 am-12:00 pm)
(12:15-1:15).
Tues. and Thurs.: (9:00 am-10:00 am)(10:15am-11:15 am)(11:00 am-12:00 pm)
(12:00pm-1:00pm)(4:45 pm-5:45 pm).
The Arthritis Foundation Aquatic Program (AFAP) (exercise w/group leader) is offered:
Tues. and Thurs.: (9:00 am-10:00 am), (11:00 am-12:00 pm), (12:00 pm-1:00 pm),
(4:45 pm-5:45 pm).
The Ai Chi class is offered:
Wednesdays (1:00-2:00).
1. Please read, fill out and sign all therapeutic pool enrollment forms, including your address
and 2 emergency contacts and either mail or bring them to the pool office. Please keep
one copy for yourself.
2. Upon acceptance into the program, you will receive notification of your session and time.
The fee is sixty dollars ($60.00) per month for 2 days a week, ninety dollars ($90.00) per
month for 3 days a week or thirty dollars ($30.00) per month for 1 day a week.
Participants have the option of paying on an annual basis at a rate of $660.00 (2x weekly)
or $990.00 (3x weekly), realizing a savings of $60.00 or $90.00 respectively. The Ai Chi
Class is $30.00 a month. Please be aware of the following if you choose to pay by the
year. We are unable to offer REFUNDS OR MAKE-UP CLASSES FOR ANY
REASON, including temporary illness, family needs, traveling out of town or re-location.
YOU MAY NOT PAY PER SESSION.
After the first payment, all subsequent payments must be submitted no later than the
15th of the month preceding the next month of participation.
Howard A. Zucker, M.D., J.D.Acting Commissioner of Health
-2-
3. All payments and completed payment forms must be put in an envelope and placed
in the locked mailbox in the Pool Office or mailed to Helen Hayes Hospital, Rt.
9W, West Haverstraw, N.Y. 10993, Attn. Pool.
4. NO CASH PAYMENTS ARE ACCEPTED.
Credit Card payments can be made using the back of the Aquatics Program Payment Receipt
form. Credit card payments will not be accepted verbally or over the phone. Your card
verification and signature are required. Please put your address on the front of the payment
form.
5. You will not receive a bill or a reminder phone call.
6. There is a $25.00 fee for a check returned for insufficient funds.
7. You are scheduled for only the session designated. Please come at least 15 minutes before
the scheduled time, as the program will begin and end on time. You must supply your
own bathing suit, towel and aquatic non-slip shoes.
We look forward to having you participate in our Aquatic Program. If you have any questions,
please call me at (845) 786-4457.
Sincerely yours,
Alyssa A. Chagares, CTRS
Aquatics Director
NAME:_________________________ DATE:___________
(Print)
HELEN HAYES HOSPITAL
West Haverstraw, New York 10993
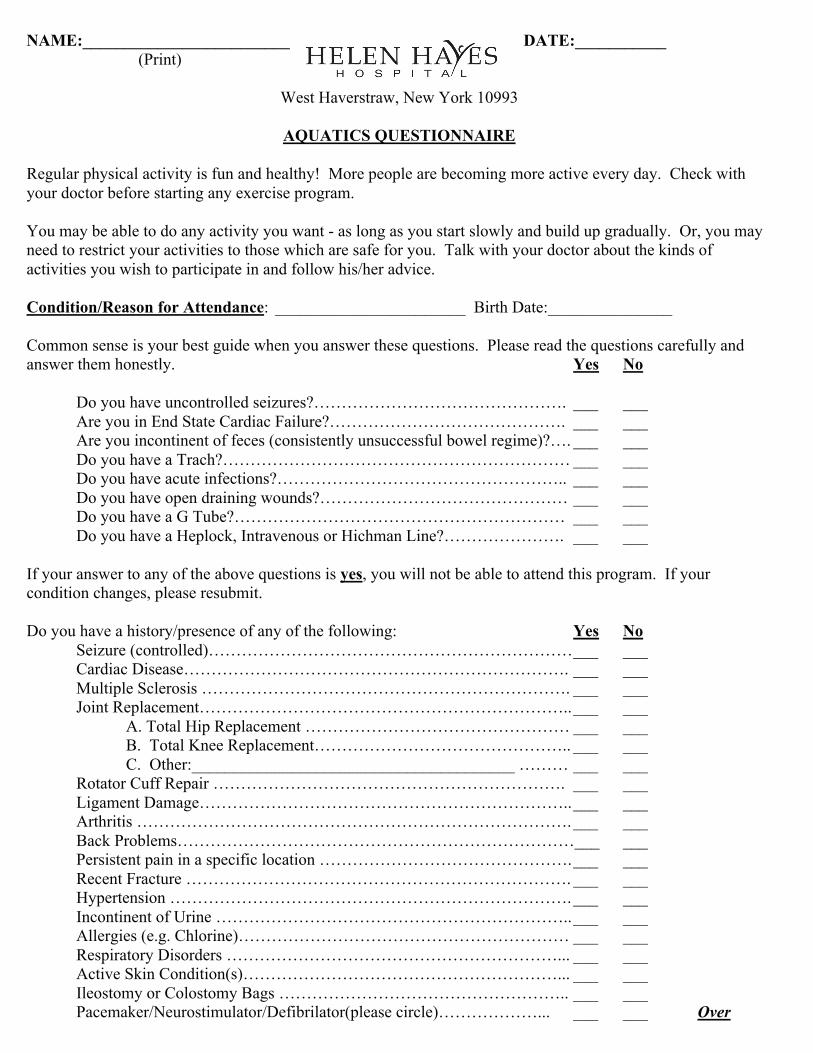
AQUATICS QUESTIONNAIRE
Regular physical activity is fun and healthy! More people are becoming more active every day. Check with
your doctor before starting any exercise program.
You may be able to do any activity you want - as long as you start slowly and build up gradually. Or, you may
need to restrict your activities to those which are safe for you. Talk with your doctor about the kinds of
activities you wish to participate in and follow his/her advice.
Condition/Reason for Attendance: _______________________ Birth Date:_______________
Common sense is your best guide when you answer these questions. Please read the questions carefully and
answer them honestly. Yes No
Do you have uncontrolled seizures?………………………………………. ___ ___
Are you in End State Cardiac Failure?……………………………………. ___ ___
Are you incontinent of feces (consistently unsuccessful bowel regime)?…. ___ ___
Do you have a Trach?……………………………………………………… ___ ___
Do you have acute infections?…………………………………………….. ___ ___
Do you have open draining wounds?……………………………………… ___ ___
Do you have a G Tube?…………………………………………………… ___ ___
Do you have a Heplock, Intravenous or Hichman Line?…………………. ___ ___
If your answer to any of the above questions is yes, you will not be able to attend this program. If your
condition changes, please resubmit.
Do you have a history/presence of any of the following: Yes No
Seizure (controlled)………………………………………………………… ___ ___
Cardiac Disease……………………………………………………………. ___ ___
Multiple Sclerosis …………………………………………………………. ___ ___
Joint Replacement………………………………………………………….. ___ ___
A. Total Hip Replacement ………………………………………… ___ ___
B. Total Knee Replacement……………………………………….. ___ ___
C. Other:_______________________________________ ……… ___ ___
Rotator Cuff Repair ………………………………………………………. ___ ___
Ligament Damage………………………………………………………….. ___ ___
Arthritis ……………………………………………………………………. ___ ___
Back Problems………………………………………………………………___ ___
Persistent pain in a specific location ………………………………………. ___ ___
Recent Fracture ……………………………………………………………. ___ ___
Hypertension ………………………………………………………………. ___ ___
Incontinent of Urine ……………………………………………………….. ___ ___
Allergies (e.g. Chlorine)…………………………………………………… ___ ___
Respiratory Disorders ……………………………………………………... ___ ___
Active Skin Condition(s)…………………………………………………... ___ ___
Ileostomy or Colostomy Bags …………………………………………….. ___ ___
Pacemaker/Neurostimulator/Defibrilator(please circle)………………... ___ ___ Over
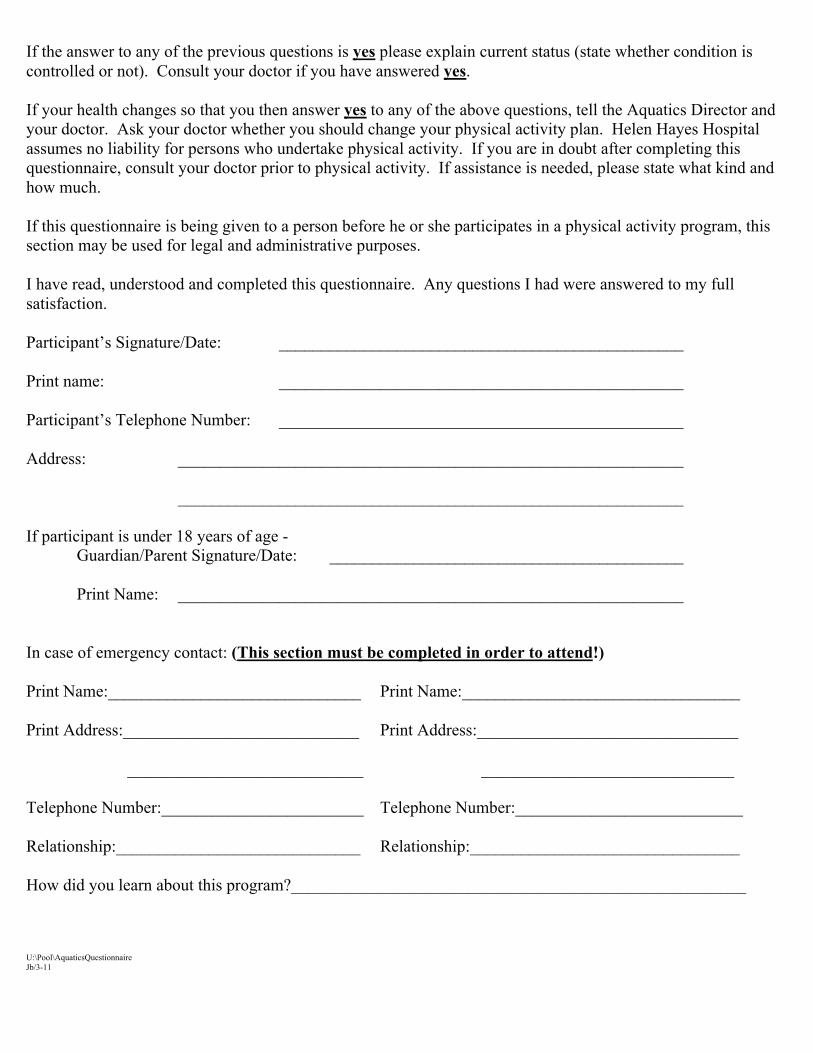
If the answer to any of the previous questions is yes please explain current status (state whether condition is
controlled or not). Consult your doctor if you have answered yes.
If your health changes so that you then answer yes to any of the above questions, tell the Aquatics Director and
your doctor. Ask your doctor whether you should change your physical activity plan. Helen Hayes Hospital
assumes no liability for persons who undertake physical activity. If you are in doubt after completing this
questionnaire, consult your doctor prior to physical activity. If assistance is needed, please state what kind and
how much.
If this questionnaire is being given to a person before he or she participates in a physical activity program, this
section may be used for legal and administrative purposes.
I have read, understood and completed this questionnaire. Any questions I had were answered to my full
satisfaction.
Participant’s Signature/Date: ________________________________________________
Print name: ________________________________________________
Participant’s Telephone Number: ________________________________________________
Address: ____________________________________________________________
____________________________________________________________
If participant is under 18 years of age -
Guardian/Parent Signature/Date: __________________________________________
Print Name: ____________________________________________________________
In case of emergency contact: (This section must be completed in order to attend!)
Print Name:______________________________ Print Name:_________________________________
Print Address:____________________________ Print Address:_______________________________
____________________________ ______________________________
Telephone Number:________________________ Telephone Number:___________________________
Relationship:_____________________________ Relationship:________________________________
How did you learn about this program?______________________________________________________
U:\Pool\AquaticsQuestionnaire
Jb/3-11
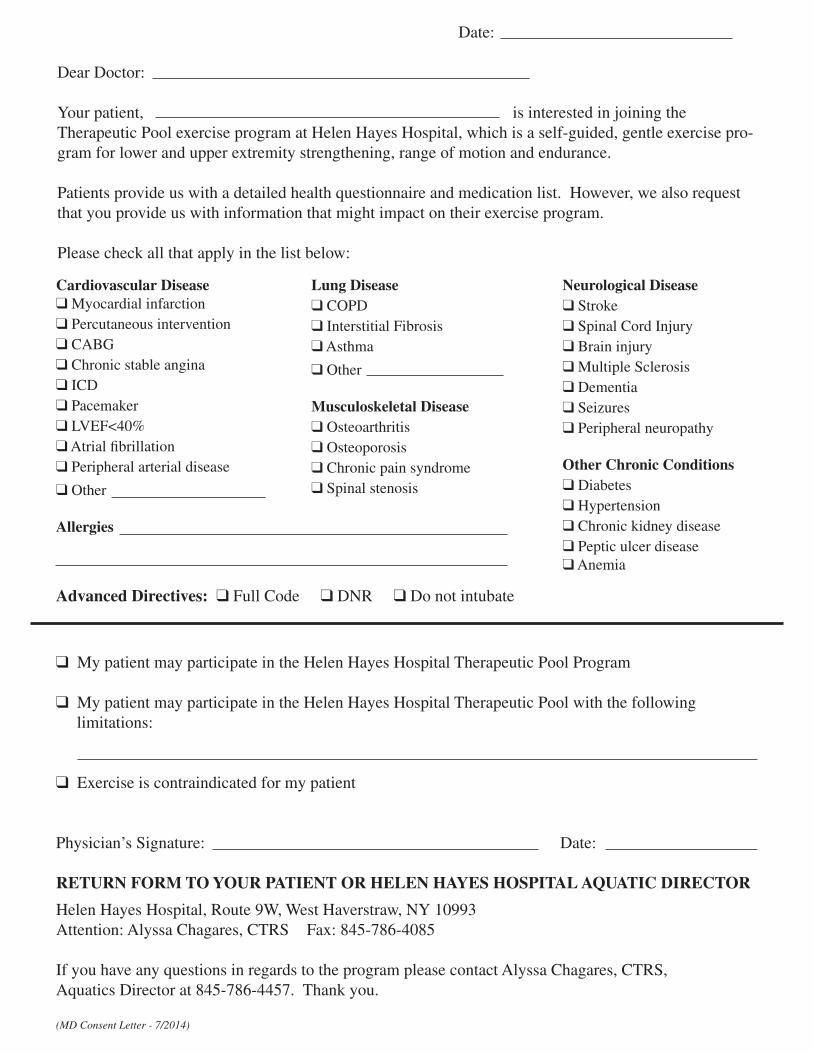
Date:
Dear Doctor: Your patient, is interested in joining the Therapeutic Pool exercise program at Helen Hayes Hospital, which is a self-guided, gentle exercise pro-gram for lower and upper extremity strengthening, range of motion and endurance.
Patients provide us with a detailed health questionnaire and medication list. However, we also request that you provide us with information that might impact on their exercise program.
Please check all that apply in the list below:
Cardiovascular Disease q Myocardial infarctionq Percutaneous interventionq CABGq Chronic stable anginaq ICDq Pacemakerq LVEF<40%q Atrial fibrillationq Peripheral arterial disease
q Other
Allergies
Lung Diseaseq COPDq Interstitial Fibrosisq Asthma
q Other
Musculoskeletal Diseaseq Osteoarthritisq Osteoporosisq Chronic pain syndromeq Spinal stenosis
Neurological Diseaseq Strokeq Spinal Cord Injuryq Brain injuryq Multiple Sclerosisq Dementiaq Seizuresq Peripheral neuropathy
Other Chronic Conditionsq Diabetesq Hypertensionq Chronic kidney diseaseq Peptic ulcer diseaseq Anemia
q My patient may participate in the Helen Hayes Hospital Therapeutic Pool Program
q My patient may participate in the Helen Hayes Hospital Therapeutic Pool with the following limitations:
q Exercise is contraindicated for my patient
Physician’s Signature: Date:
RETURN FORM TO YOUR PATIENT OR HELEN HAYES HOSPITAL AQUATIC DIRECTOR
Helen Hayes Hospital, Route 9W, West Haverstraw, NY 10993Attention: Alyssa Chagares, CTRS Fax: 845-786-4085
If you have any questions in regards to the program please contact Alyssa Chagares, CTRS, Aquatics Director at 845-786-4457. Thank you.
(MD Consent Letter - 7/2014)
Advanced Directives: q Full Code q DNR q Do not intubate
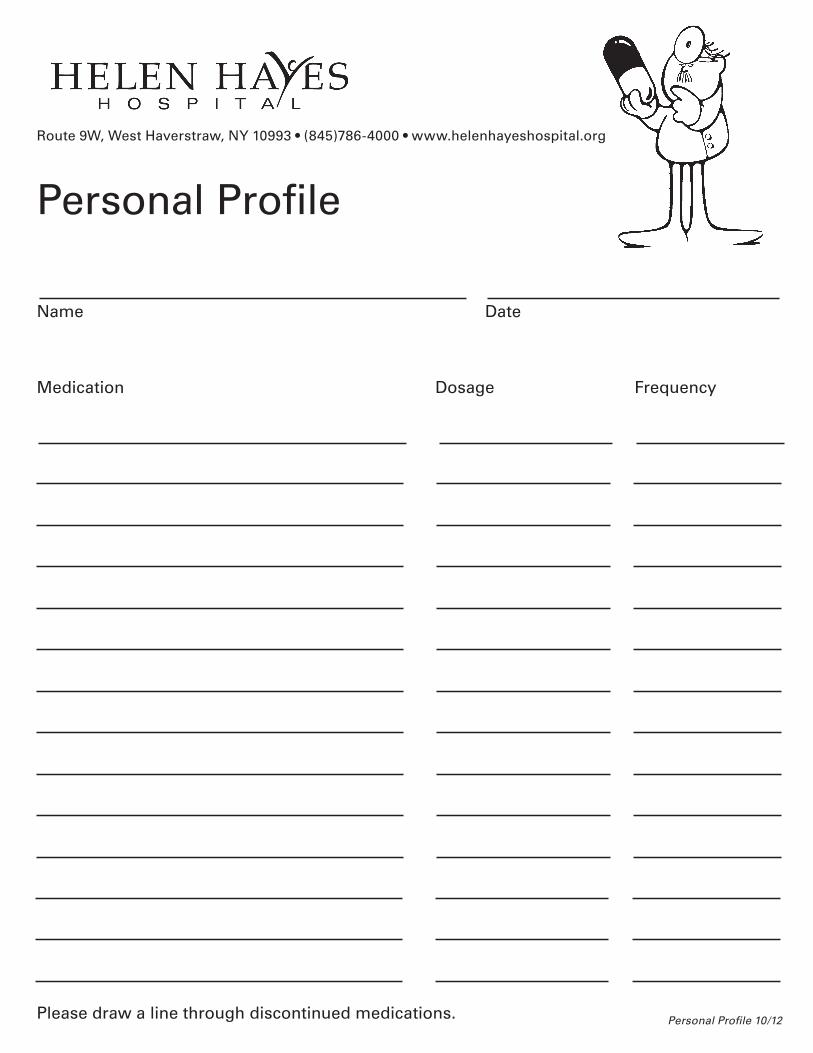
Route 9W, West Haverstraw, NY 10993 • (845)786-4000 • www.helenhayeshospital.org
Personal Profile
Name Date
Medication Dosage Frequency
Please draw a line through discontinued medications. Personal Profile 10/12
RETURN TO POOL STAFF
HELEN HAYES HOSPITAL
WEST HAVERSTRAW, NEW YORK 10993
AQUATIC EXERCISE PROGRAM
PARTICIPANT AGREEMENT
This agreement is made with (Participant)_________________________ Date:______________.
It includes the terms and conditions for participation in the Helen Hayes Hospital Therapeutic
Exercise Program as follows:
I. Attendance:
I understand that I:
A. must be consistent in my attendance and notify the aquatics director as soon as
able if I will be under medical care resulting in missing multiple sessions;
B. must be on time for each session-early or late arrivals cannot be accommodated.
C. must only attend the session I signed up for w/ the Aquatics Director;
D. The fee is NOT pro-rated for missed classes;
E. There are NO refunds of any payment.
F. There are NO make up sessions available.
II. Bathing Attire, Valuables and Shower Room Practices
A. I will bring my own bathing suit, towel and non-slip pool shoes to each session.
B. I understand that if I am incontinent of urine I must supply and wear a diaper and
rubber pants under my bathing suit. (If incontinent of feces-cannot participate
unless on bowel regimen that is working).
C. I understand that I must bring someone to assist me if I am not independent in
dressing/undressing. (There will be no one available to assist me in the shower
room).
D. I will not disrobe or remove my bathing suit in the shower area or general locker
room areas. Curtained areas have been provided for changing.
F. I am responsible for my valuables. There are lockers available for my use on
which I can put my own lock. I must remove the lock before I leave. (Helen
Hayes Hospital staff will remove any locks left on after a session has ended).
G. I will wear non-slip pool shoes at all times on the deck, in the pool and in the
locker rooms.
III. Pool Rules
A. I understand that I must abide by the Helen Hayes Hospital therapeutic pool rules
(see attached) at all times. If I fail to abide by the rules, my right to participate in
this program will be jeopardized.
B. I understand that I can only use pool equipment assigned by the therapist.
C. I understand that anyone I bring with me will wear shoe cover-ups, before
entering the pool area and remain seated during the session.
-2-
IV. Medical Status
A. I understand that I must complete an Aquatics Questionnaire (attached) before
attending an aquatics program.
B. I understand that, if I have any open draining wounds, I will not be able to go into
the pool.
C. I understand that I am responsible for ensuring that Helen Hayes Hospital is
informed of any medical problems which may impact on this program. I am also
responsible for informing Helen Hayes Hospital of any medical problems which
arise after my referral has been signed and reviewed. Failure to inform Helen
Hayes Hospital will lead to my privileges being revoked.
V. Payment Agreement
A. All payments are due by the 15th
of the month for the following month. You will
not receive a bill. If payment has not been received by that time, we will assume
that you are not returning and another participant may be assigned to your class
slot. Payments will not be accepted after the 25th
of the month for the following
month.
B. Pool participants must call the Aquatics Director at (845) 786-4457 before
returning after an absence of one month or more. Pool participants should not
assume that they will be able to return to the same class if their participation has
been interrupted.
I agree to participate in the Helen Hayes Hospital Aquatic Exercise Program to the best of my
ability and agree to my responsibilities as outlined above.
Participant Signature:____________________________________________________________
Participant Name:___________________________________Date:________________________
(Please Print)
Aquatic Director:____________________________________Date:_______________________
******************************************************************************
EA 4/25/13
KEEP FOR YOUR RECORDS
HELEN HAYES HOSPITAL
WEST HAVERSTRAW, NEW YORK 10993
AQUATIC EXERCISE PROGRAM
PARTICIPANT AGREEMENT
This agreement is made with (Participant)_________________________ Date:______________.
It includes the terms and conditions for participation in the Helen Hayes Hospital Therapeutic
Exercise Program as follows:
I. Attendance:
I understand that I:
A. must be consistent in my attendance and notify the aquatics director as soon as
able if I will be under medical care resulting in missing multiple sessions;
B. must be on time for each session-early or late arrivals cannot be accommodated.
C. must only attend the session I signed up for w/ the Aquatics Director;
D. The fee is NOT pro-rated for missed classes;
E. There are NO refunds of any payment.
F. There are NO make up sessions available.
II. Bathing Attire, Valuables and Shower Room Practices
A. I will bring my own bathing suit, towel and non-slip pool shoes to each session.
B. I understand that if I am incontinent of urine I must supply and wear a diaper and
rubber pants under my bathing suit. (If incontinent of feces-cannot participate
unless on bowel regimen that is working).
C. I understand that I must bring someone to assist me if I am not independent in
dressing/undressing. (There will be no one available to assist me in the shower
room).
D. I will not disrobe or remove my bathing suit in the shower area or general locker
room areas. Curtained areas have been provided for changing.
F. I am responsible for my valuables. There are lockers available for my use on
which I can put my own lock. I must remove the lock before I leave. (Helen
Hayes Hospital staff will remove any locks left on after a session has ended).
G. I will wear non-slip pool shoes at all times on the deck, in the pool and in the
locker rooms.
III. Pool Rules
A. I understand that I must abide by the Helen Hayes Hospital therapeutic pool rules
(see attached) at all times. If I fail to abide by the rules, my right to participate in
this program will be jeopardized.
B. I understand that I can only use pool equipment assigned by the therapist.
C. I understand that anyone I bring with me will wear shoe cover-ups, before
entering the pool area and remain seated during the session.
-2-
IV. Medical Status
A. I understand that I must complete an Aquatics Questionnaire (attached) before
attending an aquatics program.
B. I understand that, if I have any open draining wounds, I will not be able to go into
the pool.
C. I understand that I am responsible for ensuring that Helen Hayes Hospital is
informed of any medical problems which may impact on this program. I am also
responsible for informing Helen Hayes Hospital of any medical problems which
arise after my referral has been signed and reviewed. Failure to inform Helen
Hayes Hospital will lead to my privileges being revoked.
V. Payment Agreement
A. All payments are due by the 15th
of the month for the following month. You will
not receive a bill. If payment has not been received by that time, we will assume
that you are not returning and another participant may be assigned to your class
slot. Payments will not be accepted after the 25th
of the month for the following
month.
B. Pool participants must call the Aquatics Director at (845) 786-4457 before
returning after an absence of one month or more. Pool participants should not
assume that they will be able to return to the same class if their participation has
been interrupted.
I agree to participate in the Helen Hayes Hospital Aquatic Exercise Program to the best of my
ability and agree to my responsibilities as outlined above.
Participant Signature:____________________________________________________________
Participant Name:___________________________________Date:________________________
(Please Print)
Aquatic Director:____________________________________Date:_______________________
******************************************************************************
EA 4/25/13
1. Lifeguard must be present whenever the pool is in use.
2. No diving.
3. No jumping.
4. Health Department rules for sanitation and safety must be observed by every patron. Persons with physical disorders such as skin lesions, inflamed eyes, nose, mouth or ear discharges, or bandages may not swim. Spitting and other discharges into the pool is prohibited.
5. Maximum number of bathers permitted: 50
6. No running on the deck.
7. No food or drink in the pool area or locker rooms.
8. No glass in the pool area.
9. Only persons in proper bathing attire permitted in the pool. No cut-offs or rolled-up pants. No street clothes in the pool area.
10. No bare feet outside the pool deck and dressing area.
11. No personal hairdryers.
12. No gum chewing in the pool area or locker rooms.
13. Non-slip pool shoes must be worn in and out of pool and into locker rooms.
14. No cell phones.
Therapeutic Swimming Pool
~ RULES ~
Pool Rules 3/07