debility, failure to thrive, and other diagnosis reporting ... · pdf filedebility, failure to...
TRANSCRIPT

Debility, Failure to Thrive, and
other Diagnosis Reporting
Dilemmas
Janet Bull, MD FAAHPM

Faculty Disclosure
It is the policy of the Oregon Hospice Association to insure balance,
independence, objectivity, and scientific rigor in all its educational programs. All
faculty participating in any Oregon Hospice Association sponsored programs are
expected to disclose to the program audience any real or apparent affiliation(s)
that may have a direct bearing on the subject matter of the continuing education
program. This pertains to relationships with pharmaceutical companies,
biomedical device manufacturers, or other corporations whose products or
services are related to the subject matter of the presentation topic. The intent of
this policy is not to prevent a speaker from making a presentation. It is merely
intended that any relationships should be identified openly so that the listeners
may form their own judgments about the presentation with the full disclosure of
the facts.
The presenter has nothing to disclose.

Disclosures
Bull:
• Salix Pharmaceuticals – scientific advisory
board/speakers bureau
• No relevant conflict of interests

Objectives
o Understand the current political scene
and what’s driving the change
o Describe coding issues with debility
and failure to thrive
o Review elements of ICD-9 CM coding
guidelines
o Identify related and unrelated
treatments

Why Now?
o Hot topics
Growth in hospice
Increased spending in hospice
Heightened regulatory landscape
Fraud and Abuse cases increasing
Part D and hospice medications
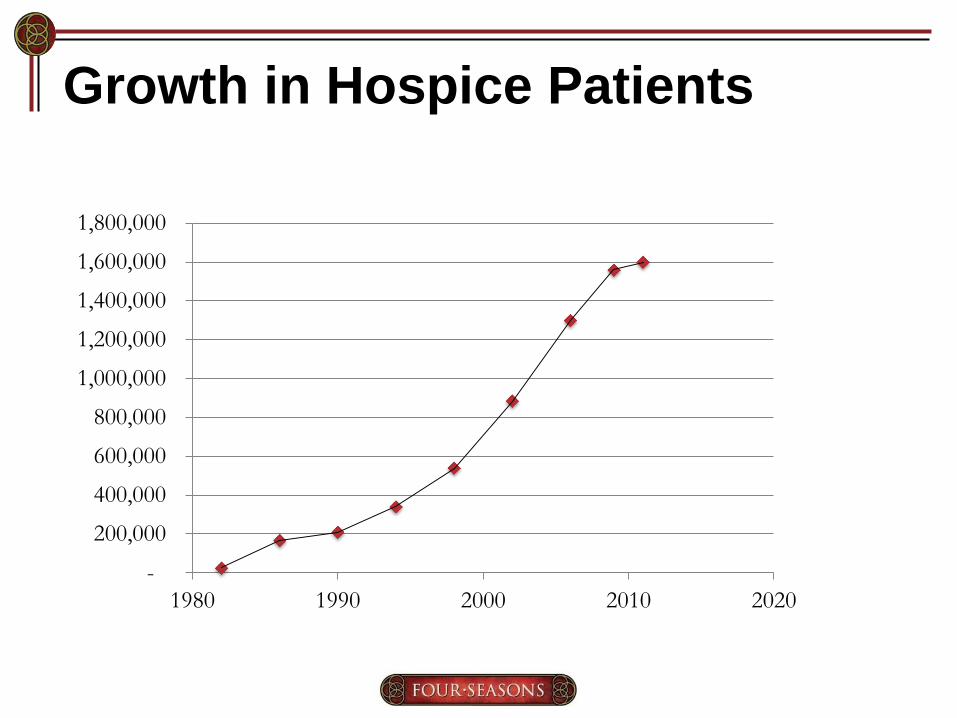
Growth in Hospice Patients
-
200,000
400,000
600,000
800,000
1,000,000
1,200,000
1,400,000
1,600,000
1,800,000
1980 1990 2000 2010 2020

FP vs NFP Medicare Certified
o 3679 providers
o 60% for profit
o Profit status has changed

Medicare Spending in Hospice
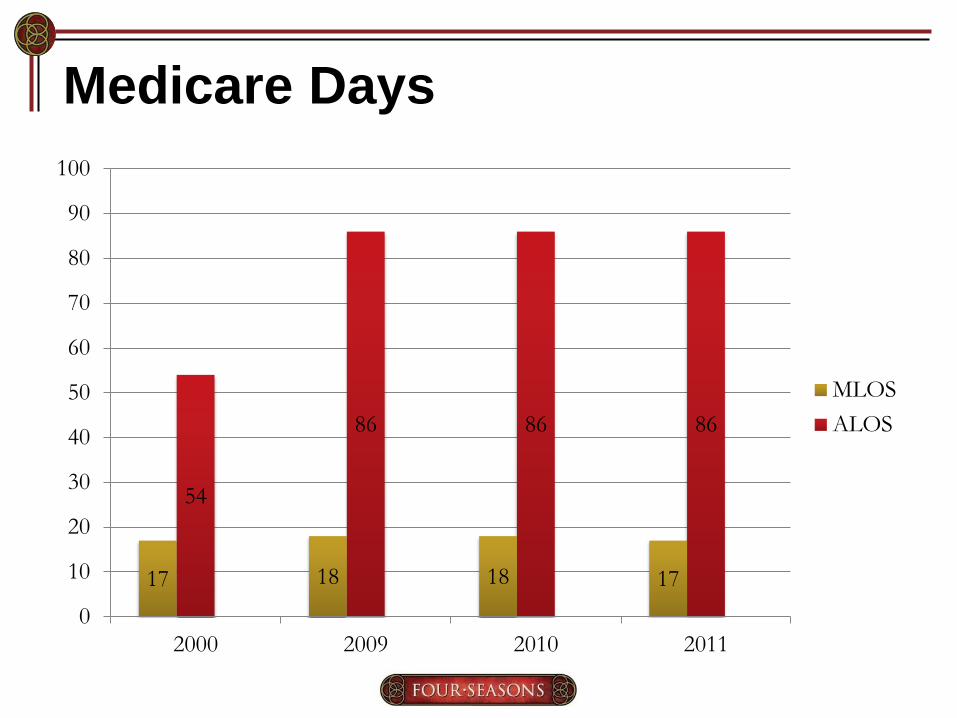
Medicare Days
17 18 18 17
54
86 86 86
0
10
20
30
40
50
60
70
80
90
100
2000 2009 2010 2011
MLOS
ALOS

Trends in Hospice Services
Year 2000 2012
# Beneficiaries 513,000 1,300,000
Medicare Costs 2,900,000 1,470,000
ALOS 54 86 (2010)
General Inpatient Level Care
o OIG 2011 report
• 2% all care GIP
• 8% hospice funding 1.2 billion dollars
• 27% hospices provided no GIP
• ALOS – 6.2 days, 11% >10 days 2% > 3
weeks
• Long LOS > 5 days
OEI-02-10-00490.

What’s the Buzz?
o Final Rule – Wage Index Report
• Issues with Diagnosis
Secondary Diagnosis
Debility/FTT
Dementia
Related vs Unrelated Meds
• Hospice Item Set – Quality Reporting
• Payment Reform
• Update on payment reform
Federal Registry 8/7/2013

Diagnosis on Hospice Claims
o Clarification of existing guidelines
o July 27, 2012 Wage Index report – “we
provided in-depth information
regarding longstanding, existing ICD-9
coding guidelines.”
o CMS looked at 3 quarters - little use of
secondary or related diagnosis –
initially 77% of all claims had just one
diagnosis

Secondary Diagnosis Wanted!
72% providers
Only report primary diagnosis
“The reporting of only one principal diagnosis does not lend to a
comprehensive, holistic, and accurate description of the
beneficiaries’ end-of-life conditions and may not fully reflect the
individualized needs in the individual’s required hospice plan of
care.”

Secondary Diagnosis
o Paper UC-04 claim – allows 17 dx
o 83714010 electronic claim – 24 dx
o CMS expects hospices to use
secondary dx
If you are not using secondary diagnosis,
need to start!

Use of Nonspecific Symptom Codes
o Cannot use any “ill defined diagnosis”
as a principle diagnosis (780-799)
o Can no longer use debility and FTT -
MACs will soon be instructed to return
claims for more definitive diagnosis,
RTP by Oct 1, 2014
o ICD-9-CM does not allow use of
nonspecific codes as principal
diagnosis

Debility & Failure to Thrive
12%
9%
6%
7%
6%
3%
0%
2%
4%
6%
8%
10%
12%
14%
2012 2007 2002
Debility
AFTT

Top Ten Principal Hospice
Diagnosis
0
20,000
40,000
60,000
80,000
100,000
120,000
140,000
160,000
180,000
Debility Lung Cancer AFTT CHF COPD Alzheimer'sDz
SenileDementia
Heart Dz CVA/Stroke Dementia inoth Dz w/o
Beh Dist.
Top Ten Principal Hospice Diagnosis 2012
2012

Debility and FTT
“Debility and FTT are not appropriate principal
diagnoses in the terminally ill population as these
diagnoses are incongruous to the comprehensive
nature of the hospice assessment, the specific,
individualized hospice plan of care and the hospice
services provided. CMS is aware that diagnosing
diseases is not always a perfect science but the
expectation is that based on the comprehensive
hospice assessment, the certifying physicians are
using their best clinical judgment in determining the
principal diagnosis and related conditions”
CMS proposal 5/2013
Furthermore….
o Growth in use of these codes – 20% of
all hospice diagnosis
o No distinguishing between Debility and
Failure to Thrive in claims

What’s the Difference?
Debility FTT
PPS < 70% ≤ 30%
BMI No requirement ≤ 21
ADLs Dependent < 2 No requirement

Medicare Claims with Debility/FTT
o 50% had ≥ 7 chronic conditions
o 75% had ≥ 4 chronic conditions
o Chronic Condition Data Warehouse

Debility/FTT Claims – no secondary dx
Associated Diagnosis % of Beneficiaries
Anemia 76
Alzheimer's or Senile Dementia 66
Rheumatoid Arthritis or Osteoarthritis 66
Ischemic Heart Disease 63
Depression 55
Heart Failure 53
Chronic Kidney Disease 43
COPD/Bronchiectasis 39
Osteoporosis 39
Stroke 34
Atrial Fibrillation 28
Hip Fracture 20
2012 chronic conditions warehouse

Example 1
Ms Doubtfire is in her second benefit
period. She was admitted with a diagnosis
of debility. Comorbidities are NYHC 3
disease, COPD, and mild dementia. Her
BMI is 18. PPS 50%. The attending feels
prognosis < 6 months
Should you discharge this patient?
Does she meet a specific LCD?
Should you change her diagnosis? If so, what?

It depends…….
o Cardiac or COPD – principle dx
(whichever you feel is more contributory)
o Secondary – comorbid that’s also
impacting prognosis
o Debility/FTT – should be used as
secondary diagnosis
o Pay for all meds, supplies, treatments
related to above conditions

Choosing Diagnosis
“It is often not a single
diagnosis that represents the
terminal illness of the patient,
but the combined effect of
several conditions that makes
the patient’s condition
terminal.”

Do not discharge if appropriate..
“CMS does not expect that these coding
clarifications will create any limitations or
barriers to accessing Medicare hospice
services by eligible Medicare beneficiaries as
coding on claims occurs after the beneficiary
has elected and accessed hospice services. In
fact, adherence to the ICD-9-CM coding
guidelines should promote access to
appropriate and comprehensive hospice
services.”

Example 2
o 94 yo WF with mild dementia,
osteoporosis, and hypothyroidism. She
has been to the ER for falls x 3,
sustained a wrist fracture. PPS 60 to
40%, weight loss of 10 pounds with BMI
of 19. Only eating 20%, 3/6 ADLs.
Do you admit?
If so, diagnosis, principal dx?
Secondary dx?
Verified by one of the MACS
o Principal Dx – Osteoporosis
o Secondary Dx – Wrist fracture, FTT
o What about Dementia?
Hypothryoidism?
This question was posed to one of the
MACS who confirmed osteoporosis as
principal dx

Example 3
o An 85 year old patient with dysphagia,
decreased oral intake, malnutrition,
weight loss, BMI of 18.6 upon
admission, decreasing functional
status, progressed from a walker to
chair to bed in less than six months,
but with no underlying diagnoses.

How to Code?
o Malnutrition – 263.9
o Dysphagia – 787.20
o Muscle weakness – 728.87
This example given in the Final Rule.
Only use ill defined if NO other principal
diagnosis relevant

Coding Guidelines
o Malnutrition
o Abnormal weight loss
“According to ICD 9 Coding Guidelines, codes that fall
under the classification “Symptoms, Signs, and other
Ill-defined Conditions”, such as “debility” and “adult
failure to thrive”, can only be used as a principal
diagnosis when a related definitive diagnosis has not
been established or confirmed by the provider.”
Answer to question posed in Final Rule

But wait! – haven’t the MACs
encouraged use of FTT/Debility?
o Palmetto MAC – specific LCD on FTT
o Furthermore they state In the event a beneficiary presenting with a
nutritional impairment and disability does not meet
the medical criteria listed above, but is still thought
to be eligible for the Medicare Hospice Benefit, an
alternate diagnosis that best describes the clinical
circumstances of the individual beneficiary should
be selected (e.g. 783.21 "abnormal loss of weight"
and 799.4 "Cachexia”)
http://www.cms.gov/medicare-coverage-database/details/lcd-details.aspx

What about NGS?
o Decline in clinical status
o PPS <70% 2/6 ADL dependence
o NGS - Contractors will not make any
changes to the edits until we receive
direction from CMS in the form of the
Change Release
Published: May 30, 2013

Recommendations o NHPCO suggests that providers proactively
review new admissions and patients at
recertification with diagnoses of debility or
adult failure to thrive and consider options for
other diagnoses that will conform to the ICD-9-
CM Coding Guidelines for primary diagnosis. (NewsBriefs – 5/23/13)
o NAHC strongly encourages hospice providers
to ensure they are including all related
diagnoses on their claims and that they are
following all ICD-9-CM coding guidelines and
sequencing rules now (Newsletter 5/10/13)

New Patient Admissions
o Avoid ill defined primary diagnosis if at all
possible
o Use LCDs for guidance
o Include ALL diagnosis affecting prognosis
on claim form
o Medication profile may be helpful in
determining diagnosis
o Narratives should reflect WHY you are
admitting this patient. If patient does not
meet LCDs then explain what is causing the
< 6 month prognosis

Existing Debility/FTT Patients
o Physician – review plan of care and note affected bodily systems, symptoms, and medications
o Change to more appropriate diagnosis based on above with use of multiple secondary diagnosis to support
o Write order to change diagnosis and document reason for change
o Adjust medications covered

Comprehensive Assessment
o Determined by the IDG
o Related and unrelated diagnosis
incorporated into plan of care
o Should be an ongoing process when
new diagnosis are added
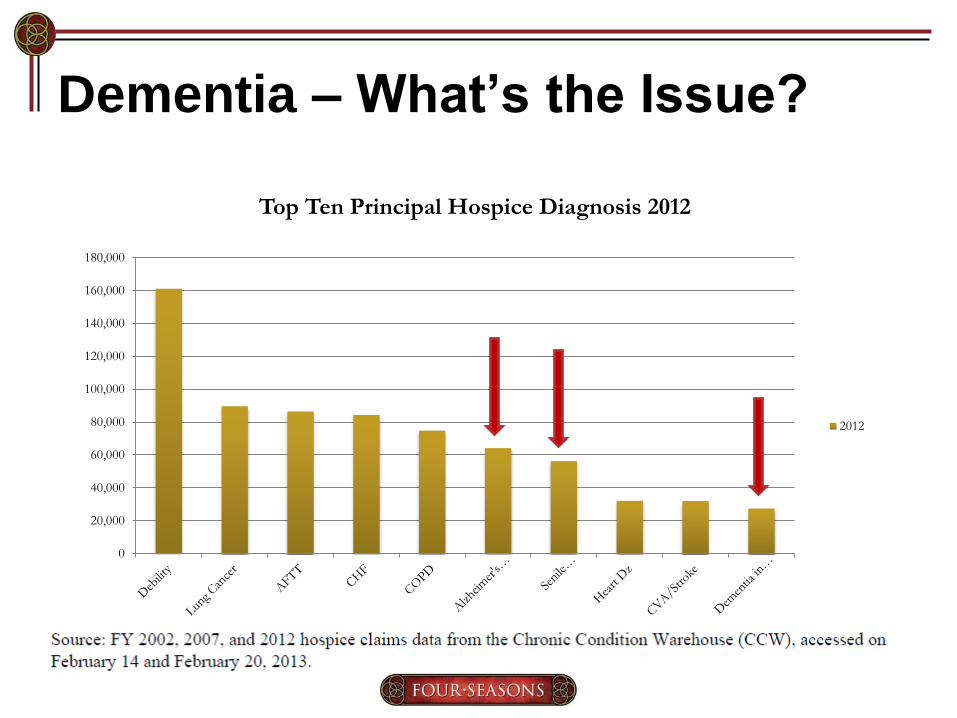
Dementia – What’s the Issue?
0
20,000
40,000
60,000
80,000
100,000
120,000
140,000
160,000
180,000
Top Ten Principal Hospice Diagnosis 2012
2012
Dementia
o Issue relates to inappropriate coding
o Alzheimer’s - 331
o Senile – 290.0
o Vascular – 290.4
o Follow ICD 9 codes for diagnosis and
sequencing rules. Do not use
manifestation codes – “in diseases
classified elsewhere”

Manifestation Codes
o Manifestations are characteristics,
signs or symptoms of an illness. When
one disease or condition causes
another disease or condition, the one
that caused it is the etiology and the
resulting second condition is the
manifestation.
o Manifestation codes cannot be
principal diagnosis

Other Dementias
Medical Codes
• Senile degeneration
of the brain – 331.2
• Frontotemporal
dementia – 331.19
• Dementia with Lewy
Body – 331.82
• Late effects of CVD
– 438
Psychiatric Codes
• Senile dementia – 290
• Dementia with
behaviors – 294.11
• Senile dementia with
delusions – 290.20

Manifestation Example 1
o Patient referred for vascular dementia –
history of CVAs, hypertension, and
peripheral vascular disease.
• Principal Diagnosis - Cerebral
atherosclerosis - 437.0 or Late Effects of
Cerebrovascular Disease - 438
• Secondary Diagnosis – Vascular Dementia
– 290.4
Palmetto used this example in their last
coalition meeting

Manifestation Code Example 2
Mr. G is a 69yo BM on dialysis with
ESRD. Renal failure is secondary to
longstanding type I diabetes. What do
you use as your principal diagnosis?
A. Diabetes, secondary ESRD
B. ESRD, secondary diabetes
C. ESRD, no secondary diagnosis

Cause of Renal Failure?
ICD-9 Guidelines
o Diabetes – primary 250.40
o ESRD – secondary 585.6
ESRD is a manifestation of diabetes.
ICD-9 codes states you need to list the
etiology as principal diagnosis and
follow the proper sequencing rules

Here’s the Confusion... o According to CMS claims manual, “the
principal diagnosis is defined as the
condition established after study to be
chiefly responsible for the patient’s
admission”
o But the manual also says to follow ICD -9
coding guidelines.
o Hospices generally list ESRD is the cause
for the patients limited prognosis and use
the LCD to support

What does CMS say?
o Use ICD 9 guidelines
o Hence in this case you would pay for
the insulin/diabetes care and renal
medications

What’s the Impact?
o Medication and treatment costs likely
to rise as more diagnosis are captured
as secondary
o Required to pay for all primary and
secondary diagnosis

Matching Hospital to Hospice Dx
o Examined patients who were
discharged from the hospital to
hospice and found about 20% time the
diagnoses did not match
o Examples given in cancer patients
o Should the principal hospice dx
conform to Uniform Hospital Discharge
Data Set (UHDDS)?

Here’s an example….
Patient with stage IV lung cancer
admitted to the hospital with dyspnea,
hypoxia, and increased weakness. On
discharge, admitted into hospice – lung
cancer not principle diagnosis in about
20% of these admissions.
Why is this occurring?

Matching to Hospital Diagnosis
o “Guidelines specify that the
circumstances of an inpatient hospital
admission diagnosis are to be used in
determining the selection of a principal
diagnosis”
o Final Rule – Federal Registry 8/7/13

Proper Coding
o HMD/staff physicians – understand
basics – buy ICD manual
o Do not use manifestation codes
o Follow proper sequencing
o Do not use mental codes 290-319
o Do not use ill defined dx 780-799
o Be as specific as you can in explaining
diagnosis so coders can code
accurately

Related VS Unrelated
It is our general view that … “hospices are required to provide virtually all the care that is needed by terminally ill patients” (48 FR 56010 through 56011). Therefore, unless there is clear evidence that a condition is unrelated to the terminal illness, all services would be considered related. It is also the responsibility of the hospice physician to document why a patient’s medical need(s) would be unrelated to the terminal illness prognosis.

Related Treatments
o Unless clear evidence that a condition
is unrelated to the terminal illness, all
services would be considered related.
o Physician needs to justify why a
diagnosis is not being covered!
o Must be documented!

Case Study
Admissions team gets a referral on Mr. L for
debility. (referral source uninformed)
o NYHA III, EF = 25%, maximally treated
o Atrial Fibrillation
o COPD moderate-severe FEV1 = 35%
o Alzheimer’s FAST 6 dementia
o 10 pound wt loss BMI = 17, albumin 2.7
o Glaucoma
o Admit under cardiac, COPD, or dementia?
o What are your secondary diagnosis?

Physician Fills Out – IDG Process
Diagnosis Related to
Prognosis
Yes or No
If no, why? ICD 9 Code
Coder to fill out
Principal Dx Heart
Failure
Y
Atrial fibrillation Y
COPD Y
Alzheimer's
?
Physician needs to
justify why if not
related
Debility Y
Malnutrition Y
Glaucoma N Does not affect
prognosis

Case Study Continued….
o Ms. L currently taking furosemide,
metoprolol, digoxin, donepezil,
memantine, tiotropium, fluticasone +
salmeterol (advair), coumadin, and
oxygen, eye drops Covered meds
include:
1. Cardiac meds and oxygen
2. Cardiac, pulmonary meds, and oxygen
3. All meds except eye drops and oxygen

Determining Covered Medications
o Principle: Heart failure – 428.0
o Secondary: Atrial fib, hypertension,
peripheral edema, depression
o Cormorbids/Unrelated: hypothryoidism,
diabetes, GERD, migraines
Harder, PharmD, CGP, Julia. (2012). To Cover or Not To Cover:
Guidelines for Covered Medications in Hospice Patients. The
Clinician. 7(2), p1-3.

Question asked to CMS – 8/13
o Principle dx – COPD
o Comorbidities - coronary artery disease and
Parkinson's disease
Doc stated unrelated to COPD and would only
cover meds/tx for COPD
CMS – this does not encompass holistic nature
to exclude other conditions. Reiterated
hospice should provide “virtually all the care.”
Must be clear evidence as why it’s not related
CMS goes on to say…..
o We have previously acknowledged that
there are those rare circumstances in
which a service may not be related to
the patient's terminal prognosis and
that this determination is to be done on
a case-by-case basis by the hospice
physician with input from the IDG.

Here’s the Irony…
o Rebasing of the nine components of
the RHC
o Drug costs = $3.74 in 2011
o Drug costs trending down
o According to Abt Consultants (CMS)
Anyone have drug costs at $3.74 ppd?

What about unrelated symptoms?
Patient with NSCLC, end stage COPD,
Class 3 heart disease, atrial fib, diabetes,
peripheral neuropathy, spinal stenosis x
10 years. Patient has been on fentanyl
300 ug and gabapentin 2700 mg/d x 5
years.
Do you cover?

Final Rule
o Cover all symptom meds – acute or
chronic
o Used to be considered an inducement
to pay for unrelated drugs
o How are hospices handling this?

Department of Health and Human
Services - Office of Inspector General
o “Medicare Could Be Paying Twice for
Prescription Drugs for Beneficiaries in
Hospice” - June 2012
http://oig.hhs.gov
o Objective: To determine whether Medicare
Part D paid for prescription drugs that likely
should have been covered under the per diem
payments made to hospice organizations.

Issue with Part D Medicare - 2010
o Hospice beneficiaries had analgesics
paid thru Part D – 334,387 prescriptions
o 14.7% beneficiaries who had Part D
o Cost was $13,000,430
o Fentanyl 39%, Oxycodone 18%
Morphine 12%, Hydrocodone 9%
Should hospices have paid for these?
OIG – 2012 report – will be more audits

Feeling the need for Zoloft yet?


Use Appreciative Inquiry…..
o Strategies to combat rising costs…
• Educate physicians on accurate coding
diagnosis that relates to prognosis
• Develop standardized forms to help with
processes of coverage determination
• Work with PBM to obtain lower costs
• If not using – develop formulary
• Consider pharmacist to review meds and
make recommendations
• Pay attention to response from MAC


Four Seasons Approach Medication is Related to the Terminal Prognosis
if it is directly related to treating the principal
diagnosis ….
AND Is used to treat symptoms related to principal diagnosis
AND Is used to treat symptoms related to therapies (chemo) used to treat
principal diagnosis
AND Is used to treat secondary conditions related to principal diagnosis
(aspiration pneumonia/pressure ulcers) for dementia patients
AND Arises as a consequence of principal diagnosis (bone fracture secondary
to metastatic bone lesion)
OR ANY secondary diagnosis which affects prognosis of ≤ 6 months
OR In the hospice physicians judgment cannot make compelling reason why
it is not related to terminal diagnosis

Cost Effective Medications
o Careful cost-effective choice of medications
• Ondansetron (Zofran) vs. Haloperidol (Haldol)
• Tiotropium (Spiriva) vs. Ipratropium (Atrovent)
• Methadone and LA morphine vs. OxyContin
• Citalopram(Celexa) vs. escitalopram (Lexapro)
• Esomeprazole (Nexium) vs. omeprazole
(Prilosec)
o Use generics when possible
o Review costs via pharmacy benefits
manager

Coding
o Physician and coder need to work
closely together

ICD 10 Codes
o Oct 1, 2014
o Understanding crosswalking or mapping will be important to physicians during transition from ICD.9 to ICD.10
o Over 68000 new codes (14000 ICD.9)
o GEMs – general equivalence mapping
o Guide to crosswalking
www.cdc.gov/nchs/icd/icd10cm.htm.

ICD 10
o Full Implementation is expected by
hospice organizations!
o Specificity out to 7 numbers
Important Questions
o Do you have a certified coder?
o http://www.cdc.gov/nchs/data/icd9/icd9c
m_guidelines_2011.pdf
o Process for coding - Secondary Codes?
o Diagnosis – “determined by physician”
when/who decides?
o Do you have an external audit?
ICD-10 Operational Perspective
o Budget
• Resource Books
• Overtime
• Education
o Staff will need to be trained
o Physicians will need to be trained
o Software, hardware, form revisions
o Mapping of old and new codes
• Doctors: Start now!
Team Effort Across Departments
o Collaboration necessary to identify
systems impacted
o Across clinical, financial and IS areas
o Include HIM
o IT – databases and necessary software
o Administration support necessary

Discussion
o Great variation among hospices
regarding related diagnosis and
medications. How do you standardize
this in your organization?
o Need to develop processes to
coordinate physician/admissions/coder

Questions that need clarification
o Do you follow ICD-9 guidelines
exclusively or the LCDs? Not mutually
exclusive.
o Diagnosis picked at admission
o IDG/team physician - related
determined at admissions and IDG
o Ongoing diagnosis – falls under same
process

Questions?
Four Seasons Center of Excellence
o HPC Solutions
o Palliative Care Immersion Course
o Mentoring – physicians, nurse practitioners and
physician assistants
www.FourSeasonsCenterofExcellence.com