definitions oligomenorrhoea: “ the occurrence of menses on only five or fewer occasions per year...
TRANSCRIPT

Definitions
Oligomenorrhoea:
“ the occurrence of menses on only five or fewer occasions per year”
2ry Amenorrhoea:
“ the absence of menses for 6 months ( or greater than three times the previous cycle intervals) in a woman who has menstruated before”
Rule out PREGNANCY
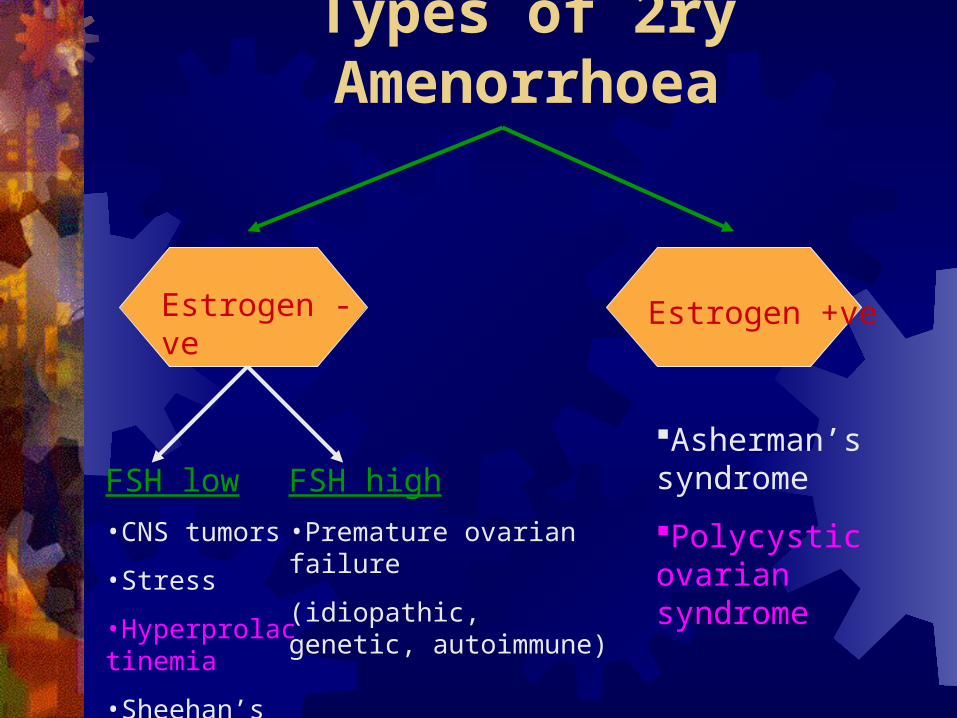
Types of 2ry Amenorrhoea
Estrogen - ve Estrogen +ve
FSH low•CNS tumors
•Stress
•Hyperprolactinemia
•Sheehan’s syndrome
FSH high•Premature ovarian failure
(idiopathic, genetic, autoimmune)
Asherman’s syndrome
Polycystic ovarian syndrome

Continue:How to check for the Estrogen status? Serum Estradiol level….. Variable
Progesterone challenge test
Endometrial thickness….
Transvaginal us scan < 5mm hypo. >6 mm Normal

Hypo-estrogenic 2ry Am’rrhoea
1. Hypothalamic-pituitary dysfunction
2. Premature ovarian failure
3. Hyperprolctinemia
1. FSH low & prolactin normal
2. FSH high & prolactin normal
3. FSH low & prolactin high
Hypothalamic-pituitary dysfunction:
Eating disorders e.g, Anorexia nervosa, extensive dieting or exercise. A loss of >10 kg … a’hoea… estrogen lllow …osteoporosis
Hypothalamic lesions
Nonsecreting pituitary adenomas
Other CNS system neoplasms
Sheehan’s syndrome
Combined care with endocrinologist,, psychotherapist,…. Etc is usually needed
Premature ovarian failure:Causes:
Chromosomal abnormalities. Amenorrhoea < 35 years of age •47 XXY ….. High risk of malignancy… gonadectomy
•Turner’s syndrome mosaic (XX/XO)
Resistant ovarian syndrome. May be due to auto antibodies against ovaries or gonadotropin receptors. Could be part of disease involving thyroid, adrenal and acid receptors in stomach
If present in younger age <35 years check auto antibodies
Premature menopause. < 45 mainly familial
High FSH & LH Low Estradiol, chromosomal analysis / ovarian biopsy


Prolactin secretion is is inhibited by dopamine from hypothalamus. No negative feed back by peripheral hormones
Hyperprolctinemia: levels > 800mu/l ( 60 ng/ml). Clinically significant if accompanied with oligo-amenorrhoea or galactorrhoea.
Interferes with menstrual cycle by suppression of pulsatility of LH secr’n and accounts for 20% of amenorrhoea and 2% of oligo in women
Hyperprolactinemic amenorrhoea increase risk of osteoporosis
Galactorrhoea is found in 50% of cases

Prolactin secreting tumours. 40-50% of cases; most are “micro-adenomas” (,10mm diameter). Macro adenoma levels >2500-3000 mU/l
Idiopathic. 40% levels are usually <2500 mIU/L
Other tumours compressing the the pituitary stalk. Rare, e.g. cranio- pahryngioma.
Primary hypothyroidism (3-5%).
Drugs (1-2%). Metochlopramide and phenothiazides are the commonest + cimetidine, haloperidol, methyl dopa and reserpine
Systemic problems.•Acromegaly
•Acute or chronic renal failure
•Herpes zoster of the breast dermatomes

Slight to moderate elevation. Repeat the test, if still high, screen for gross abnormality by lateral skull X-ray. If it shows enlargement of the pituitary fossa or erosion of the clinoid process …. CT scan to detect macro-adenoma.
Marked elevation… repeat the test + arrange CT scan ASAP. Specially urgent when headache or visual field defect present
MRI scanning offers better resolution for small micro-adenomas
An abnormal pituitary fossa may be due to the empty sella syndrome where there is congenital incompleteness of the roof of the fossa and the sub-arachnoid space extends into the fossa….. Benign condition
Micro-adenomas tend to grow slowly if at all. In up to 30% of patients spontaneous regression of micro-adenoma will occur
The treatment of choice is Dopamine agonist ( e.g. bromocriptine, or cabergoline). This will suppress prolactin secretion, correct estrogen deficiency, permits ovulation and reduce the size of most prolactinomas.
Surgery and radiotherapy are usually reserved for patients with very large tumours with extrasellar manifestations (e.g. pressure on the optic chiasma).
If pregnancy happens check visual field every 2 months and prescribe a dopamine agonist

Asherman’s syndrome
Polycystic Ovarian Disease/Syndrome

Secondary amenorrhoea following destruction of the endometrium by overzealous curettage. Mainly postpartum
Occasional vaginal spotting due to remnant island of endometrium
Multiple synechiae show up on hysterography
Management: break down intrauterine adhesions through hysteroscope and insert IUD for 10-12 months to deter reformation

1. Mrs. X was seen in the gyne clinic c/o period irregularity. Since menarche she used to having a menstrual period every 2-3 months which is heavy with clots. Now she has not had a period for 7 months. Home pregnancy test is negative on different occasions. What do you think?
2. Mrs. Y came to see you in the clinic crying in a very bad emotional state, c/o annoying acne on her face, excessive hair growth on her chin, beard and chest needing to shave every day, and loosing her head hair in an alarming rate… What do you think?
3. Mrs. Z was referred to you with h/o primary infertility for 4 years. The only abnormality in history is oligomenorrhoea ????
4. Mrs. A seen in the gyne clinic following her 3rd successive miscarriage asking for advice. What do you think?

Definition: “ the association of hyperandrogenism with chronic anovulation in women without specific underlying disease of the adrenal or pituitary gland”.
There is evidence o an autosomal dominant mode of inheritance. The male phenotype may be premature balding.
Hyperinsulinemia & insulin resistance implicated
Prevalence:
30-40% of women with amenorrhoea
75-90% of women with oligomenorrhoea
> 70% of women with anovulatory infertility
Polycystic ovaries have also been found in:
20% of asymptomatic women. US scan finding
Up to 90% of hirsute women with regular menses
Clinical features:
Subfertility . Acne/male type alopecia
Hirsutism . Family h/o maturity onset
Oligomenorrhoea DM
Obesity . Recurrent miscarriage
Dysfunctional uterine bleeding

Diagnosis & D.D :
The diagnosis is usually based on a combination of clinical, USS and biochemical criteria
High resolution transvaginal ultrasound will show the morphological feature of polycystic ovaries(multiple peripheral follicles <8 mm diameter and prominent echo-dense stroma) in up to 80% of anovulatory women.
If a woman has oligomenorrhoea, PCOS is likely in the presence of hirsutism, polycystic ovaries on ultrasound and excess circulating androgens
D.D.: hyperprolactinemia, acromegaly,CAH, androgen-secreting tumours of the ovary.


Endocrine Abnormalities:
Mean serum LH levels are usually increased, though normal levels do not exclude PCOS as LH release is pulsatile, FSH levels are normal
Serum of testosterone and androstenedione are raised in over 90% of cases
Serum Estradiol ( total & free) are within normal limits in early and mid-follicular phases. However the pattern of secretion is abnormal with no pre-ovulatory or midluteal increase. These effects may be compounded in obese women due to peripheral conversion of androgens by adipose tissue to estrone.

Metabolic abnormalities:
Women with PCOS have greater frequency and degree of hyper-insulinemia and insulin resistance
Pathogenesis:
Bloody difficult, so read it in your free time.

Management of anovulation:
If obese, weight loss would correct disorder and menstrual problem .BMI< 30
Cycle control, if does not want to conceive, by COCP or progestogens to induce withdrawal bleeding to reduce risk of endometrial cancer
Ovulation induction:Clomiphene 20-25% do not respond
Gonadotropin analogs
Laparoscopic ovarian drilling
Oral hypoglycemic agents
Management of hyperandrogenism:
Hirsutism can be treated by cosmetics and antiandrogens
Management of metabolic disorders:
Due to increased risk of DM2 and CVS disease;Carry out GTT, lipid profile in obese young women with PCOS
Ensure weight reduction
Surveillance of blood pressure
The same should be done in non-obese women with PCOS

Types of 2ry Amenorrhoea
Estrogen - ve Estrogen +ve
FSH low•CNS tumors
•Stress
•Hyperprolactinemia
•Sheehan’s syndrome
FSH high•Premature ovarian failure
(idiopathic, genetic, autoimmune)
Asherman’s syndrome
Polycystic ovarian syndrome….
FSH,LH,Prolactin, testosterone
