deformity of the feet in an aged woman
TRANSCRIPT

17
bromides, with tonics, cod-liver oil, and malt; alcoholshould, I believe, be strictly avoided. All sources ofmental anxiety and excitement should be removed, whilea quiet but nrm government of the child is provided. Theprognosis of these cases is good under proper manage-ment, and parents may be encouraged by knowledge of thefact that these nervous children often make the bestmen and women in later years, though a source ofmuch anxiety in childhood.Kensington, W.
-- ---- n__-_’ ------
ECZEMA CAUSED BY VIRGINIAN CREEPER.
BY E. LYCETT BURD, M.D. CANTAB., &c.
A CORRESPONDENCE having recently taken place on thesubject of eczema caused by the primula obconica, I thinkthe following ease will be of interest.Mrs. W——, a lady of middle age, consulted me on
Oct. 15th last on account of an attack of eczema then com-mencing. The cheeks were highly inflamed, the chin andparts round the nostrils covered by a weeping vesiculareruption ; there was also a partly papular and partlyweeping vesicular eruption on the back of the neck, wrists,arms, breast, and legs, with much irritation, heat, andpain. The eyelids were greatly cedematous, and were for atime completely closed. There was, however, no rise oftemperature, and but little constitutional disturbance. Nocause for the attack was then assigned, nor could I discoverany. Under treatment, the patient being a good one andstrictly carrying out all instructions, the attack quicklysubsided, and she became convalescent. Suddenly, how-ever, on Oct. 29th, the disease returned with, if possible,increased virulence, the face becoming again swollen andoedematous, and the vesicular weeping eruption appearingon that and other parts as before. On further considerationit was now recollected that on the day previously to eachattack Mrs. W- had been occupied in packing up andsending away to an artist friend a quantity of the leaves of Ithe Virginian creeper (Ampelopsis Hoggii). This seemed ito me hardly an adequate explanation, but the governessbad on both occasions been helping her, and on bothoccasions had been similarly attacked. The gardener, too,who had picked the leaves was also attacked with somesimilar eruption, but as he was not under my care I cannotvouch for the identity of the disease in his case. I thenlearnt that towards the end of September Mrs. W—— hadhad similar dealings with the same leaves, followed by asimilar though much slighter attack of eczema. This is tome an entirely unknown agent in the causation of eczema,nor can I find reference to a like case. I should be glad tohear if others have had a like experience.
IShrewsbury.
A NEW EPIGLOTTIC RETRACTOR.1
BY DR. J. MOUNT BLEYER,OF NEW YORK CITY.
WHILE busy several years ago in testing my tonguetractor for the purpose of forced laryngoscopy in children,and studying the action of the muscles, ligaments of thetongue and epiglottis, I found that if a firm pressure wasmade with the leaf-like projection of this instrument uponthe glosso-epiglottic ligament, a tension was produced, and
thereby the epiglottis raised and retracted against the baseof the tongue. Thh knowledge led me to construct theepiglottic retractor, of which the illustration is a facsimile.It needs no further description than the one of its applica-tion. Often patients are presented to us with an epiglottiseither misshapen or pendulous, and thereby obstructing our
1 Demonstrated before the German Surgical and Medical Society ofNew York, October, 1890.
view of the interior of the larynx, thus making a diagnosisdillicult. In order to retract the epiglottis, a 10 per cent.solution of cocaine is necessary to avoid reflex action ofthe muscles. The patient is instructed to hold his owntongue firmly by its end. The retractor, under the guid-ance of a laryngeal mirror, is passed upon the glosso-epiglottic ligament, direct pressure is then made upon it,the direction of this pressure being against the baseof the tongue. The epiglottis is seen immediatelyraised and retracted against the tongue, giving thereby athorough view of the interior of the larynx. Some prac-tice is necessary, as with all instruments for intra-
laryugeal work. This instrument, no doubt, will findits way into the armamentarium of the laryngologist. Itis manufactured by the well-known firm of Messrs. GeorgeTiemann and Co , New York City.New York.
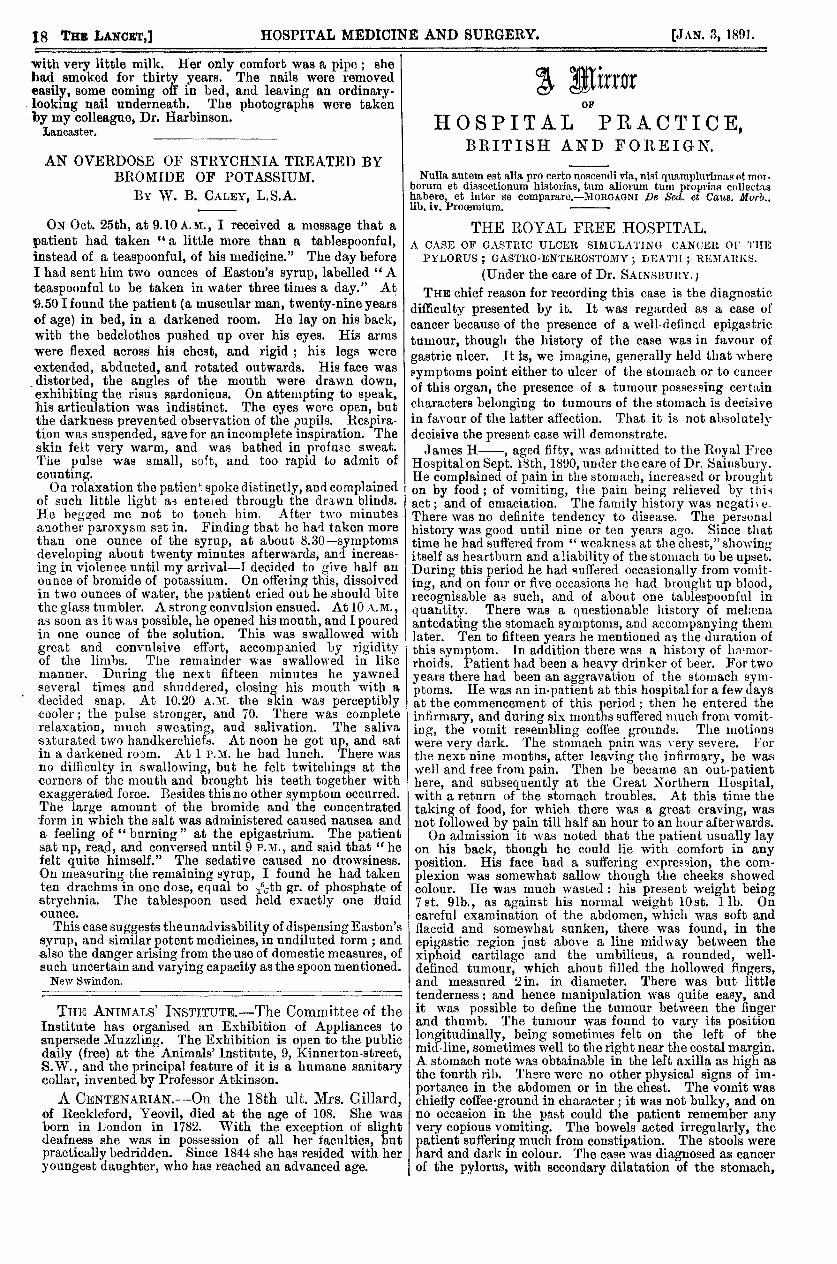
DEFORMITY OF THE FEET IN AN AGED WOMAN.BY J. J. G. PRITCHARD, L.R.C.P. LOND., &c.
TIlE accompanying illustrations faithfully depict the
appearance of the feet of an old woman who was admittedinto the Lancaster County Lunatic Asylum recently, exhibit-ing the effects of neglect, and showing the way in whichsome people still exist in civilised England.A. L-, aged seventy-four, was admitted last November
in a very dirty condition. She is quite blind from sym-pathetic ophthalmia, and is nearly deaf. Her feet presentedthe appearance seen in the engravings, with the addition of alarge amount of dirt filling up the interspaces. She walkedwith great difficulty on this account. She had lived withher son, a farm labourer, and badly off, for the last fiveyears, and had not had her toe-nails cut for the whole of
this period. She had worn her stockings both day andnight until they were worn out, and they were never
washed. The last pair she had worn six months. She hadfrequently asked to have her nails cut, as they hurt her,and she could not do so herself, but it was never done.She was troubled with sickness at first, complaining thatthe diet was too rich. She was accustomed to have a drop
of tea and a little bread, some dry potatoes for dinner,and a taste of meat on Sundays, sometimes porridge
18
with very little milk. Her only comfort was a pipe ; shehad smoked for thirty years. The nails were removedeasily, some coming off in bed, and leaving an ordinary-looking nail underneath. The photographs were takenby my colleague, Dr. Harbinson.
Lancaster. _____________
AN OVERDOSE OF STRYCHNIA TREATED BYBROMIDE OF POTASSIUM.
BY W. B. CALEY, L.S.A.
ON Oct. 25th, at 9.10 A.M., I received a message that apatient had taken "a little more than a tablespoonful,instead of a teaspoonful, of his medicine." The day beforeI had sent him two ounces of Easton’s syrup, labelled "A
teaspoonful to be taken in water three times a day." At’9.50 I found the patient (a muscular man, twenty-nine yearsof age) in bed, in a darkened room. He lay on his back,with the bedclothes pushed up over his eyes. His armswere flexed across his chest, and rigid ; his legs wereextended, abducted, and rotated outwards. His face wasdistorted, the angles of the mouth were drawn down,exhibiting the risus sardonicus. On attempting to speak,his articulation was indistinct. The eyes were open, butthe darkness prevented observation of the pupils. Respira-tion was suspended, save for an incomplete inspiration. Theskin felt very warm, and was bathed in profuse sweat.The pulse was small, soft, and too rapid to admit ofcounting.On relaxation the patient, spoke distinctly, and complained
of such little light a-3 entoed through the drawn blinds.He begged me not to touch him. After two minutesanother paroxysm set in. Finding that he had taken morethan one ounce of the syrup, at about 8.30-symptomsdeveloping about twenty minutes afterwards, and increas-ing in violence until my arrival-I decided to give half anounce of bromide of potassium. On offeiinc, this, dissolvedin two ounces of water, the patient cried out he should bitethe glass tumbler. A strong convulsion ensued. At 10 A. M.,
as soon as it was possible, he opened his mouth, and I pouredin one ounce of the solution. This was swallowed withgreat and convulsive effort, accompanied by rigidityof the limbs. The remainder was swallowed in likemanner. During the next fifteen minutes he yawnedseveral times and shuddered, closing his mouth with a
.
decided snap. At 10.20 A.M. the skin was perceptiblycooler; the pulse stronger, and 70. There was completerelaxation, much sweating, and salivation. The salivasaturated two handkerchiefs. At noon he got up, and satin a darkened room. At 1 P.M. he had lunch. There wasno difliculty in swallowing, but he felt twitchings at thecorners of the mouth and brought his teeth together withexaggerated force. Besides this no other symptom occurred.The large amount of the bromide and the concentratedform in which the salt was administered caused nausea anda feeling of "burning" at the epigastrium. The patientsat up, read, and conversed until 9 P.M., and said that " hefelt quite himself." The sedative caused no drowsiness.On measuring the remaining syrup, I found he had takenten drachms in one dose, equal to 5 th gr. of phosphate ofstrychnia. The tablespoon used held exactly one fluidounce.
This case suggests theunadvisability of dispensing Easton’ssyrup, and similar potent medicines, in undiluted form ; andalso the danger arising from the use of domestic measures, ofsuch uncertain and varying capacity as the spoon mentioned.New Swindon.
THE ANIMALS’ INSTITUTE.-The Committee of theInstitute has organised an Exhibition of Appliances to
supersede Muzzling. The Exhibition is open to the publicdaily (free) at the Animals’ Institute, 9, Kinnerton-street,S.W., and the principal feature of it is a humane sanitarycollar, invented by Professor Atkinson.A CENTENARIAN.-On the 18th ult. Mrs. Gillard,
of Reckleford, Yeovil, died at the age of 108. She wasborn in London in 1782. With the exception of slightdeafness she was in possession of all her faculties, butpractically bedridden. Since 1844 she has resided with heryoungest daughter, who has reached an advanced age.
A MirrorOF
HOSPITAL PRACTICE,BRITISH AND FOREIGN.
THE ROYAL FREE HOSPITAL.A CASE OF GASTRIC ULCER SIMULATING CANCER OF THE
PYLORUS ; GASTRO-ENTEROSTOMY ; DEATH ; REMARKS.
(Under the care of Dr. SAINSBURY.)
Nulla autem est alia pro certo noscendi via, nisi quamplurima.s etmot-borum et dissectionum historias, turn alioruni tuin propri)),s COl1GJCt:1!!habere, et inter se compra.re.—MoHGAGNl De Sed. et Caus. Morb.,lib, iv. Procemium. -
THE chief reason for recording this case is the diagnosticdifficulty presented by it. It was regarded as a case ofcancer because of the presence of a well-defined epigastrictumour, though the history of the case was in favour ofgastric ulcer. It is, we imagine, generally held that wheresymptoms point either to ulcer of the stomach or to cancerof this organ, the presence of a tumour possessing certaincharacters belonging to tumours of the stomach is decisivein favour of the latter affection. That it is not absolutelydecisive the present case will demonstrate.James H-, aged fifty, was admitted to the Royal Free
Hospital on Sept. 18bh, 1890, under the care of Dr. Sainsbury.He complained of pain in the stomach, increased or broughton by food; of vomiting, the pain being relieved by thisact; and of emaciation. The family history was negative.There was no definite tendency to disease. The personalhistory was good until nine or ten years ago. Since thattime he had suffered from " weakness at the chest," showingitself as heartburn and aliabilityof the stomach to be upset.During this period he had muttered occasionally from vomit-ing, and on four or five occasions he had brought up blood,recognisable as such, and of about one tablespooriftil in
quantity. There was a questionable history of melfena,antedating the stomach symptoms, and accompanying themlater. Ten to fifteen years he mentioned as the duration ofthis symptom. In addition there was a history of hil’!11or-rhoids. Patient had been a heavy drinker of beer. For twoyears there had been an aggravation of the stomach sym-ptoms. He was an in-patient at this hospital for a few daysat the commencement of this period ; then he entered theinfirmary, and during six months suffered much from vomit-ing, the vomit resembling coffee grounds. The motionswere very dark. The stomach pain was very severe. Forthe next nine months, after leaving the infirmary, he waswell and free from pain. Then he became an out-patienthere, and subsequently at the Great Northern Hospital,with a return of the stomach troubles. At this time thetaking of food, for which there was a great craving, wasnot followed by pain till half an hour to an hour afterwards.On admission it was noted that the patient usually lay
on his back, though he could lie with comfort in anyposition. His face had a suffering expression, the com-plexion was somewhat sallow though the cheeks showedcolour. He was much wasted : his present weight being7st. 91b., as against his normal weight 10 st. llb. Oncareful examination of the abdomen, which was soft andflaccid and somewhat sunken, there was found, in theepigastic region just above a line midway between thexiphoid cartilage and the umbilicus, a rounded, well-defined tumour, which about filled the hollowed fingers,and measured 2 in. in diameter. There was but littletenderness; and hence manipulation was quite easy, andit was possible to define the tumour between the fingerand thumb. The tumour was found to vary its positionlongitudinally, being sometimes felt on the left of themid line, sometimes well to the right near the costal margin.A stomach note was obtainable in the left axilla as high asthe fourth rib. There were no other physical signs of im-portance in the abdomen or in the chest. The vomit waschiefly coffee-ground in character; it was not bulky, and onno occasion in the past could the patient remember anyvery copious vomiting. The bowels acted irregularly, thepatient suffering much from constipation. The stools werehard and dark in colour. The case was diagnosed as cancerof the pylorus, with secondary dilatation of the stomach,