dementia and alzheimer’s disease presented by: amanda sandlin, msw adjunct professor for uaa...
TRANSCRIPT

Dementia and Alzheimer’s Disease
Presented by:Amanda Sandlin, MSW
Adjunct Professor for UAA School of Social Work&
Lisa Stanley, Care Coordination Supervisor at Alzheimer’s Resource Agency

Objectives
Increase knowledge of Alzheimer’s disease and related dementias/disorders (ADRD)
Learn statistics about ADRD, caregivers, and the community
Discuss the person-centered approach to care Review communication techniques Become familiar with local resources
What is Alzheimer’s Disease?
AD is a progressive, irreversible disease
Leads to loss of function and death of nerve cells in the brain
AD results in impaired cognition and behavior
Alzheimer’s disease is the most common cause of dementia in individuals over the age of 65
What is Dementia?

Dementia
The term dementia originates from Latin roots:“OUT OF MIND”
Dementia is not a disease in itself, but describes a group of conditions including:
Loss of intellectual function Loss of memory Confusion Behavioral changes Personality changes Loss of cognitive function

Causes of Dementia
IRREVERSIBLE
Alzheimer’s disease Pick’s disease Parkinson’s disease Lewy Body disease Vascular disease Creutzfeld-Jakob disease
POTENTIALLY REVERSIBLE
Depression Medication side-effects
or interactions Thyroid disorders Acute alcohol abuse Anemia Electrolyte imbalance
Alzheimer’s Disease Statistics Over 4.5 million people in the US have AD
People with AD will live from 5 to 20 years*
1 in 10 people have a family member with AD
7 out of 10 people with AD live at home with family caregivers
6 out of 10 people will wander*
The Human Brain The brain consists of three main parts:
The cerebrum: In control of remembering, problem solving, thinking, and feeling. It also controls movement.
The cerebellum: Controls coordination and balance.
The brain stem: Connects the brain to the spinal cord and controls automatic functions such as breathing, digestion, heart rate and blood pressure.

The Human Brain
ReadingHearing
Thinking Saying

Nerve Cells
An adult brain contains over 100 billion nerve cells, or neurons.
Nerve cells are branched together and allow the brain to send signals throughout the body- they form the basis for memories, thoughts, and feelings.
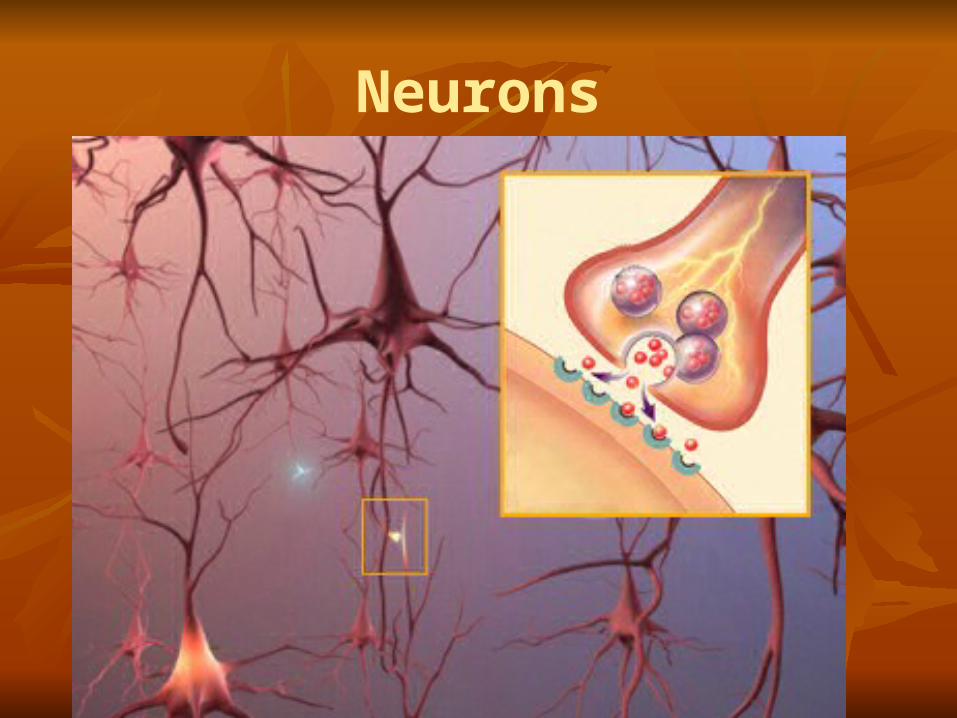
Neurons

Neurons and AD
The damage done by AD disrupts the neuron’s ability to send signals through the synapses, and the activity ofneurotransmitters.

Plaques and Tangles: Hallmark of AD
Plaques form when protein pieces called beta-amyloid clump together. Beta-amyloid comes from a larger protein found in the fatty membrane surrounding nerve cells.
Beta-amyloid is chemically "sticky" and gradually builds up into plaques.*
Scientists have not determined whether AD causes plaques and tangles, or whether plaques and tangles cause AD? However, they can be identified in all autopsied Alzheimer brains.

Plaques

Tangles

Healthy vs. Diseased Brain

Stages of Alzheimer’s disease
Four stages are typically associated with the progression of AD:
Early Stage: ForgetfulnessMiddle Stage: ConfusionAdvanced Stage: DisorientationFinal/Late Stage: Absence

Ten Warning Signs
1. Memory changes that disrupt daily life.2. Challenges in planning/problem-solving.3. Difficulty completing familiar tasks at home, work, or at
leisure.4. Confusion with time and place.5. Trouble understanding visual images and spatial
relationships.6. New problems with words in speaking or writing.7. Misplacing things and losing the ability to retrace steps.8. Decreased or poor judgment.9. Withdrawal from work or social activities.10. Changes in mood or personality.

Intellectual Symptoms
Amnesia: Loss of Memory
Aphasia: Loss of ability to speak and understand
Apraxia: Loss of motor skills and control
Agnosia: Loss of ability to recognize
Behavioral Symptoms
Early/Middle Stages: Difficulty concentrating Poor judgment Irritability, anxiety, depression Personality changes
Middle/Advanced Stages: Sleep disturbances Outbursts/Catastrophic reactions Emotional distress Paranoia Delusions Hallucinations

Early Diagnosis
Why is an early diagnosis so important? An early diagnosis can:
Rule out other possible causes of dementia symptoms Treat any reversible causes Begin medication to treat AD Discuss and plan for long-term care with
family/professionals Complete POA/Advanced Directives Participate in early-stage support groups
Long-Term Care
70% of people with AD are cared for in the home by a family caregiver.
The person with AD will eventually need 24/7 care.
Who will provide the care? Who will pay for the care needed? How will the safety and quality of life of the
individual be ensured?
Impacts of AD
Alzheimer’s disease and related disorders impact not only the person diagnosed, but also the family, the community, and the health care system.
The direct and indirect costs to Medicare, Medicaid, and businesses is estimated to be over $148 billion annually.
Impacts of AD
Researchers estimate that the number of people diagnosed with AD will double every twenty years; by 2030 65.7 million people will have AD.
A recent report completed by the Alzheimer’s Association concluded that currently the US needs an additional 3.5 million professional providers to support individuals with AD and their families.
The same report noted that there is a great need for additional social workers: only 4% specialize in geriatrics, compared to the needed 33%.

Unpaid Caregivers
The majority of people with AD are cared for by family members (70%).
In 2008 almost 10 million Americans provided 8.5 billion hours of unpaid care to individuals with AD or a related dementia, valuing $94 billion.
In Alaska, 14,539 AD caregivers provided 12,550,265 hours of unpaid care, valued at $139,307,943.00.

Unpaid Caregivers 32% of caregivers provide care for over 5 years 40% of caregivers rate stress as high or very high One-third of caregivers have symptoms of depression Family caregivers are more likely to have increased levels of
stress hormones, reduced immune functions, slow wound healing, New hypertension, and New coronary heart disease
AD caregivers are 31% more likely to reduce work hours or quit work when caring for a loved one with no significant behavioral symptoms
When caring for an individual with behavioral symptoms, AD caregivers are 68% more likely to reduce work hours, or quit work all together

How Can We Help?
Although there is no argument as to the devastating effects of AD and related disorders on the individual, the family, and the community, addressing these effects from a social work perspective can decrease negative outcomes and improve the AD journey for the family.
We must always remember that the person with AD, even in the most severe stage, can experience joy, comfort, and meaning in life.

Communication
To ensure a person-centered, strengths-based approach, it is very important for all members of the “care team” to communicate.
In addition, providers must always remember the cultural aspect and how one’s culture impacts perspectives on functioning, disability, long-term care, and caregiving.
Communication and AD
The following tips help when communicating with a person who is diagnosed with AD:
Meet the individual where they are: if the person is living in 1945, go there. Avoid reorienting the person.
Speak slowly and clearly. Choose simple words or phrases. Allow at least five seconds for the response.
Be aware of your tone of voice and facial expressions; body language is often understood when words are not.
Stand or sit directly in front of the person, and minimize other distractions.
Present only one idea or question at a time. Do not quiz the person or ask questions requiring explanations. Keep the environment calm, with low stimuli. Remember, the person may say one word but mean another; watch
for congruency in body language and other non-verbal cues.
Communicating with FamilyImportant topics to address at care planning meetings: Changes anticipated as the disease progresses Care goals and possible adjustments over time* Preparing for loss of decision-making capacity Wandering risks and precautions Harmful actions/behaviors Altered sleep/wake cycle Incontinence Recognizing and managing pain Fall risk Alternatives to restraints Diet and meals; signs of swallowing difficulty Preparation of safe foods Caregiver stress and use of respite/support groups Safety issues including driving a car, or staying alone
Community Awareness
An increased awareness of AD and related disorders will encourage prevention* and preventative behaviors* to increase positive outcomes for the community
Knowledge of resources and support programs for families coping with a diagnosis of AD allows us to appropriately refer individuals
National and Local Support
The Division of Senior and Disabilities Services(907) 269-3666
Contact DSDS for listings of local in-home service agencies, assisted living and nursing homes, and for a list of care coordinators and personal care assistants
The Alzheimer’s Disease Resource Agency of Alaska (ADRAA)(907) 561-3313www.alzalaska.org
Alzheimer’s Associationwww.alz.org

References
ADRAA Fact Sheets (available at the website www.alzalaska.org)
Alzheimer’s Association website (www.alz.org)
“Dementia Care Practice Recommendations for Professionals Working in a Home Setting”. Alzheimer’s Association; 2009.
“2009 Alzheimer’s Disease Facts and Figures”. Alzheimer’s Association; 2009.

Spring Semester Follow-Up Training
Next semester’s Field Instructor Training will:
Provide a more in-depth review of both pharmacological and non-pharmacological intervention strategies to use when working with individuals and families impacted by ADRD.
Please welcome Lisa Stanley, Care Coordination Supervisor of the Alzheimer’s Resource
Agency and learn about the agency’s services.