dendritic cell-based cancer immune therapy - c.ymcdn.comc.ymcdn.com/sites/ · dendritic cell-based...
TRANSCRIPT
Dendritic cell-based cancer immune therapyDanger signals in cancer immune therapy with dendritic cells: experience and first trends from a randomized clinical trial
ISCT 2014, April 2014

ISCT 2014 April 2014
DC-CIT basic principle
2
Monocyte collection Differentiation into DC Charging DC with antigen Antigen presentation to CTL
Treatment/in vivoManufacturing/in vitro
Tumour tissue Antigen extraction LPS/IFN-gmaturation Intranodal inoculation

ISCT 2014 April 2014
Unique characteristics of AV0113
3
Priming tumour cell-specific cytotoxic immune responses
Intranodal inoculation for optimal antigen presentation
In principle applicable to any neoplastic disease

ISCT 2014 April 2014
Unique characteristics of AV0113
4
Priming tumour cell-specific cytotoxic immune responses
Intranodal inoculation for optimal antigen presentation
In principle applicable to any neoplastic disease
ISCT 2014 April 2014
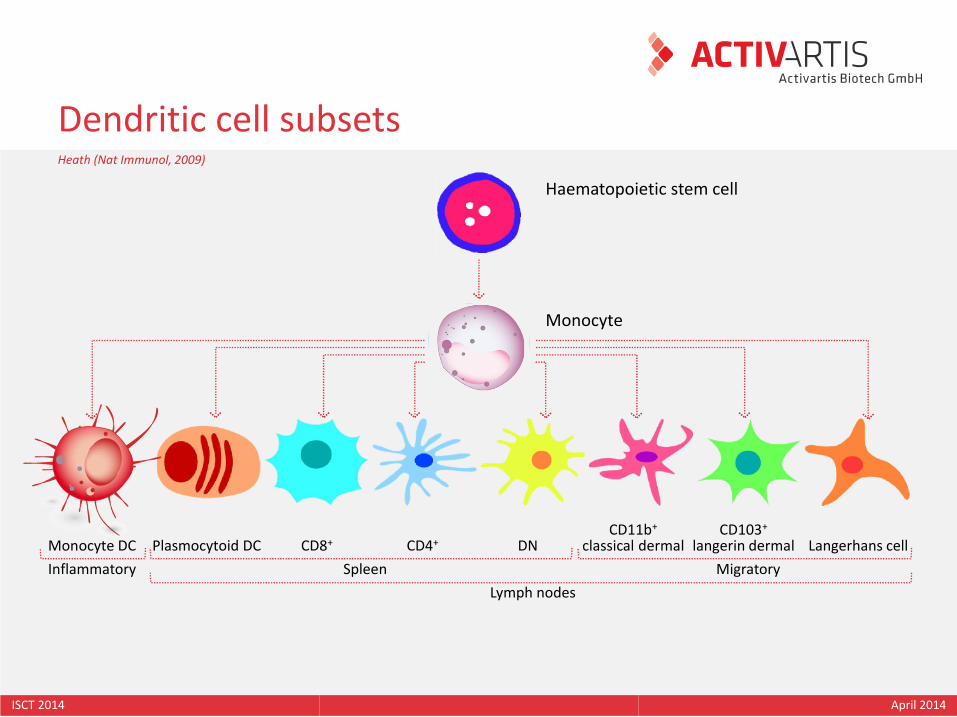
Dendritic cell subsets
Haematopoietic stem cell
Monocyte
Monocyte DC Plasmocytoid DC CD8+ CD4+ DNCD11b+
classical dermalCD103+
langerin dermal Langerhans cell
Inflammatory Spleen Migratory
Lymph nodes
Heath (Nat Immunol, 2009)

ISCT 2014 April 2014
Dendritic cell mode of action
6
ISCT 2014 April 2014
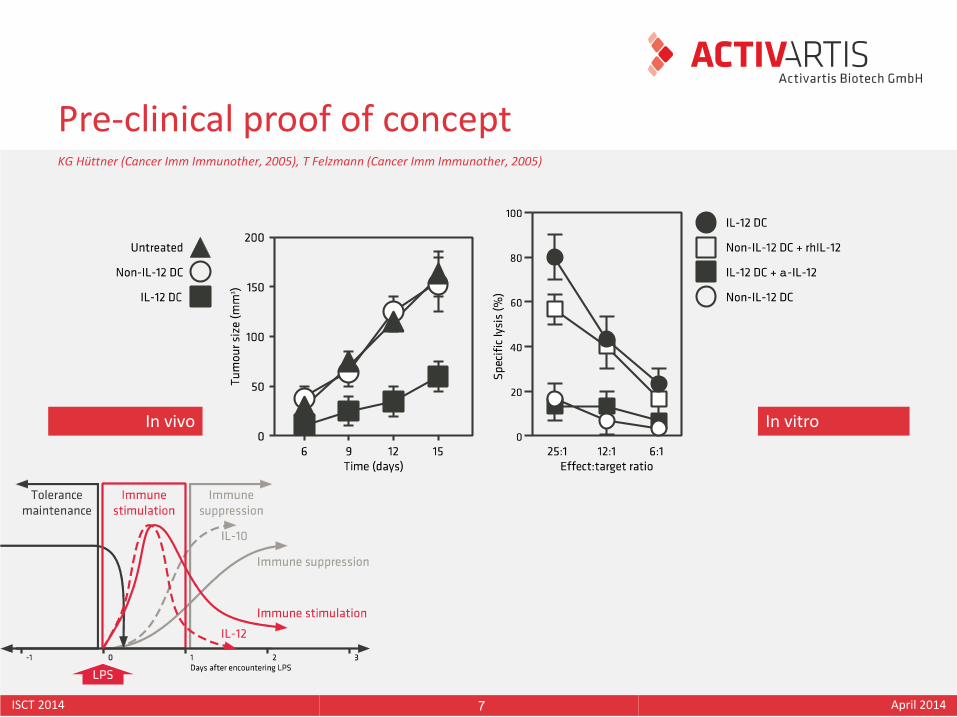
Pre-clinical proof of concept
7
In vivo In vitro
KG Hüttner (Cancer Imm Immunother, 2005), T Felzmann (Cancer Imm Immunother, 2005)

ISCT 2014 April 2014
Unique characteristics of AV0113
8
Priming tumour cell-specific cytotoxic immune responses
Intranodal inoculation for optimal antigen presentation
In principle applicable to any neoplastic disease
ISCT 2014 April 2014
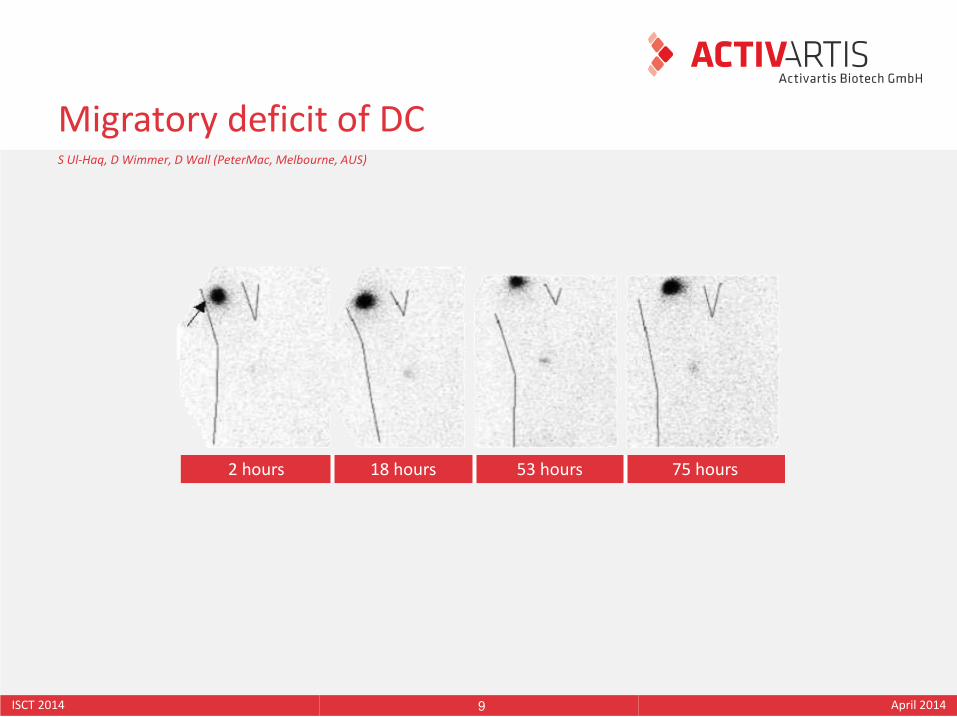
Migratory deficit of DC
9
2 hours 18 hours 53 hours 75 hours
S Ul-Haq, D Wimmer, D Wall (PeterMac, Melbourne, AUS)

ISCT 2014 April 2014
Intra-nodal application route
10
J Buchroithner (Wagner-Jauregg Hospital, Linz, Austria)
Before After

ISCT 2014 April 2014
Unique characteristics of AV0113
11
Priming tumour cell-specific cytotoxic immune responses
Intranodal inoculation for optimal antigen presentation
In principle applicable to any neoplastic disease

ISCT 2014 April 2014
Status of clinical development
12
Cancer Study type Patients Objectives
Sarcoma Safety & feasibility 20 6/20 patients alive >10 years
Kidney Safety & feasibility 13 Extended survival in 4 patients
Prostate Safety & feasibility 10 Artificial antigen
Brain Efficacy 78 Randomised efficacy study
W Holter, V Witt (St. Anna, Vienna, A), F Wimpissinger (KAR, Vienna, A), P Funovics, MB Fischer (MUW, Vienna, A)The Austrian GBM-Vax consortium (Linz, Wien, Innsbruck, Graz, Feldkirch, Salzburg)
Providing evidence for potential universal applicability

ISCT 2014 April 2014
Status of clinical development
13
Cancer Study type Patients Objectives
Sarcoma Safety & feasibility 20 6/20 patients alive >10 years
Kidney Safety & feasibility 13 Extended survival in 4 patients
Prostate Safety & feasibility 10 Artificial antigen
Brain Efficacy 78 Randomised efficacy study
W Holter, V Witt (St. Anna, Vienna, A), F Wimpissinger (KAR, Vienna, A), P Funovics, MB Fischer (MUW, Vienna, A)The Austrian GBM-Vax consortium (Linz, Wien, Innsbruck, Graz, Feldkirch, Salzburg)
Providing evidence for potential universal applicability

ISCT 2014 April 2014
Paediatric & young adult sarcoma, April/13
14
Patient Diagnosis Age Administration Outcome, April 2013 (months)
TM002 Osteosarcoma 21 s.c. Lost for follow-up
BG004 Osteosarcoma 17 s.c. 2,6
AE005 Osteosarcoma 8 s.c. 163,8 (Alive)
SiH007 Ewing sarcoma 22 s.c. 151,6 (Alive)
NH016 Ewing sarcoma 13 s.c. 138,1 (Alive)
TP017 Ewing sarcoma 22 i.n. 26,5
MK019 Osteosarcoma 10 s.c. Lost
LS020 Osteosarcoma 13 s.c. + i.n. 136,9 (Alive)
AI031 Desmoplastic small-cell sarcoma
14 i.n. 17,0
CV033 Fibrosarcoma 12 i.n. 127,8 (Alive)
DB042 Osteosarcoma 13 i.n. 14,1
DH044 Osteosarcoma 16 i.n. 80,7
RI057 Ewing sarcoma 15 i.n. 31,8
TK076 Osteosarcoma 15 i.n. 21,3
TL078 Epitheloid sarcoma 35 i.n. 103,6 (Alive)
MK092 Chondrosarcoma 34 i.n. 5,6
MA119 Osteosarcoma 15 i.n. 17,7
MS129 Osteosarcoma 19 i.n. 8,9
TA143 Myxofibrosarcoma 27 i.n. Lost for follow-up
SG155 Synovialsarcoma 32 i.n. 1,6
L Kager, V Witt, W Holter (St. Anna Children’s Hospital, Vienna, A), P Funovics (Medical University Wien, Department of Orthopaedics)

ISCT 2014 April 2014
Status of clinical development
15
Cancer Study type Patients Objectives
Sarcoma Safety & feasibility 20 6/20 patients alive >10 years
Kidney Safety & feasibility 13 Extended survival in 4 patients
Prostate Safety & feasibility 10 Artificial antigen
Brain Efficacy 78 Randomised efficacy study
W Holter, V Witt (St. Anna, Vienna, A), F Wimpissinger (KAR, Vienna, A), P Funovics, MB Fischer (MUW, Vienna, A)The Austrian GBM-Vax consortium (Linz, Wien, Innsbruck, Graz, Feldkirch, Salzburg)
Providing evidence for potential universal applicability

ISCT 2014 April 2014
Glioblastoma multiforme
16
GBM The most severe form of brain cancer
Frequency About 50 thousand cases annually
Age At any age from childhood to elderly; 2/3 of patients younger than 70 years
Treatment Surgery, irradiation, chemotherapy with Temozolomide (Temodal®)
Prognosis Average 7-8 months until relapse (PFS), 14-15 months until death (OS)
Second line Bevacizumab (Avastin®), palliative surgery
Conclusion Patients need access to novel treatment paradigms like DC cancer vaccine
www.cureglioma.info
Meeting an unmet medical need!

ISCT 2014 April 2014
The Austrian GBM-Vax consortium
17
MedUni WienKFJ/KARDonauspitalBlood Bank MedUni
Wagner-JaureggBlood Bank Red Cross Linz
LKHFeldkirch
MedUni GrazBlood Bank MedUni
MedUni InnsbruckBlood Bank MedUni
Salzburg Landesklinikum Blood Bank SALK

ISCT 2014 April 2014
GBM-Vax treatment schedule
18
ISCT 2014 April 2014
Objectives
19
Primary objective To evaluate efficacy of the dendritic cell cancer immune therapy AV0113 in patients with GBM after at least 70% surgical resection who are treated with standard chemo-therapy with radiotherapy and Temozolomide that is switched to Bevacizumab upon disease recurrence.
Progression free survival measured as percentage of non-progressive patients at 12 months post initiation of treatment.
Secondary objectives
Progression free survival measured as percentage of non-progressive patients at 18 and 24 months post initiation of treatment.Overall survival at 12, 18 and 24 months post initiation of treatment.Quality of life using ECOG (Eastern Cooperative Oncology Group) performance status (for study patients 18-70 years).

ISCT 2014 April 2014
PFS is a poor surrogate parameter in CIT
20
DC PSA/GM-CSF (Prostate)
Peptide EGFRvIII (Brain)
Poxvirus PSA (Prostate)
Ipilimumab (Melanoma)
Dendreon Celldex Bavaria Nordic BMS
Treat Control Treat Control Treat Control Treat Control
Patient number 341 171 65 Historic 82 40 403 136
Overall survival 26 22 26 n.a. 25 16 10 6
PFS 3.7 3.6 14.2 n.a. 3.8 3.7 2.8 2.8
Primary objective OS PFS PFS OS
Secondary objective PFS OS OS PFS
PW Kantoff (NEJM, 2010), PW Kantoff (JCO, 2010), JH Sampson (JCO, 2010), FS Hodi (NEJM, 2010)
A paradigm shift in the treatment of neoplastic diseases.

ISCT 2014 April 2014
Inclusion/exclusion criteria
21
Inclusion criteria Female & male, 18-70 years, qualifying for standard treatment.Glioblastoma Multiforme WHO stages IV-VI, proven by histology.At least 70% reduction of tumour mass defined by MRI.Supra-tentorial tumours.At least ECOG 3.At least 12 weeks by assessment of the attending physician.
Exclusion criteria No written informed consent.Insufficient amount of tumour tissueAnti-neoplastic chemo- or radiotherapy within 4 weeks prior to study.Pregnancy or lactation, unable or unwilling to perform safe birth control.

ISCT 2014 April 2014
36 treatment
42 control
78 randomised
105 total recruitment
56 plannedOriginal study design
Number of patients
76 amendedFor recruiting 56 “evaluable” patients
18 not randomisedWithdrawing consent, GBM not confirmed, etc
2 paediatric
7 elderly
9 safety & feasibility

ISCT 2014 April 2014
GBM-Vax 12 months survival trend, January 2014The Austrian GBM-Vax trial consortium (Linz, Wien, Innsbruck, Graz, Feldkirch, Salzburg)
Only patients receiving 2nd line BevacizumabAll patients
& AV0113 Control
3/1916% deaths
9/2045% deaths
7/25(28%)
13/30(43%)
& AV0113 Control
Perc
enta
ge s
urv
ivin
g p
atie
nts
Days

ISCT 2014 April 2014
PFS, May 2013The Austrian GBM-Vax trial consortium (Linz, Wien, Innsbruck, Graz, Feldkirch, Salzburg)

ISCT 2014 April 2014
Pseudo-progression hypothesis

ISCT 2014 April 2014
AV0113 regulatory status
26
Granted Q4/2012Q2/2013Q4/2013
EMA orphan drug designationFDA orphan drug designationAustria compassionate use programme
Q1/2014Q1/2014
FDA pre-IND meeting & INDEMA pre-submission meeting scientific advice & protocol assistance
Planned Q3/2014 EMA & FDA (conditional) marketing authorisation

ISCT 2014 April 2014
Take home message
27
Cancer immune therapy is here to stay!
Surgery Radiotherapy Chemotherapy Immune therapy

Thank you for taking the time!