dental learning dr froum part 4.pdfit is a combination of many educational courses and clinical...
TRANSCRIPT

Case Series
Knowledge for Clinical Practice
WWW.DENTALLEARNING.NET
A PEER-REVIEWED PUBLICATIONA PEER-REVIEWED PUBLICATION
DENTAL LEARNING
DentalLearning.net is an ADA CERP Recognized Provider. ADA CERP is a service of the American Dental Association to assist dental professionals in identifying quality providers of continu-ing dental education. ADA CERP does not approve or endorse individual courses or instructors, nor does it imply acceptance of credit hours by boards of dentistry. DentalLearning.net des-ignates this activity for 2 continuing education credits.
Approved PACE Program Provider FAGD/MAGD Credit Approval does not imply acceptance by a state or provincial board of dentistry or AGD endorsement. (2/1/2012) to (1/31/2016)AGD Code: 691, 692
Single Implant Placement in the Atrophic Posterior Maxilla
Osteotome-Assisted Sinus Augmentation Procedure for
Stuart J. Froum DDS, Sang-Choon Cho DDS, MS, Rodrigo Cayarga De la Hoz, DDS and Ismael Khouly DDS, MS
Inside earn
2 CE CreditsWritten for dentists,hygienists and assistants
PART 4 IN A SERIES

DENTAL LEARNING
2
www.dentallearning.net
Copyright 2012 by Dental Learning, LLC. No part of this publication may be reproduced or transmitted in any form without prewritten permission from the publisher.
500 Craig Road, First Floor, Manalapan, NJ 07726
DENTAL LEARNING
EDUCATIONAL OBJECTIVES
The overall objective of this article is to provide the reader with information on the osteotome-assisted sinus augmentation procedure.
On completing this article, the reader will be able to do the following:
1. List some of the procedures available for sinus augmentation.
2. Review the steps required for an osteotome-assisted sinus augmentation procedure.
3. Describe the medications that are required post-surgery following an osteotome-assisted sinus augmentation procedure.
4. Review the procedure required for a bone-added osteotome sinus floor elevation and its limitations.
5. Compare and contrast the hybrid technique with the osteotome-assisted sinus augmentation procedure.
SPONSOR/PROVIDER: This is a Dental Learning, LLC continuing education activity. DESIGNATION STATEMENTS: Dental Learning, LLC is an ADA CERP recognized provider. ADA CERP is a service of the American Dental Association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not approve or endorse individual courses or instructors, nor does it imply acceptance of credit hours by boards of dentistry. Dental Learning LLC designates this activity for 2 CE credits. Dental Learning is also designated as an Approved PACE Program Provider by the Academy of General Dentistry. The formal continuing education programs of this program provider are accepted by AGD for Fellowship, Mastership, and membership maintenance credit. Approval does not imply acceptance by a state or provincial board of dentistry or AGD endorsement. The current term of approval extends from 2/1/2012 - 1/31/2016. Provider ID: # 346890 Dental Learning, LLC is a Dental Board of California CE provider. The California Provider number is RP5062. This course meets the Dental Board of California’s requirements for 2 units of continuing education. EDUCATIONAL METHODS: This course is a self-instructional journal and web activity. Information shared in this course is based on current information and evidence. REGISTRATION: The cost of this CE course is $29.00 for 2 CE credits. PUBLICATION DATE: November, 2012. EXPIRATION DATE: October, 2015. REQUIREMENTS FOR SUCCESSFUL COMPLETION: To obtain 2 CE credits for this educational activity, participants must pay the required fee, review the material, complete the course evaluation and obtain a score of at least 70%. AUTHENTICITY STATEMENT: The images in this course have not been altered. SCIENTIFIC INTEGRITY STATEMENT: Information shared in this continuing education activity is developed from clinical research and represents the most current information available from evidenced-based dentistry. KNOWN BENEFITS AND LIMITATIONS: Information in this continuing education activity is derived from data and information obtained from the reference section. EDUCATIONAL DISCLAIMER: Completing a single continuing education course does not provide enough information to result in the participant being an expert in the field related to the course topic. It is a combination of many educational courses and clinical experience that allows the participant to develop skills and expertise. PROVIDER DISCLOSURE: Dental Learning does not have a leadership position or a commercial interest in any products that are mentioned in this article. No manufacturer or third party has had any input into the development of course content. CE PLANNER DISCLOSURE: The planner of this course, Monique Tonnessen, does not have a leadership or commercial interest in any products or services discussed in this educational activity. She can be reached at [email protected]. TARGET AUDIENCE: This course was written for dentists, dental hygienists, and assistants, from novice to skilled. CANCELLATION/REFUND POLICY: Any participant who is not 100% satisfied with this course can request a full refund by contacting Dental Learning, LLC, in writing. Go Green, Go Online to www.dentallearning.net take your course. Please direct all questions pertaining to Dental Learning, LLC or the administration of this course to [email protected].
There are a number of techniques available for performing sinus augmentation surgery, which has been reported to be a highly predictable procedure. The osteotome-assisted sinus augmentation procedure is a technique that enables simultaneous placement of implants in the atrophic maxilla. Carefully following specific steps as described in this article results in clinical success. Using the OASA technique, the size of the incision and reflection of the periosteal flap are minimized and the lateral window is reduced, thereby decreasing the removal of bone from the lateral sinus wall and the potential for postoperative complications, such as swelling and pain.
ABSTRACT
EditorFIONA M. COLLINS
CE Content ManagerMONIQUE TONNESSEN
Creative DirectorMICHAEL HUBERT
Art DirectorMICHAEL MOLFETTO
ABOUT THE AUTHORSStuart J. Froum DDS Dr. Stuart J. Froum is an international lecturer and has been in private practice for over 35 years. He is on the Research Com-mittee for the Academy of Osseointegration, and is the Vice President of the American Academy of Periodontology where he has previously served as Board Liaison to the Continuing Education Oversight Committee, a member of the Con tinuing
Education Committee and as a District Trustee. Dr. Froum has published over 100 articles in peer-reviewed journals, was the editor for the recently-pub lished book titled ‘Dental Implant Complications Etiology, Prevention and Treat ment’, co-author of ‘Comprehensive Periodontics for the Dental Hygienist’ (2001), and a contribut-ing author for the 11th edition of Carranza’s Clinical Periodontology as well as a co-author of 3 chapters in ‘Sinus Bone Graft’ (2006) and Implant Site Develop-ment (2010). He is also a reviewer for the Journal of Periodontology, Inter national Journal of Periodontics and Restorative Dentistry and for Compendium. Dr. Froum was awarded the William J. Gies Award for Service to the American Academy of Periodontology in 2006, the American Academy of Periodontology “The Special Citation Award” in 2005, the Hirschfeld Award – NESP in 1999, the Clinical Research Award in both 2004 and 2005, and the J. Coslet – Distinguished Lecturer Award from the University of Pennsylvania Dental School in 2003. Dr. Froum can be reached at [email protected].
Sang-Choon Cho DDS, MSDr. Sang-Choon Cho is a full-time Clinical Assistant Professor and Director of Advanced Program for International Dentists in Implant Dentistry in the Department of Periodontology and Implant Dentistry, at New York University College of Dentistry (NYUCD). He is a graduate of both the DDS program and the
Advanced Program in Implant Dentistry for International Dentists at NYUCD and also holds a dental degree and an MS degree from Kyungpook National Univer-sity in South Korea. In addition to teaching and conducting research at NYUCD, Dr. Cho serves as a liaison to the NYUCD South Korean Alumni Study Club. Dr. Cho can be reached at [email protected].
Rodrigo Cayarga De la Hoz, DDSDr. Rodrigo Cayarga is a graduate of the Advanced Program for International Dentists in Comprehensive Dentistry as well as the Advanced Program for International Dentists in Implant Dentist-ry, in which he is now a Clinical Fellow, at NYUCD. Dr. Cayarga holds a dental degree from the Universidad Francisco Marroquin
in Guatemala. Dr. Cayarga can be reached at [email protected].
Ismael Khouly DDS, MSDr. Ismael Khouly is the Clinical Research Coordinator in the Bluestone Center for Clinical Research at NYUCD.
3SEPTEMBER 2012
Introduction
Sinus augmentation surgery (SAS) has been reported to be a highly predictable procedure for creating bone in the atrophic posterior maxilla to allow implant
placement.1-4 There are several methods of accomplishing this. One of the most widely used procedures for SAS is the Lateral Window Sinus Floor Elevation (LWSFE), whereby an osteotomy “window” in the lateral wall of the sinus is made for access. An advantage of the LWSFE is that it allows direct view of the sinus cavity, direct access to the Schneiderian membrane for elevation and easy addition of an appropriate graft material. However, this procedure has the disadvantages of prolonged time, additional cost, and increased morbidity.5
Elevation of the sinus membrane can also be accom-plished with a transcrestal approach to the maxillary sinus, known as the Bone Added Osteotome Sinus Floor Elevation (BAOSFE). The transcrestal approach has been advocated as “minimally invasive” because of minimal flap reflection and less postoperative morbidity.6-7 However, limitations of this procedure include diminished accessibility, limited visibility for elevation of the sinus membrane, an inability to diagnose and treat membrane perforations, and potential paroxysmal positional vertigo.8-9 In order to avoid these complications, other approaches have been proposed, including the hybrid technique,10 the balloon-lift control system,11 use of hydrau-lic pressure,12-13 use of negative pressure14 and piezo-surgical sinus floor elevation.15
Since a crestal osteotome approach involves blind eleva-tion of the sinus floor, the extent to which the sinus floor can be safely elevated prior to membrane perforation is not readily known with this technique. Using a transcrestal sinus
elevation technique, perforation rates have been reported to range between 2.2% and 25%.15-20 In a cadaver study, Rei-ser et al19 reported a 24% membrane perforation rate using the osteotome technique when associated with proximity to either antral septae or the collateral wall of the nose. Toffler, using a Valsalva maneuver, reported a 4.3% clinically detectable perforation rate.16 The reason for this differ-ence in prevalence may be due to the difficulty in detecting small membrane perforations clinically. Moreover, with the limited access utilizing the transcrestal approach, there is little possibility to repair the membrane perforation without changing to an LWSFE approach.19-22
The purpose of this case series was to evaluate the clini-cal success of simultaneously placing single implants in the atrophic maxilla and augmenting the available native bone using a new surgical approach: the osteotome-assisted sinus augmentation (OASA) procedure. Implant survival, mor-bidity and complications with this technique were docu-mented and will be reported. Case selection criteria will be discussed, as well the advantages and disadvantages of this technique.
Materials and MethodsClinical data in this study was obtained from Implant
Database (ID). This data set was extracted as de-identified information from the routine treatment of patients at the Ashman Department of Periodontology and Implant Dentistry at New York University College of Dentistry (NYUCD). The ID was certified by the Office of Quality Assurance at NYUCD. This study was in compliance of the Health Insurance Portability and Accountability Act (HIPAA) requirements.
Osteotome-Assisted Sinus Augmentation Procedure for
Single Implant Placement in the Atrophic Posterior MaxillaPart 4 in a series.

DENTAL LEARNING
4
www.dentallearning.net
Study Subjects Fifteen consecutive posterior partially edentulous
patients with posterior maxillary atrophy who underwent single implant placement using the OASA procedure from August 2009 to August 2011 were chosen from the ID and were included in this study. The population consisted of 6 male and 9 female patients with a mean age of 52 years (range: 44 to 62). Each subject selected from the database for this study had to have conformed to the following crite-ria prior to undergoing the OASA procedure:
Inclusion Criteria:All subjects were required to have:
1. A panoramic radiograph and reformatted computed tomography (CT) scans.
2. A posterior maxillary partially edentulous area with lim-ited vertical bone height, 4-7 mm, and requiring single implant placement. (Figs. 1-2)
3. A healed ridge at least 3 months following tooth extrac-tion.
4. The final implant restoration in function for a minimum of 6 months.
Exclusion Criteria:1. Presence of uncontrolled diabetes, immunological diseases
or other systemic conditions that contraindicated surgery. 2. Radiation therapy to the head and neck region in the 12
months prior to the proposed therapy.3. Chemotherapy within a 12-month period prior to the
proposed therapy.4. Periodontal disease, or an unwillingness to undergo
needed periodontal therapy, around the remaining teeth.5. Active sinus infection, or a history of persistent sinus
infection.6. Smoking habit of one pack or more per day and an
unwillingness to enter a smoking cessation protocol.7. Psychological problems that, in the opinion of the sur-
geons, would have rendered the delivery of comprehen-sive therapy untenable.
8. Unwillingness to commit to a long-term post-therapy maintenance program. Prior to OASA surgery, a complete examination of oral
hard and soft tissues was conducted for each patient, and a dental treatment plan was formulated in conjunction with the treating restorative dentist. Diagnostic casts, wax-ups and surgical templates were also prepared prior to surgery.
In conjunction with the OASA procedure, single rough-surface implants were placed and submerged. The time between stage 1 and stage 2, abutment placement surgery, ranged from 3 to 6 months. All implants were restored as
Figure 1. Preoperative X-ray of the missing maxillary 2nd premolar tooth with < 7 mm of native bone remapping
Figure 2. Clinical preoperative view of edentulous pre-molar area

Osteotome-Assisted Sinus Augmentation Procedure for Single Implant Placement in the Atrophic Posterior Maxilla - Case Series
5SEPTEMBER 2012
single-tooth restorations. Patients were recalled every 3 months for supportive care and evaluation.
The criteria for determining survival required that the implant be in function for at least 6 months. In addition, the implant had to meet the following conditions (modifications of Albrektsson success criteria) to be considered a success:1. The individual, unattached implant be immobile when
tested clinically.2. Postsurgical periapical radiographs that demonstrated
no evidence of peri-implant radiolucency. 3. Vertical bone loss, as measured on a nonstandardized
radiograph, using the implant platform as the reference point, be less than 0.1 mm semiannually following the implant being placed in function. Periapical radiographs were taken at follow-up visits and compared with the radiographs taken after implant placement (baseline). Radiographic bone loss was computed using magnifica-tion and measurements determined by comparison of actual and radiographic implant length.
4. The implant was characterized by an absence of persis-tent and/or irreversible signs of complications such as pain, infection, neuropathy or paresthesia/anesthesia.
Description of the OASA Procedure The clinical procedures were standardized and followed
the protocol as described below:1. Patients were prescribed 2 g of amoxicillin 1 hour prior
to surgery or if allergic, 600 mg of clindamycin 1 hour prior to surgery.
2. Local infiltration anesthesia of lidocaine 2% containing epinephrine at a concentration of 1:100,000 was used, or Carbocaine 3% administered in cases where a vaso-constrictor was contraindicated.
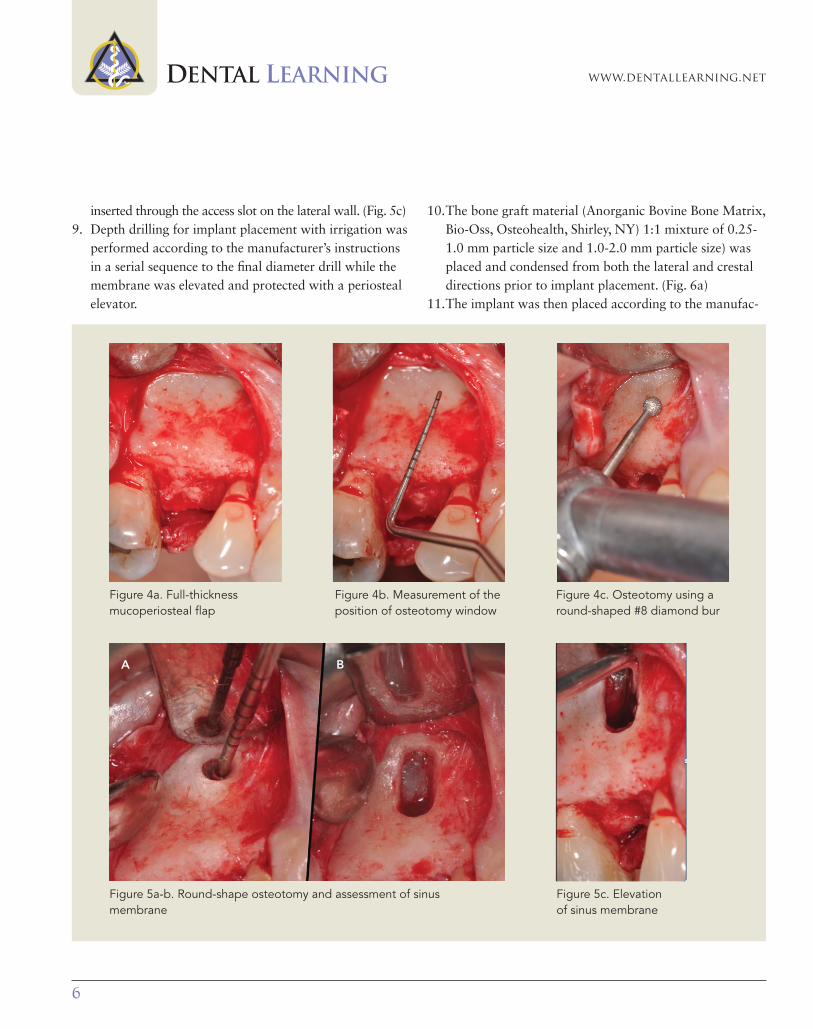
3. A midcrestal incision, between the two adjacent teeth, was performed, followed by a single vertical releasing incision from the distal aspect of the adjacent anterior tooth to the mucogingival junction. (Fig. 3) A full-thick-ness mucoperiosteal flap was raised, exposing the lateral sinus wall. (Fig. 4a)
4. A small round-shaped osteotomy consisting of a 2 to 3 mm diameter window was prepared in the lateral wall, using a high-speed round #6-#8 diamond bur with copi-ous irrigation, followed by use of a piezo-surgical tip. This window was created at the height of the apex of the planned implant. (Figs. 4b, c)
5. The integrity of the Schneiderian membrane was as-sessed visually.
6. The following algorithm was followed:a. Intact membrane – continue procedure according to
the technique.b. Perforated membrane – modification of the osteotomy
in which a wider lateral window was prepared to allow increased access to repair the membrane. The membrane was repaired using an absorbable collagen wound dressing (CollaTape, Zimmer Dental Inc, Carls-bad, CA) to completely cover the perforation, allowing the graft material to be placed in the contained space.
7. The round-shaped osteotomy made previously in the lateral wall was expanded in an apico-coronal direction, creating a vertical slot of 5-7 mm, to allow access for atraumatic elevation of the membrane from the floor of the sinus. (Figs. 5a, b)
8. The sinus membrane was fully elevated mesiodistally and medially over the drilling site, using a sinus membrane elevator (SSC1, EBI Implant, Kyungsan, South Korea)
Figure 3. Midcrestal incision and one vertical releasing incision on mesial of the first premolar tooth
DENTAL LEARNING
6
www.dentallearning.net
inserted through the access slot on the lateral wall. (Fig. 5c) 9. Depth drilling for implant placement with irrigation was
performed according to the manufacturer’s instructions in a serial sequence to the final diameter drill while the membrane was elevated and protected with a periosteal elevator.
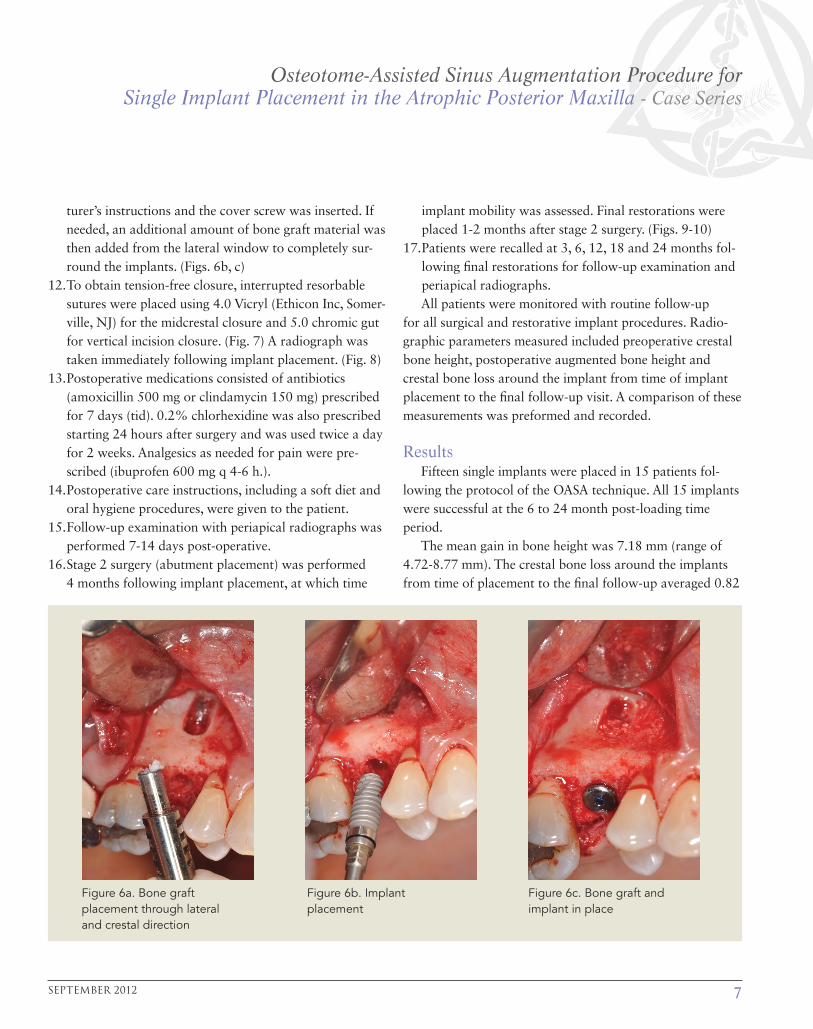
10. The bone graft material (Anorganic Bovine Bone Matrix, Bio-Oss, Osteohealth, Shirley, NY) 1:1 mixture of 0.25-1.0 mm particle size and 1.0-2.0 mm particle size) was placed and condensed from both the lateral and crestal directions prior to implant placement. (Fig. 6a)
11. The implant was then placed according to the manufac-
Figure 5c. Elevation of sinus membrane
Figure 5a-b. Round-shape osteotomy and assessment of sinus membrane
A B
Figure 4a. Full-thickness mucoperiosteal flap
Figure 4c. Osteotomy using a round-shaped #8 diamond bur
Figure 4b. Measurement of the position of osteotomy window
Osteotome-Assisted Sinus Augmentation Procedure for Single Implant Placement in the Atrophic Posterior Maxilla - Case Series
7SEPTEMBER 2012
turer’s instructions and the cover screw was inserted. If needed, an additional amount of bone graft material was then added from the lateral window to completely sur-round the implants. (Figs. 6b, c)
12. To obtain tension-free closure, interrupted resorbable sutures were placed using 4.0 Vicryl (Ethicon Inc, Somer-ville, NJ) for the midcrestal closure and 5.0 chromic gut for vertical incision closure. (Fig. 7) A radiograph was taken immediately following implant placement. (Fig. 8)
13. Postoperative medications consisted of antibiotics (amoxicillin 500 mg or clindamycin 150 mg) prescribed for 7 days (tid). 0.2% chlorhexidine was also prescribed starting 24 hours after surgery and was used twice a day for 2 weeks. Analgesics as needed for pain were pre-scribed (ibuprofen 600 mg q 4-6 h.).
14. Postoperative care instructions, including a soft diet and oral hygiene procedures, were given to the patient.
15. Follow-up examination with periapical radiographs was performed 7-14 days post-operative.
16. Stage 2 surgery (abutment placement) was performed 4 months following implant placement, at which time
implant mobility was assessed. Final restorations were placed 1-2 months after stage 2 surgery. (Figs. 9-10)
17. Patients were recalled at 3, 6, 12, 18 and 24 months fol-lowing final restorations for follow-up examination and periapical radiographs.All patients were monitored with routine follow-up
for all surgical and restorative implant procedures. Radio-graphic parameters measured included preoperative crestal bone height, postoperative augmented bone height and crestal bone loss around the implant from time of implant placement to the final follow-up visit. A comparison of these measurements was preformed and recorded.
ResultsFifteen single implants were placed in 15 patients fol-
lowing the protocol of the OASA technique. All 15 implants were successful at the 6 to 24 month post-loading time period.
The mean gain in bone height was 7.18 mm (range of 4.72-8.77 mm). The crestal bone loss around the implants from time of placement to the final follow-up averaged 0.82
Figure 6a. Bone graft placement through lateral and crestal direction
Figure 6c. Bone graft and implant in place
Figure 6b. Implant placement

DENTAL LEARNING
8
www.dentallearning.net
mm (range of 0.31-1.43 mm). One out of 15 (6.7%) mem-branes had a detectable perforation, which was repaired during surgery. (Table 1)
DiscussionThe Bone Added Osteotome Sinus Floor Elevation
(BAOSFE) procedure is considered to be a less traumatic technique than the Lateral Wall Sinus Floor Elevation (LWS-FE) procedure, with reported similar success rates.16,22-26 The results of the present study utilizing the OASA proce-dure showed a 100% implant survival rate in the atrophic posterior maxilla, which is comparable with results re-
Figure 9. Radiograph of the final implant-supported restoration
Figure 10. Clinical view of final restorationFigure 8. Periapical radiograph immediately following implant placement
Figure 7. Tension-free closure achieved with interrupted resorbable sutures

Osteotome-Assisted Sinus Augmentation Procedure for Single Implant Placement in the Atrophic Posterior Maxilla - Case Series
9SEPTEMBER 2012
ported in systematic reviews for the crestal approach, which documented implant survival rates between 93.5% and 96.4%22,23 and between 91.5% and 92.6% for the lateral window technique.2,3
However, limited accessibility and visibility for elevating the sinus membrane is one of the major limitations of the BAOSFE approach. The most common complication that oc-curs with the BAOSFE technique is the iatrogenic perforation of the Schneiderian membrane during elevation.23,27 Mem-brane perforation, according to the literature, is strongly as-sociated with the appearance of postoperative complications that include acute or chronic sinus infection, bacterial inva-sion, swelling, bleeding, wound dehiscence, loss of the graft material, and a disruption of normal sinus physiologic func-tion.8,17,21,28-35 When transcrestal “minimally invasive” sinus augmentation techniques are applied, BAOSFE, perforation of the Schneiderian membrane may not be detected unless an
intraoperative antroscopy is carried out.7 In the present study the perforation rate was 6.7%.
The primary purpose for modifying the BAOSFE with a 2-3 mm lateral window osteotomy (OASA technique) was to provide good visual access for reflecting the Schneiderian membrane at the inferior border of the sinus floor, avoid perforation of membrane and have better control of bone graft placement. Drilling with direct vision and the protec-tion of the elevated membrane with a periosteal elevator avoided the risk of an osteotome touching the membrane, which also decreased the chance of perforation related to the preparation of the osteotomy.21,24 In addition, eliminat-ing the osteotome tapping results in reduced patient dis-comfort and avoids paroxysmal positional vertigo that has been reported to be induced by head trauma with vibratory and percussive pressures on the upper maxilla.10,11 Another drawback with the BAOSFE technique is that it has been
Table 1. Data of case series with the OASA procedure
Subject # Tooth # GenderPreoperative crestal bone height (mm)
Postoperative bone height
(mm)
Gain in bone height (mm)
Implant crestal bone loss (mm)
Implant success
Membrane perforation
1 3 M 5.6 11.6 6 0.94 yes no
2 2 M 6.57 13.9 7.33 1.3 yes no
3 3 F 7 11.72 4.72 0.91 yes no
4 3 F 5.8 14.13 8.33 0.31 yes no
5 15 F 7 15.72 8.72 0.39 yes no
6 3 F 6.06 14.12 8.06 0.37 yes no
7 4 F 6.71 12.16 5.45 1.43 yes no
8 14 M 4.66 13.43 8.77 0.3 yes no
9 2 F 5.3 13.26 7.96 0.62 yes no
10 14 F 6.45 13.85 7.4 1.12 yes no
11 2 M 5.54 12.3 6.76 0.7 yes no
12 15 F 4.85 11.4 6.55 0.8 yes no
13 14 F 5.2 11.8 6.6 1.1 yes yes
14 3 M 4.3 12.4 8.1 0.9 yes no
15 15 M 5.1 12.1 7 1.2 yes no
AVE 5.74 12.93 7.18 0.82 100% 6.67%

DENTAL LEARNING
10
www.dentallearning.net
reported to be less predictable with 4 mm or less of preex-isting alveolar bone height beneath the sinus.24 When the membrane is lifted more than 3 mm, use of an endoscope is recommended due to the risk of membrane perforation, thus increasing the cost and time of the procedure.21 An average of 2-3.5 mm gain of bone height has been reported with the BAOSFE.35-36 Thus, in cases when crestal height is 4-7 mm and an implant length of 10-13 mm is desired, the BAOSFE may not achieve sufficient bone height and the risk of membrane perforation may be increased. With the OASA technique, the operator has more control of the bone graft-ing placement. Using a conventional LWSFE, bone removal
may be excessive when used for single implant placement. Utilizing the OASA technique, direct addition of the graft materials through the drilling site results in an even distribu-tion in all directions and creates a dome-shaped elevation around the implant apex. The ability to add additional bone through the window allows the graft material to surround the entire body of the implant and improves graft to bone contact.
Using the OASA technique, the size of the incision and reflection of the periosteal flap are minimized with respect to the conventional LWSFE. The lateral window is reduced, thereby decreasing the removal of bone from the lateral
Figure 11. Clinical preoperative view of hopeless 2nd premolar and missing 1st molar
Figure 13. Midcrestal incision and one vertical releasing incision on distal of 1st premolar
Figure 12. Preoperative X-ray of hopeless 2nd premolar and missing 1st molar
Figure 14. Measurement of the position of osteotomy window
Osteotome-Assisted Sinus Augmentation Procedure for Single Implant Placement in the Atrophic Posterior Maxilla - Case Series
11SEPTEMBER 2012
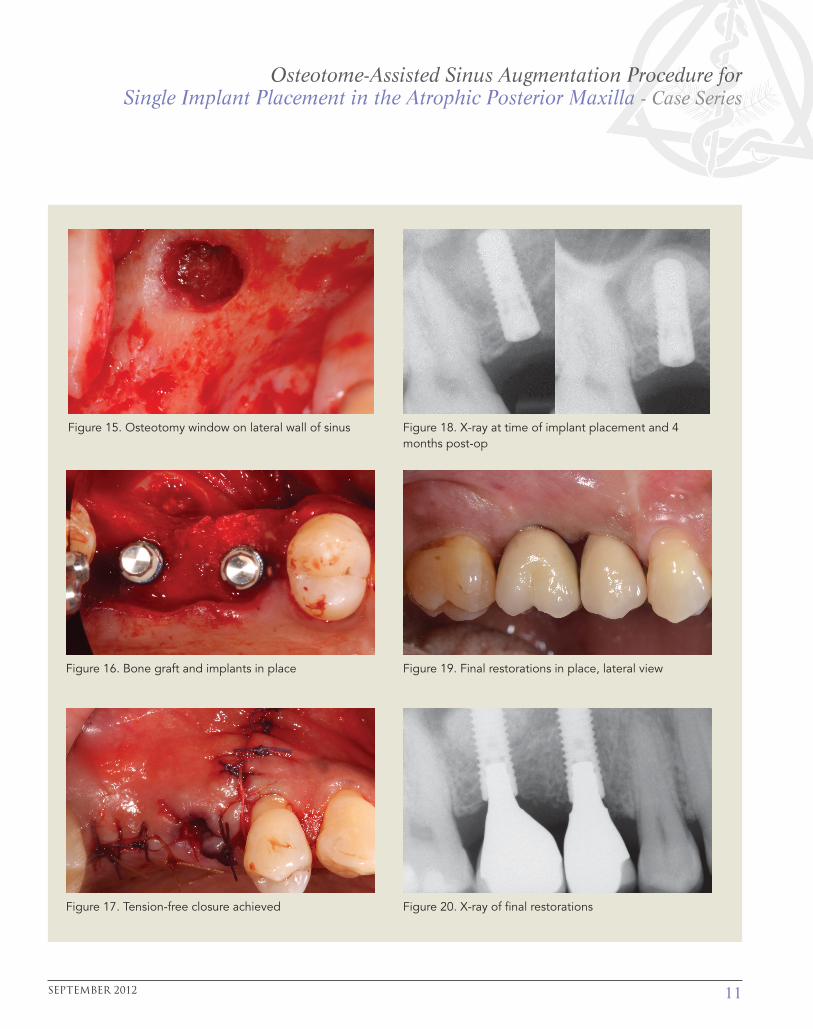
Figure 15. Osteotomy window on lateral wall of sinus Figure 18. X-ray at time of implant placement and 4 months post-op
Figure 16. Bone graft and implants in place Figure 19. Final restorations in place, lateral view
Figure 17. Tension-free closure achieved Figure 20. X-ray of final restorations

DENTAL LEARNING
12
www.dentallearning.net
sinus wall and allowing more cells from the intact sinus wall to contribute to the healing. Reduced bone removal decreases potential postoperative complications, such as swelling and pain. The limited-size lateral wall osteotomy also reduces the potential for disruption of vascular intraos-seous anastomoses in the lateral sinus wall.
Comparison of the hybrid technique (10) with the OASA procedure shows similar implant survival rates at an aver-age 27.3-month follow-up period. The hybrid technique combines a transcrestal approach with a small (3-5 mm) horizontal slot-shaped osteotomy made along the lower border of the sinus floor. The osteotomy is extended mesio-distally to include the planned implant sites. This technique can be considered a modified LWSFE when more than one implant is planned. However, the authors prefer the conven-tional LWSFE when more than one implant is required.1-4
Within the limitations of the present study with the small number of patients (15 subjects) and the relatively short follow-up period (24 months), the results showed a 100% implant success rate, a low incidence of membrane perforation (6.7%) and an average increase in bone height of 7.18 mm obtained with the OASA procedure. This technique has many advantages compared to the LWSFE and BAOSFE techniques when used for single implants or when multiple implants are placed but only one implant has deficient native bone < 7 mm that limits implant placement. (Figs. 11-20) However, additional research with more cases and long-term clinical evaluation is required to verify the results achieved in the current investigation.
References1. Boyne PJ, James RA. Grafting of the maxillary sinus floor with autogenous marrow and bone. J Oral Surg. 1980;38:613-616.
2. Wallace SS, Froum SJ. Effect of maxillary sinus augmentation on the survival of endosseous dental implants: a systematic review. Ann Periodontol. 2003;8:328-343.
3. Del Fabbro M, Testori T, Francetti L,Weinstein R. Systematic re-view of survival rates for implants placed in grafted maxillary sinus. Int J Periodontics Restorative Dent. 2004;24: 565-577.
4. Aghaloo TL, Moy PK. Which hard tissue augmentation tech-niques are the most successful in furnishing bony support for implant placement? Int J Oral Maxillofac Implants. 2007;22 Suppl:49-70.
5. Barone A, Santini S. A clinical study of the outcomes and com-plications associated with maxillary sinus augmentation. Int J Oral Maxillofac Implants. 2006;21:81-85.
6. Summers RB. The osteotome technique: Part 3—Less invasive methods of elevating the sinus floor. Compendium. 1994;15:689-708.
7. Engelke W, Schwarzwäller W, Behnsen A, Jacobs HG. Sub-antroscopic laterobasal sinus floor augmentation (SALSA): an up-to-5-year clinical study. Int J Oral Maxillofac Implants. 2003 Jan-Feb;18(1):135-143.
8. Di Girolamo M, Napolitano B, Arullani CA, Bruno E, Di Girolamo S. Paroxysmal positional vertigo as a complication of osteotome sinus floor elevation. Eur Arch Otorhinolaryngol. 2005;262:631-633.
9. Penarrocha-Diago M, Rambla-Ferrer J, Perez V, Perez-Garrigues H. Benign paroxysmal vertigo secondary to placement of maxillary implants using the alveolar expansion technique with osteotomes: a study of 4 cases. Int J Oral Maxillofac Implants. 2008;23:129-132.
10. Jung UW, Hong JY, Lee JS, Kim CS, Cho KS, Choi SH. A hybrid technique for sinus floor elevation in the severely resorbed poste-rior maxilla. J Periodontal Implant Sci. 2010 Apr;40(2):76-85.
11. Soltan M, Smiler DG. Antral membrane balloon elevation. J Oral Implantol. 2005;31(2):85-90.
12. Chen L, Cha J. An 8-year retrospective study: 1100 patients receiving 1557 implants using the minimally invasive hydraulic sinus condensing technique. J Periodontol. 2005 Mar;76(3):482-491.
13. Sotirakis EG, Gonshor A. Elevation of the maxillary sinus floor with hydraulic pressure. J Oral Implantol. 2005;31(4):197-204.
14. Suguimoto RM, Trindade IK, Carvalho RM. The use of negative pressure for the sinus lift procedure: a technical note. Int J Oral Maxillofac Implants. 2006 May-Jun;21(3):455-458.
15. Stelzle F, Benner KU. Evaluation of different methods of indirect sinus floor elevation for elevation heights of 10 mm: an experimen-tal ex vivo study. Clin Implant Dent Relat Res. 2011 Jun;13(2):124-133.
16. Toffler M. Osteotome-mediated sinus floor elevation: a clinical report. Int J Oral Maxillofac Implants. 2004 Mar-Apr;19(2):266-273.
17. Schwartz-Arad D, Herzberg R, Dolev E. The prevalence of surgi-cal complications of the sinus graft procedure and their impact on implant survival. J Periodontol. 2004 Apr;75(4):511-516.
18. Berengo M, Sivolella S, Majzoub Z, Cordioli G. Endoscopic

Osteotome-Assisted Sinus Augmentation Procedure for Single Implant Placement in the Atrophic Posterior Maxilla - Case Series
13SEPTEMBER 2012
evaluation of the bone-added osteotome sinus floor elevation procedure. Int J Oral Maxillofac Surg. 2004;33:189-194.
19. Reiser GM, Rabinovitz Z, Bruno J, Damoulis PD, Griffin TJ. Evalu-ation of maxillary sinus membrane response following elevation with the crestal osteotome technique in human cadavers. Int J Oral Maxillofac Implants. 2001;16:833-840.
20. Ferrigno N, Laureti M, Fanali S. Dental implants placement in conjunction with osteotome sinus floor elevation: a 12-year life-table analysis from a prospective study on 588 ITI implants. Clin Oral Implants Res. 2006 Apr;17(2):194-205.
21. Nkenke E, Schlegel A, Schultze-Mosgau S, Neukam FW, Wilt-fang J. The endoscopically controlled osteotome sinus floor eleva-tion: a preliminary prospective study. Int J Oral Maxillofac Implants. 2002;17:557-566.
22. Emmerich D, Att W, Stappert C. Sinus floor elevation using osteotomes: a systematic review and meta-analysis. J Periodontol. 2005 Aug;76(8):1237-1251.
23. Chiapasco M, Ronchi P. Sinus lift and endosseous implants—preliminary surgical and prosthetic results. Eur J Prosthodont Restor Dent. 1994 Sep;3(1):15-21.
24. Rosen PS, Summers R, Mellado JR, Salkin LM, Shanaman RH, et al. The bone-added osteotome sinus floor elevation technique: multicenter retrospective report of consecutively treated patients. Int J Oral Maxillofac Implants. 1999;14:853-858.
25. Tetsch J, Tetsch P, Lysek DA. Long-term results after lateral and osteotome technique sinus floor elevation: a retrospective analysis of 2190 implants over a time period of 15 years. Clin Oral Implants Res. 2010 May;21(5):497-503.
26. Horowitz RA. The use of osteotomes for sinus augmentation at the time of implant placement. Compend Contin Educ Dent. 1997 May;18(5):441-447, 450-452.
27. Fugazzotto PA, Vlassis J. Long-term success of sinus augmenta-tion using various surgical approaches and grafting materials. Int J Oral Maxillofac Implants. 1998;13:52-58.
28. Ardekian L, Oved-Peleg E, Mactei EE, Peled M. The clinical significance of sinus membrane perforation during augmentation of the maxillary sinus. J Oral Maxillofac Surg. 2006 Feb;64(2):277-282.
29. Chanavaz M. Maxillary sinus: anatomy, physiology, surgery, and bone grafting related to implantology—eleven years of surgical experience (1979-1990). J Oral Implantol. 1990;16(3):199-209.
30. Van den Bergh JP, ten Bruggenkate CM, Disch FJ, Tuinzing DB. Anatomical aspects of sinus floor elevations. Clin Oral Implants Res. 2000;11:256-265.
31. Cho SC, Wallace SS, Froum SJ, Tarnow DP. Influence of anatomy
on Schneiderian membrane perforations during sinus elevation surgery: three-dimensional analysis. Pract Proced Aesthet Dent. 2001;13:160-163.
32. Cordioli G, Mazzocco C, Schepers E, Brugnolo E, Majzoub Z. Maxillary sinus floor augmentation using bioactive glass granules and autogenous bone with simultaneous implant placement: clinical and histological findings. Clin Oral Implants Res. 2001 Jun;12(3):270-278.
33. Levin L, Herzberg R, Dolev E, Schwartz-Arad D. Smoking and complications of onlay bone grafts and sinus lift operations. Int J Oral Maxillofac Implants. 2004 May-Jun;19(3):369-373.
34. Proussaefs P, Lozada J, Kim J, Rohrer MD. Repair of the perfo-rated sinus membrane with a resorbable collagen membrane: a human study. Int J Oral Maxillofac Implants. 2004;19:413-420.
35. Cavicchia F, Bravi F, Petrelli G. Localized augmentation of the maxillary sinus floor through a coronal approach for the placement of implants. Int J Periodontics Restorative Dent. 2001 Oct;21(5):475-485.
36. Winter AA, Pollack AS, Odrich RB. Placement of implants in the severely atrophic posterior maxilla using localized management of the sinus floor: a preliminary study. Int J Oral Maxillofac Implants. 2002 Sep-Oct;17(5):687-695.
37. Tarnow DP, Wallace SS, Froum SJ, Rohrer MD, Cho SC. Histo-logic and clinical comparison of bilateral sinus floor elevations with and without barrier membrane placement in 12 patients: Part 3 of an ongoing prospective study. Int J Periodontics Restorative Dent. 2000;20:117-125.
38. Kim SM, Park JW, Suh JY, Sohn DS, Lee JM. Bone-added osteo-tome technique versus lateral approach for sinus floor elevation: a comparative radiographic study. Implant Dentistry. 2011;20(6):465-470.
39. Bain CA. Smoking and implant failure—benefits of a smoking cessation protocol. Int J Oral Maxillofac Implants. 1996;11:756-759.
WebliographyAmerican Academy of Periodontology. Position Paper. Dental Implants in Periodontal Therapy. Available at: http://www.perio.org/resources-products/ pdf/31-implants.pdf
Comprehensive Periodontal Therapy: A Statement by the American Academy of Periodontology. Available at: http://www.perio.org/resources-products/ pdf/periodontal-therapy_statement.pdf
AAP-Commissioned Review. Bone Augmentation Techniques (2007). Available at: http://www.perio.org/resources-products/pdf/lrbone-augmentation.pdf

DENTAL LEARNING
14
www.dentallearning.net
1. Sinus augmentation surgery has been reported to be a highly predictable procedure for __________ in the atrophic posterior maxilla to allow implant placement.a. filling in deficiencies of the sinus space b. increasing the available sinusc. creating bone d. a and b
2. An osteotomy “window” is made in the __________ for access, when performing the Lateral Window Sinus Floor Elevation.a. apical wall of the sinusb. lateral wall of the sinusc. nasal passaged. all of the above
3. An advantage of the Lateral Window Sinus Floor Elevation is that it allows for __________.a. direct view of the sinus cavity b. direct access to the Schneiderian membrane c. easy addition of an appropriate graft material d. all of the above
4. Elevation of the sinus membrane with a transcrestal approach to the maxillary sinus has been advocated as ‘“minimally invasive” because of __________.a. less postoperative morbidity b. minimal flap reflection c. a lower risk of periodontal diseased. a and b
5. A crestal osteotome approach involves _______ of the sinus floor. a. blind elevation b. direct visualizationc. visible reductiond. all of the above
6. Toffler, using a _________ maneuver, reported a 4.3% clinically detectable perforation rate. a. Vasallab. Valhallac. Valsalvad. none of the above
7. Membrane perforation, according to the literature, is strongly associated with _________.a. acute or chronic sinus infection b. wound dehiscence c. bacterial invasiond. all of the above
8. Patients were instructed _________ following the procedure.a. to eat a soft diet b. on oral hygiene proceduresc. on suture removald. a and b
9. One of the criteria for determining survival in the current case study was that the implant be in function for at least _________.a. 3 monthsb. 6 monthsc. 9 monthsd. 12 months
10. Using a transcrestal sinus elevation technique, perforation rates of up to _________ have been reported. a. 5%b. 15% c. 25%d. 35%
11. Radiographic bone loss was computed using magnification and measurements determined by comparison of _________ implant length. a. actual and radiographicb. actual and envisioned c. desiredd. none of the above
12. In a cadaver study, Reiser et al reported a 24% membrane perforation rate using the osteotome technique when associated with proximity to the _________.a. antral septae or the palatal canalb. antral septae or the collateral wall of the nosec. teeth or antral septaed. all of the above
13. The Bone Added Osteotome Sinus Floor Elevation (BAOSFE) procedure is considered to be _________ the Lateral Wall Sinus Floor Elevation (LWSFE) procedure, with reported similar suc-cess rates.a. a less traumatic technique thanb. as traumatic as c. a more traumatic technique thand. none of the above
14. One hour prior to surgery, patients were prescribed 2 g of amoxicillin or if allergic, 600 mg of _________.a. fibromycinb. clindamycinc. erythromycind. any of the above
15. During the osteotome-assisted sinus augmentation (OASA) procedure, a _________ incision, between the two adjacent teeth, was performed, followed by _________ releasing incision.a. midcrestal; a single horizontal b. lateral; a double verticalc. midcrestal; a single vertical d. lateral; a single vertical
CEQuizTo complete this quiz online and immediately download your CE verifica-tion document, visit www.dentallearning.net/GBR, then log into your ac-count (or register to create an account). Upon completion and passing of the exam, you can immediately download your CE verification document. We accept Visa, MasterCard, and American Express.

Osteotome-Assisted Sinus Augmentation Procedure for Single Implant Placement in the Atrophic Posterior Maxilla - Case Series
15SEPTEMBER 2012
16. Using the OASA technique, the size of the incision and reflec-tion of the periosteal flap are _________ with respect to the conventional LWSFE.a. minimizedb. maximizedc. avoidedd. none of the above
17. The integrity of the Schneiderian membrane was assessed _________ during the OASA procedure.a. radiographicallyb. manuallyc. visuallyd. all of the above
18. If during the procedure the Schneiderian membrane was found to be perforated, a wider lateral window was prepared to allow increased access to _________.a. allow for more infiltrationb. repair the membranec. remove the membraned. increase the likelihood of spontaneous repair
19. During the OASA procedure, the sinus membrane was fully elevated mesiodistally and medially over the drilling site using a _________.a. retractorb. scalpelc. sinus membrane elevatord. a and b
20. The bone graft material was placed and condensed from both the _________ directions during the OASA procedure prior to implant placement.a. incisal and midcrestalb. lateral and crestal c. vertical and crestald. all of the above
21. If an additional amount of bone graft material was required when the implant was being placed, this was added from the _________ to completely surround the implants.a. lateral windowb. vertical windowc. nasal passageway approach d. all of the above
22. Following the OASA procedure, 0.2% chlorhexidine was also prescribed starting _________ after surgery and was used twice a day for _________.a. 24 hours; 1 weekb. 48 hours; 1 weekc. 24 hours; 2 weeksd. 48 hours; 2 weeks
23. To obtain tension-free closure at the end of the OASA procedure, _________sutures were placed. a. resorbable mattressb. nonresorbable mattressc. interrupted resorbable d. interrupted nonresorbable
24. Stage 2 surgery (abutment placement) was performed _________ following implant placement.a. 1 month b. 2 months c. 3 months d. 4 months
25. Final restorations were placed _________ after stage 2 surgery. a. 1-2 monthsb. 2-3 months c. 3-4 months d. 4-6 months
26. _________ were made prior to surgery in the current case study. a. Wax-upsb. Diagnostic castsc. Surgical templates d. all of the above
27. _________ is the most common complication that occurs with the BAOSFE technique. a. Poor implant placementb. Copious bleedingc. Iatrogenic perforation of the Schneiderian membrane during
elevation d. all of the above
28. A small round-shaped osteotomy window was prepared in the lateral wall _________.a. using a high-speed round #6-#8 diamond bur with copious irrigation b. using a piezo-surgical tipc. at the height of the apex of the planned implant d. all of the above
29. Eliminating osteotome tapping during a sinus augmentation procedure _________.a. results in reduced patient discomfort b. reduces bone protruberancesc. avoids paroxysmal positional vertigo d. a and c
30. Comparison of the hybrid technique with the OASA procedure shows _________ implant survival rates.a. similarb. higherc. lowerd. none of the above
CE QUIZ

16
DENTAL LEARNINGwww.dentallearning.net
Osteotome-Assisted Sinus Augmentation Procedure for Single Implant Placement in the Atrophic Posterior Maxilla - Case Series
EDUCATIONAL OBJECTIVES• List some of the procedures available for sinus augmentation. • Review the steps required for an osteotome-assisted sinus augmentation procedure.• Describe the medications that are required post-surgery following an osteotome-assisted sinus augmentation procedure.• Review the procedure required for a bone-added osteotome sinus floor elevation and its limitations.• Compare and contrast the hybrid technique with the osteotome-assisted sinus augmentation procedure.
Please direct all questions pertaining to Dental Learning, LLC or the administration of this course to [email protected]. COURSE EVALUATION and PARTICIPANT FEEDBACK: We encourage participant feedback pertaining to all courses. Please be sure to complete the survey included with the course. Please e-mail all questions to: [email protected]. INSTRUCTIONS: All questions should have only one answer. Participants will receive confirmation of passing by receipt of a verification form. Verification forms will be mailed within two weeks after taking an examination. EDUCATIONAL DISCLAIMER: The content in this course is derived from current information and evidence. Any opinions of efficacy or perceived value of any products mentioned in this course and expressed herein are those of the author(s) of the course and do not necessarily reflect those of Dental Learning. Completing a single continuing education course does not provide enough information to give the participant the feeling that s/he is an expert in the field related to the course topic. It is a combination of many educational courses and clinical experience that allows the participant to develop skills and expertise. COURSE CREDITS/COST: All participants scoring at least 70% on the examination will receive a verification form verifying 2 CE credits. The formal continuing education program of this sponsor is accepted by the AGD for Fellowship/Mastership credit. Please contact Dental Learning, LLC for current term of acceptance. Participants are urged to contact their state dental boards for continuing education requirements. Dental Learning, LLC is a California Provider. The California Provider number is RP5062. The cost for courses ranges from $29.00 to $110.00. Many Dental Learning, LLC self-study courses have been approved by the Dental Assisting National Board, Inc. (DANB). To find out if this course or any other Dental Learning, LLC course has been approved by DANB, please RECORD KEEPING: Dental Learning, LLC maintains records of your successful completion of any exam. Please contact our offices for a copy of your continuing education credits report. This report, which will list all credits earned to date, will be generated and mailed to you within five business days of receipt. CANCELLATION/REFUND POLICY: Any participant who is not 100% satisfied with this course can request a full refund by contacting Dental Learning, LLC in writing or by calling 1-888-724-5230. © 2012
PLEASE PHOTOCOPY ANSWER SHEET FOR ADDITIONAL PARTICIPANTS.
To obtain credits:
1. Read the entire course.
2. Complete this entire answer sheet in either pen or pencil.
3. Mark only one answer for each question.
4. A score of 70% will earn your credits.
OR
For Immediate results:
1. Read the entire course
2. Go to www.dentallearning.net/OASA
3. Choose this course from the course listing
4. Log in to your account or register to create an account
5. Complete course and submit for grading to receive your CE verification document
Dental Learning, LLC
500 Craig Road, Floor One
Manalapan, NJ 07726
*If paying by credit card, please note:
Master Card | Visa | AmEx | Discover
*Account Number ______________________________
*Expiration Date _______________________________
The $29 charge will appear as Dental Learning, LLC
If paying by check, make check payable to Dental Learning, LLC.
1. A B C D
2. A B C D
3. A B C D
4. A B C D
5. A B C D
6. A B C D
7. A B C D
8. A B C D
9. A B C D
10. A B C D
11. A B C D
12. A B C D
13. A B C D
14. A B C D
15. A B C D
16. A B C D
17. A B C D
18. A B C D
19. A B C D
20. A B C D
21. A B C D
22. A B C D
23. A B C D
24. A B C D
25. A B C D
26. A B C D
27. A B C D
28. A B C D
29. A B C D
30. A B C D
COURSE EVALUATIONPlease evaluate this course using a scale of 5 to 1, where 5 is excellent and 1 is poor
1. To what extent were the course objectives accomplished overall? 5 4 3 2 1
2. Please rate your overall mastery of the educations objectives? 5 4 3 2 1
3. How would you rate the educational methods? 5 4 3 2 1
4. How do you rate the author’s mastery of the topic? 5 4 3 2 1
5. Please rate the instructor’s effectiveness. 5 4 3 2 1
6. Do you feel the references were adequate? 5 4 3 2 1
7. Would you participate in a similar course? 5 4 3 2 1
8. Was any subject matter confusing – please describe. 5 4 3 2 1
Fill in the circle of the appropriate answer that corresponds to the question on previous pages.
AGD Code: 691, 692
If you have any questions, please call Dental Learning, LLC at 1-888-724-5230.
CE ANSWER FORM (E-mail address required for processing)
All fields mArked with An Asterisk (*) Are required
Price: $29Save time and the environment by taking this course online.
*Name: Title: Specialty:
*Address: *E-mail:
*City: *State: *Zip:
*Telephone: License renewal date: AGD Identification No.