dental learning reduction ce...a mirror retraction, when administering dental local anesthesia....
TRANSCRIPT

Knowledge for Clinical Practice
WWW.DENTALLEARNING.NET
A PEER-REVIEWED PUBLICATIONA PEER-REVIEWED PUBLICATION
DENTAL LEARNING
Inside earn
1 CE CreditWritten for dentists,hygienists and assistants
Integrated Media Solutions Inc./DentalLearning.net is an ADA CERP Recognized Provider. ADA CERP is a service of the American Dental Association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not approve or endorse individual courses or instructors, nor does it imply acceptance of credit hours by boards of dentistry. Concerns or complaints about a CE provider may be directed to the provider or to ADA CERP at www.ada.org/cerp. Integrated Media Solutions Inc./Dental Learning.net designates this activity for 1 continuing education credit.
Approved PACE Program Provider FAGD/MAGD Credit Approval does not imply acceptance by a state or provincial board of dentistry or AGD endorsement.2/1/2016 - 1/31/2020Provider ID: # 346890AGD Subject Code: 132
Dental Learning, LLC is a Dental Board of California CE Provider. The California Provider # is RP5062. All of the information contained on this certi� cate is truthful and accurate. Completion of this course does not constitute authorization for the attendee to perform any services that he or she is not legally authorized to perform based on his or her license or permit type. This course meets the Dental Board of California’s requirements for 1 unit of continuing education. CA course code is 02-5062-16011.
DISCOMFORT REDUCTION DURING MAXILLARY ANESTHESIA:DISCOMFORT REDUCTION DURING MAXILLARY ANESTHESIA:A Clinical Split-Mouth Study using a High Frequency Oscillating DeviceForoud Hakim, DDS, Bernadette Alvear Fa, DDS, Karen A. Schulze, DDS, PhD, Shika Gupta BDS, DDS, Mouchumi Bhattacharyya, PhD, Marcia A. Loo, DDS

2
DENTAL LEARNING www.dentallearning.net
CE EditorFIONA COLLINS
Director of ContentBRIAN DONOHUE
Creative DirectorMICHAEL HUBERT
Art DirectorJOSEPH CAPUTO
Copyright 2016 by Dental Learning, LLC. No part of this publication may be reproduced or transmitted in any form without prewritten permission from the publisher.
500 Craig Road, First Floor, Manalapan, NJ 07726
DENTAL LEARNING
Learning Objectives
The overall goal of this article is to provide the reader with information on the management of pain and discomfort during local anesthesia. On completing this article, the reader will be able to:
1. Describe the gate-control pain theory;
2. Review the study design and study hypotheses;
3. Describe anxiety and discomfort as reported in published data; and,
4. Review the results of the clinical study and any implications for local anesthesia procedures.
SPONSOR/PROVIDER: This is a Dental Learning, LLC continuing education activity. DESIGNATION STATEMENTS: Dental Learning, LLC is an ADA CERP recognized provider. ADA CERP is a service of the American Dental Association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not approve or endorse individual courses or instructors, nor does it imply acceptance of credit hours by boards of dentistry. Dental Learning LLC designates this activity for 1 CE credit. Dental Learning is also designated as an Approved PACE Program Provider by the Academy of General Dentistry. The formal continuing education programs of this program provider are accepted by AGD for Fellowship, Mastership, and membership maintenance credit. Approval does not imply acceptance by a state or provincial board of dentistry or AGD endorsement. The current term of approval extends from 2/1/2016 - 1/31/2020. Provider ID: # 346890 Dental Learning, LLC is a Dental Board of California CE provider. The California Provider number is RP5062. This course meets the Dental Board of California’s requirements for 1 unit of continuing education. EDUCATIONAL METHODS: This course is a self-instructional journal and web activity. Information shared in this course is based on current information and evidence. REGISTRATION: The cost of this CE course is $19.00 for 1 CE Credit. PUBLICATION DATE: June, 2016. EXPIRATION DATE: May, 2019. REQUIREMENTS FOR SUCCESSFUL COMPLETION: To obtain 1 CE credit for this educational activity, participants must pay the required fee, review the material, complete the course evaluation and obtain a score of at least 70%. AUTHENTICITY STATEMENT: The images in this course have not been altered. SCIENTIFIC INTEGRITY STATEMENT: Information shared in this continuing education activity is developed from clinical research and represents the most current information available from evidenced-based dentistry. KNOWN BENEFITS AND LIMITATIONS: Information in this continuing education activity is derived from data and information obtained from the reference section. EDUCATIONAL DISCLAIMER: Completing a single continuing education course does not provide enough information to result in the participant being an expert in the field related to the course topic. It is a combination of many educational courses and clinical experience that allows the participant to develop skills and expertise. PROVIDER DISCLOSURE: Dental Learning does not have a leadership position or a commercial interest in any products that are mentioned in this article. No manufacturer or third party has had any input into the development of course content. CE PLANNER DISCLOSURE: The planner of this course, Joe Riley, does not have a leadership or commercial interest in any products that are mentioned in this article or any other products or services discussed in this educational activity. He can be reached at [email protected]. TARGET AUDIENCE: This course was written for dentists, dental hygienists, and assistants, from novice to skilled. CANCELLATION/REFUND POLICY: Any participant who is not 100% satisfied with this course can request a full refund by contacting Dental Learning, LLC in writing or by calling 1-888-724-5230. Please direct all questions pertaining to Dental Learning, LLC or the administration of this course to [email protected]. Go Green, Go Online to www.dentallearning.net to take this course. © 2016
ABOUT THE AUTHORSForoud Hakim, DDS Dr. Hakim earned his DDS in 1991 from the University of the Pacific (UP), Arthur A. Dugoni School of Dentistry and later went on to complete an MBA
from his alma mater. He is Vice Chair of the Department of Integrated Reconstructive Dental Sciences at UP and a Director in the Esthetics, Implant and Complex Care Clinic. He has lectured nationally and internationally, including seminars, continuums and hands-on workshops on topics ranging from technology, esthetic dentistry, occlusion, smile design, CAD/CAM, photography, and adhesive and composite dentistry. He also maintains a private practice in San Ramon, California. Dr. Hakim offers half-day, full-day and multi-day lectures, including customized courses and hands-on workshops.
Bernadette Alvear Fa, DDS Dr. Fa is an Assistant Professor in the Department of Integrated Reconstructive Sciences at University of the Pacific, Arthur A. Dugoni School of Dentistry.
Karen A. Schulze, DDS, PhDDr. Schulze is an Associate Professor in the Department of Integrated Recon-structive Dental Sciences, at University of the Pacific, Arthur A. Dugoni School of Dentistry.
Shika Gupta BDS, DDS Dr. Gupta is an Assistant Professor in the Department of Integrated Reconstruc-tive Dental Sciences, at the University of the Pacific, Arthur A. Dugoni School of Dentistry.
Mouchumi Bhattacharyya, PhD Dr. Bhattacharyya is a Professor of Statistics in the Department of Mathematics, at the University of the Pacific.
Marcia A. Loo, DDS Dr. Loo is an Assistant Professor with Department of Integrated Reconstructive Sciences at at University of the Pacific, Arthur A. Dugoni School of Dentistry.
Fear of pain is the primary reason for missed dental appointments, while delivery techniques and technologies have been introduced with the goal of reducing discomfort and making it possible to deliver painless local anesthesia. A number of devices have been introduced that are intended to improve patient comfort. This study of 62 subjects assessed the patient experience when local anesthesia procedures were accompanied by use of a pulsed, micro-oscillating device for patient comfort.
Abstract
Discomfort Reduction during Maxillary Anesthesia:A Clinical Split-Mouth Study using a High Frequency Oscillating Device.

3JUNE 2016
Introduction
Existing data states that the primary reason for missed dental appointments is fear of pain,1-3 and administering local anesthesia is often the
first procedure dentists and dental hygienists perform prior to delivery of care.4 Receiving injections is one of several factors that cause apprehension and anxiety in patients5-7 and may lead to systemic complications such as syncope or blood pressure elevation.8 If the patient is not adequately anesthetized, or experiences pain during the administration of anesthetic, the remaining procedure can be difficult and anxiety-ridden for both the patient and the clinician.7 This is of great concern as this anxi-ety may be passed down from generation to generation, leading to poor oral health and fewer dental visits.7,9-12 Patient comfort during the administration of anesthe-sia provides a foundation for productive and successful treatment outcomes, which in turn impacts the likelihood of patients returning to the oral healthcare setting.13,14
The introduction of topical anesthesia, improvements in needles and other novel delivery technologies have previously been reported.14,15 Delivery techniques and in-novative instrumentation have been developed in efforts to make injections of local anesthetic more comfortable for the patient.14-17 In 2010, a cordless, rechargeable, handheld device that delivers pulsed, micro-oscillations to the site where the injection is to be administered, was introduced to the dental market18 (Figure 1). The report-ed mechanism of action of this device is based on the gate-control theory of pain. The Gate control theory, first described by Melzack and Wall,18-22 indicates that the spinal cord has a “gate” that allows pain signals to travel
to the brain if carried on small nerve fibers, but does not allow pain signals to pass if carried on larger fibers. Hence, pain transmission though A-delta and C nocicep-tive fibers is depressed in the dorsal horn if nerve impuls-es are simultaneously transmitted via A-beta fibers.21
The intensity of pulsations can be increased as needed and the latex-free tips are designed with a pressure-sens-ing feature that shuts off temporarily if excessive force is applied. An LED positioned within the handle adds illumination to the injection site and an audible buzzing sound acts as an additional distractor for the patient. According to the manufacturer, this device is designed to eliminate pain when administering local anesthesia in pediatric and adult patients.18
The purpose of this split-mouth clinical study was to assess the reduction in discomfort achieved by using a high-frequency oscillating unit during the administration of maxillary local anesthesia. Multiple factors such as
Discomfort Reduction during Maxillary Anesthesia:A Clinical Split-Mouth Study using a High Frequency Oscillating Device.
Figure 1. Test device

4
DENTAL LEARNING www.dentallearning.net
discomfort, anxiety, pain, and overall satisfaction were measured. The primary hypothesis of this clinical study was that there is a significantly lower anxiety and pain level when the device is used, compared to the use of a mirror retraction, when administering dental local anesthesia.
Materials and MethodsFor this IRB-approved study (clinical trials ID:
NCT02414620), 62 patients were enrolled (35 female and 27 male). Operators in the study had successfully completed their local anesthesia curriculum and worked under the direct supervision of the approved principal investigator (faculty). Informed consent was signed by all subjects, advising them of any risks and benefits related to the study. Participation in the study was voluntary and occurred within an OSHA-compliant clinical setting.
Local Anesthesia Technique and AgentsInfiltrations are considered supraperiosteal injections
to only anesthetize the terminal branches innervating pulps and surrounding tissue limited to one or two teeth.23 In contrast, a nerve block, such as the anterior superior alveolar (ASA), is delivered close to the main nerve trunk and can produce anesthesia to a larger sur-face area. The principal investigators chose the ASA block technique in the maxillary arch to gauge “numbness” for a larger surface area while using the two different retraction modalities. The decision was made to use 2% Lidocaine with 1:100,000 epinephrine so that we could focus on patients’ perceptions with a common anesthetic along with the test device. Studies have concluded that 4% articaine produces a more significant response in the maxilla when used for buccal infiltration in comparison to 2% Lidocaine HCL with 1:100,000 epinephrine.24,25 However, we wanted patients to focus on “numbness” related to the comfort from the retraction methods ap-plied in the study. In addition, 4% solutions when used in a block have minimal, but some, risk associated with paresthesia.26
Local Anesthesia AdministrationEach patient received two injections, one on the
control side and one on the contralateral device side. A standard syringe, twenty-seven gauge short needle, and a 1.8 ml cartridge of 2% lidocaine with 1:100,000 epinephrine was used for delivery of the local anesthetic. Prior to the injection, operators felt for the infraorbital foramen extraorally for both the control site and the contralateral device site (test).
Firstly on the control side, gauze was used to dry the injection site and a small amount of topical anesthetic (20% benzocaine) was applied for one minute. Using the mouth mirror retraction technique, the operator delivered an ASA injection. The insertion site for the ASA was the mucobuccal fold above the maxillary first premolar.27 After initial penetration into the soft tissue, the needle was slowly advanced apically towards the infraorbital foramen. Once at the deposition site, 0.9 ml of anesthetic solution was administered after an aspiration test was performed. If aspiration was positive (visible blood in cartridge), the cartridge was replaced.
The soft tissue was prepared at the test site (device side) in the same manner as on the control side, including topical application of 20% benzocaine. The ASA injection was delivered by the operator using the device for retraction, again after performing an aspiration test. The same syringe and remaining anesthetic (0.9 ml) was used but the 27 gauge needle was replaced with a new one. Per the manufacturer’s training video, operators were instructed to place the oscillating device over the back part of the patient’s hand and turn the device on to give the patient an initial perception and tactile sensation of the device. Prior to the injection being administered, the device was placed in the mouth near the insertion site and kept in contact with the oral mucosa for about five seconds. Using the same injection technique as on the control side, the needle was inserted in close proximity to one of the two prong tips and advanced to the deposition site where the anesthetic was delivered. After needle removal, the pulsed, micro-oscillating device remained on

5JUNE 2016
Discomfort Reduction during Maxillary Anesthesia
1. Gender: Male ❒ Female ❒ 2a. Please rate any discomfort experienced on 2b. Please rate any discomfort experienced on right injection (Mirror) left injection (DV)
3a. Did you have any preconceived notions of 3b. Did you have any preconceived notions of the injection using the mirror for retraction? the injection using the Dental Vibe for retraction?Yes ❒ No ❒ Yes ❒ No ❒ If yes, was the anxiety level: Low ❒ Medium ❒ High ❒ If yes, was the anxiety level: Low ❒ Medium ❒ High ❒
4a. Was there penetration pain on “Mirror” side? 4b. Was there penetration pain on “DV” side?Yes ❒ No ❒ Yes ❒ No 0 If yes, was the pain: Low ❒ Medium ❒ High ❒ If yes, was the pain: LLow ❒ Medium ❒ High ❒
5a. On a scale of 1-4 rate your experience on 5b. On a scale of 1-4 rate your experience onany post op sensation you felt after the needle was any post op sensation you felt after the needle wasremoved. (Mirror) removed. (DV)No discomfort 1❒ 2❒ 3❒ 4❒ Highly uncomfortable No discomfort 1❒ 2❒ 3❒ 4❒ Highly uncomfortable
6a. How long did it take you to experience 6b. How long did it take you to experience Tingling: [ ] sec Tingling: [ ] secFeeling Fat: [ ] sec Feeling Fat: [ ] secProfound Anesthesia: [ ] sec Profound Anesthesia: [ ] sec
7. How was your experience from the two different injection methods?❒ A) The injection felt the same on both sides (No signifi cant differences)❒ B) The injection was better (more comfortable) using the Dental Vibe❒ C) The injection was worse (more pain experienced) using the Dental Vibe
8. On a scale of 1-4, 1 being extremely satisfi ed and 4 being very dissatisfi ed, please rate your experience of having the DV used on you:Extremely Satisfi ed 1❒ 2❒ 3❒ 4❒ Extremely Dissatisfi ed
9. Would you recommend or ask your dentist to use the Dental Vibe during the administration of local anesthesia?❒ D) Yes, I would want my dentist to use the Dental Vibe for all anesthetics.❒ E) Yes, I would want my dentist to use the Dental Vibe but not for all anesthetics.❒ F) No, I would not want my dentist to use the Dental Vibe during local anesthesia.❒ G) No, I was so traumatized when the Dental Vibe was used
Figure 2. Questionnaire
Evaluation of ASA Injections using Mirror Retraction versus Pulsed, Micro-oscillating Device
0No
Hurt
2Hurts
Little Bit
4Hurts
Little More
6Hurts
Even More
8Hurts
Whole Lot
10Hurts Worst
0No
Hurt
2Hurts
Little Bit
4Hurts
Little More
6Hurts
Even More
8Hurts
Whole Lot
10Hurts Worst

6
DENTAL LEARNING www.dentallearning.net
and in place for an additional fi ve seconds as instructed by the manufacturer.
Anxiety and Pain measurementAll patients received instructions and completed the
questionnaire that included the Wong-Baker28 pain rating scale as it related to the injection experience (Figure 2).
Statistical AnalysisPaired t-tests and Chi-square tests were performed for
statistical analyses, with a confi dence interval of 95% (p<0.05). Statistical analysis was performed using open source statistical software R from the Free Software Foundation’s GNU General Public License, USA, 2014.
ResultsQuestion two asked about discomfort level during
the injection of local anesthesia. There was a statistically signifi cant difference in the discomfort level during the administration of local anesthesia on the control side compared with the device side, based on the Wong-Baker Faces Pain Rating Scale (p= 0.02). More discomfort
was experienced on the control side than on the device side (Figure 3). No statistically signifi cant differences in discomfort between the control side and device side were reported by female subjects (p=0.216). Male subjects re-ported signifi cantly greater discomfort on the control side than the device side (p=0.012).
The third question enquired about preconceived no-tions regarding the injection on the respective sides. Based on the Chi-square analyses, subjects who answered that they did have preconceived notions regarding the use of mouth mirror retraction for the control side (42 out of 62) were highly likely to also report that they had pre-conceived notions regarding the use of the device on the contralateral side (39 out of 62). A similar pattern was observed for those who reported no preconceived notions for the control or device side. Comparing the control with the device side, the paired t-test found a statistically signifi -cantly greater level of anxiety in those with preconceived notions of the injection on the control side (p=0.017).
All subjects answering that they had preconceived notions were asked in a follow-up question about their anxiety level and asked to rate it as “low”, “medium” or
Figure 3. Level of discomfort experienced by subjects
Control Side Device Side
0No
Hurt
2Hurts
Little Bit
4Hurts
Little More
6Hurts
Even More
8Hurts
Whole Lot
10Hurts Worst
0No
Hurt
2Hurts
Little Bit
4Hurts
Little More
6Hurts
Even More
8Hurts
Whole Lot
10Hurts Worst

7JUNE 2016
Discomfort Reduction during Maxillary Anesthesia
“high” (Figure 4). On the control side, 64% of subjects experienced low anxiety, while 31% and 5% experienced medium and high anxiety levels, respectively. On the device side, 77% and 23% of subjects reported low and medium anxiety levels, respectively, with none reporting high anxiety.
The fourth question inquired about pain during needle penetration. It was found that subjects who reported no pain during needle penetration on the control side were highly likely to report the same for the device side (p=0.006; Figure 5). A paired t-test was conducted to compare both sides for subjects answering “yes.”
In question seven, patients were asked about their experience with both injection methods and whether there was any difference in the level of discomfort. 27 of 62 subjects experienced no difference with or without use of the device, 21 reported that local anesthesia was more comfortable on the device side, and 14 reported that it was more comfortable on the control side. Table 1 shows the distribution by gender.
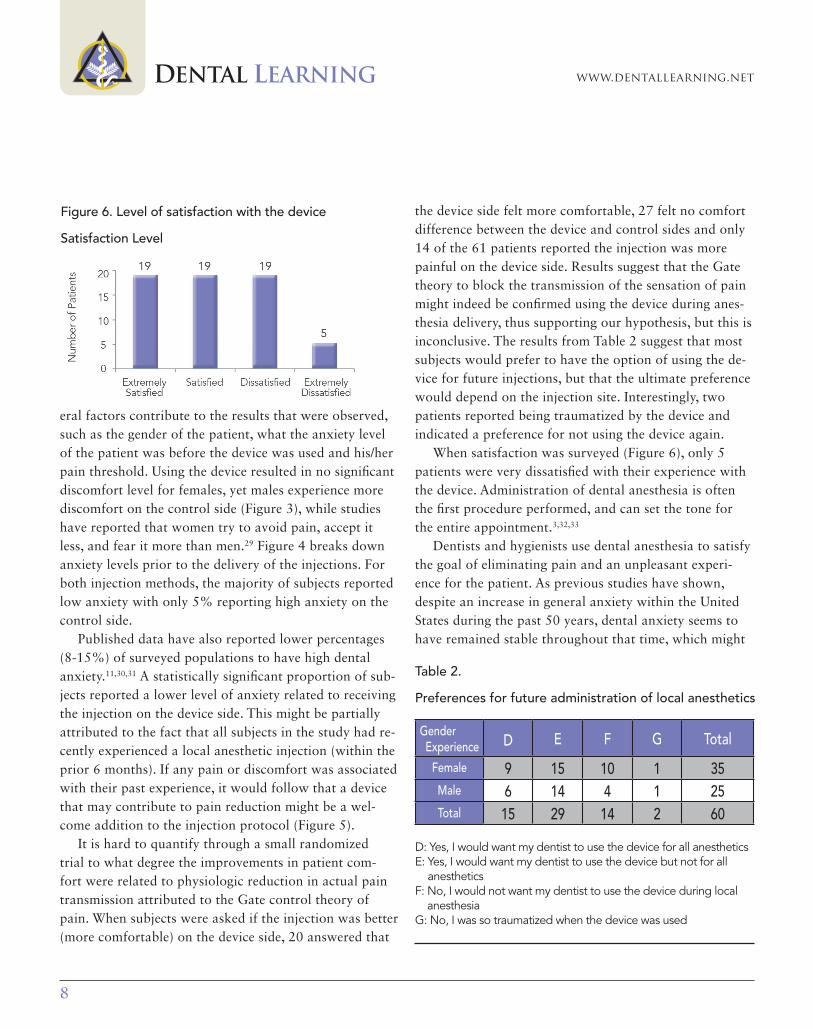
In question eight, subjects were asked to rate their overall satisfaction with the device. Findings were that 38 of 62 subjects were either extremely satisfied or satisfied, 19 were dissatisfied and 5 were extremely dissatisfied (Figure 6). In question nine, subjects were asked to report their preferences based on their experience of local an-
esthesia on the control and device sides during the study and whether they would choose device-assisted injections for future local anesthesia procedures. 44 of 62 subjects reported that they would prefer to have the device used either all or some of the time (Table 2).
DiscussionThis split-mouth study demonstrated that using a
high-frequency oscillating unit may decrease the dis-comfort associated with the delivery of local anesthesia in dental procedures. The first hypothesis that anxiety level can be lowered using the device has been confirmed, while the second hypothesis that the pain level can be reduced with the device was rejected. Interestingly, sev-
Table 1. Distribution of discomfort experience by gender
A: The injection felt the same on both sidesB: The injection was more comfortable on the device sideC: The injection was less comfortable on the device side
GenderExperience A B C Total
Female 14 13 8 35Male 13 8 6 27Total 27 21 14 62
Figure 4. Level of anxiety during administration of local anesthesia
Figure 5. Level of discomfort/pain during local anesthesia
8
DENTAL LEARNING www.dentallearning.net
eral factors contribute to the results that were observed, such as the gender of the patient, what the anxiety level of the patient was before the device was used and his/her pain threshold. Using the device resulted in no significant discomfort level for females, yet males experience more discomfort on the control side (Figure 3), while studies have reported that women try to avoid pain, accept it less, and fear it more than men.29 Figure 4 breaks down anxiety levels prior to the delivery of the injections. For both injection methods, the majority of subjects reported low anxiety with only 5% reporting high anxiety on the control side.
Published data have also reported lower percentages (8-15%) of surveyed populations to have high dental anxiety.11,30,31 A statistically significant proportion of sub-jects reported a lower level of anxiety related to receiving the injection on the device side. This might be partially attributed to the fact that all subjects in the study had re-cently experienced a local anesthetic injection (within the prior 6 months). If any pain or discomfort was associated with their past experience, it would follow that a device that may contribute to pain reduction might be a wel-come addition to the injection protocol (Figure 5).
It is hard to quantify through a small randomized trial to what degree the improvements in patient com-fort were related to physiologic reduction in actual pain transmission attributed to the Gate control theory of pain. When subjects were asked if the injection was better (more comfortable) on the device side, 20 answered that
the device side felt more comfortable, 27 felt no comfort difference between the device and control sides and only 14 of the 61 patients reported the injection was more painful on the device side. Results suggest that the Gate theory to block the transmission of the sensation of pain might indeed be confirmed using the device during anes-thesia delivery, thus supporting our hypothesis, but this is inconclusive. The results from Table 2 suggest that most subjects would prefer to have the option of using the de-vice for future injections, but that the ultimate preference would depend on the injection site. Interestingly, two patients reported being traumatized by the device and indicated a preference for not using the device again.
When satisfaction was surveyed (Figure 6), only 5 patients were very dissatisfied with their experience with the device. Administration of dental anesthesia is often the first procedure performed, and can set the tone for the entire appointment.3,32,33
Dentists and hygienists use dental anesthesia to satisfy the goal of eliminating pain and an unpleasant experi-ence for the patient. As previous studies have shown, despite an increase in general anxiety within the United States during the past 50 years, dental anxiety seems to have remained stable throughout that time, which might
Table 2.
Preferences for future administration of local anesthetics
D: Yes, I would want my dentist to use the device for all anestheticsE: Yes, I would want my dentist to use the device but not for all
anestheticsF: No, I would not want my dentist to use the device during local
anesthesiaG: No, I was so traumatized when the device was used
GenderExperience D E F G Total
Female 9 15 10 1 35Male 6 14 4 1 25Total 15 29 14 2 60
Figure 6. Level of satisfaction with the device
Satisfaction Level

9JUNE 2016
Discomfort Reduction during Maxillary Anesthesia
be attributed in part to advances in dental technologies and delivery.34 Any modality that may prove to reduce or eliminate the pain associated with dental injections, reduce the associated anxiety or improve the efficiency of anesthesia, is worthy of evaluation.13,31,32
The authors staged this study with several key points in mind:• Standardization of test and control subjects in the
randomized trial by virtue of split-mouth design.• Elimination of subject attrition via immediate response
design.• Survey questions designed to not only evaluate pain
perception via Wong-Baker faces pain rating system, but also to gauge possible placebo effect related to anxiety reduction by virtue of using a “pain reduction device.”
• Reduction of expertise bias via novice test delivery (operators with minimal and relatively equal injection experience delivered the injections, none of whom had any experience with the oscillating unit).Innovative technologies that enhance the delivery of den-
tal anesthesia have many benefits for both patient and op-erator. Further studies are needed to determine whether the oscillating device is advantageous for all dental injections.
Clinical ImplicationsWhen a pulsed, oscillating device was used, results
were mixed. Twenty-one subjects perceived less discom-fort when the device was used during local anesthesia infiltration, however 14 experienced more discomfort and 27 perceived no difference in the level of discomfort. The application reduced anxiety. Technologies that improve patient experience, related to dental anesthesia, can serve to eliminate one of the obstacles in patient care.
References1. ADA survey. Influences on dental visits. ADA News 1998;11:4.
2. Crawford S, Nissen L, Wong S, Dowling E. Quantification of patient fears regarding dental injections and patient perceptions of a local non-injectable anesthetic gel. Compend Contin Educ Dent 2005;26(2 Suppl 1):11-14.
3. Nakai Y, Milgrom P, Mancl L, Coldwell SE, Domoto PK, Ramsay DS. Effectiveness of local anesthesia in pediatric dental practice. J Am Dent Assoc 2000;131 (12):1699-1705.
4. Kaufman E, Weinstein P, Milgrom P. Difficulties in achieving local anesthesia. J Am Dent Assoc 1984;108(2):205-208.
5. Armfield JM, Milgrom P. A clinician guide to patients afraid of dental injections and numbness. SAAD Dig 2011;27:33-39.
6. Milgrom P, Coldwell SE, Getz T, Weinstein P, Ramsay DS. Four dimen-sions of fear of dental injections. J Am Dent Assoc 1997;128(6):756-766.
7. Glassman P, Peltier P. Guidelines for the administration of local anes-thesia in fearful dental patients. J Calif Dent Assoc 1995;23(9):23-26.
8. Liau FL, Kok SH, Lee JJ, Kuo RC, Hwang CR, Yang PJ, Lin CP, Kuo YS, Chang HH. Cardiovascular influence of dental anxiety during local anes-thesia for tooth extraction. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;105(1):16-26.
9. Rantavuori K, Lahti S, Hausen H, Seppä L, Kärkkäinen S. Dental fear and oral health and family characteristics of Finnish children. Acta Odontol Scand 2004;62(4):207-213.
10. Berggren U, Meynert G. Dental fear and avoidance: causes, symptoms, and consequences. J Am Dent Assoc 1984;109(2):247–251.
11. Fiset L, Milgrom P, Weinstein P, Getz T, Glassman P. Psychophysiolog-ical responses to dental injections. J Am Dent Assoc 1985;111(4):578-583.
12. Milgrom P, Vignehsa H, Weinstein P. Adolescent dental fear and control: prevalence and theoretical implications. Behav Res Ther 1992;30(4):367–373.
13. Ogle OE, Mahjoubi G. Advances in local anesthesia in dentistry. Dent Clin North Am 2011;55(3):481-499.
14. Hawkins JM, Moore PA. Local anesthesia: advances in agents and techniques. Dent Clin North Am 2002;46(4):719-732.
15. Deepika A, Rao CR, Vinay C, Uloopi KS, Rao VV. Effectiveness of two flavored topical anesthetic agents in reducing injection pain in children: a comparative study. J Clin Pediatr Dent 2012;37(1):15-18.
16. Saijo M, Ito E, Ichinohe T, Kaneko Y. Lack of pain reduction by a vibrating local anesthetic attachment: a pilot study. Anesth Prog 2005;52(2):62-64.
17. Saxena P, Gupta S, Newaskar V, Chandra A Advances in dental local anesthesia techniques and devices: an update. Natl J Maxillofac Surg 2013;4(1):19–24.
18. http://www.dentalvibe.com/index.html; accessed: May 2015.
19. Melzack R, Wall PD. Pain mechanisms: a new theory. Science 1965;11:89-90.
20. Melzack R. Recent concepts of pain. J Med 1982;13(3):147-160.
21. Wall PD. The gate control theory of pain mechanisms a re-examina-tion and re-statement. Brain 1978;101(1):1-18.
22. Melzack R. Pain: past, present and future. Can J Exp Psychol 1993;47(4):615-629.

10
DENTAL LEARNING www.dentallearning.net
23. Handbook of Local Anesthesia, 6th Ed. Malamed, S F (editor). Pub-lished by Mosby, MO, USA. Pg 188-190.
24. Srinivasan N, Kavitha M, Loganathan CS, Padmini G. Comparison of anesthetic efficacy of 4% articaine and 2% lidocaine for maxillary buccal infiltration in patients with irreversible pulpitis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;107(1):133-136.
25. Deepashri H, Kambalimath DH, Dolas RS, Kambalimath HV, Agrawal SM. Efficacy of 4% Articaine and 2% Lidocaine: A clinical study. J Maxil-lofac Oral Surg 2013;12(1):3-10.
26. Claffey E, Reader A, Nusstein J, Beck M, Weaver J. Anesthetic efficacy of articaine for inferior alveolar nerve blocks in patients with irreversible pulpitis. J Endod 2004;30(8):568-571.
27. Malamed SF. Handbook of local anesthesia. Elsevier Health Scienc-es 2014; 197.
28. Wong DL, Hockenberry-Eaton M, Wilson D, Winkelstein ML, Schwartz P. Wong’s essentials of pediatric nursing, 6th ed. St. Louis: MO, 2001; 1301.
29. Perry S, Drum M, Reader A, Nusstein J, Beck M. Effect of operator and subject gender on injection pain: a randomized double-blind study. J Endod 2015;41(2):141-145.
30. Scott DS, Hirschman R. Psychological aspects of dental anxiety in adults. J Am Dent Assoc 1982;104(1):27-31.
31. Gatchel RJ, Ingersoll BD, Bowman L, Robertson MC, Walker C. The prevalence of dental fear and avoidance: a recent study. J Am Dent Assoc 1939;107(4):609-610.
32. Changpong B, Haas DA, Locker D. Need and demand for sedation or general anesthesia in dentistry: a national survey of the Canadian population. Anesth Prog 2005;52(1):3-11.
33. Weinstein P, Milgrom P, Kaufman E, Fiset L, Ramsay D. Patient perceptions of failure to achieve optimal local anesthesia. Gen Dent 1985;33(3):218-220.
34. Smith TA, Heaton LJ. Fear of dental care: are we making any prog-ress? J Am Dent Assoc 2003;134(8):1101-1108.
35. Bågesund M, Tabrizi P. Lidocaine 20% patch vs lidocaine 5% gel for topical anaesthesia of oral mucosa. Int J of Paediatr Dent 2008;18(6):452-460.
36. Touyz LZ, Lamontagne P, Smith BE. Pain and anxiety reduction using a manual stimulation distraction device when administering local anal-gesia oro-dental injections: a multi-center clinical investigation. J Clin Dent 2004;15(3):88-92.
WebliographyDeepashri H, Kambalimath DH, Dolas RS, Kambalimath HV, Agrawal SM. Efficacy of 4% Articaine and 2% Lidocaine: A clinical study. J Max-illofac Oral Surg 2013;12(1):3-10. Available at: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3589513/.
Malamed SF, Gagnon S, Leblanc D. A comparison between artic-aine HCl and lidocaine HCl in pediatric dental patients. Pediatr Dent 2000;22(4):307-311. Abstract available at: http://www.ncbi.nlm.nih.gov/pubmed/10969438.
Sierra Rebolledo A, Delgado Molina E, Berini Aytís L, Gay Esco-da C. Comparative study of the anesthetic efficacy of 4% articaine versus 2% lidocaine in inferior alveolar nerve block during surgical extraction of impacted lower third molars. Med Oral Patol Oral Cir Bucal 2007;12(2):E139-44. Available at: http://www.medicinaoral.com/pubmed/medoralv12_i2_p139.pdf.

11JUNE 2016
Discomfort Reduction during Maxillary Anesthesia
1. Receiving injections is one of several factors that can __________.a. significantly lengthen treatment timeb. cause apprehension and anxiety in patientsc. significantly decrease mobilityd. none of the above
2. The Gate control theory indicates that the spinal cord has a “gate” that allows pain signals to travel to the brain if __________.
a. carried on small nerve fibersb. carried on large nerve fibersc. supplemented by auxiliary fibersd. a and b
3. Pain transmission though A-delta and C nociceptive fibers is depressed in the dorsal horn if nerve impulses are simultaneously transmitted via C-delta fibers.
a. Trueb. False
4. In the current study, statistically significant differences in discom-fort were found between the control side and the device side in _______.
a. female subjectsb. male subjectsc. older adultsd. children
5. When asked to report their preferences for future local anesthe-sia procedures, __________ subjects reported that they would prefer to have the device used either all or some of the time.
a. 24 of 42b. 24 of 62c. 34 of 62d. 44 of 62
6. In the current study, it was found that subjects who reported no pain during needle penetration on the control side were highly likely to report the same for the device side.
a. Trueb. False
7. The findings from this split-mouth study demonstrated that using a high-frequency oscillating unit __________.
a. may decrease the discomfort associated with the delivery of local anesthesiab. may lower a patient’s anxiety levelc. can reduce the pain level d. a and b
8. According to the authors, modalities that may __________ associ-ated with dental injections, are worthy of evaluation.
a. prove to reduce or eliminate the painb. reduce the anxiety levelc. improve the efficiency of anesthesiad. all of the above
9. Reduction of expertise bias in this study was obtained by using __________ for dental anesthetic injection.
a. operators with minimal and relatively equal injection experienceb. operators with no injection experiencec. recent post-graduatesd. operators with experience using the test device
10. When a pulsed, oscillating device was used, there was __________ for dental anesthetic injection with no adverse effects.a. an overall negative responseb. no responsec. an overall positive responsed. no positive response
CEQuiz To complete this quiz online and immediately download your CE verification document, visit www.dentallearning.net/MLA-ce, then log into your account (or register to create an account). Upon completion and passing of the exam, you can immediately download your CE verification document. We accept Visa, MasterCard, Discover, and American Express.

1. A B C D
2. A B C D
3. A B C D
4. A B C D
5. A B C D
6. A B C D
7. A B C D
8. A B C D
9. A B C D
10. A B C D
11. A B C D
12. A B C D
13. A B C D
14. A B C D
15. A B C D
16. A B C D
17. A B C D
18. A B C D
19. A B C D
20. A B C D
21. A B C D
22. A B C D
23. A B C D
24. A B C D
25. A B C D
26. A B C D
27. A B C D
28. A B C D
29. A B C D
30. A B C D
31. A B C D
32. A B C D
33. A B C D
34. A B C D
35. A B C D
36. A B C D
37. A B C D
38. A B C D
39. A B C D
40. A B C D
41. A B C D
42. A B C D
43. A B C D
44. A B C D
45. A B C D
46. A B C D
47. A B C D
48. A B C D
49. A B C D
50. A B C D
www.dentallearning.netCE ANSWER FORM (E-mail address required for processing)
*Name: Title: Speciality
*Address: NPI No.
*City: *State: *Zip: AGD Identification No.
*E-mail:
*Telephone: License Renewal Date:
Please direct all questions pertaining to Dental Learning, LLC or the administration of this course to [email protected]. COURSE EVALUATION and PARTICIPANT FEEDBACK: We encourage participant feedback pertaining to all courses. Please be sure to complete the evaluation included with the course. INSTRUCTIONS: All questions have only one answer. Participants will receive confirmation of passing by receipt of a verification certificate. Verification certificates will be processed within two weeks after submitting a completed examination. EDUCATIONAL DISCLAIMER: The content in this course is derived from current information and research based evidence. Any opinions of efficacy or perceived value of any products mentioned in this course and expressed herein are those of the author(s) of the course and do not necessarily reflect those of Dental Learning. Completing a single continuing education course does not provide enough information to make the participant an expert in the field related to the course topic. It is a combination of many educational courses and clinical experience that allows the participant to develop skills and expertise. COURSE CREDITS/COST: All participants scoring at least 70% on the examination will receive a CE verification certificate. Dental Learning, LLC is an ADA CERP recognized provider. Dental Learning, LLC is also designated as an Approved PACE Program Provider by the Academy of General Dentistry. The formal continuing education programs of this program provider are accepted by AGD for Fellowship, Mastership, and membership maintenance credit. Please contact Dental Learning, LLC for current terms of acceptance. Participants are urged to contact their state dental boards for continuing education requirements. Dental Learning, LLC is a California Provider. The California Provider number is RP5062. The cost for courses ranges from $19.00 to $90.00. RECORD KEEPING: Dental Learning, LLC maintains records of your successful completion of any exam. Please contact our offices for a copy of your continuing education credits report. This report, which will list all credits earned to date, will be generated and mailed to you within five business days of request. Dental Learning, LLC maintains verification records for a minimum of seven years. CANCELLATION/REFUND POLICY: Any participant who is not 100% satisfied with this course can request a full refund by contacting Dental Learning, LLC in writing or by calling 1-888-724-5230. Go Green, Go Online to www.dentallearning.net to take this course. © 2016
PLEASE PHOTOCOPY ANSWER SHEET FOR ADDITIONAL PARTICIPANTS.
EDUCATIONAL OBJECTIVES• Define the elements of the chain of infection;• Delineate and describe the differences in the processing of critical, semicritical and noncritical instruments;• Review the use of presoaks and cleaning of instruments;• List and describe heat sterilization options and appropriate sterilization packaging; and• Review the uses and purposes of chemical and biological indicators.
If you have any questions, please email Dental Learning at [email protected] or call 888-724-5230.
COURSE SUBMISSION: 1. Read the entire course.2. Complete this entire answer sheet in
either pen or pencil.3. Mark only one answer for each question.4. Mail or fax answer form. For immediate results:1. Read the entire course.2. Go to www.dentallearning.net/IPI-ce.3. Log in to your account or register to create an
account.4. Complete course and submit for grading to
receive your CE verification certificate.
A score of 70% will earn your credits.
Dental Learning, LLC500 Craig Road, First FloorManalapan, NJ 07726
*If paying by credit card, please note:MasterCard | Visa | AmEx | Discover
*Account Number
______________________________________________
*Expiration Date
______________________________________________
The charge will appear as Dental Learning, LLC.
If paying by check, make check payable to Dental Learning, LLC.
ALL FIELDS MARKED WITH AN ASTERISK (*) ARE REQUIRED
QUIZ ANSWERSFill in the circle of the appropriate answer that corresponds to the question on previous pages.
AGD Codes: 132
Price: $19 CE Credits: 1Save time and the environment by taking this course online.
COURSE EVALUATIONPlease evaluate this course using a scale of 3 to 1, where 3 is excellent and 1 is poor.
1. Clarity of objectives . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 2 1
2. Usefulness of content . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 2 1
3. Benefit to your clinical practice . . . . . . . . . . . . . . . . . . . . 3 2 1
4. Usefulness of the references . . . . . . . . . . . . . . . . . . . . . . 3 2 1
5. Quality of written presentation . . . . . . . . . . . . . . . . . . . . 3 2 1
6. Quality of illustrations . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 2 1
7. Clarity of quiz questions . . . . . . . . . . . . . . . . . . . . . . . . . 3 2 1
8. Relevance of quiz questions . . . . . . . . . . . . . . . . . . . . . . 3 2 1
9. Rate your overall satisfaction with this course . . . . . . . . 3 2 1
10. Did this lesson achieve its educational objectives? Yes No
11. Are there any other topics you would like to see presented in the future? __________________________________________________________________________
_______________________________________________________________________________________
Anesthesia Paper – Clinical Split Mouth Study