dentistry and endocrinology
TRANSCRIPT

Good morning

ENDOCRINOLOGY

Introduction Hormones
-chemistry of hormones
-hormone receptors
-mechanism of action Pituitary gland Thyroid gland Endocrine functions of Pancreas Adrenal cortex Adrenal medulla Endocrine functions of other organs Local hormones
CONTENTS

The various physiological activities in our body are controlled by
some chemical substances called chemical messengers or
Chemical mediators.
Chemical messengers
Secreted by Endocrine glands, nerve endings, cells of other
tissues carry the message (signal) from the controlling cells
(signaling cells) to the target cells.
Introduction
Chemical messengers
Classical hormones local hormones
Recent classification of these messengers
-Endocrine messengers
-Neurocrine messengers
-Paracrine messengers
-Autocrine messengers

Endocrine glands
Is a chemical substance that is secreted into internal body
fluids by one cell or a group of cells and has a physiological
control effect on other cells of the body.
Chemistry of hormones
- Hormones are classified depending on the chemical nature
Steroid hormones
Protein hormones
Derivatives of the amino acid- tyrosine
Hormones

Hormone receptors The receptors of the hormones are
large proteins present in the target cells.
Each receptor is highly specific for one single hormone
Situation of hormone receptors
-Cell membrane
-Cytoplasm
-Nucleus
Regulation of hormone receptors
-Up regulation
-Down regulation
Mechanism of hormonal action
1. By altering the permeability of cell membrane
2. By altering the intracellular enzyme
3. By activating the gene
The neurotrasmitter substances in a synapse or neuromuscular junction act by changing the permeability of postsynaptic membrane.
example: NMJ
1. By altering the permeability of cell membrane
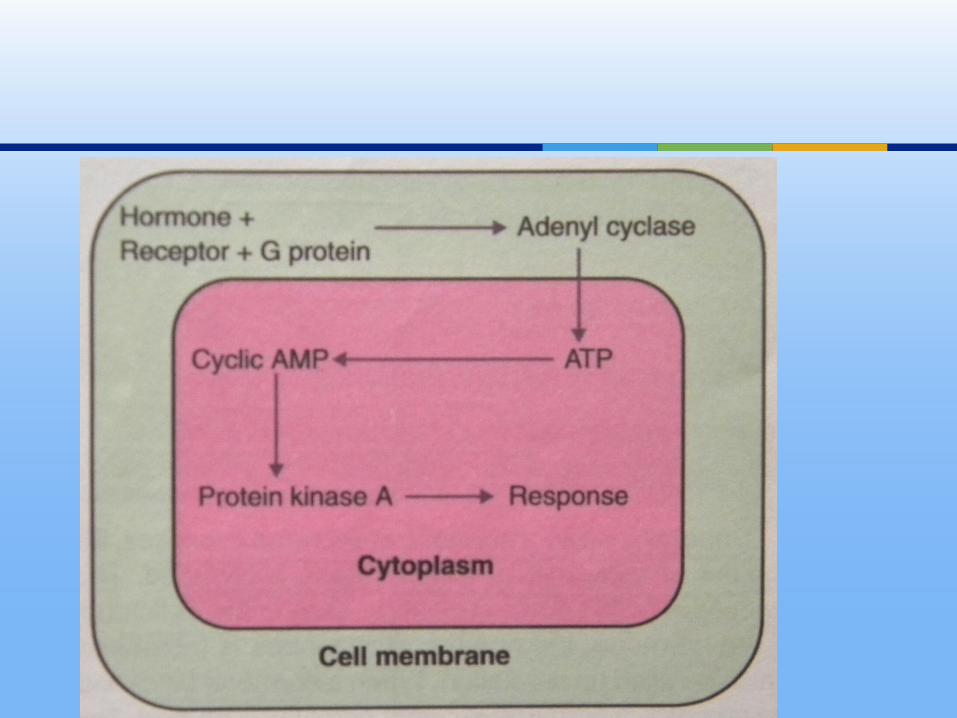
Protein hormones and catecholamines The hormone, which acts on the target cell, is called first
messenger HR-complex activates the enzymes of the cell and causes the
formation of another substance called second messenger or intracellular hormonal mediator.
- Cyclic AMP- Calcium Ions and Calmoduline- Inositol triphosphate (IP3)- Diacylglycerol (DAG)- Cyclic Guanosine Monophosphate (cGMP)
2. By Activating the Intracellular enzymes

Thyroid and steroid hormones
3. By Activating on genes
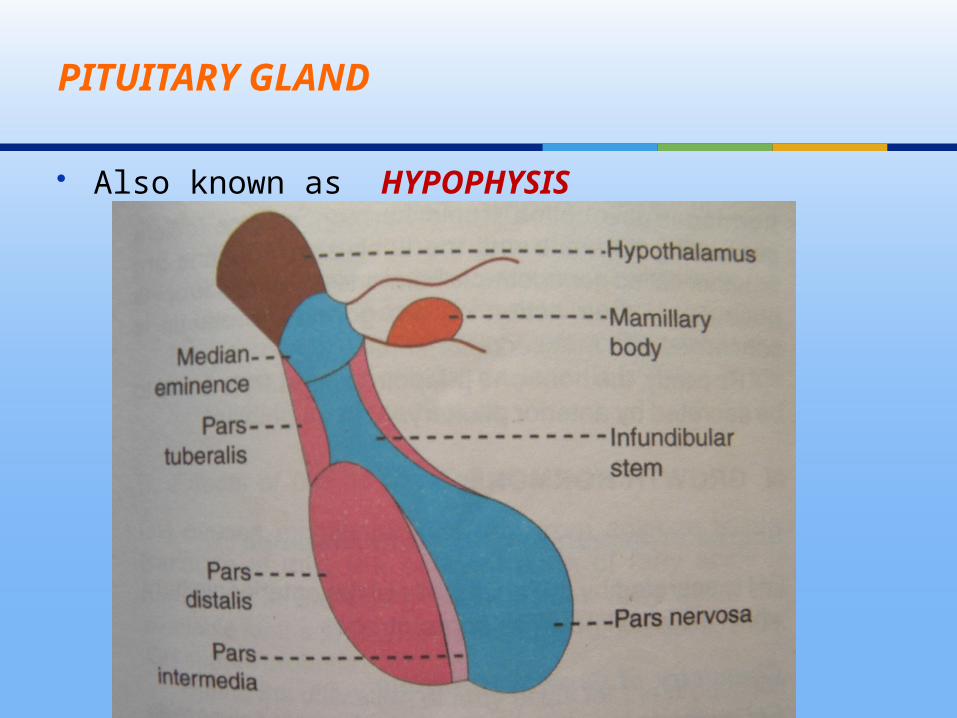
Also known as HYPOPHYSIS
PITUITARY GLAND

Regulation of secretion

HYPOTHALAMO HYPOPHYSEAL PORTAL SYSTEM

Releasing and Inhibitory hormones
GH-RH
GHRP
TRH
CRH
GnRH
GHIH
PIH

Growth hormone
Secreted by the acidophils, known as somtotropes
Is a protein, having a single chain polypeptide with
191 amino acids, 21,500mol wt
Responsible for general growth of the body
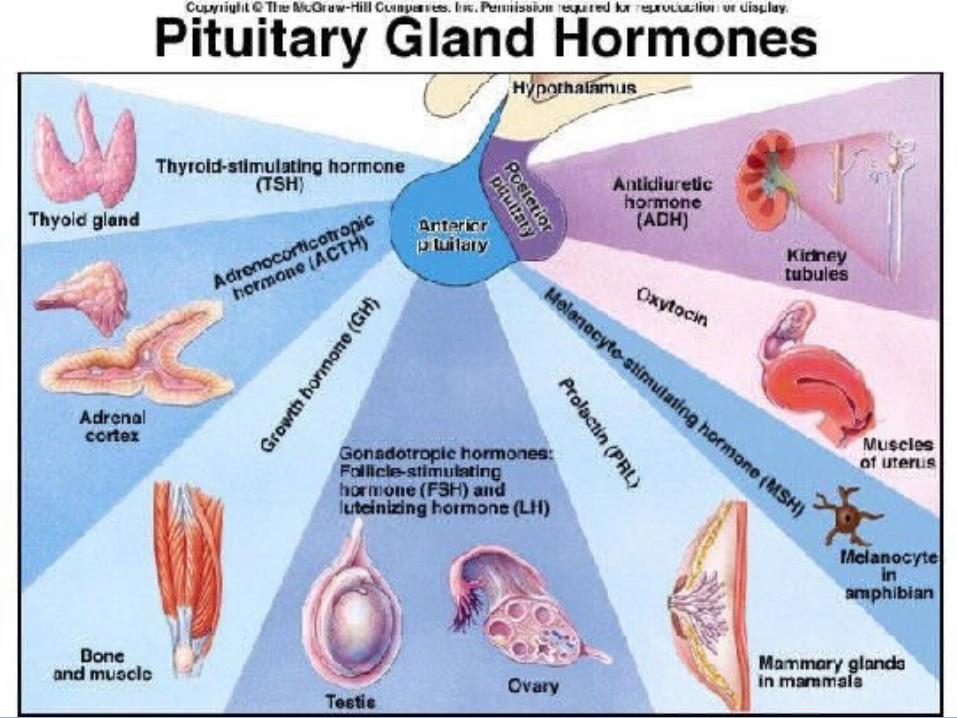
Anterior pituitary hormones

Effects of GH
Effects of GH on protein metabolism
Increases the amino acid transport through the cell membrane
Increases the RNA translation
Increases transcription of DNA to RNA
Decreases catabolism of protein

Effects of GH on fat metabolism
Excess GH
Fat mobilization from adipose tissues
Large quantities of acetoacetic acid formed by liver and released into body fluids
(Ketosis)
Resulting in fatty liver

Effects of GH on carbohydrate metabolism
GH causes conservation of glucose, by following mechanisms
-Decrease in the peripheral utilization of glucose for the production of energy
-Increase in the deposition of glycogen in the cells
- Diabetogenic effect of GH

Effect of GH on bones
GH increases the growth of the skeleton
Increase in the protein deposits by chondriocytes and osteogenic cells
And it causes conversion of chondriocytes into osteogenic cells

Mode of action GH on Bones and Metabolism
Thyroid Stimulating Hormone (TSH)
Necessary for the growth and secretory actions of thyroid gland
Adrenocorticotropic Hormone (ACTH)
Necessary for the structural integrity and the secretory activity of adrenal cortex

Follicle Stimulating Hormone
In males it accelerates spermeogenesis in combination with
testosterone
In females it is responsible for development of graafian follicle from primordial follicle
Secretion of estrogen

Luteinizing Hormone
In males it is known as ICSH
In females along with FSH it causes maturation of vesicular follicle
Ovulation
Formation and secretory functions of corpus luteum

Prolactin
Secretion of milk
β-Lipotropin
Mobilizes fat from adipose tissue and promotes lipolysis
Anti Diuretic Hormone (vasopressin) Secreted by supra optic nucleus, and paraventricular nucleus Is a polypeptide with 9 amino acids
Actions Reabsorption of water from DCT and Collecting duct In large amounts, it causes constriction of arteries
Posterior pituitary hormones

Oxytocin Secreted by paraventricular nucleus and in small quantity by
supraoptic nucleus Is a ploypeptide with 9 aminoacids
Actions Causes contraction of myoepithelial cells- ejection of milk On pregnant uterus causes contraction and helps in the
expulsion of fetus Causes contraction in non pregnant uterus and facilitate the
transport of sperms in female genital tract
Anterior pituitary Posterior pituitary
DISORDERS OF PITUITARY GLAND
HypersecretionGigantism
AcromegalyAcromegalic
gigantismCushing’s disease
Hyposecretiondwarfism
AcromicriaSimmond’s disease
orPituitary cachexia
HypersecretionSyndrome of inappropriate
hypersecretion of ADH (SIADH)
HyposecretionDiabetes insipidus
Pre-puberty: Gigantism
An overproduction of growth hormone before epiphyseal closure.
These children grow to be over 7 ft (213 cm) in height and have disproportionately long limbs
-bone growth, > 7 ft. tall


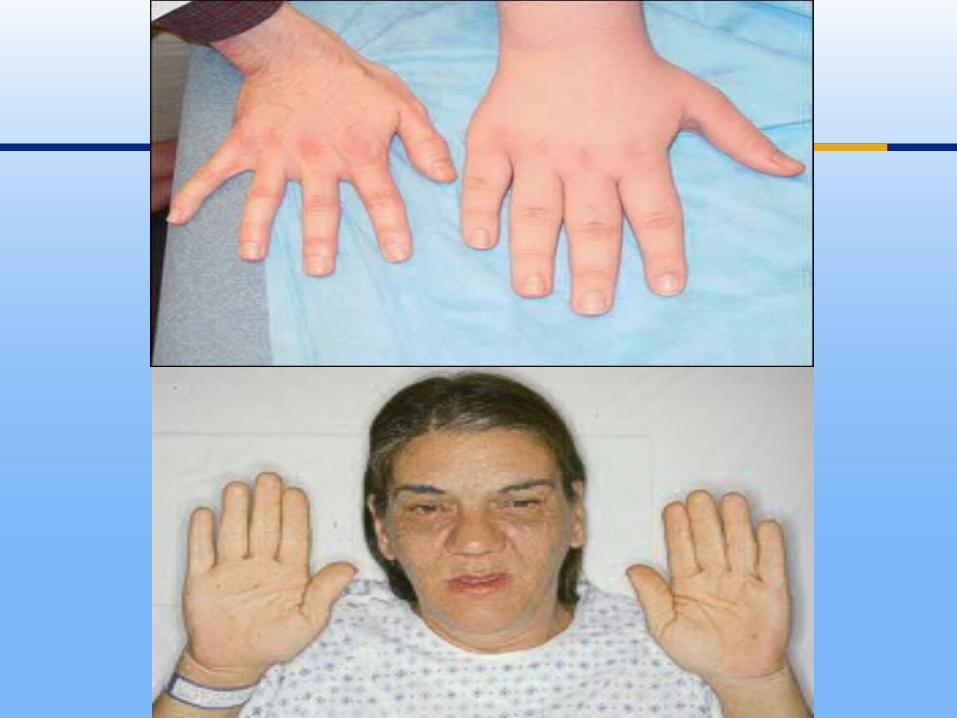
Post-puberty: Acromegaly
Some tissues still grow even after puberty :
cartilage in nose, hands, feet, ridges of eyebrow,
chin, tongue
Metabolic effects:
constant increase in blood sugar
increased insulin type 2 diabetes.
Increase muscle in tunica media narrowing of arteries,
heart attack

Excess growth hormone produced after puberty has little effect on
the growth of the skeleton, but it results in a disease affecting
terminal skeletal structures known as acromegaly

Dwarfism
Deficiency of GH in immature
individual. A deficiency of growth hormone secretion before
puberty results in pituitary dwarfism.
Pituitary dwarfs, who can be as little as 3 to 4 ft (91–122 cm) tall,
are generally well proportioned except for the head, which may be
relatively large when compared to the body.

Unlike cretins, whose dwarfism is caused by a deficiency of
thyroxine, pituitary dwarfs are not mentally retarded;
They are often sexually immature.
They can be treated by injections of synthetic growth hormone,
somatropin, which are produced by genetically engineered
bacteria.
Eruption timing and the shedding is delayed
Clinical crowns appear smaller than normal
The dental arch is smaller than normal so crowding
There is no shortening in length of anatomic crown as expected though the roots may be smaller
Dwarfism due to deficiency of somatomedin C known as Lorain dwarfism
Recombinant human GH (RnGH)
First used to treat GHD
Supply of RnGH has made it possible to supply GH for general shortness
Metabolic side effects:
- Acceleration of puberty
- Pancreatitis
- Intracranial hypertension
- May ↑ risk of leukemia and stroke
Acromicria
Deficiency of GH in adults
Due to atrophy of acidophilic cells, tumor of chromophobes and panhypopituitarism
Atrophy or thinning of extremities
Persons become lethargic and obese
Loss of sexual functions

Simmond’s disease (pituitary cachexia)
Occurs mostly in panhypopituitarism
Due to atrophy or degeneration of anterior pituitary
Rapidly developing senile decay
Loss of hair and tooth
Skin of face becomes dry and wrinkled
Syndrome of inappropriate Hypersecretion of ADH (SIADH)
Excessive secretion of ADH
The cells during cerebral tumors, lung tumors and lung
cancers secrete ADH
Sodium concentration in ECF reduced to 110 mEq/L. (Normal-142mEq/L)
When it falls below, patient may die because of convulsions and coma

Thyroid is an endocrine gland situated at the root of the neck on either side of trachea.
THYROID GLAND

Composed of large number of follicles Follicular cavity is filled with a colloidal substance known as
thyroglobulin from which secretes T3 and T4 Between the follicles, the parafollicular cells are present,
which secretes calcitonin
Histology

Thyroid hormones
T4- tetraiodothyronine
(thyroxine) T3- triiodothyronine is more potent Calcitonin
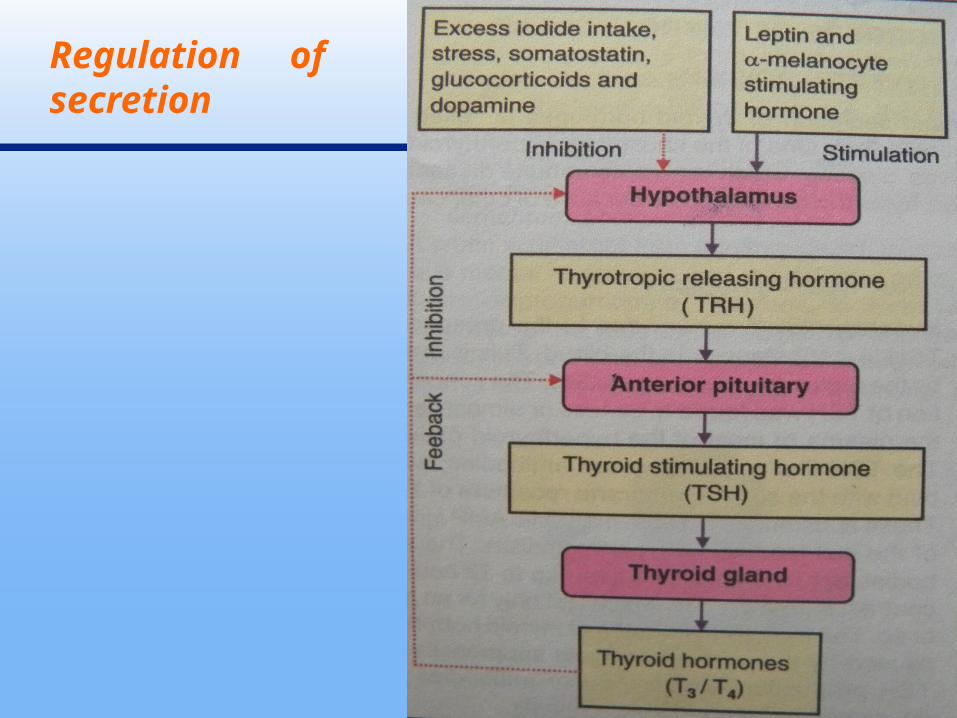
Regulation of secretion

Effect on basal metabolic rate
-It increases the metabolic rate as much as 60%-100% above
normal in all tissues except brain, retina, spleen, testes and lungs
-T3 stimulates increase in Oxygen uptake by all tissues
( metabolism of all tissues is increased)
Functions of thyroid hormones

Effect on protein metabolism
The protein synthesis is accelerated by the following ways:
-increasing the Translation of RNA
-increasing the Transcription of DNA to RNA
-increasing the activity of Mitochondria
-increasing the activity of cellular enzymes

Effect on carbohydrate metabolism
absorption of glucose from GIT uptake through cell membrane glycogenolysis, gluconeogenesis
Effect on fat metabolism
Mobilization of fat from adipose tissues and fat depots. Increases deposition of fat in liver, decreases plasma
cholesterol level

Decrease in vitamin levels due to their utilization during formation of enzymes
Increase in body temperature due to increased metabolic processes and BMR
Is important hormone to promote growth and development of brain during fetal and few years of postnatal life
Effects on CVS- HR
Force of contraction
BP

Effect on respiration Increases rate and force of respiration
Effect on GIT Increases appetite and food intake Increases secretions and movements
Effect on skeletal muscle With slight increase, muscle work with more vigor
Excessive secretion causes thyrotoxic myopathy
Effect on sleep Hypo secretion causes excessive sleep (somnolence)
Effect on sexual function Hyposecretion causes complete loss of libido Hypersecretion causes impotence
Disorders of thyroid hormones
1. Hyperthyroidism
Causes:- Grave’s Disease (commonest cause)
- Multinodular Goiter
- Thyroiditis and Others


Dental considerations
Patients with untreated hyperthyroidism can be difficult to deal with a result of heightened anxiety and irritability.
The sympathetic overactivity may lead to fainting.
Local anesthesia is the main means of pain control.
Conscious sedation is frequently desirable to control excessive anxiety. Benzodiazepens may potentiate antithyroid drugs, and therefore nitrous oxide, which is more rapidly controllable is probably safer.
Povidone iodine and similar compounds are avoided

Carbimazole occasionally causes agranulocytosis, which may cause oral or oropharyngeal ulcerations.
Otherwise treated thyrotoxic patient presents no special problems in dental treatment.
After treatment of hyperthyroidism the patients are at risk for developing hypothyroidism, which may pass unrecognized.

2. Hypothyroidism
I. Primary Hypothyroidism
Secondary Hypothyroidism
II Cretinism
Myxedema.
Cretinism
Signs like sluggish movement and croaking sound while
crying.
Retarded mental, physical and sexual growth
Because of large tongue, guttural breathing may present which
sometimes choke the baby

Myxedema
-Swelling of the face
-Bagginess under the eyes
-Non pitting type of edema due to accumulation of proteins with
hyaluronic acid and chondroitin sulfate
-Other symptoms of hypothyroidism-


Dental considerations :
The main danger is of precipitating myxoedema coma
by use of sedatives (including diazepam or midazolam), opioid
analgesics or tranquilizers.
Therefore these should be avoided or given in low dose.
Local anesthesia is satisfactory for pain control.
Conscious sedation can be carried out with nitrous oxide and oxygen.

General anesthesia may be complicated because of possible
ischemic heart disease and the danger of coma.
GA must be delayed until thyroxine has been started.

Endocrine function of pancreas is performed by the islets of Langerhans
4 types of cells of islets of langerhans
- A (alpha) GLUCAGON
- B (beta) INSULIN
- D (delta) SOMATOSTATIN
- F (PP) PANCREATIC POLYPEPTIDE
PANCREAS

Insulin is secreted by β- cells of islets of langerhans
Is a polypeptide with mol wt 5808, has two amino acid chains linked by disulfide bridges, alpha chain contains 21 and beta chain contains 30 amino acids.
Insulin
Effect on carbohydrate metabolism
High carbohydrate diet
Insulin secretion
Increased permeability of cell membrane
Transport of glucose from blood into cell
Promotes conversion of glucose to glycogen and stored in
muscle and liver Inhibits glycogenolysis, gluconeogenesis
Actions
Effect on protein metabolism Insulin accelerates synthesis and storage of proteins
Effect on fat metabolism Insulin activates the enzymes which converts glucose into
fatty acid and triglycerides Promotes the storage of fat in adipose tissue
Effect on growth Anabolism of protein -> promotes growth
Secreted by α-ells of islets of langerhans
It is a polypeptide contains 29 amino acids, mol wt 3485.
Actions of glucagon Increases glycogenolysis, gluconeogenesis
Shows lipolytic and ketogenic actions
Secretion of bile Secretion of gastric juice
Glucagon

Secreted by Hypothalamus, δ-cells of islets of langerhans, δ-cells in stomach, small intestine
Is a polypeptide, 14(pancreas) and 28(intestine) amino acids
Inhibits- glucagon, insulin, GH
Decreases the motility of stomach, duodenum, gallbladder
Increased secretion seen with increase in glucose, amino acids, cholecystokinin
Somatostatin

Secreted by Fcells or PPcells
Polypeptide with 36 amino acids
Increase secretion of glucagon
Increase secretion stimulated by presence of chyme containing more proteins
Pancreatic polypeptide

Type-1 (IDDM)
Due to deficiency of insulin
Not associated with obesity but associated with acidosis or ketosis
Occurs before 40 years- juvenile diabetes
Causes degeneration, destruction by viral infection, congenital disorder, auto immune disease of beta cells
Diabetes mellitus
Type-2 (NIDDM)
Occurs after 40 years- maturity onset diabetes
Associated with obesity
Causes- absence or reduced number of insulin receptors
Endocrine disorders like gigantism, acromegaly and cushing’s syndrome- secondary diabetes

Loss of glucose in urine
Osmotic diuresis
Polyuria, polydipsia, polyphagia
Asthenia(loss of strength)
Acidosis, circulatory shock, coma
Chronic diabetes- diabetic retinopathy- diabetic nephropathy- diabetic neuropathy
Signs and symptoms

Excessive secretion of insulin
Occurs due to tumor of beta cells
Signs and symptoms- hypoglycemia, neuroglycopenic symptoms like clonic convulsions and unconsciousness, coma
Hyperinsulinism

Good morning
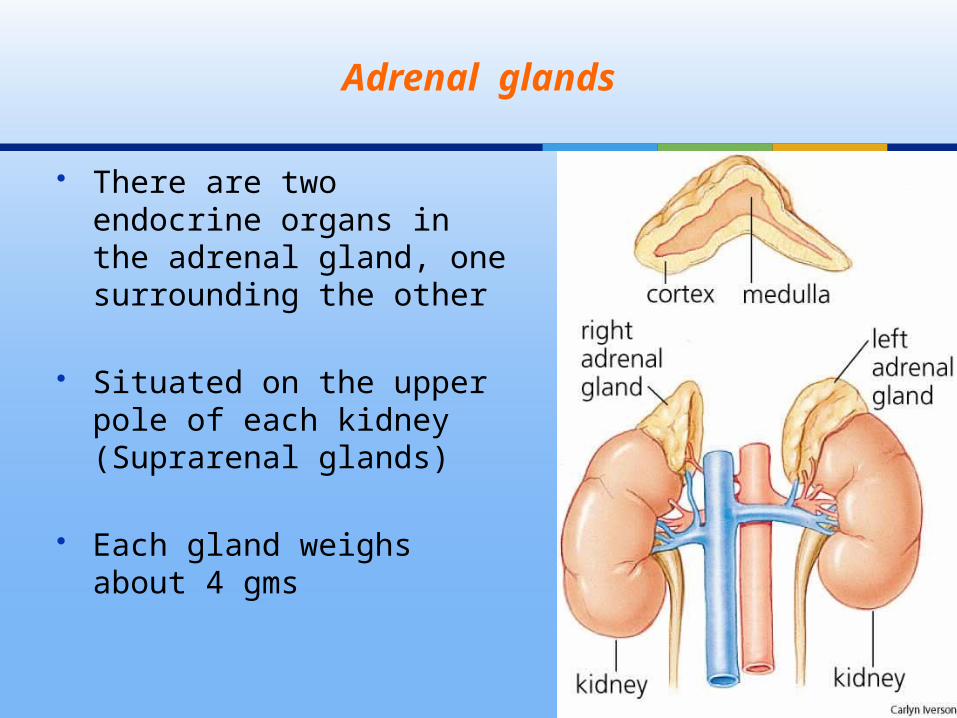
There are two endocrine organs in the adrenal gland, one surrounding the other
Situated on the upper pole of each kidney (Suprarenal glands)
Each gland weighs about 4 gms
Adrenal glands
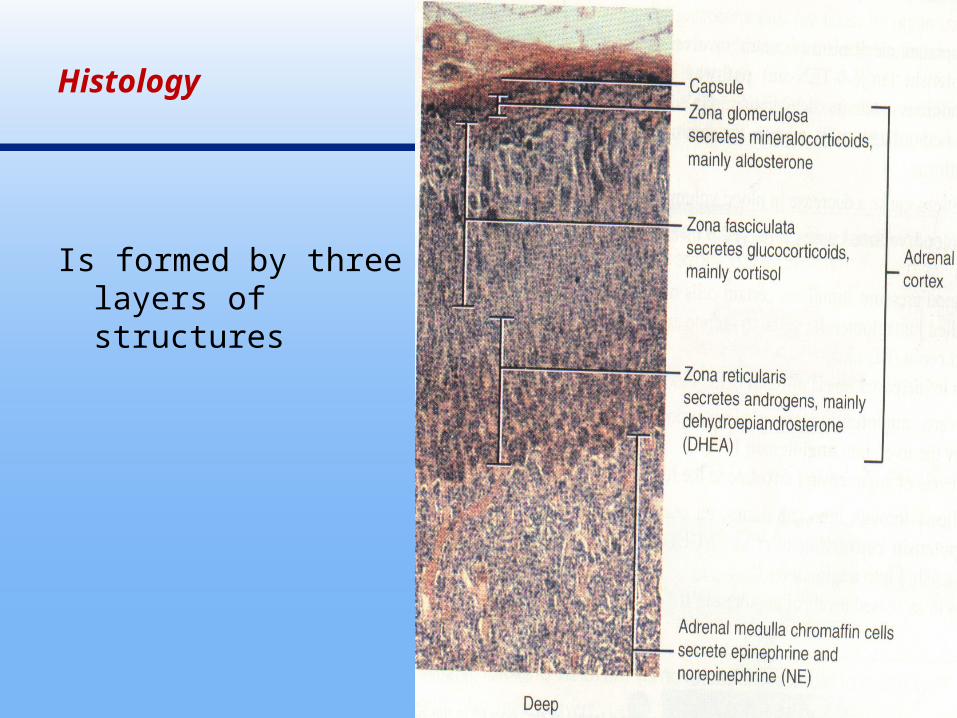
Histology
Is formed by three layers of structures

Hormones- Mineralocorticoids (Life Saving Hormone)- Glucocorticoids (Life Protecting Hormone)- Sex hormones
Are steroid in nature and synthesized mainly from cholesterol
Mineralocorticoids binds to plasma protein- globulins, glucocorticoids combine with plasma protein glucocorticoid-binding globulin or transcortin
Adrenal cortex

Mineralocorticoids- Aldosterone- 11-Deoxycorticosterone
These are C21 steroids
90% of mineralocorticoid activity is provided by aldosterone
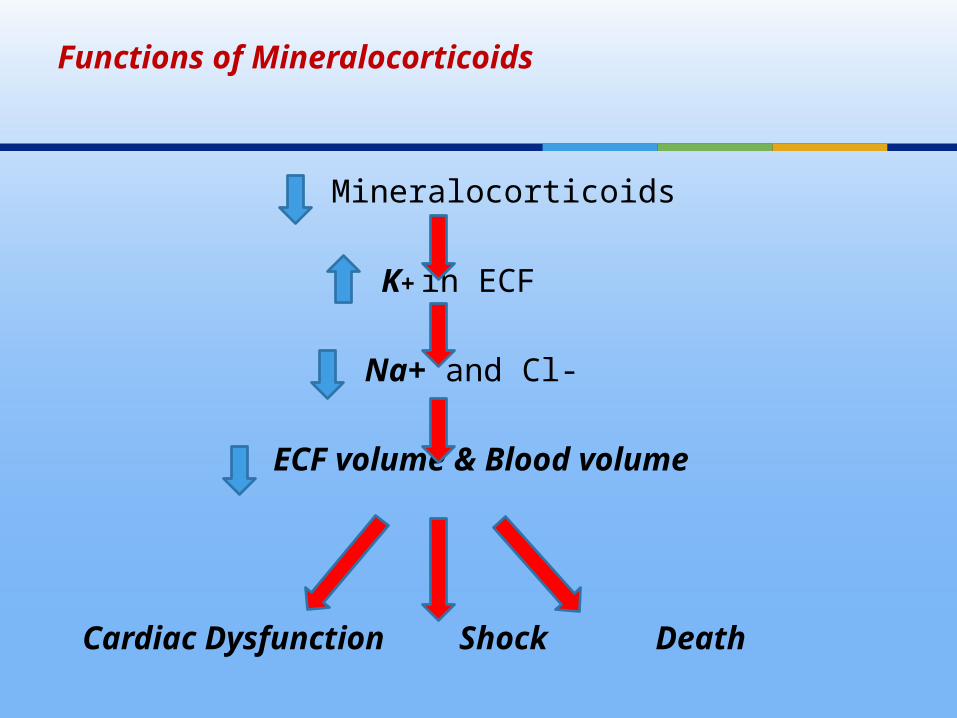
Functions of Mineralocorticoids
Mineralocorticoids
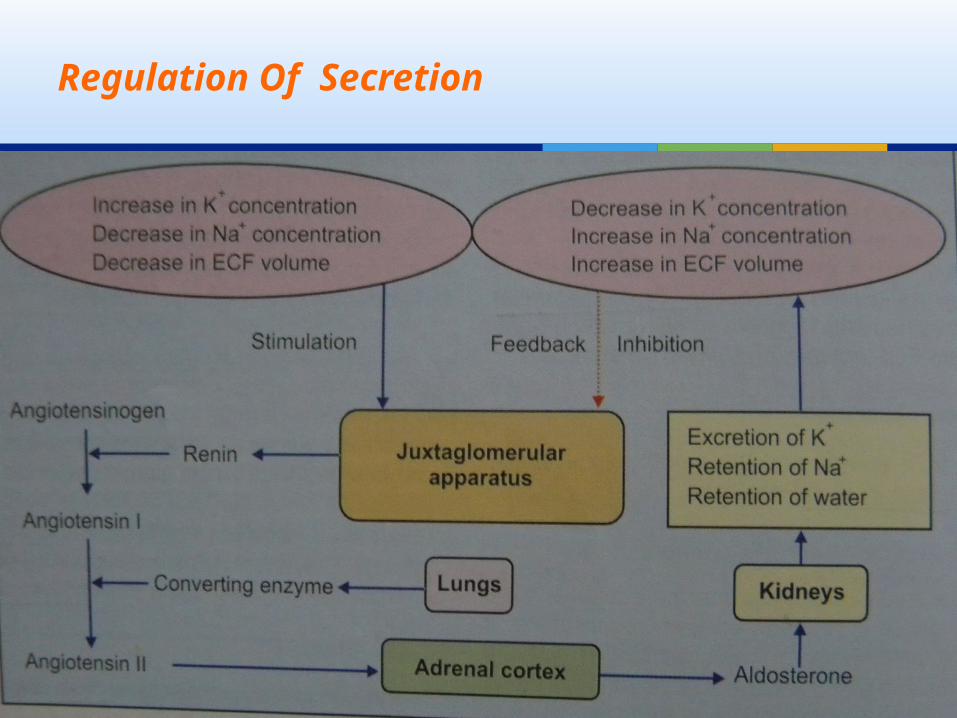
K+ in ECF
Na+ and Cl-
ECF volume & Blood volume
Cardiac Dysfunction Shock Death
On sodium ions Acts on DCT and collecting duct and increase the reabsorption
of sodium
On extra cellular fluid volume Along with sodium water also reabsorbed- increase in ECF
volume
On blood pressure Increase in ECF causes increase in BP
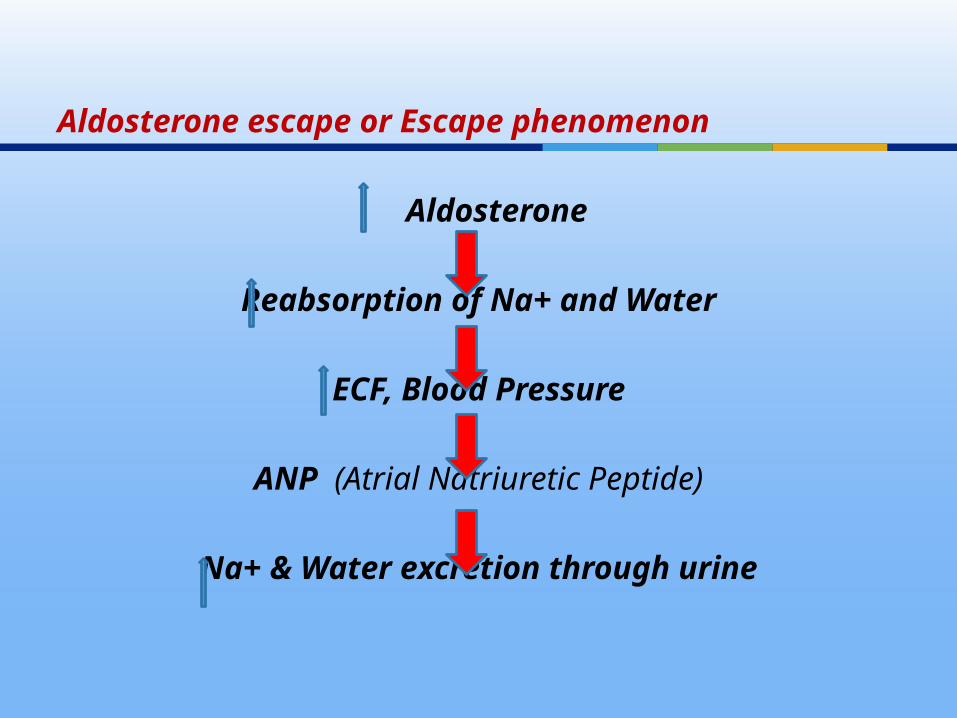
Aldosterone escape or Escape phenomenon
Aldosterone
Reabsorption of Na+ and Water
ECF, Blood Pressure
ANP (Atrial Natriuretic Peptide)
Na+ & Water excretion through urine
70.3
Regulation Of Secretion

Glucocorticoids
- Cortisol
- Corticosterone
- Cortisone
Secreted mainly by zona fasciculata, small quantity by zona reticularis
C21 Steroids having 21 carbon atoms
Life protecting hormone as it helps to withstand the stress and trauma in life
Functions of glucocorticoids
On carbohydrate metabolism Increases blood sugar level (Adrenal Diabetes)- By promoting gluconeogenesis- By inhibiting glucose uptake & utilization by peripheral cells
On protein metabolism Promotes catabolism of proteins Except for liver cells, it causes decrease protein synthesis by
inhibiting amino acid transport into cells & by inhibiting RNA formation

On fat metabolism Causes mobilization and redistribution of fats Increases ketone bodies in blood- ketogenic effect
On mineral metabolism Retains sodium, excretes potassium Inhibits calcium absorption from intestine – excretion of
calcium through urine

It accelerates excretion of water- in adrenal insufficiency causes water retention and water intoxication after water load
On CNS Insufficiency of these causes personality changes like
irritability and lack of concentration

Permissive action of glucocorticoids The actions of some hormones are executed only in the
presence of these hormones- Calorigenic effect of glucagon- Lipolytic, brochodilation & pressor action of catecholamines
- On Resistance to stress It is assumed that they enhances the resistance
- Immediate release & transport of amino acids from tissues to liver for synthesis of new proteins which are essential to withstand the stress
- Release of fatty acids produces more energy during stress- Enhancement of vascular reactivity of catecholamines
Anti- inflammatory effects Prevent the inflammatory changes in the cells caused by injury
or infection by acting at all stages of inflammation
Anti-allergic actions Prevent the various reactions in allergic conditions
Immunosuppressive effects Suppress the immune system by decreasing the number of
circulating T lymphocytes, also prevent release of inerleukin-2 by T cells

Regulation Of Secretion

Most of the hormones secreted are male sex hormones (Androgens) and in small amounts of estrogens and progesterone also secreted
The androgens are- Dehydroepiandrosterone
- Androstenedione
- Testosterone
Androgens in general are responsible for masculine feature of the body
Adrenal sex hormones
Hyperactivity Hypoactivity
Disorders of Adrenal cortex
Cushing's syndrome
Hyperaldosteronism
Adrenogenital syndrome
Addison’s diseaseAddisonian crisis
Congenital adrenal
hyperplasia
Any condition that produces an elevation in glucocorticoid levels.
Etiology Primary hypothalamic – pituitary diseases associated with
hypersecretion of ACTH (Cushing Diseases).
Microadenomas
Corticotroph cell hyperplasia.
Cushing’s syndrome (Hypercortisolism)

Primary adrenal neoplasms (ACTH independent)
Adrenal adenoma
Adrenal Carcinoma
Primary pigmented nodular adrenal hyperplasia
Carney Complex
McCune Albright Syndrome
Ectopic ACTH by a non endocrine neoplasm

Clinical Features
Obesity – centripetal, buffalo lump,
moon like facies
Reproductive dysfunction – Menstrual irregularity, loss of libido,
hirsuitism, acne
Psychiatric abnormalities – agitated depression & lethargy,
psychosis, memory and cognition affected, Insomnia.
Bone – Children – poor linear growth and weight gain.
Osteoporosis – Vertebral collapse
Pathologic fractures – rib and vertebral compression fracture
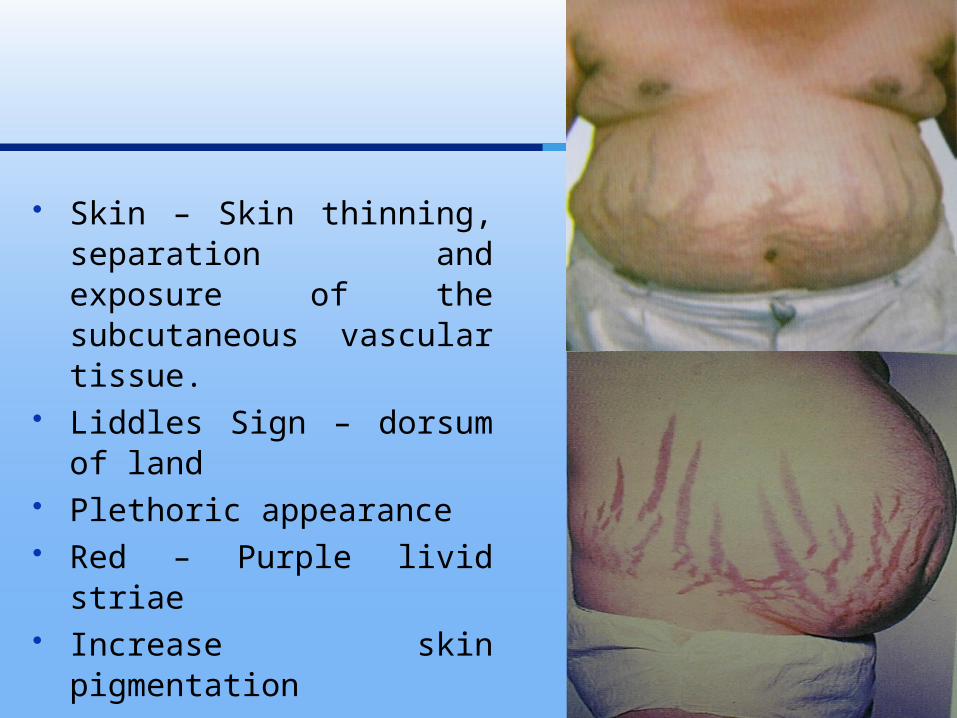
Skin – Skin thinning, separation and exposure of the subcutaneous vascular tissue.
Liddles Sign – dorsum of land Plethoric appearance Red – Purple livid striae Increase skin pigmentation
Muscle – Proximal myopathy
- Bruising Cardiovascular–Hypertension – 75% Infections – more common Fungal infections – tinea
versicolor, candidiasis. Poor wound healing
Treatment
Surgical removal of adrenal tumors & pituitary tumors. Benign tumors causing ectopic ACTH syndrome.
Medical Treatment
Metapyrone, Aminoglutethimide, Ketaconazole, Mitotane

Increased secretion of aldosterone Based on cause
Primary hyperaldosteronism
-Tumors in zona glomerulosa
Secondary hyperaldosteronism
- CCF
- Nephrosis
- Toxemia of pregnancy
- Cirrhosis of liver
Hyperaldosteronism

Signs & Symptoms
Increase in ECF & Blood volume Hypertension Prolonged depletion of K+ causes renal damage leads to
polyuria, polydipsia Muscular weakness due to K+ depletion Due to excretion of large amount of H+ ions causes metabolic
alkalosis, which in turn reduces blood calcium- tetany

Abnormal quantities of adrenal androgen secretion develops andrenogenital syndrome
Cause
Tumor of zona reticularis
Symptoms in females (Adrenal virilism)
-Increased muscular growth
-Deepening of voice
-Amenorrhea
-Enlargement of clitoris
-Male type hair growth
Andrenogenital syndrome

Symptoms in males
-Feminization
-Gynacomastia
-Atropy of testis

Due to failure of adrenal cortex to secrete all corticosteroids
Classified into
Primary – Due to adrenal cause
Secondary – Due to failure of ant pituitary to secrete ACTH
Tertiary – Due to failure of hypothalamus to secrete CRF
Addison’s disease or Chronic Adrenal Insufficiency
Signs and symptoms
Pigmentation of skin and mucus membrane
Muscular weakness
Dehydration with loss of sodium
Hypotension & Hypoglycemia
Decreased cardiac output leading to decreased size of heart
Nausea, vomiting and diarrhea
Susceptibility to any type of infection
Inability to withstand any stress

Characterized by sudden collapse associated with an increase in need for large quantities of Glucocorticoids
Causes
-Exposure to even mild stress
-Hypoglycemia due to fasting
-Trauma
-Surgical operation
-Sudden withdrawal of glucocorticoid treatment
Sudden collapse occurs, the condition becomes fatal if not treated in time
Addisonian Crisis or Adrenal Crisis or Acute Adrenal Insufficiency

Medulla is the inner part of the adrenal gland Made up of interlacing cords of cells known as Chromaffin
cells, Pheochrom cells or chromophil cells
Hormones of Adrenal medulla
-Adrenaline or Epinephrine
-Noradrenaline or Norepinephrine
-Dopamine
Adrenal medulla

Synthesis of catecholamines
Mode of action of these hormones are executed by binding with receptors called Adrenergic receptors
- Alpha adrenergic receptors (α-1 α-2 )
receptors mediate more of noradrenaline action than the adrenaline action
- Beta adrenergic receptors (β1 β2 )
β1- equal actions of both adrenaline, noradrenaline
β2- more adrenaline action than noradrenaline

On metabolism (via alpha and beta receptors )
General metabolism: Adr increases oxygen consumption, CO2
removal, BMR – calorigenic hormone
Carbohydrate metabolism: Increases glycogenolysis
Fat metabolism: Mobilization of free fatty acids from adipose
tissues
On blood (via beta receptors )
Adr decreases coagulation time, increases RBC count
Actions
On Heart (via beta receptors ) Adr has stronger effect on heart It increases Heart rate (Chronotropic effect )
Force of contraction (Ionotropic effect)
Excitability of heart muscle (Bathmotropic effect)
On Blood vessels (via alpha and beta 2 receptors) Noradr- Constriction (alpha) – Increase peripheral resistance Adr - Dilatation in skeletal muscle, liver and heart (beta 2)-
Decrease peripheral resistance

On Blood Pressure
Adr increases systolic BP, decreases diastolic BP
Noradr increases both systolic & diastolic BP
On respiration
Adr increases force and rate of respiration
Adrenaline secretion increases Fight or Flight reactions of brain
Causes contraction of smooth muscle
Increases secretion of many glands

Dopamine
Secreted by medulla and by dopaminergic neurons in some
areas of brain particularly, basal ganglia
It acts as neurotransmitter
Deficiency of dopamine, basal ganglia produces nervous
disorder called Parkinsonism

Is a condition characterized by Hypersecretion of catecholamines
Cause Tumor of chromophil cells in adrenal medulla Tumor of sympathetic ganglia (extra adrenal
pheochromocytoma)
Pheochromocytoma
Signs and symptoms
Hypertension- characteristic feature
Others- Anxiety
Chest pain
Fever, Headache
Hyperglycemia
Palpitation
Sweating and Flushing
Tachycardia
Weight loss
Pineal gland :
- secretes melatonin (inhibits onset of puberty)
Thymus :
- Endocrine glands ( secretion of Thymosin and Thymin )
Endocrine function of Kidney:
- Secretion of Erythropoietin, Thrombopoietin,Prostaglandins,
Renin, 1,25 – Dihydroxy cholecalciferol
Endocrine function of heart:
- Secretion of Atrial Natriuretic Peptide
Endocrine functions of other organs

Local hormones are the substances which act on the same area of their secretion or in immediate neighborhood
Classified into two types
Hormones synthesized in tissues-Prostaglandins and related substances, others like Acetylcholine, Serotonin, Histamine, Substance P, Heparin, Leptin, GI hormones
Hormones synthesized in Blood- Serotonin, Angiotensinogen, Kinins
Local hormones

Prostaglandins
Are unsaturated fatty acids with a cyclopentane ring & 20 carbon atoms
Synthesized from Arachidonic acid Types- PGD2, PGE2, PGF2
Actions
-Vasodilatation
-Gastric secretion
-Inhibit release of free fatty acids from adipose tissue
-Increase the velocity of sperm transport in female genital tract
-Induce abortion if injected intra-amniotically
-Stimulate jaxtaglomerular apparatus to secrete Renin

Thromboxanes (A2 & B2) Important in hemostasis by accelerating aggregation of
platelets
Prostacyclin Causes vasodilation and inhibits plate aggregation
Leukotrienes These are the mediators of allergic responses, and promote
inflammatory reactions
Lipoxins (A & B) Lipoxin A causes dilation of minute blood vessels, both inhibit
the cytotoxic effects of killer T cells
Acetylcholine It is the neurotransmitter substance at the NMJ Inhibits cardiac function & causes vasodilation
Serotonin (5-hydroxytryptamine) Inhibits impulses of pain sensation in posterior gray horn of
spinal chord, causes mood depression and sleep, vasoconstriction
Histamine During allergic condition, inflammation or damage of tissues-
vasodilation- entry of fluid and proteins from blood into affected tissue

Substance P Is a neurotransmitter substance, increases the mixing and
propulsive movements of small intestine
Heparin Produced by mast cells and basophils, is a natural
anticoagulant
Leptin Secreted by adipocytes in adipose tissue Inhibits feeding center resulting in stoppage of food intake Stimulates the metabolic reactions involved in utilization of
fat stored in adipose tissue

Kinins
Kinins are biologically active protein hormones which are circulating in blood
Two kinins in humans are- Bradykinin
- Kallidin Actions of bradykinin
-Dilates blood vessels decreases BP
-Increases permeability of capillaries edema
Kallidin is a vasodilator hormone Plasma Kallikrein activates factor XII during blood
coagulation, and are potent vasodilators

Textbook of physiology, 3rd edition Ganong
Textbook of medical physiology,7th edition Guyton
Textbook of human Physiology, Sembulingam
Davidson. TextBook of Medicine 20th ed., Elsevier Publishers
www.endocrinology.org
References

Thank You