dentistry - odontology pdf
TRANSCRIPT

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 1
Odontology
Final Exam Topic Notes 2012
(Edited)
Amit Dattani
"Education is our passport to the future, for tomorrow belongs to the people who prepare for it today."
-Malcolm X

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 2
Odontology Final Examination Topics 2012
Contents
1. Description of human dentition ............................................................................ 4
2. Definition and main parts of the tooth ................................................................. 8
3. Zsigmondy’s and the two-digit notations ............................................................11
4. Physical properties of the tooth surface .............................................................15
5. Attrition, abrasion and erosion of teeth. Degrees of degradation ..........................19
6. Tooth identifiers on the crown ................................................................................22
7. Tooth identifiers on the dental neck and root ....................................................25
8. The morphology of the maxilla............................................................................27
9. The morphology of the mandbile ........................................................................27
10. Development of the crown ....................................................................................32
11. Development of the root and formation of the periodontium .............................38
12. Phases of the tooth eruption .................................................................................41
13. Developmental dates of the teeth ........................................................................43
Tooth Morphology .......................................................................................................44
14. Description of permanent maxillary incisors .........................................................46
15. Description of permanent mandibular incisors .....................................................49
17. Description of permanent maxillary canine ..........................................................52
18. Description of permanent mandibular canine ......................................................53
19. Description of maxillary premolars .......................................................................55
20. Description of mandibular premolars ...................................................................57
21. Differentiation of premolars ..................................................................................59
22. Description of permanent maxillary molars ..........................................................60

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 3
23. Description of permanent mandibular molars ......................................................66
24. Differentiation of molars .......................................................................................71
25. Morphology of maxillary deciduous teeth ............................................................73
26. Morphology of mandibular deciduous teeth ........................................................77
27. Physical and chemical properties of enamel .........................................................84
28. Enamel structure and formations..........................................................................84
29. Physical and chemical properties of dentine ........................................................87
30. Dentine structure and formations .........................................................................89
31. Structure of the pulp .............................................................................................92
32. Functions of the pulp .............................................................................................92
33. Description of soft tissues of the periodontium ....................................................95
34. Description of hard tissues of the periodontium ..................................................98
These notes have been constructed from:
B.G Jansen Van Rendsburg – Oral Biology
Wheeler’s Dental Anatomy, Physiology and Occlusion 8th ed
The official lectures of the University of Debrecen Dental Department
Shimon Dantsis (Alumini) Notes
Netter’s Atlas of Human Anatomy 4th ed
(I am not responsible for the reproduction of any material in any way or form in this study pack.)
Please note, as I am also human there could be some mistakes. If you find any please message me on facebook so I can rectify these. I would also appreciate your feedback.
I dedicate this to the students at the University of Debrecen.
--
Amit Dattani (4th Year Dental Student)
1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 4
1. Description of human dentition
The Human Dentition is:
Diphyodont: Having two different sets of teeth through a life time, the deciduous
(Primary) teeth and the Permanent (Secondary) teeth.
Heterodont: Contains different teeth (Incisors, Canines, Premolars and Molars) which
differ in shape and properties in the same arch.
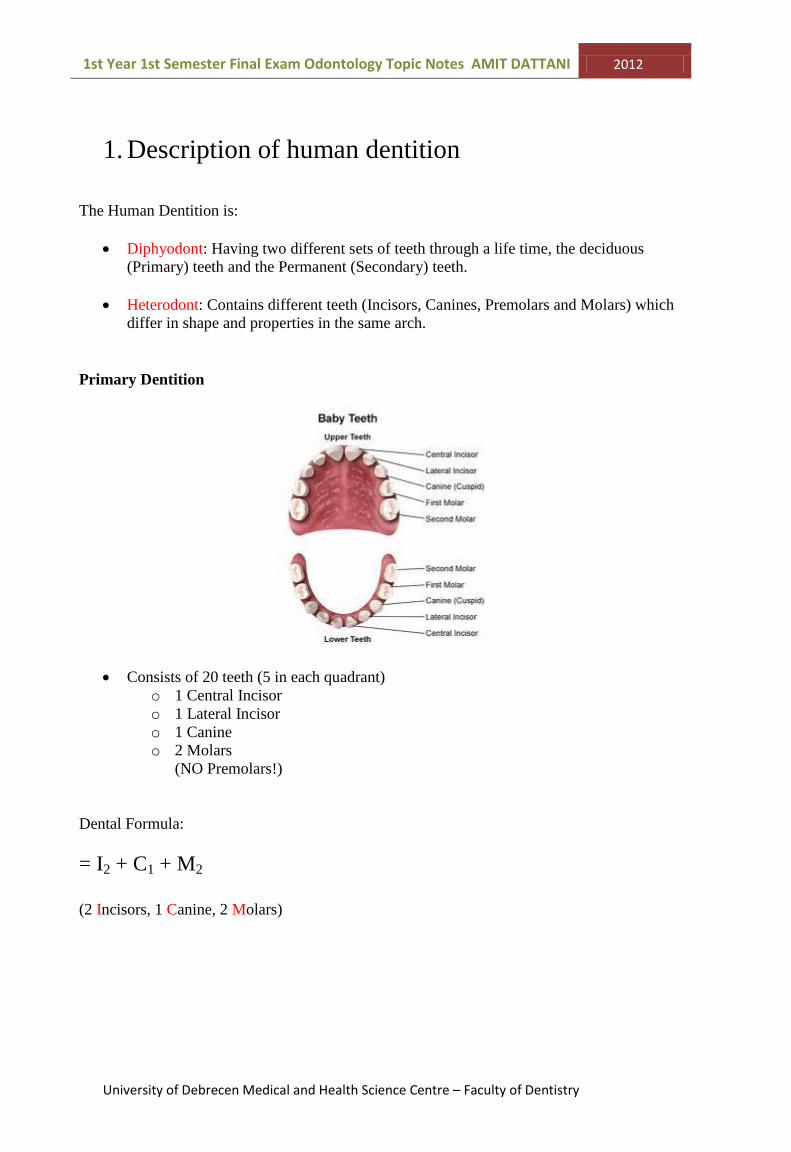
Primary Dentition
Consists of 20 teeth (5 in each quadrant)
o 1 Central Incisor
o 1 Lateral Incisor
o 1 Canine
o 2 Molars
(NO Premolars!)
Dental Formula:
= I2 + C1 + M2
(2 Incisors, 1 Canine, 2 Molars)

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 5
Permanent Dentition
Consists of 32 teeth (8 in each quadrant) o 1 Central Incisor o 1 Lateral Incisor o 1 Canine o 2 Premolars o 3 Molars
The Incisors & Canine form the Anterior teeth
The Premolars & Molars form the Posterior teeth
Permanent teeth begin to erupt at 6 years of age and continue to erupt till 17-21 years of age.
Dental Formula:
= I2 + C1 + P2 + M3
(2 Incisors, 1 Canine, 2 Premolars, 3 Molars)
A mixed dentition refers to one that is composed of primary and permanent teeth (when the
permanent teeth are erupting, after the deciduous).
Arrangement of teeth:
Upper Arch- Maxillary (stays stationary)
Lower Arch- Mandibular (moveable)

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 6
Each arch is separated into the Upper, Lower, Left and Right quadrants, separated by a
midline (an imaginary line dividing the central incisors).
Occlusion is when the maxillary and mandibular arches are in contact.
The upper teeth usually surround (on the front and both sides) the lower teeth in a normal
occlusion (contact between teeth).
The upper arch is larger than the lower arch.
Shape of the Dental Arches:
Primary:
Upper and Lower – Semicircular
1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 7
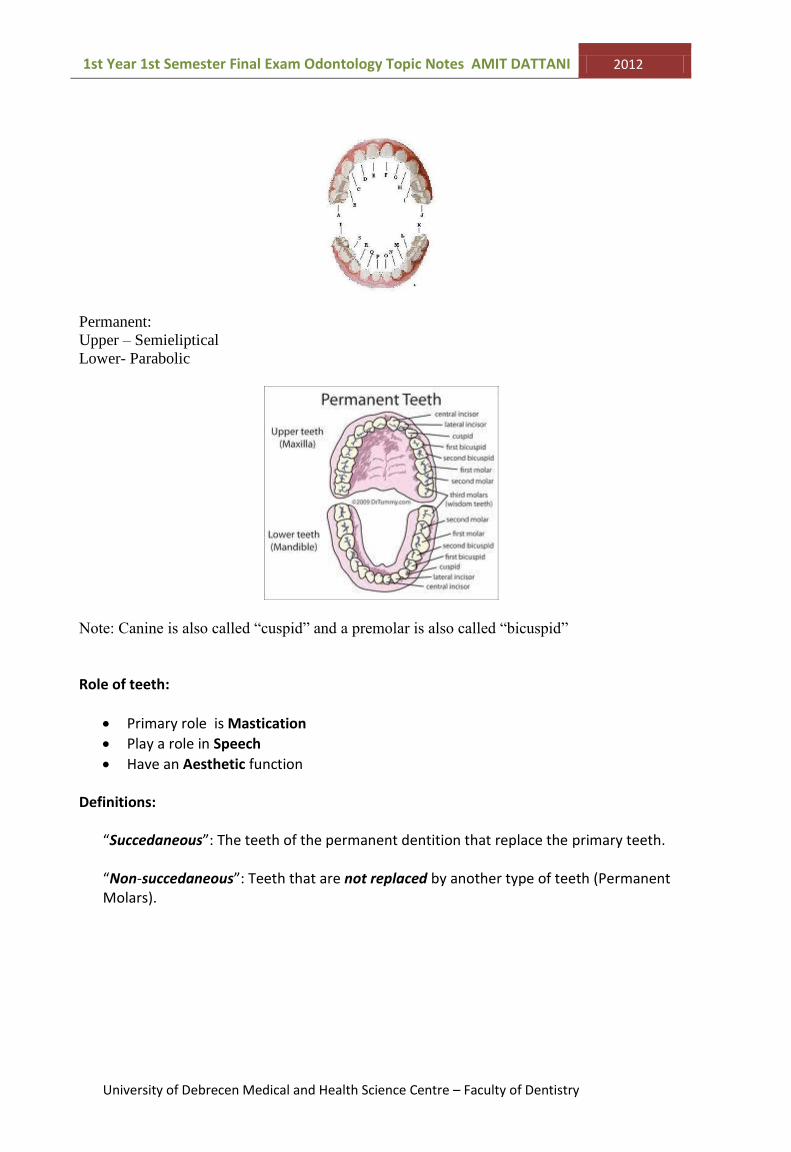
Permanent:
Upper – Semieliptical
Lower- Parabolic
Note: Canine is also called “cuspid” and a premolar is also called “bicuspid”
Role of teeth:
Primary role is Mastication
Play a role in Speech
Have an Aesthetic function
Definitions:
“Succedaneous”: The teeth of the permanent dentition that replace the primary teeth.
“Non-succedaneous”: Teeth that are not replaced by another type of teeth (Permanent Molars).

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 8
2. Definition and main parts of the tooth
“Tooth” – Independent organ belonging to the masticatory mechanism, found in oral cavity.
They have 3 main roles being mastication, speech (phonetics) and aesthetics.
A tooth has 2 main parts:
-Crown
-Root
Separated by a Cervical line/dental neck
(Cervical Line: the Cemento-Enamel Junction (CEJ) between
the crown and the root)
Basic Anatomy of the tooth:
(learn by heart now and you will understand it later…trust me on this one)
IMPORTANT: Learn detailed anatomy of tooth on Page 243 in “Oral Biology Jansen Van
Rensburg” book.
Parts of the tooth explained:
Enamel: hard tissue covering the crown of the tooth (made by ameloblasts)
Dentine: hard tissue under the enamel crown (softer than enamel). Made from odontoblasts.
1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 9
Cementum: layer of calcified tissue covering the root (sofer than dentine)
Pulp Chamber: cavity where the pulp itself is located
Pulp: The central hollow chamber of a tooth, containing delicate connective tissues, nerves
and both blood and lymph vessels. It is lined peripherally by odontoblasts.
Root Canal: contains part of the pulp chamber
Gingiva: the gum surrounding the tooth
Periodontium: the surrounding tissues of the tooth which provide support for the tooth
Made of up hard and soft tissues
Hard:
Alveolar bone
Cementum
Soft:
Gingiva
Periodontal Ligaments (PDL)
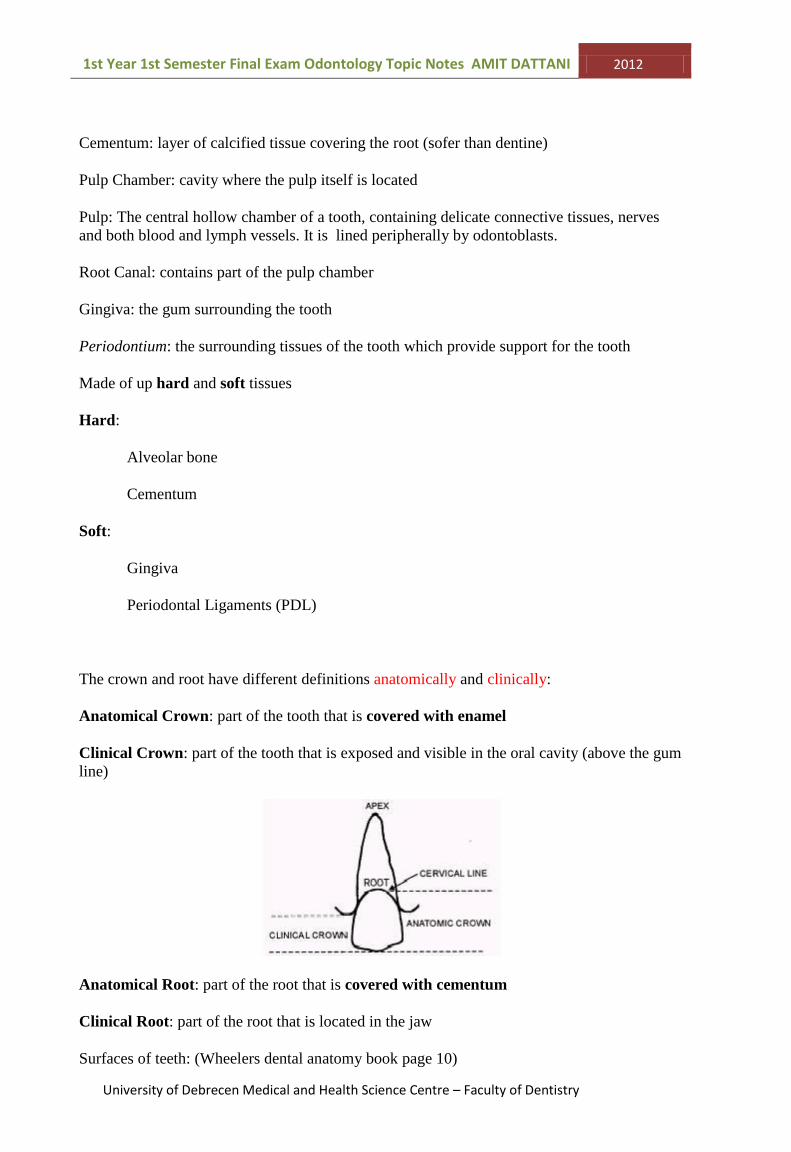
The crown and root have different definitions anatomically and clinically:
Anatomical Crown: part of the tooth that is covered with enamel
Clinical Crown: part of the tooth that is exposed and visible in the oral cavity (above the gum
line)
Anatomical Root: part of the root that is covered with cementum
Clinical Root: part of the root that is located in the jaw
Surfaces of teeth: (Wheelers dental anatomy book page 10)

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 10
Facial: the surface that faces the front (face)
Labial: facial surface of anterior teeth (Incisors and canine)
Buccal: facial surface of the posterior teeth (premolars and molars)
Lingual: surface that is closest to the tongue (only for lower jaw)
Palatal: surface that is closest to the tongue side (only for upper jaw)
Mesial: surface of the tooth that is closest to the midline (also called proximal surfaces)
Distal: surface of the tooth that is furthest away from the midline (also called proximal
surfaces)
EVERY tooth has these surfaces, and they have ONE of the following:
Incisial surface: biting surface for anterior teeth

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 11
Occlusal surface: biting surface for posterior teeth
Interproximal surface: The spaces between the proximal surfaces
3. Zsigmondy’s and the two-digit notations
In total there are 3 different notification systems.
1. Zsigmondy / Palmer Notification - (Used in the UK)
2. Universal System (2 digit numbering) - (1-32 /A-T)
3. FDI (Federation Denature International) System (2 digit numbering) – quadrant and tooth
number.
These systems are used so dental offices, staff; insurance companies can better communicate
between each other regarding exact details of certain teeth.
Adolf Zsigmondy (Hungarian Dentist) developed the idea in 1861. (Also known as the Palmer
Notification System)
He divided the teeth into 4 quadrants and each tooth was given a sign according to its location
in the mouth.
Maxillary Right Maxillary Left
Mandibular Right Mandibular Left
The teeth in each quadrant are numbered from 1-8 for an adult (permanent dentition) and
roman numerals (I-V) for the deciduous dentition (milk teeth). Roman Numbers were changed
to letters A-E for the deciduous dentition. (Roman numerals were not computer friendly so
not used today, Roman numerals used in Zsigmondy system and letters in Palmer system).
Permanent Dentition:
Maxillary Right Maxillary Left
Mandibular Right Mandibular Left
Midline (between both Central Incisors)
1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 12
E.g.
8 = Upper Right 8 (3rd
Molar)
4 = Upper Left 4 (1st Premolar)
2 = Upper Left 2 (Lateral Incisor)
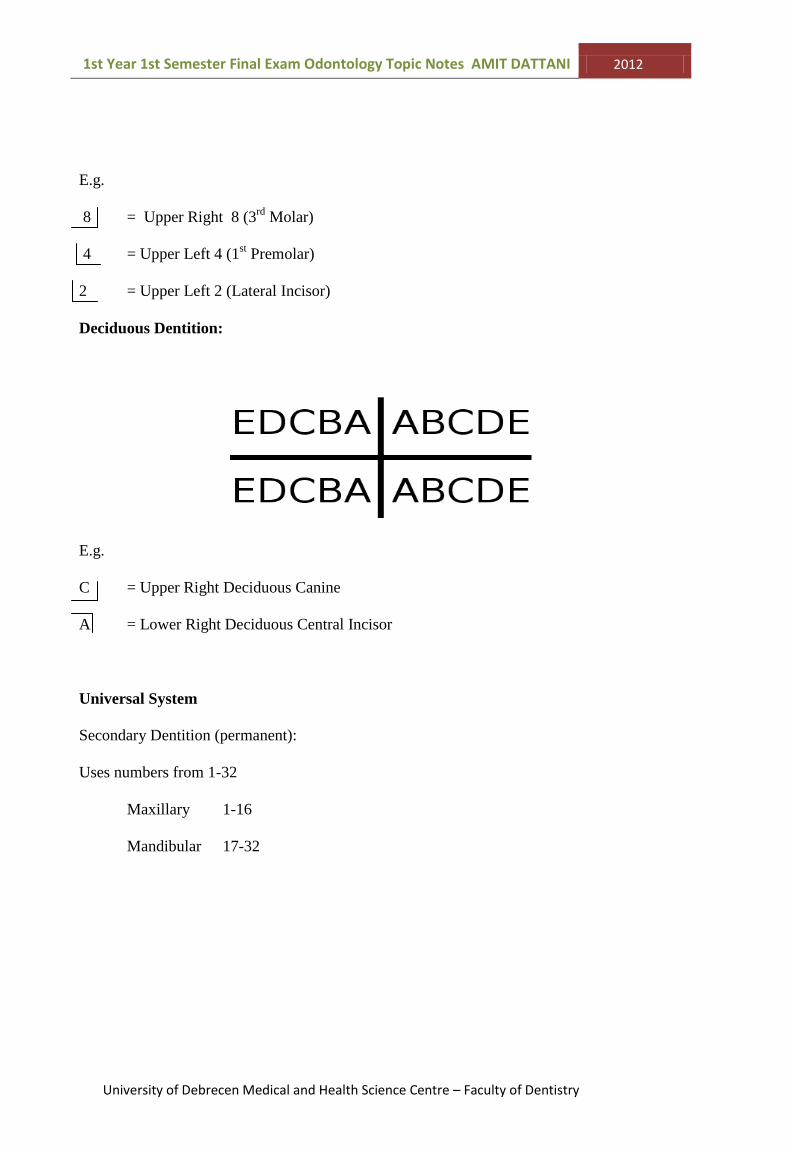
Deciduous Dentition:
E.g.
C = Upper Right Deciduous Canine
A = Lower Right Deciduous Central Incisor
Universal System
Secondary Dentition (permanent):
Uses numbers from 1-32
Maxillary 1-16
Mandibular 17-32

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 13
Primary Dentition:
Users Letters from A-T
Maxillary A-J
Mandibular K-T
E.g.
16 = Upper Left 3rd
Molar
24 = Lower left Permanent Central Incisor
N= Lower Left Deciduous Lateral Incisor
T= Lower Right Deciduous 2nd
Molar
FDI System
This system uses 2 digit numbering. (This system is used in the University clinics)
The first digit represents the quadrant number

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 14
The second digit represents the tooth number (starting from the midline)
Permanent Quadrant (mouth) Deciduous
1 Upper Right (of patient) 5
2 Upper Left 6
3 Lower Left 7
4 Lower Right 8
Quadrants:
Permanent:
Deciduous:
REMEMBER THE QUADRANTS AS A CLOCK FACE (GOING CLOCKWISE!)
E.g.
11 = Upper Right Permanent Central Incisor
18 = Upper Right 3rd
Molar
35 = Lower Left 2nd
Premolar
46 = Lower Right Permanent 1st Molar
54 = Upper Right Deciduous 1st Molar
75 = Lower Left Deciduous 2nd
Molar
REMEMBER THE QUADRANTS AS A CLOCK FACE (GOING CLOCKWISE!)

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 15
4. Physical properties of the tooth surface
Strictly speaking this topic is asking about the physical properties of the tooth surfaces, but
the examiners always like to around the topic and will ask you about other properties too.
The tooth is covered by enamel, which is the outer most layer. (The tooth surface is covered
by enamel, dentine and cementum.)
The enamel surface is the hardest tissue in our body
Covers the outer surfaces of the tooth
It is of ectodermal origin
Density
~ 2.84-3.00 grams/ml
Density decreases from the surface to the amelodentinal junction (where the enamel
and dentine meet)
During tooth development the density of enamel increases progressively
Physical Properties:
Hardest tissue in the body
96-98% Inorganic Substances (mainly hydroyapetite crystals)
o Ca10 (PO4)6(OH)2
3-4% water
1% Organic material
Outer regions are harder than the inner (deeper) regions
Composed of tightly packed rods (prisms)
o Approx 2.0-2.5mm thick in cusp tips
o Enamel prisms are the elementary components of enamel
Colour
Enamel is semi-translucent
o Thick enamel is greyish / blue-white colour
o Thin enamel is yellow-white
Discolouration by:
Oral hygiene, food deposits, ageing of patient
Calcification disorders – cause white/ brown spots
Excessive fluoride intake – through incorrect water fluoridation or medication
Tetracycline staining (pictured below) – (General Antibiotic) such as
Chlorotetracylcine
Smoking – causes yellow staining by nicotine and tar. Also causes brown deposits
found between teeth.

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 16
Strength:
Very brittle
Cushioning effect of dentin makes enamel hard to withstand
Solubility
When exposed to acid medium it is subjected to DISSOLUTION (chemical basis of
cavities).
Fluoride can incorporate into hydroxyapatite crystals and REDUCE THE
SOLUBILITY of enamel and thus increases the defence against acidogenic bacteria.
The organic matrix of enamel protects the enamel from acid action
Permeability
Selectively permeable – lets some elements pass through but not everything. E.g.
Fluoride can permeate
o Cannot permeate enamel: Calcium, Zink, Silver elements
o Can permeate enamel: Fluoride, Sodium Iodide, Iodine, Urea, Nicotinamide,
Thiourea
Other:
Lines of Retzius - might be formed as a result of disturbed mineralisation
It will cause brown, dark lines on the enamel
Shallow grooves can be seen where the lines meet the enamel surface
1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 17
Perikymata are incremental growth lines that appear on the surface of enamel as a series of
grooves.
Neonatal Line- accentuated (more visible) lines of retzius seen in histologic sections, these
lines can only form at birth and are used in forensic dentistry to identify the age of a person.
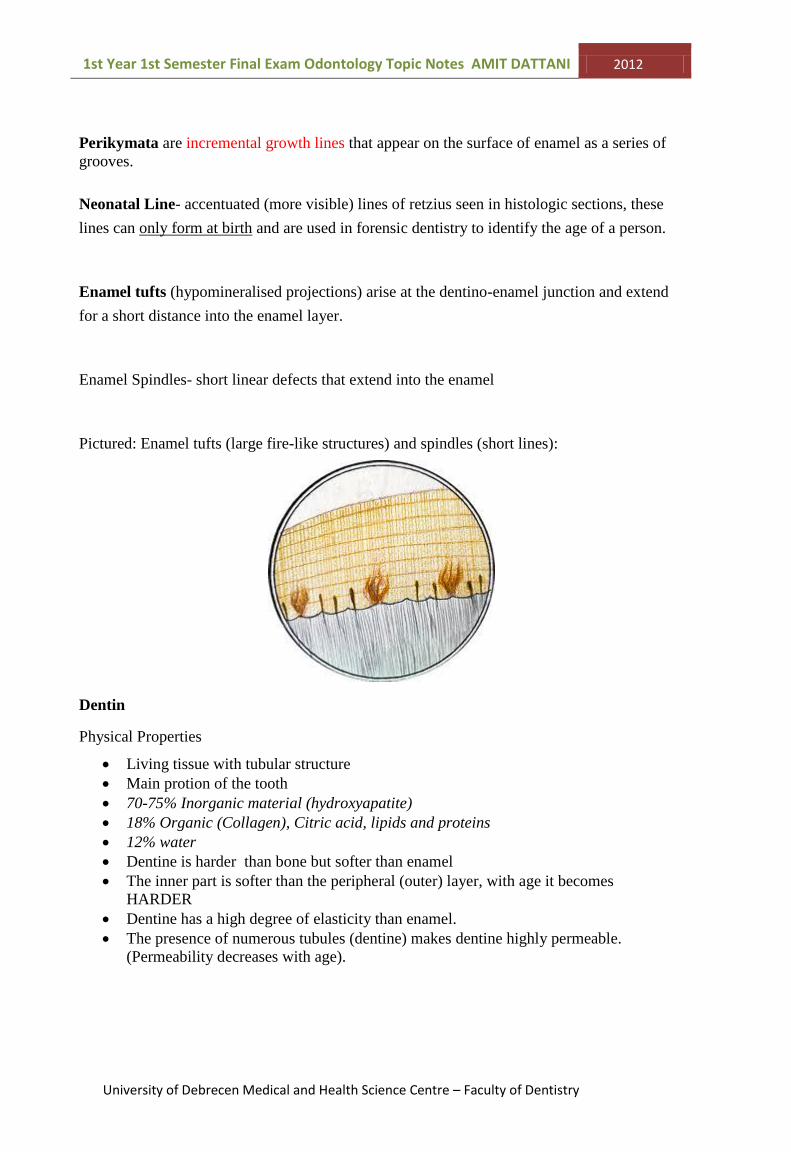
Enamel tufts (hypomineralised projections) arise at the dentino-enamel junction and extend
for a short distance into the enamel layer.
Enamel Spindles- short linear defects that extend into the enamel
Pictured: Enamel tufts (large fire-like structures) and spindles (short lines):
Dentin
Physical Properties
Living tissue with tubular structure
Main protion of the tooth
70-75% Inorganic material (hydroxyapatite)
18% Organic (Collagen), Citric acid, lipids and proteins
12% water
Dentine is harder than bone but softer than enamel
The inner part is softer than the peripheral (outer) layer, with age it becomes
HARDER
Dentine has a high degree of elasticity than enamel.
The presence of numerous tubules (dentine) makes dentine highly permeable.
(Permeability decreases with age).

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 18
Colour
Yellowish-white
Darker in deciduous teeth
Cementum
Covers the anatomical root surfaces of the teeth
Similar to bone, but cementum is avascular (No blood supply)
o 65% mineral, (inorganic) - hydroxyapatite
o 23% Organic
o 12% water
(See topic 29 for more about Dentine)
Summary:
Enamel Dentin Cementum
Inorganic mineral (%) 96-98 70-75 65
Organic (%) 1 18 23
Water (%) 3-4 12 12
Note: percentages are based on weight

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 19
5. Attrition, abrasion and erosion of teeth. Degrees of
degradation
There are three types of processes that aid loss of tooth substance:
1. Attrition
2. Abrasion
3. Erosion
Attrition
Is the wearing away of tooth structure as a physiological result of tooth-tooth contact and by
the friction of food.
Affects: occlusal surfaces (primarily) and proximal surfaces of teeth
Also bruxism (tooth grinding during stress or sleep) causes attrition
5 grades of attrition:
1. Loss of tooth material localised in the enamel
2. Dentin is exposed on tip of cusps and incisial edges
3. Dentin exposed to whole occlusal surface, enamel surrounds it
4. The process reaches the pulp chamber and the pulp may become inflamed
5. Tooth worn down to the gingival margin
Characteristics
The loss of tooth material (attrition) most commonly seen on the palatal surface (of upper
teeth) and the vestibular surface (also known as the facial surface) (of lower teeth)

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 20
Abrasion
Is the wearing away of a tooth by a mechanical process, other than mastication and tooth-
tooth contact.
Causes: excessive or improper tooth brushing, flossing or use of tooth-picks, can also be
caused by working in a polluted area.
It can produce sensitivity in teeth due to exposed dentine or thinning of enamel.
It produces deep “U” or “V” shaped depressions towards the cervical surface of the tooth
crown. It exposes the underlying dentine and thus causing increased sensitivity. (Pictured).
Most commonly canines and premolars are affected, or the buccal surface of 1st upper molars
Erosion
Is the wearing away of the non-occluding surfaces of teeth by chemical dissolution (mainly
through acid), reduction in saliva increases erosion (because saliva has antibacterial properties
and a natural buffer.)
Intrinsic origin of acid:
Regurgitation of gastric acid (habitual vomiting)
o Affects palatal and occlusal surfaces mainly.
Extrinsic origin of acid:
Diet (fruit juices – affects mainly incisors on their incisial surface)
Air pollution in working environment due to acid
Causes:
Dietary- (Fruits, juices)
Medical – (HCL replacement, Vitamin C, Aspirin), occlusal and palatal surfaces affected.
Gastric reflux – mineral loss of occlusal surfaces of the molars and palatal surface

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 21

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 22
6. Tooth identifiers on the crown
There are certain characteristics that can be seen on the crowns of teeth…
1. Angular characteristics – upper central incisor (permanent)
The distoincisial line angles are more rounded than the mesioincisial angle
2. Cervical line curvature
The cervical line that separates the crown from
the root curves differently on the Mesial &
Distal surfaces of the tooth to the Buccal &
Lingual surfaces
The curvature of the line is (pointed) more on
the Mesial aspect than the distal aspect
(pictured).
Incisial edge
Distal Surface
Mesial Surface
More rounded (greater than 90 degrees- obtuse angle
)
Less rounded (Right angled)

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 23
Curved more than the mesial side
3. Arch characteristics
Occlusal view (cross section)
Vestibular
Mesial Distal
The curvature of the mesio-vestibular crown surface is more sharply
curved than the distovestibular
4. Cervical Contour Characteristics
Occlusal view (cross section)
Mesial Distal
At the level of the cervical line the contour of the mesial part of the tooth is FLAT, but
the distal is curved
5. Cusp inclination characteristic
(Letter “D” shape formed)

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 24
The longitudinal axis of the lower posterior teeth incline lingually, but the axis of the
upper teeth is almost vertically orientated.
Right side - buccal view
Longitudinal axis – is along the length of the tooth
Vertical axis – is in direction of the length of the tooth
------------------------------------------------------------------------------------------
Note:
Attrition characteristics:
The loss of tooth material can be usually be seen on the palatal surface of
the upper teeth and the vestibular surface of the mandibular teeth
Straight vertical axis of maxillary posterior teeth
Inclined longitudinal axis of mandibular posterior teeth
1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 25
7. Tooth identifiers on the dental neck and root
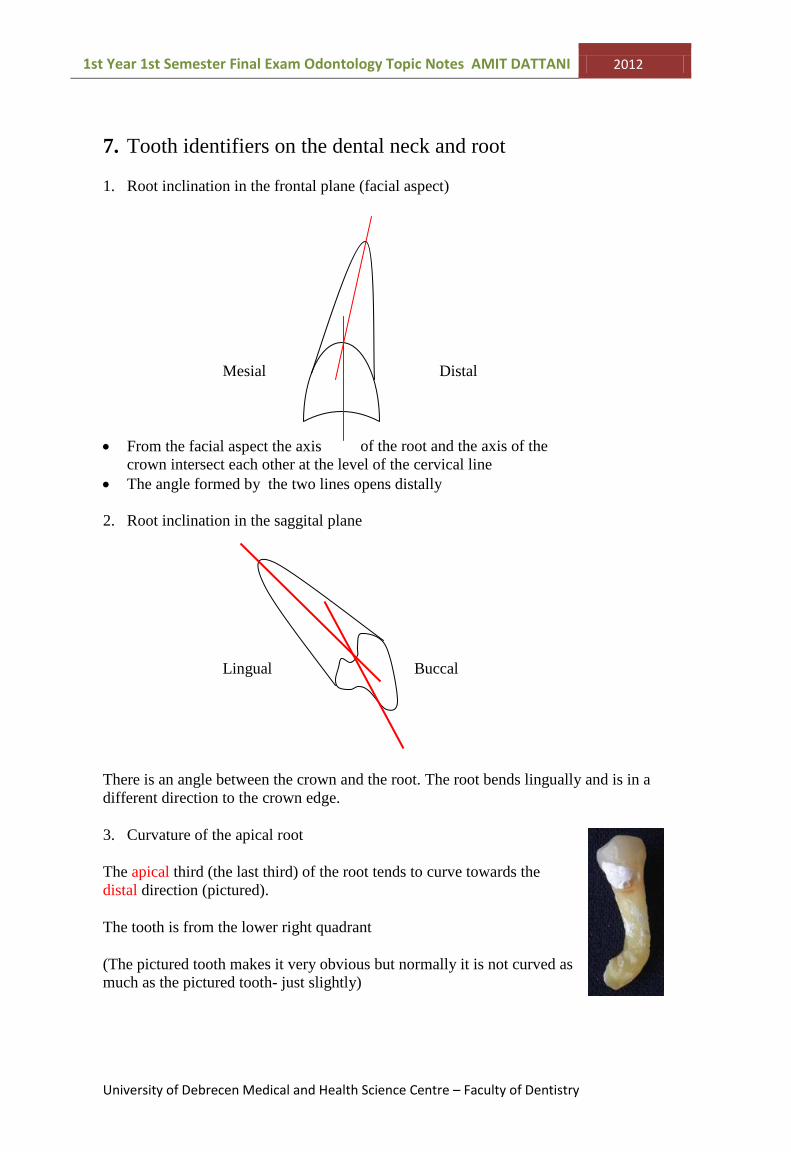
1. Root inclination in the frontal plane (facial aspect)
Mesial Distal
From the facial aspect the axis of the root and the axis of the
crown intersect each other at the level of the cervical line
The angle formed by the two lines opens distally
2. Root inclination in the saggital plane
Lingual Buccal
There is an angle between the crown and the root. The root bends lingually and is in a
different direction to the crown edge.
3. Curvature of the apical root
The apical third (the last third) of the root tends to curve towards the
distal direction (pictured).
The tooth is from the lower right quadrant
(The pictured tooth makes it very obvious but normally it is not curved as
much as the pictured tooth- just slightly)
1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 26
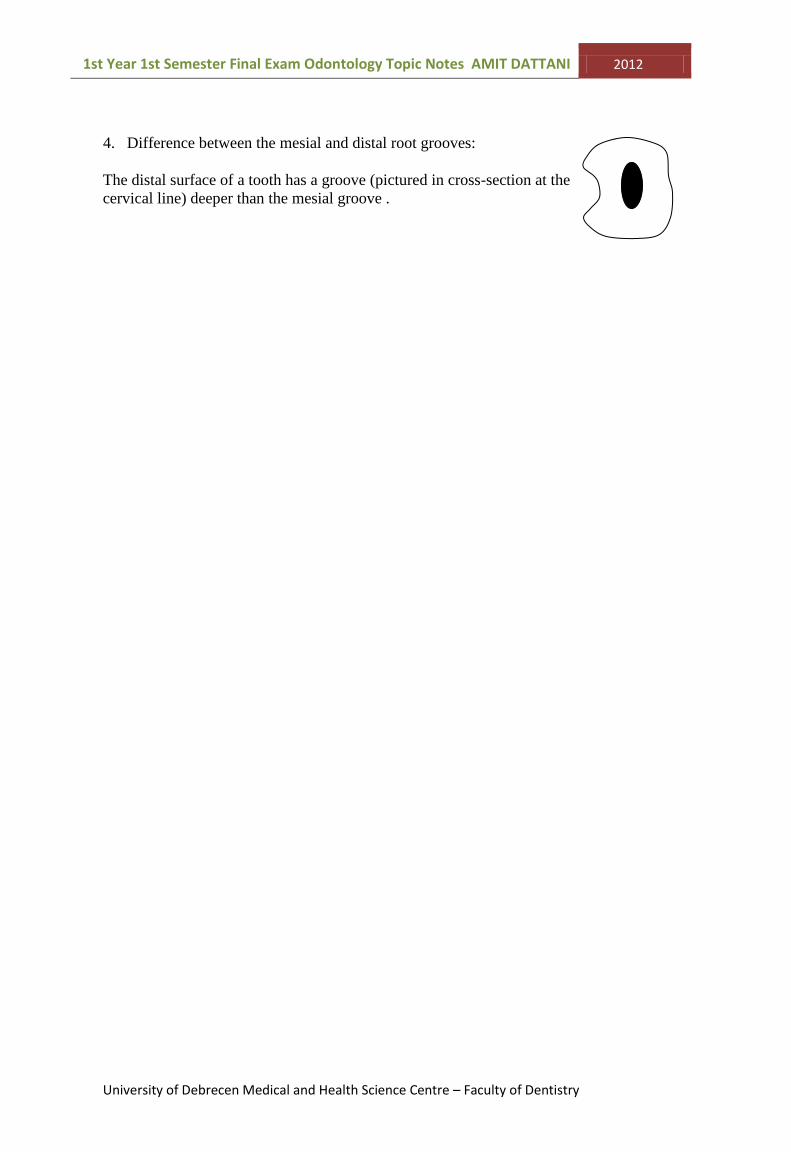
4. Difference between the mesial and distal root grooves:
The distal surface of a tooth has a groove (pictured in cross-section at the
cervical line) deeper than the mesial groove .

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 27
8. The morphology of the maxilla
9. The morphology of the mandbile
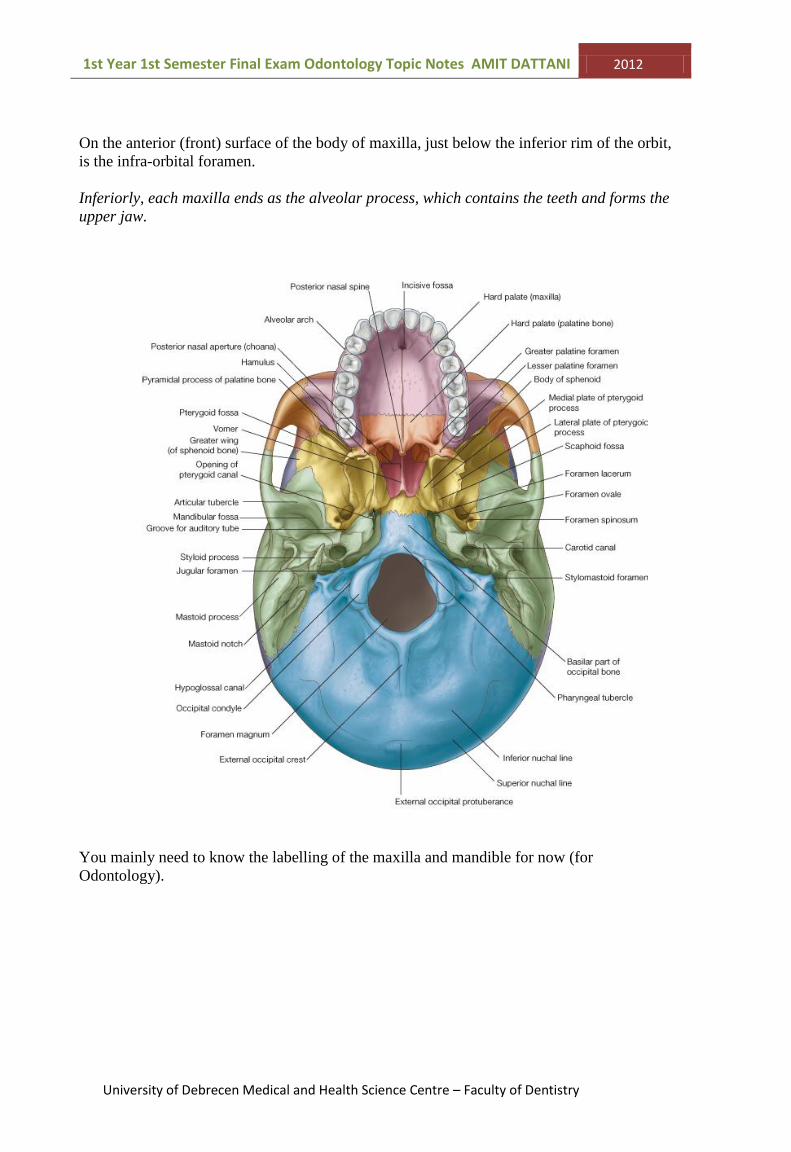
Maxilla – Purple in image above
Mandible – white/grey in image above
The part of the face between the orbit (place of eyes) and the upper teeth and each upper jaw
is formed by the paired maxillae, together known as the maxilla.
Superiorly (on top), each maxillae contribute to the inferior (lower) and medial (towards the
midline) rims of the orbit.
Laterally (towards the left and right sides), the zygomatic process of each maxillae articulates
(joins) with the zygomatic bone and medially, the frontal process of each maxillae articulates
with the frontal bone.
Laterally to the opening of the nasal cavity is the body of the maxilla
.
1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 28
On the anterior (front) surface of the body of maxilla, just below the inferior rim of the orbit,
is the infra-orbital foramen.
Inferiorly, each maxilla ends as the alveolar process, which contains the teeth and forms the
upper jaw.
You mainly need to know the labelling of the maxilla and mandible for now (for
Odontology).

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 29
Mandible
The mandible has 3 main parts:
Ramus
Body
Angle
1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 30
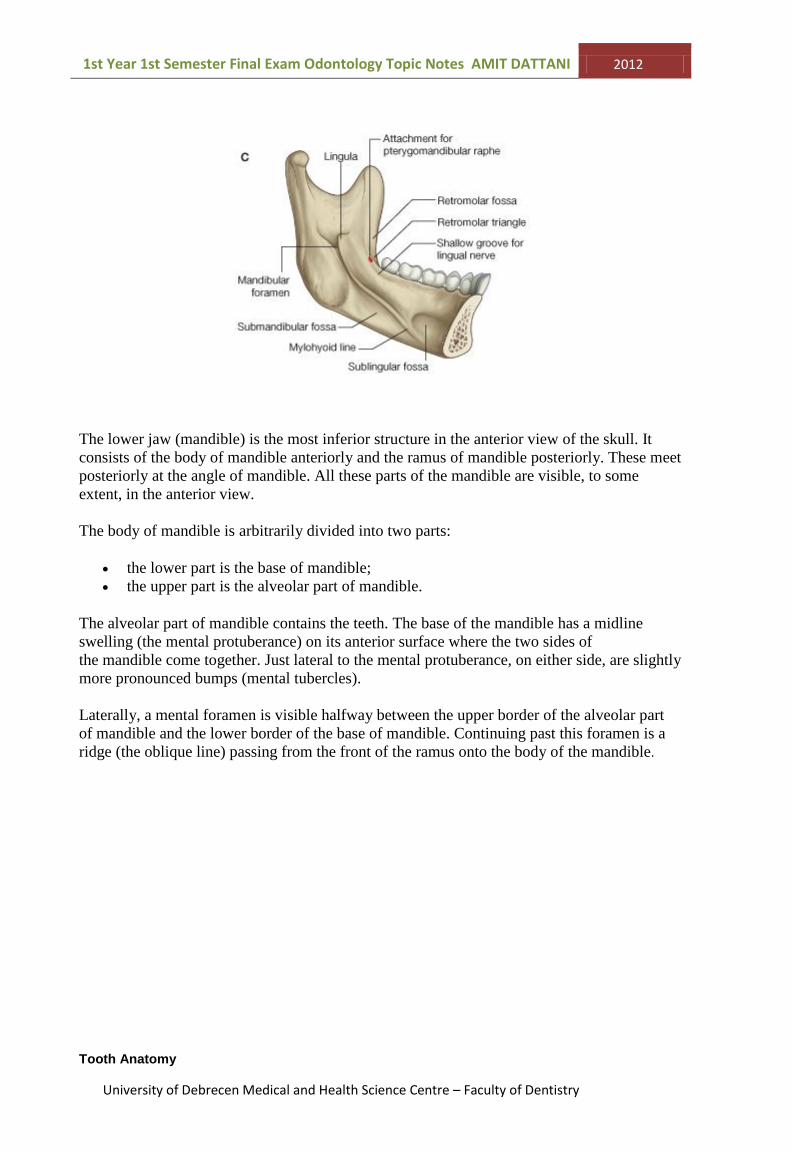
The lower jaw (mandible) is the most inferior structure in the anterior view of the skull. It
consists of the body of mandible anteriorly and the ramus of mandible posteriorly. These meet
posteriorly at the angle of mandible. All these parts of the mandible are visible, to some
extent, in the anterior view.
The body of mandible is arbitrarily divided into two parts:
the lower part is the base of mandible;
the upper part is the alveolar part of mandible.
The alveolar part of mandible contains the teeth. The base of the mandible has a midline
swelling (the mental protuberance) on its anterior surface where the two sides of
the mandible come together. Just lateral to the mental protuberance, on either side, are slightly
more pronounced bumps (mental tubercles).
Laterally, a mental foramen is visible halfway between the upper border of the alveolar part
of mandible and the lower border of the base of mandible. Continuing past this foramen is a
ridge (the oblique line) passing from the front of the ramus onto the body of the mandible.
Tooth Anatomy

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 31

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 32
10. Development of the crown
Overview
Note: “Tooth bud” – (also known as a “Tooth germ”) is an aggregation of cells that
eventually forms the tooth. The tooth bud is composed of 3 parts:
1. Enamel organ
2. Dental papilla
3. Dental follicle
1. The enamel organ is composed of the following:
Outer enamel epithelium
Inner enamel epithelium
Stellate reticulum
Stratum intermedium
These cells give rise to the ameloblasts, which produce
enamel and reduce the enamel epithelium.
The growth of the cervical loop (the location where the
outer enamel epithelium and inner enamel epithelium
join) – cells into the deeper tissues forms “Hertwig’s
epithelial rooth sheath”, which determines the shape of
the root.
(The diagram won’t make sense at the moment- its just there so you can visualise the different
parts of the enamel organ as reference after you have completed this topic.)
2. The dental papilla contains cells that develop into odontoblasts – which are ‘dentine
forming cells’. Mesenchymal cells within the dental papilla are responsible for formation
of the pulp.
3. The dental follicle gives rise to cementoblasts, osteoblasts and fibroblasts.
4.
Cementoblasts- form the cementum of the tooth
Osteoblasts- form the alveolar bone around the roots
Fibroblasts – develop the PDL (periodontal ligaments) that connect teeth to the
alveolar bone through cementum
The developing tooth bud:
The earliest steps in tooth formation (take place at the 7th week in-utero) make the
distinction between the vestibular lamina and the dental lamina. (The dental lamina
connects the developing tooth bud to the epithelial layer of the mouth).

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 33
Tooth development has 4 main stages:
1. Bud stage
2. Cap stage
3. Bell stage
4. Crown stage
1. Bud Stage
Characterised by the appearance of a tooth bud without a clear arrangement of cells
Stage begins when the epithelial cells proliferate (rapid growth) into the mesenchyme
of the jaw. (The tooth bud itself is the group of cells at the end of the dental lamina).
The epithelial lining of the oral cavity before development commences
Primary epithelial cells thicken into a ‘V’ shaped bud
The primary epithelial thickening
The epithelial thickening divides into vestibular and dental lamina

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 34
Vestibular and dental laminae
2. Cap Stage
First sign of arrangement of cells in the tooth bud
Increase in mitotic activity
Mesenchyme cells aggregate to produce the dental papilla
Tooth bud grows around mesenchymal aggregation (looks like a cap) and becomes the
enamel organ
Condensation of mesenchymal cells called the dental follicle surrounds the enamel
organ and limits the dental papilla
Eventually….
Enamel organ produces ENAMEL
Dental Papilla produces DENTINE AND PULP
Dental Follicle produces SUPPORTING STRUCTURES (cementoblasts, osteoblasts and
fibroblasts)
Cells aggregate to form the tooth bud from the dental lamina
Tooth Bud

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 35
Cap stage of development
The enamel organ looks like a cap (above).
3. Bell Stage (histo-differentiation)
The enamel organ has a Bell shape in this stage
The dental lamina disintegrates leaving the tooth separated from the epithelium
(joins later during eruption)
Cells of enamel organ separate into 4 layers:
1. Inner enamel epithelium (columnar layer) – forms ameloblasts
2. Outer enamel epithelium (cuboidal layer)
3. Stellate cells (contains alkaline phosphate, some RNA and glycogen)
4. Intermediate cells
Inner and outer epithelium grow and form the cervical loop
Inner dental enamel differentiates to form ameloblasts
Fibers, blood vessels and nerves appear in the dental papilla (forms pulp)
The enamel organ develops from oral ectoderm

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 36
The tooth germ consists of the enamel organ, the follicle and the dental papilla
4. Crown Stage (hard tissue develops)
Hard tissues form – enamel and dentine
Mitosis of inner enamel epithelium cells, it stops where the cusps form
The inner enamel epithelium cells change in shape from cuboidal to columnar
Nuclei of inner enamel epithelium cells move closer to the stratum intermedium and
away from the dental papilla
The adjacent layer of cells in the dental papilla increase in size and differentiate into
odontoblasts – cells that form dentine
After dentin formation begins, the cells of the inner enamel epithelium secrete an
organic matrix in the dentin
The matrix immediately mineralises and forms enamel
Ameloblasts- continue the process of enamel formation; adding enamel to the outer
surface of the tooth.

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 37
Formation of dentine and enamel
Root sheath of Hertwig
Root sheath of Hertwig
Determines root form
Retains a tubular form, where it divides into roots
Advanced development

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 38
Changes in the dental papilla:
During bell stage blood capillaries
appear and are indicative of metabolic
activity. This will eventually result in
dentine formation.
Nerves appear priot to the
differentiation of odontoblasts but the
nerve supply of the pulp and dentine is
poorly developed before birth.
11. Development of the root and formation of the
periodontium

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 39
Starts after determination of the crown
The inner and outer epithelial cells elongate and form the cervical loop (or root sheath
of Hertwig). There is a double layer membrane with no other membrane between
them.
The root sheath determines root form, i.e. subdivides for multiple roots.
The dental follicle differentiates to form:
1. Fibroblasts - PDL (periodontal ligaments)
2. Osteoblasts - Alveolar bone
3. Cementoblasts – Cementum
Peripheral cells of the dental papilla differentiate to from odontoblasts
These 3 cells (see above) will only secrete after the sheath of Hertwig breaks down
Cementum and PDL will start to establish
Most root development continues during eruption of teeth
When the cusp appears in the oral cavity – approximately HALF the root is formed
at this point (…be prepared to answer questions on tooth eruption times!)
The PDL will change until the bone reaches its final size and the tooth will find its
place in the jaw
Important information (generally regarding tooth development)
The function of the outer dental papilla is to provide nutrition and oxygen
Enamel is ectoderm origin (and gingiva)
Dentine, PDL, cementum, alveolar bone, pulp are mesoderm origin
Number of tooth buds in the oral cavity is 52 (20 in primary teeth and 32 in
permanent)
Definitions:
“Vestibule” – space between the teeth and the cheek/lip
“Cervical loop”- the area of the enamel organ where the inner and outer dental
epithelium cells join to each other
“Ectoderm”- the outermost layer of the three primary germ layers of an embryo
“Mesoderm”- the middle layer of the three primary germ layers, from which
connective tissue, muscle, bone, and circulatory systems develop.
“Epithelial root sheath” – continuous sheet of tissue sandwiched between the
undifferentiated mesenchyme of dental papilla and the follicle.
Periodontium
The periodontium consists of 4 parts:
1. Cementum
2. Gingiva
3. PDL
4. Alveolar bone
They are classified into hard and soft tissues:

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 40
Hard Soft
Alveolar bone PDL
Cementum Gingiva
Extra points to note:
‘Sharpeys fibers’- parts of the PDL fibers embedded in cementum and those parts of the
fibers embedded into the alveolar bone.
In simple terms – Sharpeys fibers are the end-parts of the PDL. (DO NOT say this line in
the exam! - it’s for your understanding!)…IF you do say this line in the exam be prepared
for interrogation!
‘Bone fibers’- matrix of connective tissue consisting of bundles of collagenous fibers, they
connect the PDL into the cementum.
Lamina Dura:
It is an internal layer of alveolar bone
It is cellular (osteocytes)
Periodontal fibers insert into it as Sharpey’s fibers
Sharpeys fibers

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 41
12. Phases of the tooth eruption
‘Eruption’ is the movement of teeth within and through the (alveolar) bone of the upper or
lower jaw and the overlying mucosa to reach the oral cavity.
There are 3 phases of tooth eruption:
1. Pre-eruptive phase
2. Pre-functional phase (or emergence phase)
3. Functional eruptive phase (or post-eruptive phase)
Teeth erupt at a maximal rate to reach occlusal contact, and then they continue to erupt at
a slower rate to compensate for growth and occlusal wear.
Eruption of the tooth is after completion of the crown.
Tooth development starts with mineralisation of enamel and ends with formation of the
apical foramen.
1. Pre-eruptive phase
o Movements of the developing and growing tooth germs within the alveolar process
before tooth formation
o The growing teeth move in various directions to maintain their position in the
expanding jaw, accomplished by the bodily movement and eccentric growth.
‘Bodily movement’ – shift of the entire tooth germ
‘Eccentric growth’ – part of the tooth continues to grow while the rest of the tooth
remains constant
Primary teeth move in an occlusal and facial direction with distal and mesial movement
Permanent teeth develop lingual to the levels of the incisial or occlusal levels of the
primary predecessors
All movements within this phase take place within the crypts of the developing and
growing crowns before root formation
1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 42
2. Pre-functional phase
o Starts with initiation of root formation
o Ends when the teeth reach occlusal contact
5 major events take place in this phase:
1. The secretory phase of amelogenesis is completed just before the onset of root formation
2. The intraosseous stage – root formation begins due to proliferation of epithelial root
sheath and mesenchymal tissue of the dental papilla and dental follicle.
3. The supraosseous stage – begins when the eruptive tooth moves occlusally through the
bone of the crypts and connective tissue of the oral mucosa
4. Clinical eruption- the tip of the crown enters the oral cavity by breaking through the
double layer of epithelial cells. (Half to three-quarters of the root has already been formed
by now.)
5. Active eruption - the erupting tooth continues to move occlusally at a maximum rate
(the clinical crown is exposed through the separation of the epithelium cells from the
crown)
Remember:
Clinical crown- part of the tooth exposed in the oral cavity
Anatomical crown- part of tooth covered by enamel
3. Functional eruptive phase
o Begins when teeth reach occlusion
o Continues for as long as the teeth remain in the oral cavity
o Alveolar process (alveolar bone) increases in height and density
o Teeth continue to move occlusally
o Roots continue to grown
Once occlusion is established….
Principle fibers of the PDL are established into separate groups
Nerves (for sensation- heat, cold, pain) develop from the apex to the gingival
Later in life… attrition may wear down the occlusal surface, so the teeth further erupt slightly
to compensate for the loss of tooth structure.
Mesial drift may occur- this is when the teeth move slightly medially (towards the midline).
This will cause bone slight bone resorption mesially and bone apposition distally.
Factors that affect tooth eruption:
Vasodilation – causes an increased eruption as blood vessels become bigger
Hyperemia- excess of blood in an area
o Summary: increased blood to the tooth causes faster tooth eruption
Stages in dentition (age):
Primary: 6-24 months

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 43
Permanent 6-18 years
Mixed (both primary and permanent): 6-12 years
13. Developmental dates of the teeth
Eruption dates:
Primary
Tooth Maxilla (months) Mandible (months)
Central Incisor 7.5 6.5
Lateral Incisor 8 7
Canine 16-20 16-20
1st Molar 12-16 12-16
2nd
Molar 20-30 20-30
Usually teeth erupt in pairs, one on right, one of left side
Permanent teeth erupt slightly earlier in girls than in boys
Mandibular teeth usually erupt earlier than maxillary teeth
Permanent
Tooth Maxilla (years) Mandible (years)
Central Incisor 7-8 6-7
Lateral Incisor 8-9 7-8
Canine 11-12 9-10
1st Premolar 10-11 10-12
2nd
Premolar 10-12 11-12
1st Molar 6-7 6-7
2nd
Molar 12-13 11-13
3rd
Molar 17-21 17-21
Mandibular teeth usually erupt earlier than maxillary
In the maxilla, first premolar erupts before the canine
Both in maxilla and mandible, first molar is before the canine
The first molar is usually the first permanent tooth to erupt
---------
The above information seems to be enough for this topic. But since the topic is titled as
“Developmental dates of teeth”, he could ask you about the dates of first calcification,
crown completion, root completion etc… so I have inserted a table from Wheeler’s Dental
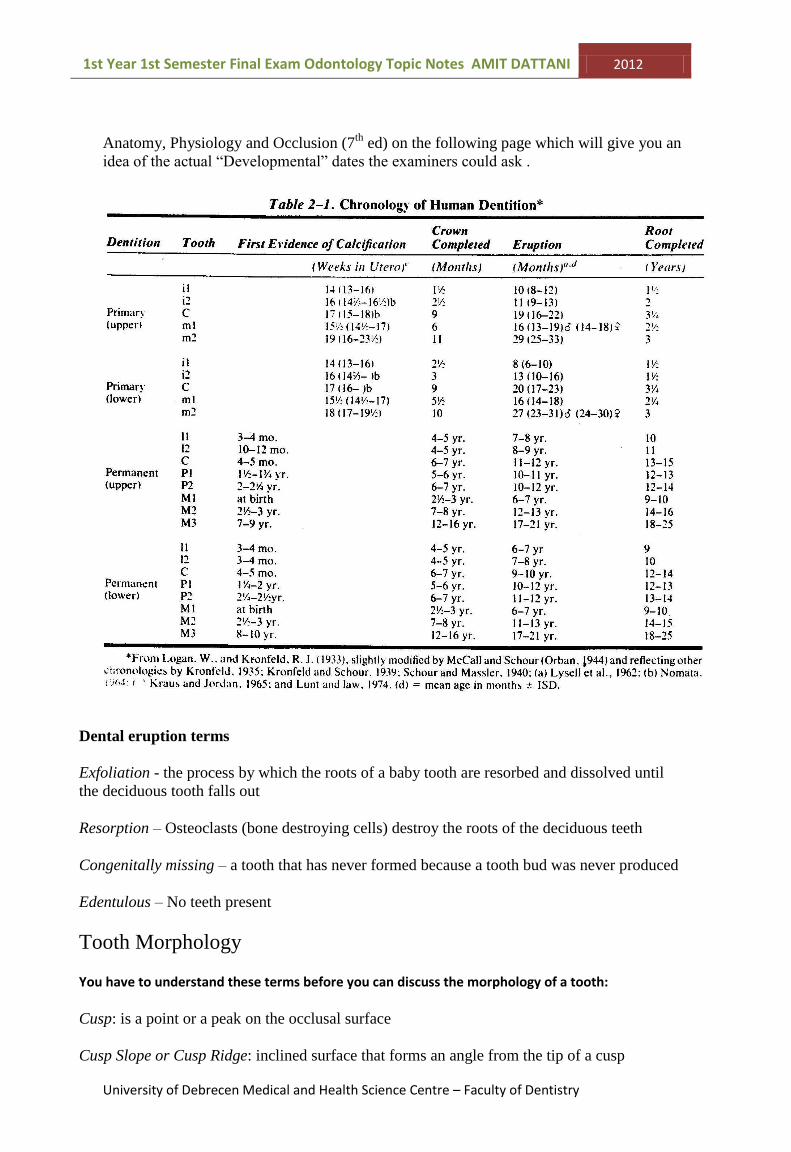
1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 44
Anatomy, Physiology and Occlusion (7th
ed) on the following page which will give you an
idea of the actual “Developmental” dates the examiners could ask .
Dental eruption terms
Exfoliation - the process by which the roots of a baby tooth are resorbed and dissolved until
the deciduous tooth falls out
Resorption – Osteoclasts (bone destroying cells) destroy the roots of the deciduous teeth
Congenitally missing – a tooth that has never formed because a tooth bud was never produced
Edentulous – No teeth present
Tooth Morphology
You have to understand these terms before you can discuss the morphology of a tooth:
Cusp: is a point or a peak on the occlusal surface
Cusp Slope or Cusp Ridge: inclined surface that forms an angle from the tip of a cusp

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 45
Cingulum: an enlargement or bump located on the crown lingually along the gingival or CEJ
(Cemento-enamel junction) on the anterior teeth
Ridge: longitudinal convexities of enamel (raised border)
Labial ridge: alinear elevation located on the labial side of the incisors/canines
Buccal ridge: alinea elevation located on the buccal side of the premolars/molars
Cusp ridge: an elevation that extends in the mesial and distal direction from the cusp
tip
Marginal ridge: elevated crests of enamel of the tooth where the sides meet the top –
the borders around the crown
Oblique ridge: elevated prominences on the occlusal surface of maxillary molars from
the tip of the mesiolingual to distobuccal cusp (only on maxillary molars is the
Distobuccal cusp and the Mesiolingual cusp).
Triangular ridge: prominent elevations, triangle in cross-section, extend from the tip
of a cusp towards the central portion of the occlusal surface. On ALL posterior teeth
Transverse ridge: made up of triangular ridges of a buccal and lingual cusp which join
to form a continuous elevation (one cusp to another)
Mamelon: a rounded prominence on the incisial ridge of a newly erupted incisor, usually
disappears as the result of mechanical wear (attrition).
Sulcus: broad depression / valley on the occlusal surface of a posterior teeth
formed by inclines of adjacent cusps or ridges which meet at an angle
Groove: A small linear depression on the surface of a tooth (It is not the kind
of groove you get on at a party!)
Developmental groove: a groove formed by the union of two lobes. It is a sharply
defined narrow linear depression
Supplemental groove: an indistinct linear depression, irregular in extent and direction
Lobe: a development segment of the tooth. As lobes develop they join to form a single unit
Fossa: a rounded / angular depression of varying size on the surface of the tooth – on ALL
posterior occlusal surfaces

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 46
Pits: when two fissures cross, they form a pit
Fissure: a fault occurring along a developmental groove caused by incomplete or imperfect
joining of lobes
Convex: curving outward or away from the focus
Concave: curving inwards or towards the focus
14. Description of permanent maxillary incisors
Maxillary Central Incisor
Root 1
Root canal 1
Pulp horns 3
Cusps 0
Eruption 7-8 years
1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 47
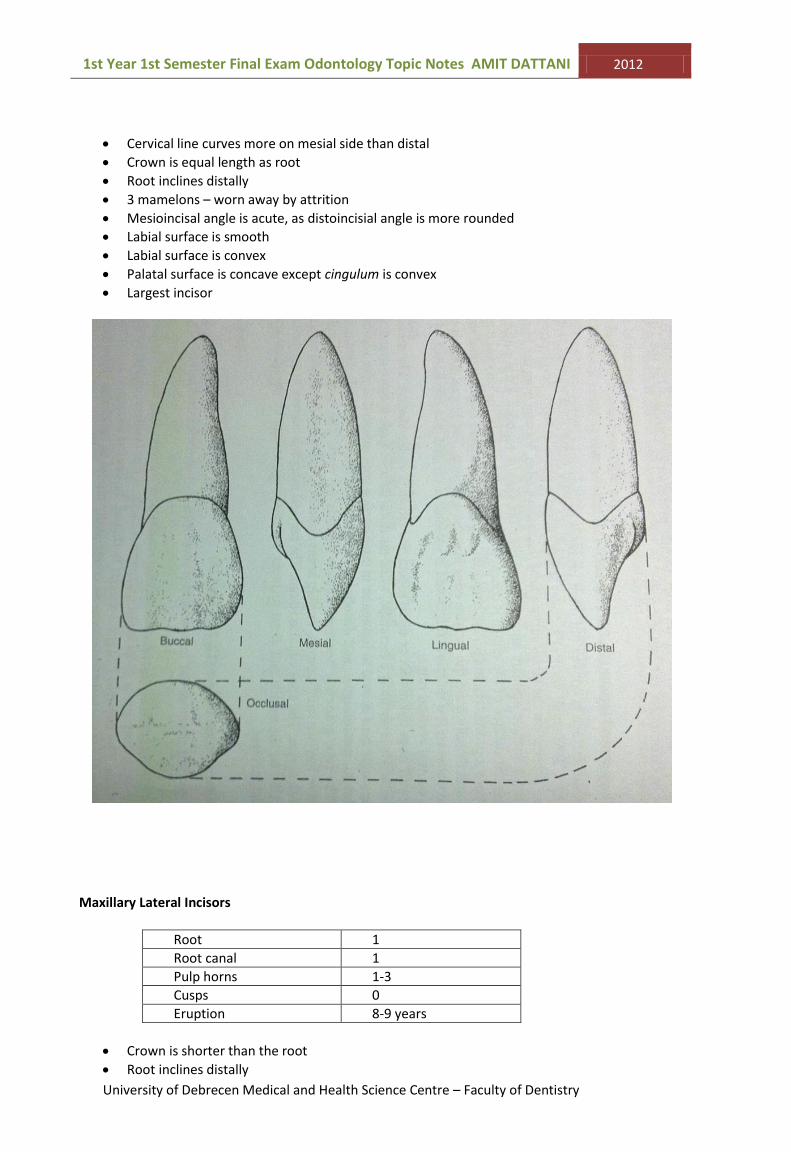
Cervical line curves more on mesial side than distal
Crown is equal length as root
Root inclines distally
3 mamelons – worn away by attrition
Mesioincisal angle is acute, as distoincisial angle is more rounded
Labial surface is smooth
Labial surface is convex
Palatal surface is concave except cingulum is convex
Largest incisor
Maxillary Lateral Incisors
Root 1
Root canal 1
Pulp horns 1-3
Cusps 0
Eruption 8-9 years
Crown is shorter than the root
Root inclines distally

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 48
Mesioincisal angle is acute, as distoincisal edge is more rounded
Labial surface more convex than Central incisor
Palatal surface more concave than Central
Less curvature on cervical line than Central
Smaller and narrower than central
Cingulum not as well developed in Lateral
Differences between Maxillary Central and Maxillary Lateral Incisor (topic 16)
Lateral crown is smaller (generally) and narrower
Root is same length
Lateral Distoincisal angle is more curved than Central distoincisal
The pulp is relatively Large in Lateral
Labial surface more convex in Lateral than of Central
Palatal surface is more concave in Lateral than Central
Less curvature of cervical line on Mesial surface of Lateral than Central
More prominent marginal ridges in Lateral than Central

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 49
Cingulum not as well developed in Lateral
15. Description of permanent mandibular incisors
Mandibular Central Incisor
Root 1
Root canal 1 or 2
Pulp horns 3
Cusps 0
Eruption 6-7 years

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 50
Root inclines distally
Root is oval shaped in cross-section
Mesioincisal and Distoincisal angles nearly identical
3 mamelons – worn away by attrition
Lingual surface is smooth
Distal groove is more marked
Smallest permanent tooth
Straight incisal edge
Small cingulum
Mandibular Lateral Incisor
Root 1
Root canal 1
Pulp horns 3
Cusps 0
Eruption 7-8 years

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 51
Mesial side longer than distal, producing a slope
Mesioincisal angle acute, distoincisal angle rounded
3 mamelons
Groove on mesial and distal surface
Differences between Mandibular Central and Mandibular Lateral Incisor (topic 16)
Lateral is slightly larger than the Central
Incisive edge is longer mesiodistally
Distal side of Lateral is rotating lingually
Crown of lateral slopes down towards distal side
Difference between Maxillary and Mandibular Incisors (topic 16)
Maxillary have more pronounced lingual fossae
Maxillary have roots that are more rounded in cross-section
Mandibular have smoother lingual anatomy without grooves and pits
Mandibular crowns are smaller and narrower relative to length
Mandibular crowns are flatter mesially and distally than Maxillary

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 52
17. Description of permanent maxillary canine
Maxillary Canine
Root 1
Root canal 1
Pulp horns 1
Cusps 1
Eruption 11-12 years

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 53
Largest and strongest tooth in mouth
All surfaces are convex
Large pointed cusp, tips placed approximately centrally
Distal slope longer than mesial
Great bulk of dentine
Bulky cingulum
Root is almost triangular in cross-section
Root inclines distally
18. Description of permanent mandibular canine
Mandibular Canine
Root 1
Root canal 1 or 2
Pulp horns 1
Cusps 1
Eruption 9-10 years

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 54
Single cusp not as pointed as in maxillary
Marginal ridge and cingulum less well developed
Crown tilts distally since mesial surface is a straight line
Well marked cingulum on lingual surface
Root possibly flattened Mesially and Distally
Vertical Mesial and Distal grooves may be present on root
Only canine that is capable of bifurcated root
Crown and root tends to lean distally
Differences between Maxillary and Mandibular Canines
Maxillary has larger pulp cavity than Mandibular
Mandibular crown is narrower mesiodistally
Mandibular cusp on incisive edge is less pointed
Cingula on Maxillary are larger and centred mesiodistally, mandibular are slightly to the distal

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 55
19. Description of maxillary premolars
Maxillary 1st Premolar
Root 2 (Buccal & Palatal- curve distally)
Root canal 2 (one in each root)
Pulp horns 2
Cusps 2 sharply defined (buccal larger than Lingual)
Eruption 10-11 years

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 56
Concave canine fossa on mesial surface of crown extending to pronounced longitudinal groove on mesial surface of root
Mesial surface of buccal cusp longer than distal Pulp tilts slightly mesially Occlusal outline more angular than maxillary 2nd Premolar Grooves form letter ‘H’ on the occlusal surface
Maxillary 2nd Premolar
Root 1 (flattened mesiodistally, curves distally)
Root canal 1
Pulp horns 2
Cusps 2 (nearly equal in size, buccal larger)
Eruption 10-12 years

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 57
No canine fossa Oval Occlusal outline Mesial slope of buccal cusp shorter than distal slope Grooves form letter ‘H’ on the occlusal surface
20. Description of mandibular premolars
Mandibular 1st Premolar
Root 1 (curves distally)
Root canal 1
Pulp horns 2
Cusps 2 (sharply defined -buccal larger than lingual)
Eruption 10-12 years
1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 58
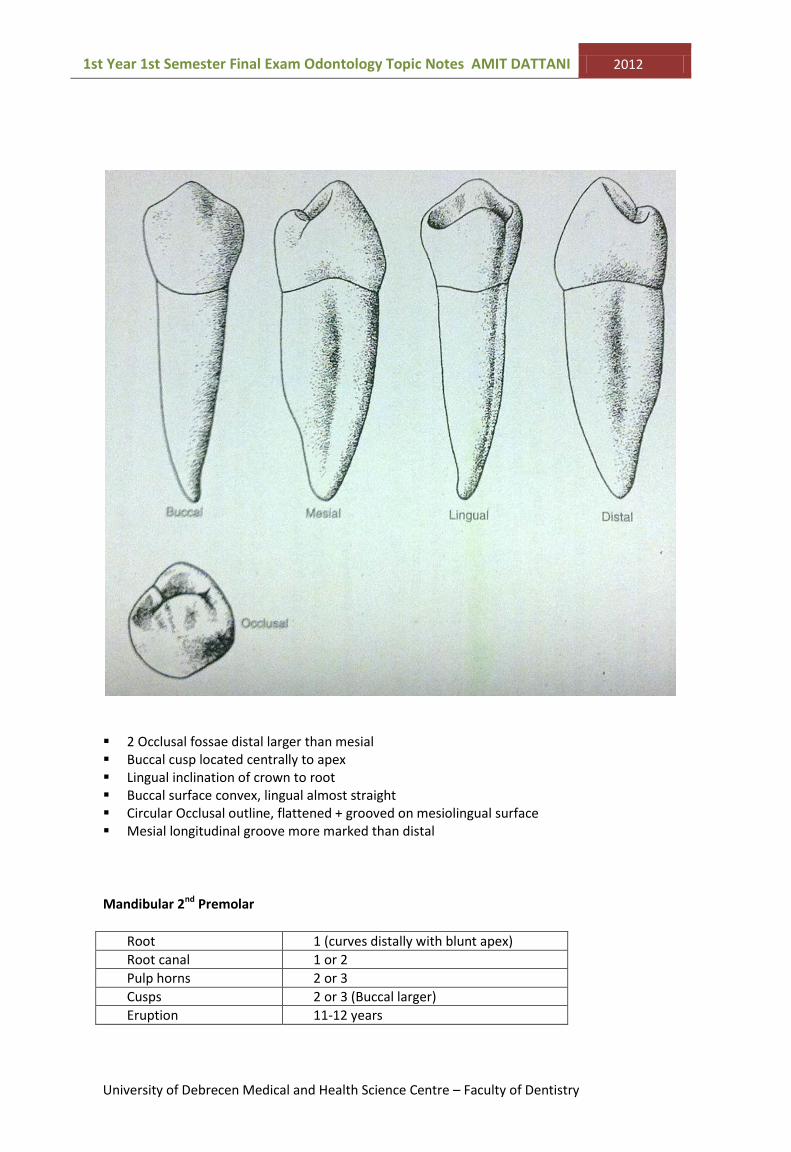
2 Occlusal fossae distal larger than mesial Buccal cusp located centrally to apex Lingual inclination of crown to root Buccal surface convex, lingual almost straight Circular Occlusal outline, flattened + grooved on mesiolingual surface Mesial longitudinal groove more marked than distal
Mandibular 2nd Premolar
Root 1 (curves distally with blunt apex)
Root canal 1 or 2
Pulp horns 2 or 3
Cusps 2 or 3 (Buccal larger)
Eruption 11-12 years

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 59
Occlusal outline like square-ish Mesial marginal ridge higher than distal No longitudinal grooves present
21. Differentiation of premolars
Difference between Maxillary and Mandibular Premolars
Mandibular crowns tilts lingually, so lingual cusp tips may be lingual to root Outline of Mandibular is rhomboidal shape as Maxillary is trapezoidal Mandibular lingual cusps are relatively MUCH shorter than mandibular buccal cusps
1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 60
Difference between Maxillary 1st Premolars and Maxillary 2nd Premolars
Maxillary 1st premolars usually have a divided root as Maxillary 2nd premolars usually have only 1 root
Maxillary 1st premolar buccal cusp larger than Lingual cusp Maxillary 2nd premolar has NEARLY equal sized cusps (buccal and lingual) Maxillary 1st premolars buccal cusp is more pointed than Maxillary 2nd premolars buccal cusp Maxillary 1st premolars occlusal surface is asymmetrical with mesial marginal ridge as
Maxillary 2nd premolars being more symmetrical with no mesial marginal ridge. Distance between the two cusps maybe greater in difference in the 1st premolar
Difference between Mandibular 1st Premolars and Mandibular 2nd Premolars
Mandibular 1st premolar buccal cusp is more pointed than Mandibular 2nd premolar buccal cusp
Mandibular 1st premolar lingual cusp is small and non-functional as Mandibular 2nd premolar cusp is functional and relatively longer
Mandibular 1st premolars have a mesiolingual groove separating the mesial marginal ridge from the lingual cusp, not found on Mandibular 2nd premolars
22. Description of permanent maxillary molars
Maxillary 1st Molar
Root 3 (1 lingual and 2 buccal)
Root canal 3 or 4
Pulp horns 4
Cusps 5 (5th is tubercle of Carabelli-non functioning)

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 61
Eruption 6-7 years

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 62
Three well developed separate roots Palatal root longest and thickest, it develops away from 2 buccal roots Buccal roots tend to curve distally Rhomboidal occlusal outline Largest maxillary tooth Mesiopalatal cusp largest Distopalatal cusp smallest Buccal cusps more pointed than palatal Crown wider buccolingually than mesiodistally 5th cusp located on the lingual side of the mesiolingual cusp Mesiolingual cusp is the largest of the four functioning cusps Mesiobuccal root has 1 or 2 root canals
Maxillary 2nd Molar
Root 3 (slight distal inclination)
Root canal 3
Pulp horns 3 or 4
Cusps 4
Eruption 12-13 years

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 63
Occlusal Palatal Buccal
Distal Mesial
Rhomboidal occlusal outline Distal cusps greatly reduced in size 3 roots less divergent Buccal roots same length, closer together Coalescence of roots more common than Maxillary 1st molar All roots same length as Maxillary 1st molar Roots more slender and lie closer together than Maxillary 1st Molar Prominent palatal and buccal developmental grooves
Maxillary 3rd Molar

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 64
Root 3 (short, often fused and curve distally)
Root canal 1
Pulp horns 3
Cusps 3 -5 (1 lingual and 2 buccal)
Eruption 17-21 years
Occlusal Palatal Buccal
Distal Mesial
Triangular occlusal outline Largest cusp is Mesiopalatal Crown appears too big for (short and fused) roots

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 65

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 66
23. Description of permanent mandibular molars
Mandibular 1st Molar
Root 2 (1 mesial and 1 distal- curved distally)
Root canal 3
Pulp horns 5
Cusps 5 (3 buccal, 2 lingual)
Eruption 6-7 years

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 67
1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 68
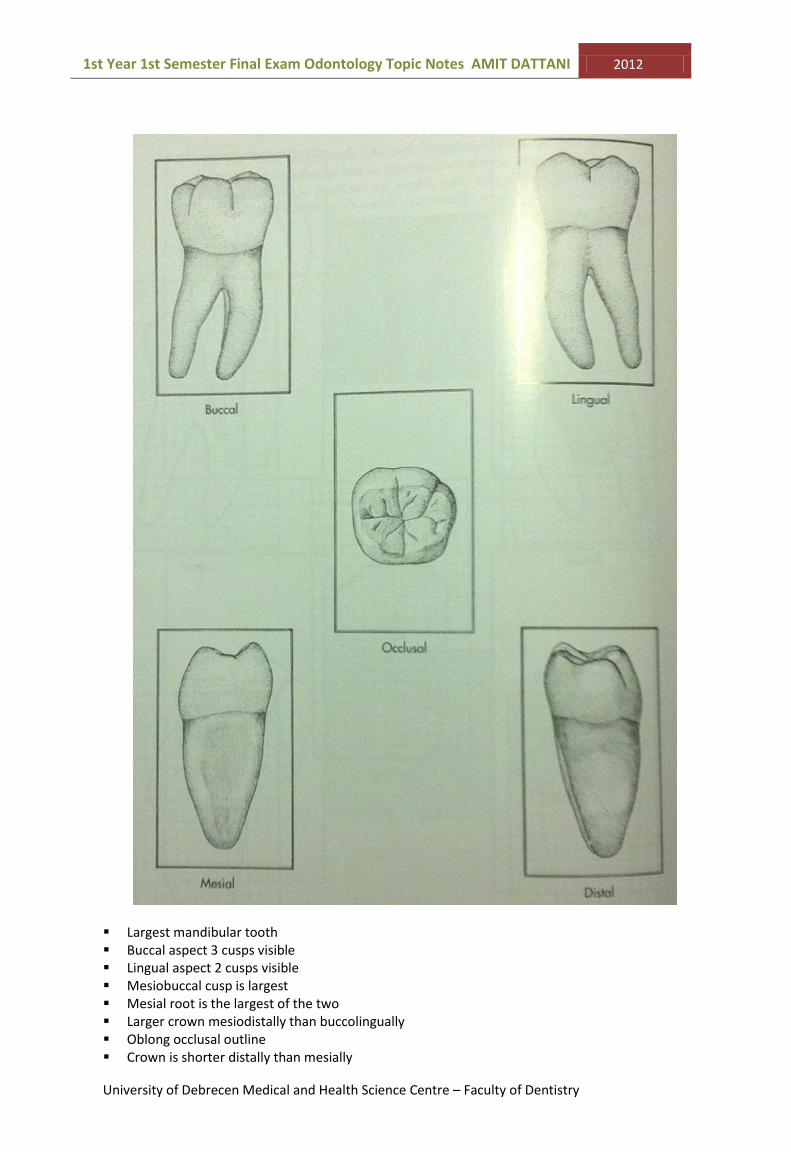
Largest mandibular tooth Buccal aspect 3 cusps visible Lingual aspect 2 cusps visible Mesiobuccal cusp is largest Mesial root is the largest of the two Larger crown mesiodistally than buccolingually Oblong occlusal outline Crown is shorter distally than mesially

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 69
Crown seems asymmetrical as buccal side longer than lingual side ‘S’ shape on occlusal surface
Mandibular 2nd Molar
Root 2 (close together, partially fused, curved distally)
Root canal 3
Pulp horns 4
Cusps 4
Eruption 11-13 years
Occlusal Lingual Buccal
Distal Mesial
Rounded-square occlusal outline Lingual cusp higher than buccal Mesial cusp larger than distal Mesial root larger than distal Crown usually smaller than Mandibular 1st Molar

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 70
Roots not as robust but maybe longer than Mandibular 1st Molar Distobuccal cusp is larger than that of the Mandibular 1st Molar Two buccal cusps of equal height Roots not as broad than of the Mandibular 1st molar ‘+’ shape on occlusal surface
Mandibular 3rd Molar
Root 2 (close together, sometimes fused, curved distally)
Root canal 3
Pulp horns 4
Cusps 4-6
Eruption 17-21 years
Mandibular 3rd Molar patterns (in the Right molar)
They can have between 4-6 cusps and the patterns are shown. (Left)
The 3rd molar can vary in shape and position – usually malformed All cusps are short and round Square occlusal outline

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 71
Marked convex buccal surface inclined lingually Roots often underdeveloped, short and thick Roots acutely incline distally
24. Differentiation of molars
There can be a lot you can say about this topic due to the different characteristics shown by
each molar.

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 72
You can start comparing the upper and lower molars and by mentioning the:
Number of roots in the upper and lower molars
The direction of the roots (mesio-distal or bucco-lingual)
The number of root canals in each moalr
You can then compare each molar individually e.g. 1st upper and 1
st lower molar, etc…
(Tip: if you learn the bullet point list on each tooth then this will be very easy!)
The tables below should be learnt extremely well.
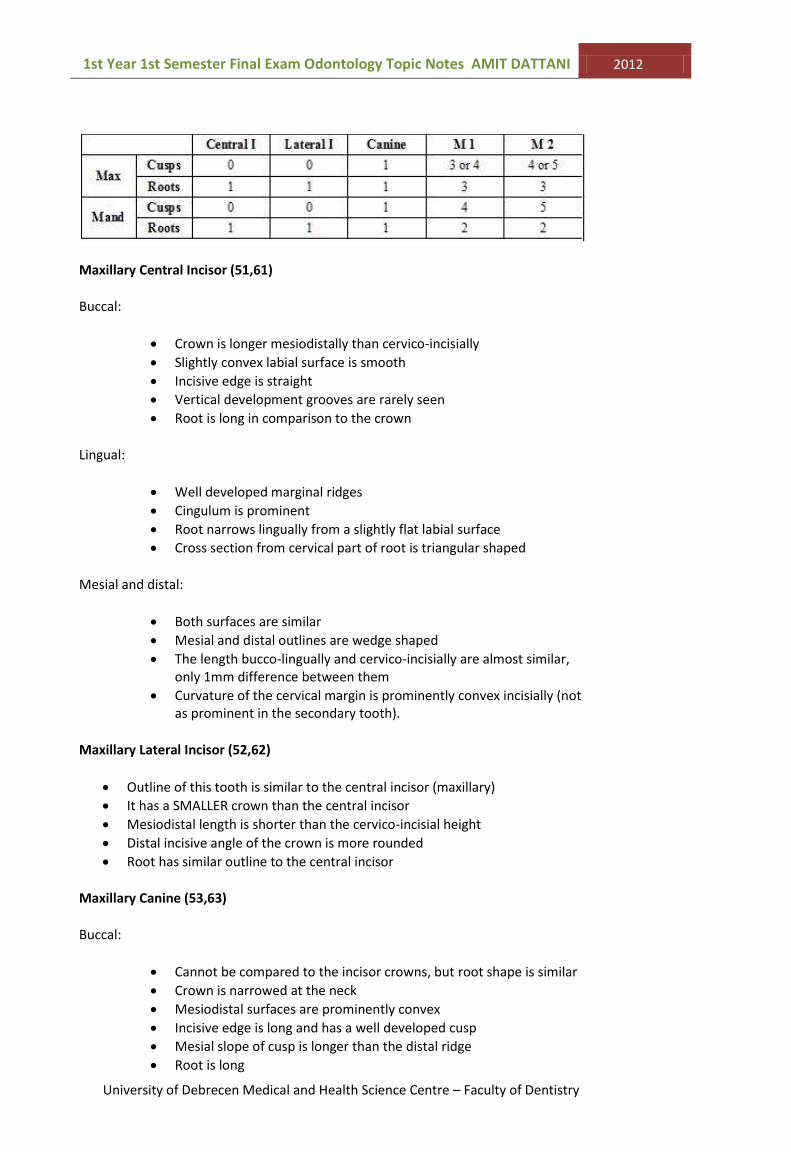
Permanent Maxillary
Permanent Mandibular

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 73
25. Morphology of maxillary deciduous teeth
1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 74
Maxillary Central Incisor (51,61)
Buccal:
Crown is longer mesiodistally than cervico-incisially
Slightly convex labial surface is smooth
Incisive edge is straight
Vertical development grooves are rarely seen
Root is long in comparison to the crown
Lingual:
Well developed marginal ridges
Cingulum is prominent
Root narrows lingually from a slightly flat labial surface
Cross section from cervical part of root is triangular shaped
Mesial and distal:
Both surfaces are similar
Mesial and distal outlines are wedge shaped
The length bucco-lingually and cervico-incisially are almost similar, only 1mm difference between them
Curvature of the cervical margin is prominently convex incisially (not as prominent in the secondary tooth).
Maxillary Lateral Incisor (52,62)
Outline of this tooth is similar to the central incisor (maxillary)
It has a SMALLER crown than the central incisor
Mesiodistal length is shorter than the cervico-incisial height
Distal incisive angle of the crown is more rounded
Root has similar outline to the central incisor
Maxillary Canine (53,63)
Buccal:
Cannot be compared to the incisor crowns, but root shape is similar
Crown is narrowed at the neck
Mesiodistal surfaces are prominently convex
Incisive edge is long and has a well developed cusp
Mesial slope of cusp is longer than the distal ridge
Root is long

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 75
Lingual:
Prominent vertical enamel ridge
Central cingulum is seen with mesial and distal marginal ridges
Lingual tubercle on the cusp tip is an elongation of the lingual ridge connecting cingulum and cusp
Lingual fossa divides the mesiolingual and distolingual halves
Mesial and distal:
Outlines are similar to the incisor’s mesial and distal aspects, but the crown is more robust in its cervical third.
Maxillary 1st Molar (54, 64)

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 76
Greatest length of the crown is between mesial and distal contact areas where the crown narrows cervically
Roots are thin, long and divergent (3 roots)
Three roots (2 buccal ,1 palatal)
Distal root is shorter than the mesial root
Division of roots is close to the cervical margin
Lingual root is the thickest
From occlusal view: the buccal surface of crown is longer than the lingual surface
2 main cusps: o Buccal o Lingual
Buccal cusp is an elongated ridge that may be partially divided into 2 or 3 smaller cusps by developmental grooves
Usually one prominent buccal developmental groove
Shallow central developmental groove present, but broad
Lingual cusp is usually divided into a large mesiolingual and smaller distolingual cusp by a distal developmental groove
The distal marginal ridge is small compared to the mesial marginal ridge.
Buccal surface of the crown shows a prominent bulge close to the cervical margin and opposite a mesiobuccal root
Cervical margin slopes in a gingival direction mesially on the buccal side, relatively straight lingually and shows a slight mesial and distal occlusal convexity.
Maxillary 2nd Molar (55,65)
Marked divergence of roots
Bulbous shape of crown
Narrowed cervical area
Short root stem
Primary second molar resembles the permanent second molar
Cusps and roots have a similar arrangement
Mesiolingual cusp is the largest and is connected to the distobuccal cusp by a low oblique ridge.
Large mesial fossa and smaller distal fossa
Tubercle of Carabelli is often present on the lingual surface of the mesiolingual cusp
Buccal cusps are almost equal size, separated by a buccal developmental groove
Occlusal surface has a central fossa with a central pit
Well developed triangualar mesial fossa with a mesial pit
Oblique ridge present in the distal triangualar fossa
Cervical line resembles the 1st molar (primary).

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 77
26. Morphology of mandibular deciduous teeth

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 78
Mandibular Central Incisor (71,81)
Buccal:
Relatively flat without developmental grooves
Mesial and distal sides become narrower cervically from the contact area
Crown is wide in comparison to cervico-incisially
Root is long and thin, narrows to a sharp apex
Incisive edge is straight
Lingual:
Cingulum and marginal ridges present
In middle and incisial third the lingual surface is flat or may have a lingual fossa
Crown and root narrow lingually
Mesial:
Typical outline of an incisor
Generally smaller tooth than upper incisor
Labio-lingually its 1 mm shorter than the upper incisor labio-lingually
Nearly flat root
Root narrows gradually apically
Cervical outline is similar to other incisors
Distal:
Outline is similar to mesial aspect of tooth
Cervical margin is less prominent in convexity incisially
Mandibular Lateral Incisor (72,82)
Similar to central incisor but slightly larger in all dimensions except labio-lingually
Cingulum maybe somewhat larger
Lingual surface is more concave than the maxillary lateral incisor
Incisive edge shows greater tendency to descent distal
Mandibular Canine (73,83)
Few differences between maxillary and mandibular canine, except for dimensions
Tooth is smaller, especially labio-lingually than the maxillary
Cervical convexities are less prominent (labially and lingually)
Striking difference is: longer distal cusp ridge compared to mesial cusp ridge (in contrast to the ridges of the maxillary canine)

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 79

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 80
Mandibular 1st Molar (74,84)
Occlusal surface is elongated mesiodistally
4 cusps, relatively indistinct
This tooth does not resemble any other molar
Mesial surface descends nearly vertically from the contact area
Distal surface convexity is similar to other deciduous molars
Cervical margin opposite the mesial root descends apically
Cervical margin is straight on lingual surface, slight convexity towards occlusal direction on the mesial and distal surfaces
Buccal surface of crown shows prominent bulge near cervical line
2 roots, mesial and distal
Roots are long, thin and divergent
Occlusally, the mesiolingual cusp is the largest and is separated by a small distolingual cusp by a lingual developmental groove
Buccal developmental groove separates the two buccal cusps
Large distal fossa, central development groove (CDG) starts here
CDG passes between mesiolingual and mesiobuccal cusps and ends in a mesial pit, in the smaller triangualar fossa.
Mandibular 2nd Molar (75,85)
Apart from general differences, this tooth resembles the permanent lower 1st molar- same number and arrangement of cusps and roots
Crown in comparison to the 1st primary molar, shows a more bulbous shape by a mesio-cervical constriction (not descending in a straight line)
Much larger than the 1st primary molar
Mesial and distal roots are long, thin and divergent. Bifurcate close to cervical margin
Occlusal surface has 5 cusps, (3 buccal + 2 lingual)
3 buccal cusps are more or less same size as are the lingual cusps
Total mesiodistal buccal surface is longer than the length of the lingual surface
Irregular central developmental groove runs from a mesial pit in the mesial triangular fossa to the distal pit in the distal triangular fossa
Transverse developmental grooves separate the 3 buccal cusps and 2 lingual cusps
The mesial and distal grooves continue as the buccal developmental groove and the lingual separates the two lingual cusps
Cental pit is where the lingual and mesiobuccal grooves meet the central groove

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 81

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 82
Articulation (occlusion) of the deciduous dentition
1. Mesial surfaces of upper and lower central incisors meet at midline of dental arch
2. Upper central incisors articulate with the lower central incisor and the mesial third of the lateral incisor. The incisive edges of the lower anterior teeth make contact with the lingual surface of the upper incisors.
3. Upper lateral incisor articulates with the lower lateral incisor and part of the lower canine mesially
4. Upper canine articulates with the remaining distal part of the lower canine crown and the mesial part of the 1st lower molar
5. The upper 1st molar articulates with the distal two-thirds of lower 1st molar and the mesial part of the 2nd lower molar
6. The upper 2nd moalr articulates with the remaining part of the lower 2nd molar and extends distally, beyond the distal surface of the lower 2nd molar
Mineralisation and eruption
Mineralisation begins at about 4 months of intra-uterine life
By 6 months all teeth are actively mineralised
Usually no teeth present in mouth at birth
Statistics only show an AVERAGE time of mineralisation, eruption etc… but cannot be used EXACTLY because no two individuals develop the same way.
Differences between the Deciduous and Permanent Teeth
1. Deciduous teeth are smaller overall than the permanent
2. Enamel of deciduous is whiter and more opaque, therefore, crown is a
lighter colour than permanent tooth

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 83
3. Enamel of deciduous is more permeable and more easily worn down but
permeability is lessened when tooth resorption starts
4. Depth of enamel is thinner and more consistent in deciduous (0.5-1mm
thick) and is 2.5mm thick in permanent
5. Deciduous have a pronounced cervical margin, the enamel bulges at the CEJ
6. Deciduous anterior crowns are bulbous with a pronounced cingulum
7. Newly erupted deciduous crowns are more pointed than permanent
8. Deciduous roots are shorter, less strong and lighter in colour than
permanent
9. Deciduous:
Anterior roots are longer in proportion to crown
Posterior are more divergent to allow for developing permanent
successor, they flare out more from each other wider than crown
10. Permanent pulp chambers are larger and follow exterior morphological
shape of tooth, tendency of less dentine
11. Deciduous root canals are very fine
12. Deciduous teeth have a more constant morphology, with less variations
than permanent
13. Deciduous CEJ is less sinuous than permanent
14. Deciduous dentition has 20 teeth, permanent has 32 teeth

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 84
27. Physical and chemical properties of enamel
(see topic 4 – enamel part)
28. Enamel structure and formations
Basic structural components are the enamel rods / prisms.
The enamel rods have a round head and a narrow tail. The heads are commonly directed
towards the incisal edge /towards cusps and the tail towards the necks.
The rods are composed of hexagonal hydroxyapatite crystals. Crystals have different
orientation (heads and tails) with respect to the Tomes Process.
Lines of Retzius:
Brown lines begin at the amelodentinal junction and reach the surface of the enamel. Each
line indicates amelogenesis. The first line surrounds the dentin tip. Lines of retzius form as a
result of disturbed mineralisation. The place where the lines meet the surface of enamel,
shallow grooves are seen, called perikymata.
Bands of Hunter-Schreger: Longitudinal cross-sections of enamel viewed by reflected light, appears as light and dark
bands, found in the inner part of enamel. It is caused by successive changes in direction,
followed by groups of enamel rods in the horizontal plane, which cause change in the angle of
light.

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 85
Enamel Tufts: Small branching defects found only at the DEJ, projecting into the enamel, have no clinical significance.
Enamel Spindles: Dentinal tubules found within the enamel – more abundant in cusp tips. Arise when a single odontoblasts process invades the pre-ameloblast layer during dentin development.

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 86
Enamel Lamellae: (Thin unmineralised structures) Primary: in unerupted teeth, due to shrinkage of enamel during final stages of amelogenesis Secondary: in post-eruptive phase, has the same appearance but as a result of occlusal trauma
Tomes process: Secretory surface of amelogenesis

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 87
Amelogenesis occurs in the crown stage of tooth development, always AFTER dentin formation
2 main stages of Amelogenesis
1. Secretory stage- in which proteins and organic matrix form a partially mineralised enamel 2. Maturation stage – mineralisation is completed
Secretory:
Cells of inner enamel epithelium differentiate to form ameloblasts, release enamel proteins
Enamel matrix mineralised by enzyme, alkaline phosphate
Enamel formation continues outward, away from the dentin
After first layer, the tomes process is produced
Maturation:
Ameloblast stops producing enamel
Starts to transport proteins used to complete mineralisation
29. Physical and chemical properties of dentine

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 88
Dentine forms the main bulk of the tooth, it is composed of: o 70% inorganic material (mainly hydroxyapatite) o 20% organic (mainly collage and lipids etc…) o 10% water
Softer than enamel but harder than cementum
Inner dentine is softer than outer dentine
Dentine has a tubular structure – therefore dentine has a higher permeability than enamel
Dentine has nerves and so is sensitive
Types of Dentine
Mantle dentine o First formed dentine – a the DEJ i.e. closest to enamel o Less mineralised than primary dentine
Primary dentine o Forms bulk of the tooth o Very regular tubular structure o When the root apex is closed (during formation) the primary dentine is finished
and secondary dentine starts formation
Secondary dentine o Formed after root formation o Formed slower than root formation o Less regular tubular structure than primary dentine o Its deposition reduces the pulp chamber
Tertiary dentine / reparative dentine o Deposited in reaction to noxious / traumatic stimuli e.g. caries, dental
procedures – it protects the pulp o Deposited in a localised area o Has a very few and irregular tubules
Predentine o Not completely mineralised layer 10-20um wide o Remains between odontoblasts and mineralised dentine o Contains a lot of organic matrix o After inorganic materials deposited (hydroxyapatite crystals) it becomes
mineralised to primary dentin o Predentine is mineralised in spherical forms,then the spherical forms fuse
together and predentine forms primary dentine
Physical properties
Main bulk of tooth
Living tissue with a tubular structure
Yellowish-white in permanent teeth
It is sensitive tissue, it contains very small nerve branches
It is elastic and permeable
Age affects permeability and hardness. o With age it becomes less permeable o With age hardness increases
Softer than enamel but is harder than cementum
Softer inner part of dentine
Dentine is a tooth germ in the bell stage

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 89
Inner cell of dental papilla will differentiate into odontoblasts (dentine forming cells later)
Functions of dentine
Acts as a main (bulk) portion of a tooth
Protects the pulp
Supports enamel
30. Dentine structure and formations
The three main types of dentine are primary, secondary and tertiary (topic 29)

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 90
Odontoblasts are dentine forming cells
A single cell layer covers the pulpal surface and can have different forms
They are functioning as living cells as long as the tooth is vital and when needed they react to stimulus in order to form tertiary dentine
Odontoblast processes are cytoplasmic extensions that enter the dental tubules. Each process has branches and it has a secretory function.
Dental tubules: are narrow parallel channels that do not follow a straight course. They have two curvatures, a primary and a secondary. “S” shaped curvature – primary, are layered. A secondary curvature can be seen under higher magnification. Some tubules can penetrate through the enamel (enamel spindles).
o Inside the tubules we can find odontoblasts processes and fluid o Around the tubules we can find two kinds of dentine:
1. Peritubular dentine:
o Which circles the tubules like a ring o Very hard o Highly mineralised o Absent in the pre-dentin and interglobular dentine o Its thickness increases with age
2. Intertubular dentine: o Found between tubules o Softer than peritubular dentine o It is built from a well organised collagen fiber network
Sometimes we can find small areas in the dentine, which are not fully mineralised. We can divide these into two groups:
Interglobular dentine: irregularly shaped structures near the ADJ (amelodentinal junction)
Granular layer of Tomes: near cementum, seen as dark areas, resulting from irregular loops of the dentinal tubules. (see image)
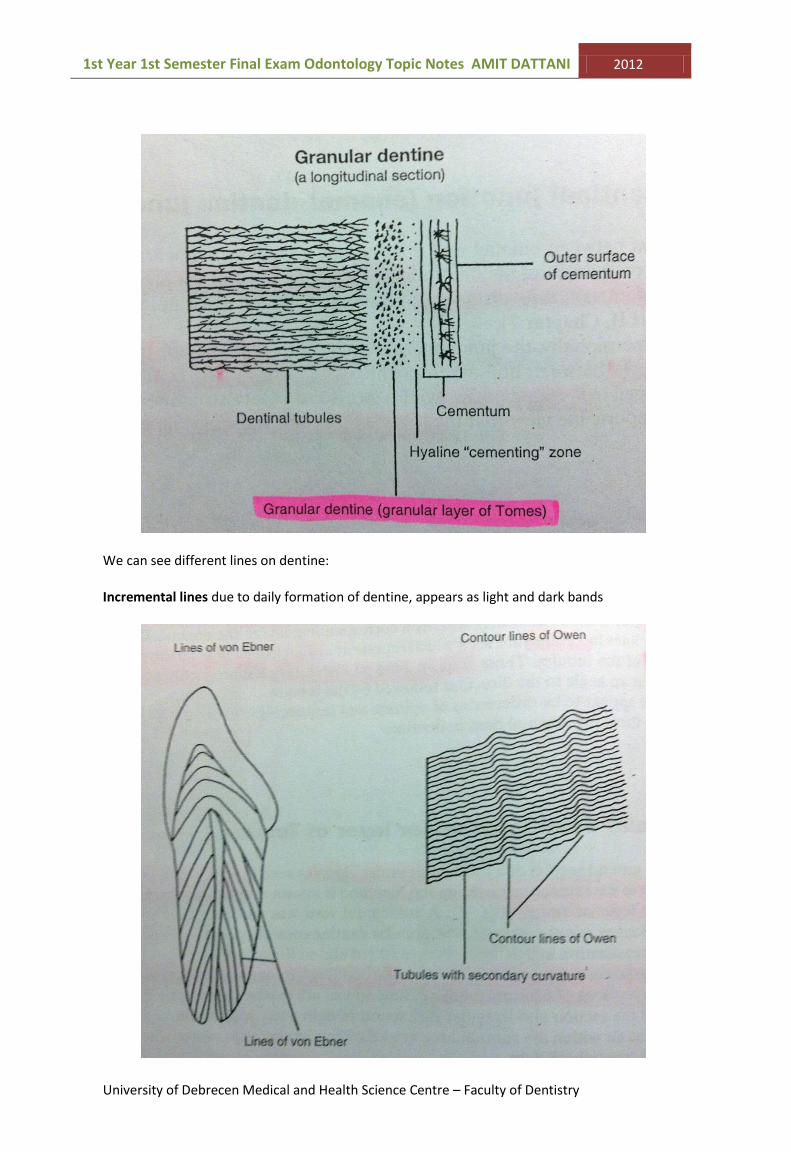
1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 91
We can see different lines on dentine:
Incremental lines due to daily formation of dentine, appears as light and dark bands

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 92
1. Contour lines of Owen: different events of major changes in body metabolism, might cause hypomineralisation of the dentine
2. Neonatal lines (lines of Von Ebner): hypomineralisation line, can be seen only in milk teeth or permanent first molars
Dentine formation: dentinogenesis is the first identifiable stage in the crown stage and root development.
It must occur before enamel formation
The different stages result in different kinds of dentine formation
Odontoblasts differentiate from the dental papilla
31. Structure of the pulp
32. Functions of the pulp
The dental pulp consists of a delicate vascular connective tissue with specialised cells
The pulp is concerned with reactions of the tooth to stimuli
It has 5 main functions:
1. Inductive and formative function o Interacts with the inner enamel epithelium and leads to differentiation of
odontoblasts into dentine o …this leads on to the differentiation of ameloblasts to form enamel.
2. Reparative function o Acts as a method of protection to isolate the pulp from any kind of stimuli e.g. low
grade attrition 3. Defensive, or protective function
o Causes an inflammatory response in the pulp in reaction to acute irritation e.g. bacteria, deep cavity preparation or irritating filling.
4. Nutritive function o The blood nourishes dentine and enamel through odontoblasts
5. Sensory function o Stimuli causes pain which acts as a protective function

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 93
General appearance and structure
The dental cavity within each tooth is occupied by the dental pulp, which is surrounded by dentine except for the apical foramen, which is surrounded by cementum.
The pulp chamber can be theoretically split into two parts, the coronal pulp and the radicular pulp (root pulp)
The pulp communicates with the periapical tissues (tissues around the root) through its foramen. The foramen consists of nerves, blood vessels and lymph vessels passing through.
It is normal to see more than one small accessory foramen that connects the root canal to the periapical tissues.
The shape of the dental pulp is somewhat similar to the shape of the tooth.
The pulp horns are located as small “pointed” parts of the pulp that are located beneath cusps
Pulp is composed of:
o Cells
Odontoblasts- found close to predentin
Cell free zone- layer of Weil, beneath the odontoblasts cant be seen in developing tooth
Cell rich zone- rich in capillary and nerve network

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 94
Fibroblasts- are the most numerous cells of the pulp. Provides elasticity to the blood vessels.
o Blood vessels o Lymph vessels o Nerves o Thin collagenous fibers o …in a gelatinous ground substance
The pulp has a very rich blood supply; vessels enter and leave through the apical foramen.
Nerve supply
Both myelinated and unmyelinated nerve fibres are found in the dental pulp
Myelinated- are terminal branches of the trigeminal nerve. They can only register pain; they enter the root canals and branch out forming the plexus of Raschkow. They become unmyelinated as they reach the odontoblasts layer.
Unmyelinated - they are located in the walls of blood vessels and innervate the smooth muscle cells to regulate vasoconstriction.

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 95
33. Description of soft tissues of the periodontium
As mentioned previously, the periodontium consists of:
1. Alveolar bone 2. Cementum 3. Gingiva 4. PDL
These tissues surround and support the tooth; all components except from the gingival arise in the dental follicle.
The soft tissues of these is the Gingiva and the PDL
Gingiva
Surrounds the teeth and is bound to the buccal and lingual plates of the alveolar process
It is pale pink in colour and can be coloured by natural pigmentation

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 96
The part of the gingival closest to the cervical region is not directly attached to the tooth and is known as the free gingiva. In other cases it is known as attached gingiva.
Gingival fibers are collagen fibers that are found in the lamina propria and have an important role in maintaining and supporting the tooth. The fibers work as a functional unit, but they are arranged in 5 subgroups:
1. Dentogingiva – between the cementum and the lamina propria (beneath the junctional epithelium and marginal gingiva).
2. Dentoperiosteal – from the cementum into the periosteum (muscle) 3. Trans-septal – from the cementum and connect adjacent teeth in the arch 4. Alveologingival – from the bony alveolar crest to the lamina propria 5. Circular – run around the neck of the tooth and maintain a tight gingival collar

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 97
The interdental gingiva contains all the fiver groups illustrated above and the trans-septal fibers
The gingiva is supplied by branches of the infraorbital, nasopalatine, buccal, mental, lingual and palatine arteries.
Periodontal Ligament
It is a connective tissue that binds the tooth to the alveolar bone. It communicates with the bone marrow of the alveolar process through vascular channels (volkmann’s canals). They have nerve fibers that respond to occlusal pressure. (Note: fibroblasts synthesise fibres that become the PDL)
It’s situated within a ‘ground substance’ mainly composed of glycosaminoglycans, glycoproteins, and glycolipids. Cells making up the PDL are fibroblasts, epithelial cell rests of Malassez, osteoblasts, Osteoclasts, cementoblasts, macrophages and undifferentiated mesenchymal cells. The collagen fibers pass from the cementum and pass through the periodontal space and are embedded into the alveolar bone as Sharpey’s fibers.
The ligament has a sensory, supportive and protective function to withstand the forces of mastication and other forces alike. They also resist light occlusal impacts and have slight mobility as a cushion.
The width of the periodontal space varies from 0.1mm - 0.4mm
The periodontal fibers
Collagen is the most important structural component of the periodontal ligament. There are 5 principle fibers of the periodontium:
1. Alveolar crest group – similar to tran-septal fibers 2. Horizontal group - run horizontally below the alveolar crest 3. Oblique group- most numerous fibers and are found just beneath the coronal level 4. Apical group – surrounding the root apex 5. Inter-radicular group – at the division of roots

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 98
The periodontal fibers
The PDL are supplied by branches of the superior and inferior alveolar arteries, the apical region is supplied by branches of pulpal arteries of individual teeth.
34. Description of hard tissues of the periodontium
The hard tissues of the periodontium are cementum and alveolar bone
Cementum
Covers the root surface
Its colour is yellow
Softest between the dental mineralised tissues
Softer than enamel and dentine because it is less mineralised
Its chemical composition is similar to that of bone o 65% inorganic o 23% organic o 12% water
The main role of cementum is to serve as a medium in which the PDL can attach and stabilise the teeth
o 2 main types of cementum Acellular – lack of cellular components and covers the root surface Cellular – in the apical third of the tooth (last third)

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 99
Cells of the cementum:
1. Cementocytes- are cementum cells, they are cementoblasts and are embedded in cementum during cementogenesis
2.
3. Cementoblasts – located on the surface of cementum and produce the matrix and fibers of cementum
4. Cementoclasts – break down cementum
In the cementum we can find intrinsic and extrinsic fibers, sharpey’s fibers (collagen fibers which are embedded into cementum and alveolar bone, they are extensions of the PDL).
Alveolar bone

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 100
The alveolar process is that part of the jaw in which the teeth are found (tooth bearing). It is therefore composed of alveolar bone and supporting bone. The remaining jaw-bone is supporting the alveolar process as basal bone.
After eruption the bone is covered by a thick cortical bone and within it is spongy bone (also known as ‘Cancellous bone’).
Lamina dura – is a thin plate of alveolar bone, in the alveolar sockets that allows the passage of blood vessels to the periodontal ligament.
I hope my notes help you in passing and understanding Odontology.
Wishing you the very best in your career.

1st Year 1st Semester Final Exam Odontology Topic Notes AMIT DATTANI 2012
University of Debrecen Medical and Health Science Centre – Faculty of Dentistry 101
Amit Dattani
"Education is our passport to the future, for tomorrow belongs to the people who prepare for it today."
-Malcolm X