dermatology for primary care: recognizing common skin tumors albert g. caruana jr., md resident’s...
TRANSCRIPT
Dermatology for Primary Care:Recognizing Common Skin Tumors
Albert G. Caruana Jr., MDResident’s Conference
April 23, 2004Presbyterian Hospital of Dallas

AcrochordonAcrochordon Have various names: fibroepithelial polyp, skin
tag, squamous papilloma. Oval skin excrescence on a broad or narrow
stalk, can be brown or flesh colored. A pedunculated tumor. Occur more frequently in obese patients. Location: axilla (48%), neck (35%), also inguinal
region. Majority of patients (78%) have less than 3
lesions per area. They begin to appear after 2nd decade of life. They cease growing after the 5th decade of life.

AcrochordonAcrochordon
Composed mainly of loose fibrous tissue (like superficial dermis), covered by thin layer of epidermis.
They are benign. Can be irritating to patients (caught in clothes
and jewelry). Treatment:
Can be snipped off by scissors electrocautery

AcrochordonAcrochordon
Acrochordon: “skin tags.” Round, black-colored, fleshy excrescences on a broad or narrow stalk (left). Clustering of lesions, the groin here, is commonin patients with obesity.

AcrochordonAcrochordon
Acrochordon: “skin tags.” Can present on or around the eyelid (left) or oftenin the axilla (right). Axilla and neck are most common locations.

The most common benign skin neoplasm. No malignant potential.
Origin is unknown. Become more frequent as we age. Diagnosis is easy to make clinically, biopsy
is usually not necessary. Study has shown clinical diagnostic
accuracy of 99% by dermatologists. Tend to occur on trunk most often, but can
appear on head and extremities. Lesions contained entirely in epidermis,
treat with cryosurgery or curettage.
Seborrheic KeratosisSeborrheic Keratosis
Size can range from 0.2 to 3.0 cm in diameter. Can have smooth surface or be rough and cracked. Characteristic “stuck-on” appearance. Color can be tan, brown, or black. The height of the lesion can vary. Can resemble melanoma (SK has uniform surface
appearance). Key to visual diagnosis is identification of horn
cysts Black or pearly-white cysts either embedded
in or on the surface of the lesion. These are dilated follicular ostia filled with
keratin.
Seborrheic KeratosisSeborrheic KeratosisAppearance:
Seborrheic KeratosisSeborrheic Keratosis
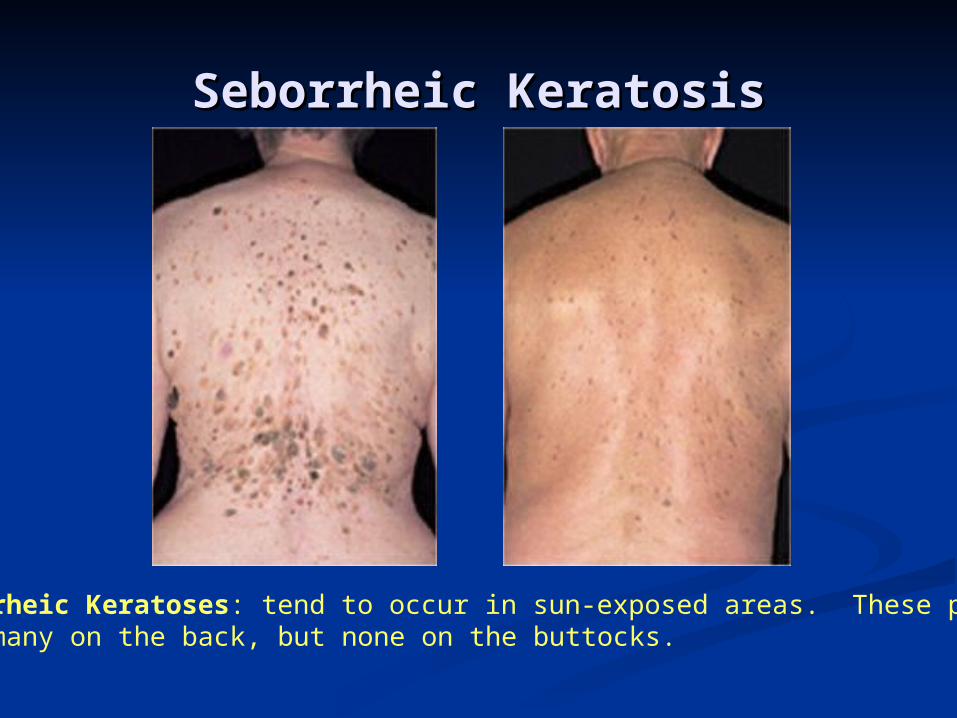
Seborrheic Keratoses: tend to occur in sun-exposed areas. These patientshave many on the back, but none on the buttocks.

Seborrheic KeratosisSeborrheic Keratosis
Seborrheic Keratosis: May be flat with some scale (left) or raised (right) with deep cracks.

Seborrheic KeratosisSeborrheic Keratosis
Seborrheic Keratosis: have characteristic horn cysts. They can be white and deeper seated (left) or black and superficial (right).

Seborrheic KeratosisSeborrheic Keratosis
Seborrheic Keratoses: flat lesions are often brown, can often form near hairline(left). They also commonly can be found under the breasts, where they can Become red and macerated (right).
Seborrheic Keratosis:Seborrheic Keratosis:Melanoma Look-AlikesMelanoma Look-Alikes
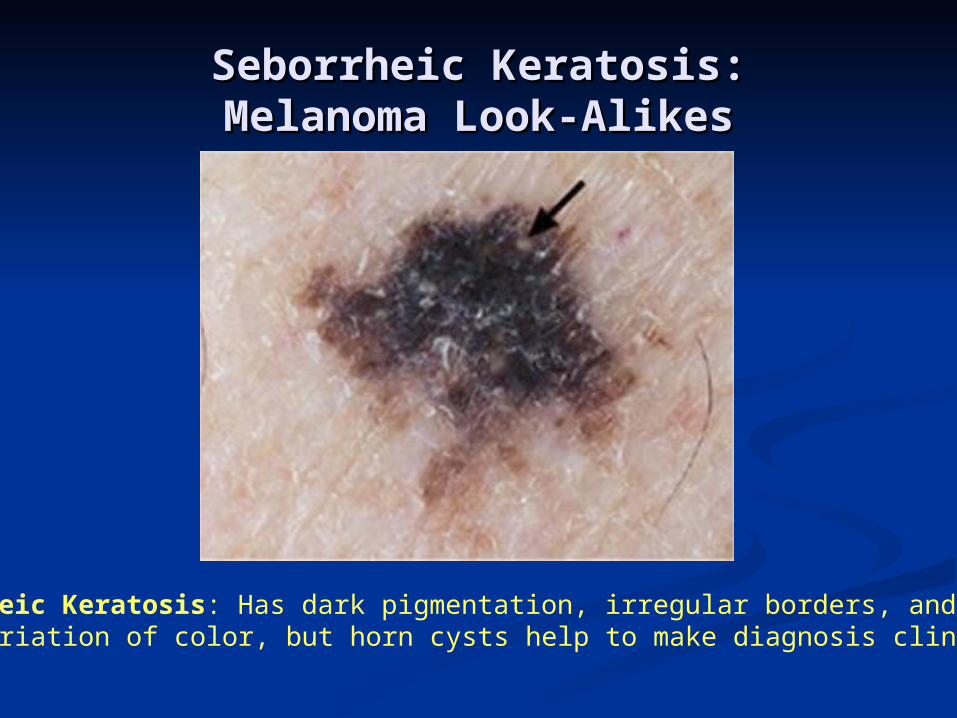
Seborrheic Keratosis: Has dark pigmentation, irregular borders, and some variation of color, but horn cysts help to make diagnosis clinically.

Seborrheic Keratosis:Seborrheic Keratosis:Melanoma Look-AlikesMelanoma Look-Alikes

Have swollen and irregular borders. Develop an erythematous base. Can develop nummular dermatitis around edges. Common in intertriginous areas where skin is
macerated. Itching Develop inflammation around other SK’s that are
not mechanically aggravated. Severely affected lesions can appear like oozing,
red masses with a friable surface. Confused with melanoma or pyogenic granuloma.
Treat with topic steroids or remove all lesions.
Seborrheic KeratosisSeborrheic KeratosisInflammed SK’s:

Seborrheic Keratosis:Seborrheic Keratosis:Inflammed SK’sInflammed SK’s
Seborrheic Keratosis: Often only one lesion is inflammed, but many canbecome inflamed at once (left). This lesion has minimal inflammationat the base (right).

Seborrheic Keratosis:Seborrheic Keratosis:Inflammed SK’sInflammed SK’s
Seborrheic Keratosis: As inflammation worsens, scale may obscuretypical features (left). With severe inflammation, mass may oozeAnd lose all typical features (right).

Dermatosa Papulosa NigraDermatosa Papulosa Nigra
Multiple brown to black dome-shaped papules. Occur on face of young to middle-aged African
Americans. Thought to be a type of seborrheic keratosis.

KeratoacanthomaKeratoacanthoma A common benign epithelial tumor. Thought to be a variant of squamous cell
carcinoma. Unknown etiology. Incidence 104 per 100,000. Mean age of onset is 64 years. Disease of elderly. Seasonal association implies role of UV radiation
in development. Will appear on sun-exposed areas most
commonly, followed by the trunk. Also develops at sight of previous trauma. Most rapidly grow and eventually regress. There are rare variants (2%) which are
destructive.

KeratoacanthomaKeratoacanthoma
Rapid growth phase: starts as a small domed-shape papule that may mimic molluscum contagiosum. Will progress in weeks to grow 1-2cm and often
develop a central keratin-filled crater with crusting.
Untreated, will stop growing in about 6 weeks Stable phase: will remain unchanged for a
variable length of time. Regression phase: will diminish in size,
eventually disappearing, leaving behind a scar. Often regresses in 2 to 12 months.
Appearance & Natural History:

KeratoacanthomaKeratoacanthoma
Can be difficult to distinguish from squamous cell carcinoma (particularly nodular SCC).
This lesion retains a smooth surface, unlike SCC.
This can be treated medically or surgically, as it is a scarring lesion.
Large KA on face may require Mohs’ surgery. Medical therapy options:
5-FU creams (Efudex, Carac). Remove crust prior to application or pretreat with a 40% urea cream (Vanamide). Response in 1-6 wks.
5-FU intralesional injection. Less efficacious on slow growing lesions.
Intralesional methotrexate. Treat monthly. Imiquimod (Aldara) – QOD for 4 - 12 weeks.

KeratoacanthomaKeratoacanthoma
Keratoacanthoma: smooth, dome-shaped papules or nodules, often with a central keratin plug.

Common benign lesion. Most commonly occur on
anterior surface of legs. Fibrous reaction to insect
bite, truama, viral infection.
Can be asymptomatic, painful, or slightly pruritic.
Raised, pink or brown papule.
Can be hard, scaly. “Dimpling test”
Will retract beneath the skin surface when compressed.
DermatofibromaDermatofibroma

Common small tumors of enlarged sebaceous glands.
Start as pale, yellow papules on forehead, cheeks, nose.
Develop telangectasias and central umbilication.
Occur after age 30 in 25% of the population.
May look like BCC. But lesions of SH are soft to palpation.
Can express sebum. Treated with
electrocautery.
Sebaceous HyperplasiaSebaceous Hyperplasia

Actinic KeratosisActinic Keratosis Also called solar keratosis. Squamous cell carcinoma confined to the
epidermis. Commonly thought of as a “pre-cancerous” lesion. Induced by sun-exposure, years of cumulative
exposure are required. Lesions increase with age. Can spontaneously regress if sun-exposure is
removed. Lesions have increased vascularity
(erythematous). Develops adherent white or yellowish scale. Can bleed if picked. Many lesions are more readily identified by rough
texture than appearance.

Actinic KeratosisActinic Keratosis
Actinic Keratosis: classic appearance with scale and crust on anerythematous base (left). Many AKs on the face, the surroundingskin has irregular pigmentation and some dilated vessels (right).
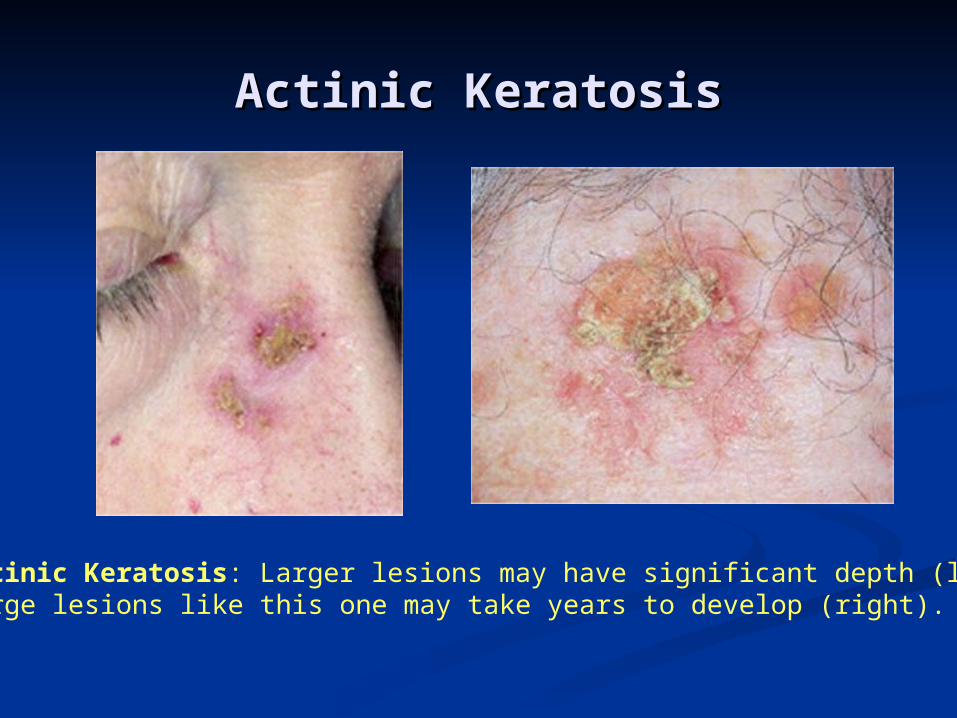
Actinic KeratosisActinic Keratosis
Actinic Keratosis: Larger lesions may have significant depth (left).Large lesions like this one may take years to develop (right).

Actinic KeratosisActinic Keratosis Can progress to SCC: intra-epithelial lesion spreads
to involve the papillary or reticular dermis. Risk of transformation is 0.085% per lesion per
year. 60% of SCC develop from actinic keratosis. AK can be difficult to distinguish from SCC,
particularly thickened hypertrophic AK’s. Worrisome signs: induration, oozing, inflammation. Clinical variants:
Cutaneous horn Spreading pigmented AK (can resemble SK or
melanoma) Actinic chelitis (scaling, red lesion on lower lip
with cracking or ulceration).

Actinic KeratosisActinic Keratosis
Actinic Keratosis: thicker lesions can develop into squamous cellcarcinoma (left). AK’s can often clinically appear like SCC (right).

Actinic Keratosis: Pigmented Actinic Keratosis: Pigmented AK’sAK’s
Pigmented Actinic Keratosis: Can resemble a scaling lentigo, aSK, or a melanoma in some cases.
Actinic KeratosisActinic Keratosis
Regular use of sunscreen is essential. Cryosurgery is preferred since this method separates
epidermis from the dermis. It may leave hypopigmented lesions.
For many lesions, topical 5-FU therapy may be preferred.
Incorporated into rapidly growing cells, causing cell death. Normal cells unaffected.
Duration of therapy depends on location (2-8 weeks). Treatment causes marked inflammation in phases:
Early inflammatory phase (erythema) Late inflammatory phase (burning, edema, stinging, oozing) Lesion disintegration phase (erosion, ulceration, eschar
formation, re-epithelialization)
Treatment:

Actinic Keratosis: TreatmentActinic Keratosis: Treatment
Actinic Keratosis: Treatment with topical 5-FU follows a predictable clinical progression of inflammation of lesions. Right: 3 weeks after starting treatment.

Basal Cell Basal Cell CarcinomaCarcinoma
Most common type of skin cancer. Commonly presents as recurring bleeding or
scabbing wound. Can occur at any age, but most common after age 40. Locally invasive, aggressive, and destructive. Limited capacity to metastasize. Often occurs in areas not sun-exposed (behind ears,
medial canthus). Weaker causal relationship with UV exposure than
SCC. 85% located on head and neck, 25-30% on the nose
alone. Tumor arises from basal keratinocytes and the
surrounding adnexal structures (hair follicles, eccrine sweat ducts).

Basal Cell Basal Cell CarcinomaCarcinoma Progression unpredictable: long periods of
stability followed by rapid progression or regression.
Clinical types: nodular, pigmented, sclerosing, superficial.
Nodular BCC: Most common type of BCC. Pearly-white or pink, dome-shaped papule. They may be flat. Often has telangectasia. Center may ulcerate, bleed, and develop crust
and scale (“rodent ulcer”). Any non-healing ulcer that fails to respond to
treatment should be biopsied to rule out BCC.

Basal Cell Basal Cell CarcinomaCarcinoma
Classic appearance of nodular BCC: pink or pearly dome shaped papuleswith telangectasias.

Basal Cell CarcinomaBasal Cell Carcinoma
Nodular BCC: “Rodent-Ulcer” with central scaling and crusting.

Basal Cell CarcinomaBasal Cell Carcinoma
Nodular BCC: small lesions can be easyTo miss on physical exam.
Nodular BCC: On leg. Consider when A chronic ulcer fails to improve with therapy.

Basal Cell Basal Cell CarcinomaCarcinomaPigmented BCC: Contains melanin. May resemble melanoma or seborrheic
keratosis. Look for pearly-white, transluscent borders.
Sclerosing (Morpheaform) BCC: Innocuous surface appearance which can mask
deep and wide extension. Pale-white to yellow, waxy, firm, flat to slightly-
raised. Can look like localized scleroderma. Borders are indistinct. Requires wide excision.

Basal Cell CarcinomaBasal Cell Carcinoma
Pigmented BCC: Can have variable amounts of melanin. Look for elevated,Pearly-white borders.

Basal Cell CarcinomaBasal Cell Carcinoma
Sclerosing (morpheaform) BCC: flat, firm, waxy, resembling a scar or localized scleroderma

Basal Cell Basal Cell CarcinomaCarcinoma
Superficial BCC: Least aggressive variety. Most often seen on trunk or extremeties. Can occur on the face. Well-circumscribed, oval to round, red and
scaling plaque. Tend to bleed easily. May resemble eczema or psoriasis. Examine borders, which will be raised and
pearly-white. Tension on surrounding skin may make border
characteristics more obvious.

Basal Cell CarcinomaBasal Cell Carcinoma
Superficial BCC: well circumscribed, with raised pearly-white borders, red, scaly, and sometimes resembling eczema.

Basal Cell CarcinomaBasal Cell CarcinomaTreatment Algorithm:

Mohs’ Micrographic SurgeryMohs’ Micrographic Surgery

Squamous Cell CarcinomaSquamous Cell Carcinoma Unlike BCC, these lesions have significant chance
of metastasis. Risk Factors: childhood sun exposure, blistering
sunburns, light skin, outdoor occupations, freckling, hazel/blue eyes.
UV radiation is involved in the pathogenesis of SCC. Found in sun-exposed areas (scalp, back of hands,
pinna). Actinic keratosis is most common precursor lesion. Capacity for metastasis related to lesion size and
location. Thickness of lesion best predictor:
One study found recurrent tumors always at least 4mm thick and all fatal tumors at least 10mm thick.
Surgical margins 2-4mm depending on grade.

Squamous Cell CarcinomaSquamous Cell Carcinoma
A red, keratotic papule with surface scale. Resembles AK.
A nodular lesion that had been previously treated with cryotherapy.

Squamous Cell CarcinomaSquamous Cell Carcinoma
SCC on the lip of a patient who has spent years working outdoors.

Squamous Cell CarcinomaSquamous Cell CarcinomaTreatment Algorithm
Malignant MelanomaMalignant Melanoma Malignancy of melanocytes with high metastatic
potential. Increasingly common: incidence in Caucasians has
tripled in last 40 years. Lifetime risk in 1987 was 1 in 123. By 2010 will be 1 in
50. Incidence in African Americans 1/20 that of Caucasians,
in Hispanics, 1/6. Causes 75% of cancer deaths in the United States. Median age of diagnosis is 53. Significant association with UVA exposure (280-320nm). Risk highest to those that tan poorly and get
intermittent sun exposure. Four major clinical subtypes: superficial spreading,
lentigo maligna melanoma, nodular, acral-lentiginous melanoma.

Malignant Melanoma: Risk FactorsMalignant Melanoma: Risk Factors
Risk Status:Risk Status: Relative Risk:Relative Risk:History of atypical moles, family hx of History of atypical moles, family hx of MM, having more than 75-100 molesMM, having more than 75-100 moles
3535
Previous Nonmelanoma skin cancerPrevious Nonmelanoma skin cancer 1717Congenital Nevus (>20cm)Congenital Nevus (>20cm) 5-155-15History of previous melanomaHistory of previous melanoma 9-109-10Family hx of melanoma in first degree Family hx of melanoma in first degree relativerelative
88
ImmunosuppressionImmunosuppression 6-86-8
(Greatly Increased Risk)

Malignant Melanoma: Risk FactorsMalignant Melanoma: Risk Factors
Risk Status:Risk Status: Relative Risk:Relative Risk:Atypical nevi (2-9)Atypical nevi (2-9) 5-75-7Many nevi (50-100)Many nevi (50-100) 3-53-5Many nevi (26-50)Many nevi (26-50) 1.8-4.41.8-4.4Chronic tanning with UVA Chronic tanning with UVA (including PUVA for (including PUVA for psoriasis)psoriasis)
5.45.4
(Moderately Increased Risk)

Malignant Melanoma: Risk FactorsMalignant Melanoma: Risk Factors
Risk Status:Risk Status: Relative Relative Risk:Risk:
Repeated Blistering Sunburns:Repeated Blistering Sunburns:
Three EventsThree Events 3.83.8Two EventsTwo Events 1.71.7
FrecklingFreckling 3.03.0Fair skin, inability to tanFair skin, inability to tan 2.62.6Red or blonde hairRed or blonde hair 2.22.2Single atypical nevusSingle atypical nevus 2.32.3
(Mildly Increased Risk)

Malignant Melanoma:Malignant Melanoma:Recognizing Suspicious NeviRecognizing Suspicious Nevi
The evolution of the benign mole (acquired nevi):• Lentigo simplex (freckle)• Pigmented junctional nevus (flat)• Pigmented compound nevus (elevated)• Flesh-colored intradermal nevus (more elevated)• This occurs over decades

Malignant Melanoma:Malignant Melanoma:Recognizing Suspicious NeviRecognizing Suspicious Nevi
The ABCD’s of moles: Asymmetry Borders
Scalloped edges Color
Uneven pigmentation
Various shades brown, black, red
Diameter Greater than 6mm

Malignant Melanoma:Malignant Melanoma:Recognizing Suspicious NeviRecognizing Suspicious Nevi
Sign:Sign: Implication:Implication:Changes in ColorChanges in Color
Sudden darkening Sudden darkening (brown or black)(brown or black)
Increased number of tumor cells, Increased number of tumor cells, with varying density (and thus with varying density (and thus
pigmentation)pigmentation)
Spread of color onto Spread of color onto previously normal skinpreviously normal skin
Tumor cells migrating through Tumor cells migrating through epidermis (horizontal spread)epidermis (horizontal spread)
Red colorRed color Vasodilation and inflammationVasodilation and inflammation
White colorWhite color Areas of regression, inflammation Areas of regression, inflammation (hypopigmentation) or even “halo” (hypopigmentation) or even “halo”
effecteffect
Blue colorBlue color Pigment deep in the dermis, a sign Pigment deep in the dermis, a sign of increasing depth of tumorof increasing depth of tumor

Malignant Melanoma:Malignant Melanoma:Recognizing Suspicious NeviRecognizing Suspicious Nevi
Sign:Sign: Implication:Implication:Changes in Changes in BordersBorders
Irregular Irregular outline outline
(scalloping)(scalloping)
Malignant cells Malignant cells migrating horizontally migrating horizontally
at different ratesat different rates
Satellite Satellite pigmentationpigmentation
Malignant cells Malignant cells migrating past migrating past borders of the borders of the primary tumorprimary tumor
Development Development of haloof halo
Destruction of the Destruction of the melanocytes by melanocytes by
immunologic reaction immunologic reaction and inflammationand inflammation
A halo nevus.

Malignant MelanomaMalignant MelanomaSuperficial Spreading Melanoma (SSM)
Comprises 70% of melanomas. More immature histologically than lentigo
maligna. Rapid phases of radial growth and regression. Most common in 4th to 5th decade of life. Can occur anywhere on body. Most common on back of either sex or the legs of
women. Known for random combinations of colors. Color becomes more varied as time progresses. Radial growth phase can last months to years. Nodules can appear as lesion get larger than 2.5cm

Malignant MelanomaMalignant MelanomaSuperficial Spreading Melanoma (SSM)
SSM: note irregular borders and varied color patterns. There are also white areas of tumor regression.

Malignant MelanomaMalignant MelanomaSuperficial Spreading Melanoma (SSM)
SSM: Angular notching occurs as tumor regresses. These later lesions show thickened areas that imply vertical growth phase.

Malignant MelanomaMalignant MelanomaNodular Melanoma (NM)
Comprises 15-20% of melanomas. Poorly-differentiated histologically. Does not
respect histologic boundaries of skin. Male to female ratio 2:1. Most often dark brown, red-brown, red-black. Can be amelanotic (1.8-8% of NM). Dome-shaped, polypoid, or pedunculated. Most common on trunk and legs. Most commonly mis-diagnosed subtype
(mistaken for hemangioma, dermatofibroma, dermal nevus).
Often ulcerates and bleeds.

Malignant MelanomaMalignant MelanomaNodular Melanoma (NM)
NM: Thickened nature of lesions reveal its tendency for verticalgrowth. Color may vary.

Malignant MelanomaMalignant MelanomaNodular Melanoma (NM)
NM: Often ulcerate and bleed. Note the amelanotic (flesh-colored)lesion pictured to the right.
Malignant MelanomaMalignant MelanomaLentigo Maligna Melanoma (LMM)
Comprises 4-15% of melanomas. Presents in 6th to 7th decades of life. Radial growth phase called lentigo maligna
(Hutchinson’s Freckle), which may last for years. Some LM never progress. Risk of progression related to age:
For 45yo patient, lifetime risk of progression 4.7%. For 65yo patient, lifetime risk of progression 2.2%.
Tend to have bizarre shape from years of growth and regression.
Nodules do not develop until lesions as large as 5-7cm.

Malignant MelanomaMalignant MelanomaLentigo Maligna Melanoma (LMM)

Malignant MelanomaMalignant MelanomaLentigo Maligna Melanoma (LMM)

Malignant MelanomaMalignant MelanomaAcral Lentiginous Melanoma (ALM)
Comprises 2-8% of melanomas for Caucasians, but 30-75% for Hispanics, African Americans, and Asians.
Most often seen in males over age 60. Appears on palms of hands, soles of feet (most
common), mucous membranes, or terminal phalanges.
Grows slowly over years. Similar presentation to LM and LMM. These tend to be flat and are ignored by patients
early on. Can be deeply invasive. Usually presents late when nodule forms. Poor
prognosis. Hutchinson’s sign: pigmented band at proximal nail
fold.
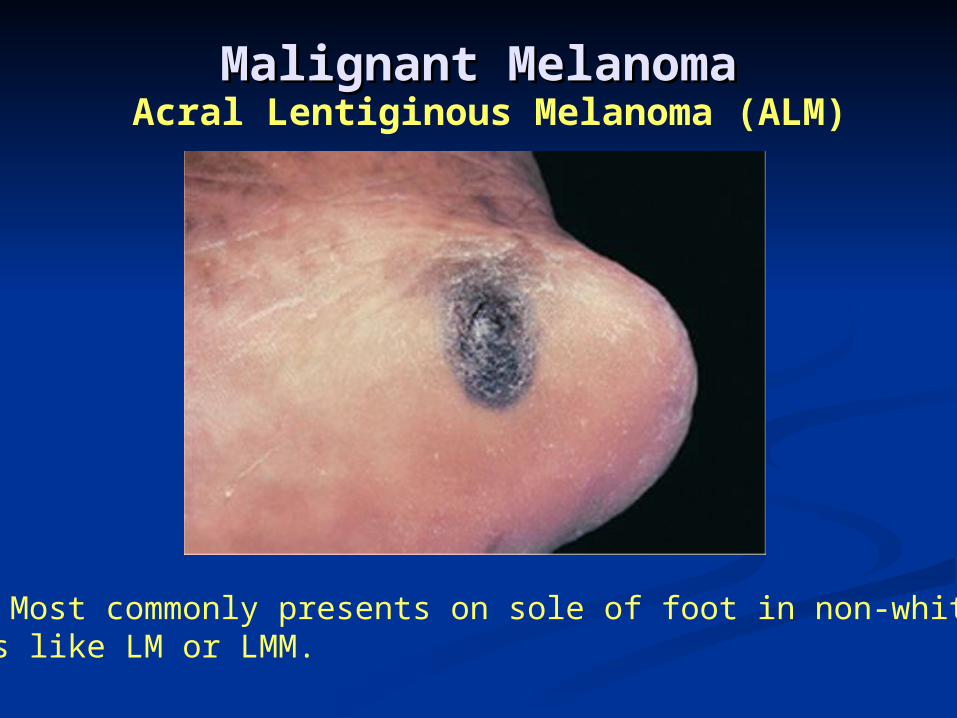
Malignant MelanomaMalignant MelanomaAcral Lentiginous Melanoma (ALM)
ALM: Most commonly presents on sole of foot in non-whites.Looks like LM or LMM.

Malignant MelanomaMalignant MelanomaAcral Lentiginous Melanoma (ALM)
ALM: Pigmented band starting at proximal nail fold is calledHutchinson’s sign. Can have peri-ungual spread (right).

Malignant MelanomaMalignant MelanomaTreatmentTreatment
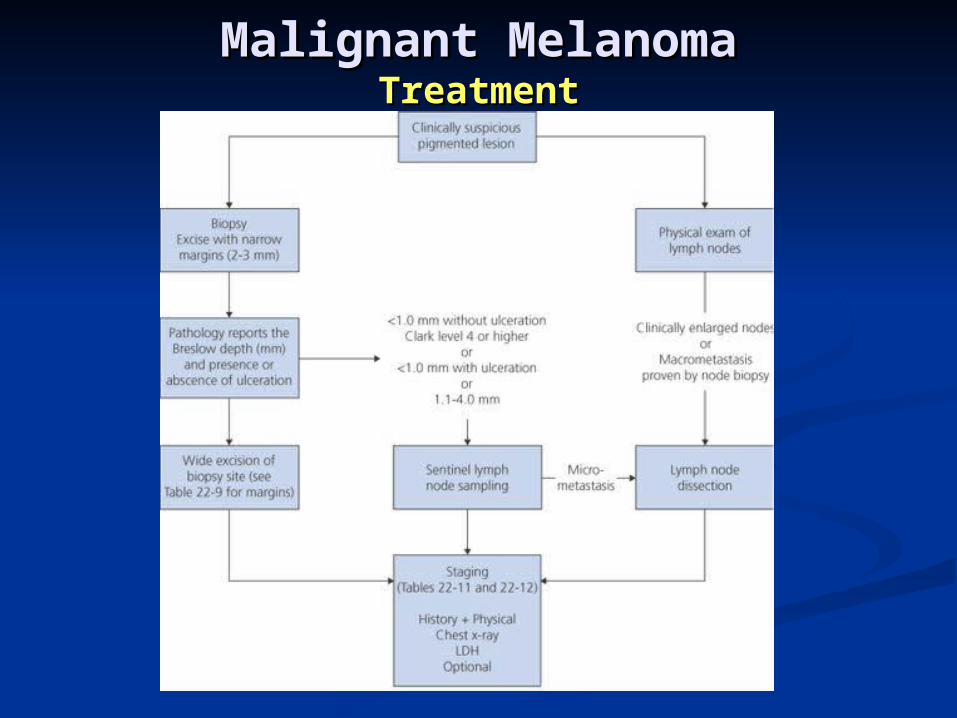
Malignant MelanomaMalignant MelanomaTreatmentTreatment

ReferencesReferences
de Braud F. Khayat D. Kroon BB. Valdagni R. Bruzzi P. de Braud F. Khayat D. Kroon BB. Valdagni R. Bruzzi P. Cascinelli N. Cascinelli N. MalignantMalignant melanomamelanoma. . Critical Reviews Critical Reviews in Oncology-Hematology. 47(1):35-63, 2003 Jul.in Oncology-Hematology. 47(1):35-63, 2003 Jul.
Fitzpatrick T. Johnson R.A. Wolf K. Fitzpatrick T. Johnson R.A. Wolf K. Color Atlas and Color Atlas and Synopsis of Clinical Dermatology: Common and Synopsis of Clinical Dermatology: Common and Serious DiseasesSerious Diseases. Third Edition, 1997 McGraw-Hill.. Third Edition, 1997 McGraw-Hill.
Habif: Habif: Clinical DermatologyClinical Dermatology, 4th ed., 2004 Mosby, , 4th ed., 2004 Mosby, Inc. Inc.
Vargo N. Vargo N. BasalBasal cellcell andand squamoussquamous cellcell carcinomacarcinoma. . Seminars in Oncology Nursing. 19(1):12-21, 2003 Feb.Seminars in Oncology Nursing. 19(1):12-21, 2003 Feb.
Wong CS. Strange RC. Lear JT. Wong CS. Strange RC. Lear JT. BasalBasal cellcell carcinomacarcinoma. . BMJ. 327(7418):794-8, 2003 Oct 4.BMJ. 327(7418):794-8, 2003 Oct 4.