dermatology in the icuv scleroderma-like disorder that affects both the skin and internal organs v...
TRANSCRIPT

Keyan Matinpour, MD Houston Methodist Hospital
Dermatology in the ICU
Disclosures
u I do not have a financial interest/arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict of interest in the context of the subject of this presentation
Presentation Overview
v Brief Overview of Cutaneous Manifestations of Systemic Disease
v Drug Reactions
Cutaneous Manifestations of Systemic Disease
v Frequently encountered in ICU setting v May be the initial sign of an internal disease
Liver Disease
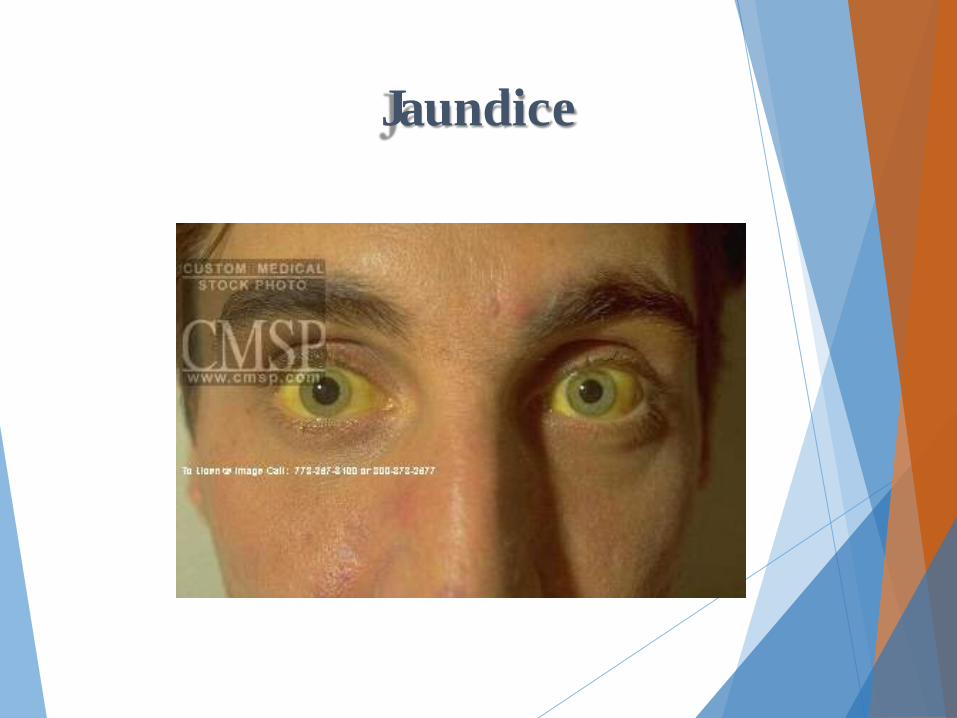
Jaundice
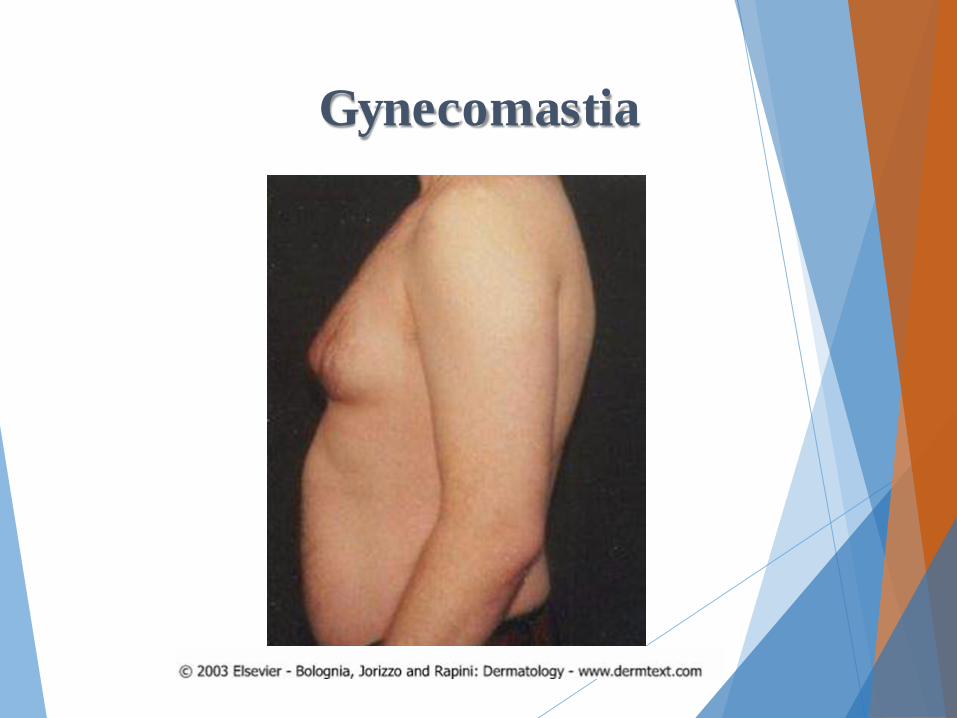
Gynecomastia

Kaput Medusa
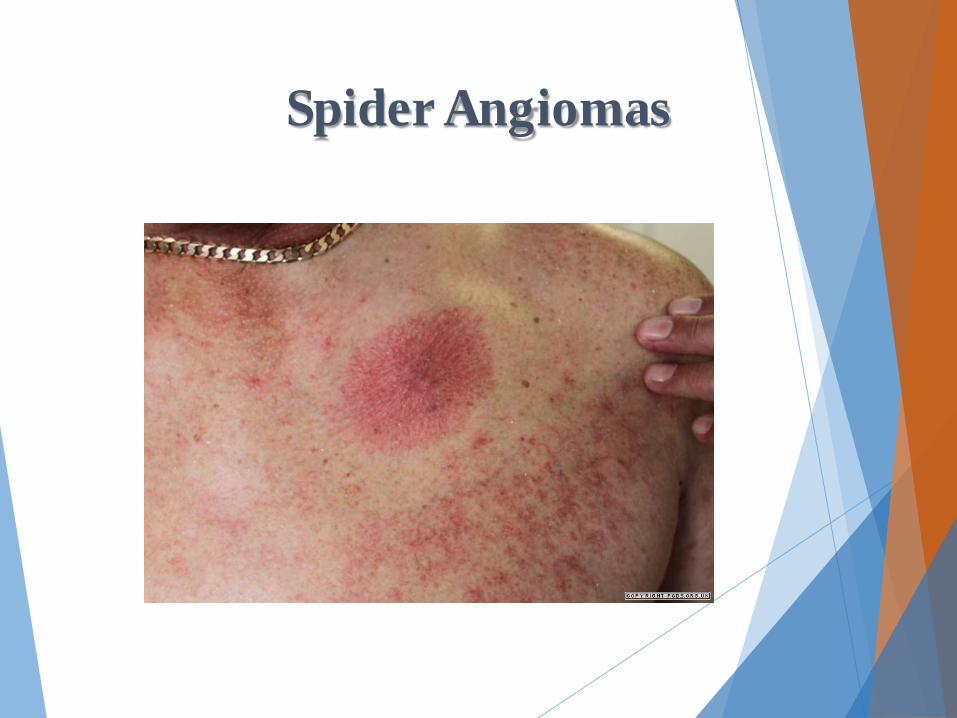
Spider Angiomas
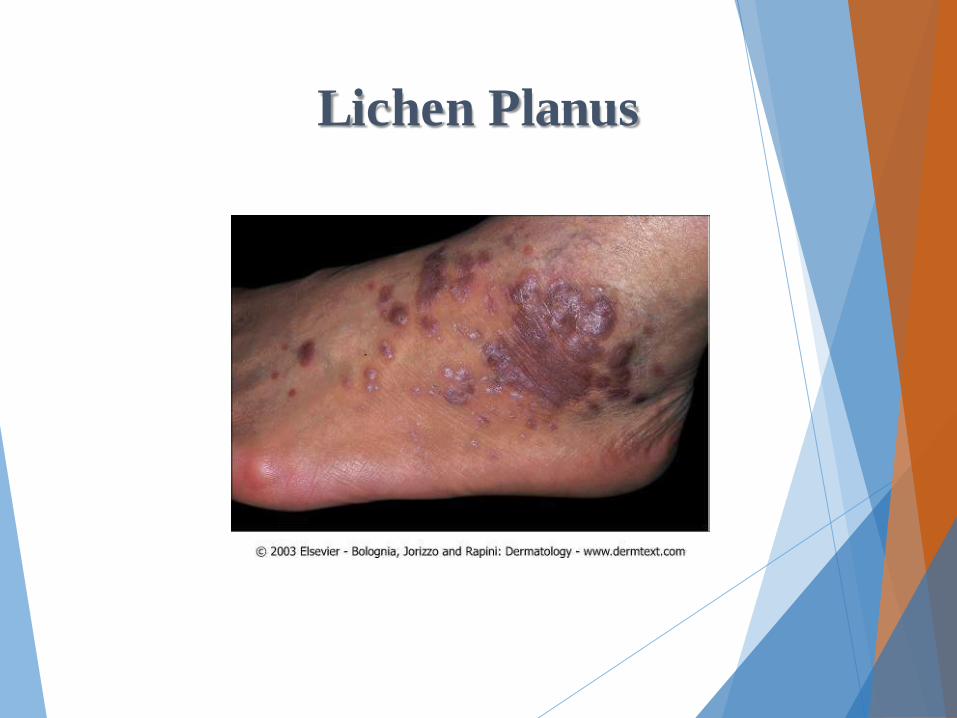
Lichen Planus

Lichen Planus
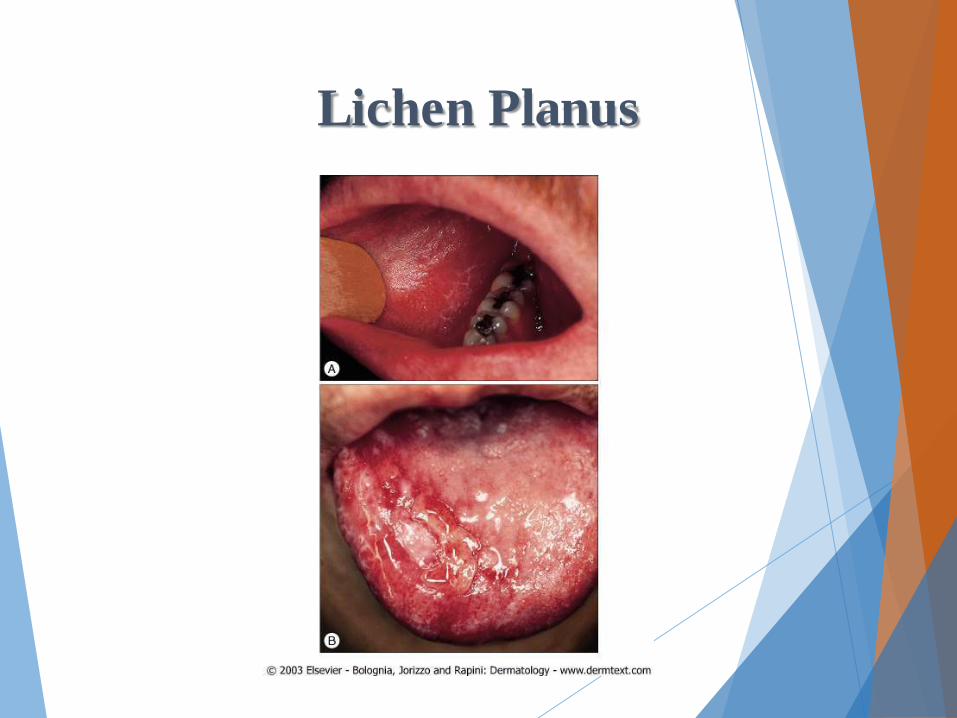
Lichen Planus
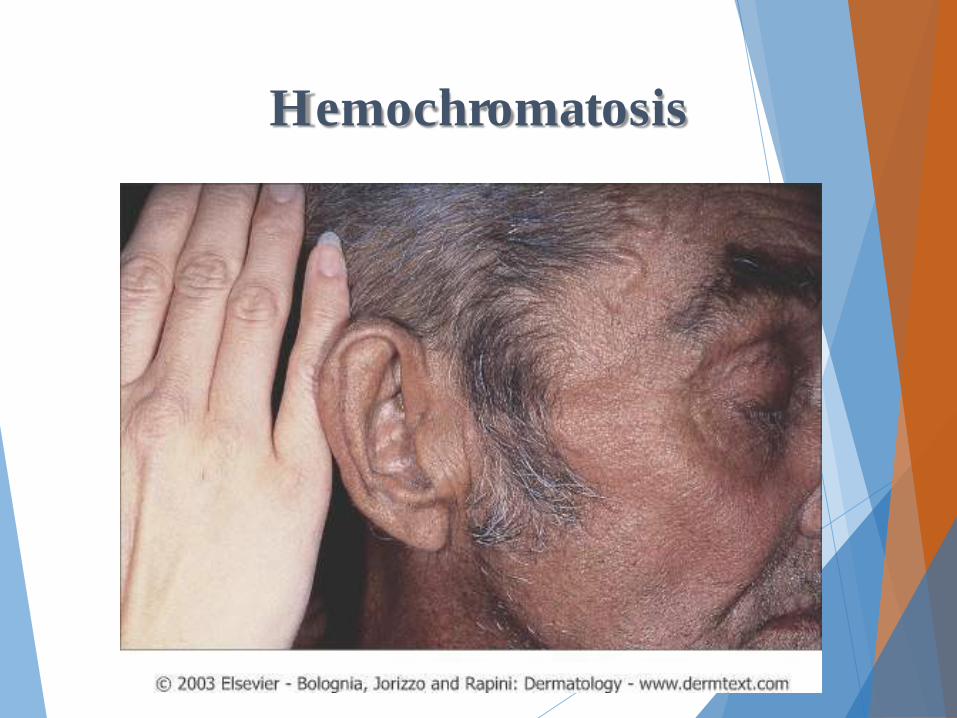
Hemochromatosis

Porphyria Cutanea Tarda
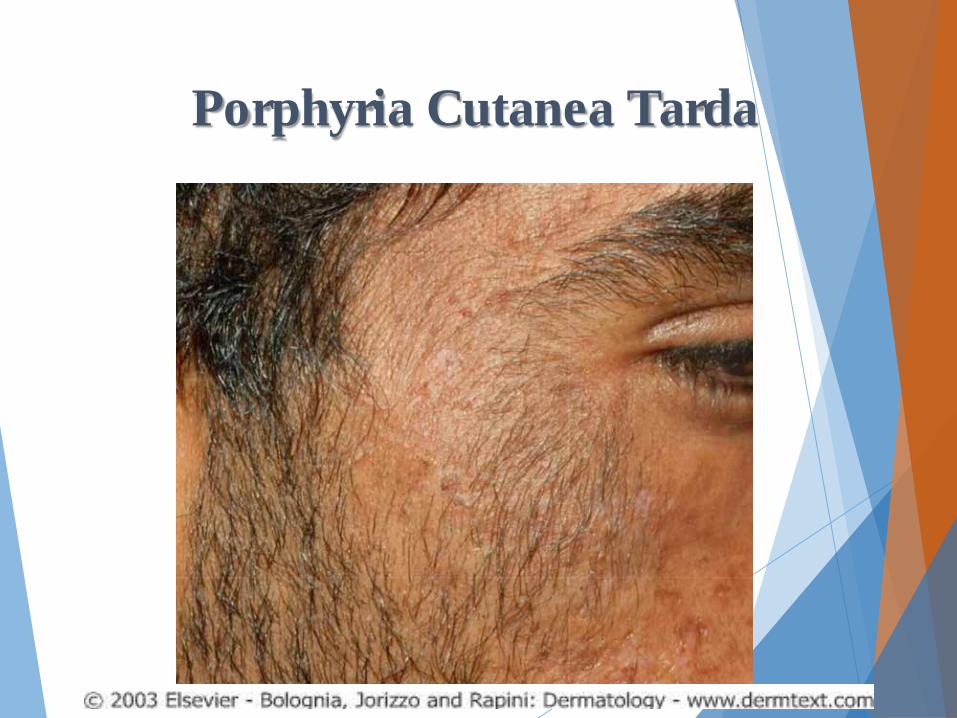
Porphyria Cutanea Tarda

Xanthomas

Xanthomas

Xanthomas

Tendinous Xanthomas
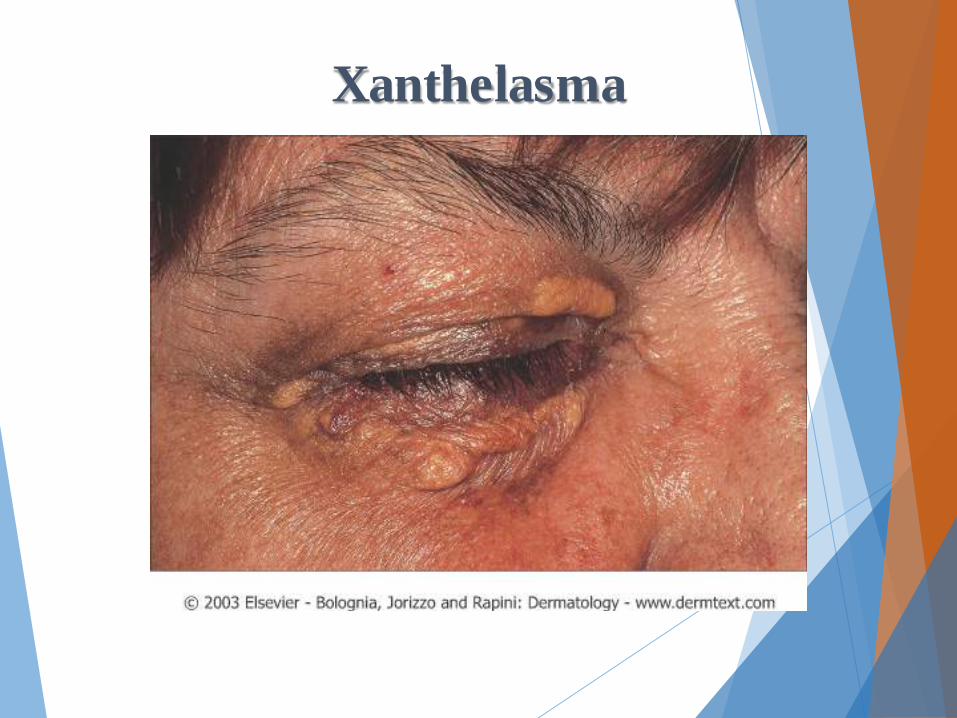
Xanthelasma

Renal Disease

Pruritus
Pruritus
v Optimize Dialysis
v Gentle cleansing of skin (minimal soap)
v Emolients TID
v Topical Steroids BID v Triamcinilone 0.1% Ointment
v Menthol Cream
v Systemic Anti-histamines and steroids ineffective
v Narrowband UVB mainstay of outpt therapy
v Transplant

Acquired Perforating Disorder (Kyrle Disease)

Nephrogenic Systemic Fibrosis

Nephrogenic Systemic Fibrosis

Nephrogenic Systemic Fibrosis
v Scleroderma-like disorder that affects both the skin and internal organs
v Renal insufficiency and exposure to gadolinium-based contrast agents
v Patterned, thick, indurated plaques distributed symmetrically on the extremities
v erythematous to hyper pigmented plaques with an irregular advancing edge with an “amoeboid” appearance
v Confluent involvement on the extremities often results in joint contractures.
v Treatment is unsatisfactory
v Steroids and other immunosuppressive
Calciphylaxis

Calciphylaxis

Calciphylaxis
Calciphylaxis
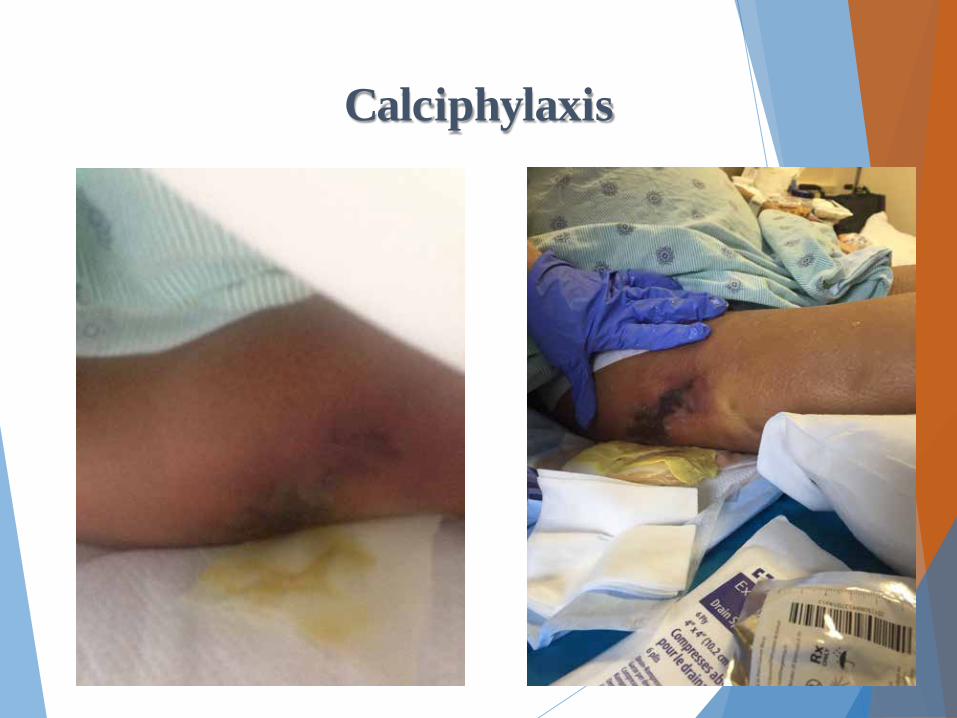
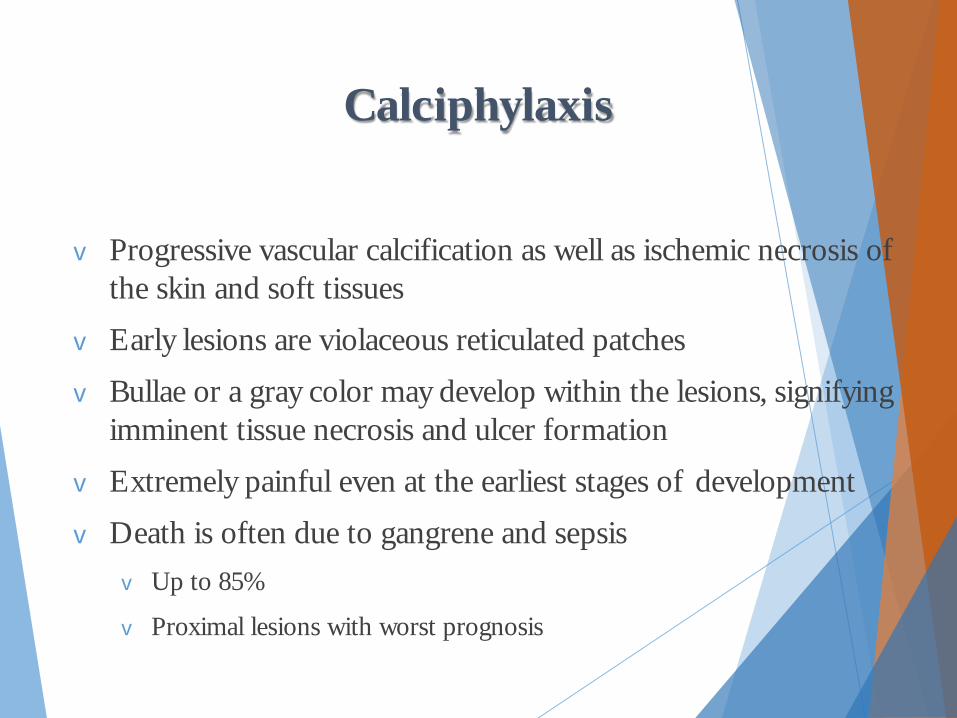
v Progressive vascular calcification as well as ischemic necrosis of the skin and soft tissues
v Early lesions are violaceous reticulated patches
v Bullae or a gray color may develop within the lesions, signifying imminent tissue necrosis and ulcer formation
v Extremely painful even at the earliest stages of development
v Death is often due to gangrene and sepsis v Up to 85%
v Proximal lesions with worst prognosis

Calciphylaxis
v Treatment: vNormalization of the calcium-phosphate product
by low calcium dialysis/PTH levels
v Phosphate binders v calcium acetate and magnesium carbonate
v Aggressive wound care
v Sodium thiosulfate
v Pamidronate

Pulomonary Disease
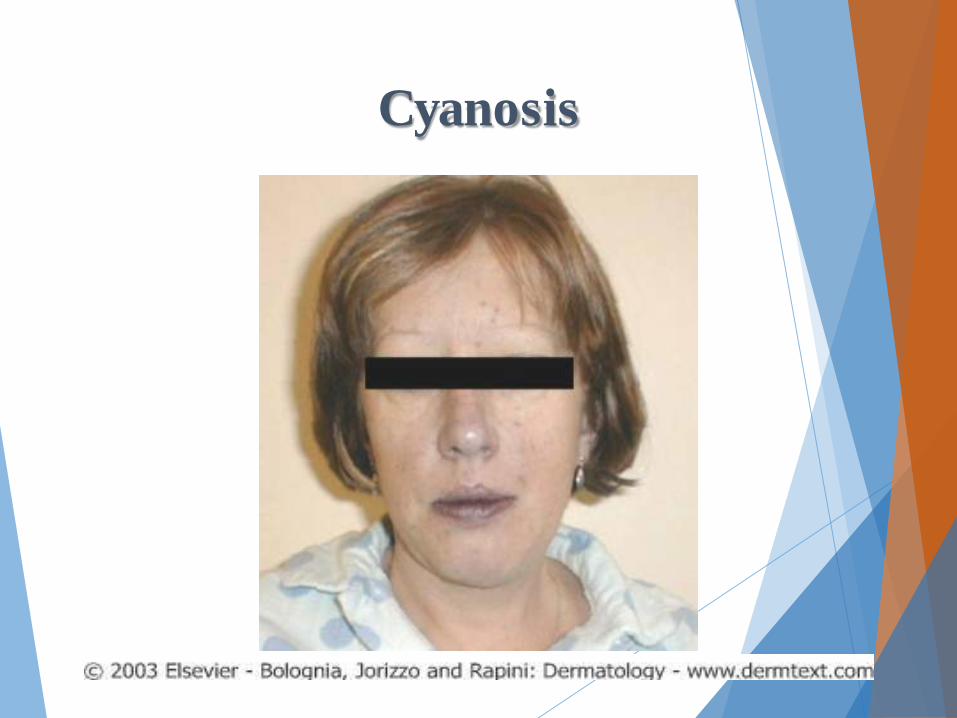
Cyanosis

Acquired Nail Clubbing
Nail Clubbing v Can be congenital or acquired
v Congenital heart disease/ Cystic Fibrosis
v 80% of acquired associated with pulmonary disease v CHF/IBD/HIV/Hyper Thryoid/Carcinoma/Cirrhosis
v Enlargmeent of soft tissue of the distal digit
v Nail plate has greater than 180° widening of the angle between the proximal nail fold and the nail plate

Sarcoidosis

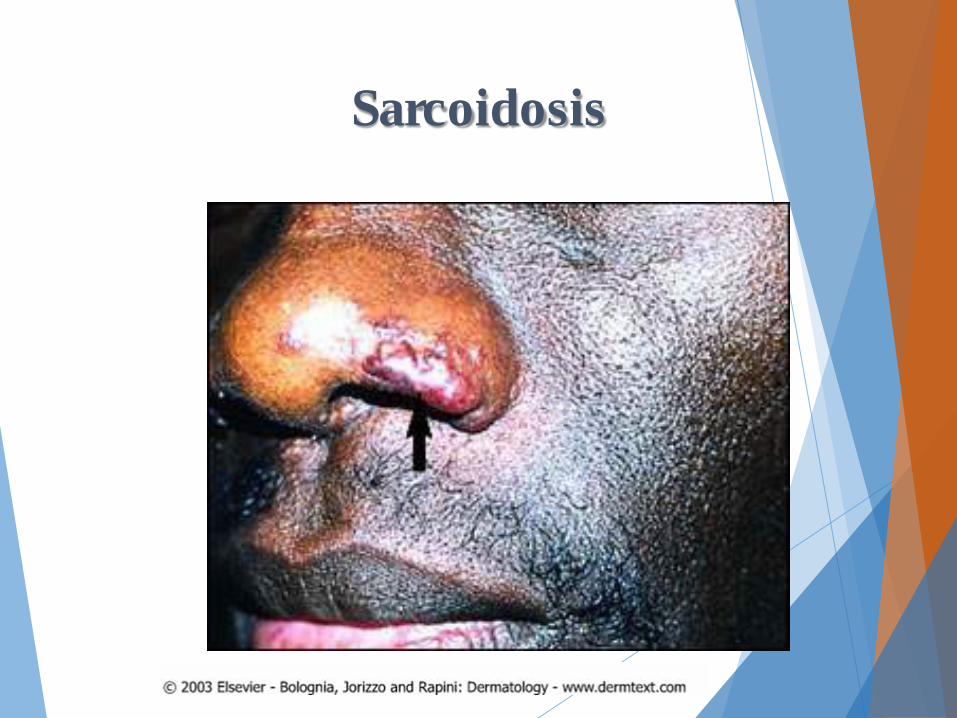
Lupus Pernio
Sarcoidosis

Sarcoidosis

Sarcoidosis
Sarcoidosis

Sarcoidosis
Sarcoidosis
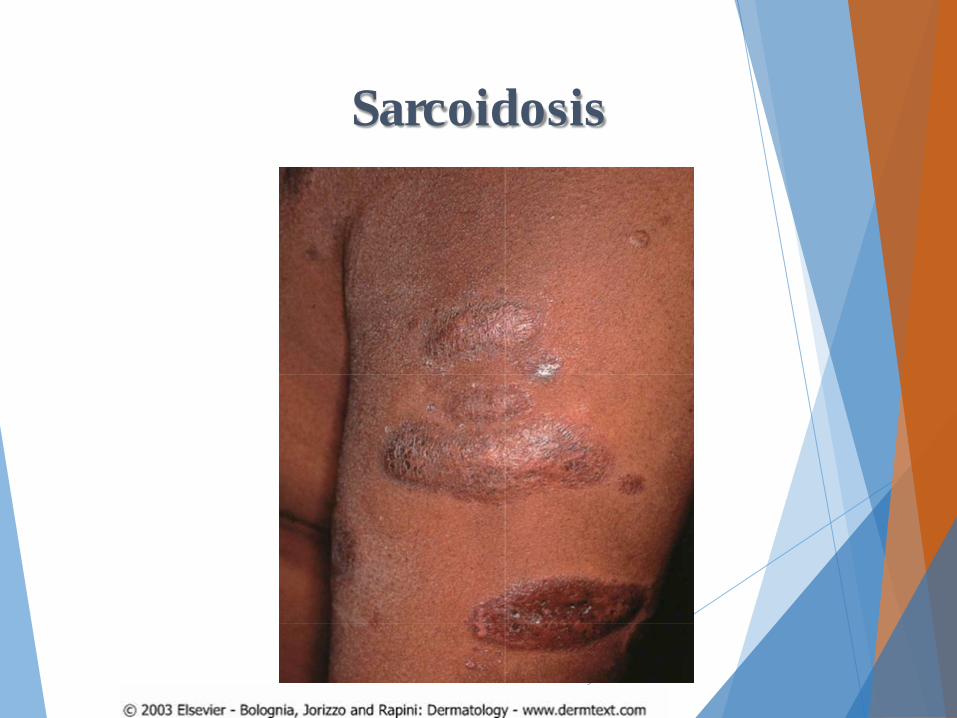
v Systemic granulomatous disease of unknown etiology
v Cutaneous manifestations in up to one-third of patients
vMay be the first clinical sign of the disease
v Red–brown to violaceous papules and plaques appear most often on the face, lips, neck, upper back and extremities
v Classic finding is the development of within pre-existing scars or at sites of prior trauma
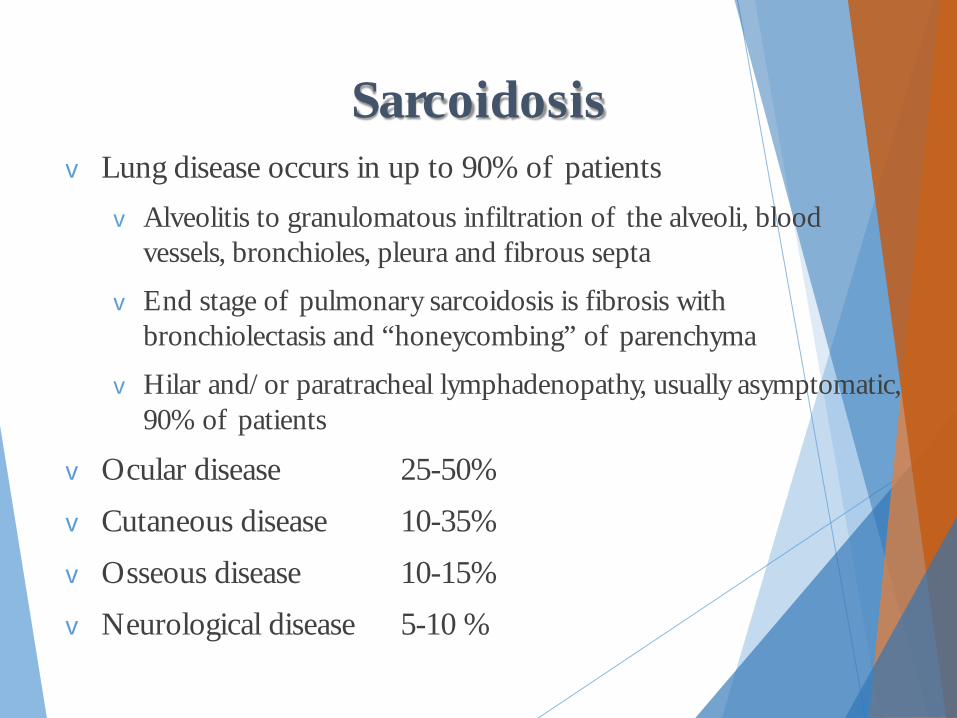
Sarcoidosis v Lung disease occurs in up to 90% of patients
v Alveolitis to granulomatous infiltration of the alveoli, blood vessels, bronchioles, pleura and fibrous septa
v End stage of pulmonary sarcoidosis is fibrosis with bronchiolectasis and “honeycombing” of parenchyma
v Hilar and/or paratracheal lymphadenopathy, usually asymptomatic, 90% of patients
v Ocular disease 25-50%
v Cutaneous disease 10-35%
v Osseous disease 10-15%
v Neurological disease 5-10 %

Lofgren’s Syndrome

Lupus Vulgaris
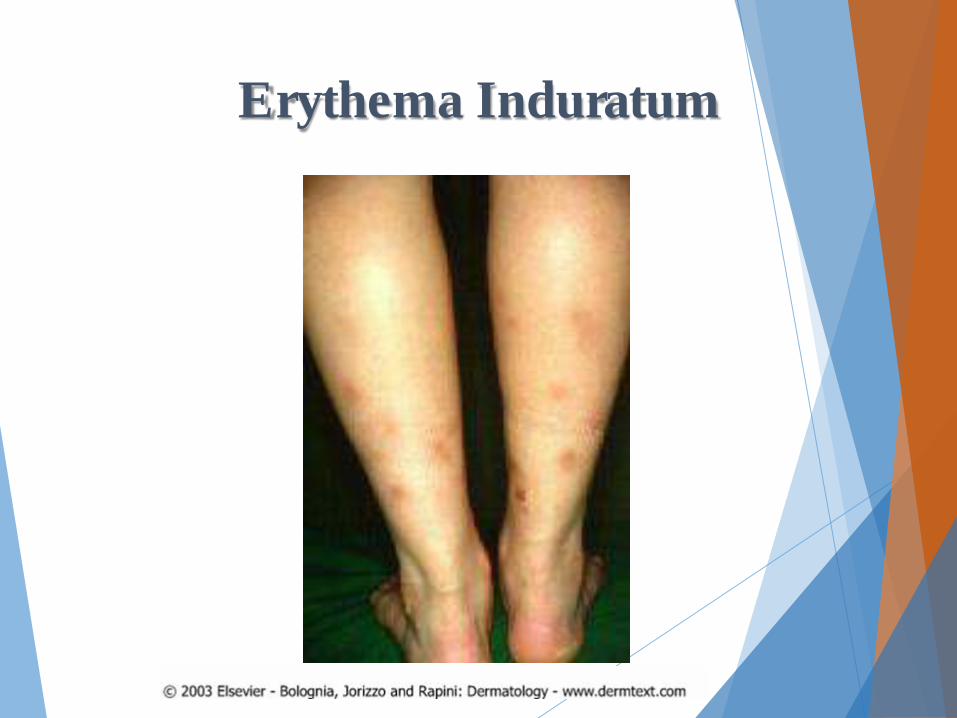
Erythema Induratum
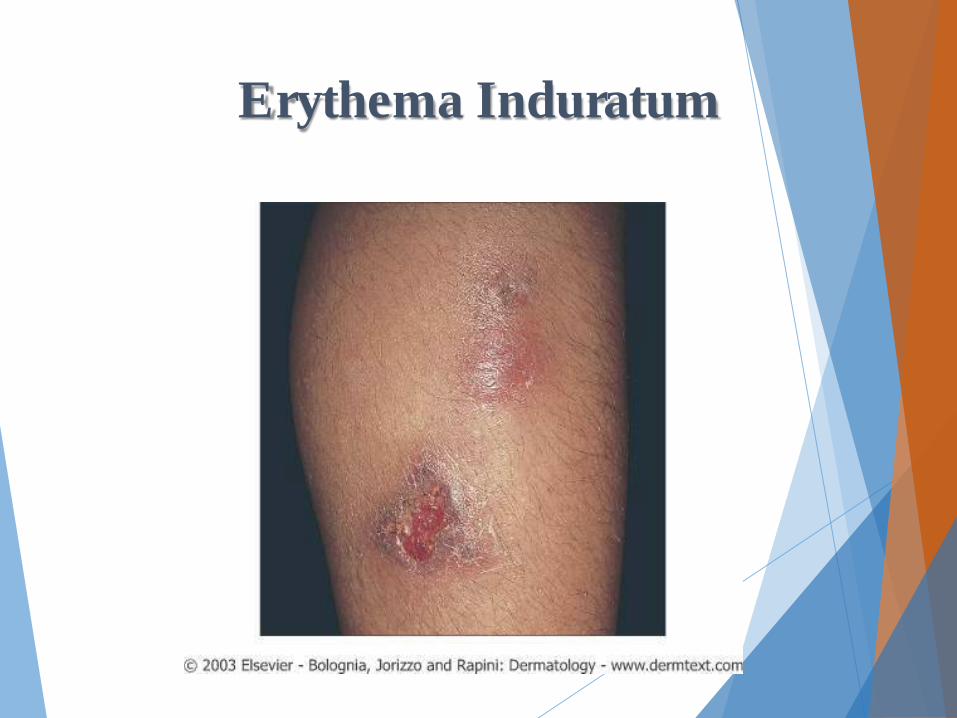
Erythema Induratum
Cardiovascular Disease

Endocarditis
Janeway lesions
Osler’s Nodes
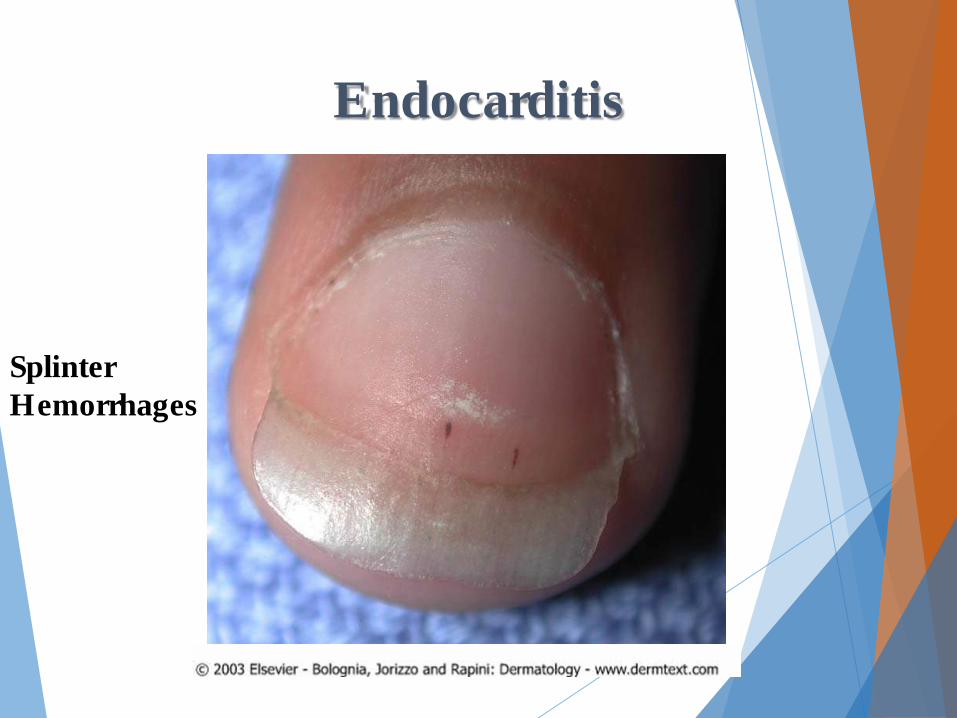
Endocarditis
Splinter Hemorrhages
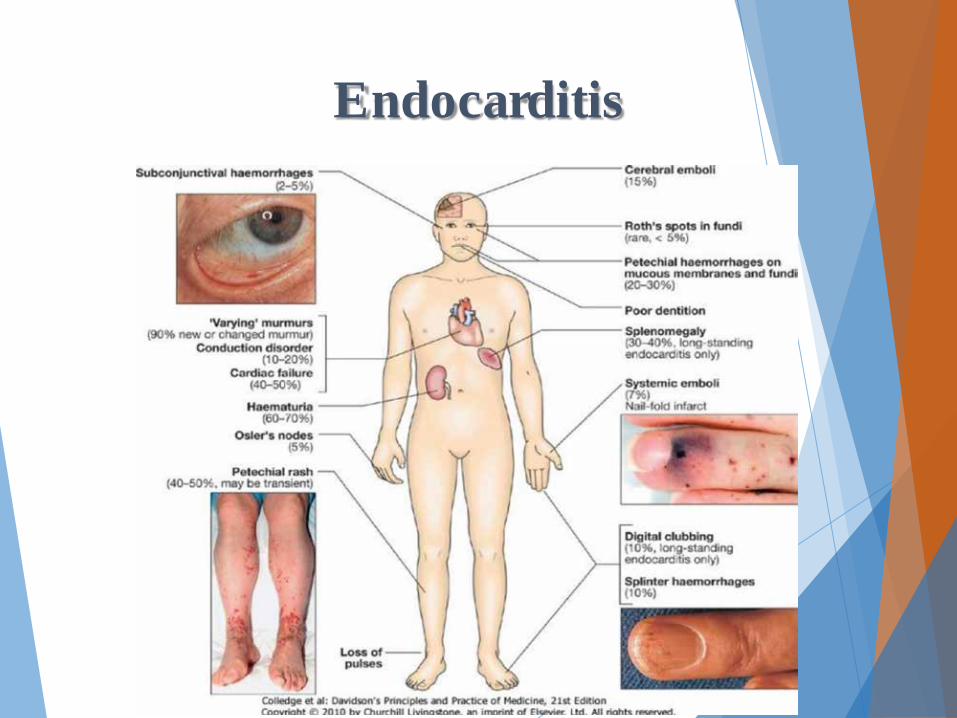
Endocarditis
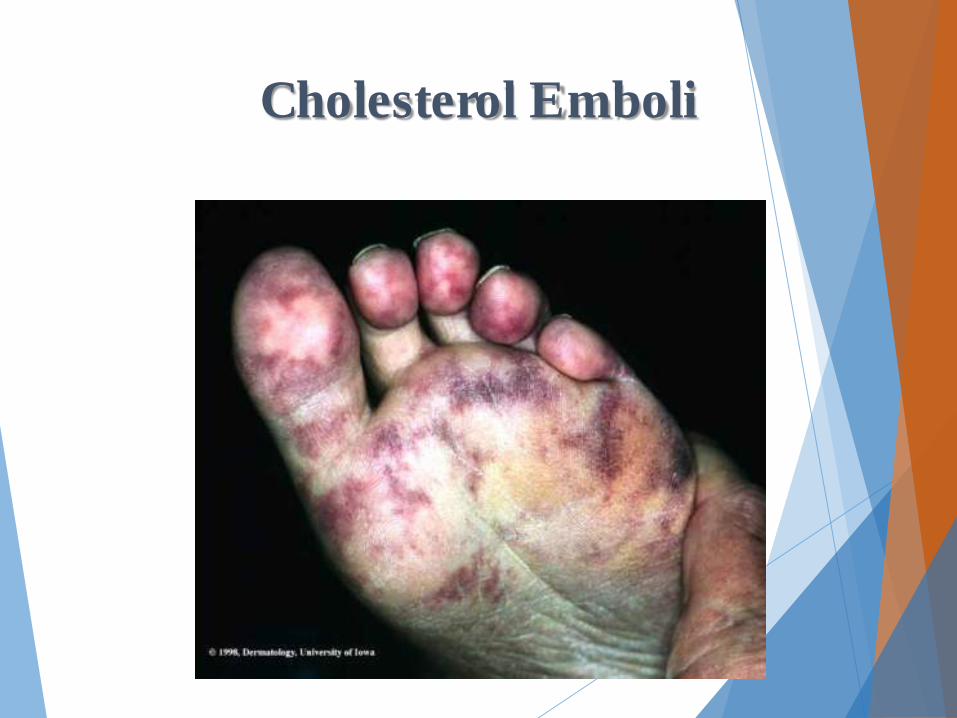
Cholesterol Emboli
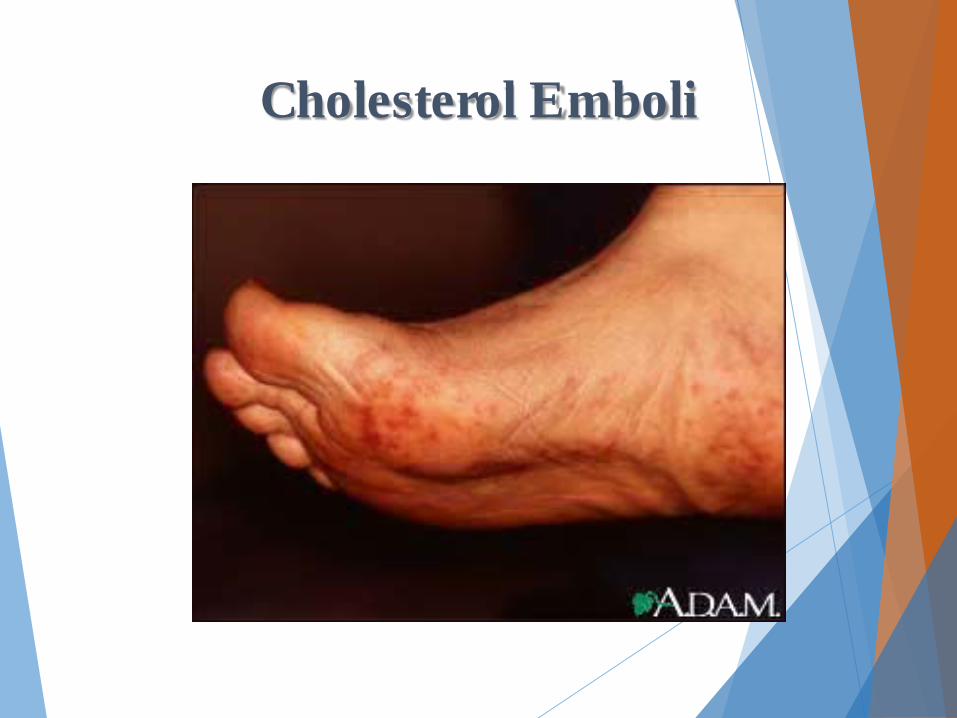
Cholesterol Emboli

Endocrine Disorders
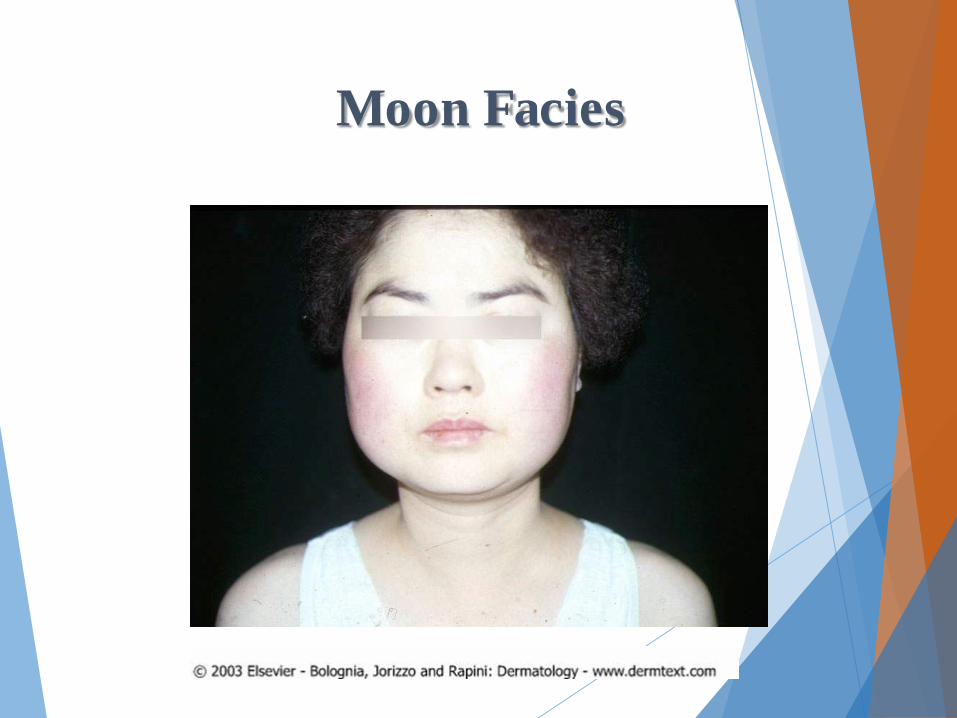
Moon Facies
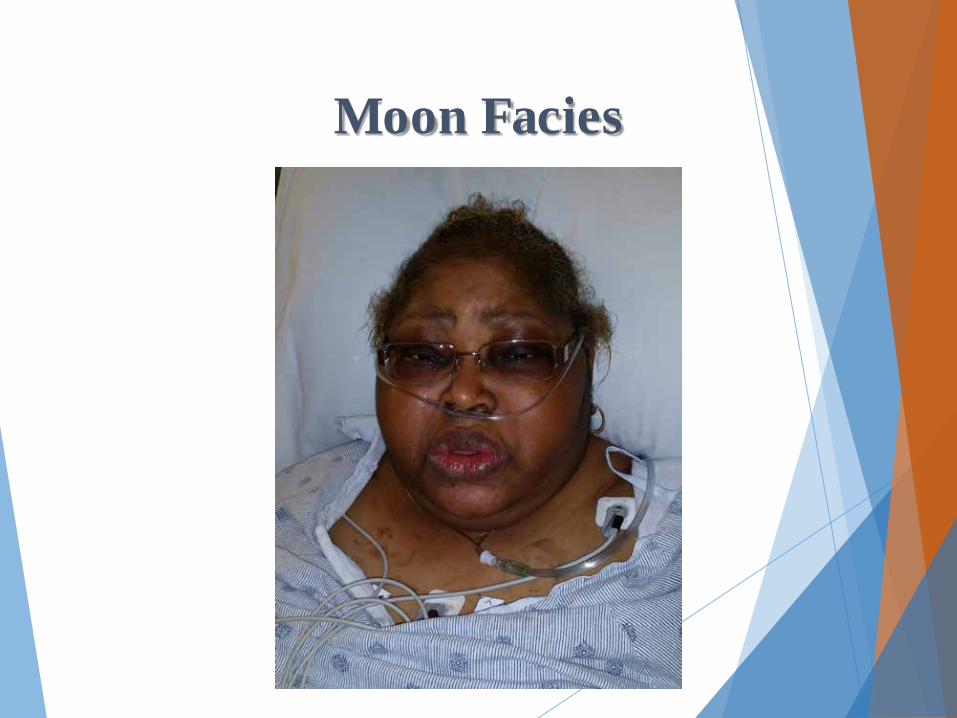
Moon Facies
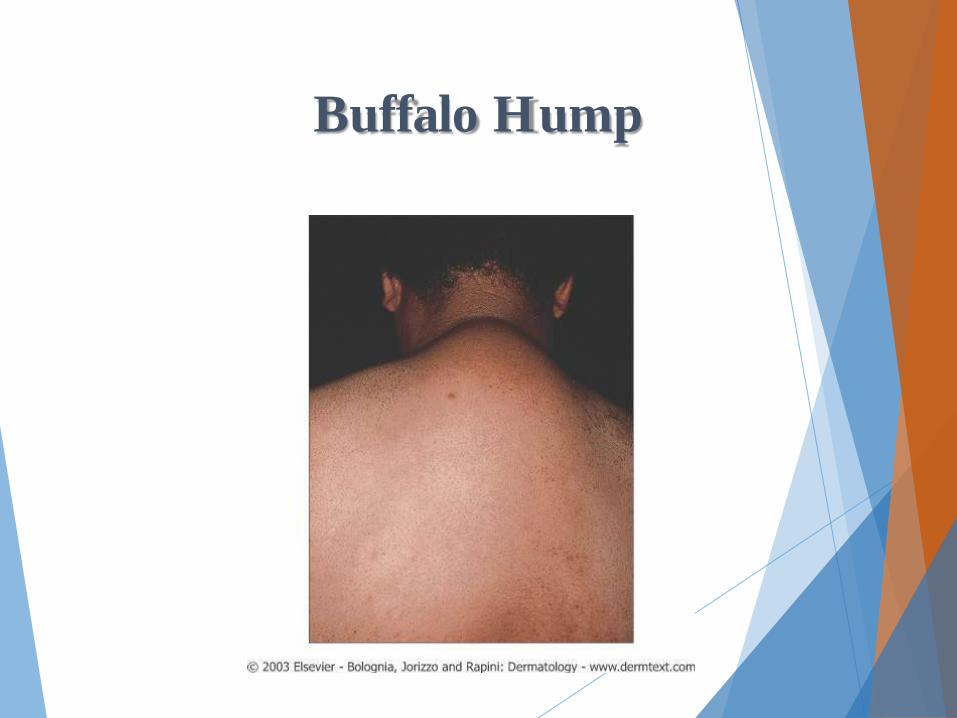
Buffalo Hump
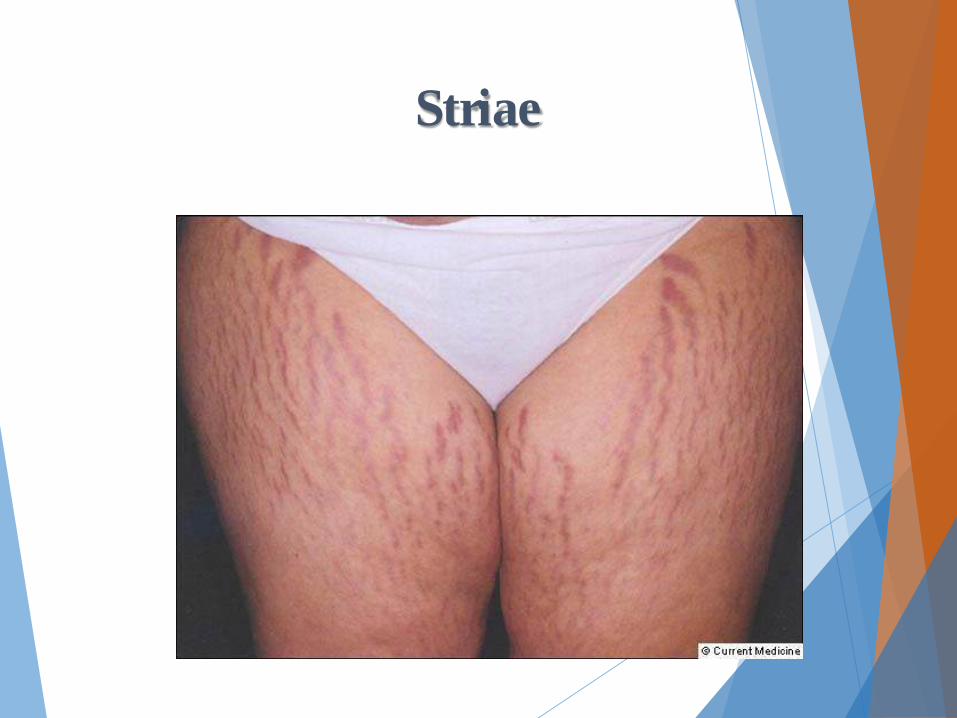
Striae
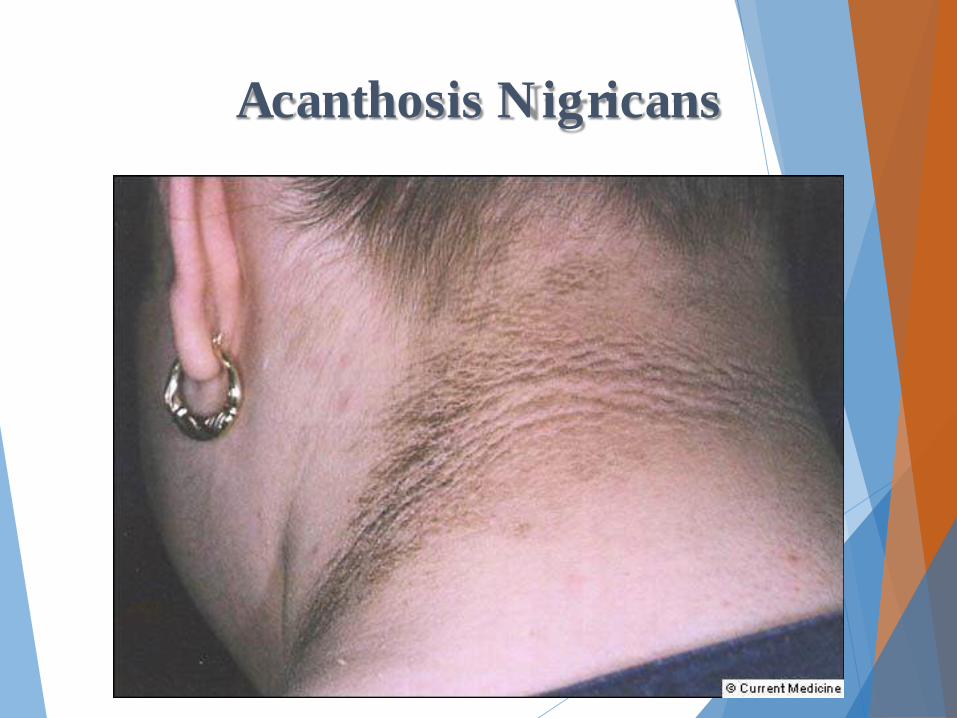
Acanthosis Nigricans
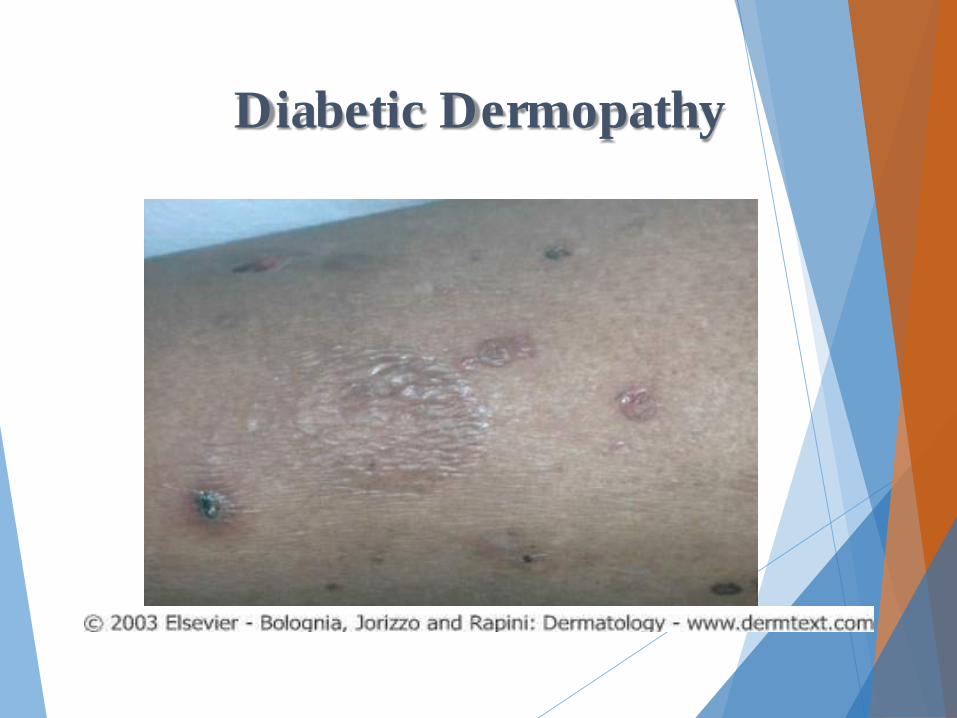
Diabetic Dermopathy
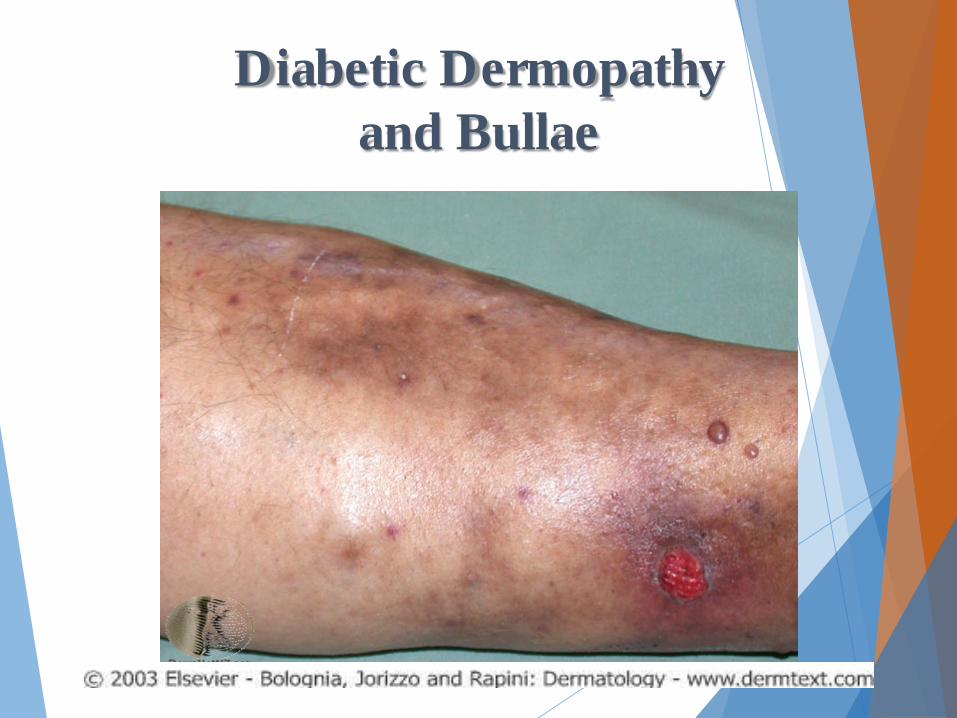
Diabetic Dermopathy and Bullae
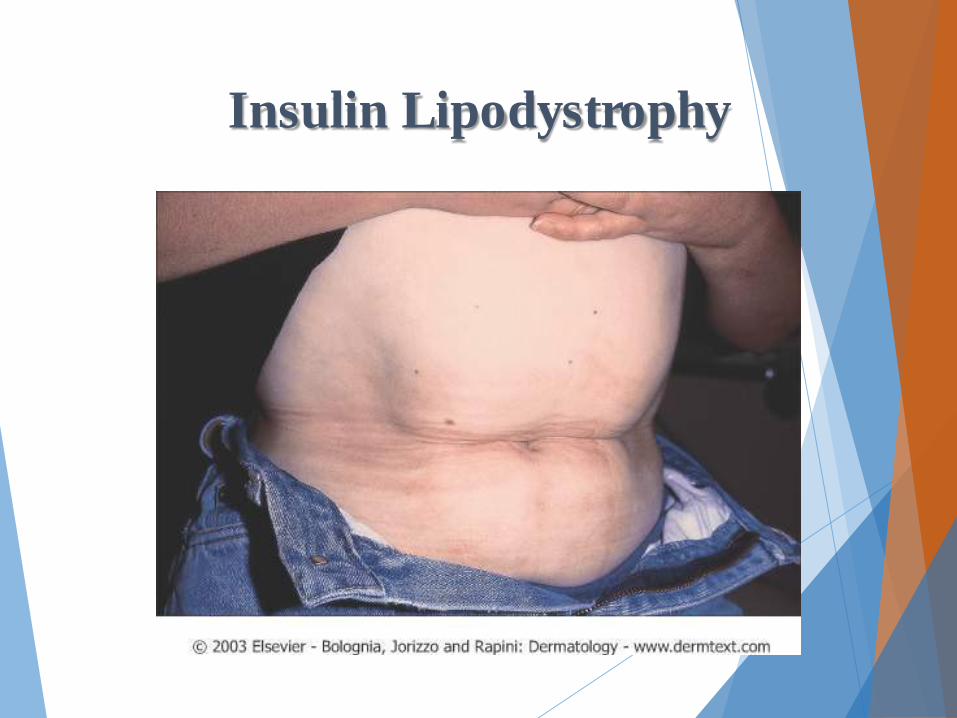
Insulin Lipodystrophy
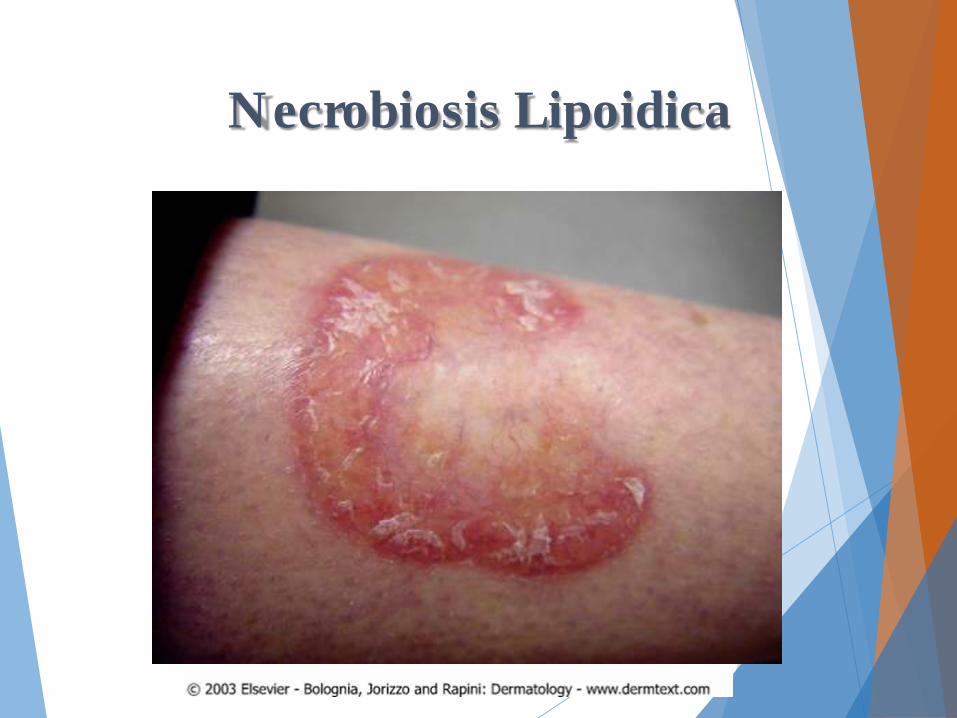
Necrobiosis Lipoidica

Necrobiosis Lipoidica

Granuloma Annulare

Granuloma Annulare

Granuloma Annulare

Granuloma Annulare

Graves
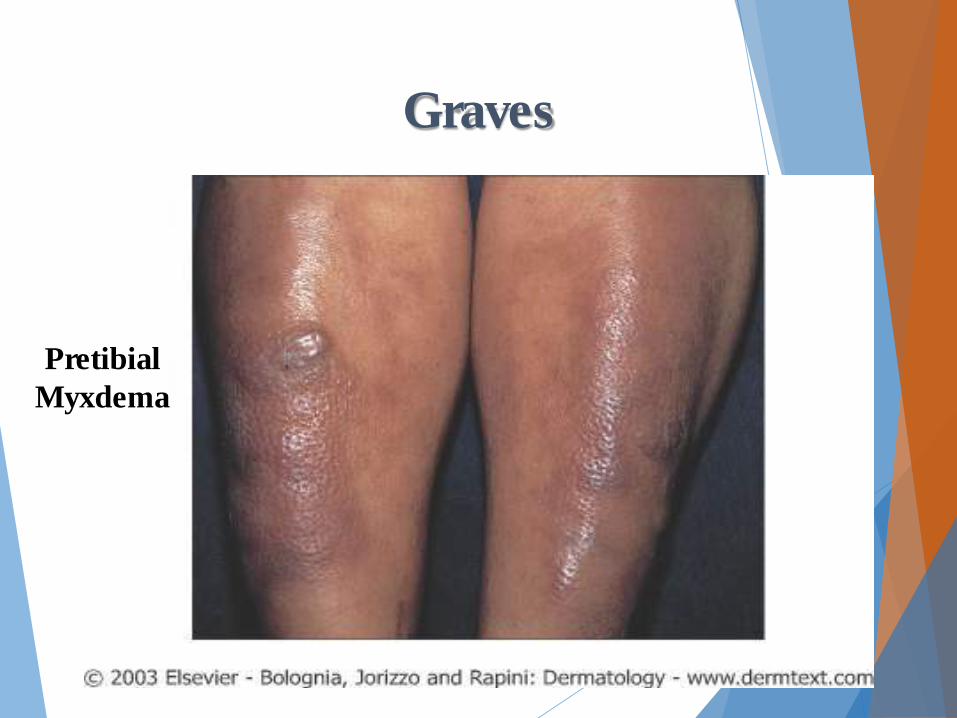
Graves
Pretibial Myxdema
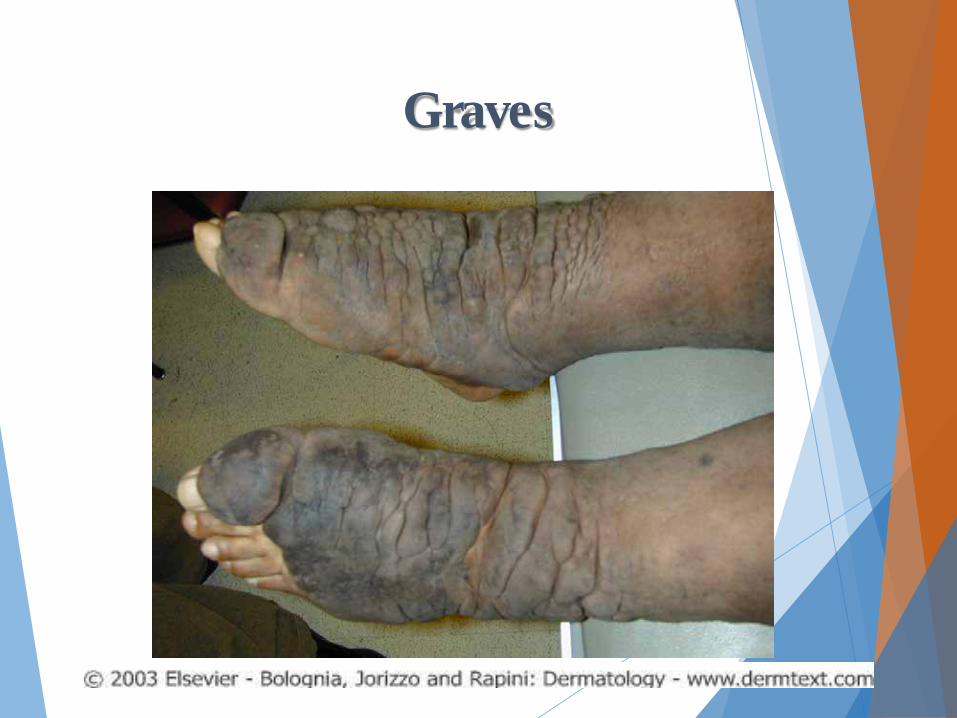
Graves
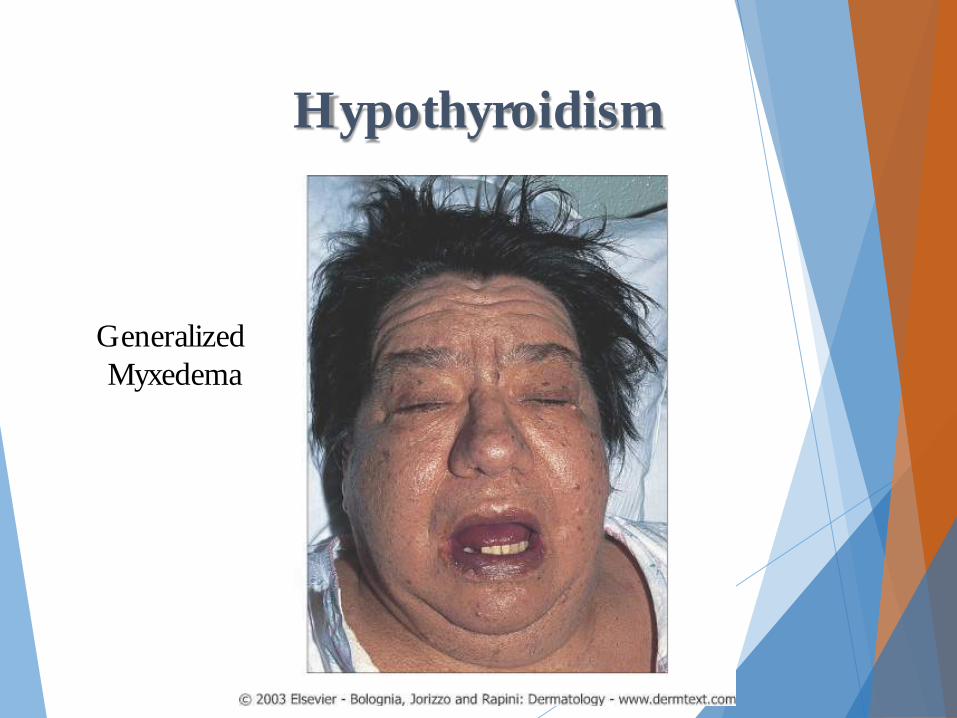
Hypothyroidism
Generalized Myxedema
Connective Tissue Disease
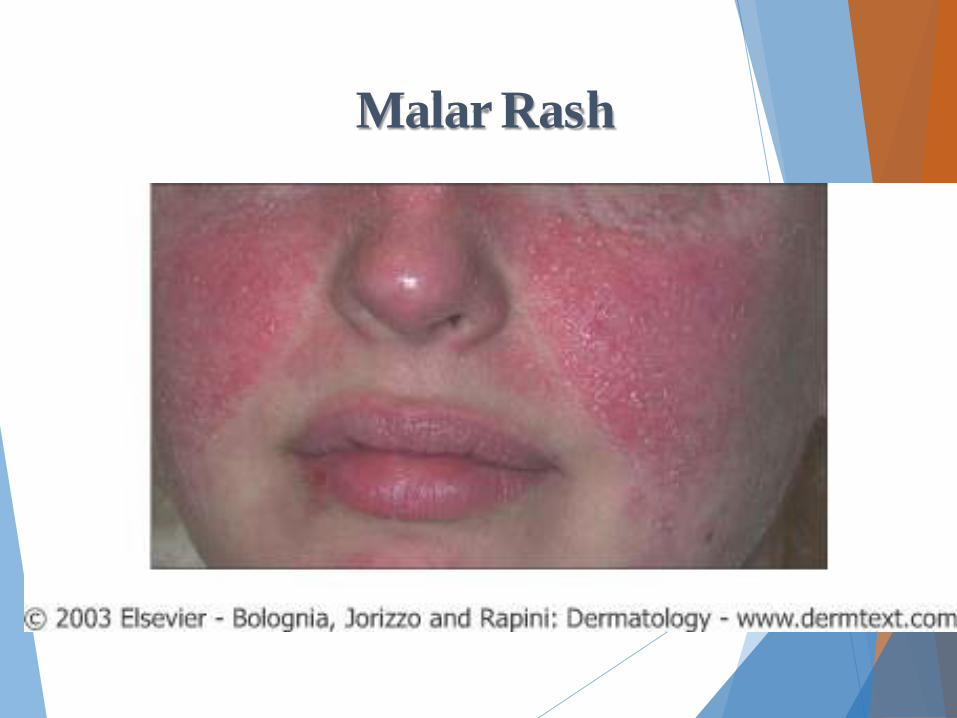
Malar Rash
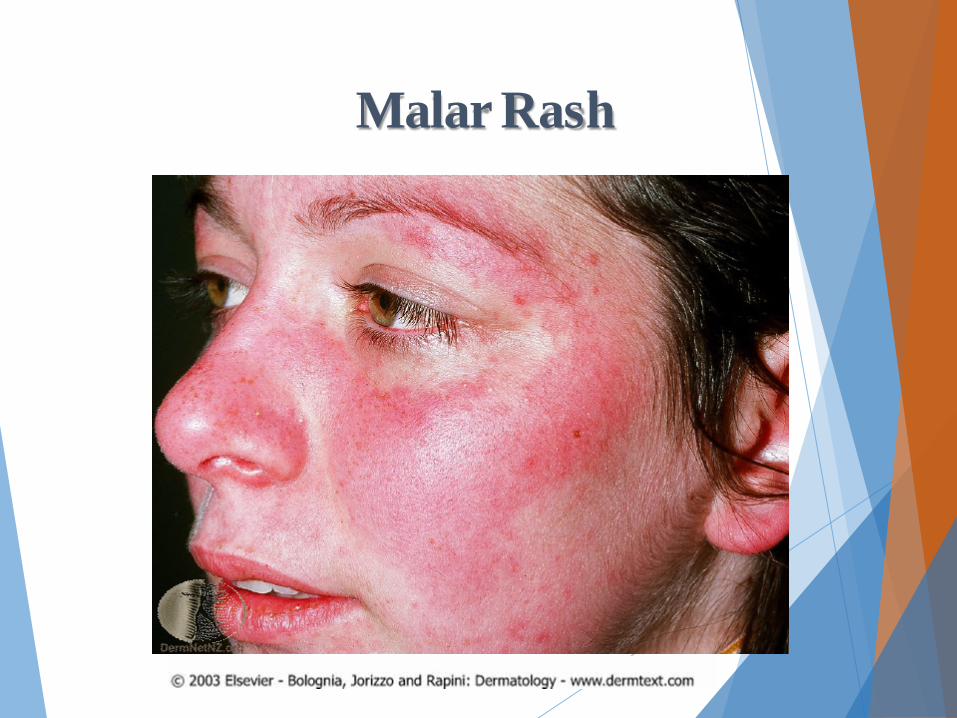
Malar Rash

Discoid Lesions
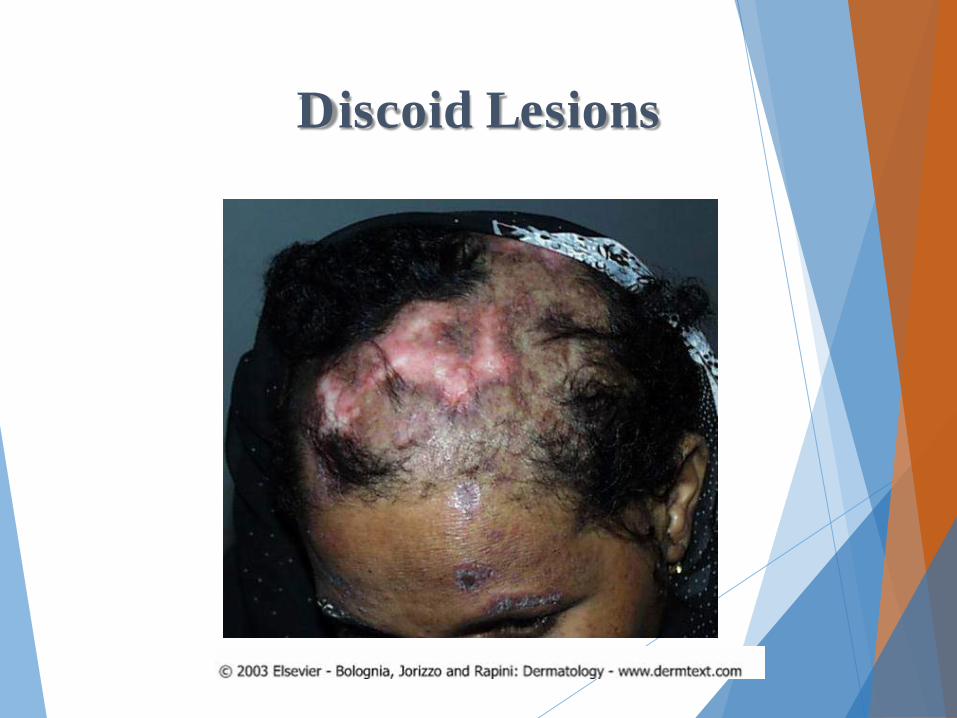
Discoid Lesions
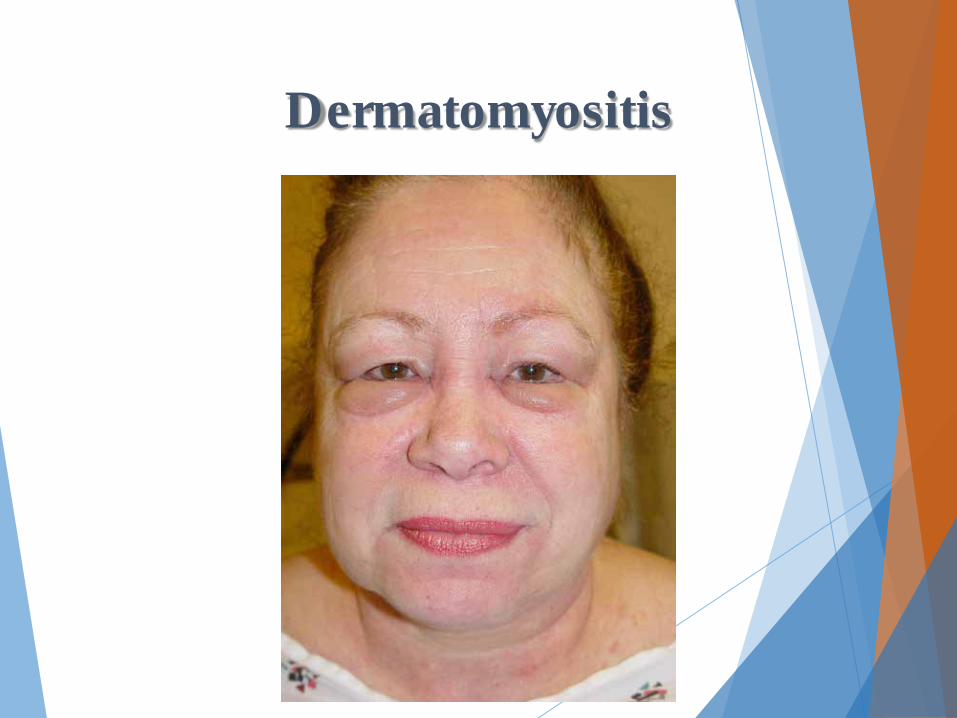
Dermatomyositis
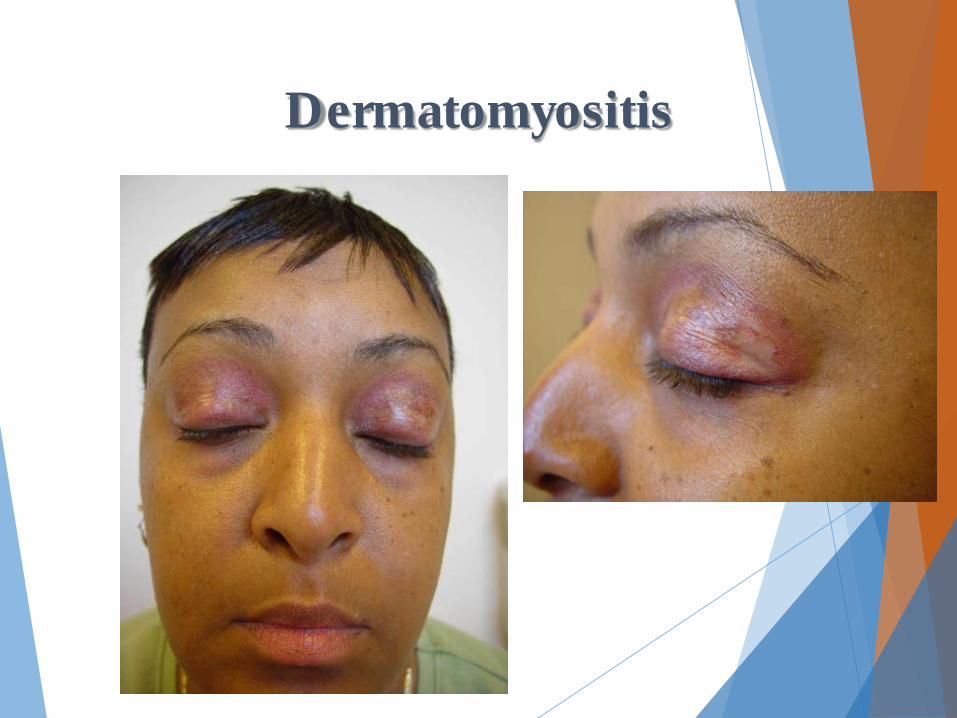
Dermatomyositis
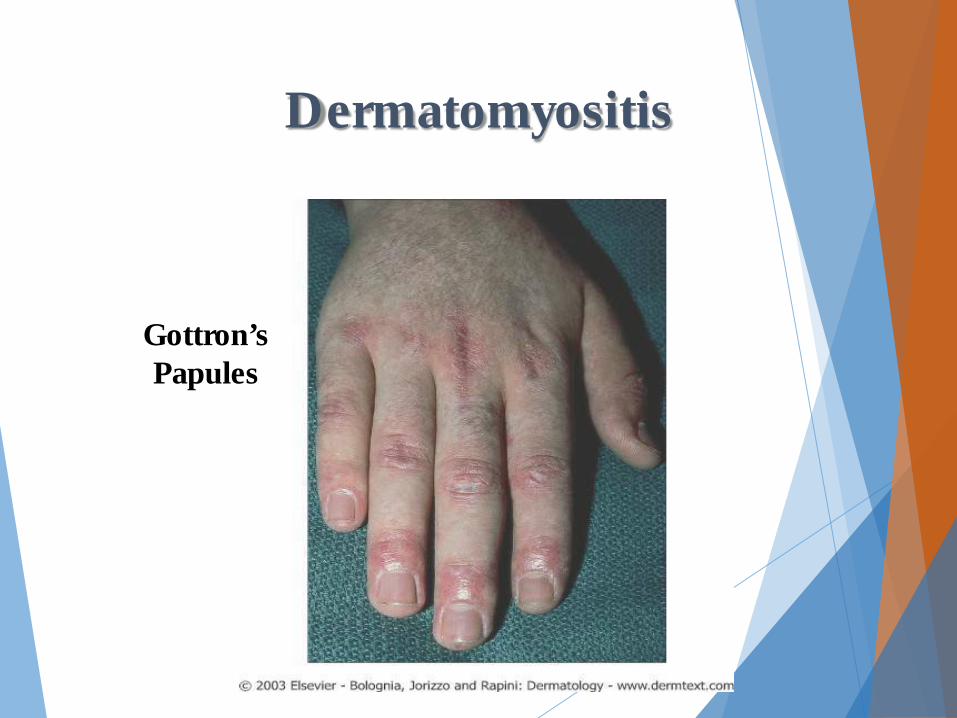
Dermatomyositis
Gottron’s Papules

Dermatomyositis
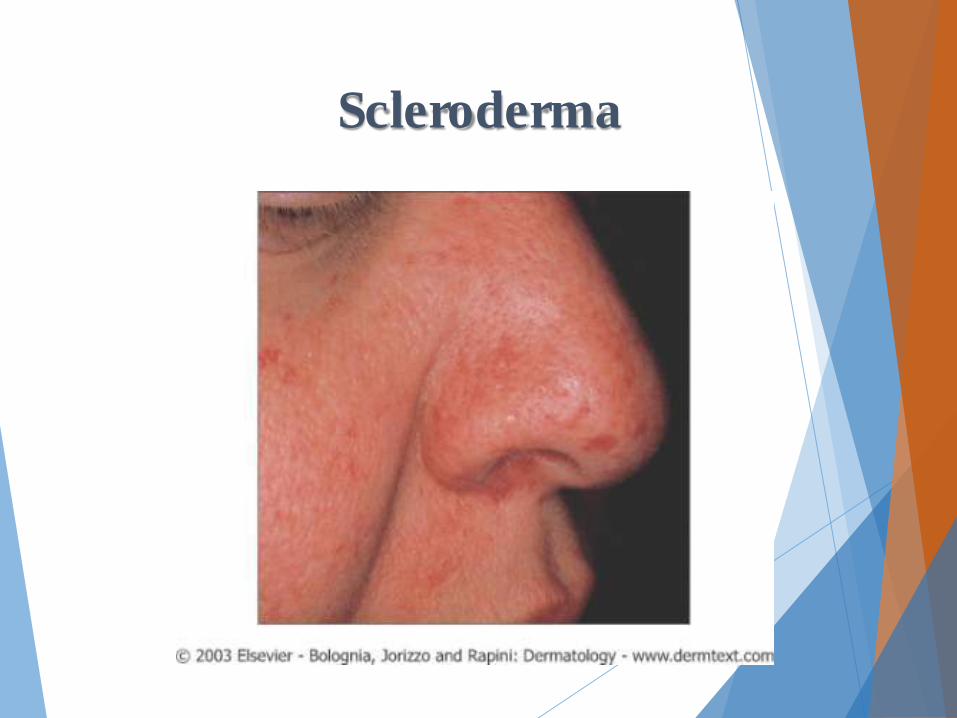
Scleroderma
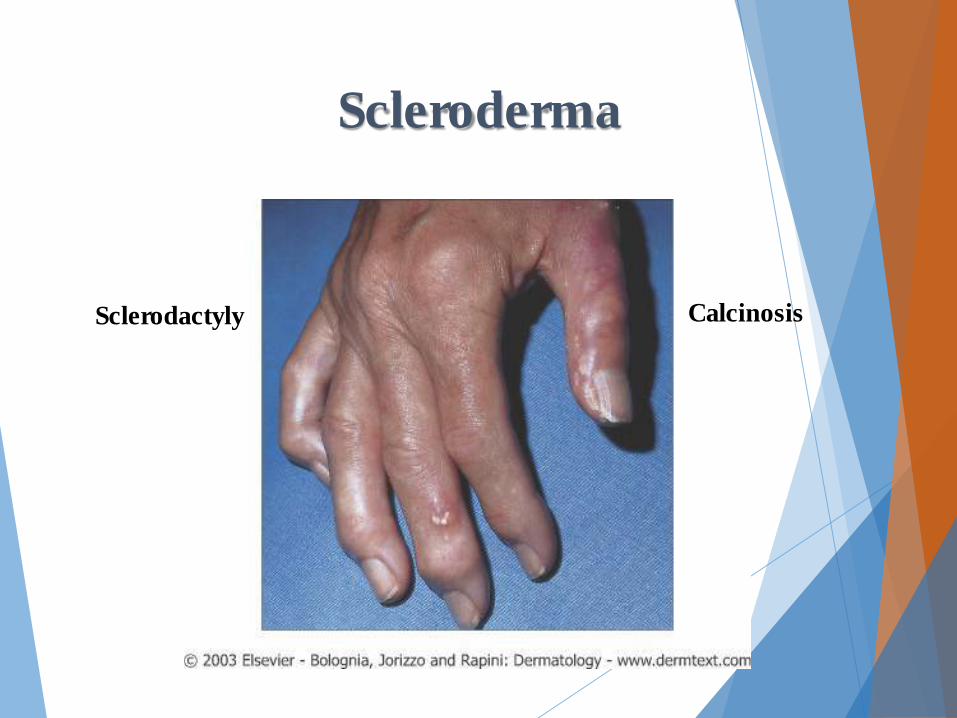
Scleroderma
Sclerodactyly Calcinosis

Scleroderma
Sclerodactyly Calcinosis
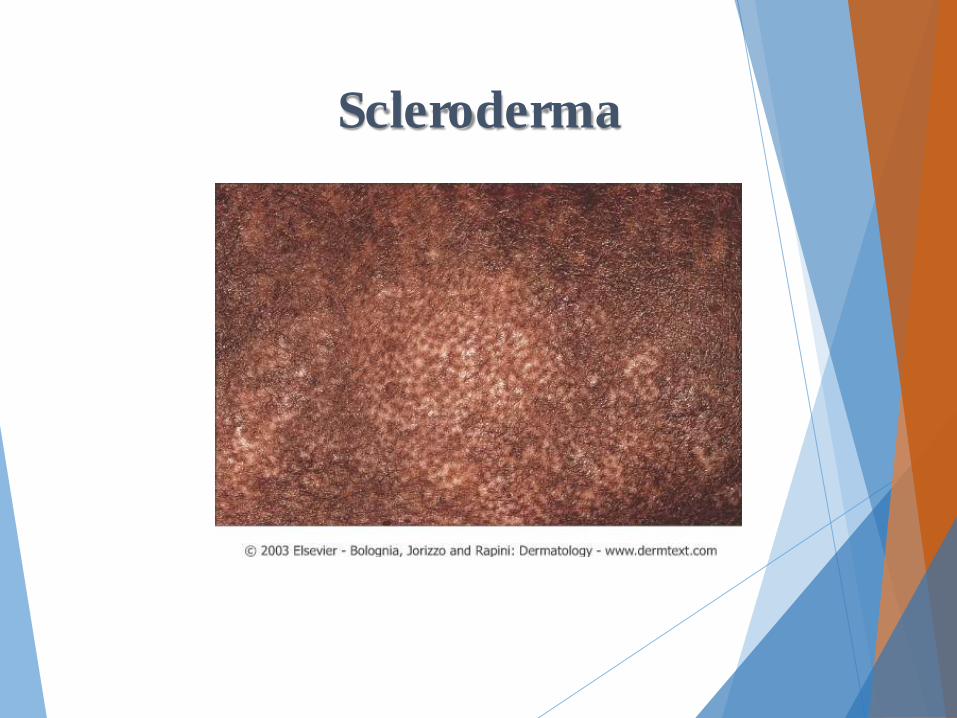
Scleroderma
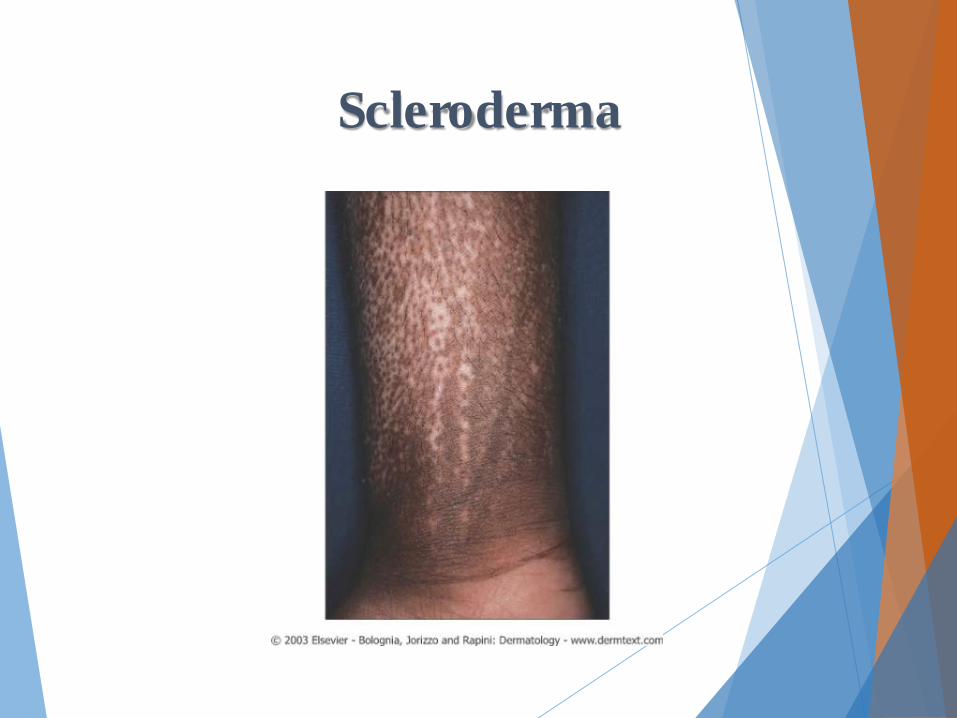
Scleroderma
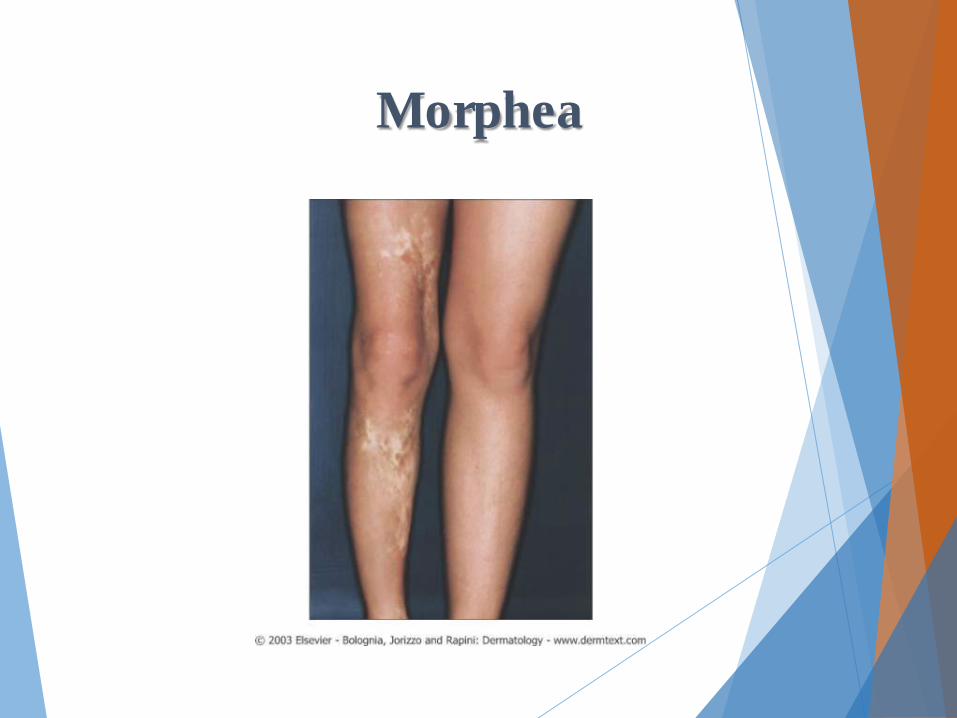
Morphea

Morphea

Morphea
Drug Reactions
Drug Reactions v The skin is common target for adverse drug reactions
v Logical approach is needed based on clinical characteristics, chronologic factors and use of a literature search
v Drug reactions can have a polymorphous morphology v Urticaria, purpura, full thickness epidermal necrosis, annular
patches
v Exanthematous eruptions and urticaria are the two most common
v Early differentiation between a severe drug eruption vs an uncomplicated drug eruption is critical v Dermatological consultation can be useful

Severe Cutaneous Adverse Reactions
v Drug reaction with eosinophilia and systemic symptoms (DRESS)/drug-induced hypersensitivity syndrome (DIHS)
v Stevens–Johnson syndrome and Toxic epidermal necrolysis
v Bullous drug eruption (Linear IG-A, Pemphigus, Vulgaris, Bullous Pemphigoid)
v Anaphylaxis
v Anti-coagulant induced skin necrosis
v Generalized Fixed Drug

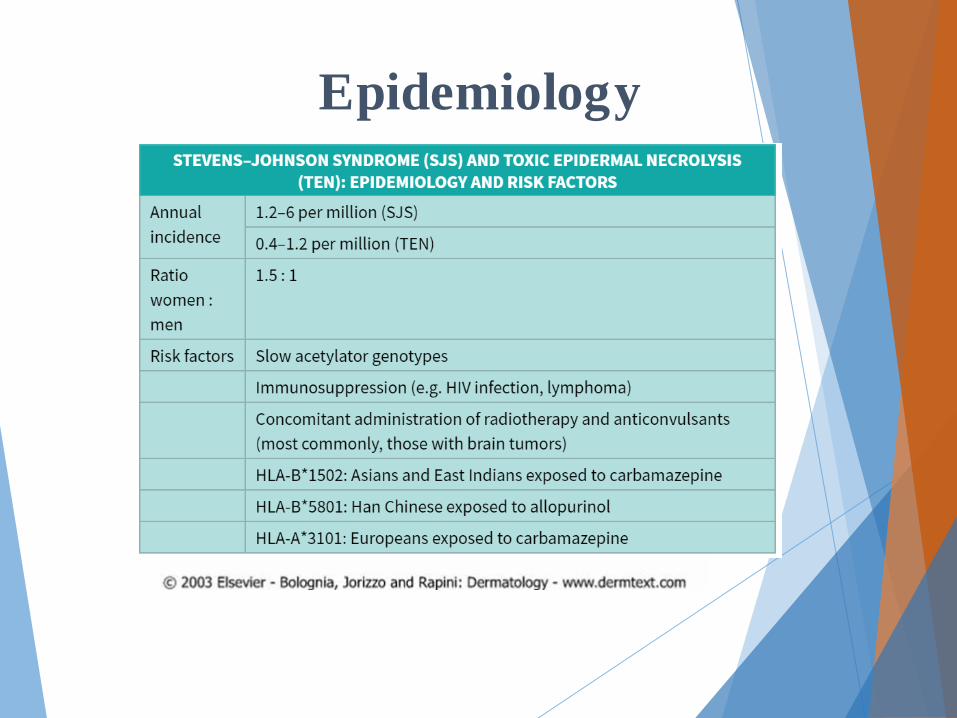
Epidemiology
v 2% of all drug-induced skin reactions are considered “serious”
v 1 in every 1000 hospitalized patients will have a serious drug reaction
vWorld Health Organization definition: v “if it results in death, requires hospitalization or
prolongation of existing hospital stay, results in persistent or significant disability/incapacity, or is life-threatening”

Epidemiology
v Increased age, female gender, and number of drugs
v AIDS (10-50x greater Morbilliform risk to Sulfa) v Primary responsible drugs penicillins,
cephalosporins, sulfonamides, anti-epileptic, and nonsteroidal anti-inflammatory drugs (NSAIDs).

Pathogenesis
v Immune Mediated Drug Eruptions v Non Immune Mediated v (sometimes predictable)
v Idiosyncratic
Pathogenesis
v Immune Mediated Drug Eruptions vIgE-dependent drug reactions vCytotoxic drug-induced reactions vImmune complex-dependent drug reactions vCell-mediated reactions

Immune Mediated Drug Eruptions
v IgE-dependent drug reactions (formerly type I, Gell–Coombs classification):
v Urticaria, angioedema and anaphylaxis
v Cytotoxic drug-induced reactions (antibody against a fixed antigen; formerly type II):
v Petechiae secondary to drug-induced thrombocytopenia
v Immune complex-dependent drug reactions (formerly type III):
v Vasculitis, serum sickness and certain types of urticaria
v Possible delayed-type, cell-mediated drug reactions (formerly type IV; sometimes not well defined):
v Exanthematous, fixed and lichenoid drug eruptions, Stevens–Johnson syndrome (SJS) and TEN.

Pathogenesis
vNon Immune Mediated (sometimes predictable) vOverdose, Cumulative Toxicity, Drug-Drug
Interaction
v Exacerbation of Disease (androgen/steroids acne)
vDelayed (arsenic induced SCC, alkylating agent induced leukemia)
Pathogenesis
v Idiosyncratic vDRESS vSJS/TEN vDrug reactions in HIV
Making the Diagnosis
vClinical Characteristics vPrimary lesions
vUrticarial, erythematous papule, pustule, purpuric papule, vesicle or bulla
vDistribution and number of lesions
vMucous membrane involvement, facial edema
vAssociated signs and symptoms:
vfever, pruritus, lymph node enlargement, visceral involvement
Making the Diagnosis
vChronological Factors vDocument all drugs to which the patient has been
exposed (including OTC and complementary) and the dates of administration
vDate of eruption
vTime interval between drug introduction (or reintroduction) and skin eruption
vResponse to removal of the suspected agent

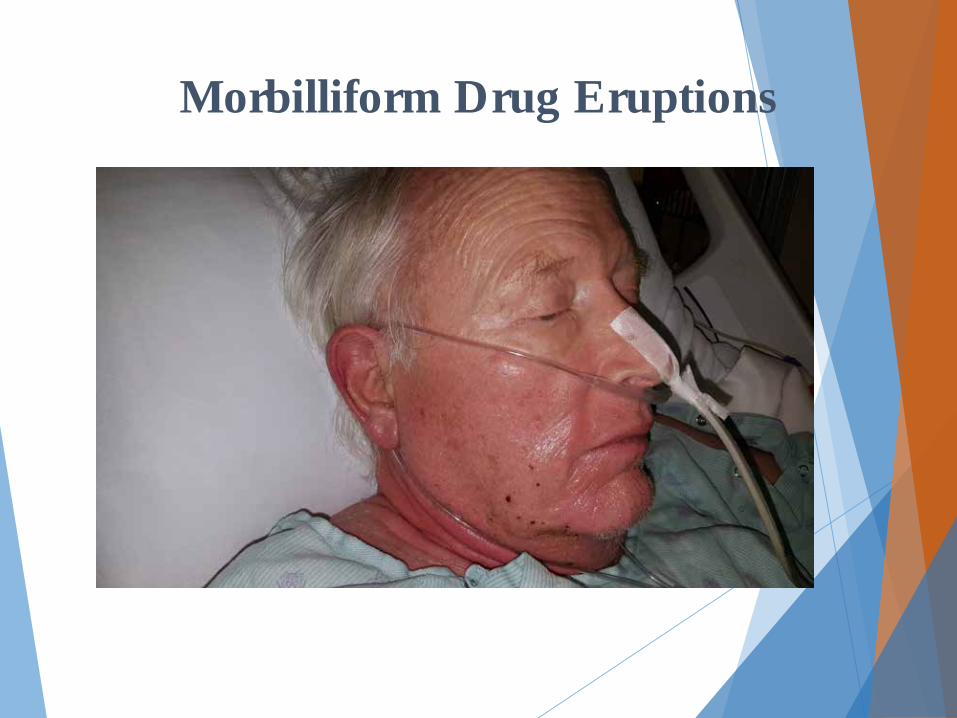
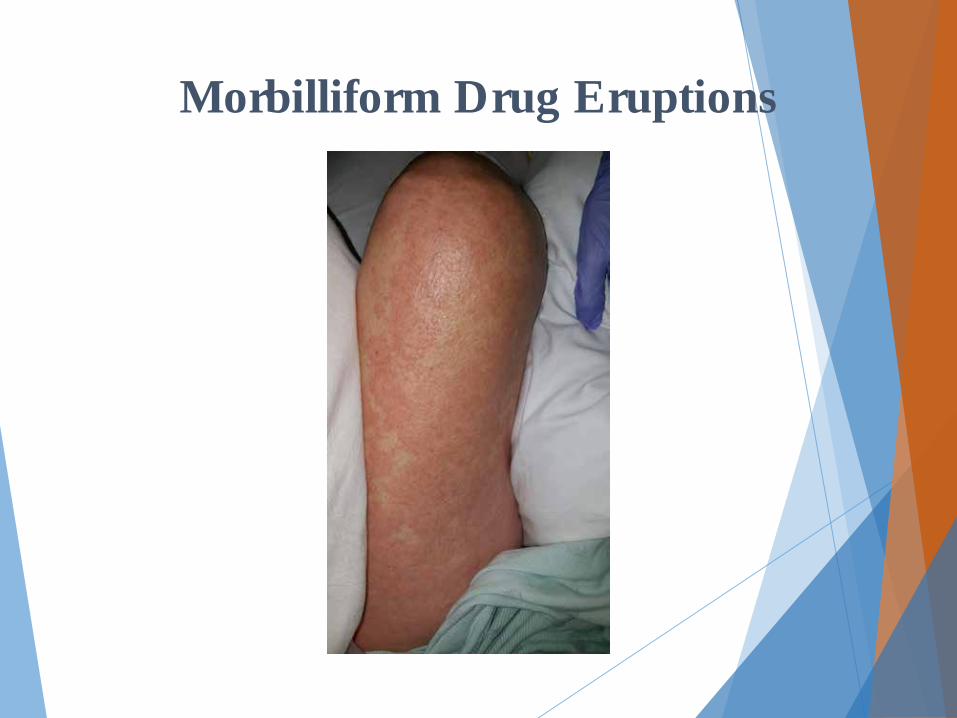
Morbilliform Drug Eruptions
v Most common drug rash v Usually begins 7-14 days after beginning medication v Erythematous maculopapular eruption, + pruritis v No mucosal involvement v May have low-grade fever but usually do not appear
toxic v Penicillins, sulfa, cephalosporins, anticonvulsants v DDx: Viral exanthem, DRESS, SJS/TEN

Morbilliform Drug Eruptions

Morbilliform Drug Eruptions

Morbilliform Drug Eruptions

Morbilliform Drug Eruptions

Morbilliform Drug Eruptions

Morbilliform Drug Eruptions

Morbilliform Drug Eruptions

Morbilliform Drug Eruptions

Morbilliform Drug Eruptions
Morbilliform Drug Eruptions
Morbilliform Drug Eruptions

Morbilliform Drug Eruptions

Morbilliform Drug Eruptions
v Treatment is largely supportive v Topical antipruritics and corticosteroids may help to
alleviate pruritus
v Discontinuing the offending agent is the first therapeutic measure
v “Treating through”, i.e. continuing the drug despite the cutaneous eruption, can be considered when the suspected drug is of paramount importance for the patient and there is no satisfactory

Morbilliform Drug Eruptions
v Dissapears within a few weeks v Few patients may experience a progressive
worsening, leading to erythroderma
v Whether continuation of the drug can lead to SJS is debatable
v “Leaving the same station”, they may be on different tracks from the beginning.
Urticaria and Angioedema
v Transient erythematous and edematous papules and plaques
v Pruritic v Individual lesions last less than 24 hours v Occurs on re-exposure to causative agent v <10% urticaria caused by drugs v Penicillins, cephalosporins, sulfa, tetracyclines,
NSAIDs
Urticaria and Angioedema
v Angioedema is transient edema of dermis and subcutaneous tissue
v Ace inhibitors, NSAIDs, Penicillins, Cephalosporins, contrast dyes
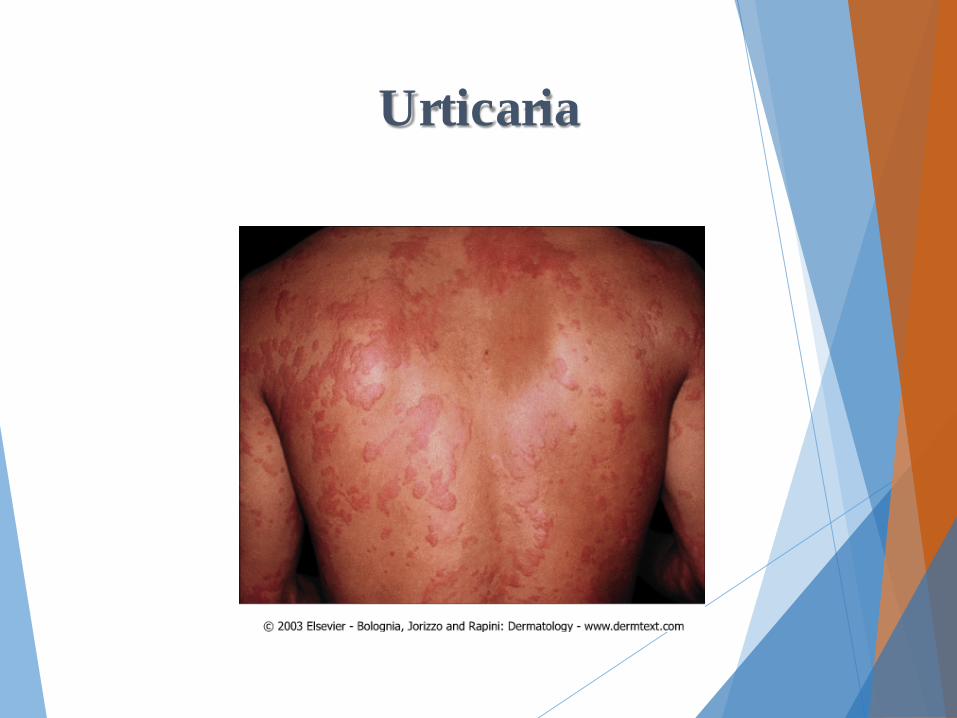
Urticaria
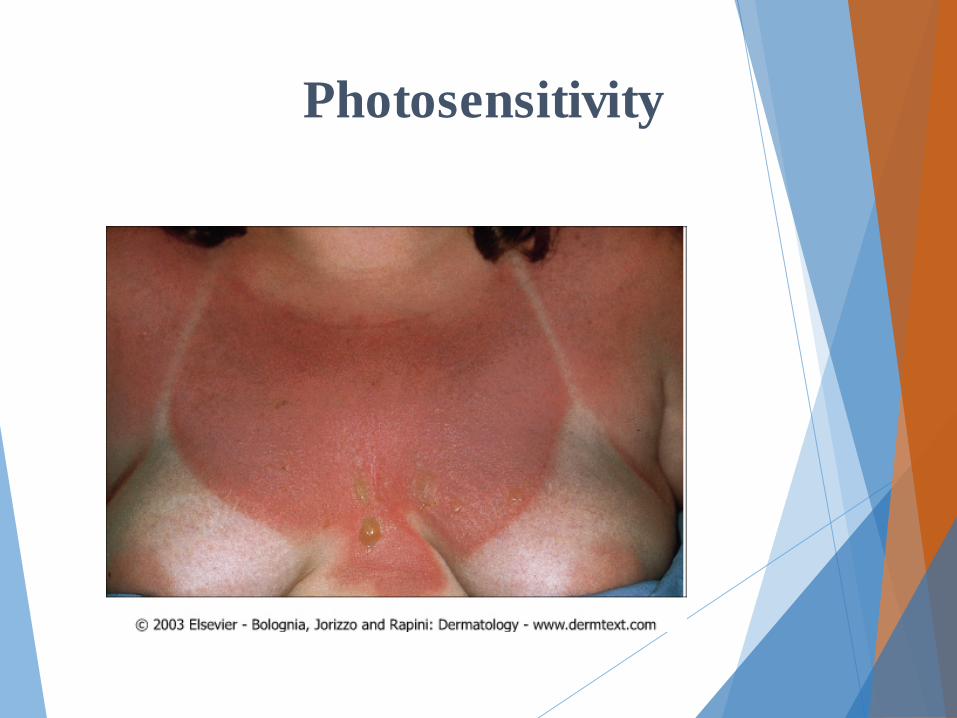
Photosensitivity
v Light + Drug = photosensitivity eruption
v Seen on sun-exposed skin
v Erythema +/- pruritus
v Tetracyclines, NSAIDs, fluoroquinolones, sulfa drugs
Photosensitivity
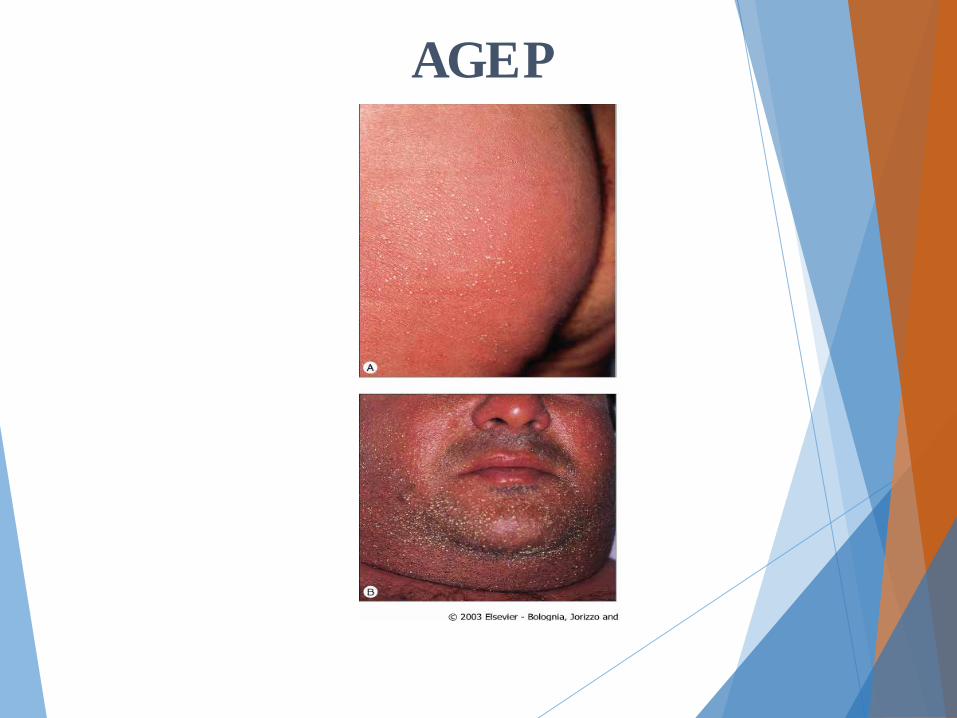
Acute Generalized Exanthematous Pustulosis (AGEP)
v Small pustules on edematous, erythematous skin; burning or pruritic
v Starts about 2 days after starting the drug
v Systemic signs: High fever, eosinophilia, transient renal dysfunction, normal LFTs
v Beta-lactam antibiotics, macrolide antibiotics most common causes
AGEP
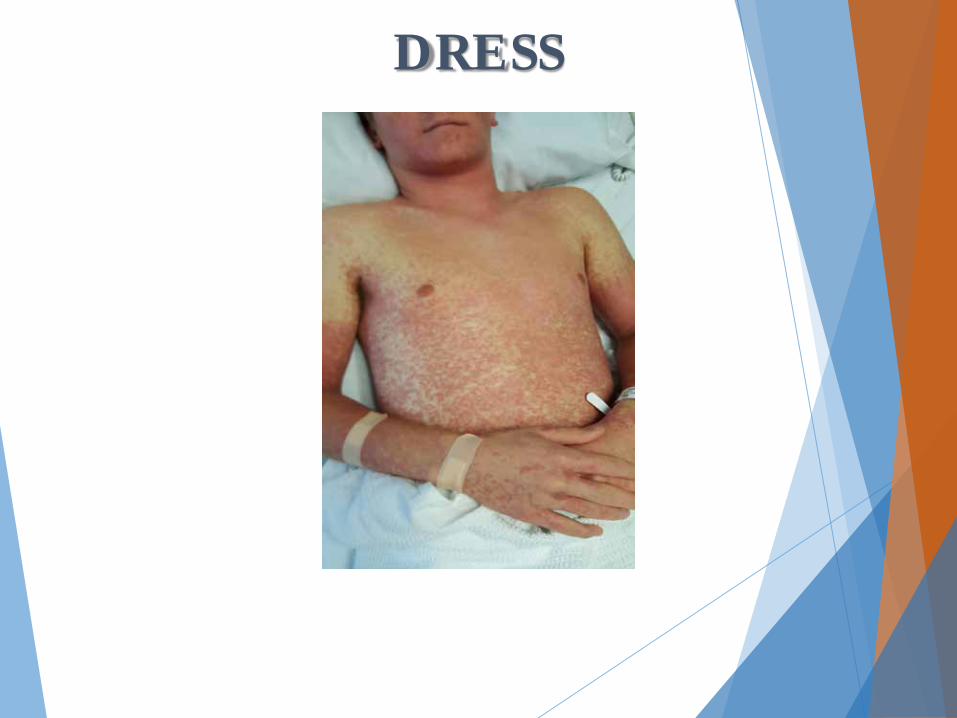
Drug Reaction with Eosinophilia and Systemic Symptoms
(DRESS)/Hypersensitivity Syndrome v Morbilliform à edematous with follicular accentuation;
morphology varies v 2-6 weeks after beginning offending drug v Systemic signs: Fever, hepatitis, eosinophilia, myocarditis,
nephritis, pneumonitis, atypical lymphocytosis, arthritis, lymphadenopathy
v Hepatitis may be fatal v Anticonvulsants (phenytoin, lamotrigine, carbamazepine),
sulfa drugs, allopurinol most common causes

Drug Reaction with Eosinophilia and Systemic Symptoms
(DRESS)/Hypersensitivity Syndrome v Lymph nodes are often enlarged v Arthralgias or even arthritis may be seen. v Most common (and usually the most severe) site of visceral involvement is the
liver v Sometimes fulminant v Responsible for the majority of deaths (10% of cases)
v Myocarditis, interstitial pneumonitis, interstitial nephritis, thyroiditis and even infiltration of the brain by eosinophils may be observed.
v Allopurinol induced gastrointestinal bleeding v Serial CBC with diff, CMP, initial C-Xray, EKG, and TSH

DRESS
DRESS

DRESS

DRESS

DRESS
Treatment of DRESS v Early withdrawal of the offending drug is mandatory
v Corticosteroids represent the first line of therapy
v Systemic corticosteroids are recommended for life-threatening involvement of the lung and heart because the inflammation is responsive to corticosteroids.
v Not particularly useful for reversing kidney and/or liver disease.
v Relapse can occur when the dosage is tapered
v Steroid therapy sometimes weeks to months
v Serial CBC with Diff, CMP, TSH
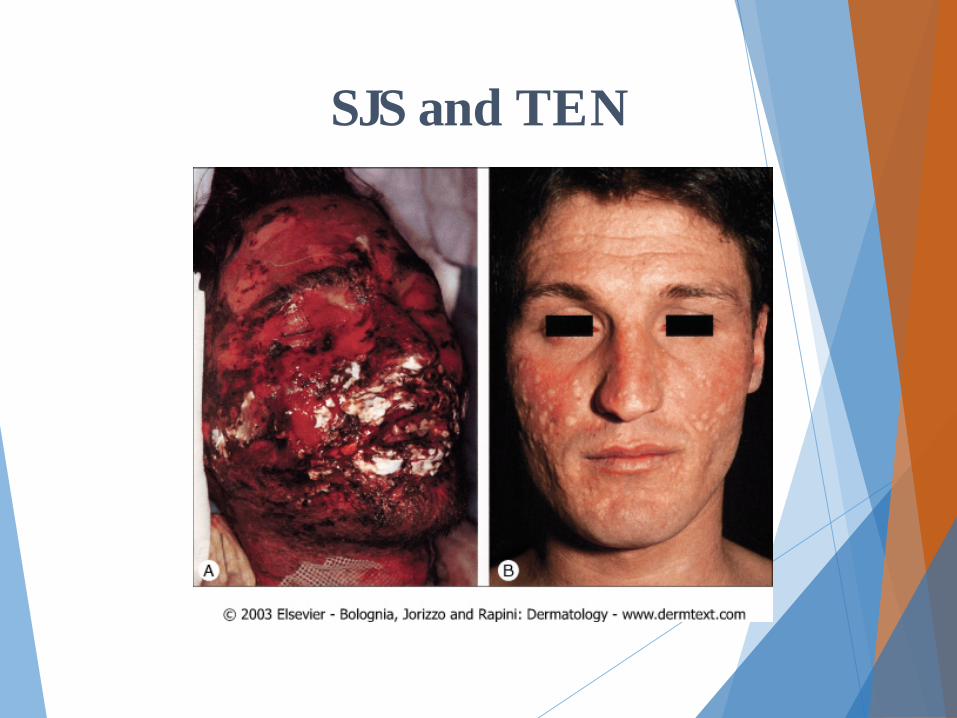
Stevens-Johnson Syndrome (SJS) and Toxic Epidermal Necrolysis (TEN)
v Consider both on a spectrum of disease v Cell-mediated reactionàapoptosis v 7-21 days after drug exposure v Erythematous and purpuric macules and
targetoid lesions, leading to flaccid bullae and full thickness epidermal detachment, leaving dermis behind
SJS and TEN
v Palms and soles often involved v Systemic signs: Fever, prodrome with URI-type
symptoms, mucosal lesions v Prone to fluid imbalance, sepsis v NSAIDs, sulfa, allopurinol, anticonvulsants,
penicillins
Epidemiology

Mucosal erosions Non-infectious conjunctivitis
SJS and TEN

SJS and TEN
SJS and TEN

Sequelae v Death occurs in every third patient
v infections (S. aureus and Pseudomonas aeruginosa)
v Massive transepidermal fluid loss v Electrolyte imbalance
v inhibition of insulin secretion/ insulin resistance
v Hypercatabolic state
v Complications of TEN best managed in intensive care units.
Sequelae v Re-epithelialization is complete in most cases within
3 weeks
v Healing is not perfect v Symblepharon
v Conjunctival synechiae
v Entropion
v Ingrowth of eyelashes
v Cutaneous scarring
v Irregular pigmentation
Sequelae
v Healing Sequelae v Eruptive melanocytic nevi
v Persistent erosions of the mucous membranes
v Phimosis
v Vaginal synechiae
vNail dystrophy
vDiffuse hair loss

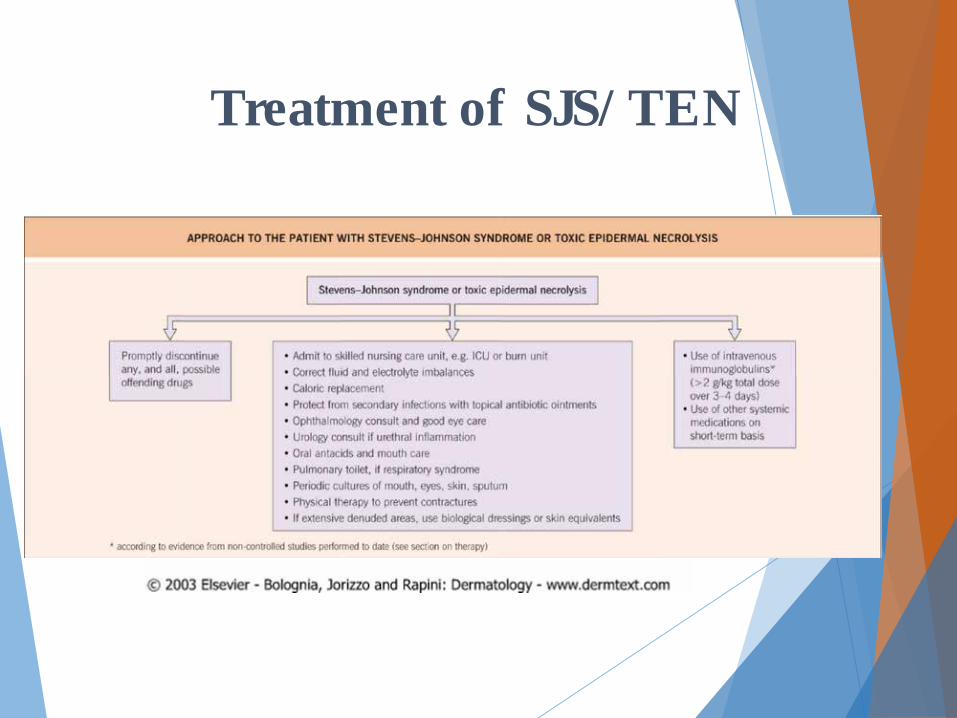
Treatment of SJS/TEN v Early withdrawal of the offending drug is mandatory
v Wound Care: v Detached areas, particularly on the back and pressure sites in
contact with the bed, should be covered with Vaseline® gauze until re-epithelialization has occurred
v Serous and/or bloody crusts cleaned daily with isotonic sterile sodium chloride solution
Treatment of SJS/TEN v Nostrils cleaned daily with a sterile cotton swab,
moistened with isotonic sterile sodium chloride solution, and antibiotic ointment
v Mouth rinsed QID with isotonic sterile sodium chloride solution
v Anogenital region and interdigital spaces short applications of silver nitrate solution (0.5%) in the case of maceration
Treatment of SJS/TEN
v Ophthalmology consult v Eyes cleansed daily with isotonic sterile sodium
chloride solution
vOphthalmic antibiotic ointment applied to the eyelids
v Antibiotic eyedrops should be administered three times a day to the cornea v reduce bacterial colonization minimize scarring.

Treatment of SJS/TEN
v 1g/kg/day of IVIg for three consecutive days (total dose of 3 g/kg) v Can check stat IGA levels before infusion if available
v No specific therapies for SJS and TEN have shown efficacy in prospective, controlled clinical trials v Cyclosporine (3–4 mg/kg/day)
v Cyclophosphamide (100–300 mg/day)
v Plasmapheresis, N-acetylcysteine (2 g/6 h)
v TNF-α antagonists (e.g. etanercept, infliximab)
Treatment of SJS/TEN

Potentially Dangerous Signs
v Cutaneous: Skin pain, necrosis, bullae/vesicles, mucous membrane changes, palpable purpura, tissue swelling, arthritis
v Rashes of SJS/TEN, DRESS, and morbilliform rashes may all look similar initially
v Other: fever, lymphadenopathy, SOB/wheeze v Labs: eosinophilia, abnormal LFTs, atypical
lymphocytes
References
v Bologna J, Jorrizo JL, Rapini RP, et. al.,
Dermatology 3rd edition, Elsevier 2012. v Callen J, Jorrizo JL, Bolona J, et. al.,
Dermatological Signs of Internal Medicine 4th edition, Elsevier 2009
v Robson KJ, Piette WW. Cutaneous manifestations of systemic diseases. Med Clin North Am. 1998, 82: (6): 1359-1380