dermatology - love
TRANSCRIPT
Dermatology
Justin Love, MPAS, PA-C
Loma Linda University
Department of Dermatology

Description
• Why is the description so important in dermatology?
– Allows for proper communication between specialties
– Will prioritize the patient placement into clinic or when
to be seen as inpatients
– Can sometimes make the Dx over the phone
• Two phrases to avoid
– Lesion, Mass, growth – can sometimes be confusing
or misleading
– “Macuolpapular” – implies drug eruption, typically all
rashes have a macular component, and a papular
component (active vs inactive)

Morphology - Primary
• Macule - flat, nonpalpable, <1.0cm
• Papule - raised, palpable, <1.0cm
• Patch - flat, nonpalpable, >1.0cm
• Plaque - raised, palpable, >1.0cm
• Vesicle – fluid filler blister, <1.0cm
• Bulla – fluid fill blister, >1.0cm
• Nodule – firm/solid, deeper than a papule
• Cyst – fluid filled nodule
• Pustule – pus filled papule/plaque

• Macule: non-palpable, < 1 cm

Patch: non-palpable, > 1 cm

Papule: palpable, < 1 cm

Plaque: palpable, > 1 cm

Nodule: A firm (indurated) lesion that is thicker or deeper than the average papule or plaque

Cyst: a firm filled nodule with an associated pore/ostia, >1cm

Vesicle: Elevated with clear fluid, < 1 cm

Bulla: elevated with clear fluid, > 1 cm

Pustule: a follicular based pus filled papule

Morphology - Secondary
• Erosion
• Ulcer
• Excoriation
• Fissure
• Scale
• Crust
• Scar

Erosion: superficial loss of tissue

Ulceration: reaches at least the depth of the dermis

Excoriation: Scratched, similar to abrasion but self inflicted

Fissure: cleft, groove, cracked usually linear

Scale: shedding, flaky rough to touch

Crust: thick, rough to touch

Scar: healed wound, sore, burn, surgery

Arrangement
• Linear
• Round/nummular – no central clearing
• Annular – central clearing
• Iris/targetoid
• Group/herpetiform
• Zosteriform/dermatomal
• Reticular





Atopic Dermatitis
• EPIDEMIOLOGY
90% of patients with AD have disease onset before the
age of 5 years
AD is thought to arise from an interaction between
environmental and genetic factors
maternal history of atopy was found to be one of the
strongest risk factors

Pathogensis
• Genetics–study of 372 AD patients, 59% had respiratory allergies and 73% reported a positive family history of atopy
.
–AD related to defective filaggrin appears to be inherited in a
semidominant fashion, and increased IgE levels, predisposed to
asthma(AD, asthma and allergic rhinitis)
Pathogensis
• Immunology– Respiratory allergy is commonly (70% of patients) associated
with childhood and adult AD
– most frequent allergens are dust mites, pollen, animal dander
and molds
– Food allergies occur primarily in infants and children with
moderate to severe AD
– Microbial agents, especially Staphylococcus aureus, colonize
over 90% of AD skin lesions
– predisposed to viral (herpes simplex virus, molluscum
contagiosum and human papillomavirus) and superficial fungal
(Trichophyton rubrum and Malassezia species) skin infections

Clinical Features
• AD skin is characterized by severe dryness with an impaired barrier function of the stratum corneum
• higher transepidermal water loss and lower skin surface hydration levels
• Three classical stages of AD–infantile, childhood and adulthood
• Acute predominates in infantile form, whereas chronic changes typify adult intensely pruritic, erythematous, edematous papules and plaques, often with secondary excoriations, vesicles, oozing and serous crusting can be seen.
• Subacute skin lesions appear as erythematous papules and
plaques, with scaling and excoriations as secondary changes.
• Chronic AD is characterized by thickened, hyperkeratotic plaques
with lichenification as well as prurigo nodularis.

Atopic Dermatitis
• 3 stages
– infantile 2mo – 2y
• seborrheic dermatitis
more likely if <2mo
• clue: SD, pt comfortable
– childhood 2y – 10y
– adult
• pruritus is hallmark
– precedes rash
– “the itch that rashes” itch-
scratch cycle
• distribution
– nummular = coin shaped
– hand / foot dermatitis
• eczematous, scaly
• dy idrotic = “tapioca
pudding-like” vessicles on
lateral fingers
– papular
• usually in darker skinned
pts
– location specific = eyelid,
scrotal, nipple, etc






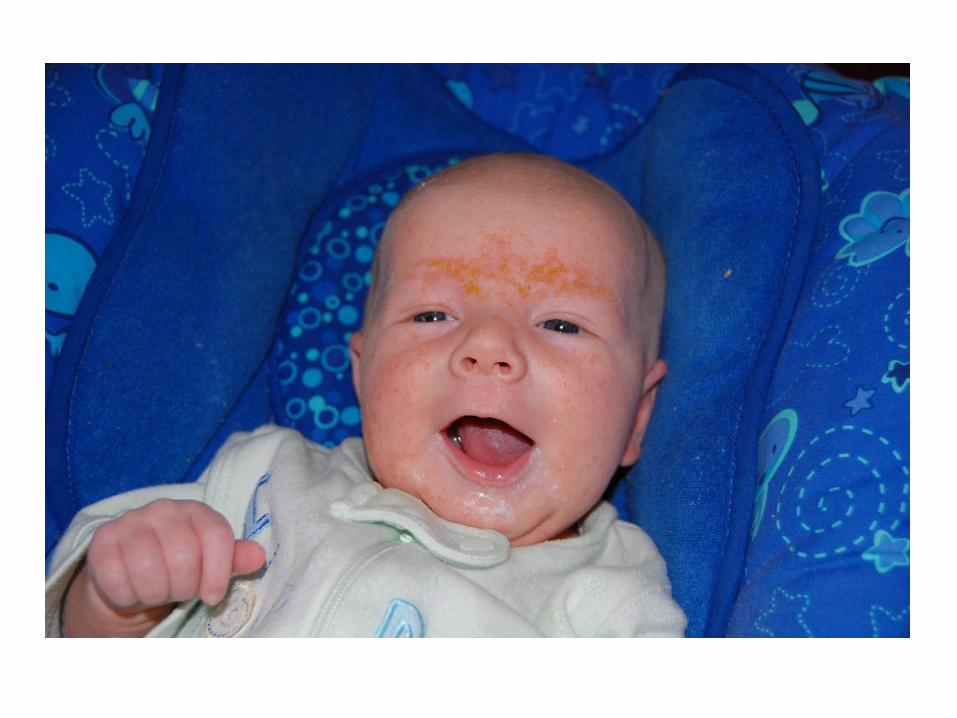
Infantile Atopic Dermatitis
• facial involvement
– erythema and scaling of cheeks
– chin 2/2 drooling, subsequent repeated washing
scalp, neck, forehead, wrists, extensor extremeties
• child’s capacity to scratch
– spares diaper area
– crawling extensor surfaces
• exudative
• development
– normal growth if < 50% of BSA
– impaired growth with more extensive disease





Pathology & Diagnostic Test
• The histologic features of AD vary according to stage of the lesion
sampled
• Peripheral blood eosinophilia is often seen in patients with AD-
neither sensitive nor specific enough to be of diagnostic utility
• Total IgE levels-elevated, minor diagnostic criterion
• radioallergosorbent testing (RAST)-elevated, relationship between
high IgE levels to foods, pollens, dust mites & aggravation AD is
controversial.
s
RAST is high IgE high

Diagnostic Criteria
MAJOR (3+)
• pruritus
• typical morphology,
distribution
– adults: flexural lichenification
– infants: facial, extensor
• chronically relapsing
• personal, family h/o atopy
– asthma, hay fever, AD
MINOR (3+)• xerosis
• ichthyosis/hyperlinear palms/keratosis pilaris
• IgE reactivity (RAST test
• serum IgE
• early age of onset
• cutaneous infxn tendency
• tendency to non-specific hand/foot dermatitis
• nipple eczema
• cheilitis
• recurrent conjunctivitis
• Dennie Morgan folds
• keratoconus
• anterior subcapsular cataracts
• orbital darkening
• facial pallor / erythema
• pityriasis alba
• itch when sweating
• intolerance to wool and lipid solvents
• perifollicular accentuation
• food hypersensitivity
• environmental &/or emotional factors infl course
• white dermatographism
Dry skinformation of dry, fish-like scales
Recent Literature
• maternal dietary restrictions during pregnancy or lactation does not prevent
atopic disease
• exclusive breastfeeding for at least 4 mo.s prevents or delays the
occurrence of atopic dermatitis, cow’ s milk allergy, and wheezing in early
childhood in at risk infants
• no clear evidence
– supporting the use of soy-based infant formulas for the purpose of
allergy prevention
– after 4-6 mo.s, delaying solid food introduction, including highly
allergenic foods, has a significant protective effect
Childhood Atopic Dermatitis
• less exudative
• atecubital / popliteal fossae, flexor wrists, eyelids, face common sites
• lichenified, indurated plaques
• growth retardation
– > 50% BSA involvement
– rebound growth with treatment


Childhood Atopic Dermatitis
• prognosis
– 40% resolve by age 5
– 40% carry to adulthood
• unfavorable prognostic factors
– widespread dermatitis in childhood
– family h/o AD
– associated bronchial asthma
– early age of onset
– female sex
– persistent dry / itchy skin in adult life

Adult / Adolescent AD
• erythematous, scaly, papular, exudative or lichenified plaques
• classic sites = antecubital / popliteal fossae, flexor wrists, around neck, eyelids
• lichenification, prurigo-like nodules
• darker skinned individuals
– hyper- and hypopigmentations
– papular variants

Adult / Adolescent AD
• pruritus occurs in crises or paroxysms
• flares triggered by heat or stress
– decreased itch perception
– difficulty delivering sweat to surface and in transepidermal water loss (TEWL)
• improvement occurs with time, uncommon after middle life
• new onset HIV may serve as trigger r/o if high risk





Associated clinical findings and
complications
• Pruritus
• Xerosis
• Keratosis pilaris•
Ichthyosis vulgaris
• Dennie–Morgan lines
• Palmoplantar hyperlinearity
• Pityriasis alba
• Lichenification
• Infection
• Edema
• Complications of treatment
protein in the skin called keratin forms hard plugs within hair follicles.
Round or oval, colorless patches of skin appear on the face, upper arms, neck, and upper middle of the body. scales.

Associated clinical findings
• pityriasis alba
– poorly marginated, hypopigmented slightly scaly patches
on cheeks
– typically in young children
• keratosis pilaris
– horny, agminated, follicular erythematous lesions
– outer aspects of upper arms legs, cheeks, buttocks
• hyperkeratosis, hyperpigmentation dirty neck
grouped together

keratosis pilaris

pityriasis alba

Ophthalmologic Abnormalities
• 10% develop cataracts
– anterior most common
– posterior subcapsular well-established complication of systemic steroids
– more common in severe atopic dermatitis
• 1% develop keratoconus
– elongation and protrusion of the corneal surface
– considered to be 2/2 continuous rubbing of eye or as a degenerative change
– onset usually p/ adolescence
Atopic Dermatitis
secondary to

Staphylococcus Colonization
• staph colonization nearly universal
– lesion superinfection common
– antibiotic of benefit during flares
• recovered in
– 90+% lesions vs 76% uninvolved skin
– 79% anterior nares in atopics vs 10% nonatopics
• staph exacerbates atopic derm
– organism superantigen production T-cell activation
– organism superantigen production alternative glucocorticoid receptor expression topical steroid resistance

Superinfection
• flat warts / molluscum contagiosum
– chemical treatments (salicylic acid, cantharidin) poorly tolerated
– destruction (cryosurgery, electrosurgery, curretage for molluscum) often required to clear lesions
• dermatophyte infections
• widespread vaccinia infxn (eczema vaccinia)
– vaccinations against smallpox contraindicated
– even if atopic dermatitis in remission
• coxsackie A16 virus (eczema cosackium)
Atopic dermatitis







Management
• parental education key
• heavy emollients
– barrier disruption (ceramide, fillagrin deficiency)
– moisturize after TCS
• avoid hot showers, pat dry after shower
• antihistamines
• treat erythematous pruritic areas
– truly active, areas pt is scratching at
– lichenification / pigmentation will take mo.s-yr.s to resolve
• avoid potential allergens
– bathe with allergen free cleanser (Cetaphil, Vanacream)
– wear white cotton, avoid wool

Management
• topical corticosteroids
– AE: irreversible atrophy, striae, systemic absorption with HPA axis inhibition
• avoid mid-high potency on face/axillae/groin
– interrupted therapy
• AE
• tachyphylaxis
– ointments better absorption, more effective than creams
– better to tx hi potency x short term than lo potency x long term
– occlusion efficacy (but also risks (wet wraps))
• topical calcineurin inhibitors (Elidel, Protopic)
– steroid sparing
– great for facial involvement, days not using TCS
– approved for children > 2y
rapid decrease in the response to a drug due to previous (long term) exposure
hypothalamic-pituitary-adrenal
major part neuroendocrine syst- controls reactions to stress and regulates processes
TCS
block the inflammation process, which is part of the body's immune response. This can relieve itching and improve the rash of atopic dermatitis. They are a type of immunosuppressant

Management
SEVERE / RECALCITRANT CASES
• work-up for associated immunodeficiency, genodermatosis
– Wiskott - Aldrich = eczema, thrombocytopenia, pyogenic infxn
– hyper IgE (Job) syndrome = eczema, recurrent sinopulmonary infxns
–erythroderma (icthyosis linearis circumflexa), trichorrhexis invaginata
• phototherapy (UVB, PUVA)
• immunosuppresants (cyclosporine)
• avoid sy stemic steroids…rebound flare
Netherton's syndrome = atopic diathesis, icthyosiformsusceptibility
Contact Dermatitis
Irritant and Allergic

Irritant Contact
• localized to contact site (hands, face)
• direct cytotoxic effect inflammatory response, not immunologic
• Pathogenesis
– Penetration through permeability barrier
– Mild damage to keratinocytes
– Release of mediators of inflammation
• TNF-a, IL-6 and IL-1B
Contact dermatitis

ICD Subtypes
Acute ICD
• Developes 2/2 potent irritant exposure, often an occupational accident
• Must be a potent irritant, most commonly acids and alkaline solutions resulting in chemical burns
• Symptoms include burning, stinging and soreness
• Physical signs: erythema, edema, bullae and necrosis
Irritant Contact dermatitis

ICD Subtypes
• acute delayed ICD– retarded inflammatory response
– anthralin, benzalkonium chloride, ethylene oxide
– rxn not seen until 8-24h after exposure
– mimics ACD, however burning > pruritus
• irritant reaction ICD– wet chemical environments
– hairdressers, caterers, metal workers
– scaling, redness, vesicles, pustules, erosions
– begins under occlusive jewelry
ICD Subtypes
• cumulative ICD– multiple subthreshold insults, without sufficient time for
barrier restoration
– lichenification/hyperkeratosis
– pruritus, pain
–
• asteatotic dermatitis / eczema craquele– dry winter months
– elderly, frequently bathe without remoisturization
– dry icthyosiform scale, superficially cracked
– intense pruritus
Examples include soaps, water, household products...


ICD Subtypes
• pustular acneiform ICD– metals, croton oil, mineral oil,
tars, greases, cutting and metal fluids, naphthalenes
– Chloracne– Consider when folliculitis or
acneiform lesions develop in setting outside of typical acne
• airborne ICD– Developes in irritant exposed
sensitive skin– Distinguish from photoallergic
reactions by looking for involvement of upper eyelids, philtrum and submental regions
• frictional ICD– lichenification, acanthosis,
hyperkeratosis
hyperpigmented, velvety plaques
thickening of the stratum corneum

Irritants
• acids – inorganic > organic
• alkalis – more painful/destructive (with
exception of HF)
– wet cement (+/- concurrent chromate ACD)
• metal salts– cobalt
– mercury bluish linear pigmentation tongue, gums
– thimerosal
• solvents– benzene petechial eruption
(aplastic anemia)
– turpentine
• alcohols
• detergents/cleansers
• disinfectants– ethylene oxide
– aldehydes, iodines
– quaternium ammonium salts
• plastics

Irritants
• food
• water = universal solvent
– maceration intertrigo (+/- candida)
• bodily fluids
– urine, feces diaper rash, incontinent pts
– drool angular cheilitis (+/- candida)
• plants
– spurges (poinsetta) milky sap
– oxalate crystals (tulips, daffodils) bulb sorter’s disease
• caterpillars = puss (wooly), Io (green, red stripe)


ACD Pathogenesis
• type IV delayed type hypersensitivity reaction
• allergen specific rxn
• requires prior sensitization– initial contact sensitization primed T-cell milieu
– low concentration of allergen cytokine release eczematous dermatitis 8-96h after exposure
• allergens– > 3000 chemicals known to cause ACD
– low MW
– lipid soluble
– low concentration required
Allergic contact dermatitis

ACD Clinical
• rash initially localized to site of contact
• may spread to other areas (in contrast to ICD)
• Id/autoeczematization • activated epidermal T cells migrate locally or through
the circulation dermatitis at remote sites
(hypersensitivity)
• most often seen in ACD assoc c/ stasis dermatitis
• symmetric

Id to Poison Ivy

urticarial to milk
neosporin / mastisol / sutures / anesthetics
toilet seat

Occupations at risk for ACD
Textile workers disperse dyes, formaldehyde
Cashiers nickel
Construction chromate, cobalt
Shoemakers formaldehyde, chromate
Hairdressers PPD, fragrance, cocamidopropyl
betane
Medical thiuram (latex)
Dentistry gluteraldehyde (disinfectant, cold
sterilizer), thiuram, acrylates
Masseuse essential oils, botanicals

Patch Test
• True test– 2 panels = 23 allergens + 1 control
– 3rd panel = expanded allergen series
• preservatives = diazolidinyl urea, imidazolidinyl urea, quinolone mix
• steroids = budesonide, tixocortol-21-pivalate
• North American Contact Dermatitis Group (NACDG) = 45 allergens
• European Standard= 26 allergens
Patch Test
• 1st read = 48h (remove patches)
• 2nd read = 72h – 1wk– delayed response = bacitracin, corticosteroids,
gold, disperse blue dyes, PPD, neomycin
– distinguish irritant from allergic• common mild irritant allergens = nickel, carba,
potassium dichromate, chlorhexidine, glutaraldehyde, formaldehyde, cocamidopropyl betaine
• many allergens near irritant threshold
• irritant decrescendo response = in severity between reads
Management
• Avoidance
• Photoprotection for photodermatitis
• Education• American Contact Dermatitis Society (www.contactderm.org)
allergen avoidance lists
• Contact Allergen Replacement Database (CARD) safe shopping lists
• topical/systemic steroids
• antihistamines
• wound care

Top 10 Allergens
METALS
• gold
• cobalt
• nickel
• (thimerosol)
PRESERVATIVES
• formaldehyde
• quaternium-15
• thimerosal
ANTIBIOTICS
• neomycin
• bacitracin
FRAGRANCES
• balsam of Peru
• fragrance mix

Nickel
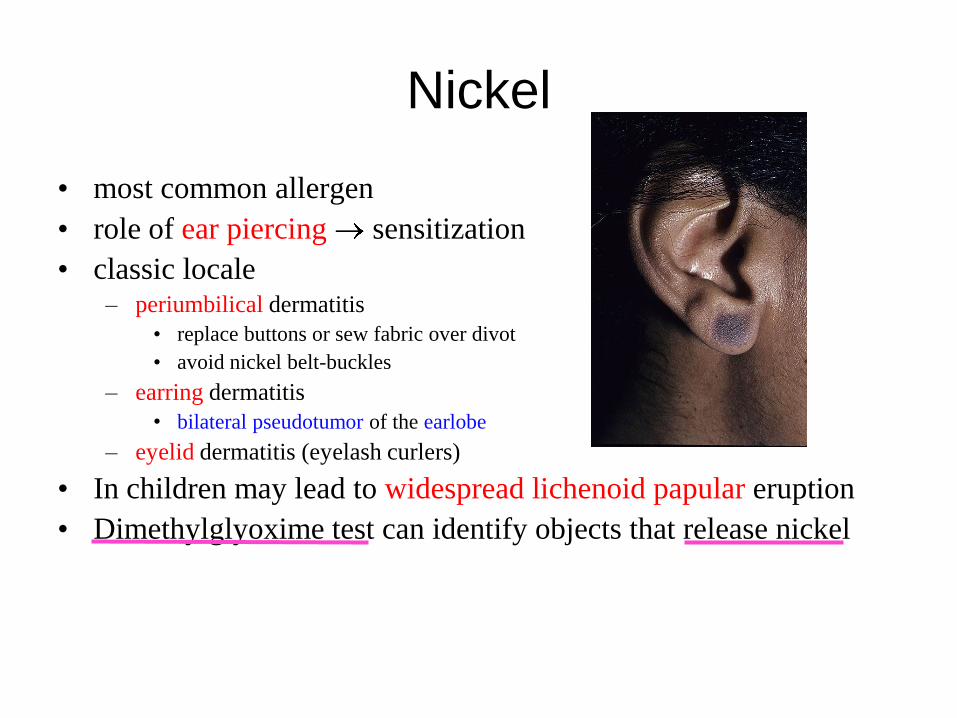
Nickel
• most common allergen
• role of ear piercing sensitization
• classic locale– periumbilical dermatitis
• replace buttons or sew fabric over divot
• avoid nickel belt-buckles
– earring dermatitis
• bilateral pseudotumor of the earlobe
– eyelid dermatitis (eyelash curlers)
• In children may lead to widespread lichenoid papular eruption
• Dimethylglyoxime test can identify objects that release nickel

Neomycin

Neomycin
• 2nd most common allergen
• Neosporin aka “triple antibiotic ointment” polymyxin B, bacitracin and neomycin
• Neomycin is also found in:
– Hemorrhoid creams, otic and ophthalmic preparations and in topical steroid preparations
• co-reactivity with bacitracin
• cross-reactivity with aminoglycosides

Poison Ivymicrovesicular
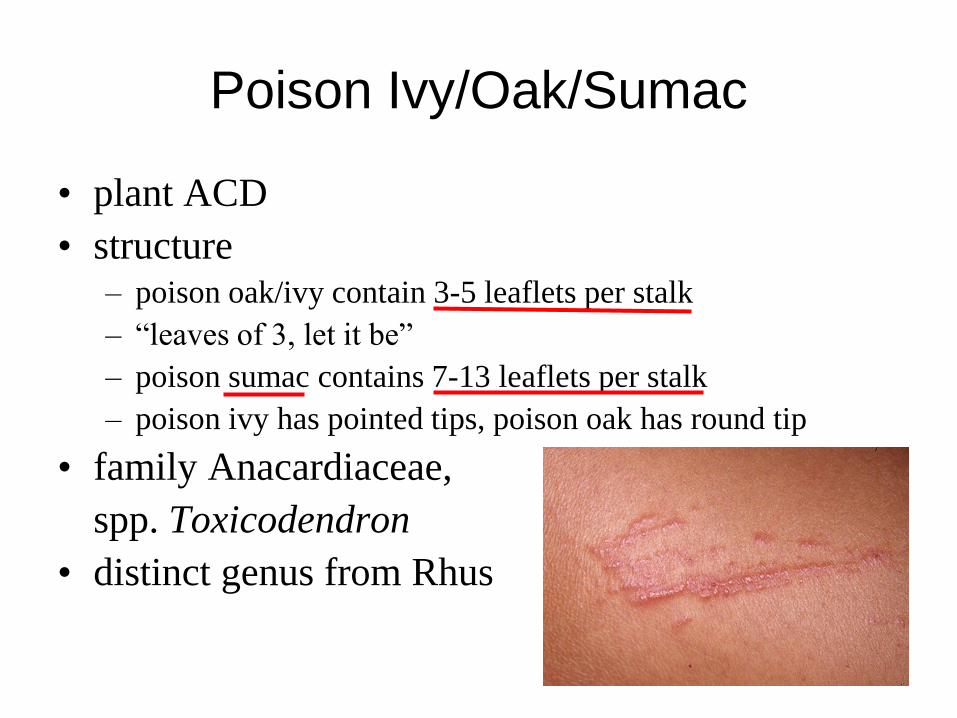
Poison Ivy/Oak/Sumac
• plant ACD
• structure– poison oak/ivy contain 3-5 leaflets per stalk
– “leaves of 3, let it be”
– poison sumac contains 7-13 leaflets per stalk
– poison ivy has pointed tips, poison oak has round tip
• family Anacardiaceae,
spp. Toxicodendron
• distinct genus from Rhus

Treatment
• Wash body should be thoroughly washed with copious amounts of
water. Soap may be used afterwards, but early use of soap may
expand the area of resin on the body.
• potent topical corticosteroids only help if applied during the earliest
stages of the outbreak-no vesicles or blisters
• Systemic corticosteroids-very effective dose of 1–2 mg/kg/day,
slowly tapered over 2-3 weeks
• Antihistamine doesn't take care of pruritus, but alows pt to sleep.-

SEBORRHEIC DERMATITIS
• confined to skin regions with high
sebum production &large body
folds
• link to sebum overproduction
and the commensal yeast
Malassezia
SEBORRHEIC DERMATITIS
• Epidemiology
– Infantile-self-limited and confined to the first 3 months of life
– Adult-chronic with a peak in the fourth to sixth decades
– no indication of a genetic predisposition
• Associated with?
• HIV, Parkinson‟s, mood disorders
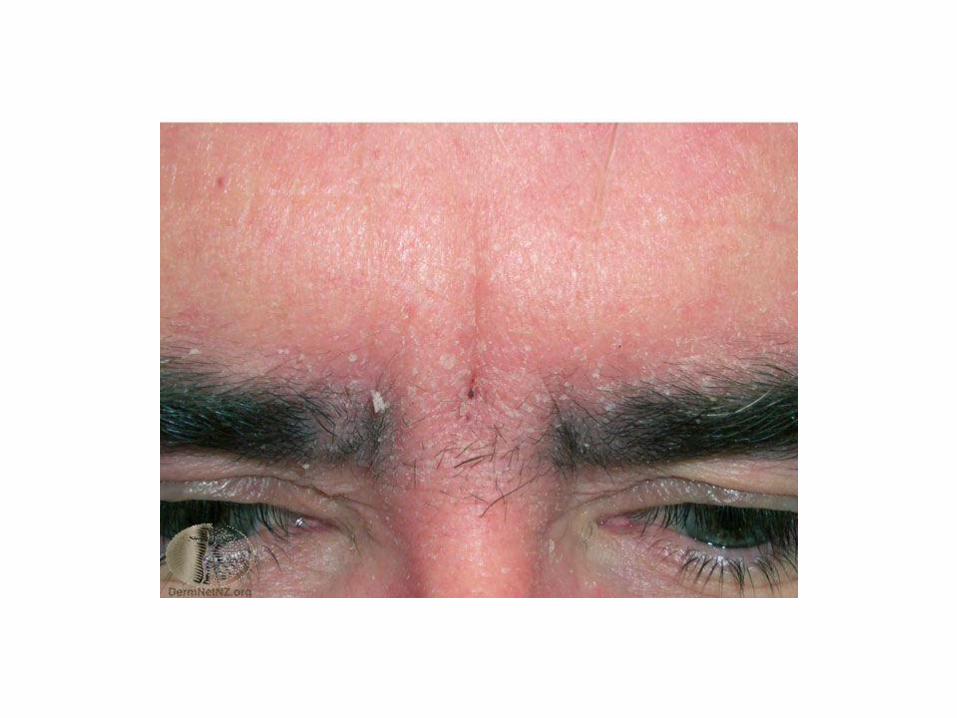
Clinical Features
• sharply demarcated patches or thin plaques that vary from pink–
yellow to dull red to red–brown in color with bran-like to flaky
mostly due to irritation (e.g. overenthusiastic treatment)
• a predilection for areas rich in sebaceous glands, e.g. the scalp,
face, ears, presternal region and, less often, the intertriginous areas
(e.g. the axillae, inguinal and inframammary folds, and umbilicus)
• a mild course with little or moderate discomfort
• Immunocompromised?
"greasy" scales; vesiculation and crusting may occur but are rare and

Infantile seborrheic dermatitis
• 1 week after birth and may persist
for several months
• mild greasy scales adherent to the
vertex and anterior fontanelle
regions
• coherent scaly and crusty mass
covering most of the scalp („cradle
cap‟)
• axillae and inguinal folds
• Superimposed infection with
Candida species may occur

Adult seborrheic dermatitis
• less often on central upper chest
and the intertriginous areas
• slight to moderate fine white or
greasy scaling of the scalp and
terminal hair-bearing areas of the
face, without significant erythema
or irritation
• symmetric: forehead, medial
portions of the eyebrows, upper
eyelids, nasolabial folds and
lateral aspects of the nose,
retroauricular areas, and
occasionally the occiput and neck
SEBORRHEIC DERMATITIS
• DDX– AD, Irritant diaper dermatitis, Infantile psoriasis, Langerhans cell
histiocytosis, Wiskott–Aldrich syndrome, tinea capitis, psoriasis,
systemic lupus erythematosus, rosacea
SEBORRHEIC DERMATITIS
• Infantile seborrheic
dermatitis
– bathing and the application
of emollients
– Ketoconazole cream (2%)-
if persistent
– Short courses of low-
potency topical
corticosteroids may be
used initially to suppress
inflammation
– Avoidance-strong
keratolytic shampoos, or
mechanical measures
• Adult seborrheic dermatitis
– topical azoles
ketoconazole-
shampoo/cream
– initial stages- low-potency
topical corticosteroids &
emollients
– Second-line-zinc pyrithione
& tar shampoos

NUMMULAR DERMATITIS
• coin-shaped lesions
• Men are affected slightly more often and at a later age than women
(>50 vs <30 years, respectively).
• pathogenesis has not been fully clarified? Microbial vs contact
sensitization
• defined as an eruption of round (discoid) eczematous patches
almost exclusively of the extremities- well demarcated, may be
acutely inflamed with vesicles and weeping
• excoriations are often prominent, usually takes a very chronic
course

NUMMULAR DERMATITIS
• DDX
– atopic dermatitis &
dissemination secondary to
contact dermatitis, stasis
dermatitis. Psoriasis,
Bowen's disease, mycosis
fungoides and tinea
corporis.
• Treatment
– Medium- to high-potency
topical corticosteroid
ointments, topical
tacrolimus or pimecrolimus
– phototherapy macrolide lactones or calcineurin inhibitors
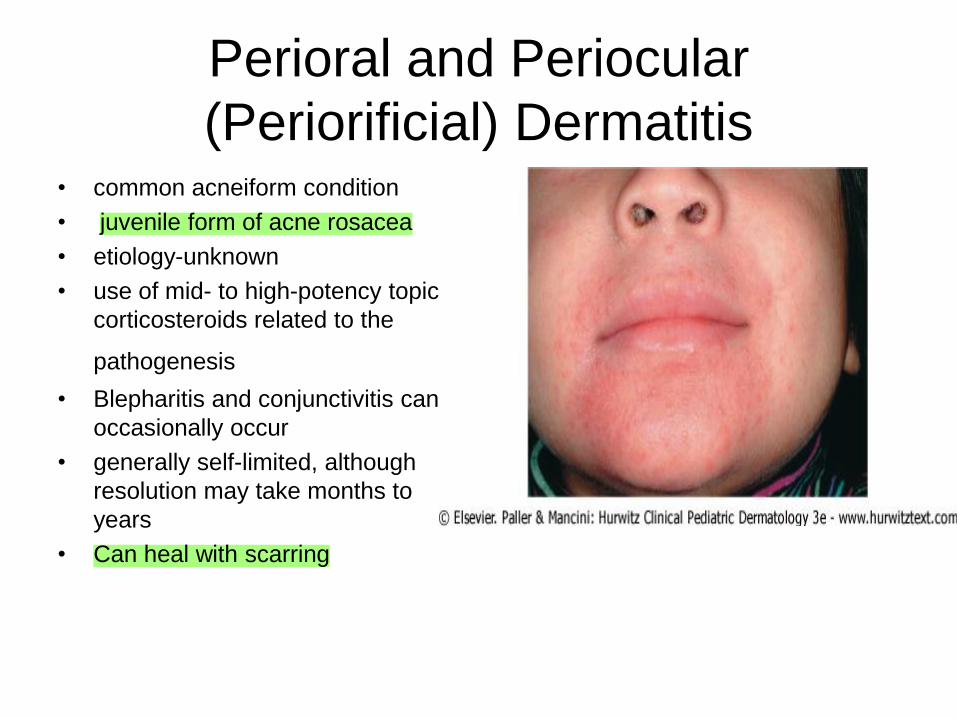
Perioral and Periocular
(Periorificial) Dermatitis • common acneiform condition
• juvenile form of acne rosacea
• etiology-unknown
• use of mid- to high-potency topical
corticosteroids related to the
pathogenesis
• Blepharitis and conjunctivitis can
occasionally occur
• generally self-limited, although
resolution may take months to
years
• Can heal with scarring

Perioral and Periocular
(Periorificial) Dermatitis• DDX
– Seborrheic Dermatitis, Acne
Vulgaris, Erythromelanosis
Faciei and Keratosis Pilaris
Rubra, Lupus Erythematosus,
Demodex Folliculitis

Perioral and Periocular
(Periorificial) Dermatitis• Tx
– Topical• Metronidazole 0.75% and 1% qd to
bid [cream, gel or lotion]
• Sodium sulfacetamide (with or
without sulfur and/or urea)10% qd
to bid [cream, foam, lotion,
suspension or wash](with sulfur)
• Azelaic acid 15% and 20% bid
[cream or gel]
• Bp/clindamycin 5% / 1% qd [gel]
•Tretinoin 0.01% to 0.1 % qd
[cream or gel]
• Tx
– Oral
• Tetracycline 250–500 mg qd to bid
• Doxycycline50–100 mg qd to bid,
20 mg bid, 40 mg qd
• Minocycline 50, 75, 100 mg qd to
bid; 40, 90, 135 mg (1 mg/kg) qd
• Erythromycin 200, 250, 333,
400, 500 mg (30–50 mg/kg/daily)
[bid to qid, depending on dose]
•Azithromycin250
–500 mg (5
–10
mg/kg)3times/week
• Isotretinoin10 to 40 mg qd
•
Please be aware of S/E peds pt!!
Not for pregnant women
2 form of contraceptive

STASIS DERMATITIS
• Clinical spectrum of chronic venous insufficiency of the lower
extremities
• Prevalence rates rise with age, and women are affected more often
than men
• venous ulcers are almost invariably accompanied by this form of
dermatitis
• Venous hypertension slows blood flow in microvasculature, distends
capillaries & damages capillary permeability barrier, allowing passage fluid & plasma proteins into the tissue (edema) &
deposition)
• Release of inflammatory mediators tissue remodeling,
lipodermatosclerosis
extravasation of erythrocytes (stasis purpura and hemosiderin

STASIS DERMATITIS
• Occurs-medial supramalleolar regions where microangiopathy is most intense,
• Dermatitis occurs dilated varicose veins, inflammation is known to induce epidermal dysfunction (hyperproliferation, barrier impairment, desquamation).
• Dry skin very common finding w/ CVI, and stasis dermatitis displays features of asteatotic eczema.
• severely pruritic- oozing and crusting
• Contact sensitization to components of topical therapies found in 58-86% of patients
Chronic venous insufficiency CVI

STASIS DERMATITIS
• DDX-
– straightforward diagnosis
– asteatotic eczema
– irritant or allergic contact
dermatitis
– psoriasis
– mycosis fungoides
• Tx-
– management of venous
hypertension adequate
compression bandages or
stockings(if ulcer present must
r/o arterial)
– lifestyle changes
– exercise calf muscles
– removal of insufficient
saphenous veins
– topical corticosteroids and
emollients

Diaper Dermatitis
• most common cutaneous disorder of infancy & early childhood
• being prolonged contact with urine and feces, skin maceration, and,
in many cases, secondary infection with bacteria or Candida
albicans
• three most common types of diaper dermatitis are chafing
dermatitis, irritant contact dermatitis, and diaper candidiasis

Diaper Dermatitis
• Chafing Dermatitis
– most prevalent form
– friction is the most pronounced (the inner surfaces of the thighs,
the genitalia, buttocks, and the abdomen)
– presents as mild redness and scaling and tends to wax and
wane quickly, frequent diaper changes and good diaper
hygiene.

Diaper Dermatitis
• Irritant Contact Dermatitis
– buttocks, the vulva, perineal
area, lower abdomen, and
proximal thighs, with sparing
of the intertriginous creases
– etiology-potential roles for
ammonia, bacteria, and
bacterial products and urine
pH
– petrolatum-based formulations
as a barrier
• Diaper Candidiasis
– suspected whenever a
diaper rash fails to respond
to usual therapy.
– Candidiasis possible 2/2
systemic antibiotic therapy
and should be considered
in any diaper dermatitis
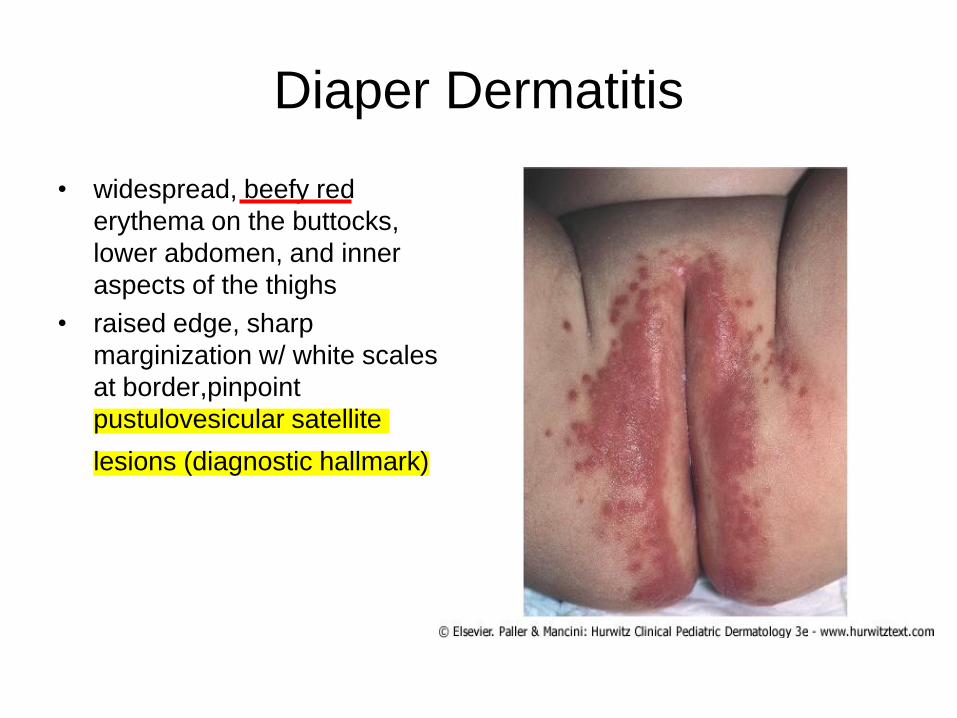
Diaper Dermatitis
• widespread, beefy red
erythema on the buttocks,
lower abdomen, and inner
aspects of the thighs
• raised edge, sharp
marginization w/ white scales
at border,pinpoint
pustulovesicular satellite
lesions (diagnostic hallmark)
Diaper Dermatitis
• DDX-
– Seb derm
– Psoriasis
– Intertrigo
– Jacquet's dermatitis
– Perianal pseudoverrucous
papules and nodules
– Miliaria
– Folliculitis
– Impetigo
– Scabies
– acrodermatitis enteropathica,
cystic fibrosis, biotin deficiency
– Allergic contact dermatitis,
– Atopic dermatitis
• DDX-
– Atopic dermatitis
– Granuloma gluteale infantum
– Langerhans cell histiocytosis
– Burns Child abuse
– Epidermolysis bullosa
– Congenital syphilis
– Varicella/herpes
– Tinea cruris
– Chronic bullous dermatosis of
childhood
– Bullous mastocytosis
Diaper Dermatitis
• Tx– appropriate etiology
– Educating
– keeping the skin dry, protected, and infection-free
– Zinc oxide and petrolatum-based formulation
– low-potency, nonfluorinated topical corticosteroid (i.e., 1% H.C.)
– Stronger steroids and combination antifungal-corticosteroid
preparations should be avoided
– appropriate systemic antibiotic
– Candidal infection requires the use of a topical antifungal agent
(i.e., nystatin, azoles)

Dyshidrosis
• Dyshidrotic eczema
• not a disorder of the sweat gland
• most common in adults, can occur
in children
• Emotional stress and hot weather
may exacerbate the condition
• DDX
– inflammatory tinea
pedis/manuum
– photoinduced pompholyx-
like hand dermatitis
– dyshidrosiform pemphigoid
cutaneous
– T-cell lymphoma
– scabies(children)
– infantile acropustulosis
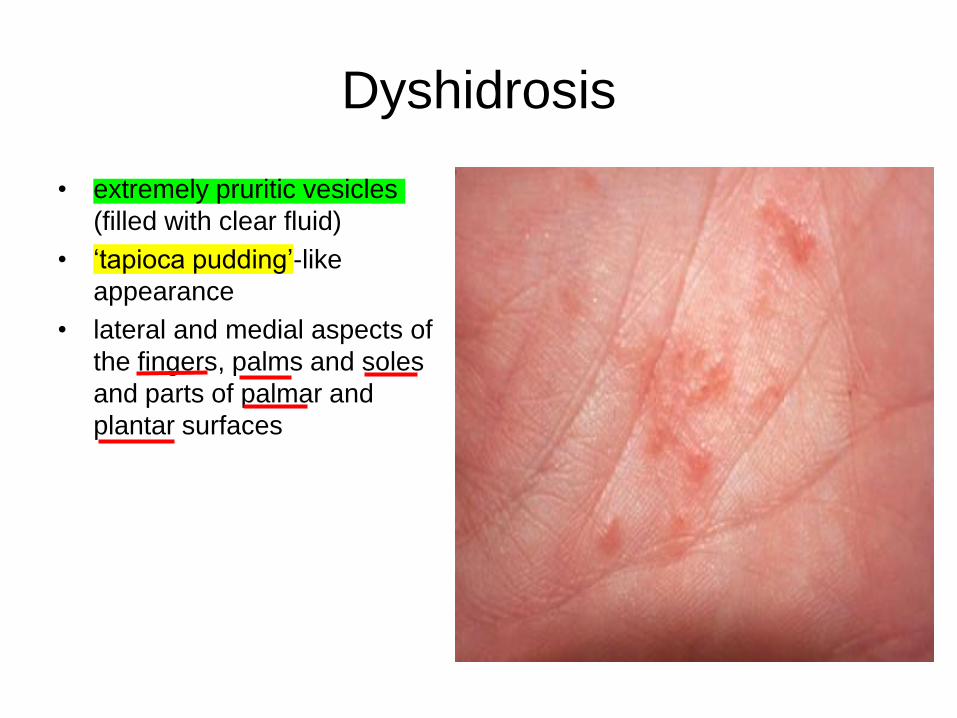
Dyshidrosis
• extremely pruritic vesicles
(filled with clear fluid)
• „tapioca pudding‟-like
appearance
• lateral and medial aspects of
the fingers, palms and soles
and parts of palmar and
plantar surfaces

Dyshidrosis
• Tx
– identification and treatment
of underlying causes
– High-potency topical
corticosteroids
– Topical calcineurin
inhibitors and phototherapy
(e.g. broadband or
narrowband UVB, UVA1,
PUVA)
– Short courses-systemic
corticosteroids severe
outbreaks
• Tx
– Severe recalicitrant-
azathioprine, methotrexate
and mycophenolate mofetil
(although mycophenolate
mofetil-induced dyshidrosis
has been described)
– Botulinum toxin injection
– Psychotherapy
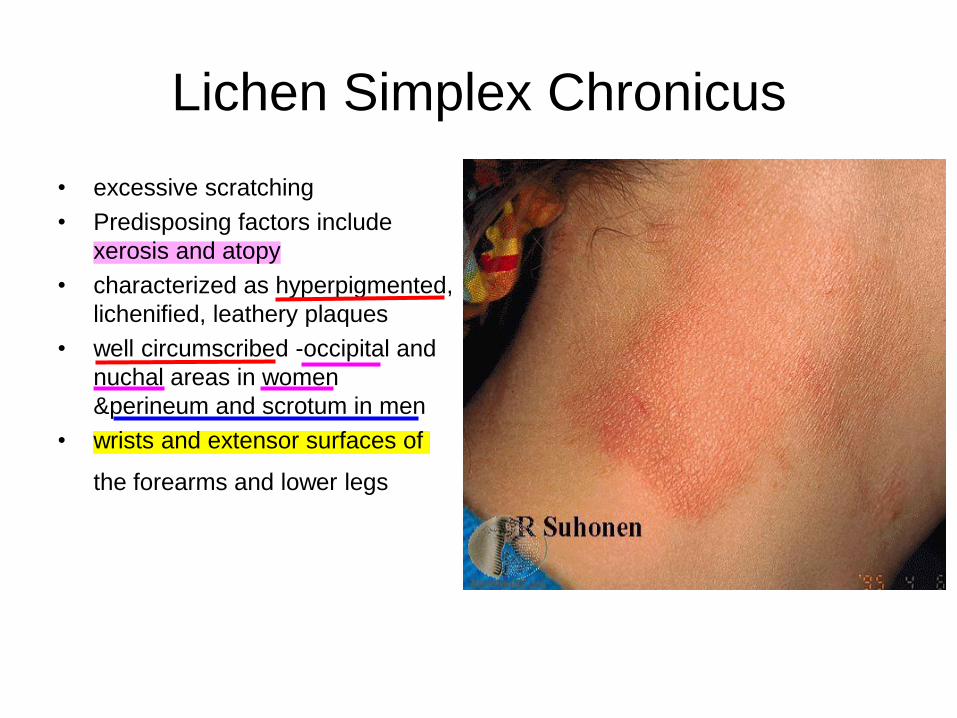
Lichen Simplex Chronicus
• excessive scratching
• Predisposing factors include
xerosis and atopy
• characterized as hyperpigmented,
lichenified, leathery plaques
• well circumscribed -occipital and
nuchal areas in women
&perineum and scrotum in men
• wrists and extensor surfaces of
the forearms and lower legs
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Lichen Simplex Chronicus
• Tx
– breaking the itch-scratch cycle
– Antipruritics
– Moisturizers
– Topical corticosteroids under occlusion
– Intralesional corticosteroids
– situational stressors-psychological

Tinea Corporis
• Fungi that invade keratinized tissue via keratinases
– Hair, Nails, S.cornuem
• Dermatophytes
– Trichophyton, Microsporum, Epidermophyton
– Trichophyton rubrum-most common dermatophyte
worldwide
– occur most frequently in postpubertal, except tinea
capitis
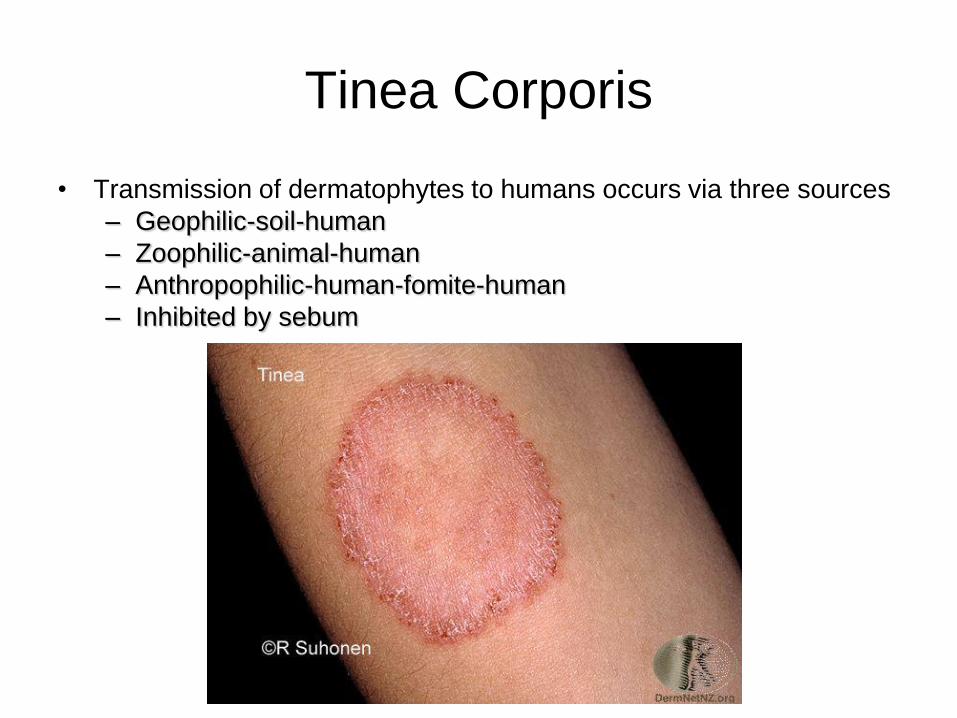
Tinea Corporis
• Transmission of dermatophytes to humans occurs via three sources
– Geophilic-soil-human
– Zoophilic-animal-human
– Anthropophilic-human-fomite-human
– Inhibited by sebum
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Tinea Corporis
• Incubation-1 to 3 weeks
• Spreads centrifugally w/ central clearing annular lesions
of varying sizes
• Scaly, although scale may be lessened or absent if
topical corticosteroids have been used (tinea incognito)
• Pustules within the active border, can be vesicular,
granulomatous or verrucous in appearance.
• Symptoms include pruritus and burning
• Dx made via KOH, occasional fungal cx & PAS stain via
bx

QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

Tinea Corporis
• DDX-
– Nummular eczema, Atopic,
Stasis, Contact, Seborrheic,
Pityriasis versicolor, Pityriasis
rosea, Parapsoriasis,
Erythema annulare
centrifugum, Annular
psoriasis, Subacute lupus,
Granuloma annulare,Impetigo
• Tx
– Topical antifungals-first line
– Systemic antifungal
therapy-higher incidence
and increased severity of
side effects-Fluconazole,
Griseofulvin, Itraconazole,
Terbinafine

Tinea Pedis
• Epidemiology and pathogensis similar to corporis
• soles of feet interdigital web spaces
• most common location for dermatophyte infections
• more common in adults and is found around the world, affecting
both sexes
• most believe acquried going barefoot (locker rooms, gyms, public
facilities), no specific susceptibility has been determined
• T. rubrum, T. mentagrophytes, E. floccosum and T. tonsurans (in
children)-typical dermatophytes
• Four types-Moccasin, Interdigital, Inflammatory (vesicular),
Ulcerative

QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Moccasin
Interdigital/maceration
Inflammatroy
Tinea Pedis
• Dx, DDX and Tx-similar to tinea corporis
• Erythrasma can be diagnosed with Wood's light examination
because of its coral-red fluorescence; empiric treatment with topical
erythromycin
• oral antifungals should be considered in diabetics,
immunocompromised patients, and those with moccasin type
• other dermatophyte infections often associated with tinea pedis-
tinea cruris, onychomycosis and tinea manus
chronic superficial infection of the intertriginous areas of the skinErythrasma

Tinea Versicolor
• Caused by Malassezia furfur
• occurs in tropical climates w/ high ambient temperatures & high
humidity, also in temperate climates
• Malassezia has an oil requirement for growth, increased incidence
in adolescents and sebum-rich areas of the skin, has been
implicated in seborrheic dermatitis and atopic dermatitis
• potassium hydroxide (KOH) examination-‟ziti and meatballs‟
• Other factors have been implicated-oily skin, excessive sweating,
immunodeficiency, poor nutrition, pregnancy and corticosteroid use

Tinea Versicolor
• multiple oval to round patches or thin plaques with mild scale
• upper trunk and shoulders, are the favored sites of involvement.,
less frequently, lesions are seen on the face (more so in children),
scalp, antecubital fossae, submammary region and groin
• most common colors are brown (hyperpigmented) and
tan(hypopigmented) occasionally there is mild inflammation leading
to a pink color
• asymptomatic and the major concern is its appearance.

QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Tinea Versicolor
• DDX
– vitiligo, pityriasis alba,
postinflammatory
hypopigmentation, seborrheic
dermatitis, pityriasis rosea,
tinea corporis and secondary
syphilis may mimic the
disease
• Tx
– Ketoconazole (1% or 2%)
or 2.5% selenium sulfide
shampoo is quite effective
– azole/allylamine creams
and lotions
– nystatin, salicylic acid and
a variety of over-the-
counter dandruff shampoos
– Systemic tx-ketoconazole,
fluconazole or itraconazole
may provide simple and
effective

Drug Eruptions
• Exanthematous or morbilliform eruptions are the most common
• Urticaria, Angioedema and Anaphylaxis
• Photosensitivity
• Vasculitis
• Neutrophilic Drug Eruptions
• Drug Reaction with Eosinophilia and Systemic Symptoms:
Hypersensitivity Syndrome
• Bullous Eruptions
• Drug-induced bullous pemphigoid

Drug Eruptions
• skin is one of the most common targets for adverse drug reactions
• women are more susceptible than men
• increases with the age of the patient, as well as the number of drugs
taken by the patient
• In a retrospective cohort study from the Netherlands of 13 679
patients from general practices, the most frequently reported skin
reactions to antimicrobials were due to
trimethoprim/sulfamethoxazole (2.1% of users), fluoroquinolones
(1.6%) and penicillins (1.1%).
• Common eruptive cutaneous drug eruptions are hypersensitivity
reactions with an underlying immunologic mechanism

Drug Eruptions
• Immunologically Mediated Drug Reactions
– IgE-dependent drug reactions (formerly type I, Gell-Coombs
classification): urticaria, angioedema and anaphylaxis.
– Cytotoxic drug-induced reactions (antibody against a fixed
antigen; formerly type II): petechiae secondary to drug-induced
thrombocytopenia
– Immune complex-dependent drug reactions (formerly type III):
vasculitis, serum sickness and certain types of urticaria
– Possible delayed-type, cell-mediated drug reactions (formerly
type IV) versus undefined: exanthematous, fixed and lichenoid
drug eruptions, as well as Stevens-Johnson syndrome (SJS) and
TEN.
Drug Eruptions
• Non-immunologic Mechanisms
– Overdose, Pharmacologic side effects, Cumulative toxicity,
Delayed toxicity, Drug-drug interactions, Alterations in
metabolism, Exacerbation of disease
• complete list of current (as well as past) medications, including
prescription, non-prescription/over-the-counter, and complementary
or alternative treatments
• time between initiation of drug & onset of eruption is a key element
in identifying offending drug-most immunologically mediated drug
reactions occur within 8 to 21 days after initiation of a new
medication
• usual practice is to discontinue all drugs that are non-essential
Drug Eruptions
• Exanthematous Drug Eruptions
– most common adverse drug reactions affecting the skin
– maculopapular drug eruptions
– erythematous macules that sometimes become slightly palpable; the distribution is usually symmetric, begins on the trunk and upper extremities and progressively becomes confluent
– polymorphous with morbilliform or sometimes urticarial lesions on the limbs, confluent areas on the thorax and purpuric lesions on the ankles and feet
– possibility of a more severe drug-induced eruption-edema of face or a marked peripheral blood hypereosinophilia( hypersensitivity syndrome/DRESS) and mucous membrane lesions or painful or dusky skin, which may announce TEN or SJS.
– A biopsy of morbilliform-not particularly helpful

QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

Drug Eruptions
• DDX-viral exanthems (e.g.
Epstein-Barr virus,
enteroviruses, adenovirus,
early HIV, human herpesvirus
type 6 [HHV-6], parvovirus
B19), which are often
indistinguishable
• drug etiology is favored in
adults, whereas a viral cause
is favored in the pediatric
population
• Tx-largely supportive, Topical
corticosteroids may help to
alleviate pruritus,discontinuing
the offending agent is the first
therapeutic measure
• drugs have a significantly
higher incidence (>3% of
patients): aminopenicillins,
sulfonamides, cephalosporins
and anticonvulsants
• ACEI, NASIDS

Lichen Planus
• idiopathic inflammatory disease of the skin and mucous membranes
• pruritic, violaceous papules that favor the extremities
• has been associated with multiple disease processes and agents, including viral infections, autoimmune diseases, medications, vaccinations and dental restorative materials
• fifth or sixth decade, with 2/3 patients developing the disease between the ages of 30 and 60 years
• Variants- Bullous, atrophic,
hypertrophic,
Ulcerative/Erosive, Inverse,
Linear, Annular, Lichen
planopilaris
• Assoc w/hep c more with oral
LP
• VirusesHSV,Varicella,
HHV6, Hep C
• VaccineHep B
• Drugs
• Contact allergensnickel(ID), amalgem
• Neoplasms

Lichen Planus
• Flexor surfaces
• Wickham striae
• small, polygonal-shaped,
violaceous, flat-topped papule;
some papules are umbilicated
• slightly shiny
• Pruritic
• Koebner phenomenon

QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

Lichen Planus
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

Lichen Planus
• Dx made via clinical features and bx
• DDX
– lupus erythematosus (LE), lichen nitidus, lichen striatus, lichen
sclerosus, pityriasis rosea, erythema dyschromicum perstans
(ashy dermatosis), psoriasis, annular lichenoid eruption,
lichenoid GVHD and secondary syphilis
• Tx
– TSC(superpotent), Topical calcineurin inhibitors, Intralesional
corticosteroids, Intramuscular triamcinolone acetonide [0.5-1
mg/kg/month X 3-6 months], Phototherapy, Oral metronidazole,
Antimalarials, Systemic retinoids

PITYRIASIS ROSEA
• healthy adolescents and young adults
• absence of significant systemic manifestations & spontaneous resolution provides great consolation to the patient
• ages of 10 and 35 years
• no racial predilection
• eruption lasts 6 to 8 weeks
• cause of pityriasis rosea remains elusive-(HHV-7)
• herald patch is a skin- to pink- to salmon-colored patch or plaque with a slightly raised advancing margin
PITYRIASIS ROSEA
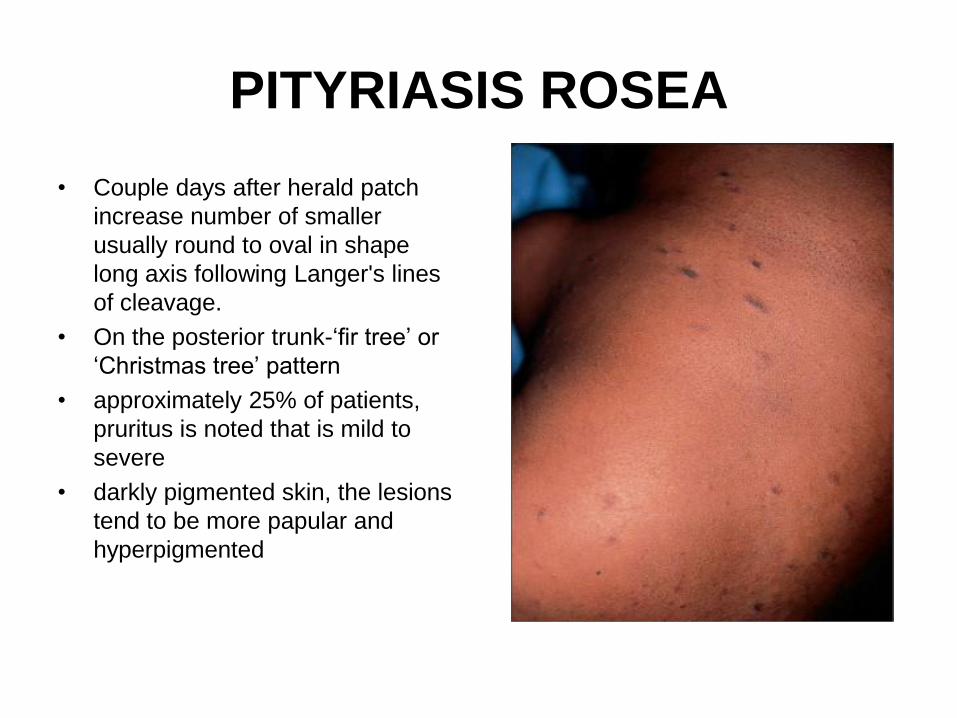
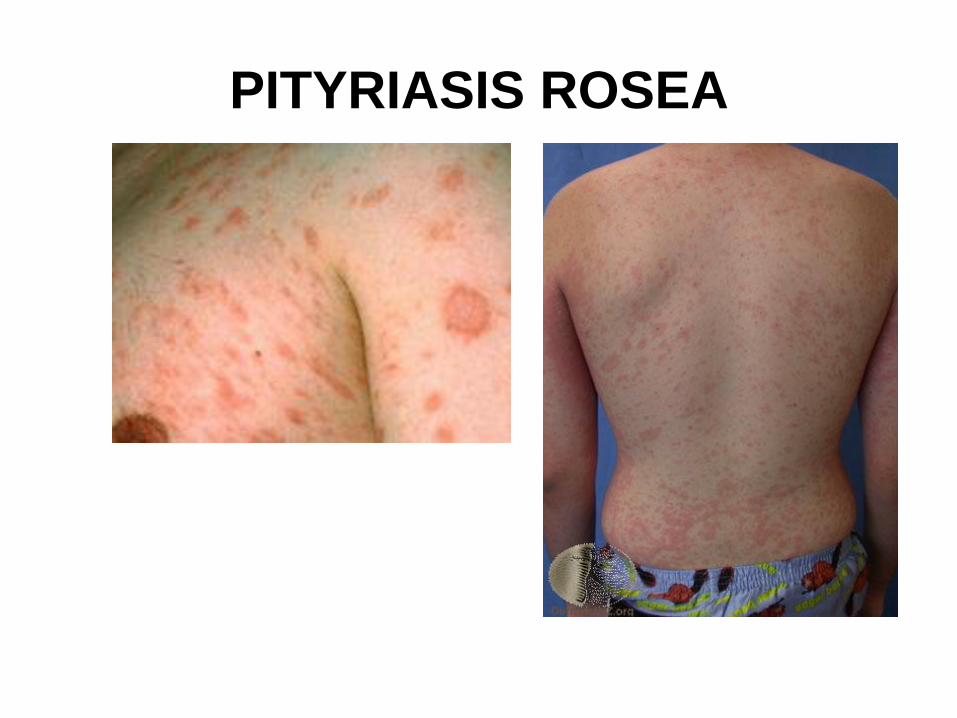
• Couple days after herald patch
increase number of smaller
usually round to oval in shape
long axis following Langer's lines
of cleavage.
• On the posterior trunk-„fir tree‟ or
„Christmas tree‟ pattern
• approximately 25% of patients,
pruritus is noted that is mild to
severe
• darkly pigmented skin, the lesions
tend to be more papular and
hyperpigmented
PITYRIASIS ROSEA
• clinical picture is quite characteristic and the histopathology
relatively non-specific.
• DDX-secondary syphilis, drug eruptions, tinea corporis, nummular
eczema, guttate psoriasis
• Tx- patient education and reassurance, low- to medium-strength
topical corticosteroids, UVB light treatments or natural sunlight
exposure and oral antihistamines 73% of patients had complete
resolution after receiving 14 days of erythromycin
Psoriasis
• The impact of psoriasis on quality of life is significant given its
chronicity and prevalence (up to 2% worlds population)
• US and Canada, prevalences as high as 4.6%
• Africans, African-Americans, Norwegian Lapps, and Asians of
between 0.4% and 0.7%
• Psoriatic arthritis probably occurs in 5-30% of the patients
• skin lesions appear well before the psoriatic arthritis
• peaks in age of onset-one at 20-30 years of age and at 50-60 years.
In approximately 75% of patients-before the age of 40 years
• positive family history has been reported by 35% to 90%
• Obesity, increased alcohol consumption, and an increased
incidence of smoking have all been associated with psoriasis

Psoriasis
• associated with several: HLA-B13,
HLA-B17, HLA-B37 and HLA-
Bw16
• Triggers
– cutaneous injury-Koebner
phenomenon, sunburn, viral
exanthems, 2-6wk lag
– psychogenic stress
– HIV (greater dz severity)
– strep pharyngitis guttate
(1-2wk lag)
– hypocalcemia pustular
psoriasis
• Triggers
– Drugs
– steroid withdrawal
– -blockers
– Lithium
– IFN
– Terbinafine
– ACE-I
– Antimalarials
– NSAIDs
– GCSF
– Rapid tapers of corticosteroid

Psoriasis
• symmetric distribution of
sharply defined erythematous
scaly plaques
• scalp, elbows, knees and
presacrum predilection, as are
the hands and feet, genitalia
are involved in up to 30%.
Plaques may persist for
months to years at the same
locations

Psoriasis

Psoriasis
• Guttate psoriasis-2% of the
patients, common form of the
disease in children, preceding
severe upper respiratory
infection,
Psoriasis
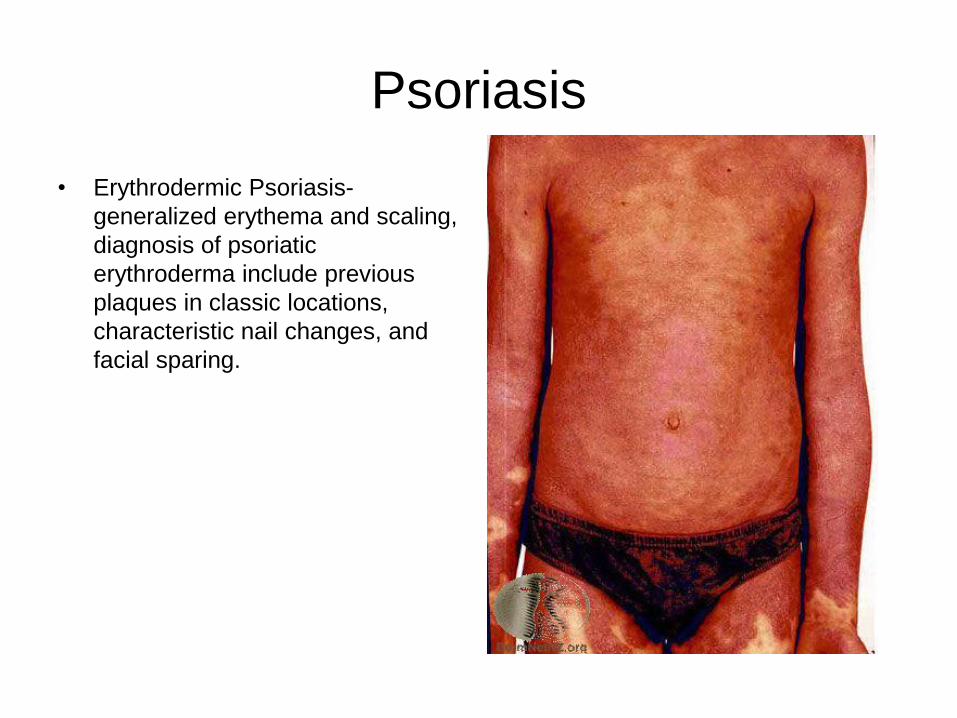
• Erythrodermic Psoriasis-
generalized erythema and scaling,
diagnosis of psoriatic
erythroderma include previous
plaques in classic locations,
characteristic nail changes, and
facial sparing.

Psoriasis
• pustular psoriasis-erythema and
the appearance of sterile pustules
dominate clinical picture,
• triggering factors-pregnancy, rapid
tapering of corticosteroids (or
other systemic therapies),
hypocalcemia, infections, in case
of localized disease, topical
irritants

Psoriasis
• Pustulosis of the palms and soles-
sterile‟ pustules of the
palmoplantar surfaces admixed
with yellow–brown macules scaly
erythematous plaques may also
be seen
• commonly associated with sterile
inflammatory bone lesions

Psoriasis
• Acrodermatitis continua of
Hallopeau- rare manifestation,
pustules are seen on the distal
portions of the fingers, nail bed
shedding of nail plates
Psoriasis

Psoriasis
• DDX-mycosis fungoides variant of cutaneous T-cell lymphoma (CTCL) keratotic eczema of the palms and soles pityriasis rubra pilaris drug reactions intertrigo seborrheic dermatitis, cutaneous candidiasis, tinea incognito
• Clinical picture and bx to confirm dx
• Tx-
– Vitamin D3 Analogues-inhibits epidermal proliferation, (Dovonex, Vectical), max app 100g/week, CI-Abnormality in bone or calcium metabolism, Renal insufficiency, Allergy Pregnancy, lactation

Psoriasis
• TCS- first-line therapy in mild to moderate psoriasis • Indications-
– Mild to moderate psoriasis: first-line treatment as monotherapy or in combination
– Severe psoriasis: often in combination with a vitamin D3 analogue, topical retinoid, anthralin or tar
– Monotherapy for flexural and facial psoriasis (usually mild strength
– Recalcitrant plaques often require occlusion (plastic, hydrocolloid
• CI-
– Bacterial, viral and mycotic infection
– Atrophy of the skin
– Allergic contact dermatitis due to corticosteroids or constituents of the formulation
– Pregnancy or lactation
• 80% of patients treated with high-potency topical corticosteroids experience clearance
• Combination topical therapy

Psoriasis
• Anthralin
– inhibits mitogen-induced T-lymphocyte proliferation and neutrophil chemotaxis
– treatment in an inpatient setting or day-care center
– Indications-second-line treatment as monotherapy or in combination
– CI-Unstable plaque psoriasis in a phase of progression, pustular and erythrodermic psr
• Topical Retinoids: tazarotene (Tazorac)
– second-line treatment as monotherapy
– Selectively binds RAR-beta and RAR-gamma
– epidermal proliferation, inhibits transglutaminase and K16 expression
– max BSA = 10-20%
– CI-Unstable plaque psoriasis, Erythrodermic psoriasis, Allergic contact dermatitis, Pregnancy and lactation

Psoriasis
• Photo(chemo)therapy
– BB or NB UVB(311nm), UVA oral or topical psoralen
– Mod-Severe: first line
– CI-Insufficient efficacy of UVB and PUVA• Pustular psoriasis (UVB and PUVA)• Erythrodermic psoriasis (UVB and PUVA)• Light-sensitive dermatoses (UVB and PUVA)• Photodermatoses (UVB and PUVA)• Phototoxic systemic or topical medications (UVB and PUVA)• Vitiligo (UVB and PUVA)
• Previous history of arsenic exposure, excessive irradiation or excessive photo(chemo)therapy (UVB and PUVA)
• Excessive exposure to UV light• Previous cumulative PUVA therapy >2000 J/cm2• Immunosuppressive medication• Previous history of skin cancer (UVB and PUVA)• Men and women in reproductive years without contraception (PUVA)• Pregnancy and lactation (PUVA)• Liver and kidney impairment (PUVA)• Cataracts (PUVA)
I-

PsoriasisSYSTEMICS
• Methotrexate
– Severe chronic(>20 BSA), pustular, erythrodermic, psoriatic arthritis, Severe nail psr
– lymphocyte effect
– max effect = 8-12wk
– CI-kidney function (creat cl <60 ml/min), Concomitant medications, pregnancy and lactation, planning to have children liver function abnormalities, hepatitis, severe anemia, leukopenia, thrombocytopenia, active infections Peptic ulcer (active) unreliable patient
– AE: liver tox, pancytopenia
• Cyclosporine
– Severe, failed conv tx
– rapid clearance
– blocks IL2 upregulation
– CI-Impaired renal function, Uncontrolled hypertension,Past or present malignancy, Concomitant immunosuppressive therapy, drugs affecting cyclosporine pharmacokinetics, history of arsenic exposure, history of excessive photo(chemo)therapy, Concurrent photo(chemo)therapy, Active infections, Pregnancy or lactation, immunodeficiency, Severe chronic organ dysfunction Non-compliance, Alcohol and drug abuse
– AE: HTN, renal tox

Psoriasis
• Acitretin
– Severe monotherapy
– pustular, erythrodermic
– CI-liver/kidney dysfxn, Pregnancy and lactation Women of
childbearing potential who cannot guarantee adequate
contraception during and up to 3 years following discontinuation
of acitretin, hyperlipidemia, especially hypertriglyceridemia,
concomitant medications and hepatotoxic meds,diabetes
mellitus, alcohol abuse
– AE: hyperlipidemia, liver tox

Psoriasis
BIOLOGICS
• T-cell activation inhibitors(Alefacept)
• TNF- inhibitors(Etanercept, Infliximab, Adalimumab)
• CI-Significant viral, bacterial or fungal infections,Increased risk for developing sepsis, Active tuberculosis Immunocompromised or immunosuppressed, Pregnancy* (anti-TNF agents are category B, efalizumab is category C, alefacept is category B), Allergic reaction to the biologic agent, Excessive chronic exposure to UVR or photo(chemo)therapy
• AE: immunosuppresion
– Etanercept AE: demyelinating dz, lupus-like syndrome
– Adalimumab AE: thrombocytopenia
– Infiximab CI in CHF

EM/SJS/TEN
• Erythema Multiforme (rarely caused by drugs) is a distinct disease from Stevens-Johnsons Syndrome / Toxic Epidermal Necrolysis (caused by drug)
• EM does not commonly progress to SJS/TEN
• SJS and TEN same fatal disease spectrum
• Skin is major target organ for many drug reactions
• Drug reactions usually 7-21 days after drug exposure, not next day typically
• It is often very difficult to identify the exact drug causing the reaction

Erythema Multiforme
• acute, self-limited,
• abrupt onset of symmetrical fixed red
papules,
• typical and/or occasionally „atypical‟
papular target lesions
• precipitated by an infection, particularly
HSV
• Minor-ext, face, mild to no mucosal, no
systemic sx
• Major-ext, face, severe mucosal,
systemic sx
– fever and asthenia(weakness) of
varying degrees, arthralgias w/
joint swelling, pulmonary. Renal,
hepatic and hematologic
abnormalities-rare
• Pathogensis
– Infection(90%)
• HSV 1,2
• Mycoplasma Pneumoniae
• Histoplasma Capsulatum
• Drugs <10%
• Exposures (poison ivy)
• Systemic disease (rare)(IBD,
LE/Rowell‟s
syndrome,Bechets)



Erythema Multiforme
• Painful mucosal erosions – usually
absent in EM minor
• Natural History
– Abrupt 24-72 hours
– 50% preceded by herpes
labalis 3-14 days
– Last up to 2 weeks
• Recurrences quite common
when?
– Each spring

Erythema Multiforme

Erythema Multiforme
Erythema Multiforme
• DDX-Urticaria, fixed drug
eruptions subacute cutaneous LE,
erythema annulare centrifugum,
and several forms of vasculitis
• Dx-skin bx, good H&P,
• Tx-topical antiseptics for eroded
skin lesions and
antiseptic/antihistamine rinses and
local anesthetic solutions for oral
lesions
– Tx underlying cause-bacterial
vs viral
– HSV-associated EM- acyclovir (10
mg/kg/day in divided doses)
valacyclovir (500-1000 mg/day)
famciclovir (250 mg twice daily)
systemic corticosteroids (e.g.
prednisone [0.5–1 mg/kg/day]) or
pulse methylprednisolone [1
mg/kg/day for 3 days]) should be
considered, despite the absence
of controlled studies
– azathioprine (100 mg/day for
several months), prednisone (0.5
mg/kg/day for several months),
thalidomide, dapsone,
cyclosporine, mycophenolate
mofetil and PUVA(no controlled
trials

Stevens-Johnson Syndrome (SJS)
Toxic epidermal necrolysis (TEN)
• Rare, acute and life-threatening mucocutaneous diseases that are
almost always drug-related
• unpredictable course
• annual incidence of 1.2-6 and 0.4-1.2 per million persons
• TEN affects women more frequently than men, with a ratio of 1.5:1,
and the incidence increases with age
• Patient groups particularly at risk
– AIDS (1000x greater risk!)
– Slow acetylator genotypes
– Immunocompromised (HIV, lymphoma)
– Brain tumor patients undergoing radiotherapy and concomitantly
receiving antiepileptics
Stevens-Johnson Syndrome (SJS)
Toxic epidermal necrolysis (TEN)
• mortality rates
– 25% to 50%-TEN
– 5% for patients-SJS
• Pathogensis
– Massive Keratinocyte Apoptosis
– Overwhelms phagocytes‟ ability to eliminate apoptotic cells
• Drugs associated
– Allopurinol
– Aminopenicillins
– Amithiozone (thioacetazone)
– Antiretroviral drugs
– Barbiturates
– Carbamazepine
– Chlormezanone
– Phenytoin antiepileptics
– Lamotrigine
– Phenylbutazone
– Piroxicam
– Sulfadiazine
– Sulfadoxine
– Sulfasalazine
– Trimethoprim–sulfamethoxazole

Stevens-Johnson Syndrome (SJS)
Toxic epidermal necrolysis (TEN)
• SJS <10%
• TEN >30%
• Typical interval between the onset
of drug therapy and SJS/TEN is
between 1 and 3 weeks (2 months
for aromatic anticonvulsants)
• Epidermal detachment
• Initial sx-fever, stinging eyes, and
pain upon swallowing can precede
cutaneous 1-3 days
• Erythema and erosions of the
buccal, ocular and genital
mucosae are present in more than
90% of patients
Stevens-Johnson Syndrome (SJS)
Toxic epidermal necrolysis (TEN)
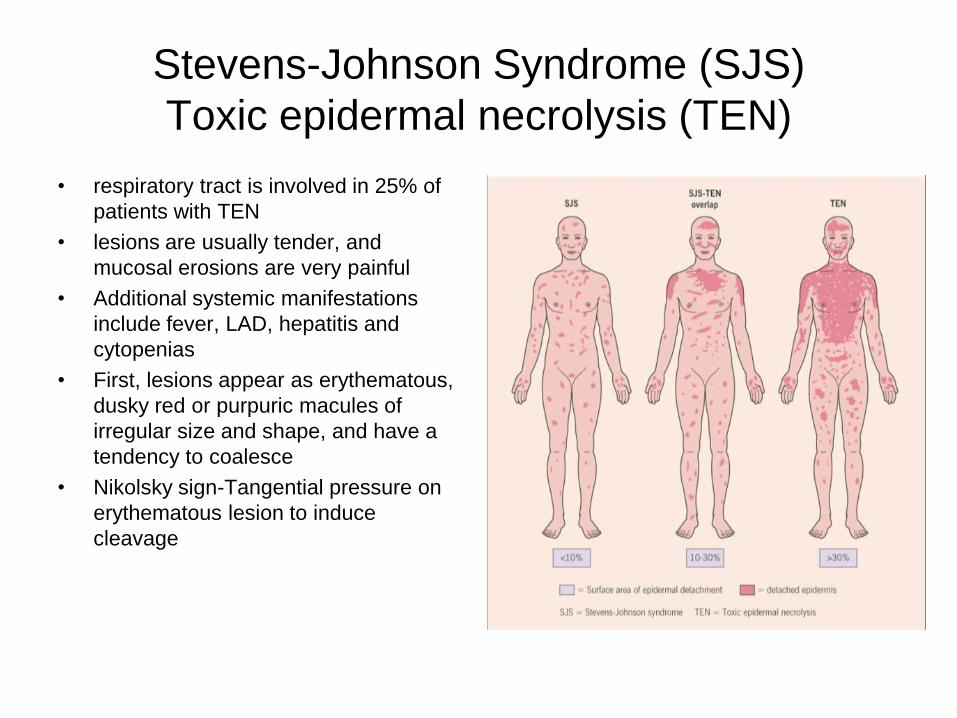
• respiratory tract is involved in 25% of
patients with TEN
• lesions are usually tender, and
mucosal erosions are very painful
• Additional systemic manifestations
include fever, LAD, hepatitis and
cytopenias
• First, lesions appear as erythematous,
dusky red or purpuric macules of
irregular size and shape, and have a
tendency to coalesce
• Nikolsky sign-Tangential pressure on
erythematous lesion to induce
cleavage

Stevens-Johnson Syndrome (SJS)
Toxic epidermal necrolysis (TEN)
Stevens-Johnson Syndrome (SJS)
Toxic epidermal necrolysis (TEN)
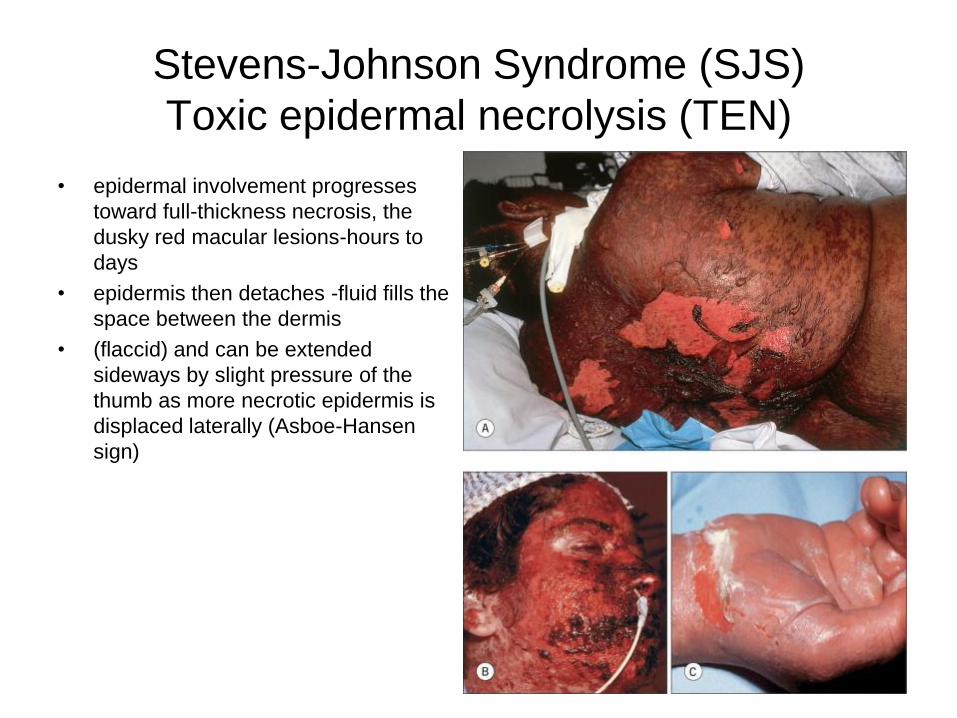
• epidermal involvement progresses
toward full-thickness necrosis, the
dusky red macular lesions-hours to
days
• epidermis then detaches -fluid fills the
space between the dermis
• (flaccid) and can be extended
sideways by slight pressure of the
thumb as more necrotic epidermis is
displaced laterally (Asboe-Hansen
sign)

Stevens-Johnson Syndrome (SJS)
Toxic epidermal necrolysis (TEN)
• SCORTEN
• 1 point for ?
– Age >40
– Heart rate >120
– Malignancy
– BSA above 10%
– Serum Urea >10 mmol/l
– Serum Bicarbonate <20
mmol/l
– Serum glucose > 14mmol/l
• Mortality rate
– 0-1 - 3.2%
– 2 - 12.1%
– 3 - 35.8%
– 4 - 58.3%
– >5 - 90%

Stevens-Johnson Syndrome (SJS)
Toxic epidermal necrolysis (TEN)
• DDX-EM. SSSS, AGEP and
generalized fixed drug eruption,
Paraneoplastic pemphigus, drug-
induced linear IgA bullous dermatosis
(LABD), Kawasaki disease, LE, and
severe acute GVHD
• Tx
– early diagnosis,
– Discontinue all meds
– Protect against hypovolemia,
electrolyte imbalance, renal
insufficiency and sepsis
– Burn care/ ICU
– Careful manipulation
– Vaseline gauze on denuded areas
– Regular eye exam by optho
– Periodic cultures of eyes, sputum,
drainage
– Steroid efficacy controversial
– IVIg 1g/kg/day x 3 - 4 days

Stevens-Johnson Syndrome (SJS)
Toxic epidermal necrolysis (TEN)

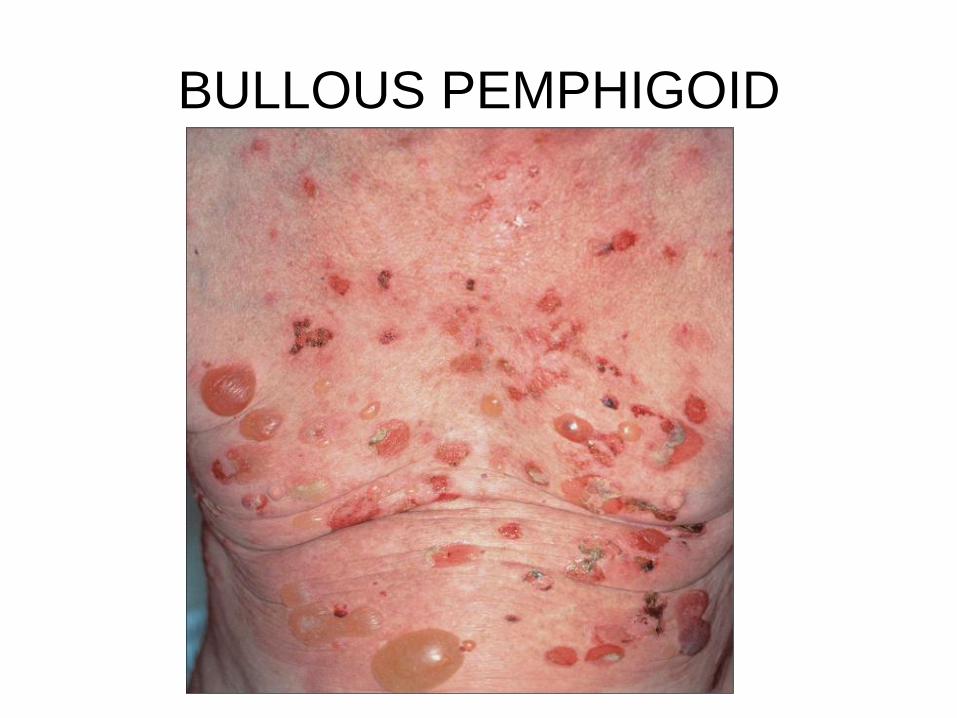
BULLOUS PEMPHIGOID
• most common autoimmune subepidermal blistering disease, and it
predominantly affects the elderly
• after 60 years of age
• patients over 90 years of age appears to be about 300-fold higher
• higher predominance in men
• immune-mediated disease-self-antigens: the BP antigen 180
(BP180, BPAG2 or type XVII collagen) and the BP antigen 230
(BP230 or BPAG1)
• Manifestations extremely polymorphic(bullous vs nonbullous)
BULLOUS PEMPHIGOID
• Nonbullous-non-specific mild to severe pruritus w/o excoriated, eczematous, papular and/or urticarial lesions that may persist for several weeks or months
• Bullous-vesicles and bullae on apparently normal or erythematous, annular or figurate pattern blisters are tense, up to 1–4 cm leaving eroded and crusted areas,
• Symmetrical distribution pattern, and they predominate on the flexural aspects of the limbs and the lower trunk, including the abdomen. Within intertriginous zones, vegetating plaques can be observed.
• increased risk of malignancy in patients with BP appeared to be marginal-ca screening correlate w/ sx
• Triggers-trauma, burns, radiotherapy or UV irradiation
• Assoc w/ psr & LP
BULLOUS PEMPHIGOID

BULLOUS PEMPHIGOID

BULLOUS PEMPHIGOID

BULLOUS PEMPHIGOID
• Drug Induced BP
– Diuretics (e.g. furosemide,
bumetanide)
– Analgesics (e.g.
phenacetin)
– D-penicillamine
– Antibiotics (e.g. amoxicillin,
ciprofloxacin)
– Potassium iodide
– Gold
– Captopril
• Dx & DDx
– Clinical
– Histo, IIF, DIF
– DIF-fine, linear, continuous
deposits of IgG and/or C3
along the epidermal
basement membrane
– EBA, LABD, CP,drug
reactions, contact
dermatitis, prurigo
nodularis, urticarial
dermatitis, vasculitis,
arthropod, scabies

BULLOUS PEMPHIGOID
• Tx-Mild and/or localized
disease
– Superpotent TCS
– Nicotinamide in association
w/ minocycline or
tetracycline
– Erythromycin, penicillins
– Dapsone, sulfonamides
– Topical immunomodulators
(e.g. tacrolimus)
• Tx-extensive/persistent
disease
– Superpotent TCS
– Oral corticosteroids
– Azathioprine
– Mycophenolate mofetil
– MTX
– Chlorambucil
– Cyclophosphamide
– IVIg
– Plasma exchange
– Rituximab

Acne Vulgaris
• disorder of the pilosebaceous unit
• primarily a disorder of adolescence(85% btw between 12 & 24 y/o)
• sebaceous gland is controlled primarily by hormonal stimulation
– High in 1st 6 mos
– Decreases at 1yr + stabilizes
– Dramatically increases at adrenarche, correlating w/androgen
production and acne
– Stable in adulthood
– Decreases in women at menopause and men in 6th and 7th
decade
• Propionibacterium acnes contributes significantly to the production
of acne- Gram-positive, non-motile rods

Acne Vulgaris
• Sticky corneocytes proliferate in infrainfundibulum
• Comedone expands, sebaceous lobule regresses
• Pressure increases, comedo ruptures, keratin and sebum are
extruded
• Inflammation ensues
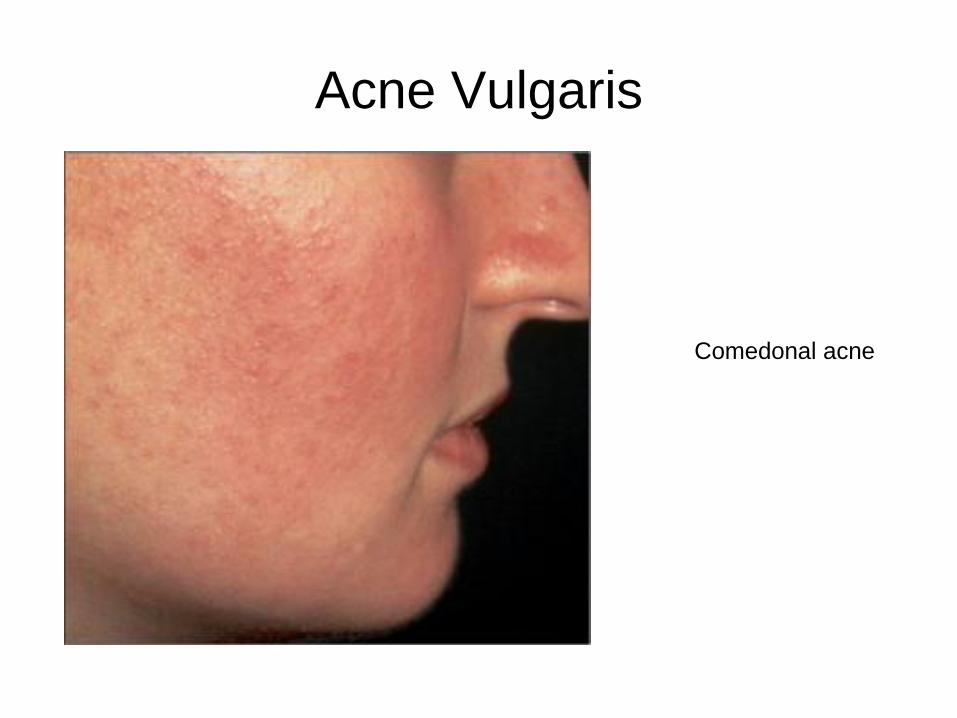
Acne Vulgaris
Comedonal acne

Acne Vulgaris
Closed comedones
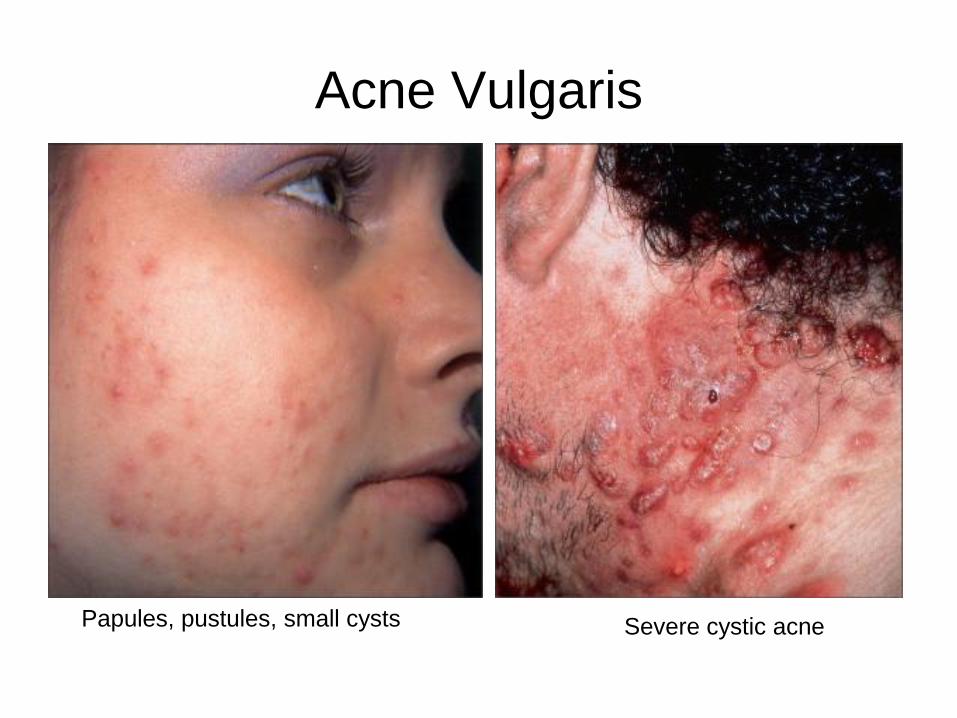
Acne Vulgaris
Papules, pustules, small cysts Severe cystic acne
Acne Vulgaris
• papules, pustules, nodules and cysts of varying severity
• lesions progresses, nodules form and become markedly inflamed, indurated and tender
• severe nodulocystic acne, these lesions frequently coalesce to form massively inflamed complex plaques that can include sinus tracts.
• DDX-– Milia
– Sebaceous hyperplasia
– Eruptive vellus hair cysts
– Steatocystoma multiplex
– Corticosteroids and anabolic steroid induced
– Contact acne
– Follicular mucinosis
– Rosacea
– Folliculitis
– Keratosis Pilaris
• Not an exhaustive list

Acne Vulgaris
• Tx-Mild comdonal
– 1st line-Topical retinoid(adaplene, tretinoin, tazarotene)
– 2nd line-azelaic acid, salicyclic acid
• Tx-Mild papular/pustular
– 1st line-Topical retinoid(adaplene, tretinoin, tazarotene) and topical antibiotic
– 2nd line-add azelaic or salicyclic acid
• Tx-Mod papular pustular nodules
– 1st line-oral antibiotic, topical retinoid, BPO, isotretinoin(only if multi nodules/recalcitrant)
– 2nd line-alt oral anitbiotic, azelaic or sal acid
• Tx-Severe
– 1st line-isotretinoin w/wo oral prednisone, intralesional corticosteroid
– 2nd line-oral dapsone

Acne Vulgaris
• Tx-multi tx modalities, compliance is an issue with multi product!
• Isotretinoin / Accutane ( 5 - 6 months) Last Resort
– Sebaceous gland atrophy, P. acnes unable to thrive,
– Normalization of follicular keratinization
– 1 mg/kg/d for total of 120-150 mg/kg to prevent relapse
– S/E-Xerosis, dry eyes + lips, bloody nose, alopecia, headaches, myalgias pseudotumor cerebri (N/V, blurred vision) cutaneous Infections (S. aureus), lab Abnormalities (lipids, LFTs, leukopenia) psych (Mood swings, but no increase in suicidality), skeletal hyperostoses, poor wound healing, exuberant granulation tissue**Teratogenicity ( 2 Forms of BC)
• other tx
– Extraction, blue light, laser, etc

Rosacea
• common in fair-skinned individuals
• Incidence third and fourth decades of life
• vascular hyperreactivity
• Blushing, gradual reddening
• Foods/liquids induce facial vasodilation
• increased incidence Parkinson's
• Demodex folliculorum-mite w/in sebaceous follicles of the head that
has been implicated as a cause of rosacea for decades, but the
evidence is largely circumstantial
• Propionibacterium acnes probably plays a role
• oral niacin worsens
• Topical steroids

Rosacea
• Four types-erythematotelangiectatic (vascular), papulopustular
(inflammatory), phymatous and ocular
• Erythematotelangiectatic(vascular)-Flushing and persistent central
facial erythema with or without telangiectasia.
• Papulopustular-Persistent central facial erythema with transient
papules and/or pustules
• Phymatous-Thickening skin, irregular surface nodularities and
enlargement(nose, chin, forehead, cheeks or ears)
• Ocular- Foreign body sensation in the eye, burning or stinging,
dryness, itching, ocular photosensitivity, blurred vision,
telangiectasia of the sclera or other parts of the eye, or periorbital
edema

Rosacea
Vascular type

Rosacea
Inflammatory rosacea

Rosacea
Rhinophyma Phymatous & inflammatory

Rosacea
Occular
Rosacea
• Dx-clinical, bx only severe
persistent cases
• DDX-perioral derm,
granulomatous rosacea,
pyoderma faciale, steroid
rosacea, Seb derm, Acne,
Erythromelanosis Faciei and
Keratosis Pilaris Rubra, Lupus
Erythematosus, Lupus Miliaris
Disseminatus Faciei, Demodex
• Tx-topical
– Metronidazole-topical therapy
daily to BID
– Azelaic acid cream
– BPO if not too irritating, topical
anitbiotics not very effictive,
– topical tretinoin
– Sulfa based face washes
• Tx-oral
– Tetracyclines-anti-inflammatory
– Isotretionoin-severe cases
• Tx-surgical
– IPL or PDL
– electrosurgery
– CO2 laser

Folliculitis
• very common disorder
• Culture contents often fails to
identify a bacterial pathogen
• Staphylococcus aureus is the
most common
• Perifollicular pustules, arising
on an erythematous base
• pierced by a hair
• Tender,painful, pruritic
• Neck,scalp, beard area, upper
trunk, buttocks and
thighs,axillae and groin
• Areas of terminal hair
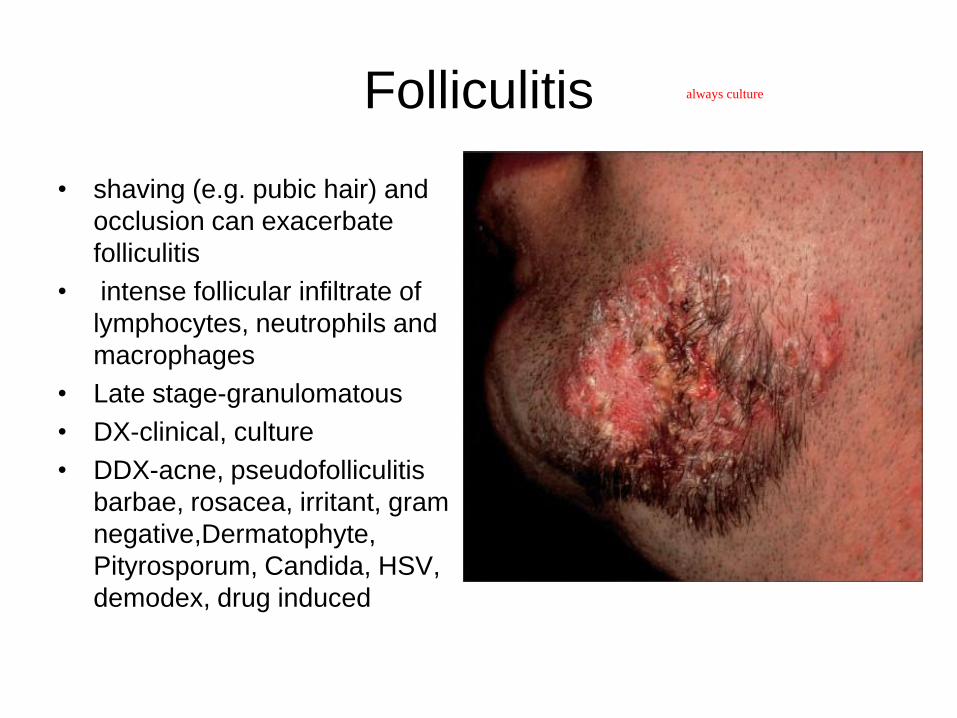
Folliculitis
• shaving (e.g. pubic hair) and
occlusion can exacerbate
folliculitis
• intense follicular infiltrate of
lymphocytes, neutrophils and
macrophages
• Late stage-granulomatous
• DX-clinical, culture
• DDX-acne, pseudofolliculitis
barbae, rosacea, irritant, gram
negative,Dermatophyte,
Pityrosporum, Candida, HSV,
demodex, drug induced
•
always culture

Folliculitis
• Tx-cx dependent, for cx negative/acne-BPO, topical clinda, oral tetracycline
• Irritant-d/c agent, tcs-midpotency
• Gram neg(klebsiella/enterbacter)-topical gent/BPO, quinolones (e.g.
ciprofloxacin)
– Hot tub(p.aeruginosa)-self-limited, severe or immunocompromised host:
ciprofloxacin, 500 mg po bid for 7–14 days Water(chlorine (0.4–1.0
ppm, pH 7.2–7.4) and changed every 6–8 weeks)
• Dermatophyte/PityrosporumCandida-topical or oral antifungals
• HSV-Acyclovir 200 mg po 5 times per day for 5–10 days,
Famciclovir 500 mg po tid for 5–10 days, Valacyclovir 500 mg po tid for 5–
10 days
• Demodex- 5% permethrin cream

SEBORRHEIC KERATOSIS
• common benign, more common in
Caucasian populations and to affect
men and women with equal incidence
• begin to appear during the fourth
decade of life
• sun exposure implicated
• solitary or multiple, tan to black,
macular, papular or verrucous lesions
• waxy , velvety or verrucous, „stuck-on‟
appearance
• occur anywhere except mucous
membranes, palms and soles
• very rare sign of Leser–Trélat-abrupt
increase size and number(internal
malignancygastric or colonic
adenocarcinoma, breast ca,
lymphoma)
waxy
stuck-on

SEBORRHEIC KERATOSIS
• SCC, cutaneous melanoma, BCC, KA, and SCC in situ have been associated w/SKs-represents a coincidental neoplasm developing in adjacent skin
• Dx-clinial appearance, possible bx
• DDx-dermatosis papulosa nigra, stucco keratoses,inverted follicular keratoses, acrochordon, verruca vulgaris, condyloma acuminatum, acrokeratosis verruciformis, tumor of the follicular infundibulum, eccrine poroma, Bowen's disease, SCC, solar lentigo, melanocytic nevus and melanoma
• Tx-asx(cosm only), Sx-destruction(LN2, curettage)
biopsy it
asymptomatic
Actinic Keratosis
• AKs are most often found in fair-skinned individuals
• accounted for 3 million annual visits to dermatologists in the US during the early 1990s
• 80% of AKs occur on the head, neck and upper extremities (dorsal hands and forearms),more often in individuals w/ prior history, increasing age, men. AKs are also markers for an increased risk for developing invasive NMSC(SCC)/(BCC)
• resistance to UV-induced keratinocyte apoptosis-contributes to pathogenisis(much more extensive…carcinogensis, cell cy s, oncogenes, tumor suppersor genes) p53 protein is a key factor for integrating pathways regulating DNA synthesis, DNA repair and apoptosis.
• Prolonged UV exposure/intense UV expousre holiday

Actinic Keratosis
• number of mutations in a cell increases with time and partially
explains the increasing risk for acquiring cancer as we age
• inactivation of p53 facilitates angiogenesis-essential for tumor mass
expansion
• „precancerous‟ or „premalignant‟ because the aty pical keratinocy
within these lesions are confined to the epidermis
• Environmental risk factors- Cumulative/occupational sun exposure,
Intermittent/recreational sun exposure, PUVA, tanning beds,Ionizing
radiation,chemicals (arsenic), human papillomavirus, cigarette
smoking

Actinic Keratosis
• Risk factors-
– Fair skin, always burn, never tan, freckling, red hair, light eye
color
– Genetic syndromes-rare
– Chronic non-healing wounds, longstanding DLE, LP, nevus
sebaceous
– Organ TPLT, chronic lymphocytic leukemia treated with
fludarabine, AIDS patients with HPV infection
Lupus on skin only

Actinic Keratosis
• likelihood of an invasive SCC evolving from a given AK has been
estimated to occur at a rate of 0.075-0.096% per lesion per year
• sun-damaged skin of the head, neck, upper trunk and extremities
may report tenderness
• rough erythematous papule with white to yellow scale
• Advanced lesions thicker and well defined w/hyperkeratosis and
erythema,in areas of highest sun exposure(ears,forehead, nasal
bridge, malar eminences, dorsal hands, extensor forearms,scalp in
bald individuals)

Actinic Keratosispale, papule
flaky

Actinic Keratosis

Actinic Keratosis
• Dx-clinical and histo
• DDX-SCCis, SCC, maybe sk
• Tx-Cyrotherapy, 5-FU, imiqiumod 5%,
topical diclofenac, Photodynamic therapy
ear, lip, nose so take biopsy tell about scars
in situ
It will make them red and ugly for 2 wks
cutting blood supply w laser
SCC
• UV solar radiation is also a major etiologic factor
• UV radiation received over time
• „classic cancer‟, as it has precursor lesions, tumor progression and the potential to develop metastatic disease
• metastases is infrequent (less than 5%)
• mucocutaneous interfaces(lips, genitalia and perianal area) more aggressive, higher risk of metastases
• The precise genetic events and number of mutations required for malignant transformation are unknown
• actinic keratoses and Bowen's disease-precursor-slight to severe dysplasia
• Alterations in the p53 gene are the most common genetic abnormalities
• Lip-30% risk of developing metastasis regional lymph nodes, but distant hematogenous spread can also be observed
SCC
• incidence of SCC has been rising worldwide in all age groups over
the last several decades at an estimated 3-10% per year
• Same risk factors apply to AK‟s
• Men have a 3:1 greater SCC mortality rate compared to women
• described as keratotic, pink, erythematous
patch/plaque/nodule/papule
biopsy

SCCis (aka Bowen‟s Disease)superficial squamos cells

Bowenoid Papulosis(SCCis in
genital warts)

SCC(Marjolin‟s Ulcer (scars)
Verrucous Carcinoma

SCC
High-risk sites include the lip and ear

Keratoacanthomatype of squamos cell rapid growth 1 month
Volcanic in appearance

SCC
• Dx-clinical and histo
• DDX-BCC, atypical
fibroxanthoma,
neuroendocrine carcinoma,
amelanotic melanoma,
adnexal tumors, prurigo
nodularis, verruca and irritated
seborrheic keratosis.
• Tx-Standard exc
– 6mm margins for SCC(high
risk lesions)
– 10% recurrence rate
• ED&C
– Cure rate 97-98% (smaller the
better)
• Curettage alone
– 96% cure rate (avoids
hypertrophic scar)
electrodissecation & curette

SCC
• Mohs Micrographic Surgery
– 1% recurrence rate over 5 years
– 5.6% recurrence in prior recurrent BCCs
– Preferred treatment in:
• Recurrent type
• Poorly delineated
• High-risk
• Incompletely removed BCC
• Sites of tissue conservation
• Need for reliable clear margins

SCC
• Radiation
– Use if surgery is contraindicated
– Disadvantages:
• Lack of margin control
• Poor cosmesis in some patients (scars worsen with time,
unlike surgery)
• Prolonged course of therapy
• Increased risk for future skin cancers
• High recurrence rates
BCC
• Sun exposure and anatomic site appear to be of etiologic
importance
• development of BCCs is restricted to skin containing pilosebaceous
units
• commonly develop on the face, and in particular on the nose,
suggests that anatomic site
• BCC appears to have a capacity for infinite growth and spontaneous
regression is not a feature
• virtually never develop metastases
• no known precursors (with the possible exception of p53 clones)
• BCC is the most common skin cancer in humans
• Men generally have higher rates of BCC than do women
BCC
• Women have a greater frequency of BCC on the lower extremities
while men have more ear lesions
• incidence of BCC is increasing
• increase with age and the median age at diagnosis is 68 years
• Mortality from BCC is quite rare and can occur in
immunocompromised patients
• metastatic BCC are more likely from tumors with aggressive
histologic patterns (morpheaform, infiltrating, metatypical,
basosquamous)
• Perineural space invasion an indicator of aggressive disease
• Metastases often involve regional lymph nodes, lungs, bone and
skin
• Risk factors similar to AK, SCC

BCC
• Variants of BCC include nodular, superficial, morpheaform, cystic,
basosquamous, micronodular, and fibroepithelioma of Pinkus
• 60% of all primary BCCs are nodular type presents as a raised,
translucent papule or nodule with telangiectasias, and has a
propensity for the face
• Superficial BCC commonly presents as an erythematous macule or
thin plaque, and it may be difficult to differentiate clinically from AK,
SCC in situ, or a benign inflammatory lesion appears on trunk and
extremities, the head and neck also may be affected
• Morpheaform BCC derives its name from an appearance similar to a
plaque of morphea/sclerosing presents as a flat, slightly atrophic
lesion, or as a plaque without well-demarcated borders, often
difficult to differentiate from a scar
pink pairly papule
BCC
• con‟t morpheaform-actual size of the cancer is often much greater
than the clinical extent of the tumor
• Cystic BCCs have a clear or blue–gray appearance and exude a
clear fluid if punctured or cut. If the lesion is in the periorbital area, it
may be confused with a hidrocystoma
• Basosquamous carcinoma (metatypical BCC) is a tumor that has
basaloid histologic features as well as eosinophilic squamoid
features of SCC, behave more like SCC more aggressive and
destructive likely to metz(9-10%) and reoccur after tx
• Micronodular basal cell carcinoma-very destructive, subclinial
spread, high reoccurence ratespresent as macules, papules, or
slightly elevated plaques and may be difficult to differentiate from
nodular BCC
BCC
• Fibroepithelioma of Pinkus rare variant presents as a pink plaque or
nodule smooth, may be pedunculated on the lower back difficult to
distinguish clinically from amelanotic melanoma
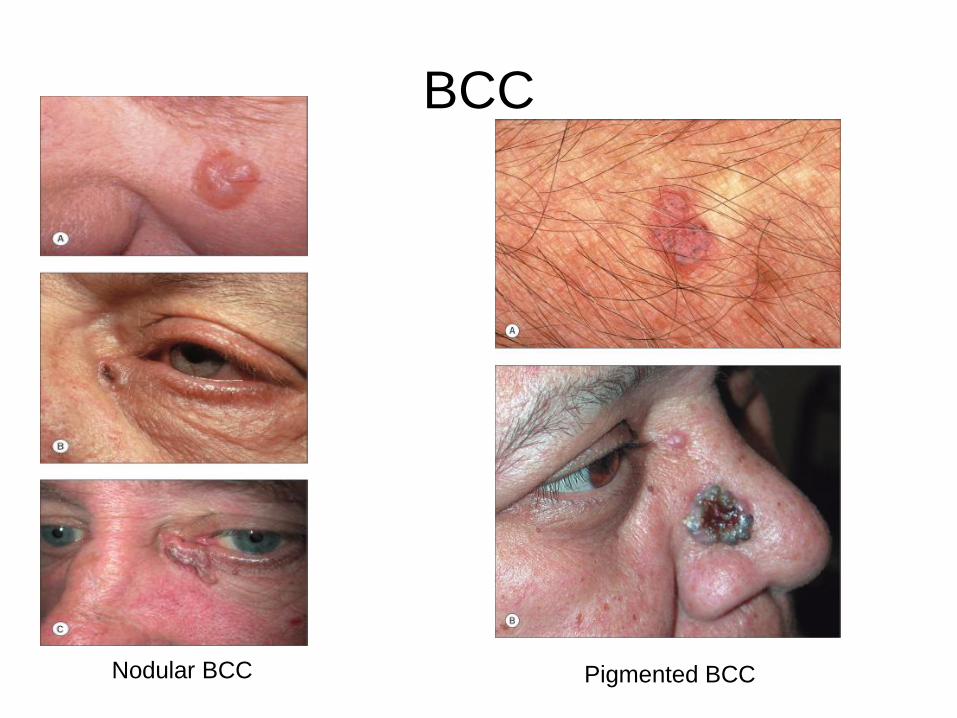
BCC
Nodular BCC Pigmented BCC

BCC
Superficial bcc
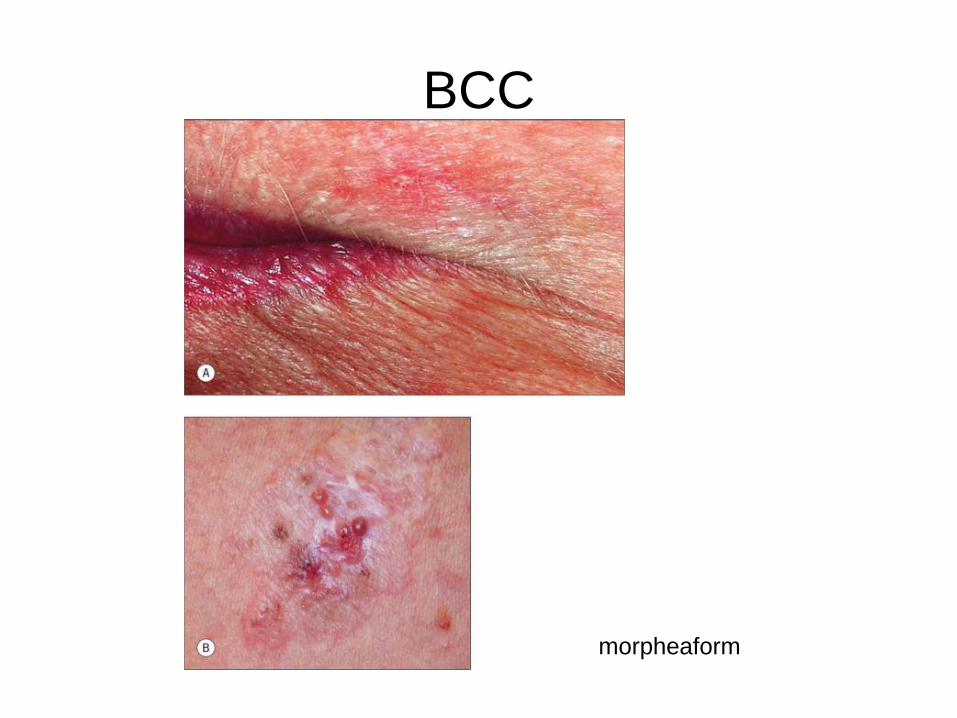
BCC
morpheaform
BCC
• Dx-clinical and histo
• DDX-AK, SCC(is), AMM, inflammed SK, hidrocystoma
• TX- Standard excision
– 4mm margins for BCC
– ED&C, Curettge alone, Mohs for high risk types and sites, XRT,
medical management, photodynamicaldera
radiation

Melanoma
• Melanoma is a malignancy arising from melanocytes-incidence and
overall mortality rates have been rising in recent decades
• most common forms of cancer in young adults,up to one-fifth of
patients develop metastatic disease, which usually is associated
with death
• Germline genetic mutations and polymorphisms can predispose
individuals to melanoma
• CDKN2A(gene locus)
• Immunogenic tumor(provokes immune response)- Halo nevi,Vitiligo-
like depigmentation,Higher rate of melanoma in immunosuppressed
pts
• melanoma incidence rate in Australia is the highest world-wide
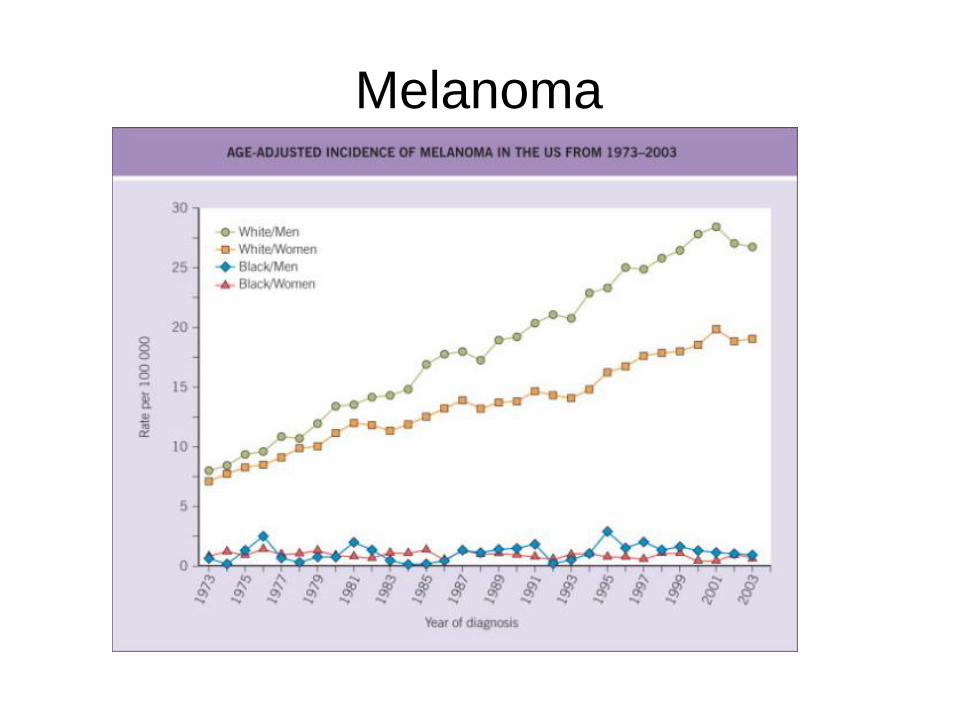
Melanoma
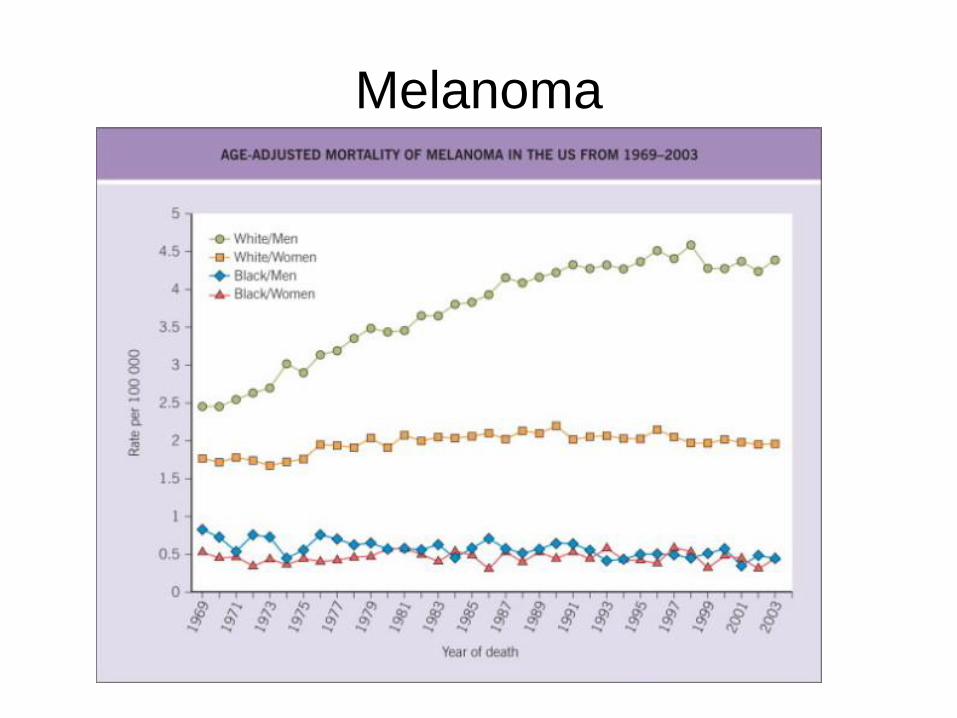
Melanoma
Melanoma
• Risk factors
– Genetic(Family history of atypical (dysplastic) nevi or melanoma,
lightly pigmented skin, tendency to burn, inability to tan, red hair
color, dNA repair defects (e.g. xeroderma pigmentosum))
– Environmental factors(Intense intermittent sun exposure,
sunburn, residence in equatorial latitudes)
– Phenotypic expressions of gene/environment
interactions(Melanocytic nevi: – Increased total number,
Multiple atypical (dysplastic), congenital (particularly large axial
lesions with multiple satellites), ephelides, personal history of
melanoma
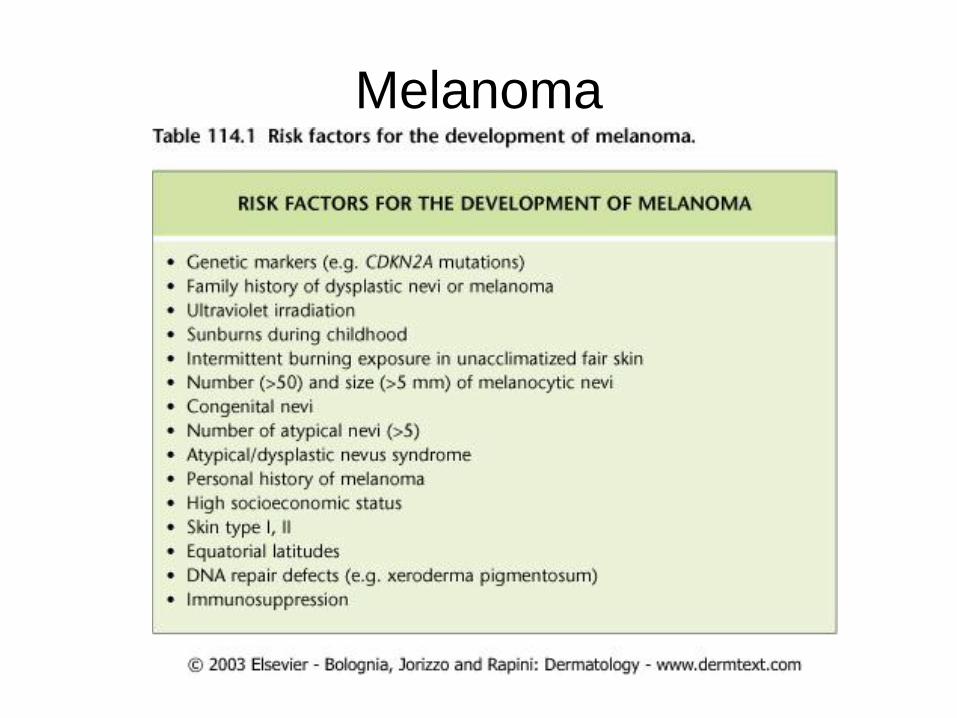
Melanoma
Melanoma
• Types
– Superficial spreading – 70%-Any site, preference for lower
extremities (women), trunk (men and women)-radial growth-More
pagetoid spread, less solar elastosis
– Nodular – 15-30%-Any site, preference for trunk, head, neck-no
radial growth-Nodule with more rapid vertical growth
– Lentigo maligna melanoma-5-15%-Face, especially nose and
cheeks-radial growth-Slower growth over years within sun-
damaged skin
– Acral lentiginous melanoma-5-10%-Palms, soles, nail unit-radial
growth-Most common melanoma type in patients with darker
skin types
men in their back

Melanoma
Superficial spreading melanoma
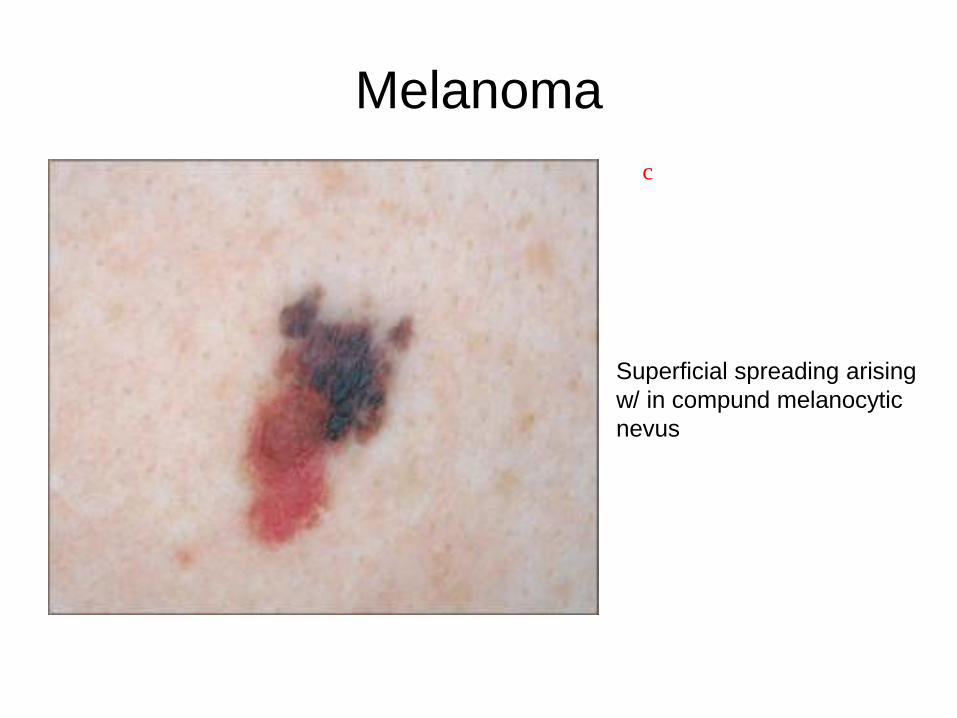
Melanoma
Superficial spreading arising
w/ in compund melanocytic
nevus
c

Melanoma
Nodular melanoma
no waxy appearance, no cystic look

Melanoma
Acral lentiginous melanoma Melanoma in situ of the nail
more common in AA

Melanoma
• Hutchinson sign-pigmentation of
the periungual tissues--is a
valuable clue to the diagnosis of
subungual melanoma

Melanoma
• Pregnancy
– Melanocyte-stimulating hormones elevated
– Darkening of nevi(more than 10% of women, 1st 3 months)
– Increased pigmentation
– Not a risk factor though
– Transplacental metastases can arise

Melanoma stagging system
how much to cut

Melanoma
• Dx-Early detection is a key factor
– history of change in the color, shape or size of a pigmented skin
lesion over the course of months is the most sensitive clinical
sign
– Public awareness campaign-ABCD's of melanoma: Asymmetry,
Border irregularity, Color variegation, and Diameter greater than
5 mm. These have recently been joined by ‟E' for „evolving‟ to
connote the importance of change as mentioned above
– BX!!!!
• DDX-Nevi, non-melanocytic stimulators
exsitional Bx

Melanoma
• DDX-melanocytic– Acral nevi
– Ancient nevi
– Black (hypermelanotic) nevi
– Blue nevi and variants
– Clonal nevi
– Combined nevi
– Congenital nevi biopsied shortly after birth
– Deep penetrating nevi
– Atypical (dysplastic, Clark's) nevi
– Halo nevi
– Hyperplasia of melanocytes in sun-damaged skin
– Melanocytic proliferation overlying a benign neoplasm
– Longitudinal melanonychia
– Melanosis of mucosal regions
– Nevi arising within areas of lichen sclerosus
– Nevi exposed to UV radiation
– Nevi in genital regions (including milk-line nevi and flexural nevi)
– Nevi in patients with epidermolysis bullosa
– Nevi on or around the ear
– Pigmented streaks in melanoma scars
– Proliferating nodules in giant congenital nevi in neonates
– Recurrent (persistent) nevi
– Reticulated (ink-spot) lentigo
– Spitz nevi and variants
• DDX-non-melanocytic– Paget's disease
– Extramammary Paget's disease
– Pigmented epidermotropic metastasis of breast carcinoma
– Epidermotropic neuroendocrine carcinoma
– Bowen's disease (pagetoid or pigmented)
– Pagetoid reticulosis
– „Clear-cell‟ artefacts around keratinocy tes
– Complete regression of skin tumors other than malignant melanoma (e.g. lichen planus-like keratosis, halo nevi)
– Pigmented basal cell carcinoma
– Pigmented actinic keratosis
– Dermato.broma
– Seborrheic keratosis
– Pigmented poroma and pigmented porocarcinoma
– Pigmented pilomatricoma
– Subungual hematoma
– Black heel (hemorrhage in stratum corneum caused by trauma)
– Pyogenic granuloma
– Tinea nigra
– Thrombosed hemangioma, angiokeratoma

Melanoma
• Management
– Bring pt back for a total body skin
exam
– Studies – usually a CBC, CMP,
LDH & CXR
• Limited value for melanomas
<4mm -surgery is going to
want most of these anyway
for pre-op
– New marker not routinely used -
S100beta and MIA
– StageIII/IV – MRI head, CT
chest/abd/pelvis, PET scan or
PET-CT
the deeper the worse
Melanoma
• SLNB
– Primary melanomas >1.0mm
• Provides info on subclinical nodes with minimal morbidity
• Identifies metastatic nodes for early therapeutic dissection
• Identifies candidates for IFN alpha
NOT theraputic however
• SLNB- Exceptions– For those patients with a lesion <
1mm a selective SLN biopsy will be performed. Those patients who we would consider (Controversial, no nationwide guidelines)
– 1. Those with a depth between 0.75-0.99 mm
– 2. Clark level IV or higher
– 3. Ulceration
– 4. Those with some “soft” poor prognostic criteria: head and
neck or trunk melanomas, male sex, evidence of regression, vascular or neural invasion
• We have had 2 young women with positive lymph nodes with thin melanomas
Sentinel lymph node biopsy

SCABIES
• Worldwide problem and all ages, races and socioeconomic groups are susceptible
• Environmental factors-overcrowding, delayed treatment of primary cases, and lack of public awareness of the condition
• Transmitted directly by close personal contact, sexual or otherwise, or indirectly via fomite transmission
• Prevalence is higher in children and in people who are sexually active
• Spread of the infestation between family members and close contacts is common
• Crusted scabies-compromised immune systems (e.g. the elderly, people infected with HIV, and transplant patients) as well as those with decreased sensory functions (e.g. patients with leprosy or paraplegia)

SCABIES
• Sarcoptes scabiei var. hominiscauses human scabies
• entire 30-day life cycle of mites is completed within the epidermis
• female mite will lay 60-90 eggs, which require 10 days to mature
• incubation period before symptoms-days to months
• first-time infestations- 2-6 weeks before the host's immune system becomes sensitized to the mite or its byproducts, resulting in pruritus and cutaneous lesions
• Asymptomatic scabies-infested individuals are not uncommon, and these individuals can be
considered „carriers•
SCABIES
• history distribution,types of lesions, and pruritus form the basis of the clinical diagnosis
• intense pruritus at night exacerbated by a hot bath or shower
• Symmetrical-interdigital/web spaces, flexural aspect of the wrists, axillae, behind the ears, waist, ankles, feet, buttocks and belt area
• men-penile and scrotal lesions are common
• women-areolae, nipples and genital area are often affected
• infants, elderly and immunocompromised-all skin surfaces are susceptible, including the scalp and face

SCABIES
• small erythematous papules are
present, excoriations
• vesicles, indurated nodules,
eczematous dermatitis and
secondary bacterial infection are
common
• pathognomonic sign is the burrow-
wavy, thread-like, grayish-white
and 1-10 mm in length

SCABIES

SCABIES
• Dx-mineral oil examination in which skin scrapings from infested
areas are inspected under light microscopy for adult mites, eggs
and/or fecal pellets
• DDx- atopic, contact or nummular dermatitis, autosensitization („id‟
reaction), pyoderma, dermatitis herpetiformis, bullous pemphigoid,
and other insect bites should be considered
• Tx-Topical
– Permethrin cream (5%)Originally a single, overnight treatment;
current recommendation is to repeat on day 8; RF-Allergy to
formaldehyde; Good, but some signs of tolerance developing.
– Lindane lotion (1%)Topically overnight, on days 1 and 8,RF-for
CNS toxicity, age <2 years, pregnancy, breastfeeding, areas of
eroded skin; Poor, resistance very common(not used anymore)

SCABIES
• Tx-topical
– Crotamiton (10%)Topically overnight, on days 1, 2, 3 and 8; RF-
for irritant contact dermatitis, denuded skin; Very poor; has
antipruritic properties and may be used for post-scabetic pruritus
• Tx-oral
– Ivermectin (200–400 mg/kg); commercially available as 3 and 6
mg tablets; Orally on day 1 and 14; RF-for potential CNS toxicity,
<15 kg, pregnancy, breastfeeding; Excellent
• Pruritus and lesions can persist for 2-4 weeks after successful
treatment

Lice(head)
• Lice are bloodsucking,
wingless insects belonging to
the order Anoplura
• worldwide with no strict
limitations based upon age,
sex, race or socioeconomic
class
• children 3-11 years of age
have the highest incidence
• more frequently observed in
girls
• head louse, Pediculus capitis

Lice(head)
• Transmission occurs via direct head-to-head contact or by fomites such as combs, brushes, blow-dryers, hair accessories, bedding, helmets and other head gear
• head lice do transmit coagulase-positive Staphylococcus aureusand group A Streptococcus pyogenes by carrying these organisms on their external surfaces.
• scalp, behind the ears and the nape of the neck-pruritus, excoriations, erythema, pyoderma, and scaliness of the scalp and posterior neck are common
• diagnosis is made by id of nits and/or adult lice on the scalp hair, viable eggs are tan to brown in color
• occ pt will present with a low-grade fever, irritability, lymphadenopathy and a secondary bacterial infection
•

Lice(head)
Lice(head)
• DDX-seb derm, psoriasis
• Tx-similar to that of scabies,
– With all topical preparations (regardless of package instructions), two applications, 1 week apart, are advisable in order to:
• (1) kill any nits that survived treatment
• (2) better defend against the seemingly growing resistance to most pediculicides
• (3) reduce the risk of reinfestation by means of fomites
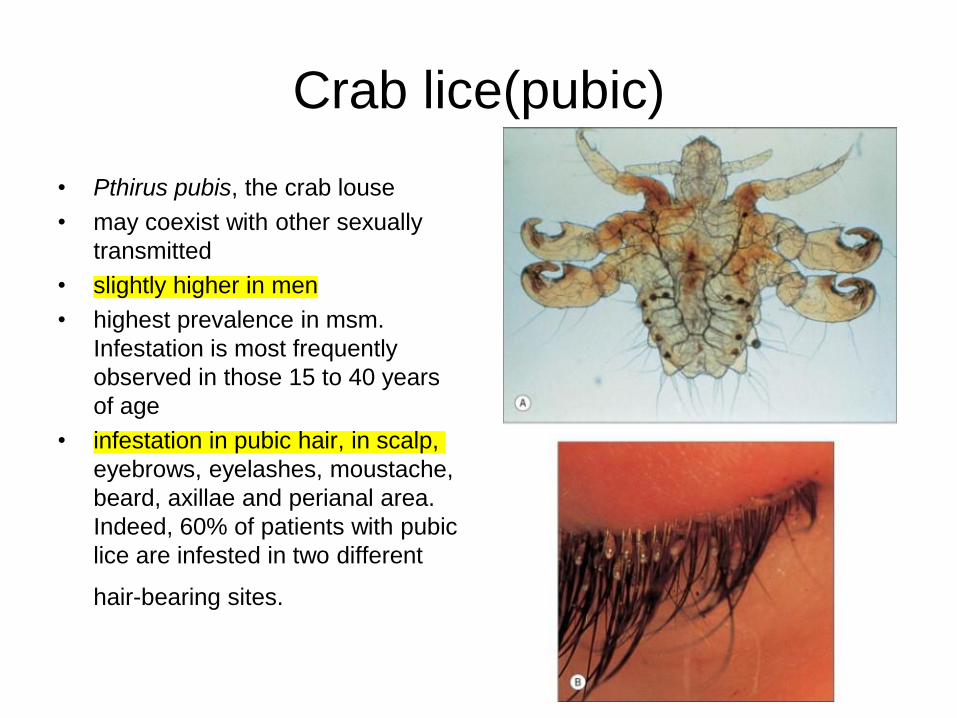
Crab lice(pubic)
• Pthirus pubis, the crab louse
• may coexist with other sexually
transmitted
• slightly higher in men
• highest prevalence in msm.
Infestation is most frequently
observed in those 15 to 40 years
of age
• infestation in pubic hair, in scalp,
eyebrows, eyelashes, moustache,
beard, axillae and perianal area.
Indeed, 60% of patients with pubic
lice are infested in two different
hair-bearing sites.

Crab lice(pubic)
• skin-colored or simply appear as hemorrhagic crusts, may be
erythema around the hair follicles, excoriations, secondary bacterial
infection, and lymphadenopathy
• DDX-ID diagnostic, all infestation and bites, other other ds w/pruritus
• Tx-all tx should be given 1 week apart, tx similar to scabies

Body Lice
• associated with overcrowding, poor hygiene, poverty, wars and natural disasters
• primary vectors for several diseases caused by Rickettsia, Borreliaand Bartonella species
• Pediculosis corporis is caused by an infestation of humans and their clothing by Pediculus humanus var. corporis, infestation requires an inability to wash and change clothes
• transmitted by the body louse-epidemic typhus (caused by Rickettsia prowazekii), relapsing fever (caused by a spirochete, Borrelia recurrentis), and trench fever and bacillary angiomatosis or endocarditis (caused by Bartonella quintana)
• Transmission not by louse bites but contaminated fecal pellets being scratched into excoriated skin or inhalation of dry, powdery louse feces from infected bedding or clothing.
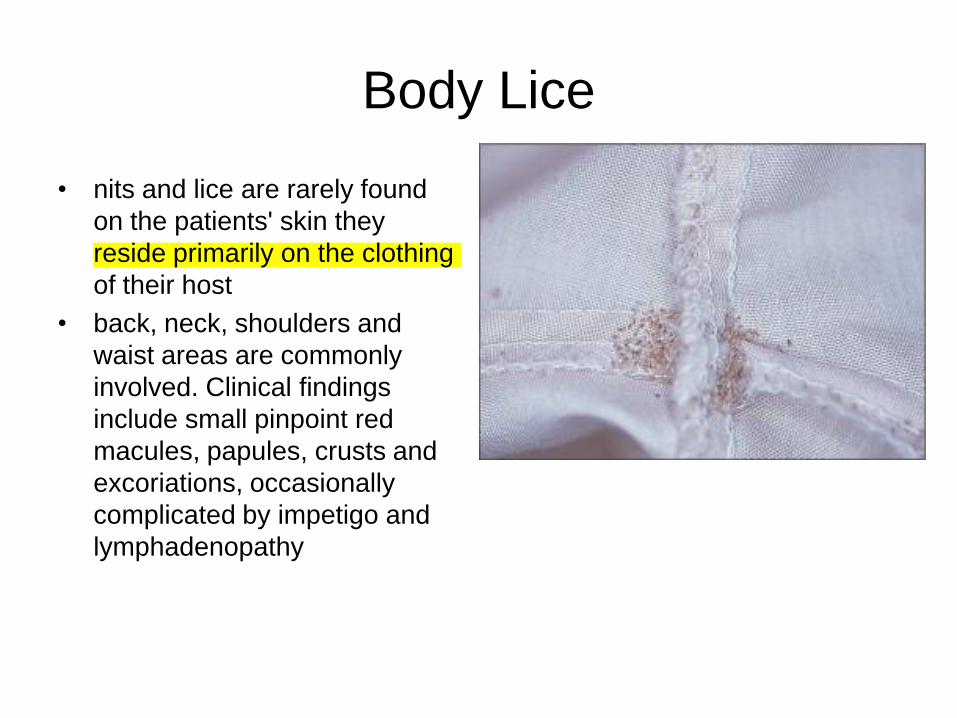
Body Lice
• nits and lice are rarely found
on the patients' skin they
reside primarily on the clothing
of their host
• back, neck, shoulders and
waist areas are commonly
involved. Clinical findings
include small pinpoint red
macules, papules, crusts and
excoriations, occasionally
complicated by impetigo and
lymphadenopathy

Body Lice
• DDX-any condition causing pruritus
• Preferably, the clothing and bedding of infested individuals are
discarded in tightly sealed, plastic biohazard bags and incinerated
• involves fumigating the clothing and heating it to a temperature of
65°C for 15-30 minutes

Spider Bites
• Black widows are large, shiny black
spiders with a large round abdomen
• Found in woodpiles, in shoes and
under outhouse seats
• In Latrodectus mactans, an hourglass
design is seen on the abdomen most
common in North America
• Lactrodectus mactans; alpha-
lactrotoxin; bites are painful; releases
Neurotoxin: Ach is irreversibly
releasedsevere pain in local
muscles crampy abd pain, chills,
vomiting, paralysis, mimicks acute
abdomen, rhabdomyolysis
• Benzodiazepines and intravenous
calcium gluconate can be helpful for
the associated tetany
Spider Bites
• Loxosceles spiders are found throughout the world. In the US, L. reclusa, L. laeta, L. rufescens, L. deserta and L. arizonica cause skin necrosis
• Brown recluse spiders are commonly found in south central US, from Tennessee and Missouri to Oklahoma and Texas, often found in woodpiles, attics and under radiators.
• Brown spiders are non-aggressive
• diagnosis can now be confirmed either by an enzyme immunoassay to detect Loxosceles venom in a skin biopsy
• Sphingomyelinase D interacts with serum amyloid protein gravity dependent state
• majority of bites do not cause serious reactions
• Dermonecrotic reactions can present as dry, necrotic eschars or ulceration; sys rxn-DIC, Coombs'-positive hemolytic anemia

Spider Bites
• Most bites can be treated with
rest, ice and elevation
• more widely available agents
such as dapsone, colchicine,
triamcinolone and prednisone
have been inconsistent and
often disappointing
• Antivenin
• Avoid heat and immediate
surgery as they can spread
venom
• Augmentin 2/2 infection

Spider Bites
• Tegenaria agrestis- Large, hairy,
aggressive spiders found in dark,
moist areas, especially basements
• found in the northwest US,
Canada and Europe
• Hobo spider toxins may cause
local necrosis and directly affect
the CNS
• Systemic symptoms include
headache, nausea and weakness;
hemolysis and thrombocytopenia
• Funnel shapped web
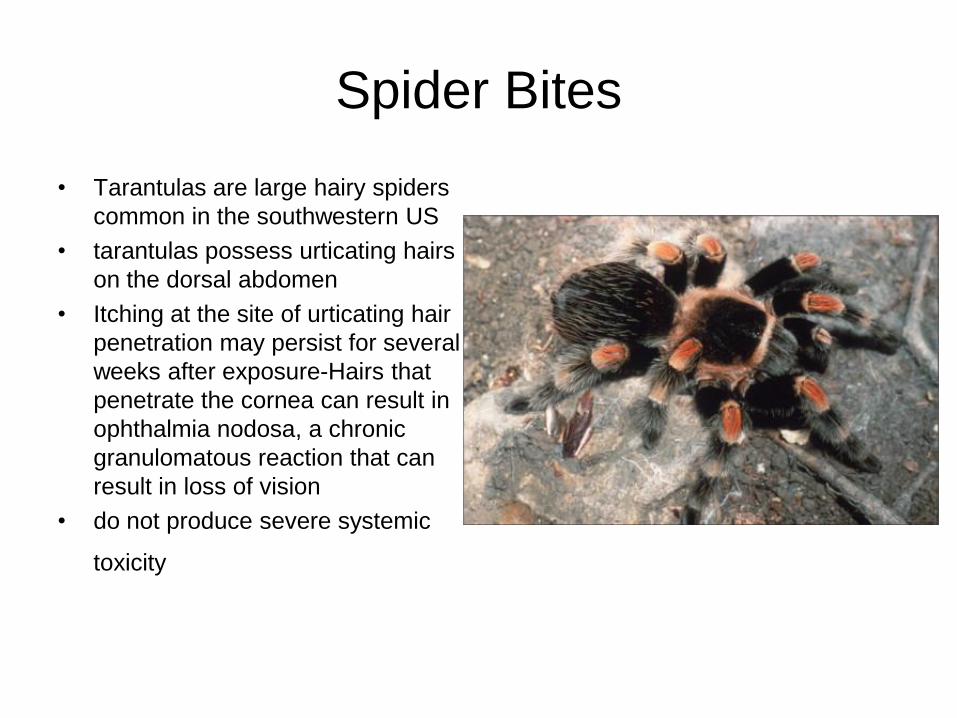
Spider Bites
• Tarantulas are large hairy spiders
common in the southwestern US
• tarantulas possess urticating hairs
on the dorsal abdomen
• Itching at the site of urticating hair
penetration may persist for several
weeks after exposure-Hairs that
penetrate the cornea can result in
ophthalmia nodosa, a chronic
granulomatous reaction that can
result in loss of vision
• do not produce severe systemic
toxicity

Androgenetic Alopecia
• 80% of Caucasian men by age 70
• Genes and hormones are
implicated, inheritance is
polygenic
• Hormones in AGA
– Testosterone-Increased
muscle mass
– Growth of the phallus &
scrotrum
– Voice change
– Sex drive
– Terminal pubic and axillary
hair fibers

AGA
• Hormones in AGA
– Testosterone
• Increased muscle mass
• Growth of the phallus & scrotrum
• Voice change
• Sex drive
• Terminal pubic and axillary hair fibers
– Testosterone is converted to DHT by 5 alpha reductase which
leads to temporal scalp hair recession, acne, growth of the
prostate, growth of terminal hairs in the beard region, external
ears, nostrils & limbs
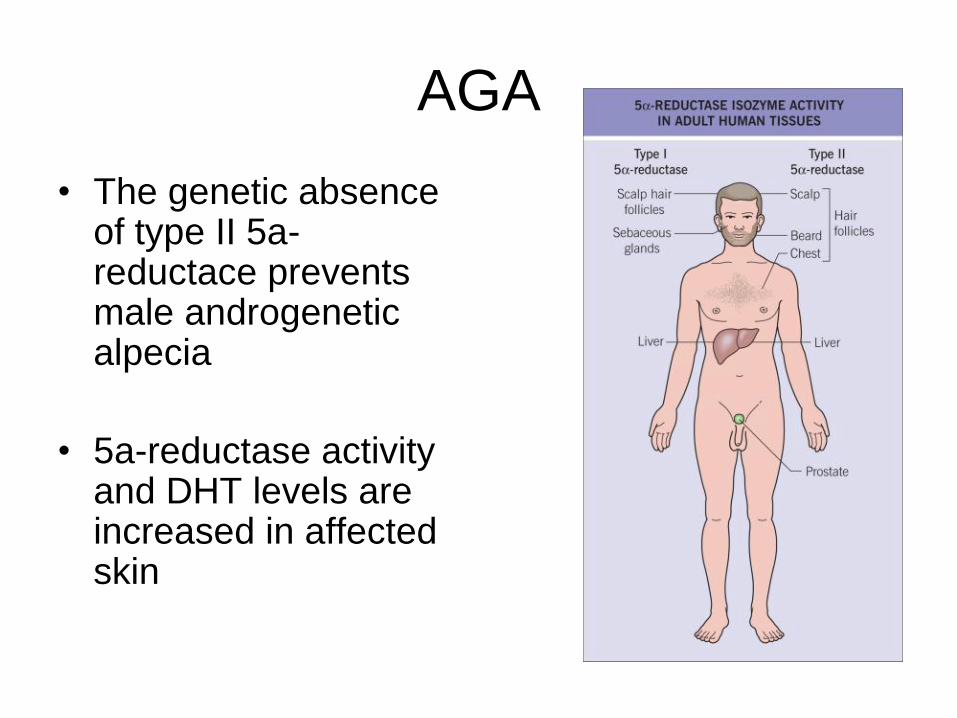
AGA
• The genetic absence of type II 5a-reductace prevents male androgenetic alpecia
• 5a-reductase activity and DHT levels are increased in affected skin
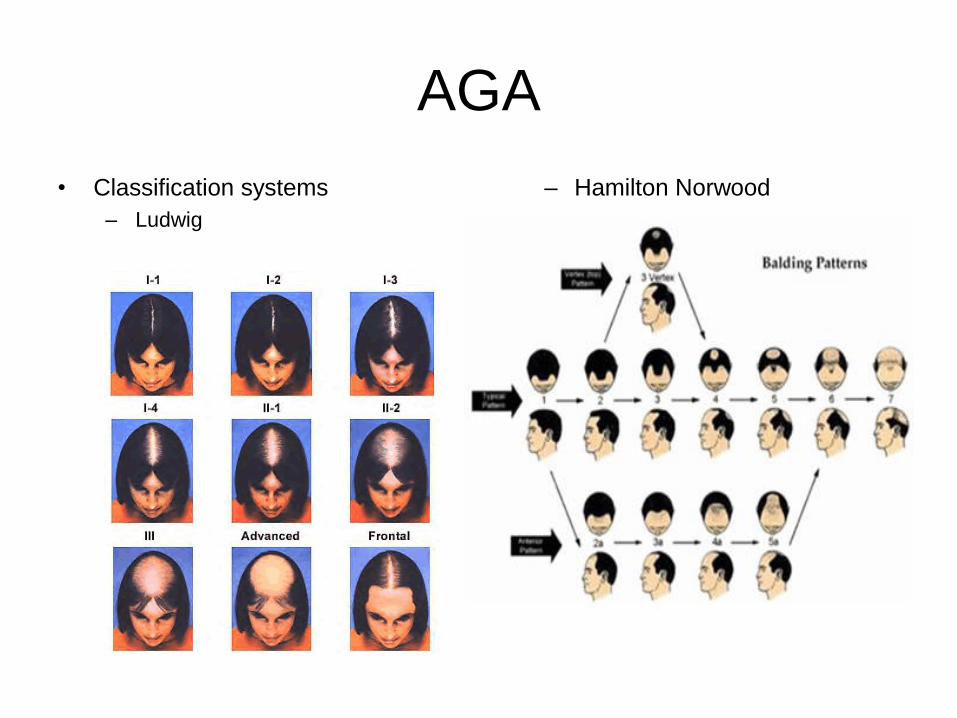
AGA
• Classification systems
– Ludwig
– Hamilton Norwood

AGA
• DDX-other non scarring alopecias,
• Dx-clinical in men bx to confirm, hair loss in women
should suggest the possibility of pathologic
hyperandrogenism, and appropriate screening laboratory
tests (total and free testosterone,
dehydroepiandrosterone sulfate, and 17-hydroxy-
progesterone) should be performed

AGA
• Tx
– Hair transplant
– Minoxidil 2% and 5%, 1ml applied to scalp bid
– Finasteride 1mg po daily
• Stops hair loss in 90% of men for at least 5 years
• Can regrow hair in 65% of men
– hyperandrogenemia in women-Oral contraceptives,
spironolactone or even finasteride(off-label use, birth defects)

Alopecia Areata
• 0.1% to 0.2% of the population
• Normal follicle keratinocytes lack MHC class I and II giving them immunologic privilege
• In AA human leukocyte antigens become expressed by the hair follicle
• T lymphocytes then interact with hair matrix cells causing destruction
• presents as round or oval patches of non-scarring hair loss
• Short „exclamation mark‟ hairs (i.e. distal end broader than the proximal end) can often be seen, particularly at the margins of areas of alopecia
• Other presentations include alopecia totalis (loss of all scalp hair), alopecia universalis (loss of all scalp and body hair and an ophiasis pattern (band-like pattern of hair loss along the periphery of the temporal and occipital scalp)
localized hair loss
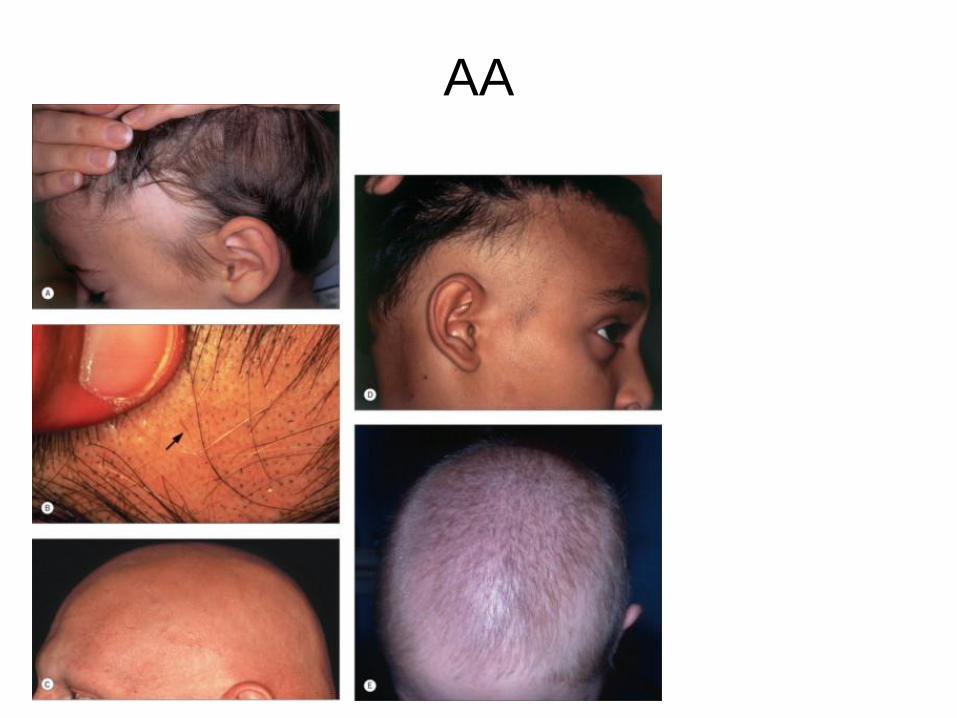
AA

AA
• Assoc Disease
– Atopy (allergic rhinitis, atopic dermatitis, asthma); >40% in some studies
– Autoimmune thyroid disease (e.g. Hashimoto's thyroiditis), vitiligo, inflammatory bowel disease
– Autoimmune polyendocrinopathy syndrome type 1 (autosomal recessive; due to mutations in the autoimmune regulator gene [AIRE]; up to 30% of patients have alopecia areata)
– Type 1 diabetes increased in relatives of patients with alopecia areata

AA
• DDx
– Tinea capitis, trichotillomania, temporal triangular
alopecia, traction alopecia, secondary syphilis and
loose anagen syndrome, pressure-related alopecia,
aplasia cutis and „burnt-out‟ cicatricial alopecia. The
diffuse variant may initially be confused with telogen
effluvium and androgenetic alopecia
• DX-history and clinical examination is sufficient to
distinguish between these conditions, but a scalp biopsy
may be needed.
scaring or no scaring
AA
• Tx– May improve on its own
– Topical steroids – clobetasol (1)
– IL steroids - 3-5mg/ml - into the mid dermis, q 4-8 wks (1)
– Minoxidil (2)
– Immunotherapy: Squaric Acid, anthralin, diphenylcyclopropenone (2)
– Systemic steroids (2)
– PUVA (2)
– Excimer laser (3)
– Photodynamic therapy (3)
– Systemic cyclosporine (3)
intralesional

Onychomycosis
• affects men more than
• challenging to manage due to difficulty in diagnosis, long treatment
periods, potential side effects of systemic medications, and the
frequent recurrence
• dermatophytes as well as non-dermatophytes-3 main pattern types
– distal/lateral subungual with invasion via the hyponychium (most
common)
– white superficial with direct invasion into the superficial nail plate
(often due to T. mentagrophytes)
– proximal subungual with direct invasion under the proximal nail
fold (immunocompromised hosts)
• discomfort and pain associated with trimming the nails, running
Onychomycosis
• frequently associated with chronic tinea pedis
• most common causative pathogens are T. rubrum, T.
mentagrophytes and E. floccosum
• Toenail more common than fingernail, 80% reoccur
• Clinical and Histologic examination of formalin-fixed, PAS-stained
nail plates is a quick and reliable method for diagnosing
onychomycosis
• Tx-preferred terbinafine 250mg daily x3months, check LFT‟s prior to
tx and mid-way, lower reoccurrence rates than iatraconazole, other
antifungals avalible many med interactions
– Topical cicloprox 8% nail lacquer-expensive

Onychomycosis

Paronychia
• affected digit becomes swollen, red and painful
• Compression of the nail fold may produce pus drainage
• most commonly due to bacteria, in particular Staphylococcus aureus
or Streptococcus pyogenes, and follows minor trauma to the nail
• Recurrent episodes of acute paronychia should raise the suspicion
of an HSV infection. Viral cultures, direct fluorescent antibody assay,
and/or PCR should be obtained to identify the responsible agent.
• Tx-drainage of the abscess, systemic antibiotics according to culture
results, systemic antivirals when due to HSV

Paronychia

Condyloma Acuminatum
• Caused by human Paillomavirus
• transmission
– direct skin : skin
– indirect contaminated surfaces (swimming pool, gym)
– aerosolized
• laser, ED&C
• absence of viral envelope resistance to dessication
– recurrent respiratory papillomatosis = HPV -6, -11
• childhood vertical trans., adult genital : oral
– cellular target = basal keratinocytes
– maceration promotes
• Genital warts are uncommon in prepubertal children and are of special concern to healthcare providers- may have been caused by sexual abuse should always be carefully considered
• one of the most common sexually transmitted infections (STI) among adolescents and adults

Condyloma Acuminatum
• Most genital papillomavirus infections resolve spontaneously
• median duration of high-risk HPV infections in women is reported to be 8 months and persistence is observed in 30% after 1 year and in 9% after 2 years of observation
• HPV-16, -18, -31 and -45 are found in approximately 80% of cervical cancers worldwide
• Immune suppression in HIV-infected patients or organ transplant-infections are more frequent, tend to persist, and more often progress to intraepithelial neoplasias
• Recurrent respiratory papillomatosis (RRP)-exophytic lesions of airways and not seen by dermatologists. It occurs in a juvenile- or adult-onset form and is caused by HPV-6 and -11, low incidence RRP is the most common benign tumor of the larynx and the second
most common cause of hoarseness in children
Condyloma Acuminatum
• non-enveloped dsDNA virus
• cellular target = basal keratinocytes(enter through break in skin)
• oncogenicity
– HPV-16, -18, - 31, -33, -45
– cervical cancer, bowenoid papulosis, upper aerodigestive malignancies, SCC
– HPV -5, -8 SCCs in EDV
• Most will resolve w/in 2 years
• external genitalia and the perineum, perianally, or in adjacent areas
such as the inguinal fold and the mons pubis

Condyloma Acuminatum
• Condylomata-one to several
millimeters in diameter
• discrete, sessile, smooth-surfaced
exophytic papillomas
• skin-colored, brown or whitish
(especially when macerated in
moist areas)
• pedunculated or broad-based
papillomas up to several
centimeters in diameter
• large confluent plaques and may
extend into the vagina, the
urethra, or the anal canal, but
rarely beyond the dentate line
Condyloma Acuminatum
• DDX-diagnosis of skin and genital warts is uncomplicated if typical clinical features
are present
• Dx-hx, clinical, histo
• Tx
– Cryotherapy, TCA, excision, curettage, laser
– Salicylic acid
– Cantharadin (occlusion)
– Imiquimod
• 3x per wk x 16wks
– 5-fluorouracil
– Podofilox (Condylox) – cytotoxic
• BID x 3 days in weekly cycles
– Cimetidine – activates Th1 cells to make IL-2 and interferon
– Cidofovir (topical, systemic)
– Intralesional candida, trychophyton, mumps antigens, bleomycin

Verruca Vulgaris
• person-to-person transmission
• Cutaneous warts are caused by a small group of specific HPV types
• prevalence of 20% in schoolchildren and a decline
• One of the three most common dermatoses in children and occur with equal frequency in both sexes. Patients living in larger households often report an infected cohabitant
• The majority of warts will regress spontaneously within 1-2 years
• Reinfection with the same HPV type appears uncommon after clearance, suggesting that protective type-specific immunity may develop
• Pathogensis similar for all HPV
• hyperkeratotic, exophytic and dome-shaped papules or nodules associated typically with HPV-1, -2 or – 4

Verruca Vulgaris
• commonly located on fingers,
the dorsal surfaces of hands,
and other sites prone to
trauma such as knees or
elbows, but may occur at any
anatomic location
• Palmar and plantar appear as
thick, endophytic papules on
palms, soles, and lateral
aspects of the hands and feet,
with gently sloping sides and a
central depression
• painful to pressure when
walking

Verruca Vulgaris
• DDX-Seborrheic keratoses, actinic
keratoses, cornu cutaneum,
keratoacanthoma, lesions of
acrokeratosis verruciformis,
angiokeratoma and amelanotic
melanoma may resemble common
warts, LP
• Dx-clinical and histo
• Cryotherapy, TCA, excision, curettage, laser
• Salicylic acid
• Cantharadin (occlusion)
• Imiquimod
– 3x per wk x 16wks
• 5-fluorouracil
• Podofilox (Condylox) – cytotoxic
– BID x 3 days in weekly cycles
• Cimetidine – activates Th1 cells to make IL-2 and interferon
• Cidofovir (topical, systemic)
• Intralesional candida, trychophyton, mumps antigens, bleomycin

Viral Exanthems
• Varicella-Zoster Virus (HHV-3)
– Etiologic agent of chicken pox
and herpes zoster (shingles)
– High morbidity and mortality in
immunocompromised hosts
– Transmission via airborne
droplets or direct contact with
vesicle fluid
– Incubation 11-20 days
– Extremely contagious(80-
90%)
– Zoster = reactivation of latent
VZV

Viral Exanthems
• Primary Varicella (Chickenpox)
– Fever, malaise, myalgia
– Erythematous, pruritic macules
and papules
– Start on scalp and facetrunk
and extremities
– Dew drops on a rose petal
– Hallmark: Lesions in all stages of
development

Viral Exanthems
• Herpes Zoster (Shingles)
• Complication: Ramsay-Hunt Syndrome
– VZV infection of the geniculate ganglion of the facial nerve
– Zoster involves external ear
– Facial paralysis – ipsilateral
– Tinnitus or other auditory symptoms

Viral Exanthems
• Varicella in Pregnancy
• First 20 weeks of gestation:
– Congenial varicella syndrome:
– hypoplastic limbs, ocular and CNS abnormalities
• 5 days before and 2 days after delivery
– Neonatal varicella
– Neonate develops at 5-10 days of age
– Treat with VZIG + IV Acyclovir

Viral Exanthems
• DDX-HSV, vesicular viral exanthems (Coxsackie, ECHO), pityriasis
lichenoides et varioliformis acuta (PLEVA), rickettsialpox, a drug
eruption, contact dermatitis, and, occasionally, insect bites or even
scabies
• Dx-clinical diagnosis, based upon both the history (e.g. initial
episode versus multiple recurrences; previous history of varicella or
receipt of the varicella vaccine) & the physical examination, is very
important because a decision regarding instituting antiviral therapy
is critical
• Tzanck smear(cannot differentiate HSV types) and/or a DFA(allows
distinction) are initially performed
• Histo not too helpful b/w VZV and HSV(need staining)
• PCR is a highly sensitive molecular technique and its use as a
diagnostic test of choice is increasing

Viral Exanthems
• Varicella in children-symptomatically with antipyretics, antihistamines, calamine lotion and tepid baths
• acyclovir has been shown to decrease the duration and severity of varicella infection(24 to 72 hours from start)
• Acyclovir is clearly recommended for varicella in the adult population
• Varicella zoster immunoglobulin (VIG)-prophylaxis for all susceptible immunocompromised individuals
• VZV vaccine (Oka strain; Varivax®)-ages 12 months and 4-6 years
• herpes zoster-early tx within 72 hours of the onset of the first vesicle, is optimal, but initiation of antiviral therapy after 72 hours but within 7 days also appears to be beneficial
• Acyclovir, famciclovir and valacyclovir are all FDA-approved for the treatment of zoster in immunocompetent individuals and result in decreased disease duration and pain.
• Intravenous acyclovir is indicated for the treatment of zoster in immunocompromised patients as well as those with serious complications

Viral Exanthems
• Epstein-Barr Virus (HHV-4)-causes
– Infectious mononucleosis
– Endemic Burkitt‟s lymphoma
– Oral hairy leukoplakia
– Nasopharyngeal carcinoma
– Post-transplant lymphoproliferative disorders
– Gianotti-Crosti Syndrome

Viral Exanthems
• EPSTEIN–BARR VIRUS (HHV-4)
– seropositivity approaches 60-80% in children of developing countries;
similar rates are reached during adolescence in the US
– Most children with primary EBV infection will have either no symptoms
or a mild, non-specific, febrile illness.
– adolescents and young adults, primary infection with EBV results in the
infectious mononucleosis syndrome in 50% of individuals. In the US, the
annual incidence of infectious mononucleosis is 45.2 cases per 100 000
– EBV is transmitted primarily through infectious saliva, although its
presence in genital secretions and breast milk has been reported
– Cell-mediated immunity to EBV infection is persistent and protects
against developing infectious mononucleosis syndrome with virus
superinfection later in life.

Viral Exanthems
• Infectious mononucleosis
– Fever, pharyngitis,
lymphadenopathy
– Malaise, headache, myalgias
– Hepatosplenomegaly
– Commonly morbilliform
eruption 7-10 days after
treatment with ampicillin
• Cross-reaction between
anti-EBV antibodies and
penicillin-like drug
• Desquamation 1 week
later
– Affects teens and young
adults

Viral Exanthems
• Oral Hairy Leukoplakia– Slightly raised white plaque on lateral tongue
– Corrugated appearance
– HIV and immunocompromised

Viral Exanthems
• DDx-group A streptococcal infection, acute viral hepatitis, drug
reaction with eosinophilia and systemic symptoms (DRESS),
toxoplasmosis, lymphoma, and primary CMV, HHV-6 and HIV
• Dx-mild to moderately elevated hepatic transaminase levels, mild
thrombocytopenia and an absolute and relative lymphocytosis
• Diagnosis is usually made by a positive monospot test (a simple
slide test that detects IgM heterophile antibodies) or increased titers
of heterophile antibodies; the latter are >1:40 in approximately 90%
of young adults infected with EBV
• EBV-specific serologies are often needed

Viral Exanthems
• Tx-self-limited and treatment is supportive

Viral Exanthems
• Congenital CMV(HHV-5)
– In immunocompetent hosts, 95% of infections are asymptomatic or subclinical
– inversely proportional to socioeconomic status
– in the US, congenital CMV infection occurs in approximately 0.5-1.5% of all newborn infants
– Transmission- is via body fluids, including saliva, blood, urine, semen, breast milk and cervical and vaginal secretions, transplanted organs and hematopoietic stem cells.
– spread indirectly by contaminated fomites, such as toys.
– Transplacental transmission of CMV to the fetus is more likely in the setting of a primary infection in the mother, with 40% of fetuses becoming infected, compared to less than 1% in recurrent cases
– incubation period of 4 to 8 weeks
– „mononucleosis-like syndrome‟ similar to that seen with EBV is the most common clinical presentation in immunocompetent persons

Viral Exanthems
• morbilliform, urticarial, petechial or purpuric, develops in
a small percentage of patients
• administration of ampicillin during this symptomatic
period leads to a cutaneous eruption in 80-100% of
individuals
• clinical course is benign and self-limited, rare
complications include hemolytic anemia,
thrombocytopenia, granulomatous hepatitis, Guillain–
Barré syndrome, meningoencephalitis, myocarditis,
interstitial pneumonia, arthritis, and gastrointestinal and
genitourinary symptoms (e.g. gastroenteritis).

Viral Exanthems
• Congenital CMV
– Infection during 1st and 2nd trimester
– SGA, microcephaly, retinitis, colobomas, intracranial calcifications
– #1 infectious cause of deafness and mental retardation in the U.S.
– Most common congenital viral infection
– TORCH syndrome
– Blueberry muffin baby

Viral Exanthems
• DDX-EBV-induced infectious mononucleosis, toxoplasmosis, viral
hepatitis and lymphoma
• Dx- Culture of CMV (from infected tissues) in human fibroblasts is
„gold standard‟ for definitive diagnosis, takes a few days to several
weeks for confirmation. Nowadays,
• more rapid detection of CMV in tissue cultures (within 24-48 hours)
is possible with the shell vial assay in which monoclonal antibodies
are used to detect antigens associated with early CMV replication
• most commonly employed laboratory tests analyze peripheral blood
for the presence of CMV antigenemia or CMV DNA (the latter PCR-
based test is necessary in the setting of neutropenia)
Viral Exanthems
• Tx
– prevention plus prophylaxis or pre-emptive antiviral treatment in
susceptible individuals
– First line: Ganciclovir, Valganciclovir
– If no reponse Foscarnet and Cidofovir

Viral Exanthems
• HHV-6(Roseola)
– most common in young children, occurring between the ages of
6 months and 3 years in 95% of cases
– Transmission is through infected saliva
– clinical manifestations of exanthem subitum occur in about 30%
of those with primary HHV-6 infections
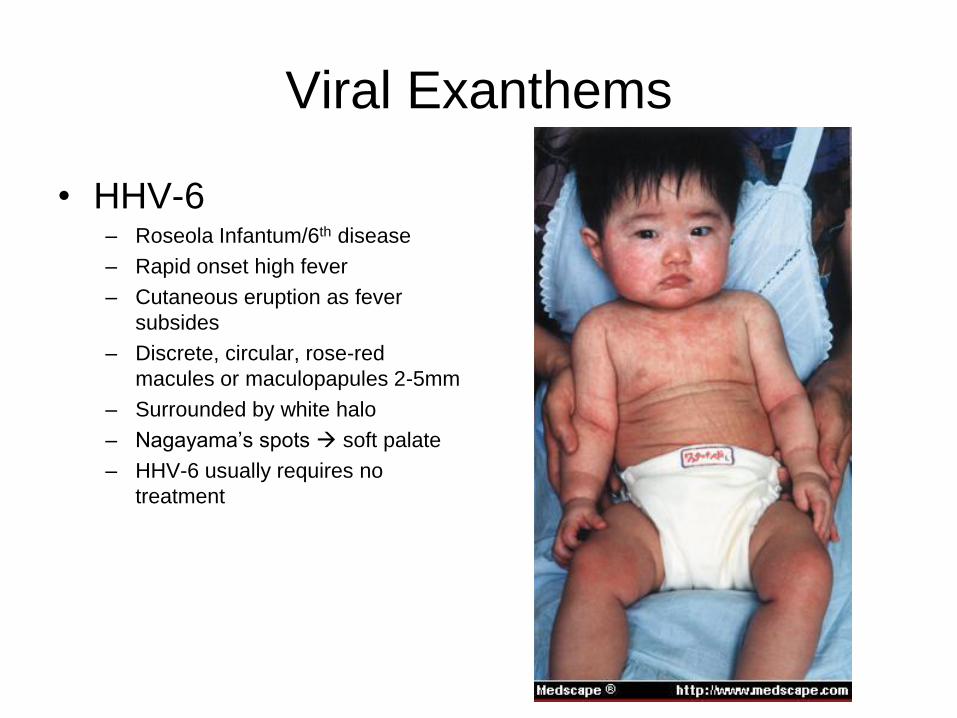
Viral Exanthems
• HHV-6– Roseola Infantum/6th disease
– Rapid onset high fever
– Cutaneous eruption as fever
subsides
– Discrete, circular, rose-red
macules or maculopapules 2-5mm
– Surrounded by white halo
– Nagayama‟s spots soft palate
– HHV-6 usually requires no
treatment

Viral Exanthems
• DDx-(rubeola, rubella, and enterovirus, adenovirus, EBV, and
parvovirus infections) as well as scarlet fever, Rocky Mountain
spotted fever, and Kawasaki disease
• Dx-hx and clinical, PCR detection of cell-free HHV-6 DNA in serum
or plasma has diagnostic value
• Tx-benign and requires no treatment

Viral Exanthems
• HHV-7
– Can also cause roseola
– Possible role in pityriasis rosea
– epidemiology appears to be similar to that of HHV-6
– HHV-7 has not been clearly associated with any clinical disease

Viral Exanthems
• HHV-8
– transmission are not well understood
– Kaposi's sarcoma-associated herpesvirus (KSHV), is a latent
virus found in the vast majority of all types of Kaposi's sarcoma
(KS)
– classic form of KS peaks after the sixth decade of life and
typically occurs in men of Mediterranean and Ashkenazi Jewish
descent. HIV-positive men who have sex with men are at
extreme risk, developing KS at a rate 20 000 times greater than
that of the general population
– KS is a vascular endothelial malignancy

Viral Exanthems
• Associated with 2 neoplasms:
– Kaposi‟s sarcoma
– Castleman‟s disease
• Lymphoproliferative disorder defined as "a localized hyperplasia of lymphoid follicles with and without a germinal center formation and marked capillary proliferation with endothelial hyperplasia
• 4 types of KS:
– Classic KS
– AIDS-related KS
– Immunosuppression-KS
– African endemic KS

Viral Exanthems
• DDx-acroangiodermatitis (pseudo-KS), bacillary
angiomatosis, ecchymosis, hemangioma, angiosarcoma,
pyogenic granuloma and pseudolymphoma/lymphoma
• Dx-confirmed by a skin biopsy
• Tx-cryotherapy, radiotherapy, topical alitretinoin,
intralesional interferon-α and systemic chemotherapy,
and, for AIDS-related KS, highly active antiretroviral
therapy (HAART). Of note, the latter has markedly
reduced the incidence of AIDS-related KS. Surgery is
usually not effective.

Molluscum Contagiosum
• With the eradication of smallpox, molluscum contagiosum (MC)
became the only remaining poxvirus infection to specifically afflict
humans. This disorder is caused by the MC virus (MCV), a member
of the Molluscipox genus of Poxviridae
• Most common infections in humans
• Poxviridae
• MC is a common, benign, self-limited process in children. It also
occurs in adults, usually as a sexually transmitted disease, and
more recently has been observed with increasing frequency in
immunocompromised hosts, most notably HIV-infected individuals.
Transmission is via skin-to-skin contact and, less commonly,
fomites.
Molluscum Contagiosum
• MC lesions are firm, umbilicated pearly papules with a waxy surface
• occur anywhere, most common in skin folds and the genital region
• Widespread, large and occasionally deforming lesions may be seen in the setting of immunosuppression, particularly AIDS
• An associated molluscum dermatitis is common, especially in children with atopic dermatitis. Inflammation of MC lesions is sometimes seen
• DDx-appendageal tumors, verrucae, condylomata acuminata, basal cell carcinoma, juvenile xanthogranuloma, melanocytic nevi (especially Spitz nevi), papular granuloma annulare, pyogenic granuloma or pyoderma
• Dx-clinicial and histo if necc

Molluscum Contagiosum
• Tx
– Most papules of MC resolve spontaneously
– curettage, manual expression, liquid nitrogen, chemovesicants, topical keratolytics, topical cidofovir, tape stripping and laser
– In children, application of cantharidin is a safe and effective therapy, which has the added benefits of being painless and non-traumatic, more visits than curettage

Cellulitis
• infection of the deep dermis and subcutaneous tissue caused most
commonly by Str. pyogenes and S. aureus-in adults
• in childhood is caused by S. aureus, and less commonly by H.
influenzae
• mixture of Gram-positive cocci and Gram-negative aerobes and
anaerobes is associated with cellulitis surrounding diabetic ulcers
and decubitus ulcers
• Lymphedema, alcoholism, diabetes mellitus, intravenous drug
abuse, and peripheral vascular disease all predispose to cellulitis.
Recurrent bouts of cellulitis may be caused by damage to the
lymphatic system (e.g. previous lymph node dissection, saphenous
vein harvest or prior episode of acute cellulitis)

Cellulitis
• often preceded by systemic symptoms, such as fever,
chills and malaise
• cardinal signs of inflammation: rubor (erythema), calor
(warmth), dolor (pain), and tumor (swelling)
• ill-defined, non-palpable borders
• In severe infections, vesicles, bullae, pustules or necrotic
tissue may be present. Ascending lymphangitis and
regional lymph node involvement may occur.
• Children usually have cellulitis of the head and neck
region, whereas in adults the extremities are most often
affected

Cellulitis
• DDX-lower extremity
cellulitis includes deep
vein thrombosis and other
inflammatory diseases,
such as stasis dermatitis,
superficial
thrombophlebitis, and
panniculitis (especially
lipodermatosclerosis)

Cellulitis
• Dx
– usually clinical, needle aspiration and skin biopsy
– leukocyte count is usually normal or only slightly elevated
– Blood cultures are almost always negative in immunocompetent hosts
• Tx
– 10-day course of an oral antibiotic that has good Gram-positive coverage
– Hospitalization and parenteral antibiotics should be reserved for patients who are seriously ill and those who have facial cellulitis.
– Diabetic or decubitus ulcers complicated by cellulitis require broad-spectrum coverage (e.g. piperacillin/tazobactam or, in penicillin-allergic patients, metronidazole plus ciprofloxacin)
– Immobilization and elevation, as well as the application of wet dressings to areas with bullae or exudate, are recommended.
– If signs and symptoms do not improve after 24-36 hours of treatment, cultures and sensitivities should be obtained and antibiotics adjusted accordingly.
– NSAIDs may mask the signs and symptoms of deeper necrotizing infections and should be avoided when treating cellulitis
Erysipelas
• primarily an infection of the dermis with significant lymphatic
involvement. It has a distinctive clinical presentation and is most
often caused by Str. pyogene s (group A streptococci)
• disease of the very young, the aged, the debilitated, and those with
lymphedema or chronic cutaneous ulcers
• Women outnumber men, except for very young patients, where boys
are more commonly affected.
• increased frequency during the summer months
• less often caused by group G, B, C or D. S. aureus, Pneumococcus
species, Klebsiella pneumoniae, Yersinia enterocolitica, and
Haemophilus influenzae type b have been known to cause an
erysipelas-like infection.
•

Erysipelas
• well-defined margins, involves the face or the lower extremity is the most common location
• incubation period of 2 to 5 days, there is an abrupt onset of fever, chills, malaise and nausea.
• A few hours to a day later, a small plaque of erythema develops that progressively spreads, clearly demarcated from uninvolved tissue, hot, tense and indurated with non-pitting edema.
• painful to palpation and may burn
• LAD w/o lymphatic streaking.
• Pustules, vesicles, bullae and small areas of hemorrhagic necrosis may also form
Erysipelas
• DDx-cellulitis and other soft tissue infections (e.g. erysipeloid, necrotizing fasciitis) as well as inflammatory causes of „pseudocellulitis‟ (e.g. Sweet's syndrome, contact dermatitis)
• Dx-Clinical, Routine laboratory evaluation will show an elevated leukocyte count with a left shift. Swabs from local ports of entry, pustules or bullae, the throat, and the nares
• Culture of skin biopsy specimens-yield poor results, especially in immunocompetent hosts
• Anti-DNase B and ASO titers are good indicators of streptococcal infections
• Tx-10-14-day course of penicillin is the treatment of choice for erysipelas caused by streptococci. Although macrolides such as erythromycin may be used in penicillin-allergic patients(increase in macrolide resistance among certain strains of Str. Pyogenes)
• Hospital admission and intravenous or intramuscular antibiotics should be reserved for children and debilitated patients

Impetigo
• common, highly contagious, superficial skin infection that primarily affects children
• Two most common responsible organisms:
– Staphylococcus aureus
– Streptococcus pyogenes
• Mode of spread:
– Person-to-person contact
– Contact with fomites
• Two types of impetigo:
– Non-bullous impetigo
• Honey-colored crusts at sites of minor trauma
– Bullous impetigo
• Caused by S. aureus
• Localized form of SSSS
• Blister formation
• Mediated by exfoliative toxin binding to Dsg1
• Acantholysis in granular layer
• Lesions can occur on intact skin

Impetigo
• DDx-– Non-bullous impetigo-
• Insect bites, Eczematous dermatoses, Herpes simplex viral infection, candidiasis, varicella tinea corporis scabies, pediculosis, pemphigus foliaceus
– Bullous impetigo• Bullous insect bite, thermal
burns, HSV, Autoimmune bullous dermatoses (e.g. linear IgA bullous dermatosis, bullous pemphigoid), bullous erythema multiforme,Stevens–Johnson syndrome

Impetigo
• Tx-
– local wound care, including cleansing, removal of crusts, and
application of wet dressings
– mupirocin 2% ointment or fusidic acid cream or ointment can be
prescribed
– β-lactamase-resistant penicillin
- or - macrolide
- or - first- or second-generation cephalosporin

Vasculitis
• Pathogensis
– Immune complex deposition in vascular wall
– Complement fixation
– Increased neutrophil/lymphocyte adhesion to endothelial cells
– Endothelial cell damage
– Complement also causes mast cell degranulation increased
vascular permeability

AUTHORS' PROPOSED CUTANEOUS VASCULITIS CLASSIFICATION SCHEME.
Caliber of affected
vessel
Classification Subclassification
Small Cutaneous small vessel
vasculitis
Henoch–Schönlein purpura
Acute hemorrhagic edema of
infancy
Urticarial vasculitis
Erythema elevatum diutinum
Small and medium-sized Secondary Infections
Inflammatory disorders (e.g.
autoimmune connective tissue
diseases)
Drug exposure
Neoplasms
Cryoglobulinemic
ANCA-associated Microscopic polyangiitis
Wegener's granulomatosis
Churg–Strauss syndrome
Medium-sized Polyarteritis nodosa (PAN) Classic (systemic) PAN
Cutaneous PAN
Large[*] Temporal arteritis[†]

Vasculitis
• Cutaneous findings of vasculitis depend upon which vessels are primarily involved
• palpable or macular purpura, but urticarial papules, pustules, vesicles, petechiae or erythema multiforme-like lesions
• favor dependent sites, areas under tight-fitting clothing, reflecting the influence of hydrostatic pressure and stasis on the pathophysiology.
• the lesions are asymptomatic, but they can be associated with burning, pain and pruritus.
• In contrast to small vessel disease, medium-sized vessel vasculitis typically presents with livedo reticularis, retiform purpura, ulcers, subcutaneous nodules and/or digital necrosis.
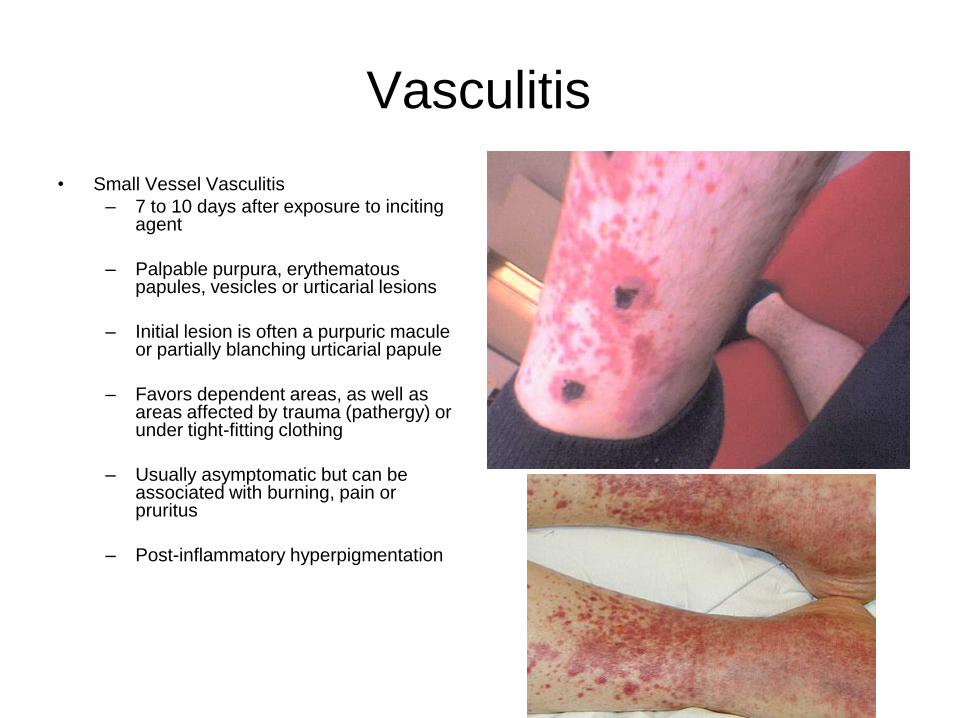
Vasculitis
• Small Vessel Vasculitis
– 7 to 10 days after exposure to inciting agent
– Palpable purpura, erythematous papules, vesicles or urticarial lesions
– Initial lesion is often a purpuric macule or partially blanching urticarial papule
– Favors dependent areas, as well as areas affected by trauma (pathergy) or under tight-fitting clothing
– Usually asymptomatic but can be associated with burning, pain or pruritus
– Post-inflammatory hyperpigmentation

Vasculitis

Vasculitis(scvv)
• Henoch-Schonlein Purpura (HSP)
– Most common in children < 10 yo, associated with a preceding respiratory infection
– Acute onset of purpura, arthralgias and colicky abdominal pain
– Macular erythema or urticarial papules
– Progress to inflammatory purpuric macules and papules
– Predilection for lower extremities and buttocks
– Lesions regress in 10 to 14 days, with resolution of skin involvement over a period of several weeks to months
– Recurrences in 5-10% of patients

Vasculitis(scvv)
• HSP
– GI complication-Intussusception/GI bleeding/Acute surgical
abdomen
– rare potential chronic problem after cutaneous lesions of HSP resolve- Chronic renal failure, Continue to follow UA and serum Cr

Vasculitis(scvv)
• Acute Hemorrhagic
Edema of Infancy– Children 4 to 24 months of age
– Antigenic trigger: Viruses, Bacteria, Drugs
(Antibiotics and NSAIDS), Immunizations
– Presents abruptly with large rosette-shaped
purpuric and petechial plaques
– Favors face, ears and extremities
– Painful, edematous, coin-shaped or targetoid
– Can involve the trunk and genital region:
scrotum
– Facial edema
– Fever but non-toxic appearing
– Mucosa/visceral involvement RARE
– Resolution in 1 to 3 weeks.

Vasculitis(scvv)
• Urticarial Vasculitis– Erythematous, indurated wheals
– Trunk and proximal extremities
– Distinguish from urticaria:
• Lesions persist beyond 24
hours
• Associated with burning and
pain rather than pruritus
• Resolve with
postinflammatory
hyperpigmentation

Vasculitis(small/med)
Wegener‟s Granulomatosis
Necrotizing granulomatous
inflammation of the upper and lower
respiratory tracts
– Recurrent epistaxis, mucosal ulcerations, nasal septal perforation, and saddle nose deformity
– Dyspnea, cough, hemoptysis or pleuritis
• Glomerulonephritis
• Palpable purpura, oral ulcers, nodules, gingival hyperplasia, and livedo reticularis
• immune factor is positive c-ANCA
• treatment of choice-Cyclophosphamide
Vasculitis(small/med)
• Churg-Strauss– First: symptoms of allergic rhinitis, nasal polyps and asthma, may
persist for years
– Second: peripheral eosinophilia, respiratory tract infections and gastrointestinal symptoms
– Third: full-blown systemic vasculitis with granulomatous inflammation, which can occur several years to decades after the initial symptoms
– Cutaneous findings in 55% of patients
– Palpable purpura, subcutaneous nodules (typically on the scalp or extremities)
• Less often, urticaria, livedo reticularis, retiform purpura and papulonecrotic lesions
– Majority have p-ANCA against myeloperoxidase
– Leading cause of death-Granulomatous inflammation of myocardium
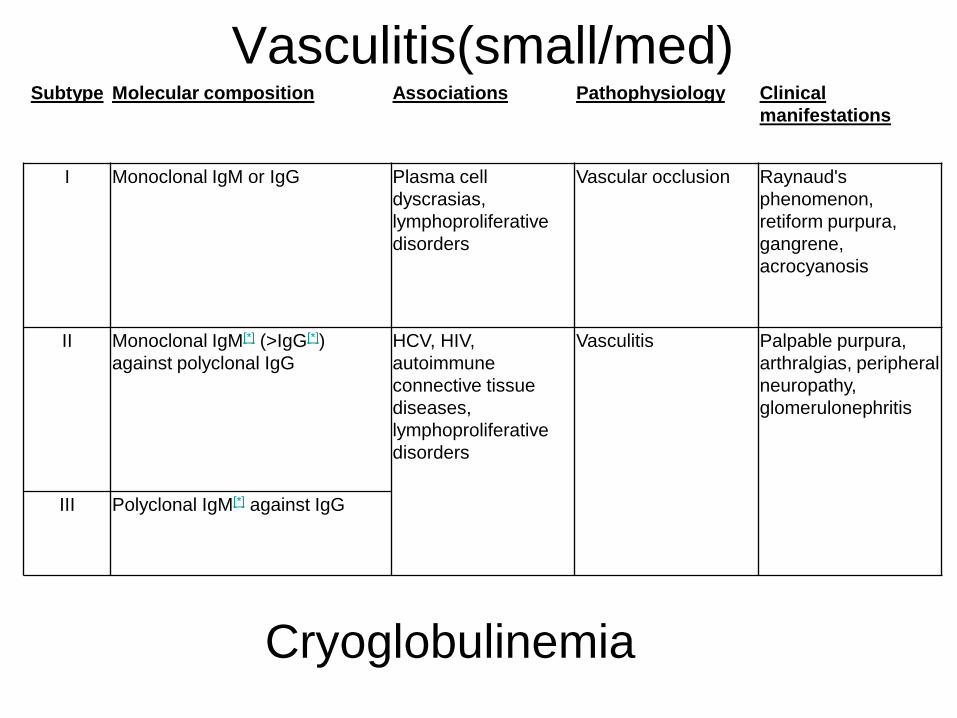
Vasculitis(small/med)Subtype Molecular composition Associations Pathophysiology Clinical
manifestations
I Monoclonal IgM or IgG Plasma cell
dyscrasias,
lymphoproliferative
disorders
Vascular occlusion Raynaud's
phenomenon,
retiform purpura,
gangrene,
acrocyanosis
II Monoclonal IgM[*] (>IgG[*])
against polyclonal IgG
HCV, HIV,
autoimmune
connective tissue
diseases,
lymphoproliferative
disorders
Vasculitis Palpable purpura,
arthralgias, peripheral
neuropathy,
glomerulonephritis
III Polyclonal IgM[*] against IgG
Cryoglobulinemia
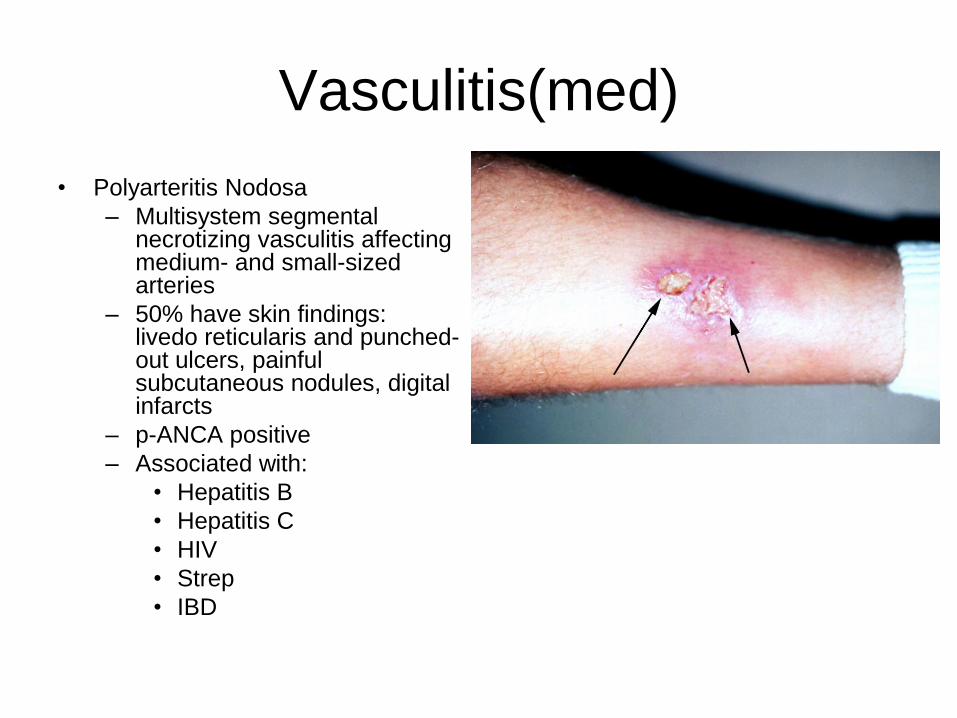
Vasculitis(med)
• Polyarteritis Nodosa
– Multisystem segmental necrotizing vasculitis affecting medium- and small-sized arteries
– 50% have skin findings: livedo reticularis and punched-out ulcers, painful subcutaneous nodules, digital infarcts
– p-ANCA positive
– Associated with:
• Hepatitis B
• Hepatitis C
• HIV
• Strep
• IBD
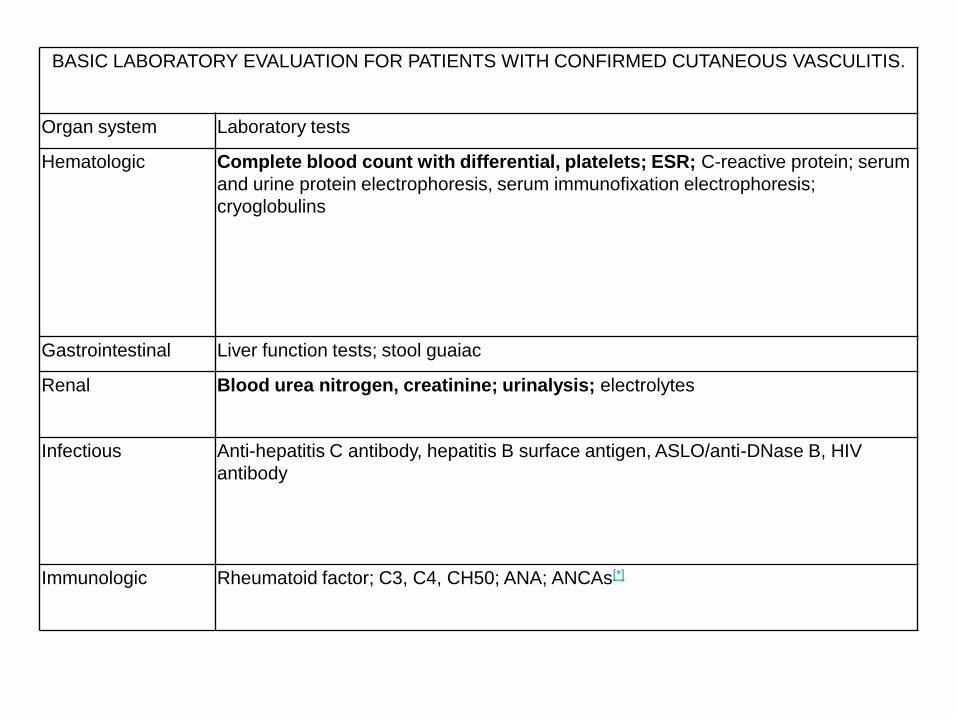
BASIC LABORATORY EVALUATION FOR PATIENTS WITH CONFIRMED CUTANEOUS VASCULITIS.
Organ system Laboratory tests
Hematologic Complete blood count with differential, platelets; ESR; C-reactive protein; serum
and urine protein electrophoresis, serum immunofixation electrophoresis;
cryoglobulins
Gastrointestinal Liver function tests; stool guaiac
Renal Blood urea nitrogen, creatinine; urinalysis; electrolytes
Infectious Anti-hepatitis C antibody, hepatitis B surface antigen, ASLO/anti-DNase B, HIV
antibody
Immunologic Rheumatoid factor; C3, C4, CH50; ANA; ANCAs[*]
Vasculitis
• Tx
– determine whether the disease is either primary or secondary to an
underlying condition (e.g. infection, inflammatory disease, drug
exposure or neoplasm) that can be treated (or, in the case of
medications, discontinued)
– next step is to evaluate the patient for systemic involvement
– based on the extent and severity of systemic involvement
– CSVV frequently resolves without any treatment avoidance inciting
trigger.
• mild skin-limited disease, supportive measures (e.g. leg elevation,
avoiding tight clothing, rest) or symptomatic therapy (e.g.
antihistamines, NSAIDs) may be all that is necessary.
• Topical corticosteroids, calcineurin inhibitors and antihistamines are
sometimes used, but there are no data to support this practice.
Vasculitis
• Tx
– Chronic (>4 weeks) or more severe cutaneous disease may require more aggressive systemic- Colchicine (0.6 mg orally two to three times daily), Dapsone (50-200 mg/day orally) can lead to improvement of mild to moderate, chronic lesions, but it can take several weeks to induce a response
– severe, ulcerating or progressive cutaneous disease- short course of high-dose oral corticosteroids (e.g. up to 1 mg/kg/day of prednisone), Immunosuppressive agents such as azathioprine (2 mg/kg/day) and methotrexate (<25 mg weekly)
– significant systemic vasculitis (e.g. ANCA-associated vasculitides)- high-dose corticosteroids in combination with cyclophosphamide. More recent data suggest that
mycophenolate mofetil and azathioprine may help
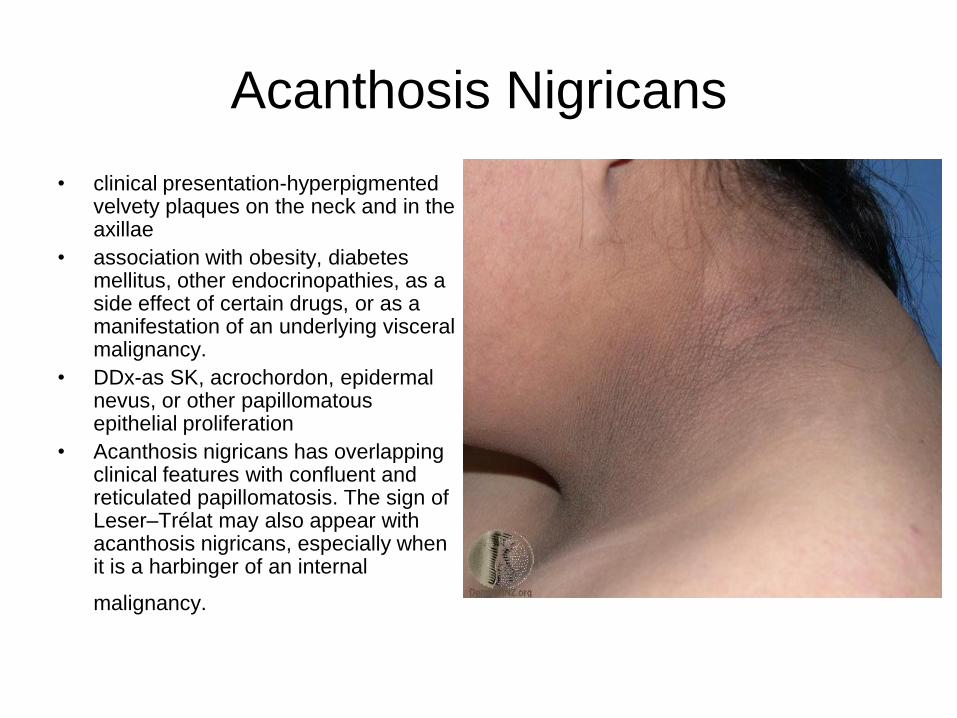
Acanthosis Nigricans
• clinical presentation-hyperpigmented velvety plaques on the neck and in the axillae
• association with obesity, diabetes mellitus, other endocrinopathies, as a side effect of certain drugs, or as a manifestation of an underlying visceral malignancy.
• DDx-as SK, acrochordon, epidermal nevus, or other papillomatous epithelial proliferation
• Acanthosis nigricans has overlapping clinical features with confluent and reticulated papillomatosis. The sign of Leser–Trélat may also appear with acanthosis nigricans, especially when it is a harbinger of an internal
malignancy.

Burns(thermal)
• 1st-Epidermis only, pain, tenderness, erythema, no blistering, Heals without scar
• 2nd-(superficial)-Epidermis and superficial dermis, Severe pain, tenderness, serous or hemorrhagic bullae, deep rubor, erosion and exudation Heals in 10–21 days with mild but variable scarring, More extensive epidermal necrosis with vertical elongation of keratinocytes, Necrotic areas may have serous crust w/neutrophils, fibrin and cellular debris, subepidermal bullae possible
• 2nd-(deep)-Epidermis and most of dermis destroyed, including deep follicular structures, Intense pain but reduced sensation, deep red to pale and speckled in color, serosanguineous bullae and erosions, may appear devitalized initially, prolonged healing time, hypertrophic scars and marked wound contracture

Burns(thermal)
• 3rd-Full-thickness epidermal and
dermal destruction, Dry, hard,
charred, non-blanching,
insensitive areas, coagulation
necrosis,small lesions heal with
significant scarring, most require
surgical correction
superficial second-degree burn

Burns(thermal)
Second degree

Burns(thermal)
3rd degree

Burns(thermal)
• definitive diagnosis of wound
depth may not be possible for the
first 24 to 72 hours because of
vascular occlusive changes
• severity of burn injuries is based
upon depth and BSA involvement.
BSA is estimated in adults by the
„rule of nines‟

Burns(thermal)
• Necrosis of the epidermis occurs in about 45 minutes at 47°C
(117°F), but only 1 second at 70°C (158°F)
• Denaturation and coagulation of cellular proteins occur in thermal
injury.
• Interstitial edema develops from altered osmotic pressure and
capillary permeability
• chemical mediators with vasoactive and tissue-destructive
properties are released, including prostaglandins, bradykinin,
serotonin, histamine, lipid peroxides and oxygen radicals
• Heat-related illness accounted for more than 8000 deaths in the US
between 1979 and 1999, and is responsible for 7% of wilderness
deaths

Burns(thermal)
• DDx-Heat cramps, heat
syncope, heat edema, heat
exhausation, heat stroke
• most important diagnostic
issue with thermal burns is the
depth of the injury
• important distinction is the
degree of neurologic
compromise
• Tx
– removal from the hot
environment, rest, rehydration,
restoration of electrolyte
balance, and evaluation of
involved systems
– assessment of
cardiopulmonary status as
well as the extent and depth
– cool compresses, cleaned
gently to remove any foreign
material, infection prevention,
– proper healing environment
Burns(thermal)
• Con‟t Tx
– Topical antimicrobial effective in burn wound care include silver sulfadiazine, mafenide acetate and silver nitrate. Silver sulfadiazine has gained wide acceptance for both pediatric and adult burn tx-absorption can lead to leukopenia.
– silver sulfadiazine produces a pseudoeschar that may interfere with burn depth assessment. Superficial wounds may require little additional therapy
– Deeper burn wounds need more aggressive therapy, the most popular approach being serial excision
– 3rd degree excised early
– Newer skin substitutes such as acellular dermal matrix (AlloDerm®), bilaminar collagen-chondroitin sulfate and silicone (Integra®) and cultured epithelial autografts are gaining popularity
Decubitus Ulcers
• An ulcer is a wound with loss of epidermal and dermal layers
• INFLAMMATION
platelets, damaged parenchymal
cells growth factors, cytokines
activate inflammatory cells, fibroblasts
vasodilation, permeability, PMNs
____________________________
PROLIFERATION
within hrs
cells detach from BM migrate
MØs phagocytize, release VEGF
granulation tissue formation
____________________________
REMODELING
fibrobalsts remold collagen matirx
strength, thickness
PATHOGENESIS
• pressure
– > 32mmHg at risk
– > 70mmHg rapid ulcer formation
– 150mmHg lying on hospital mattress
– bone : muscle interface
• shearing forces
– HOB > 30 shearing forces in sacral/coccygeal area
• friction
– dragging across bed sheets
– damage to stratum corneum
• moisture

Decubitus Ulcers
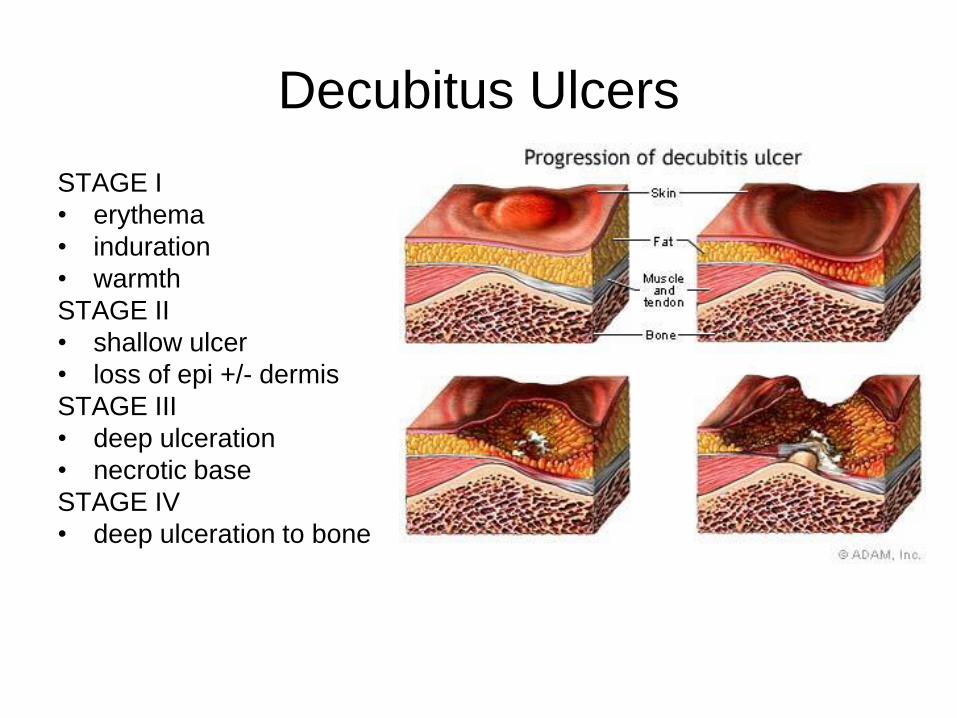
Decubitus Ulcers
STAGE I
• erythema
• induration
• warmth
STAGE II
• shallow ulcer
• loss of epi +/- dermis
STAGE III
• deep ulceration
• necrotic base
STAGE IV
• deep ulceration to bone

Decubitus Ulcers
• The US Department of Health and Human Services
reports that approximately 10% of all hospitalized
patients and 25% of nursing home patients have
pressure ulcers, most of which develop during the first
few weeks of hospitalization
• approximately 20%-at home
• 70% occur in patients over 70 years of age
• 95% on lower body, pelvic, legs
• Risk factors that predispose to the development of
pressure ulcers include prolonged immobility, sensory
deficit, circulatory disturbance, and poor nutrition

Decubitus Ulcers
• labs
– anemia/polycythemia, infection
• CBC
• ESR, CRP
– nutritional satus
• albumin/pre-albumin, transferrin/ferritin, vit A/C, zinc
– throbogenic state, vasculitis
• protein C/S, antithrombin III, lupus anticoagulant, anticardiolipin, factor V Leiden
• cryoglobulins/cryofibrinogens, RF, ANA, hep B/C
• biopsy
– r/o malignancy (Marjolin ulcer), vasculitis, panniculitis
– r/o unusual ulcer causes
– tissue culture (bacterial, mycobacterial, fungal)
• patch testing

Decubitus Ulcers
• Tx-
• nutrition
– sound nutrition essential to wound healing
– carbohydrates, fats cellular energy
– protein anabolic repair
– vitamins A, C, E
– selenium, thiamine, zinc, copper, manganese, pathotenic acid
– bariatric surgery risk
• infection
– polymicrobial
– staph, anaerobes (Pseudomonas, enterobacter)
– mycobacterial, fungal lack signs of intense inflammation
Decubitus Ulcers
• rotation q 2h
• appropirate mattress, pillows, foam wedges, booties
• stage IV surgical debridement
• debridement
– enzymatic
• controversial
• collagenase (Santyl)
• papain (Panafil, Accuzyme)
– mechanical
• wet-moist saline
• surgical
• antiseptics
– chlorhexidine, acetic acid, providone-iodine cytotoxic to open wounds
• growth factors
– topical becaplermin (Regranex) 0.01% gel
• diabetic ulcers
• black box = risk of cancer mortality with 3+ tubes
Decubitus Ulcers
• Fonder M. A. , et al. Treating the chronic wound. J Am Acad Dermatol
2008;58:185-206.
• moist environment
– wounds heal best in moist environment
– dry wounds further tissue death
– occlussive dressings infection rate
– caution in wounds with heavy exudate, macerated tissue
• semi-occlusive dressings
– semipermeable to gass, moisture
– Impermeable to liquids
– hydrogels, alginates, foams, films
Decubitus Ulcers
Pressure / Decubitus
Stage I- Film ( friction), thin Hydrocolloid
Stage II, III- Hydrocolloid, Foam, Hydrogel, Debriding agent
Stage IV- Alginate, Hydrofiber, Debriding agent
DDX- Buerger‟s Disease, Cryofibrinogenemia

Leg Ulcers
• Venous Ulcer
– Prevalence increases with age, as demonstrated by one study
which found that >85% of those affected were over 64 years of
age
– Risk factors for the development of leg ulcers include obesity
and a history of significant leg injury, deep venous thrombosis
and/or phlebitisIn addition, the factor V Leiden mutation is more
prevalent in patients with venous ulcers than in the general
population
– incidence of venous ulcers is equal in men and women
– recurrence rate can be over 70%
Leg Ulcers
• ulcer subtypes
– venous
– arterial
– neuropathic (diabetic)
– pressure/decubitus
– vasculitic
– other: infectious, malignancy, PG, NLD, vasculitic, vaso-occlusive, panniculitis, drug induced (hydroxyurea), genetic (Klinfelter)
• venous insufficiency risk factors
– obesity
– phlebitis
– DVT, factor V Leiden
– neuromuscular dyfunction
• pathogenesis
– tissue ischemia theories
• distension of capillary bed
fibrinogen leakage
capillary fibrin cuffs O2depriv
• fibrin traps growth factors
inavailablity
• white cell trapping release
collagenase, free radicals, TNF
– inappropriate wound healing

Leg Ulcers

Leg Ulcers
• Venous Stasis
• edema
– limb heaviness, aching
• stasis changes
– hemosiderin in macs, extravasated RBCs
• red-brown dusky disoloration
• petechiae
– stasis dermatitis = eczematous
• lipodermatosclerosis
– aka sclerosing panniculitis
membranous lipodystrophy
– woody induration
– inverted champagne bottle
– fibrosed sub q, arabesque bodies

Leg Ulcers
• DDx-cellulitis(acute, unilateral, erythema, induration, warmth, systemic sx)
• Venous Ulcer
– medial
– large
– along sup saphenous v.
– may involve entire
circumference
– irregularly shaped
– superficial
– yellow fibrinous base w.
beefy red tissue beneath

Leg Ulcers
Venus Ulcer
ATROPHIE BLANCHE
• aka livedoid vasculopathy
• smooth ivory white atrophic sclerotic plaques
• peripheral trelengectasias
• ulcerations of various sizes
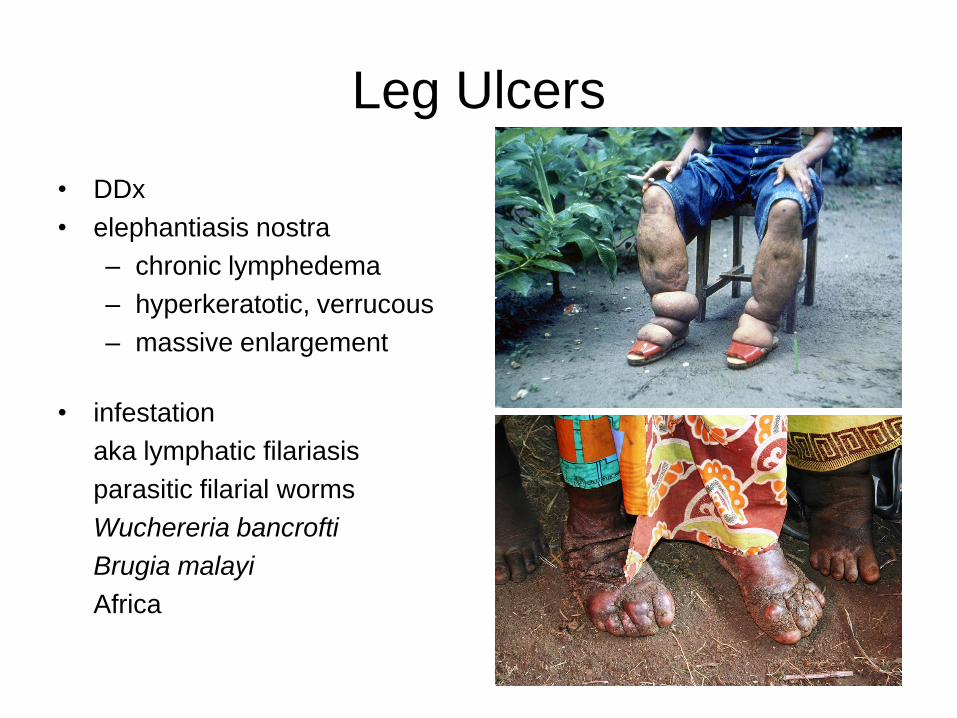
Leg Ulcers
• DDx
• elephantiasis nostra
– chronic lymphedema
– hyperkeratotic, verrucous
– massive enlargement
• infestation
aka lymphatic filariasis
parasitic filarial worms
Wuchereria bancrofti
Brugia malayi
Africa
Leg Ulcers
• Venous
• labs
– anemia/polycythemia, infection
• CBC
• ESR, CRP
– nutritional satus
• albumin/pre-albumin, transferrin/ferritin, vit A/C, zinc
– throbogenic state, vasculitis
• protein C/S, antithrombin III, lupus anticoagulant, anticardiolipin, factor V Leiden
• cryoglobulins/cryofibrinogens, RF, ANA, hep B/C
• biopsy
– r/o malignancy (Marjolin ulcer), vasculitis, panniculitis
– r/o unusual ulcer causes
– tissue culture (bacterial, mycobacterial, fungal)
• patch testing

Leg Ulcers
• venous
– compression ~40mmHg (cautionn in PAD), leg elevation
– debridement of necrotic fibrinous debris
• All other tx methods similar to that of decubitus-nutrition, infection control, wound care and dressing
• Tx underlying cause

Leg Ulcers
• Arterial
– PAD 10% in the general population over the age of 45
years
– risk factors are age >40 years, cigarette smoking and
diabetes mellitus, hyperlipidemia, hypertension,
hyperhomocysteinemia, male gender, and sedentary
lifestyle.
– Peripheral arterial disease increases the risk of death
from cardiovascular causes even in the absence of a
history of a myocardial infarction or ischemic stroke
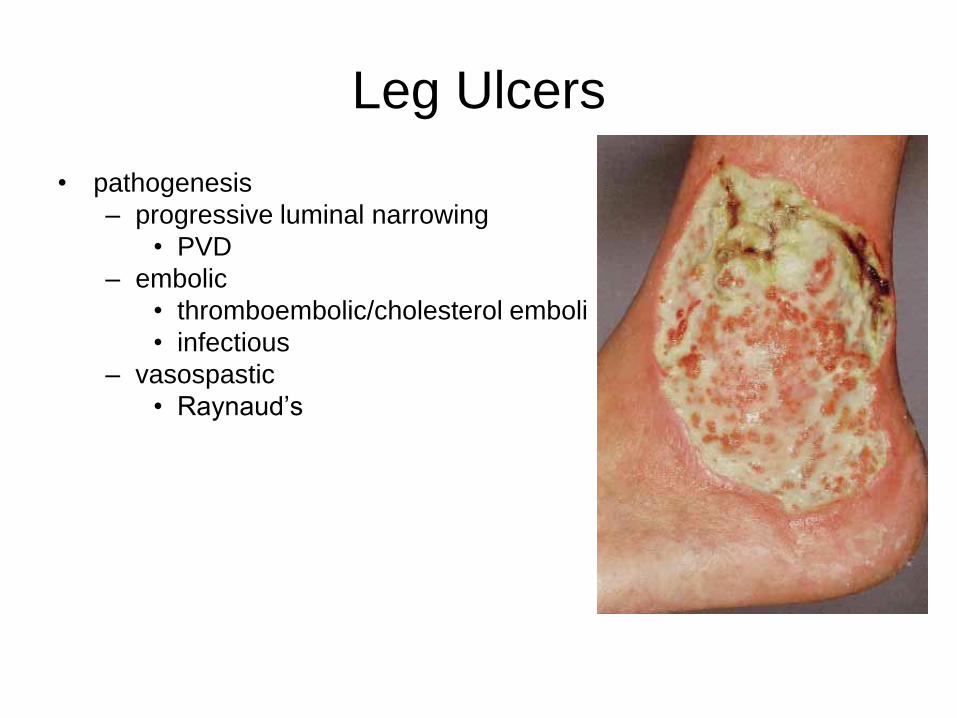
Leg Ulcers
• pathogenesis
– progressive luminal narrowing
• PVD
– embolic
• thromboembolic/cholesterol emboli
• infectious
– vasospastic
• Raynaud‟s
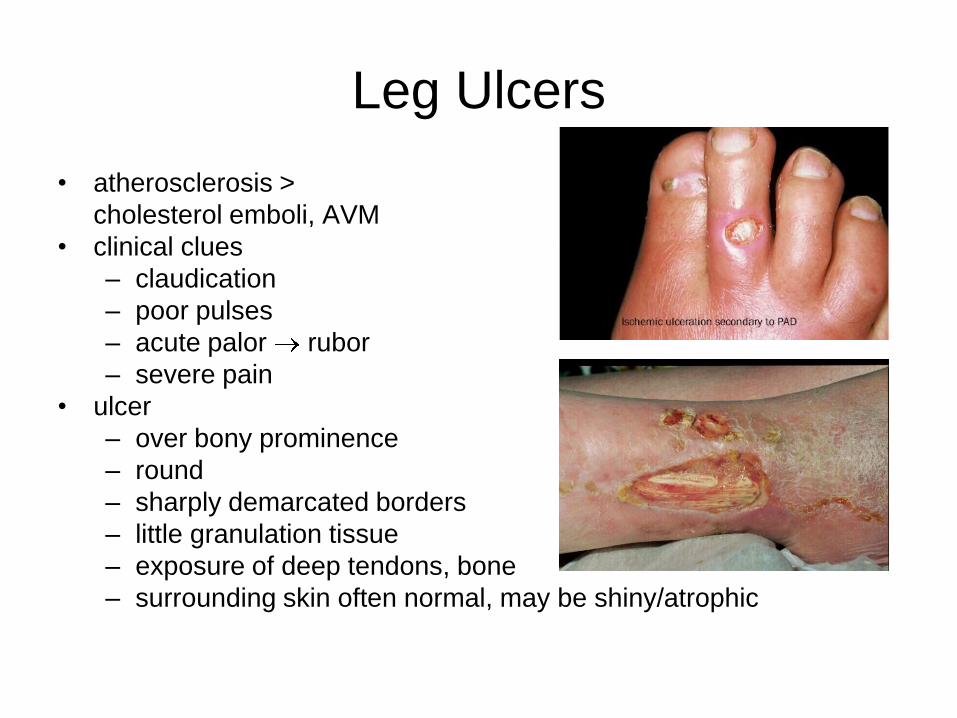
Leg Ulcers
• atherosclerosis >
cholesterol emboli, AVM
• clinical clues
– claudication
– poor pulses
– acute palor rubor
– severe pain
• ulcer
– over bony prominence
– round
– sharply demarcated borders
– little granulation tissue
– exposure of deep tendons, bone
– surrounding skin often normal, may be shiny/atrophic

Leg Ulcers
• labs
– anemia/polycythemia, infection
• CBC
• ESR, CRP
– nutritional satus
• albumin/pre-albumin, transferrin/ferritin, vit A/C, zinc
– throbogenic state, vasculitis
• protein C/S, antithrombin III, lupus anticoagulant, anticardiolipin, factor V Leiden
• cryoglobulins/cryofibrinogens, RF, ANA, hep B/C
• biopsy
– r/o malignancy (Marjolin ulcer), vasculitis, panniculitis
– r/o unusual ulcer causes
– tissue culture (bacterial, mycobacterial, fungal)
• patch testing
Leg Ulcers
• Tx-
• arterial
– angioplasty +/- bypass
• Wound care , dressings, nutrition issues similar to prev wounds

Leg Ulcers
• Neuropathic and Diabetic Ulcers
– The most common cause of neuropathic foot ulcers in the US is diabetes mellitus, 20% of the 16 million people in the US known to have diabetes will develop an ulcerated foot at some time during their lifetime
– Of these, 15-25% will require an amputation
– major cause of non-traumatic lower-extremity amputations in the US is in fact non-healing diabetic foot ulcers, which are responsible for 85% of all amputations
– Risk factors include male gender, diabetes for >10 years, poor glucose control, and associated cardiovascular, retinal or renal complications.
– Other causes of peripheral neuropathy that are associated with neuropathic ulcers include spinal cord lesions, spina bifida, alcohol abuse, medications and leprosy.

Leg Ulcers

Leg Ulcers
• combination
– peripheral neuropathy
• sensation loss trauma
• motor dysfxn foot deformities
• autonomic dysfxn dry, brittle skin
– macrovascular dz
• calcification of arteries pulse exam less reliable
• pallor on limb elevation, rubor with dependency
• shiny, atrophic skin, hair loss, onychodystrophy
– impaired wound healing
• HbA1C
– > 9% risk
– > 12% WBC fxn altered
• chemotaxis, adherence
• phagocytosis, intracellular bacterocidal activity

Leg Ulcers
Leg Ulcers
• labs
– anemia/polycythemia, infection
• CBC
• ESR, CRP
– nutritional satus
• albumin/pre-albumin, transferrin/ferritin, vit A/C, zinc
– throbogenic state, vasculitis
• protein C/S, antithrombin III, lupus anticoagulant, anticardiolipin, factor V Leiden
• cryoglobulins/cryofibrinogens, RF, ANA, hep B/C
• biopsy
– r/o malignancy (Marjolin ulcer), vasculitis, panniculitis
– r/o unusual ulcer causes
– tissue culture (bacterial, mycobacterial, fungal)
• patch testing
Leg Ulcers
• DDx-arterial, venous, other causes of peripheral neuropathy, ACD
• Tx-nutirtion, infection control
– aggressive debridement (surgical, enzymatc)
– pressure off loading
– address vascular dz
– Wound care , dressings similar to prev

EIC
• present to clinicians because of medical or cosmetic concerns, or
due to discomfort from mechanical irritation or inflammation of the
cyst
• histologic features determine the definitive diagnosis
• Can occur any where on body
• most common cutaneous cysts
• most common on the face and upper trunk
• range from a few millimeters to several centimeters in diameter
• derive from the follicular infundibulum
• multiple epidermoid cysts may occur in individuals with a history of
significant acne vulgaris

EIC
• Multiple cysts may also occur in
the setting of Gardner syndrome
(familial adenomatous polyposis)
and in nevoid basal cell carcinoma
syndrome
• Non-inflamed epidermoid cysts
are usually asymptomatic, but,
with pressure, cysts contents may
be expressed that may have an
objectionable odor
• Rupture of the cyst wall can result
in an intensely painful
inflammatory reaction, and this is
a common reason for presentation
to a physician's office
EIC
• Tx-excision is curative
• incision and expression of the cyst contents and wall
through the surgical defect
• If the entire cyst wall is not removed, the cyst may recur.
• Inflamed epidermoid cysts may require incision and
drainage,occasionally, antibiotic therapy
• Intralesional triamcinolone may be helpful in speeding
the resolution of the inflammation.
Hidradenitis Suppurativa
• targets apocrine gland-bearing skin sites
• axillae and anogenital region
• starts at or soon after puberty
• women are affected three times as often as men
• thought to represent an inflammatory disorder originating from the
hair follicle
• Rupture of the follicle allows introduction of its contents, including
keratin and bacteria, into the surrounding dermis This excites a
vigorous chemotactic response and abscess formation. Epithelial
strands are generated, possibly from ruptured follicular epithelia,
and form sinus tracts

Hidradenitis Suppurativa
• inflammatory nodules and sterile abscesses develop in the axillae, groin, perianal and/or inframammary areas
• tender and extremely painful
• sinus tracts and hypertrophic scars form
• chronic drainage, leading to a marked degree of frustration, embarrassment, self-consciousness and depression, especially when the discharge is malodorous
• discharged fluid is often a mixture of serous exudate, blood and pus, in varying proportions
• Complications include- anemia, secondary amyloidosis, lymphedema, and fistulae to the urethra, bladder, peritoneum and rectum
• Other complications include hypoproteinemia, nephrotic syndrome and arthropathy.
• Squamous cell carcinoma, sometimes with metastasis, may be an occasional complication of chronic scarring disease.

Hidradenitis Suppurativa

Hidradenitis Suppurativa
• DDx-staphylococcal furunculosis, Crohn's disease, granuloma inguinale, mycetoma and tuberculosis
• Dx- clinical, histo, infection control
• Tx-Many are successful some of the time, but none are successful all of the time
– weight reduction
– measures to reduce friction and moisture
– ILK 5mg
– topical clindamycin-Staphylococcus aureus
– 5-day courses of intranasal mupirocin are used in nasal carriers of S. aureus.
– Incision and drainage should be minimized because it may result in scarring and chronic sinus tract formation.

Hidradenitis Suppurativa
• Systemic corticosteroids (prednisone 60-80 mg/day)-improves initially then flare once d/c‟d
• Isotretinoin has not been particularly effective
• Specific systemic antibiotics are chosen on the basis of the results of bacterial cultures
• cyclosporine and TNF-α inhibitors
• Surg/exc-often not helpful

Lipomas
• benign tumors composed of mature lipocytes
• among the most common neoplasms in humans
• often solitary
• most commonly-beyond the fourth decade of life
• incidence in men to be higher than in women
• incidence of lipomas is increased in overweight individuals, diabetics, and patients with elevated serum cholesterol
• predilection are the neck, trunk, arms, proximal lower extremities, and buttocks
• round to oval, soft, mobile subcutaneous nodules with a normal overlying epidermis
• asymptomatic, unless they encroach upon and compress nerves, in which case they may be painful
Lipomas
• DDx-epidermoid cysts
• Dx-clinial and histo
• Tx-easily excised

Melasma
• common, acquired disorder, characterized by symmetric,
hyperpigmented patches with an irregular outline that occur most
commonly on the face. It is most prevalent among young to middle-
aged women who are Hispanic, Asian or of African or Middle
Eastern descent
• Exacerbating factors include pregnancy, oral contraceptives and, of
course, sun exposure
• following exposure to UV irradiation (or another inducer),
hyperfunctional melanocytes within involved skin produce increased
amounts of melanin as compared to uninvolved skin
• Potential aggravating factors include other medications (e.g.
phenytoin-related anticonvulsants, phototoxic drugs) and
autoimmune thyroid disease

Melasma
• Light to dark brown or brown–gray patches with irregular
borders appear primarily on the face
• three classic patterns–centrofacial, malar and
mandibular
• Additional sites of involvement include the extensor
forearms and the mid upper chest
• fade during the winter months and they frequently either
first appear or are accentuated following exposure to UV
irradiation or during pregnancy
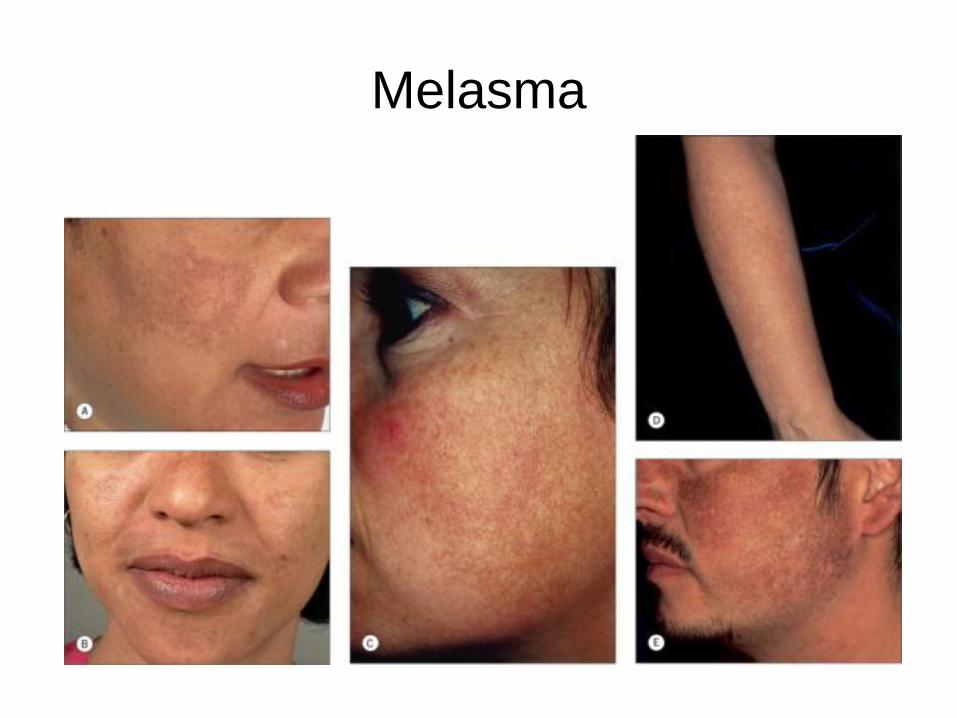
Melasma

Melasma
• DDx-Drug-induced hyperpigmentation or discoloration, Postinflammatory hyperpigmentation, Actinic lichen planus, Lichen planus pigmentosus, Lichen planus pigmentosus, Pigmented contact dermatitis, Exogenous ochronosis, Acquired bilateral nevus of Ota-like macules (Hori's nevus), Erythema dyschromicum perstans
• Dx-hx, clinical, possible bx
• Tx-sun protection, broad-spectrum sunscreens w/o all tx will fail
• While epidermal pigmentation is somewhat amenable to topical therapies and chemical peels, dermal pigmentation is notoriously difficult to treat.
• hydroquinone (2-4%), tretinoin (0.05-0.1%) and a corticosteroid (class V–VII)
• topical lightening include glycolic acid, kojic acid (a tyrosinase inhibitor), and azelaic acid (15-20%; also an inhibitor of tyrosinase)
• Salicylic acid and glycolic acid peels can be used as adjunctive therapy
• Deeper chemical peels, laser therapy (e.g. Q-switched ruby)
Vitiligo
• acquired, idiopathic disorder characterized by circumscribed
depigmented macules and patches
• 0.5-2% of the general population worldwide
• age of onset is approximately 20 years
• absence of functional melanocytes
• autoimmune theory proposes that alterations in humoral or cellular
immunity result in the destruction of melanocytes
• most common form of vitiligo is a totally amelanotic macule (or
patch) surrounded by normal skin
• fairly discrete margins, and they are round, oval or linear in shape
• Lesions enlarge centrifugally over time, but the rate may be slow or
rapid

Vitiligo
• face, dorsal aspect of the hands,
nipples, axillae, umbilicus,
sacrum, and inguinal and
anogenital regions.
• Typically, facial vitiligo occurs
around the eyes and mouth (i.e.
periorificial), and on the
extremities it favors the elbows,
knees, digits, flexor wrists, dorsal
ankles and shins

Vitiligo
• Localized
– Focal: one or more macules in one area, but not clearly in a segmental distribution
– Unilateral (segmental): one or more macules involving a unilateral segment of the body lesions stop abruptly at the midline
– Mucosal: mucous membranes alone
• Generalized
– Vulgaris: scattered patches that are widely distributed
– Acrofacial: distal extremities and faceMixed: various combinations of segmental, acrofacial and/or vulgaris
• Universal
– Complete or nearly complete depigmentation

Vitiligo

Vitiligo
• case-by-case basis is unpredictable
• Associations:
– IDDM
– Pernicious Anemia
– Grave‟s Disease
– Hashimoto‟s Thyroiditis
– Addison‟s Disease
– Alopecia areata
• DDx-chemical leukoderma, the leukodermas associated with melanoma or scleroderma, postinflammatory depigmentation, and the late stages of treponematosis or onchocerciasis, postinflammatory hypopigmentation, pityriasis (tinea) versicolor, or other cutaneous infections (e.g. leprosy). Prior treatment with potent topical corticosteroids can also lead to hypomelanosis.

Vitiligo
• Tx
– NB-UVB, PUVA, TCS-for small localized, 0.1% tacrolimus ointment,
Minigrafting is the simplest method, 20% monobenzyl ether of
hydroquinone (MBEH), applied once to twice daily to the affected areas
for 9-12 months or longer
– MBEH is a potent irritant and/or allergen, and an open use test should
be performed before more widespread application(only for small area of
normal pigment)

Urticaria
• recurrent whealing of the skin
• pruritic, pink or pale swellings of the superficial dermis that may have an initial flare around them
• Lesions may be a few millimeters in diameter or as large as a hand, and numerous or single.
• Hallmark-individual lesions come and go w/in 24 hours
• as high as 30% in the general population
• Urticaria is a worldwide disease and may present at any age.
• The peak incidence depends on etiology
• female:male ratio of approximately 2:1 for chronic urticaria
• mast cell is the primary effector cell of urticaria
• Mast cell granules contain preformed mediators of inflammation, the
most important of which is histamine

Urticaria
• Immunologic
– Autoimmune (autoantibodies against FceRI or IgE)
– IgE-dependent (allergic)
– Immune complex (vasculitic)
– Complement- and kinin-dependent (C1 esterase inhibitor def)
• Non-immunologic
– Direct mast cell-releasing agents (e.g. opiates)
– Vasoactive stimuli (e.g. nettle stings)
– Aspirin, other non-steroidal anti-inflammatory drugs, dietary
pseudoallergens
– Angiotensin-converting enzyme inhibitors
Urticaria
• important to distinguish urticaria from urticarial dermatoses, such as
urticarial drug eruptions, eosinophilic cellulitis and bullous
pemphigoid
• „here today and gone tomorrow‟ (i.e. they last less than 24 hours)
• Wheals may be small or large, single or multiple
• Classification
– Ordinary urticaria (all urticaria not classified below)
– Physical urticarias
– Urticarial vasculitis (defined by vasculitis on skin biopsy)
– Contact urticaria (induced by percutaneous or mucosal
penetration)
– Angioedema without wheals
– Distinctive urticarial syndromes
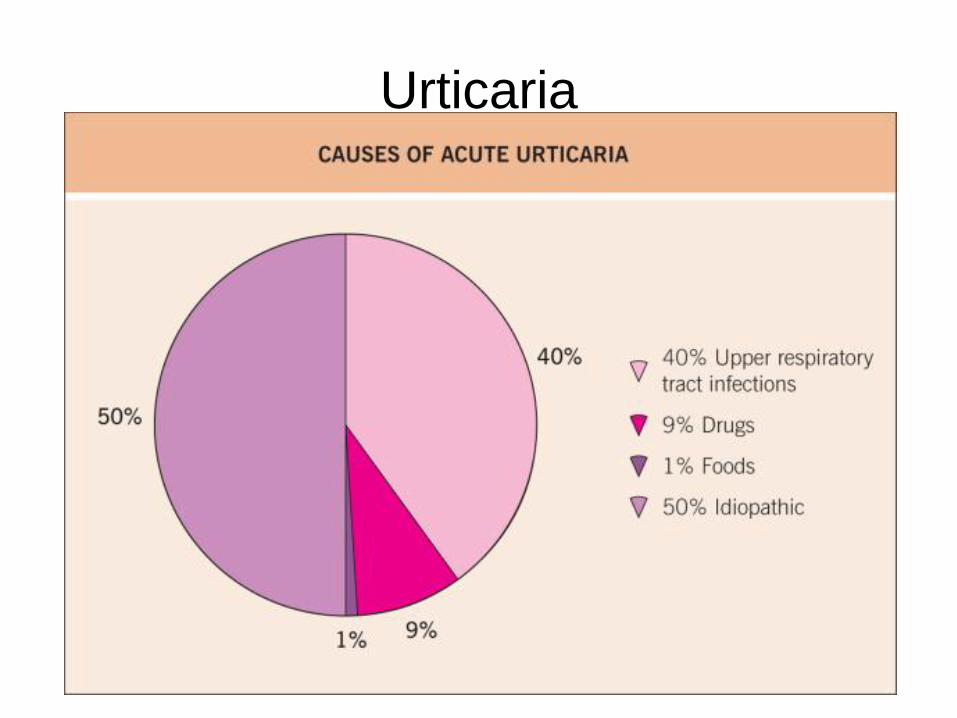
Urticaria

Urticaria
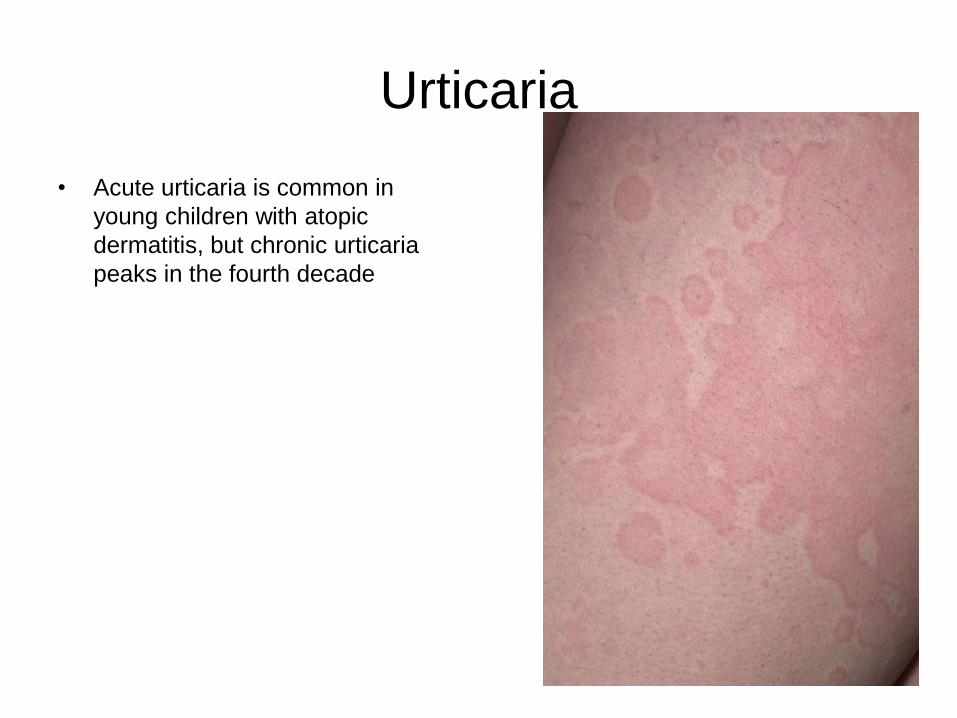
Urticaria
• Acute urticaria is common in
young children with atopic
dermatitis, but chronic urticaria
peaks in the fourth decade

Urticaria
• Chronic– Autoimmune
• Thyroid ds
• Vitiligo
• Insulin-dependent diabetes
• RA
• Pernicious anemia
– Infectious
• H. Pylori
• Parasitic infection
• Gastric anisakiasis simplex
• Dental infection
• G.I. Candidasis

UrticariaCold urticaira

Urticaria
dermatographism

Urticaria
Pressure urticaria
Urticaria
• Urticarial vasculitis
– >24 hours
– Histo will show LCV
– Choose newest lesion when performing bx
– Causes-hep b,c, SLE, sjorgrens, lyme ds, infectious
mononucleosis, Drugs(cimetidine, diltiazem)

Urticaria
• DDx
– insect bite reactions (papular urticaria), acute febrile neutrophilic
dermatosis (Sweet's syndrome), pre-bullous pemphigoid (i.e.
urticarial bullous pemphigoid), acute facial contact dermatitis,
urticarial drug reactions (e.g. antibiotics)
• Dx
– comprehensive history and phys exam is essential
– CBC, ESR, ANA, bx,
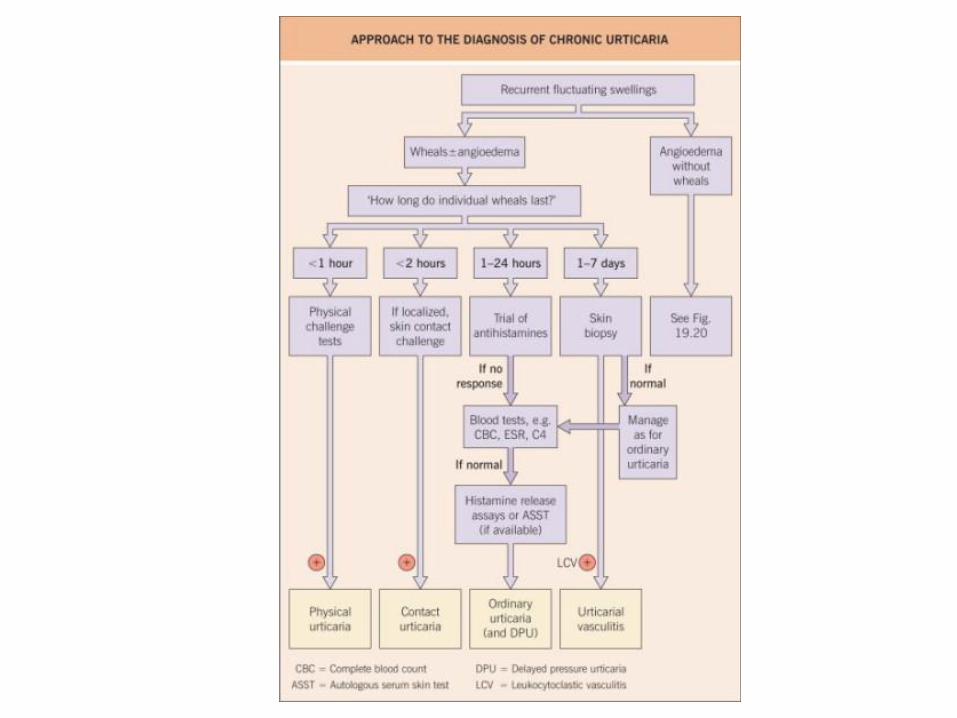
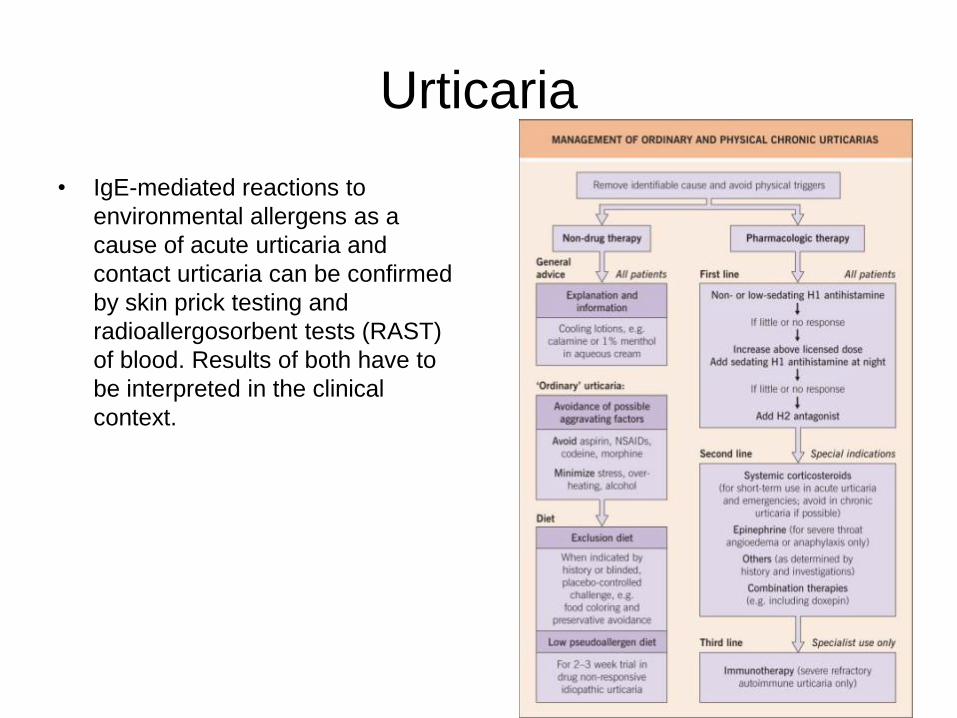
Urticaria
• IgE-mediated reactions to
environmental allergens as a
cause of acute urticaria and
contact urticaria can be confirmed
by skin prick testing and
radioallergosorbent tests (RAST)
of blood. Results of both have to
be interpreted in the clinical
context.

Urticaria
• Tx-1st line antihistamine
• Classic (sedating)
– Chlorpheniramine -4 mg tid (up to 12 mg at night)
– Hydroxyzine-10–25 mg tid (up to 75 mg at night)
– Diphenhydramine-10-25 mg at night)
– Doxepin-10-mg at night
• 2nd gen
– Acrivastine-8 mg tid
– Cetirizine-10 mg once daily
– Loratadine-10 mg once daily
– Mizolastine-10 mg once daily

Urticaria
• Newer 2nd gen
– Desloratadine-5 mg once daily
– Fexofenadine-180 mg once daily
– Levocetirizine- 5 mg once daily
• H2 antagonist
– Cimetidine-400 mg bid
– Ranitidine-150 mg bid
Topical Corticosteroids
• Superpotent(1)
– dermatoses resistent to intermediate or high potency TCS,
– avoid extensive app(>50g weekly),
– for short term use only(2-3 weeks at a time),
– Do not use on the face, axillae, submammary area or groin,
– avoid use in infants and children under 12,
– best for thick lichenified or hypertrophic skin
• High(2&3)
– Severe
– Avoid ext use(>50g weekly)
– Short term use(2-3 weeks at a time)
– Do not use on the face axillae, submammary are or groin
– Avoid use in infants and children under 12
– Best for thick, lichenified or hypertrophic skin

Topical Corticosteroids
• Intermediate(4&5)
– Moderate
– Best for short term tx of extensive dermatoses
– Avoid extended use(>1-2 weeks in infants and children
– Best on trunk and ext
– Safer for short term use on thin skin
• Low(6&7)
– Steroid sensitive
– Preferred for large areas
– Best if long term tx required
– Best choic for face, axilla, groin, and other occluded
– Infants and children
– Best for thin skin

Topical Corticosteroids