designing babies: what the future holds - · pdf filedesigning babies: what the future holds...
TRANSCRIPT

- Vol 10, Supp I. 2005 24-26 Reproductive BioMedicine Online: www.rbmonline.com/Article/1638 on web I December 2004
Designing babies: what the future holds
Dr Yury Verlinsky is a graduate, postgraduate and PhD ot Kharkov University of the tormerUSSR, His research interests include cytogenetics, embryology and prenatal andpreimpiantation genetics. He introduced polar body testing for preimpiantation geneticdiagnosis and developed the methods for karyotyping second polar body and individualblastomeres. He has published over 100 papers, as well as three books on preimpiantationgenetics.
Yury Verlinsky
Reproductive Genetics Institute, 2825 North Halsted Street, Chicago, IL, 60657 USACorrespondence: e-mail: [email protected]
AbstractAdvances in reproductive technology have opened new opportunities to avoid inherited diseases in offspring. Thepreimpiantation genetic diagnosis (PGD) of human embryos permits those embryos carrying gene disorders or a non-diploidchromosome con,stilution to be identified. Numerous disease genes including those with a late onset have been identifiedand the conditions averted in children. Risks of abortion have been reduced, and the incidence of live births raised afterPGD. It is also possible to select embryos with human leukocyte antigens (HLA) identical to those of a sick elder sibling.and then use stem cells from cord blood at birtli to supply the necessary therapy. This form of treatment has alleviated theinherited disease in many recipients. The outlook and ethics of this approach to the alleviation of human disorders arediscussed.
Keywords: assisted human reproduction, designer babies, HLA typing, preimpiantation genetic diagnosis
IntroductionThere are many and various debates on the ethics of thetechniques and technologies I will introduce here, 1 was askedto speak about human designer babies. The background of theterm "designer" baby has t?een initiated by journalists and notby scientists to describe several different reproductivetechnologies. These technologies have one thing in common.They give the parents more control over the characteristics oftheir offspring than other forms of conception. The problem iswhether it is ethical for doctors and parents to design babies byselecting or altering an embryo and bring it to a full-term fetus.Should this procedure be made illegal? Should there be limitsto such practices? And what exactly are the differenttechniques for designing babie.s?
Unfortunately, the term is very imprecise and it is diffieult tountangle its various meanings in the public mind. It can meanvarious things. Human embryos can be assessed for variousdisorders or for unknown diseases. The sex of a child at birthcan be prearranged by choosing embryos for this specificsexual trait. Genetic testing ean be done for therapeutic or forcosmetic reasons. All these features come out of one basket.and this raises the nature of the argument for designing the
babies, it can help to prevent certain genetic diseases, soreducing the financial and emotional strains on the parents ifthey want the best for their children. Why shouldn't we usethis technology? As of today, these techniques are used only bythose parents who need the help of a fertility clinic to havetheir children. Since they are investing so much time, energy,money and effort to have a baby shouldn't they have a healthyone? In any case, a great number of naturally conceivedembryos are rejected naturally because of their disorderedgrowth. Many such defects can also be identified by scanningembryos in their preimpiantation development. They maysimply be discarded if it is discovered that their inheritance canlead to anomalous forms of growth. In such cases, we arereplacing Nature, who routinely takes care to reject such cases.
Argurnents against designing babies could lead to objectionsabout our attempting to produce healthy babies. Once we startdown the slippery slope of eliminating embryos because theyare diseased, whal is to stop us from choosing babies for theirphysical, physiological or psychological traits? There isalways a looming shadow of eugenics, involving the practiceof improving the human gene pool by eliminating undesiredembryos. This motivation has. in the past, spurred somegovernments in Europe and in the US to use various methods
Ethics. Law and Moral Philosophy of Reproductive Bionietlicine. Vol. I. No. I. March 2tXI5© 2005 Rcpri'diiciivc Healthcare LimitedPublished by Reproductive Healthcare Limited
Ethics - Designing babies - ¥ Verlinsky
sueh as modifying fertilization, selective breeding and racialhatred to apply such eugenic systems to their eitizens. Onthe other hand, could we breed races of supermen? Who isto criticize the various sources of genetic enhancement? Willthis new technology only be available to the wealthy, whowill hence avoid problems infiicted on lower classes due totheir suffering from inherited disabilities and diseases?Worst of all, will the discrimination against people alreadyborn with such a disability increase as they are perceived asgenetically inferior?
Economic factors and pressures might also come to have asignificant role in making choices regarding the nature ofcharacteristics in newborn babies. Insurance companies, forexample, may refuse to cover newborn malformations thatcould have been corrected before implantation. They mayalso have concerns over parents designing their child.Widespread concerns apply to such matters, whieh beganwhen transferring the process of procreation from home tothe laboratory and turning it into a sort of manufacturingprocess, Whal is happening in this field today is highlypractical and possible, while everything whatever that wassaid before is now just simply speculation. Deeper questionsmust be answered about this new and burgeoning field. Havewe really designed anybody? The answer is no. Have wereally designed anything? The answer is yes. What have wedesigned? PGD is a medical diagnostic procedure allowingthe design to avoid the pregnancy with congenital disease. Isthere a need to apply it? It can offer an alternative to prenataldiagnosis. If this i.s not done by PGD. it can be achieved onlyby aborting the afflicted fetuses.
What is bringing us to enlarge our programmes of PGD, andwhat advantages does it give us? Data from our centre usingPGD to identify trans locations before implantation showedthat PGD contributes to a sevenfold reduction of abortion ratesfor the same group of patients, improving the number ofpatients taking healthy babies home tremendously: fiO'/r of ourpatients delivered a normal baby, healthy and free of thefamilial impairment. There is also another benefit of PGD ascompared with prenatal diagnosis performed for pre-existingMendelian disorders. We performed PGD for 92 single-genedisorders covering various types of different mutations. Bynow, we have performed 360 cycles for single-gene disordersand have achieved embryo transfer in 90% of these eases.Currently, we have established 195 pregnancies. Expandingapplications of PGD are possible, and decisions must be takenabout ethical approval to use PGD rather than prenataldiagnosis, such as in PGD for genetic predisposition for late-onset disorders, as It is doubtful if termination of pregnancywill be acceptable after prenatal diagnosis identifies that thebaby carries such disorders.
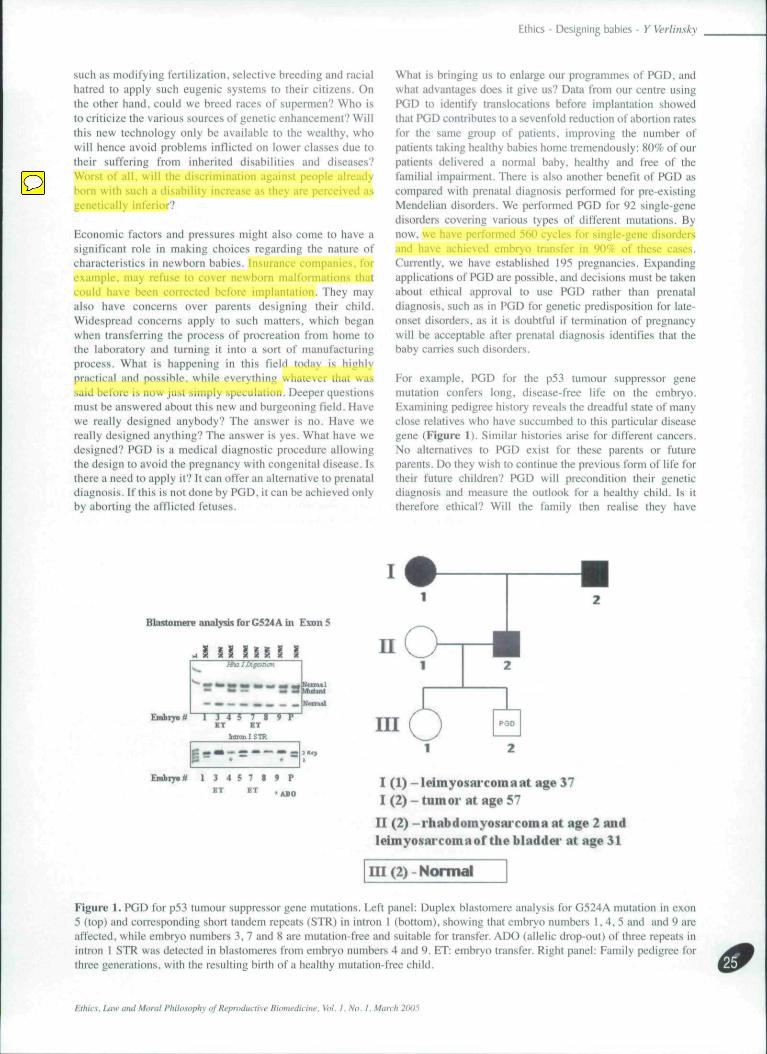
For example, PGD for the p53 tumour suppressor genemutation confers long, disease-free life on the embryo.Examining pedigree history reveals the dreadful state of manyclose relatives who have succumbed to this particular diseasegene (Figure 1), Similar histories arise tor different cancers.No alternatives to PGD exist for these parents or futureparents. Do they wish to continue the previous form of life fortheir future children? PGD will precondition their geneticdiagnosis and measure the outlook for a healthy child. Is ittherefore ethical? Will the family then realise they have
BlastoRiere analysis for C524 A in Exon5
A i
-
S
-
1
-Embryo*^ 1 J 4 5 7 * 9 P
ET BT
Embiyntf 1 3 4 5 7 I 9 PBT ET . . « „ I (1) -leimyosni'comaat »ge 37
I (2) - tumor lit nge 57n (2) -rhabdomyosHi'coma at age 2 aiidleimyosai'comaof Uiebladdei- at age 31
HI (2)-Normal
Figure 1. PGD for p53 tumour suppressor gene mutations. Left panel: Duplex blastomere analysis for G524A mutation in exon5 (top) and corresponding short tandem repeats (STR) in intron t (bottom), showing that embryo numbers 1.4.5 and and 9 areaffected, while embryo numbers .1, 7 and 8 are mutation-free and suitable for transfer, ADO (allelic drop-out) of three repeats inintron I STR was detected in blastomeres from embryo numbers 4 and 9. ET: embryo transfer. Right panel: Family pedigree forthree generations, with the resulting birth of a healthy mutation-free child.
Ethics, IMW and Mural Philosophy of Reproductive Biomedicine. Vol. I. No. I. March 2005
Ethics - Designing babies - Y Verlinsky
moditled pedigrees in their more distant family to avoid thelreqiieneies of children with these inherited conditions'? A familyciirryingagene for early onset disease may already have a siblingwtio is affected by a disease gene at the age of 33 and 42. In thissituation, the family had decided to have etiildren, but when thetime comes ttiey may regret theirehoiecTtxiay, they donot haveto have lo deliver sueh children with severe inherited disorders.The choice is up to them. They could move to PGD and tiave twoor three healthy children without risk of disease. Who sees anyethieal problem with that? One might think that a mother whosefamily has been rigorously aftccted with a specillc inheriteddisease and had to face it herself is in a belter position to decide.
Surely it is a kinder moral attitude for parents while in theiryounger or middle ages to spare their children from such aterrible fate. The mother would certainly know what sueh a lifeinvolves. Some fonns of designing babies olTer longer, healthier,more pteasant lives. The presence of a disease gene in a child,and the feiuful knowledge that a parent also carries it, has beenremoved by PGD for the whole of their life.
Another and quite different PGD approach involves alleviatingdisease and death in a young memtx:r of the family. Thisoccurred with a family who arc now very well known to have[reated one of their children using stem cells from a laternewbom baby. It involved diagnosing embryos for transfer thathad a specific set of genes. This set would not include iuiy diseasegenes in the family. The embryo was also typed for its HLAantigens to ensure its cord blood could be taken at birth andinjected into a matched sick sibling. Cord blotxt is well known tobe full of stem cells. In this case, the embryos had been sclcclcdas being free of Fanconi anaemia and HLA-matched with thoseof the sick sibling called Molly (Verlinsky et al., 2001). Mollyhad Fanconi anaemia, was very ill, and cord btood .stem cellsfrom her newborn PGD sibling could save her life. Otherwise,she would soon be dead. After this treatment, her life, iind that ofthe newborn donor, will be continuous and free of disease.
A British couple was also treated in a similar manner. This timea younger child saved the life of an older one who hadDiamond-Black fan anemia (Verlinsky et al.. 2(K)4). WithoutPGD, the piirents had no choice, except for a horrible life for theirehiid while they tried using natural conception to have anotherbaby matching their sick child and hopefully helping to save itslife. The chances of saving it in these circumstances would havetwen very low. The couple applied to the UK Human Fertilisationand Embryology Authority (HFEA), who did not give approvalfor the PGD to he carried out in UK. Hence, they came to ourChicago latxjratory to use the approach of designer babies. Asuccessful treatment was achieved for ihis couple and their eldersibling was safe. The HFEA, the British fertility watchdog,announced very recently that it will broaden the rules on embryoscreening to allow of birth of designer babies for wider cures ofsick siblings. Our clinic has received increasing numbers ofrequests for HLA typing with PGD throughout the whole of thisyear.
There is also another wider application for PGD in assistedreproduetive technology: considerably improving pregnancyrates iind substantially reducing spontaneous abortion rate. Thisis our goal at present and it involves scoring the numtx;r ofchromosomes in embryos before they are transferred to theirmothers. According to our data, the reproductive history of
couples prior to PGD showed an abortion rate of 68*5!- afternatural conception, or IVF not involving PGD. In contrast, theirabortion rate after PGD was reduced to 28.4%, improvingimplantation and take home baby rate, which was 70.7% afterPGD, compjired with 32% in the same group of patients prior toPGD. It is of interest that PGD also reduces considerably thefrequency of multiple pregnancies, as by avoiding the transfer ofchromosomally abnormal embryos we can now transfer oneembryo or a maximum of two to decrease the possibility ofmultiple births. So we have gained many benefits byimplementing PGD in our IVF practice. Overall, we have carriedout 3(XX) PGD cycles, which resulted in >6(K) pregnancies and>450 babies bom free of disease.
A dynamic future?What is the future? In a recent article in the London Times (29September 2004) about stem cell therapy, it was stated that DrWilmut has received permission to clone human embryos withgenetic disorders in order to be able to develop the possibletreatment. We have a difterent approach. We created a repositoryof human embryonic stem cells, including some carrying varioustypes of inherited disease (Verlinsky era/., 2005). Many of themare derived from afflicted embryos iind were donated by patientswho did not wish to have them for transfer. So we have theirpermission to create stem cell lines, which will pmvide a sourceof cells helping to create new therapies for existing disease. Ithink this is one of the ways to go. Other different and equallyprovocative approaches are also being proposed. For example,we could make t>etter human beings by knowing how to addgood genes to iheir embr\'os. Should we do this - what is wrongwith it? It is a complex question to ask.
How far can this technology take us? Will technology inevitablylead to a world of human tieings who arc partly man-made?Suppose parents could add 30 poinis to their children's IQ. Whowould want to do it? And if parents did not. would their childrenhave a low IQ as compared with other treated children in theneighbourhood? A final point. We know now how ptiwerful genetherapy ean tx". We can turn monkeys into workaholics. Maybesome employers would like to pul in an application fomi. Iwould.
References
Verlinsky Y, Rechit.sky S. Schoolcraft W et al. 2001 Preimplantationdiagnosis for Fanconi anemia combined with HLA matctiing.Jourmil of the Airn'riciin Mciiiiul Association 2S5. 3130-3 i 33.
Verlinsky Y, Rec!iit.sky S, Sharapova T el al. 2004 PreiinpiantationHLA typing. Journal of ihe American Medical Association 291,2079-3085.
Veriinsky Y. Strelchenko N. Rectiitsky S et al. 2(K)3 Humanembryonic stem ccli lines with genetic disorders. ReproductiveBioMedicine Online 10. 105-110.
Received 18 November 2004; refereed and accepted 19November 2004.
Ethics. IMW and Moral Philiisophy i)f Repniduviive Biomedicine. Vol. I. No. I. March 2005
